6 THE LANCET, JANUARY 2, 1971 teaching or administration: the inability of the Re- search Councils to proffer a golden handshake is one of the severest handicaps under which they labour. The university benefits in turn from specialised expertise close at hand and from occasional teaching by truly professional investigators. The arrangement has only one potential disadvantage. Some university teachers are inclined to envy the time and resources their research-committed fellows are able to devote to the cultivation of their special interests. This difficulty is less likely to cause trouble where it is clearly evident that the research unit's finance is entirely independent of the university's general budget and that its special resources are not purchased at the expense of the general academic body. Conclusion In conclusion I would plead for a clear recognition that teaching and research must go hand in hand. For most of us they are simultaneous preoccupations of equal impo~ance. Even if he is the master of no esoteric techniques the good teacher is bound to be curious, bound to find his work bristling with questions and un- solved problems some of which can be answered by careful observation or simple experiment. It is equally vital that the excelient reputation of British medical research for scrupulous accuracy and intellectual honesty should be preserved and developed. Without reasonable facilities for research, medical practice will not only stand still but it will decline, because the best of our younger men will go where they are more freely available. There aresome unattractive political omens at the moment. However, I hope and believe that the Association of Anmsthetists will not be too respectable to join in any demo that the Presidents of the Royal Colleges decide to lead down Whitehall under the banner "Hands off the Research Councils " SELF-LIMITING EPISODES OF RECURRENT THYROTOXlCOSIS D. G. McLART~ W.-'D. ALEX~DER R. MeG. HAP, DE~ J.W.K. ROBERTSON Gardiner Institute, University Department Of Medidne, Western Infirmary, Glasgowj and Regional Department of Clinical Physics and Bioengineering 5 patients with recurrent thyrotoxicosis Summary experienced a remission without anti- thyroid therapy. The initial episode of thyrotoxicosis was treated with carbimazole, and after completing treatment the patients remained in remission for periods of up to 16 months. At the time of recurrence clinical features of thyrotoxicosis were accompanied by elevation of thyroid radioiodine uptake, protein- bound iodine, and free-thyroxine index. Subsequent clinical improvement was paralleled by a return of values to normal. Conventional treatment of these relapses of thyrotoxic0sis by radioiodine therapy or subtotal thyroidectomy might not have conferred any advantage on these patients. Introduction DUmNG the past 5 years we have observed the course of thyrotoxicosis in a group of patients treated with carbimazole and triiodothyronine.l,~ Following anti- thyroid~drug therapy the patients were given tri- iodothyronine for many months, so that repeated studies of thyroid suppression could be made. We describe here the remission of thyrotoxicosis without specific treatment in 5 patients in whom thyrotoxicosis had recurred during the period while they were receiving trilodothyronine alone. The question arises whether conventional treatment (with radioiodine or by subtotal thyroidectomy) of the relapses of thyro,. toxicosis would have conferred any advantage, since these thyrotoxic episodes were in anycase self-limitingi Patients and Methods The general plan of the study has been described and results in 93 patients have been recorded2 All the patients were treated with carbimazole in an initial dose of 30 mg: or 40 mg. daily, reduced when the patient became euthy~ roid to a maintenance dose of 15-20 rag. daily in divided doses. Every patient received 80 ~zg. of triiodothyronine daily, divided into four doses, in conjunction with the carbimazole therapy. The 20-minute thyroid uptake, serum-protein-bound-iodine, triiodothyronine-resin up~ take, and free-thyroxine index were measured as previously described.l. 4 Triiodothyronine 80 ~zg. daily was continued after stopping the antithyroid drug• In all 5 patients to be described suppression of the 20~ minute thyroid 13~I uptake into the normal range (below 8Wo) developed during treatment of the initial attack of thyrotoxic0sis with carbimazole. After stopping carbima- zole a euthyroid clinical state and thyroid suppressibility by triiodothyronine persisted for up to 16 months befor~ relapse occurred. Case-reports Case 1 (fig. 1) When first seen this 40-year-old woman gave a 4-week history of increasirig anxiety and nervousness. The thyroid was diffusely enlarged, estimated to be 40 g. on palpation, and the scintiscan showed a uniform uptake pattern. Clinical examina~ign showed features of thyrotoxicosis and the free-thyroxirm index was 11.2 (upper limit of normal 8)~ The 20-mmute~thyroid uptake of xs~I was 13-9% (nppe! limit of normal: 8%). After 10 months' treatment wit~ earbimazole and triiodothyronine the 20-minute uptake had fallen t 0, 2~%. Carbimazole was stopped but triiodo- thyrou'me continued. 5 months later the 20-minute uptake rose t O 27" 1Wd and the free-thyroxine index to 11.4. At this time She corhpIained of heat intolerance, and clinically she was mildly thyrotoxic. A month later, without any further treatment, her symptoms had improved, and this was con- firmed by a fall in the 20-minute uptake. It was therefore decided not to restart antithyr0id-drug therapy, and by the 9th month the patient was clinically euthyroid apart from sinus tachycardia. She continued to improve and remains euthyroid and symptom-free. Case 2 (fig. 2) This woman of 3fcomplained of lassitude and breathless- ness for 2 months. The thyroid was diffusely enlarged (about 30 g.) with a bruit, and the scintiscan showed a u ni~ form uptake pattern. The clinical diagnosis 'of thyrotoxi, cosis was conf~med by a free*thyroxine index of 15.9 and 20-minute thyroid ~32I uptake of 23"5%. No fall in uptake was observed after a triiodothyronine suppression re_st. She was treated with carbimazole and triiodothyronine for 5 months, and at this time the 20~-minute xa2Iuptake had
Transcript
6 THE LANCET, JANUARY 2, 1971
teaching or administration: the inability of the Re- search Councils to proffer a golden handshake is one of the severest handicaps under which they labour. The university benefits in turn from specialised expertise close at hand and from occasional teaching by truly professional investigators. The arrangement has only one potential disadvantage. Some university teachers are inclined to envy the time and resources their research-committed fellows are able to devote to the cultivation of their special interests. This difficulty is less likely to cause trouble where it is clearly evident that the research unit 's finance is entirely independent of the university's general budget and that its special resources are not purchased at the expense of the general academic body.
Conclusion In conclusion I would plead for a clear recognition
that teaching and research must go hand in hand. For most of us they are simultaneous preoccupations of equal impo~ance. Even if he is the master of no esoteric techniques the good teacher is bound to be curious, bound to find his work bristling with questions and un- solved problems some of which can be answered by careful observation or simple experiment. I t is equally vital that the excelient reputation of British medical research for scrupulous accuracy and intellectual honesty should be preserved and developed. Without reasonable facilities for research, medical practice will not only stand still but it will decline, because the best of our younger men will go where they are more freely available. There aresome unattractive political omens at the moment. However, I hope and believe that the Association of Anmsthetists will not be too respectable to join in any demo that the Presidents of the Royal Colleges decide to lead down Whitehall under the banner "Hands off the Research Councils "
SELF-LIMITING EPISODES OF R E C U R R E N T T H Y R O T O X l C O S I S
D. G. McLART~ W.-'D. ALEX~DER
R. MeG. HAP, DE~ J . W . K . ROBERTSON
Gardiner Institute, University Department Of Medidne, Western Infirmary, Glasgowj and Regional Department of
Clinical Physics and Bioengineering
5 patients with recurrent thyrotoxicosis Summary experienced a remission without anti-
thyroid therapy. The initial episode of thyrotoxicosis was treated with carbimazole, and after completing treatment the patients remained in remission for periods of up to 16 months. At the time of recurrence clinical features of thyrotoxicosis were accompanied by elevation of thyroid radioiodine uptake, protein- bound iodine, and free-thyroxine index. Subsequent clinical improvement was paralleled by a return of values to normal. Conventional treatment of these relapses o f thyrotoxic0sis by radioiodine therapy or subtotal thyroidectomy might not have conferred any advantage on these patients.
Introduction DUmNG the past 5 years we have observed the course
of thyrotoxicosis in a group of patients treated with carbimazole and triiodothyronine.l,~ Following anti- thyroid~drug therapy the patients were given tri- iodothyronine for many months, so that repeated studies of thyroid suppression could be made. W e describe here the remission of thyrotoxicosis without specific treatment in 5 patients in whom thyrotoxicosis had recurred during the period while they were receiving trilodothyronine alone. The question arises whether conventional treatment (with radioiodine or by subtotal thyroidectomy) of the relapses of thyro,. toxicosis would have conferred any advantage, since these thyrotoxic episodes were in anycase self-limitingi
Patients and Methods The general plan of the study has been described and
results in 93 patients have been recorded2 All the patients were treated with carbimazole in an initial dose of 30 mg: or 40 mg. daily, reduced when the patient became euthy~ roid to a maintenance dose of 15-20 rag. daily in divided doses. Every patient received 80 ~zg. of triiodothyronine daily, divided into four doses, in conjunction with the carbimazole therapy. The 20-minute thyroid uptake, serum-protein-bound-iodine, triiodothyronine-resin up~ take, and free-thyroxine index were measured as previously described.l. 4 Triiodothyronine 80 ~zg. daily was continued after stopping the antithyroid drug•
In all 5 patients to be described suppression of the 20~ minute thyroid 13~I uptake into the normal range (below 8Wo) developed during treatment of the initial attack of thyrotoxic0sis with carbimazole. After stopping carbima- zole a euthyroid clinical state and thyroid suppressibility by triiodothyronine persisted for up to 16 months befor~ relapse occurred.
Case-reports Case 1 (fig. 1)
When first seen this 40-year-old woman gave a 4-week history of increasirig anxiety and nervousness. The thyroid was diffusely enlarged, estimated to be 40 g. on palpation, and the scintiscan showed a uniform uptake pattern. Clinical examina~ign showed features of thyrotoxicosis and the free-thyroxirm index was 11.2 (upper limit of normal 8)~ The 20-mmute~thyroid uptake of xs~I was 13-9% (nppe! limit of normal: 8%). After 10 months' treatment wit~ earbimazole and triiodothyronine the 20-minute uptake had fallen t 0, 2~%. Carbimazole was stopped but triiodo- thyrou'me continued. 5 months later the 20-minute uptake rose t O 27" 1 Wd and the free-thyroxine index to 11.4. At this time She corhpIained of heat intolerance, and clinically she was mildly thyrotoxic. A month later, without any further treatment, her symptoms had improved, and this was con- firmed by a fall in the 20-minute uptake. It was therefore decided not to restart antithyr0id-drug therapy, and by the 9th month the patient was clinically euthyroid apart from sinus tachycardia. She continued to improve and remains euthyroid and symptom-free.
Case 2 (fig. 2) This woman of 3fcomplained of lassitude and breathless-
ness for 2 months. The thyroid was diffusely enlarged (about 30 g.) with a bruit, and the scintiscan showed a u ni~ form uptake pattern. The clinical diagnosis 'of thyrotoxi, cosis was conf~med by a free*thyroxine index of 15.9 and 20-minute thyroid ~32I uptake of 23"5%. No fall in uptake was observed after a triiodothyronine suppression re_st. She was treated with carbimazole and triiodothyronine for 5 months, and at this time the 20~-minute xa2I uptake had
The same scale is used to show the 20-mlnute thyroid "~I uptake % and the free-thyroxine (T4) index.
fallen to 4.3%. Carbimazole was stopped, bu t the triiodo- thyrofiine was continued. Dur ing the 3rd month the 20-minute uptake rose to 9"9% and reached 15.8% during the 5th month. This rise was paralleled by an increase in the free-thyroxine index. T h e patient complained of excessive sweating and heat intoIerance, and on examination was mildly thyrotoxic with a pulse-rate of 100 per minute.
During subsequent visits, however, there was evidence of definite clinical improvement, and this was confirmed by a steady decline of both the free-thyroxine index and 20-minute ~s2I uptake to normal levels.
Case a (fig. a) A woman of 37 presented with a 9-month history of
F i g . 2 - - T h y r o i d f u n c t i o n i n e a s e 2.
nervousness, irritability, and weight- loss. Her thyroid was diffusely enlarged (approximately 50 g.), and the scintiscan demonstrated a diffuse uptake pattern. The free-thyroxine index was 25'8 and 20-minute 136I uptake 33.5%. Treatment was be- gun with carbimazole and triiodo- thyronine and continued for 14 months, by which time the 20- minute uptake had fallen to 5"9%. When earbimazole was stopped the patient remained well and symptom- free, but during the 16th month the free-thyroxine index rose to 15.7. Clinically there was evidence of thyrotoxicosis with weight-loss and symptoms of anxiety. In view of our previous experience the patient was observed carefully over the follow- ing months, and during this t ime there was evidence of a continuing improvement paralleled by a re turn
of the 20-minute thyroid uptake and free-thyroxine index to normal levels. Case 4 (fig. 4)
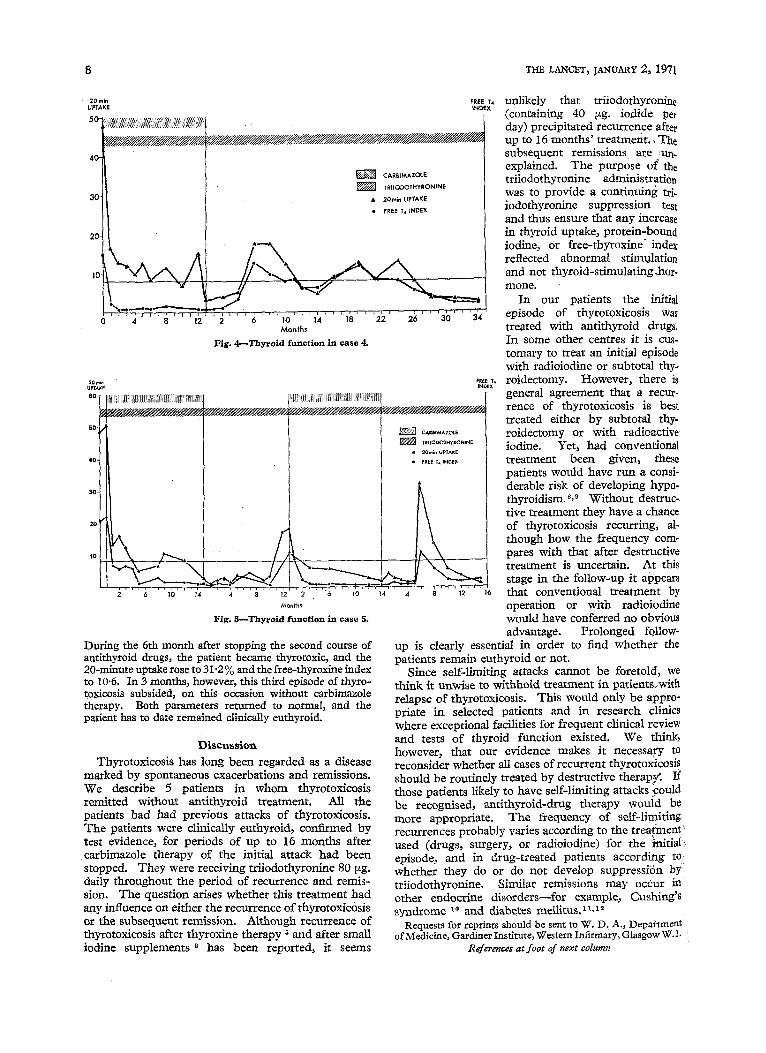
This 37-year-old woman complained of weight-loss, excessive sweating, and nervousness. , The thyroid was diffusely enlarged (about 50 g.) with a bruit, and seintiscan showed a uniform uptake pattern. The free-thyroxine index was 14"9 and the 20-minute 1~6I uptake 48.0%. Treatment with carbimazole and triiodothyronine was begun, and by 13 months the 20-minute uptake had fallen to 3-4%. At this point carbimazole was discontinued but triiodothyronine continued in a dose of 80 t~g. daily. 6 months later the 20-minute 1~2I uptake rose to 17"6% and
the free-thyroxine index to 12.8. The FrenT, patient 's clinical state was compatible INDEX with mild thyrotoxicosis. She improved,
bu t during the 16th month the 20-minute uptake rose to 8"2% and the free-thyroxine index to 8.2. Because clinical improve- ment again followed carbimazole was not restarted, and when last reviewed the patient was euthyroid with a 20-minute uptake of 2.7% and free-thyroxine index of 2.7.
Case 5 (fig. 5) A woman of 33 complained of neck
34 swelling, excessive sweating, and tired- ness for 4 weeks. Her thyroid was diffusely enlarged (approximately 50 g.) with a bruit, and the scintiscan showed a uniform uptake "pattern. The free-
Free T, thyroxine index was 20-5 and the 20- IND0X minute 136I uptake 48:7%. A triiodo-
~////////////////p] thyronine suppression test showed no fall in uptake. Treatment with carbimazole and triiodothyronine was started, and 15 months later the 20-minute uptake had fallen to 2.9%. Carbimazole was stopped but triiodothyronine continued in a dose of 80 tzg. daily. 12 months later thyro-
toxicosis recurred, the free-thyroxine index rising to 17.2. The patient was re- started on a second course of carbimazole and triiodothyronine, and suppression again developed, the 20-minute uptake faUing to 1-3% after 14 months ' treat- ment. Triiodothyronine was continued throughout the period of observation.
8 THE LANCET, JANUARY 2, 1971
20 mln UPTAKE 50
4 , 0 ~ ; ,i:.::::u
FREE T4 INDEX
CAREIMAZOLE TRIIODOTHYRONJNE
• 20rn~n UPTAKE • FREE T,4 INDEX
t ~ , ~ - , ~ , r ~ , , r , . . . . . . . . . . . . . . . . ' . . . . . . - . . . . . o 4 s 12 2 6 To 14 i s 22 26 3o -~4
M o n t h s
Fig. 4---Thyrold funct ion in case 4.
20mln uerAge FREE T, INDEX
Months
Fig. 5 ~ T h y r o i d func t ion in case 5.
During the 6th month after stopping the second course of antithyroid drugs, the patient became thyrotoxic, and the 20-minute uptake rose to 31"2 % and the free-thyroxine index to 10"6. In 3 months, however~ this third episode of thyro- toxicosis subsided, on this occasion without carbimazole therapy. Both parameters returned to normal, and the patient has to date remained clinically euthyroid.
Discussion
Thyrotoxicosis has long been regarded as a disease marked by spontaneous exacerbations and remissions. We describe 5 patients in whom thyrotoxicosis remitted without antithyroid treatment. All the patients had had previous attacks of thyrotox/cosis. The patients were clinicakly cuthyroid, confirmed by test evidence, for periods of up to 16 months after carbimazole therapy of the initial attack had been stopped. They were receiving triiodothyrozfine 80 [zg. daily throughout the period of recurrence and remis- sion. The question arises whether this treatment had
• J o
any influence on either the recurrence of thyrotoxlcosls or the subsequent remission. Although recurrence of thyrotoxicosis after thyroxine therapy 5 and after smaU iodinc supplements 6 has been reported, it seems
unlikely that triiodothyronine (containing 40 ~tg. iodide per day) precipitated recurrence after up to 16 months ' treatment. ,The subsequent remissions are :un- explained. The purpose of* the triiodothyronine administration was to provide a continuing tri. iodothyronine suppression test and thus ensure that any increase in thyroid uptake, protein-bound iodine, or free-thyroxine-index reflected abnormal stimulation and not thyroid-stimulating.hor- mone.
In our patients the initial episode of thyrotoxicosis was treated with antithyroid drugs. In some other centres it is cus- tomary to treat an initial episode with radioiodine or subtotal thy- roidectomy. However, there is general agreement that a recur- rence of thyrotoxicosis is best treated either by subtotal thy- roidectomy or with radioactive iodine. Yet, had Conventional treatment been given, these patients would have run a consi- derable risk of developing hypo- thyroidism. S,E Without destruc- tive treatment they have a chance of thyrotoxicosis recurring, al- though how the frequency corn- pares with that after destructive treatment is uncertain. At this stage in the follow-up it appears that conventional treatment by operation or with radioiodine would have conferred no obvious advantage. Prolonged follow-
up is clearly essential in order to find whether the patients remain euthyroid or not.
Since self-l/m/ring attacks cannot be foretold, we think i t unwise to withhold treatment in patient~with relapse of thyrotoxicosis. This would only be appro- priate in selected patients and in research ¢linics where exceptional facilities for frequent clinical review and tests of thyroid function existed. We think, however, that our evidence makes it necessa~r to reconsider whether all cases of recurrent thyrotoxicosis should be routinely treated by destructive therapy'. If those patients likely to have self-limiting attacks ~ould be recognised, anti thyroid-drug therapy would be more appropriate. The frequency of self-limiting recurrences probably varies according to the t reatment used (drugs, surgery, o; radioiodine) for the initial episode, and in drug-treated patients according t o whether they do or do not develop suppressi6n by triiodothyronine. Similar remissions may occur in other endocrine disorders--for example, Cushing's syndrome 10 and diabetes mellitus, zl,m
Requests for reprints should be sent to W. D. A.~ Depa~ment of Medicine, Gardiner Institute, Western Infirmary, Glasgow W.1.
References at foot of next column
TIlE LANCET, JANUARY 2 , 1971 9
S C R E E N I N G F O R B A C T E R I U R I A
IN P R E G N A N C Y
D. H. LAWSON*
A. W. F. MILLERt Queen Mother's Hospital and ~Vestern Infirmary,
Glasgow
The incidence of asymptomatic bac- Summary teriuria in 1160 patients screened in
early pregnancy was 4.6%. This finding was baged on the examination of a single midstream specimen of urine. The incidence of bacteriologically confirmed urinary-tract infection developing during pregnancy in the whole group was 4 .1%-and in t,h~bacteriurics 16"6%. Only 19.1% of patients who developed an acute urinary infection, during the pregnancy had bacteriuria on initial screening. The value of screening for bacteriuria as a method of preventing acute pyelo- nephritis is therefore questioned, and it is suggested that laboratory resources might be better concentrated on the follow-up of patients who develop a proven infection during pregnancy.
Introduction ASYMPTOMATIC bacteriuria has been widely studied
in the past ten years since the observation of Kass x that nearly half the patients with bacteriuria in early pregnancy developed symptoms of acute urinary-tract infection later in the pregnancy. In 1962 he noted a high incidence of prematurity and fetal loss in such patients and suggested that these complications could be reduced by treating the bacteriuria. * Little 8 sup- ported Kass in regarding pyelonephritis of pregnancy as preventable by the detection and treatment of asymptomatic bacteriuria in early pregnancy. Kincaid- Smith and Bullen 4 found a raised incidence of acute pyelonephritis, prematurity, pre-eclampsia, and peri- natal loss in bacteriuric patients. Successful treatment of the bacteriuria reduced the incidence of acute pyelonephritis but not of the other complications. Pyelonephritis in pregnancy was not eradicated by the treatment, however, and they suggested that under-
* Present address: Department of Clinical Pharmacology, Tufts Uni- versity School of Medicine, Waltham, Mass., U.S.A.
t Present address: University Department of Obstetrics and Gyn~ecology~ Royal Maternity Hospital, Rottenrow, Glasgow C.4.
DR. MCLARTY ~ OTHERS: REFERENCES
I. Alexander, W. D., Harden, R. McG., Shimmins, J., McLarty, D., McGill, P. Lancet, 1967, ii, 681.
2. Alexander, W. D., Harden, R. MEG., McLarty, D., Shimmins, J. M c~abollsm, I968, 18, 58. -
3. Alexander, W. D., McLarty~ D. G., Robertson, ~., Shlmmlns, j . , Brownlie, B. E. \V.~ Harden, R. MEG., Patel, A. R.ff. din. Endocr. 1970, 30, 540.
4. Clark, F., Horn, D. B. ibid. 1965, 25, 39. S. Dymling, $. F., Becker, D. V. ibid. 1967, 27, 1487. 6. Alexander, W. D., Harden, R. McG., Koutras, D. A., Wayne, E.
Lancet, 1965, ii, 866. 7. Hedley, A. J., Fleming, C. J., ~hesters, M. L, Michie, W., Crooks,
~. Br. reed. ft. 1970,r i, 519. 8. Nofal, M. M., Be~erwaltes, W. H., Patno, M . E. ft. Am. reed. Ass.
1966, 197, 605. 9. Dunn, ]'. T., Chapman, E. M. N e w gngL ft. Med. 1964, 271, 1037.
I0. Barnett, L G., Nabarro, J. D. N., LeQuesne, L. P. Proc. R. Soc. Med. 1970, 63, 10. "
lying chronic renal disease was the cause of both the bacteriuria and the increased incidence of prematurity, fetal loss, and pre-eclampsia.
Other workers have remained unconvinced of the link between bacteriuria and these complications.S, s Further, Dixon and Brant 6 pointed out that only 31.8% of those developing an acute urinary-tract infection in their series did in fact have asymptomatic bacteriuria on first screening--a figure similar to that of Pinkerton et al. 7
Significant bacteriuria was considered by Kass to be present when more than 100,000 organisms per ml. of urine were present in at least two consecutive clean midstream urines. The collection of so many speci- mens at a busy antenatal clinic and subsequent bac- terial counting impose a considerable burden on both the clinic and laboratory staff. The present survey was carried out to assess the value of this screening-test in the Qt~een Mother's Hospital, Glasgow, and to test the feasibility of using only one midstream specimen for this purpose.
Patients and Methods Specimens were obtained from unselected patients at
their first visit to the antenatal clinic. The vulva was cleaned with sterile water and a clean-catch midstream specimen was collected in a sterile honey-pot, The collec- tion of all the specimens was under the direct supervision of one nurse throughout the study. The urine was refriger- ated at 4°C until plating, which took place not more than three hours after collection.
Bacteriuria was said to be present if the organismal count was 105 per ml. of urine or more. Specimens with 104-105 organisms per ml. were regarded as having doubtful bacteriuria, and the remainder were regarded as sterile.
Results 1160 patients were studied. 54 patients (4.6%) had
asymptomatic bacteriuria on first screening and a further 89 patients (7.7%) had counts in the doubtful range (104-105 organisms per ml.).
Urinary-tract Infection ( U. T.L ) The incidence of this complication in the different
groups is shown in table I, where it can be seen that
TABLE I--INCIDENCE OF U.T.I, IN DIFFERENT GROUPS
Group
Total no. (1160) Bacteriuric (54) Doubtful (89) Negative (1017)
Clinically significant
94 (8"1%) 15 (27"7%) 9 (10"1%)
70 (6"9%)
Bacteriologically confirmed
47 (4.1%) 9 (16-6%) 6 (6.7%)
32 (3.1%)
94 patients developed symptoms suggestive of urinary- tract infection. We examined the urine of 53 of these patients and found more than 10 s organisms per nil. of urine together with pus cells in 47 at the time of symptoms; the urine of the other 6 patients was sterile. , The remaining 41 patients were treated by their own doctor either without bacteriological exami- nation of the urine or after examination in another laboratory.
The success of the screening-test in predicting the development of urinary-tract infection is shown in table ii. Only, 15"9% of those developing clinical urinary-tract infection had significant bacteriuria on