83
Chemical injuries
| Date post: | 15-Apr-2017 |
| Category: |
Healthcare |
| Upload: | sameer-gade |
| View: | 113 times |
| Download: | 0 times |

Chemical injuries
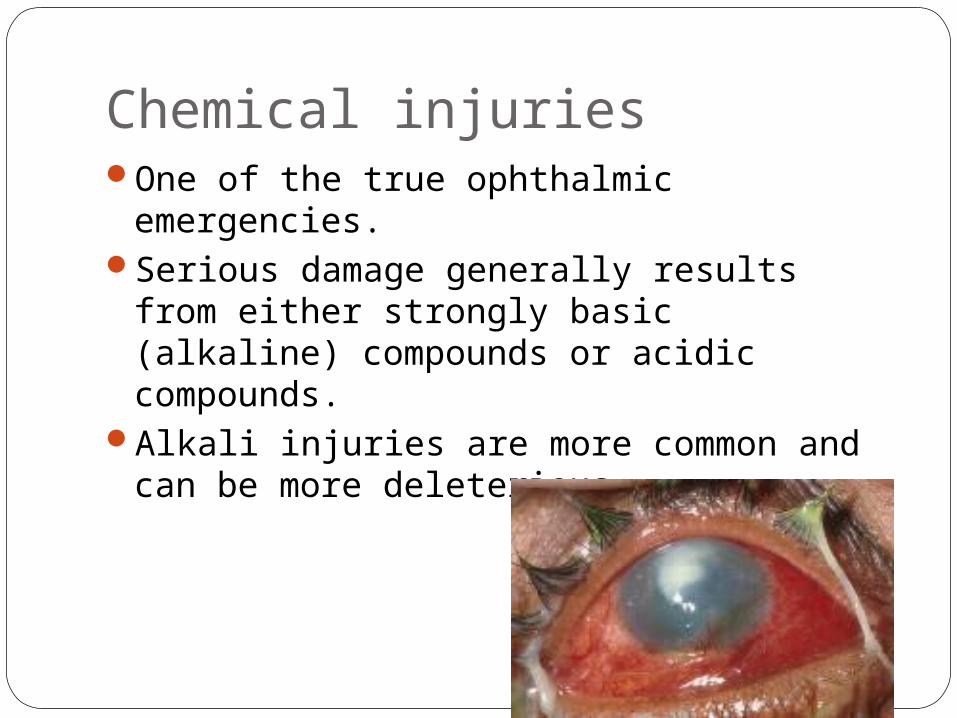
Chemical injuriesOne of the true ophthalmic emergencies. Serious damage generally results from
either strongly basic (alkaline) compounds or acidic compounds.
Alkali injuries are more common and can be more deleterious.

Epidemiology Chemical injuries are responsible for
approximately 7% of work-related eye injuries .
More than 60% of chemical injuries occur in workplace accidents, 30% occur at home, and 10% are the result of an assault.

Mortality/Morbidity
As many as 20% of chemical injuries result in significant visual and cosmetic disability.
Only 15% of patients with severe chemical injuries achieve functional visual rehabilitation.
Age Chemical injuries can strike any population.However, most injuries occur in patients
aged 16-45 years.
Sex
Males are 3 times more likely to experience chemical injuries than females.

Chemical agentsAlkalic
Acidic
Alkali agents :Ammonia, potassium hydroxide, magnesium
hydroxide, and lime.
Ammonia (NaOH) tend to produce the most serious injuries.
Magnesium hydroxide found in fireworks may combine with thermal injury to produce a
particularly devastating injury.
Lime(CaOH2) particularly in the form of plaster, is the most commonly encountered alkali injury; fortunately, it tends to cause less severe injury.

Acidic agentsSulfuric, sulfurous, hydrofluoric, nitrous,
acetic, chromic,and hydrochloric acids.Sulfuric acid injury is the most commonly
seen, usually after battery explosions.The most severe acid injuries are
associated with hydrofluoric acid.
Interaction of chemical agent to corneal tissue. The severity of this injury is related to type,
volume, concentration, duration of exposure, and degree of penetration of the chemical .
The mechanism of injury differs slightly between acids and alkali.

Acid injury Acids dissociate into hydrogen ions and
anions in the cornea, e.g.: HCl= H++Cl-The hydrogen molecule damages the
ocular surface by altering the pH, while the anion causes protein denaturation, precipitation, and coagulation .
Protein coagulation generally prevents deeper penetration of acids.
Hydrofluoric acid is an exceptionIt behaves like an alkaline substance
because the fluoride ion has better penetrance through the stroma than most acids, leading to more extensive anterior segment disruption.

Alkali injury Alkaline substances dissociate into a
hydroxyl ion and a cation in the ocular surface. e.g.: NaOH= Na+ + OH-
The hydroxyl ion saponifies cell membrane fatty acids, while the cation interacts with stromal collagen and glycosaminoglycans.
This interaction facilitates deeper penetration into and through the cornea and into the anterior segment.

Classification of chemical injuriesHughes classification. Modified Hughes classification.Roper Hall classification.Duas clasification.

Hughes classificationMildMild Erosion of corneal epithelium, faint Erosion of corneal epithelium, faint
haziness of cornea, no ischemic haziness of cornea, no ischemic necrosis of conjunctiva or sclera.necrosis of conjunctiva or sclera.
ModeraModerat--ely t--ely severesevere
Corneal opacity blurs iris details, mild Corneal opacity blurs iris details, mild ischemic necrosis of conjunctiva or ischemic necrosis of conjunctiva or sclera.sclera.
Very Very severesevere
Blurring of pupillary outline, significant Blurring of pupillary outline, significant ischemic necrosis of conjunctiva or ischemic necrosis of conjunctiva or sclera.sclera.

The Modified Hughes classification
A grade I injury involves little or no loss of limbal stem cells and presents with little or no evidence of ischemia.
A grade II injury involves subtotal loss of limbal stemcells and presents with ischemia of less than one-half of the limbus.
The Modified Hughes classificationA grade III injury involves loss of >1/2 to
total limbal stem cells with preservation of the proximal conjunctival epithelium.
A grade IV injury involves total limbal stem-cell loss as well as loss of the proximal conjunctival epithelium and presents with extensive damage to the entire anterior segment.
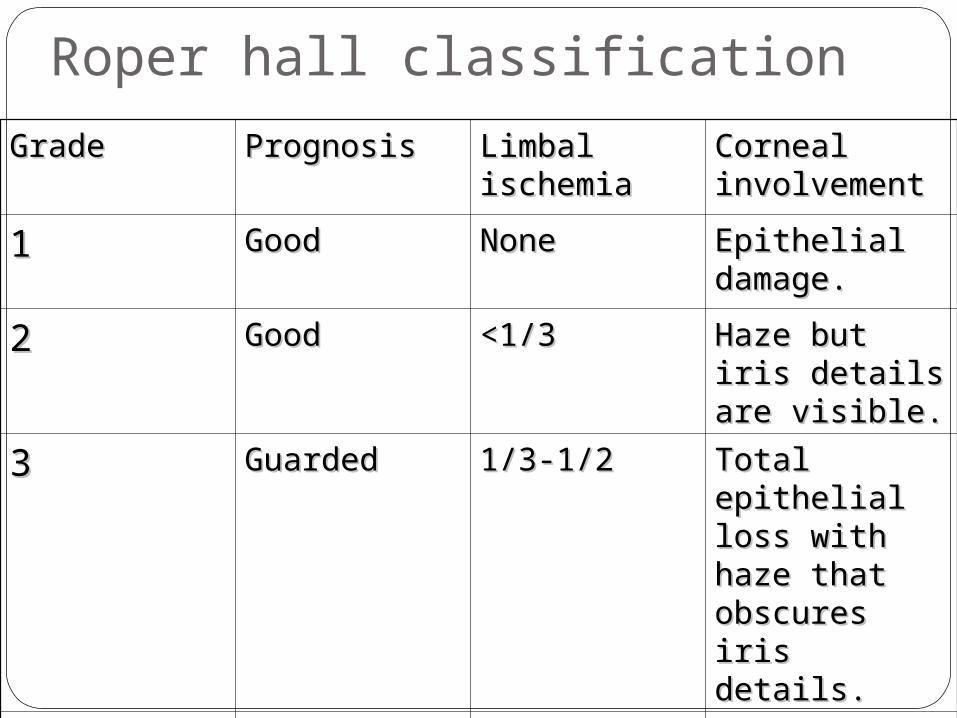
Roper hall classificationGradeGrade PrognosisPrognosis Limbal Limbal
ischemiaischemiaCorneal Corneal involvementinvolvement
11 GoodGood NoneNone Epithelial Epithelial damage.damage.
22 Good Good <1/3<1/3 Haze but iris Haze but iris details are details are visible.visible.
33 GuardedGuarded 1/3-1/21/3-1/2 Total Total epithelial loss epithelial loss with haze that with haze that obscures iris obscures iris details.details.
44 PoorPoor >1/2>1/2 Cornea Cornea opaque with opaque with iris pupil iris pupil details details obscuredobscured
Why new classification?The successes and failures reported for ocular
surface reconstruction procedures vary from centre to centre even for the same grade of burns .
This difference is largely a reflection on the inadequacy of the present classification system. (Roper Hall classification)
Suppose for grade IV burns, In the Roper-Hall classification grade IV implies between 50%–100% limbal ischaemia and is equated with a poor prognosis.
However, with present management strategies, an eye with 50% or even 75% limbal ischaemia can expect a good to fair outcome, whereas an eye with 100% ischaemia is very likely to have a poor outcome.

Duas clasificationGradeGrade PrognosisPrognosis Clinical findingsClinical findings
limbal limbal involvement involvement
Conjunctival Conjunctival involvementinvolvement
Analogue Analogue scalescale
11 V. goodV. good 0 clock hours of 0 clock hours of limbal limbal involvement involvement
0% 0% 0/0% 0/0%
22 GoodGood 3 clock hours of 3 clock hours of limbal limbal involvement involvement
30% 30% 0.1–3/0.1–3/1–29.9% 1–29.9%
33 GoodGood >3–6 clock >3–6 clock hours of limbal hours of limbal involvement involvement
>30–50% >30–50% 3.1–6/ 3.1–6/ 31–50% 31–50%
44 Good to Good to guardedguarded
>6–9 clock >6–9 clock hours of limbal hours of limbal involvement involvement
>50–75% >50–75% 6.1–9/6.1–9/51–75% 51–75%
55 Guarded to Guarded to poorpoor
>9–<12 clock >9–<12 clock hours of limbal hours of limbal involvement involvement
>75–<100% >75–<100% 9.1–11.9/9.1–11.9/75.1–75.1–99.9% 99.9%
66 Very poorVery poor Total limbus (12 Total limbus (12 clock hours) clock hours) involved involved
Total Total conjunctiva conjunctiva (100%) involved (100%) involved
12/12/100% 100%

The analogue scale records accurately the limbal involvement in clock hours of affected limbus/percentage of conjunctival involvement.
While calculating percentage of conjunctival involvement, only involvement of bulbar conjunctiva, up to and including the conjunctival fornices is considered.
The term “limbal involvement” is preferred
over “limbal ischaemia” because total loss of limbal epithelium (including the stem cells) can occur despite little ischaemia but has potentially the same consequences.

Although limbal ischaemia is usually associated with loss of limbal stem cells, this is not always the case .
Transient ischaemia, or ischaemia occurring soon after the injury but recovering in the ensuing days, may allow limbal stem cells to survive, recover or repopulate the affected sector.

Grade 1 (duas classification) No limbal and
conjunctival involvement

Grade 3 (4.5/30%) ocular surface burn .
Four and a half clock hours of limbus involvement with 30% conjunctival involvement .
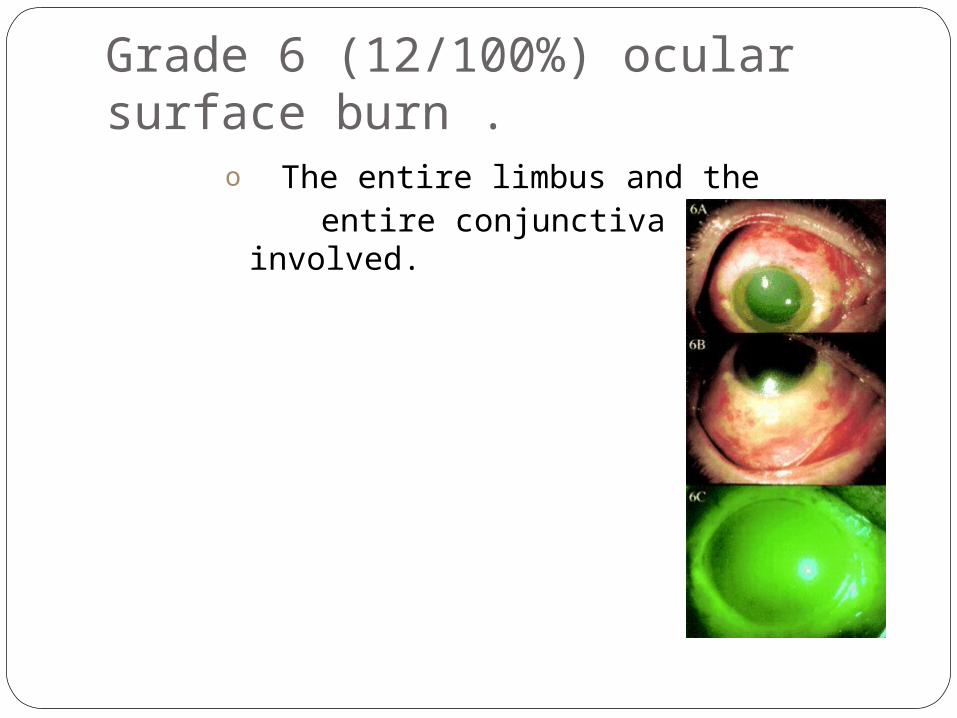
Grade 6 (12/100%) ocular surface burn .
o The entire limbus and the entire conjunctiva are involved.

PathophysilogyAcute stage (immidiate to 1 week):
depending on degree of chemical penetration, corneal and conjunctival epithelium, keratocytes, corneal nerves, endothelium, iris ,ciliary body, lens epithelium suffer losses to some degree.
IOP elevation : bimodal Initial peak: compression of globe d/t
shortening of collgen fibers. Second peak: TM damage, TM
obstruction by inflammatory cells.

Corneal clouding: d/t stromal oedema and changes in proteoglycans.
Infiltration of ocular structures by PMNs, monocytes, etc.

Early repair phase (1 to 3 weeks)Inflammation parallels the epithelial
regeneration.Conjunctival and corneal epithelium begins to
regenerate.Corneal opacities begin to clear, they clear
completely during this period in mild to moderate injuries.
Invasion of fibroblasts and synthesis of new collagen reach a peak by 14 days after injury.
It is during this stage that corneal ulceration tends to occur.
Late repair phaseCorneal vascularization in more severe
corneal injuries.Tear film abnormality: 1)aqueous deficiency :d/t damage to
accessory lacrimal glands and scarring of ductule opening of major lacrimal gland.
2)Mucin deficiency: d/t damge to goblet cells.
Permanent loss of corneal innervation: resulting in neurotrophic keratitis.
IOP hypotony d/t severe damage to cilliary
bodyGlaucoma d/t damage to outflow
channels: TM scarring, extensive PAS.Symblepharon :proportional to extent of
conjunctival necrosis.
Three main pathophysiologic mechanisms are target for treatment.
(1) Regeneration of ocular surface epithelium and its state of differentiation.
(2) Stromal matrix remodelling, including repair and degradation.
(3) Inflammation.
EPITHELIAL INJURY, REPAIR, ANDDIFFERENTIATION
Both conjunctival epithelium and limbal stem-cell populations may resurface the chemically injured corneal epithelium.
Conjunctiva-derived epithelium never fully expresses corneal epithelial phenotypic features.
Reestablishment of a phenotypically normal corneal epithelial surface with limbal stem cell-derived cell populations is the first major principle in the therapeutic management.
CORNEAL STROMAL MATRIX INJURY,REPAIR, AND ULCERATION
Matrix metalloproteinases (MMP), are responsible for the initial rate-limiting cleavage of collagen molecules.
Excessive degradation of the matrix by MMP–1 and MMP–8, relative to type I collagen synthesis, may result in enzymatic degradation of the corneal stroma, a process referred to as sterile corneal ulceration.
Exploitation of known pharmacologic intervention,which helps shift the balance toward repair, rather than ulceration, is the second major principle in the management of severe chemical injuries.

INFLAMMATIONThe association of inflammatory cell
infiltration (especially with polymorphonuclear leukocytes) into the corneal stroma with sterile corneal ulceration is well documented.
Persistent inflammation may delay reepithelialization and perpetuate continued recruitment of additional inflammatory cells.
Rigorous control of inflammation is the third major principle in the therapeutic management of severe chemical injuries.

CLINCAL COURSE AND EVALUATIONMcCulley has divided the clinical course of
chemical injuries into four distinct pathophysiologic and clinical phases.
1.Immediate 2.Acute (days 0–7) 3.Early repair (days 7–21) 4.Late repair (day 21 to several months
later) phases.

IMMEDIATE PHASE
The extent of surface involvement can be determined by the size of the corneal and conjunctival epithelial defects.

The depth of corneal and intraocular penetration can be estimated by evaluating corneal clarity, intraocular inflammation, intraocular pressure,and lens clarity.

The depth of ocular surface penetration, and possible limbal stem-cell damage, can be evaluated indirectly by assessment of vascular ischemia and necrosis of limbal and bulbar conjunctiva.
ACUTE PHASEDuring the first week, important
parameters that should be monitored include evidence of reepithelialization ,intraocular pressure, and progressive ocular inflammation.
Grade I injuries tend to heal.Slow but progressive reepithelialization
in grade II injuries. Grade III and IV injuries show no
reepithelialization.
EARLY REPAIR PHASE
During the early repair phase, epithelial migration continues in less severe injury (grade II) but remains delayed in more
severe injuries (grades III and IV).In severe chemical injuries, a second wave
of inflammatory cell infiltration begins after 7 days and continues to progress over the next several weeks.

LATE REPAIR PHASECorneal inflammation,collagen synthesis,
and collagenase activity are peaking.A type I healing pattern (normal epithelial
recovery)corresponds to a grade I limbal stem-cell injury in that restoration of an intact and phenotypically normal corneal epithelial surface has occurred by this stage.
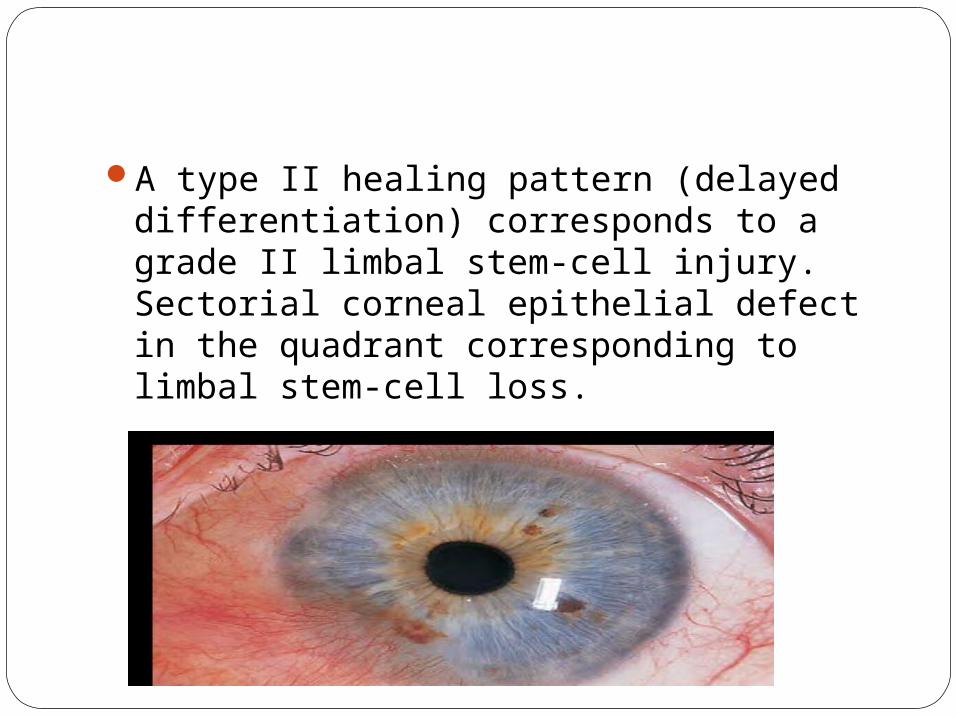
A type II healing pattern (delayed differentiation) corresponds to a grade II limbal stem-cell injury. Sectorial corneal epithelial defect in the quadrant corresponding to limbal stem-cell loss.
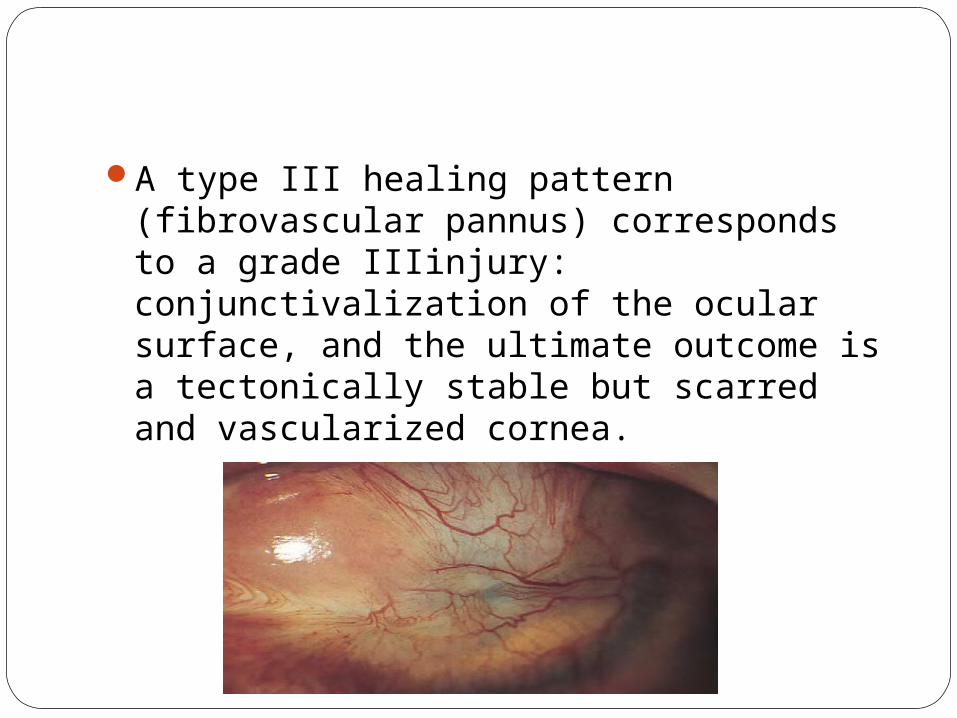
A type III healing pattern (fibrovascular pannus) corresponds to a grade IIIinjury: conjunctivalization of the ocular surface, and the ultimate outcome is a tectonically stable but scarred and vascularized cornea.
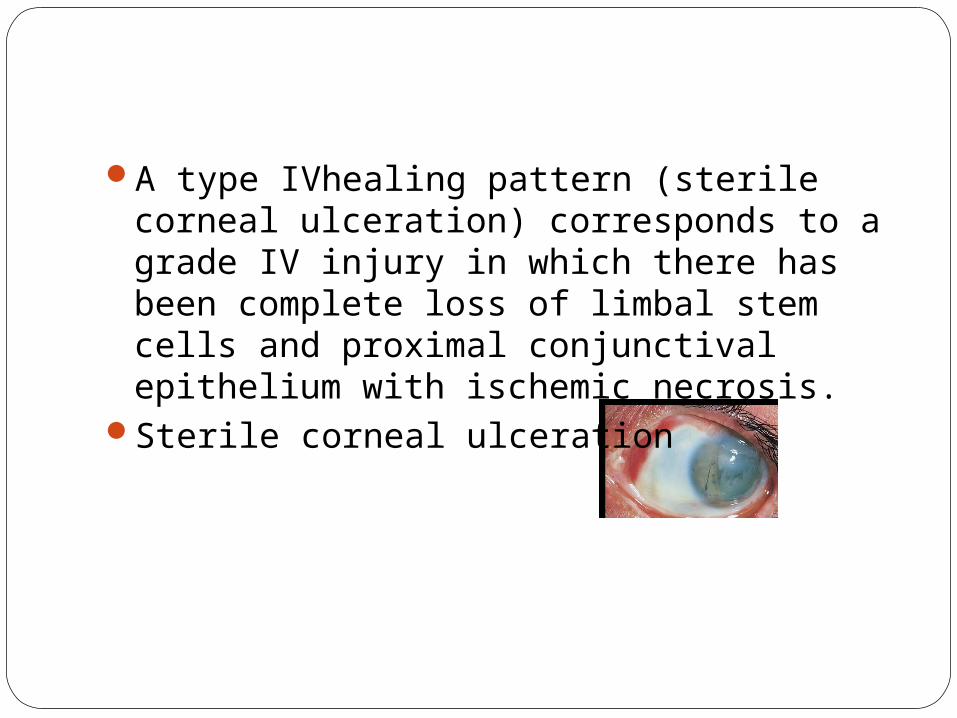
A type IVhealing pattern (sterile corneal ulceration) corresponds to a grade IV injury in which there has been complete loss of limbal stem cells and proximal conjunctival epithelium with ischemic necrosis.
Sterile corneal ulceration
TreatmentMedical therapy
Surgical therapy

MEDICAL THERAPYManagement of the severely chemically
injured eye must be directed toward: Promoting ocular surface epithelial
recovery with proper phenotypic transdifferentiation,
Augmenting corneal repair by supporting keratocyte collagen productionand minimizing ulceration related to collagenase activity, and
Controlling inflammation.
IrrigationEarly attempts at irrigation by the
patient and coworkers usually are inadequate, permitting significant penetration of the chemical agent.
Copious irrigation with any nontoxic irrigating solution must be immediately initiated on presentation, irrespective of the prior history of irrigation.
Irrigation for a minimum of 30 min and checking the pH of tears for evidence of neutrality is recommended.

Failure to achieve neutrality often is evidence of a retained reservoir of chemical in the eye.
This is particularly true in plaster injuries, in which particles embedded in the upper tarsal conjunctiva can provide continued slow release of alkali into the tear film.
Using topical anesthesia, all particles should be removed with fine forceps or by
scraping with a disposable scalpel (e.g., Bard–Parker No. 15 blade).
DébridementDébridement of necrotic corneal
epithelium is necessary to allow proper reepithelialization, irrespective of the severity of the injury.
It is important to débride necrotic conjunctival tissue because this tissue has been shown to be a nidus of continued inflammation from retained caustic materials.
PROMOTE EPITHELIAL WOUND HEALINGAND DIFFERENTIATIONThe recovery of an intact and
phenotypically normal corneal epithelium is the rate-limiting determinant of prognosis of a chemical injury.
Initially, aggressive medical therapy is indicated to facilitate reepithelialization.

Tear SubstitutesThe use of topical Tear Substitutes may
be useful in facilitating corneal epithelial migration ingrade I and II injuries and in minimizing conjunctival scarring and symblepharon formation after grade III and IV injuries.
After reepithelialization, frequent administration of unpreserved tear substitutes and administration of ointments at bedtimemay be necessary to benefit persistent keratopathy and recurrent epithelial erosions.
Occlusive therapyAlthough there is a theoretical advantage
to protecting the migrating epithelium from the ‘windshield-wiper’ effect of the eyelids, occlusive therapy (patching, taping) is of little use in the acute care of the chemically injured eye.
If epithelial defects persist into the early and late repair phases, the cause usually is persistent inflammation or limbal stem-cell deficiency, both of which are unresponsive to occlusive therapy.

Hydrophilic Contact LensMay facilitate corneal epithelial
regeneration and prevents symblepheron formation.
Lens with greatest oxygen permeability should be preferred.

SUPPORT REPAIR AND MINIMIZEULCERATION Ascorbate It is a cofactor in the rate-limiting step of collagen
formation.
Damage to the cilliary body epithelium by intraocular chemical injury results in decreased secretion of ascorbate and a reduction in its concentration in the anterior chamber.
Both topical and systemic ascorbate have been shown to decrease the incidence of sterile corneal ulceration after chemical injury.
Topical application is superior to systemic supplementation.
Collagenase InhibitorsTetracycline derivatives are efficacious in
reducing collagenase activity. It is due to chelation of zinc at the active
site of the collagenase enyzme.Doxycycline is the most potent tetracycline
collagenase inhibitor.

CONTROL INFLAMMATIONCorticosteroids:Corticosteroids traditionally have been the
mainstay of therapy for the reduction of tissue injury related to acute inflammation.
Corticosteroids have no adverse effect on the rate of epithelial wound healing.( in the setting of acute inflammation)
By decreasing inflammatory cell infiltration, they may facilitate migration indirectly by partially ameliorating inflammation-induced delays in corneal epithelial migration.

Corticosteroids do interfere with stromal repair by impairing both keratocyte migration and collagen synthesis.
Fortunately, the deleterious effects of corticosteroids do not become apparent until the early repair phase.
The key to successful corticosteroid use is to maximize the antiinflammatory effect during the ‘window of opportunity’ in the first 7–10 days, when there is little risk associated with corticosteroid use.
Late repair phase corticosteroid-related complications are more likely to occur.
Therapy can be modified by tapering corticosteroids by substituting progestational steroids nonsteroidal antiinflammatory drugs (NSAIDs).

Progestational Steroids
Progestational steroids have less antiinflammatory potency than do corticosteroids but have only a minimal effect on stromal repair and collagen synthesis.
Medroxyprogesterone 1% to inhibit collagenase and reduce ulceration after chemical injury.

Progestational steroids may be substituted for corticosteroids after 10–14 days, when suppression of inflammation still is required but interference with stromal repair is undesirable.

NSAIDsNSAIDs may prove to be an effective
additive for corticosteroids in the first week and a substitute or additive for progestational steroids after the first week.

CitrateCitrate is a calcium chelator that decreases
the membrane and intracellular levels of calcium, resulting in impaired chemotaxis, phagocytosis, and release of lysosomal enzymes of polymorphonuclear leukocytes.
It significantly reduces the incidence of corneal ulceration.

SURGICAL THERAPYCONJUNCTIVAL AND TENON’S
ADVANCEMENT (TENOPLASTY)The use of conjunctival and Tenon’s
advancement, or tenoplasty, is based on the principle of using vital connective tissue within the orbit to reestablish limbal vascularity and to facilitate corneal reepithelialization with conjunctival epithelium.
This technique is recommended to facilitate initial stabilization of a grade IV injury.
AMNIOTIC MEMBRANE TRANSPLANTATIONAM Action Mechanisms Provides a new basement membraneProvides a new stroma that exerts Antiinflammatory action Antiscarring action Antiangiogenic action

It consists of an avascular stromal matrix, a thick basement membrane, and an epithelial monolayer.
When used with the basement membrane
oriented downward, the amniotic membrane acts like a biologic bandage contact lens or an ‘onlay’ (patch) graft, promoting epithelialization beneath the membrane.
When used with basement membrane oriented upward it acts like an ‘inlay’ graft, which promotes epithelialization over its surface.
Irrespective of the transplantation technique, amniotic tissue facilitate reepithelialization if complete or partial limbalstem-cell function is present.

In cases of incomplete limbal stem-cell loss, it may be effective in the treatment of persistent epithelial defects, recurrent epithelial erosions, and persistent epitheliopathy, and in the reduction of chronic inflammation.
In cases of complete limbal stem-cell function, it may be used in conjunction with limbal stem-cell transplantation.

LIMBAL STEM-CELL TRANSPLANTATIONThis technique is the best method of
reestablishing a phenotypically correct corneal epithelial surface early in the clinical course of a grade III or IV injury.
Conjunctival limbal autograft transplantation (CLAU):
In unilateral cases of chemical injury or asymmetric chemical injuries.
Is usually performed by harvesting contralateral limbal stem cells from the uninjured or less injured fellow eye.

In severe bilateral injuries, limbal allograft transplantation from a living relative or a cadaver donor are the only viable options.
Living-related conjunctival limbal allograft transplantation (lr-CLAG):the limbal stem
cells are harvested from a close relative and transferred to the injured eye.

Keratolimbal allograft transplantation (KLAT)
It is a technique for transferring limbal stem cells from a donor cadaver to treat severe bilateral injuries.
Ex vivo expansion of limbal stem cells:This procedure involves the dissection of
a small piece of donor limbal tissue, growth and expansion of viable limbal stem cells in culture, and transplantation of the epithelial sheet to the recipient eye.


MUCOSAL MEMBRANE TRANSPLANTATIONMechanical abnormalities of the bulbar and
palpebral conjunctiva related to progressive scarring include restriction of extraocular movement, fornix foreshortening and obliteration, symblepharon formation, incomplete lid closure, cicatricial entropion, trichiasis, and lid margin keratinization.
In bilateral cases, mucosal membrane grafts are used to reconstruct the fornix and restore normal lid–globe relations.
Such grafts do not restore the corneal epithelial functions.
Harvesting of mucosal grafts from nasal mucosa may improve impaired goblet cell function of the conjunctiva.
PENETRATING KERATOPLASTYAn optical penetrating keratoplasty may
be attempted after appropriate rehabilitation of the ocular surface has been achieved.
Performing limbal stem-cell transplantation prior to penetrating keratoplasty or doing the procedures simultaneously in order to facilitate more rapid visual rehabilitation.

KERATOPROSTHESISKeratoprosthesis may be useful in bilateral,
severe chemical injury in which the prognosis is hopeless for penetrating
keratoplasty because of irreparable damage to the ocular surface.
Improved keratoprosthesis design and better postoperative management now offer an improved prognosis.


SPECIFIC THERAPY Acute Phase1. Topical corticosteroids every 1–2 h.2. Topical sodium ascorbate 10% every 2 h.3. Topical sodium citrate 10% every 2 h.4. Topical tetracycline 1% ointment four times a day.5. Topical cycloplegics as needed.6. Topical antiglaucoma medications as needed.7. Systemic sodium ascorbate 2 g orally four times a day.8. Systemic doxycycline 100 mg orally twice a day.9. Consider amniotic membrane transplantation. (grade II and III)10. Consider conjunctival and Tenon’s advancement. (grade IV)
Early Repair Phase1. Discontinue or taper (with close
observation) topical corticosteroids.2. Begin progestational steroids (Provera
1%), NSAIDs, or both, topically every 1-2 hr.
3.Continue topical and systemic sodium ascorbate.
4. Continue topical sodium citrate.5. Continue topical tetracycline and
systemic doxycycline.

Late Repair Phase1. Taper medical therapy after
reepithelialization is complete(grade I or II).
2. Limbal stem-cell transplantation +/– amniotic membrane transplantation (for grade III or IV injuries).
3. Tectonic procedures (tissue adhesive, small- or largediameter keratoplasty), if necessary.
Late Rehabilitation1. Ocular surface reconstruction (amniotic
membrane transplantation, conjunctival transplantation, mucous membrane transplantation).
2. Limbal stem-cell transplantation.3. Penetrating keratoplasty.4. Keratoprosthesis.

BEWARE OF !!!














![Seminar at Bogor -Chemical Contaminants- Submission [Compatibility Mode]](https://static.documents.pub/doc/80x56/55cf9966550346d0339d3340/seminar-at-bogor-chemical-contaminants-submission-compatibility-mode.jpg)



