52
The Management of Seizure Disorders

The Management of Seizure Disorders

Prevalence of Seizure Disorders
• General US Population: – 8% of Americans will experience at least 1
seizure in their lifetime
• Recurrence Rates:– 23-80% will have a recurrence within 5 yrs
• Bimodal distribution– peak onset at newborn-younger age groups,
then again in patients > 65

What is the difference between convulsions and seizures?
• Convulsion – forceful involuntary contraction or spasm of voluntary muscles
– the physical manifestation of a seizure in the brain
• Seizure– uncontrolled, synchronized electrical discharge of neurons
within the brain which interferes with normal function
• Epilepsy– chronic disorder diagnosed after 2 or more seizure episodes
characterized by paroxysmal, transient disturbances of brain function

Seizure Manifestations
• Abnormal firing is the result of changes occurring within these cells:
– increased excitability
– decreased inhibitory processes
– interference with normal metabolic processes
– propagation of abnormal firing along pathways

Kindling Theory
The kindling hypothesis in epileptogenesis. Adapted from Lynch MW
et al. Curr Opin Neurol. 1996;9:97-102.

Mechanism of Seizure Spread
• Ion channel problems
• Decreased inhibition
• Reduction in excitation
• Alteration in extracellular potassium/calcium

Ion Channel Problems
• Alteration in neuronal membrane function due to changes in voltage-regulated ion channels in neuronal membranes
• Lead to excess depolarization or excess action potential firing
• AEDs may reduce repetitive firing of neurons by producing a use-dependent blockade of sodium channels– carbamazepine, phenytoin, lamotrigine
• These allow normal frequency of nerve firing and inhibit abnormally fast rates of discharge by increasing time the
inactiviation gate of the sodium channel is closed
Decreased Inhibition
• Allows excessive neuronal firing to occur thus
acting as a site for genesis and spread of discharge
• GABA - major inhibitory neurotransmitter in the
forebrain
• GABA opens receptor-operated chloride channels
that lead to hyperpolarization and make epileptic
firing less likely
• BDZs, barbiturates, valproic acid

Reducing Excitation
• Excitatory neurotransmission is mediated through glutamate or related compounds
• NMDA receptor is predominantly involved in high frequency discharges
• AEDs which effectively block the NMDA receptor could reduce focal epileptogenesis, slow synchronization of the discharge or slow/block spread of seizure
Extracellular Changes
• Extracellular concentrations of potassium and calcium decrease during a seizure
• Causes greater excitability of neurons and may promote seizure initiation or spread
• Phenytoin suppresses epileptic discharges in an altered ionic environment, therefore it is more effective in epileptic tissue than in normally functioning brain areas

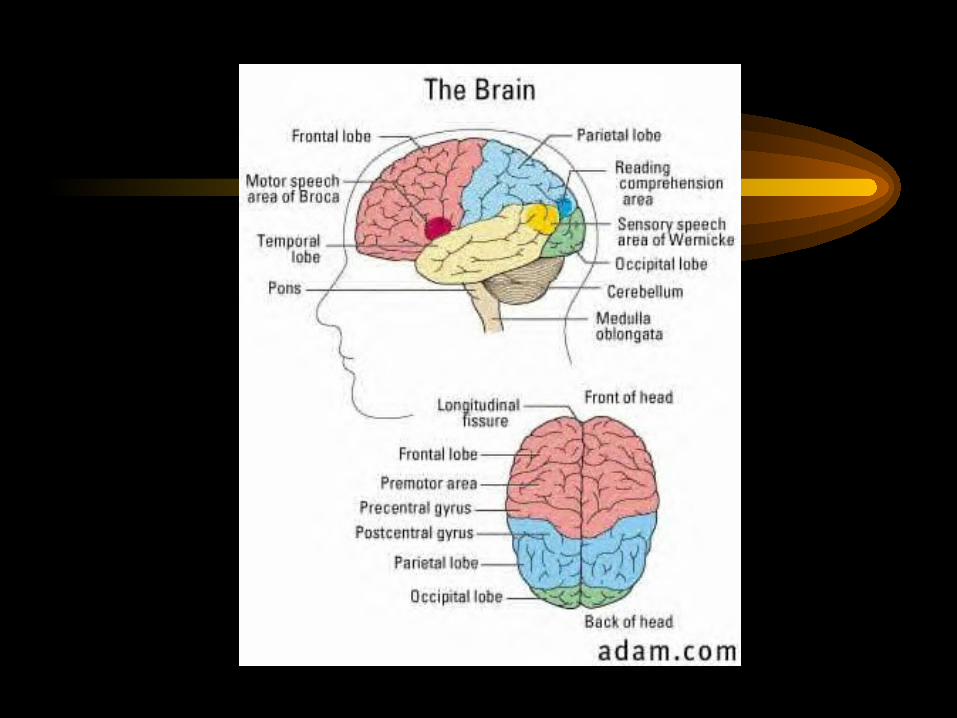
Seizure Manifestations
• Depend on portion of the brain affected
• Seizures occurring in the frontal or parietal lobe result in manifestations on the contralateral side
• R frontal left arm
• L parietal R face
• Temporal auditory
• Occipital visual
Signs and Symptoms of Seizure
• Incontinence• Movement Disorders• Falls• Memory Loss• Loss of attention• Headache• Scalds, bruises
• Tongue laceration• Chipped tooth• Sensory changes
– smell
– taste
– sight
– sound

Differential Diagnosis
• Cardiac syncope
• Transient ischemic attacks
• Meniere’s syndrome
• Psychiatric disorders

Seizure Precipitants
• Head trauma• CV Disease• Sleep deprivation• Stress• Hormonal changes
– menses, pregnancy, puberty
• Metabolic disorders• Anatomic abnormalities
– Tumors/neoplasm
• Genetic traits• Infectious processes• Medications• Alcohol withdrawal
Conditions that lower the seizure threshold:

Metabolic Disorders Precipitating Seizures
• Hypoglycemia
– more likely to occur when Glu < 30mg%
• Hyponatremia - Na <115mEq/L
• Hypernatremia - Na > 160mEq/L
• Hypocalcemia - Ca < 2.5mEq/L

Medications Associated with Seizures
• Amphetamines
• Bupropion
• Clozapine
• Cocaine
• Diphenhydramine
• Haloperidol
• Imipenam/cilastin
• Isoniazid
• Lithium
• Loxapine
• Meperidine• Metronidazole• Molindone• MAO inhibitors• PCNs• Phenothiazines• Pseudoephedrine• Theophylline• Thioxanthines• Tramadol• TCAs

Assessment of Seizures
• Complete & document ASAP following event• First clinical signs• Duration of seizure event• Order of body parts involved• Eye position, pupil size and reactivity• Movement type and side involved• Breathing pattern• Postictal behavior

How are seizures classified?
• Clinical & electrophysiologic
manifestations
• Focal point of origin in the brain
• Level of consciousness
International Classification of Seizures
• Partial Seizures – Simple Partial Seizures
– Complex Partial Seizures
– Partial Seizures evolving to Secondarily Generalized Seizures
• Generalized Seizures– Absence, Myoclonic, Clonic, Tonic, Tonic-Clonic,
Atonic
• Unclassified

Partial Seizures
• Seizures begin locally• Simple Partial
– without impairment of consciousness
– frequency = 10%
• Complex Partial– with impairment of consciousness
– frequency = 35%
• Secondarily generalized– partial onset evolving to generalized tonic-clonic
– frequency = 10%


Generalized Seizures
• Bilaterally symmetrical and without local onsetType Frequency– Tonic-Clonic (Grand Mal) 30%– Absence (Petit Mal) 10%– Myoclonic– Clonic– Atonic– Infantile spasms


Status Epilepticus • Prolonged seizure of any kind without recovery period of
consciousness between attacks• > 30 minutes of continuous seizure activity• Experienced by 1-7% of patients with previously
diagnosed epilepsy, may be as high as 42%• Causes:
– noncompliance with AED therapy, withdrawal of AED therapy
– metabolic changes
• Risk increases with:– stroke, tumor, trauma, infection

Status Epilepticus
• Muscular contractions and hypoxia can cause lactic acid
release causing sever acidosis, hypotension and shock
• Excessive heat is generated and may correlate to severity
of brain injury
• Airway obstruction and increase in salivation can cause
aspiration pneumonia
• May result in decrease in cognitive function and
prolonged SE may cause neuronal death


Management of Acute Seizure Activity
• Protect from injury, move furniture
• Turn head to side to prevent aspiration
• Insure adequate airway
• Loosen restrictive clothing
• Do Not Place Anything in the Mouth!
• Get emergency help if seizure persists
• Document the event

If you witness a seizure ...

Management of Seizures
• Define seizure type
• Assess drug efficacy
• Consider drug side-effect profile
• Account for patient-specific factors
• Consider dosage form availability
• Compliance
• Cost $$$


Goal of Therapy
• Ideally = eliminate seizures• Realistically = control or reduce the frequency,
minimize adverse effects, optimize the quality of life• When assessing efficacy of regimen consider:
– seizure severity
– frequency reduction
– duration of seizure-free periods
– extent of side effects
– patient’s acceptance of regimen

1. Therapy should be initiated with a single AED based on
seizure type, MOA and adverse effects
2. Dosage should be titrated to optimize seizure control and
minimize side effects
3. If first agent fails, begin another agent from the initial
therapy group
4. Alternative agents and polytherapy are reserved for
patients who fail monotherapy
Management of Seizures
Management of Status Epilepticus
• CBC, electrolytes• IV Glucose, Thiamine• Lorazepam 2-4mg • Diazepam suppository• Phenytoin or Fosphenytoin• Phenobarbital• Midazolam and Pentobarbital• Identify Precipitating Factors

Primary Antiepileptic Agents
• Benzodiazepines
– Clonazepam
– Diazepam
– Lorazepam
• Carbamazepine
• Oxcarbazepine
• Ethosuximide..Absence seizure
• Felbamate
• Gabapentin….neuropatic pain.
• Lamotrigine
• Levetiracetam
• Phenobarbital
• Phenytoin
• Primidone
• Tiagabine
• Topiramate
• Valproic Acid
• Vigabatrin
• Zonisamide

AED Based on Seizure Type

Potential MOA of AEDs
AED Contraindications• CBZ - AV heart block, bone marrow depression,
blood dyscrasias• Felbamate - blood dyscrasias, bone marrow
depression, hepatic function impairment• Phenobarbital - porphyria• Phenytoin - sinus bradycardia, AV block, SA
block, Adams-Stokes syndrome• Valproic acid - Severe hepatic function impairment
Adverse Drug Reactions with AEDs
• ADRs occur frequently with AED therapy
(31%)
• More common with multi-drug regimens
and higher doses
• ADRs may not always correlate with serum
drug concentrations

Adverse Drug Reactions with AEDs• Life-threatening vs. Non-life threatening• Toxicity
– nystagmus, ataxia, anorexia, GI
• CNS Effects– drowsiness, sedation, dizziness
– may develop tolerance to after first few weeks
• Hemotologic – s/s: fever, sore throat, bruising, bleeding
– CBZ, Phenytoin, Felbamate, Ethosuximide
• Hepatotoxicity– Phenytoin, Valproic acid


Drug Interactions with AEDs• Pharmacokinetic:
– protein-binding interactions• valproate and phenytoin
– enzyme induction----P450….GEAR• carbamazepine, phenobarbital, phenytoin, primidone
– enzyme inhibition---p450• felbamate, valproate
• Pharmacodynamic:
– additive CNS effects• blurred vision, dizziness, ataxia

Pharmacokinetics of AEDs

Patient Monitoring
• Seizure frequency
• ADRs
• Comorbid conditions
• Cognitive function
• Drug interactions
• Serum drug concentrations

When do you measure serum levels?
• Titration phase or after dosage adjustments…phenytoin etc
• Suspected AED-related toxicity
• Confirmation of overdose
• Suspected medication noncompliance
• Undesired therapeutic response
• Unstable hepatic function
• New drug interaction

Serum Concentrations of AEDs

Principles of AED Therapy
• Not all patients need to be treated for their lifetime
• Treat the patient - Not the level
• Factors associated with good prognosis:– few tonic-clonic seizures prior to the start of
AED therapy– years seizure-free on AED therapy– normal EEG

Considerations in Discontinuation of AEDs
• History of patient’s epilepsy
• Probability of remaining seizure free
• Duration since last seizure
• Risk factors for recurrence
• Risks of long-term tx with AED
• Patient’s concerns of adverse effects
• Patient’s concerns of additional seizures

When to consider withdrawal?
• Seizure free for 2 to 4 years
• Experiencing intolerable side effects outweighing
benefit of therapy
• History of single seizure
• Normal neurologic exam and EEG
• Those on prophylactic therapy with no h/o seizure

Guidelines for Discontinuation
• Avoid abrupt discontinuation…taoper off
• Discontinue most toxic drugs first
• Length of taper?
– Medical Research Council’s Antiepileptic Drug
Withdrawal Study Group suggests to taper over 6 months
• Reduce dose in 30 day intervals by 25%
• If seizures recur, reinstate the last effective dose
Nonseizure uses of AEDs
• Behavioral disturbances• Drug withdrawal• Mood disorders• Pain syndromes• Neurogenic Pain• Restless legs syndrome• Trigeminal neuralgia….Carbamazepine• Tremor• Migraine prophylaxis

Questions?
• Distribute Case #1
• Responsible for Questions 1- 9
• Meet back for Large Group Facilitation this
afternoon at 3pm.

















