UNIVERSITATIS OULUENSIS MEDICA ACTA D OULU 2006 D 878 Jouko Laurila SURGICALLY TREATED ACUTE ACALCULOUS CHOLECYSTITIS IN CRITICALLY ILL PATIENTS FACULTY OF MEDICINE, DEPARTMENT OF ANAESTHESIOLOGY, DEPARTMENT OF SURGERY, DEPARTMENT OF PATHOLOGY, UNIVERSITY OF OULU; DEPARTMENT OF INFECTION CONTROL, OULU UNIVERSITY HOSPITAL D 878 ACTA Jouko Laurila
Transcript
ABCDEFG
UNIVERS ITY OF OULU P .O . Box 7500 F I -90014 UNIVERS ITY OF OULU F INLAND
A C T A U N I V E R S I T A T I S O U L U E N S I S
S E R I E S E D I T O R S
SCIENTIAE RERUM NATURALIUM
HUMANIORA
TECHNICA
MEDICA
SCIENTIAE RERUM SOCIALIUM
SCRIPTA ACADEMICA
OECONOMICA
EDITOR IN CHIEF
EDITORIAL SECRETARY
Professor Mikko Siponen
Professor Harri Mantila
Professor Juha Kostamovaara
Professor Olli Vuolteenaho
Senior assistant Timo Latomaa
Communications Officer Elna Stjerna
Senior Lecturer Seppo Eriksson
Professor Olli Vuolteenaho
Publication Editor Kirsti Nurkkala
ISBN 951-42-8097-0 (Paperback)ISBN 951-42-8098-9 (PDF)ISSN 0355-3221 (Print)ISSN 1796-2234 (Online)
FACULTY OF MEDICINE, DEPARTMENT OF ANAESTHESIOLOGY, DEPARTMENT OF SURGERY, DEPARTMENT OF PATHOLOGY,UNIVERSITY OF OULU;DEPARTMENT OF INFECTION CONTROL,OULU UNIVERSITY HOSPITAL
D 878
AC
TA Jouko Laurila
D878etukansi.kesken.fm Page 1 Tuesday, May 2, 2006 10:22 AM
A C T A U N I V E R S I T A T I S O U L U E N S I SD M e d i c a 8 7 8
Academic Dissertation to be presented with the assent ofthe Faculty of Medicine, University of Oulu, for publicdiscussion in the Auditorium 1 of Oulu UniversityHospital, on May 26th, 2006, at 12 noon
Laurila, Jouko, Surgically treated acute acalculous cholecystitis in critically illpatientsFaculty of Medicine, Department of Anaesthesiology, Department of Surgery, Department ofPathology, University of Oulu, P.O.Box 5000, FI-90014 University of Oulu, Finland; Department ofInfection Control, Oulu University Hospital, P.O. Box 22, FI-90029 OYS, Finland Acta Univ. Oul. D 878, 2006Oulu, Finland
AbstractAcute acalculous cholecystitis (AAC) is an insidious and increasingly recognized complication ofcritical illness, whose pathogenesis is poorly understood and clinical picture obscure. Diagnosis isdifficult and there is no consensus on treatment.
The medical records of all ICU patients who had undergone open cholecystectomy due to AACduring the years 2000–2001 and 2003–2004 were examined for clinical and organ failure data. Theindication for open cholecystectomy was a suspicion of AAC based on clinical signs and symptomsof sepsis or deteriorating multiple organ dysfunction without other obvious foci and/or radiological(computed tomography or ultrasound) findings indicative of cholecystitis.
A total of 73 patients had operatively treated AAC during the study periods, giving an incidenceof 0.9% of all admissions (73/8184) and an incidence of 6.7% among the long-stayers (ICUstay >5days). The hospital mortality of these patients was 43%. Infection was the most common admissiondiagnosis followed by cardiovascular surgery. The patients were severely ill, the mean (SD)APACHE II score being 25.5 (6.4) and the mean (SD) SOFA score 10.2 (3.5) on admission. In thosepatients who had AAC as the only intra-abdominal complication of multiple organ dysfunction,cholecystectomy was followed by a remarkable improvement of individual and total SOFA scores bythe seventh postoperative day.
The AAC gallbladders were histologically and immunohistologically compared to normalgallbladders and to gallbladders of patients with acute calculous cholecystitis (ACC). The ACCpatients were admitted into hospital because of primary acute gallbladder disease, were treated on anormal ward and did not have severe sepsis or multiple organ dysfunction. The typicalhistopathological features of AAC (34 cases) in the gallbladder wall were bile infiltration, lymphaticdilatation and leucocyte margination of blood vessels, while epithelial degeneration and defects,widespread occurrence of inflammatory cells and extensive and deep muscle layer necrosis weretypical features of ACC (28 cases).
Tight junction proteins (claudin-1, -2, -3, -4, occludin, ZO-1 and E-cadherin) were uniformlyexpressed in normal gallbladder epithelium, with the exception of claudin-2, which was present inless than half of the cells. In AAC, the expression of cytoplasmic occludin and claudin-1 wasdecreased compared to control group. In ACC, the expression of claudin-2 was increased, but theexpression of claudin-1, -3 and -4, occludin and ZO-1 was decreased compared to normal or AACgallbladders.
In conclusion, AAC is associated with severe illness, infection, long intensive care unit stay anddeteriorating multiple organ dysfunction. Open cholecystectomy is one important contributing factorto reverse the course of multiple organ dysfunction in these patients. Histological andimmunohistological studies suggest that AAC is a manifestation of systemic inflammatory disease,while ACC is a local inflammatory and often infectious disease.
Keywords: acalculous cholecystitis, intensive care, multiple organ dysfunction, sequentialorgan failure assessment, surgery of gallbladder, tight junction
Acknowledgements
This study was carried out in the Intensive Care Unit, Department of Anaesthesiology, Oulu University Hospital, in co-operation with the Departments of Infection Control and Surgery and the Department of Pathology, University of Oulu, in the years 2000-2006.
I wish to express my sincere gratitude to: Professor Tero Ala-Kokko, M.D., Ph.D., Head of the ICU and my supervisor, for his
tireless encouragement and generous support during this study. Our excellent cooperation in research and clinical work has been of utmost importance during these years.
Professor Seppo Alahuhta, M.D., Ph.D., Head of the Department of Anaesthesiology, for providing me optimal working conditions during the course of this study.
Docent Hannu Syrjälä, M.D., Ph.D., Head of the Department of Infection Control, my second supervisor, for most valuable support and guidance during this work and all the years we have worked together in the ICU.
Juha Saarnio, M.D., Ph.D., for close cooperation in clinical work and research and for sincere friendship during these years. His encouraging emails even during the small hours of the day were of great help in accomplishing this work.
Vesa Koivukangas, M.D., Ph.D, for his valuable work as a co-author and for his keen interest in research and clinical work in the intensive care unit.
Docent Tuomo Karttunen, M.D., Ph.D., and Docent Ylermi Soini, M.D., Ph.D., for excellent scientific collaboration.
Professor Olli Takkunen, M.D., Ph.D., and Docent Hannu Paajanen M.D., Ph.D., the official reviewers of this manuscript, for their constructive criticism and expert advice.
All my colleagues in the Department of Anaesthesiology, both those who have worked with me daily in the ICU and those who have visited ICU less frequently but have worked hard in the evenings and during the nights. Special thanks go to my colleague and teacher Erkki Saarela, M.D., who was Head of the ICU at the time when I started my work there.
All my colleagues in the Departments of Surgery, Neurosurgery, Infection Control, Internal Medicine and Radiology for very good cooperation during these years.
The staff of the intensive care unit for excellent cooperation throughout these years. In spite of your hard work, you have had time for joy and laughter. Special thanks go to the study nurses Maarit Finnberg, Tarja Lamberg and Sinikka Sälkiö, who always were
willing to help me with the data. Special thanks also go to Ms Riitta Vuento for her skilful technical assistance in the studies III and IV.
Pasi Ohtonen, MSc for statistical advice. Sirkka-Liisa Leinonen, Lic. Phil., for the careful revision of the English of the original
papers and this thesis. Finally, I wish to express my warmest thanks to my wife Päivi for taking care of our
home and children while I spent time on this project. She was also my co-author, helped with the statistics and figures of the publications and persistently fought against the viruses that threatened “my data”. Without her loving support and encouragement, this work would have never been completed.
Special thanks belong to my children Katja, Elisa, Mikko and Hanna for the joy and laughter they bring to our everyday life and for their patience and belief that this work would be finished some day. Maybe this summer…
This work was financially supported by Health Care Foundation of North Finland, which is gratefully acknowledged.
Abbreviations
AAC acute acalculous cholecystitis ACC acute calculous cholecystitis APACHE acute physiology and chronic health evaluation score CT computed tomography GI gastrointestinal IBD inflammatory bowel disease ICU intensive care unit JAM junctional adhesion molecule MODS multiple organ dysfunction syndrome MOF multiple organ failure SAPS simplified acute physiology score SIRS systemic inflammatory response syndrome SOFA sequential organ failure assessment TJ tight junction US ultrasonography WBC white blood cell
List of original publications
This thesis is based on the following original articles, which are referred to in the text by their Roman numerals. In addition, some unpublished data are presented.
I Laurila J, Syrjälä H, Laurila PA, Saarnio J & Ala-Kokko TI (2004) Acute acalculous cholecystitis in critically ill patients. Acta Anaesthesiol Scand 48: 986-991.
II Laurila J, Laurila PA, Saarnio J, Koivukangas V, Syrjälä H & Ala-Kokko TI (2006) Organ system dysfunction following open cholecystectomy for acute acalculous cholecystitis in critically ill patients. Acta Anaesthesiol Scand 50: 173-179.
III Laurila JJ, Ala-Kokko TI, Laurila PA, Saarnio J, Koivukangas V, Syrjälä H & Karttunen TJ (2005) Histopathology of acute acalculous cholecystitis in critically ill patients. Histopathology 47: 485-492.
IV Laurila JJ, Karttunen TJ, Koivukangas V, Laurila PA, Syrjälä H, Saarnio J, Soini Y & Ala-Kokko TI. Expression of tight junction proteins in acute acalculous and calculous cholecystitis. (Submitted).
Contents
Abstract Acknowledgements Abbreviations List of original publications Contents 1 Introduction ................................................................................................................... 13 2 Review of the literature ................................................................................................. 15
2.1 Anatomy, physiology and histology of the gallbladder...........................................15 2.2 Acute acalculous cholecystitis (AAC) ....................................................................16
2.2.1 Historical aspects and incidence......................................................................16 2.2.2 Etiology and pathophysiology .........................................................................17
2.2.2.1 Visceral hypoperfusion and ischemia .......................................................17 2.2.2.2 Systemic inflammatory response ..............................................................18 2.2.2.3 Bile stasis..................................................................................................19
2.2.3 Diagnosis of AAC............................................................................................20 2.2.3.1 Clinical signs, symptoms and laboratory investigations...........................20 2.2.3.2 Ultrasonography .......................................................................................20 2.2.3.3 Computed tomography .............................................................................21 2.2.3.4 Hepatobiliary scintigraphy........................................................................21 2.2.3.5 Percutaneous aspiration of gallbladder .....................................................22 2.2.3.6 Histological findings in cholecystitis........................................................22
2.3 Tight junctions.......................................................................................................24 2.3.1 General structure of the tight junctions............................................................24 2.3.2 TJ proteins .......................................................................................................26
2.3.2.3 JAMs ........................................................................................................28 2.3.2.4 ZO family.................................................................................................28 2.3.2.5 E-cadherin ................................................................................................28
2.3.3 Tight junctions and diseases ............................................................................29 3 Aims of the study........................................................................................................... 30 4 Patients and methods ..................................................................................................... 31
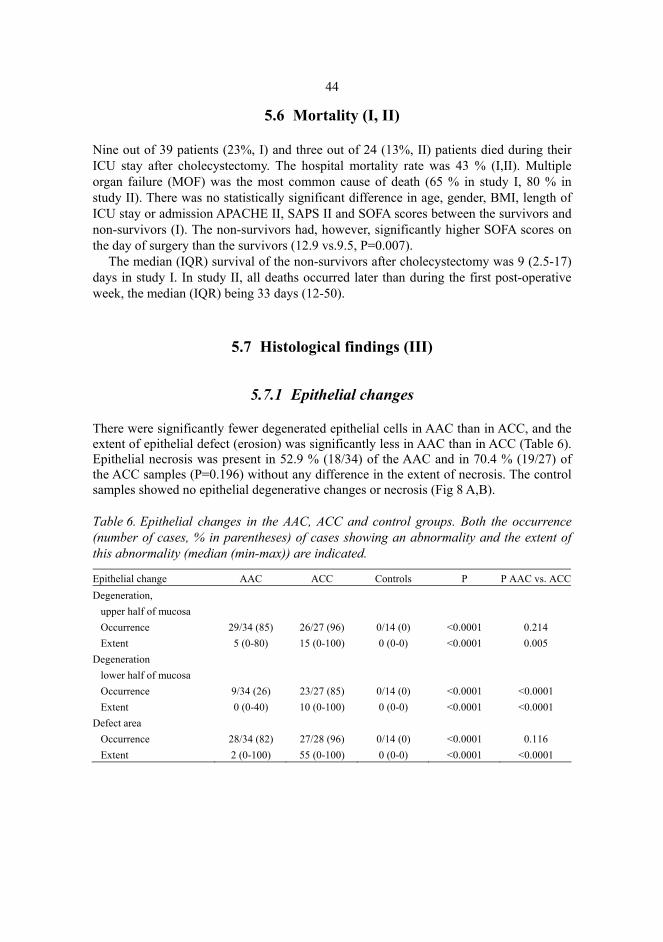
5.7.1 Epithelial changes............................................................................................44 5.7.2 Inflammatory cells...........................................................................................45 5.7.3 Lymphatic follicles and vascular changes .......................................................45 5.7.4 Bile infiltration and Rokitansky-Aschoff sinuses ............................................45 5.7.5 Necrosis in the muscle layer and subserosal adipose tissue.............................45
6 Discussion ..................................................................................................................... 53 6.1 General discussion..................................................................................................53 6.2 Incidence and concomitant factors of AAC............................................................53 6.3 Diagnostic and treatment challenges ......................................................................54 6.4 Multiple organ failure and outcome........................................................................55 6.5 Histological findings...............................................................................................56 6.6 Tight junction proteins in AAC and ACC...............................................................56
7 Conclusions ................................................................................................................... 58 References Original publications
1 Introduction
Acute acalculous cholecystitis (AAC) refers to acute inflammation of the gallbladder in the absence of gallstones (Glenn & Becker 1982, Barie & Eachempati 2003). Acute calculous cholecystitis (ACC) is caused by gallstones that obstruct the cystic duct and lead to distension, edema, bile stasis, inflammation and, often, bacterial infection of the gallbladder (Crawford 1999).
To date, the literature concerning AAC in critically ill patients is quite limited. There are some retrospective reports on patient series focusing mainly on predicting factors and diagnostic findings (Flancbaum et al. 1985, Shapiro et al. 1994, Molenat et al. 1996, Mariat et al. 2000, Puc et al. 2002, Ryu et al. 2003, Wang et al. 2003) but there are no studies comparing the different treatment modalities. In most cases, AAC has been reported as a complication of trauma or in postoperative patients. During the last few decades, AAC has been diagnosed with increasing frequency in ICU patients, probably because more and more seriously ill patients are treated for longer times in ICU (Glenn & Becker 1982, Barie & Eachempati 2003). The growing awareness of AAC and the improved imaging technologies have also led to an increasing number of AAC diagnoses.
There are no generally accepted diagnostic criteria for AAC, and the treatment of choice of AAC is also controversial (Melin et al. 1995, Boggi et al. 1999, Shapiro 1999, McChesney et al. 2003). There are, for example, no prospective controlled studies available to compare the conservative, percutaneous and surgical treatments of AAC. Furthermore, there are only a few studies concerning the histological changes in AAC, and the histopathology described so far has mostly been considered similar in acalculous and calculous cholecystitis (Glenn 1979, Jessurun & Albores-Saavedra 2001).
Gut hypoperfusion has a pivotal role in the development of multiple organ dysfunction syndrome (MODS) in septic patients (Doig et al. 1998, Hassoun et al. 2001). It is also proposed to be an important factor in the pathogenesis of AAC (McChesney et al. 2003). Recently, there has been growing interest in the study of the epithelial barrier function and its role in the pathophysiology of MODS in critically ill patients (Fink & Delude 2005). In this respect, tight junctions (TJ), i.e. the apical cell-cell contacts in epithelial and endothelial cell sheets, may be important. So far, however, tight junctions have been investigated only in experimental sepsis models, but not in septic or critically ill patients or even in normal or inflamed gallbladders.
14
This study was carried out to evaluate the incidence, predisposing factors, clinical picture and diagnostic and histological features of surgically treated AAC and to find out the effect of surgical treatment on organ function in critically ill patients having AAC.
2 Review of the literature
2.1 Anatomy, physiology and histology of the gallbladder
Bile is formed in hepatic cells, and it is composed of bile salts, cholesterol, lecithin, bilirubin and electrolytes. The main function of bile is to facilitate the absorption of fatty acids and other lipids from the intestinal tract.
The gallbladder of a normal adult is a pear-shaped sac, 10 cm long and 3-4 cm wide, with a volume of 40 – 70 ml, lying in the depression of the posterior aspect of the right lobe of the liver. Its wall is 1-2 mm thick, depending on whether the organ is in a relaxed or contracted state. The primary functions of the gallbladder are to concentrate, store and release bile. It also liberates mucosubstances from its surface epithelial cells and the mucous glands. Approximately 800 – 1000 ml of bile flows daily into the gallbladder from the liver. The contraction and evacuation of the gallbladder are promoted mainly by cholecystokinin liberated from the proximal small intestine. (Frierson 1992).
The gallbladder absorbs water from bile. If too much water or bile acids are absorbed, if too much cholesterol is secreted in bile, or if the evacuation of the gallbladder is impaired, gallstones may develop. About 90 percent of gallstones are composed of cholesterol, while the remainder are made of pigments, such as calcium salts and bilirubin. Biliary sludge is a mixture of cholesterol crystals and calcium salts present in bile and may progress to gallstones or completely disappear. Biliary sludge may also lead to complications, including acute cholecystitis and acute pancreatitis (Lee et al.1992, Ko et al. 1999).
The blood supply to the gallbladder comes from the celiac trunk, through the common hepatic and right hepatic arteries into the cystic artery, which again divides into two arteries, one in the free surface of the gallbladder and the other between the gallbladder and the liver. However, significant individual variation exists. The superior mesenteric artery supplies the whole small bowel from the duodenum to the caecum, the ascending colon and a great part of the transverse colon. The inferior mesenteric artery supplies the remainder of the colon and the rectum. The splanchnic venous circulation passes through the portal venous system, and the venous drainage of the gallbladder leads partly directly to the liver and partly to the portal venous system. (Frierson 1992).
16
Lymphatic channels from the gallbladder lead to lymph nodes on the gallbladder neck or the cystic duct, and these channels then lead superiorly to lymph nodes near the hepatic hilum or inferiorly to lymph nodes of the hepatoduodenal ligament and then to lymph nodes on the celiac axis (Frierson 1992).
The gallbladder is innervated from the hepatic branch of the celiac nerve, which consists primarily of sympathetic fibres, and from the hepatic branch of the vagus nerve, which consists primarily of parasympathetic fibres (Tabata 1994). The gallbladder wall consists of surface epithelium, lamina propria, smooth muscle, subserosal fat and peritoneal surface. The folds surrounding the lumen of the gallbladder are lined by a single row of tall columnar cells with basally located nuclei. These cells are supported by fine lamina and lamina propria with numerous small blood vessels. The lamina propria contains, in addition to small blood vessels, loose connective tissue, elastic fibres, nerve fibres and lymphatic channels. The smooth muscle consists of loosely arranged bundles of circular, longitudinal and oblique fibres that do not form well-developed layers. The subserosal layer contains adipocytes, collagen fibres, fibroblasts, blood vessels, nerves and lymphatics. Rokitansky-Aschoff sinuses represent herniations of epithelium into lamina propria, smooth muscle or subserosal connective tissue. (Frierson 1992)
2.2 Acute acalculous cholecystitis (AAC)
2.2.1 Historical aspects and incidence
AAC refers to acute inflammation of the gallbladder without evidence of gallstones and it occurs in 2-15 % of all cases of acute cholecystitis (Howard 1981, Glenn & Becker 1982, Johanning & Gruenberg 1998). Common preceding factors are major surgery, multiple trauma and burn injury, but sepsis, end-stage renal disease, leukemia, bone marrow transplantation and systemic lupus erythematosus have also been associated with AAC (McDermott et al. 1985, Stevens et al. 1988, Raunest et al. 1992, Topeli et al. 1996, Wiboltt & Jeffrey 1997, Kamimura et al. 1998, Rady et al. 1998, Wang et al. 2003).
AAC rarely occurs as an isolated event, but normally accompanies MODS and most often develops on the second week of severe illness or later (Rady et al. 1998, McChesney et al. 2003). Most AAC patients are male (Thompson et al. 1962, Shapiro et al.1994). In children, acute acalculous cholecystitis represents 30 - 70 % of all cases of acute cholecystitis, and infection and trauma are common preceding factors (Tsakayannis et al. 1996, Imamoglu et al. 2002). In this work, we concentrate on AAC as a complication of severe illness in adult patients.
AAC was first described 160 years ago by Duncan, who reported a fatal case of perforated acalculous cholecystitis in a patient who had undergone surgery for a femoral hernia (Duncan 1844). By 1970, altogether 80 sporadic cases of AAC had been reported in the English-language literature (Lindberg et al. 1970). This includes one series of 12 Vietnam war casualties who developed AAC during their recovery 10 to 35 days after the primary injury and after 2-11 surgical procedures prior to cholecystectomy. The incidence
17
of AAC in severely wounded US soldiers in USAF Hospital during Vietnam war was 0.5 % (12/ 2412). (Lindberg et al. 1970)
Our present knowledge about AAC in intensive care patients is still based mainly on case reports and retrospective studies, and there are only a few prospective studies with small patient series. In addition, the verification of AAC in these studies has been based variably on clinical, imaging, laboratory and operative findings.
In a retrospective review of over 10,000 surgical intensive care patients, the incidence of operatively confirmed AAC was 0.2 % (Kalliafas et al. 1998). After cardiovascular surgery, the incidence of AAC has been shown to be 0.3-0.5 % (Sessions et al. 1993, Rady et al. 1998, Barie & Eachempati 2003, McChesney et al. 2003) and after aortic surgery 0.7 -0.9 % (Ouriel et al. 1984, Hagino et al. 1997). In ICU long-stayers (> 7 days) the incidence of AAC after cardiovascular surgery was 3 % (30 / 876) (Rady et al. 1998). In a prospective study of 92 ICU patients with acute renal failure, the incidence of AAC based on ultrasonography (US) and laboratory criteria was 17 % (Stevens et al. 1988). AAC was also screened in two studies of multiple trauma patients (injury severity score >11), where 10.6 % and 18 % of the patients developed US criteria of AAC and, respectively, 4.4 % and 8.2 % underwent cholecystectomy confirming the AAC diagnosis (Raunest et al. 1992, Pelinka et al. 2003). The incidence of AAC was recently studied in a mixed medical-surgical ICU, and 4 % (14/346) of the patients developed operatively confirmed AAC (Mariat et al. 2000).
The reported mortality of ICU patients with AAC has been high (22 - 71 %) reflecting the severe underlying diseases (Stevens et al. 1988, Hagino et al.1997, Kalliafas et al. 1998, McChesney et al. 2003, Pelinka et al. 2003).
2.2.2 Etiology and pathophysiology
The etiology of AAC is considered to be multifactorial, and the precise pathophysiology is still unclear. Ischemia and reperfusion injury, systemic inflammatory response and biliary stasis are the most often proposed mechanisms for the disease.
2.2.2.1 Visceral hypoperfusion and ischemia
Normally, the hepato-splanchnic blood flow accounts for 25-30 % of cardiac output and the regional oxygen extraction in the splanchnic region is slightly higher than whole-body extraction (Dahn et al. 1987). In acute cardiogenic or hypovolemic shock, the sympathetic nervous system and other vasoactive mediators cause strong vasoconstriction in the mesenteric resistance and capacitance vessels providing a large blood volume to the vital organs reducing the splanchnic flow (Toung et al. 2000). In an experimental fat embolism model, decreased systemic oxygen delivery was followed by a decrease of mesenteric oxygen delivery, but intestinal oxygenation remained unaffected, probably due to increased oxygen extraction (Rautanen et al. 1996).
18
In septic shock, the splanchnic circulation is regulated by numerous inflammatory mediators, and the splanchnic flow can be normal, increased or decreased. In addition to the changes in flow, tissue integrity can be compromised by increased metabolism, impaired oxygen extraction and possible redistribution of flow (Tenhunen et al. 2003).
The assumption that visceral hypoperfusion and hypotension are important mechanisms for AAC is supported by the fact that AAC has mostly been described in association with hypovolemic shock, major surgery, multiple trauma or septic shock (Lindberg et al. 1970, Kalliafas et al. 1998, Rady et al. 1998, McChesney et al. 2003). Decreased arterial pressure combined with possibly increased intraluminal pressure impairs gallbladder perfusion and easily results in ischemia. Ischemia, on the other hand, renders the gallbladder mucosa vulnerable to the toxic effects of bile acids. Furthermore, the gallbladder vessels have been shown to be very sensitive to various inflammatory mediators (Becker et al. 1980, Cullen et al. 2000). Vasoactive drugs, which are commonly used in these situations, can also impair splanchnic circulation (De Backer et al. 2003, Martikainen et al. 2003). In addition, the increased sympathetic tone often associated with these situations, may be important. In animal studies sympathectomy has prevented experimental AAC in shock (Howard et al. 1952).
The assumption of ischemia as an important pathogenetic factor in AAC is also supported by microangiographic findings. Severe microcirculatory disturbances and small vessel occlusion were shown in AAC in contrast to ACC, where strongly dilated arterioles and regular filling of the capillary network was found (Warren 1992, Hakala et al. 1997). In addition to ischemia, reperfusion injury can be a significant pathogenetic factor as well. Taoka produced macroscopic and histologic cholecystitis in dogs by 45 minutes of ischemia followed by 90 minutes of reperfusion, whereas ischemia alone did not induce cholecystitis (Taoka 1991). The autonomic nervous system may also have a role in the development of AAC, because an animal study showed that ischemia-reperfusion after autonomic denervation caused more severe cholecystitis than ischemia-reperfusion alone (Tabata 1994). This could explain the increased risk of AAC after gastrectomy and esophagectomy with vagotomy (Inoue & Mishima 1988, Paull 2001).
2.2.2.2 Systemic inflammatory response
The systemic response to injury, trauma or infection includes a huge number of different mediators, including pro- and anti-inflammatory cytokines, activated neutrophils, monocytes, microvascular endothelial cells, neuroendocrine reflex and complement, coagulation and fibrinolytic system (Bone et al. 1992, Levy et al. 2003, Hotchkiss & Karl 2003, Annane et al. 2005). This response functions to save the organism and results in recovery and rehabilitation. The response can also be overwhelming and break out of control, leading to multiple organ failure and death. AAC may represent one end-organ phenomenon in this response. In animal studies, endotoxin and inflammatory mediators, such as activated factor XII and platelet-activating factor, have been shown to induce acute inflammation in the gallbladder wall similar to that seen in clinical AAC (Becker et al. 1980, Kaminski et al. 1990, Kaminski et al. 1994, Cullen et al. 2000). Subsequently, endotoxin has been demonstrated to decrease bile acid synthesis and secretion, and this,
19
together with gallbladder hypomotility, has been suggested to predispose to bacterial proliferation, translocation and endotoxin absorption in the small intestine, resulting in a vicious circle. These studies have also suggested that the gallbladder wall may be more sensitive to the effects of inflammatory mediators than other areas of the alimentary tract or other organs (Becker et al. 1980, Cullen et al. 2000). The mechanism of how inflammatory mediators influence epithelial cells and the barrier function in critical illness is not completely clear. Alterations in the structure and function of epithelial and endothelial tight junctions may be important in the pathogenesis of end-organ failures in MODS (McConnell & Coopersmith 2005) (see chapter 2.3. Tight junctions).
2.2.2.3 Bile stasis
Bile stasis has been implicated in the pathogenesis of AAC for decades, and bile stasis may also alter the chemical composition of bile, which can promote local injury in gallbladder mucosa (Glenn & Becker 1982, Lee 1990, Barie & Eachempati 2003). Normally, a fatty meal causes vagal stimulation and cholecystokinin release from intestinal mucosa, which leads to contraction of the gallbladder and relaxation of the sphincter of Oddi, resulting in evacuation of the gallbladder. Dysfunction of gallbladder smooth muscle and dysfunction of the sphincter of Oddi have been shown to be associated with bile stasis and inflammation of the gallbladder wall similar to AAC (Parkman et al. 2000, Cullen et al. 2000, Barnes et al. 2004, Gomez-Pinilla et al. 2005). Endotoxin has also been shown to decrease the contractile responses of the gallbladder to hormonal and neural stimuli, leading to bile stasis (Cullen et al. 2000).
Fever, dehydration and fasting have been suggested to increase bile viscosity and to obstruct the cystic duct (Glenn 1947). Prolonged total parenteral nutrition has similarly been reported to result in AAC (Petersen & Sheldon 1979, Roslyn et al. 1983), but later studies have shown that AAC also developed in patients on enteral feeding and in patients not receiving parenteral nutrition (Savoca et al. 1990b, Shapiro et al. 1994, Rady et al. 1998).
Opioid analgesics may increase biliary pressure due to spasm of the sphincter of Oddi and the effect of morphine has been shown to be stronger than that of pethidine (Joehl et al. 1984, Wu et al. 2004). The role of opioids in the development of AAC has been emphasized in many reports, partly because most of the described patients have been trauma or postoperative patients in need of analgesics (Flancbaum et al. 1985, Pelinka et al. 2003). A notable proportion of them have also received multiple blood transfusions, and it has been suggested that transfusions lead to an increased bile pigment load and cause injury to the gallbladder wall (Lindberg et al. 1970). However, others have found no difference in the amount of blood transfused into AAC patients as compared with control patients (Long et al. 1978).
Bile stasis may also be induced by mechanical ventilation. In an animal study, ventilation with positive end-expiratory pressure of 7- 10 cmH2O increased hepatic venous pressure, decreased portal perfusion and increased resistance to flow through the choledochoduodenal junction (Johnson & Hedley-Whyte 1975). Different modes of mechanical ventilation may also have different effects on the gallbladder by decreasing or
20
increasing splanchnic perfusion and by inducing different hormonal and cytokine responses (Perttilä et al. 1989, Lee et al. 1998, Ranieri et al. 1999, Mutlu et al. 2001). On the other hand, many patients not on mechanical ventilation have developed AAC (Orlando et al. 1983, Flancbaum et al. 1985).
Most authors agree that the etiology of AAC can be multifactorial, and that the pathophysiology of the disease in any one patient can be a combination of the above mechanisms (Shapiro et al. 1994, Kalliafas et al. 1998, Rady et al. 1998). Bacterial invasion is generally regarded as a complication of an already diseased gallbladder (Boland et al. 1993).
2.2.3 Diagnosis of AAC
2.2.3.1 Clinical signs, symptoms and laboratory investigations
The diagnosis of AAC is usually based on clinical, laboratory, radiologic and/or operative findings. The clinical diagnosis is difficult because the majority of patients are critically ill, sedated and unable to communicate about their symptoms. The frequently presented clinical signs and symptoms of AAC are pain, tenderness and mass in the right upper abdominal quadrant, fever, nausea, vomiting, jaundice, diarrhoea, abdominal discomfort, alteration of mental status and sudden deterioration of overall clinical condition. These symptoms have, however, been nonspecific in critically ill patients and may be present or absent in AAC patients. Leukocytosis, leukopenia and elevated values of liver function tests are widely used to prove or disprove a suspicion of AAC, but their diagnostic value is also low. (Howard 1981, Flancbaum et al. 1985, Shapiro et al. 1994, Kalliafas et al. 1998, Rady et al. 1998, Pelinka et al. 2003, Trowbridge et al. 2003).
2.2.3.2 Ultrasonography
Ultrasonography is a widely recommended imaging modality of the gallbladder (Barie & Eachempati 2003, Wang et al. 2003). Sonographic findings in AAC include increased wall thickness (> 3.5 mm), increased gallbladder volume (hydrops), intraluminal sludge (increased echogenicity within the gallbladder lumen), pericholecystic fluid, sonographic Murphy’s sign (pain on inspiration while pressing on the gallbladder with the US probe) and presence of intramural gas. None of the above-mentioned findings alone are very sensitive, and a combination of three of them is generally needed for a diagnosis of AAC. (Raunest et al. 1992, Molenat et al. 1996, Mariat et al. 2000, Boland et al. 2000, Puc et al. 2002, Pelinka et al. 2003, Wang et al. 2003).
The sensitivity and specificity of US in AAC vary, depending on the patient population studied. In non-ICU patients the sensitivity and specificity of US in evaluating suspected acute cholecystitis is high, but in ICU patients diagnostic accuracy decreases remarkably (Boland et al. 1994, Shea et al. 1994, Puc et al. 2002, Pelinka et al. 2003). Imaging findings can be compromised by bowel gas, ascites and abdominal dressings and
21
drains. Several recent studies have documented the high incidence of abnormal gallbladder sonograms in ICU patients without evidence of the disease. In a study on 44 medical-surgical ICU patients, the gallbladder was systematically screened by ultrasound, and 57 % of the patients had at least three sonographic abnormalities. Only one of these patients developed AAC during the hospital stay. No statistical correlation was found between sonographic findings suggestive of cholecystitis and clinical or laboratory parameters. (Boland et al. 2000) In another study of 62 critically ill trauma patients, US had a sensitivity of only 30 % and specificity of 93 % in the detection of AAC (Puc et al. 2002). In a recent prospective study of 255 severely traumatized patients requiring intensive care for more than four days, 27 patients developed highly pathologic ultrasound changes in the gallbladder. However, six of these patients (22%) were closely monitored without any interventions and their US findings normalized within 3 weeks. (Pelinka et al. 2003) Futhermore, US has not been able to identify the patients likely to develop complications, such as necrosis and perforation (Wang et al. 2003). Despite some promising results of colour doppler ultrasound in the diagnosis of acute cholecystitis, the method has not proved very helpful in clinical practice (Jeffrey et al. 1995, Draghi et al. 2000, Boland et al. 2000).
2.2.3.3 Computed tomography
The most commonly described computed tomography (CT) findings in AAC are thickening of the gallbladder wall, mucosal irregularity, luminal distention, increased bile density (sludge), intramural or intraluminal gas, intraluminal hemorrhage, pericholecystic fluid collections and obscurity of the liver-gallbladder interface. The reported sensitivities and specificities of CT vary, but have generally been higher than for US. (Mirvis et al. 1986, Fidler et al. 1996, Harvey & Miller 1999, Bennett et al. 2002). In a recent study of CT findings in operatively confirmed acute cholecystitis (AAC and ACC), the sensitivity and specificity of preoperative CT were more than 90 %, but the sensitivity to discover gangrenous cholecystitis was only 29.3 % (Bennett et al. 2002). The disadvantages of CT are the need to transport the critically ill patient to the radiology department and the need for radiocontrast agent, which may be harmful for the renal function.
2.2.3.4 Hepatobiliary scintigraphy
Hepatobiliary scintigraphy is performed by administering intravenously iminodiacetic acid compounds labelled with radioactive technetium 99m, which are rapidly taken up and excreted by a normal liver. Isotope scanning is used to sequentially visualize the liver, extrahepatic bile ducts, gallbladder and duodenum. Nonvisualization of the gallbladder with normal visualization of the liver and bile ducts in 30 minutes – 4 hours supports the diagnosis of acute cholecystitis. (Prevot et al. 1999, Mariat et al. 2000, Barie & Eachempati 2003) In spite of some positive reports on the specificity and sensitivity of cholescintigraphy in critically ill patients (Shapiro et al. 1994, Flancbaum et al. 1995, Mariat el al. 2000), it has not gained wide popularity, partly because of the time-
22
consuming study design in a nuclear medicine laboratory, where the facilities are usually not intended for the treatment of severely ill patients.
2.2.3.5 Percutaneous aspiration of gallbladder
AAC is primarily a non-infectious disease, and bacterial invasion is regarded as a secondary event (Boland et al. 1993). In addition, many critically ill patients are on broad-spectrum antibiotics, which diminished the possibility of positive bacterial culture. That is why percutaneous aspiration of the gallbladder is of limited value and is not routinely recommended (Boland et al. 1993).
2.2.3.6 Histological findings in cholecystitis
The inflammatory reactions in the gallbladder wall in acalculous and calculous cholecystitis have been regarded histologically similar in both types of cholecystitis, including edema, mucosal ulceration, leukocytic infiltration, vascular congestion, abscess formation and gangrenous necrosis (Glenn 1979, Crawford 1999). In AAC, thrombosis and focal necrosis in blood vessels in the serosa and muscularis layers have also been shown to be characteristic features (Glenn & Becker 1982).
2.2.4 Treatment
The historical treatment of choice for AAC has been cholecystectomy, but during the last two decades percutaneous cholecystostomy has been suggested as an alternative to cholecystectomy (Melin et al. 1995, Davis et al. 1999, Spira et al. 2002). There are no randomized studies to compare percutaneous cholecystostomy and open or laparoscopic cholecystectomy in AAC patients. Medical treatment includes hemodynamic optimization with vasoactive drugs and antimicrobial treatment, in spite of the fact that only a small number of gallbladders in AAC have cultured positively (Barie & Eachempati 2003). The reported mortality rates of patients with AAC have been high (10-67 %) irrespective of the treatment, mostly due to the serious underlying diseases and the rapid progression to gangrene and perforation (Orlando et al. 1983, Johnson 1987, Shapiro et al. 1994, Rady et al. 1998).
2.2.4.1 Cholecystectomy
The incidence of gangrene in AAC has been high (27 - 78 %) in many studies where the gallbladder has been removed (DuPriest et al. 1979, Orlando et al. 1983, Shapiro et al. 1992, Kalliafas et al. 1998, Rady et al. 1998, Wang et al. 2003). This makes direct inspection of the gallbladder and cholecystectomy very reasonable treatment. In the same procedure, other intra-abdominal problems mimicking AAC can also be identified and managed (Barie & Eachempati 2003). Furthermore, the lack of correlation between
23
symptomatology and US findings and the incidence of necrosis and gangrene of the gallbladder has made many authors prefer cholecystectomy over cholecystostomy in the treatment of AAC (Orlando et al. 1983, Shapiro 1999, Wang et al. 2003). Laparoscopic cholecystectomy may cause less tissue damage than open cholecystectomy, but ventilatory, cardiovascular or hormonal side-effects may be severe in critically ill patients. There are, however, some reports on small patient series (2-10 patients) with good results even in critically ill patients (Brandt et al. 1994, Almeida et al. 1995, McClain et al. 1997).
2.2.4.2 Percutaneous cholecystostomy
Percutaneous cholecystostomy has gained popularity during the last decades. It is minimally invasive and can be accomplished under local anesthesia even on severely ill patients. The gallbladder is punctured under sonographic control via an anterior or anterolateral transhepatic or transperitoneal approach through the bed of the gallbladder, and a pigtail catheter is passed into the gallbladder over a guidewire. (Akhan et al. 2001). Rapid improvement should take place if the procedure is performed properly. Reported complications are catheter dislodgement, bile leakage causing peritonitis, hemorrhage, cardiac arrhythmia and hypotension from procedure-related bacteremia (van Sonnenberg et al. 1992, Akhan et al. 2001).
2.2.4.3 Transpapillary endoscopic cholecystostomy
In this technique, the cystic duct is located during endoscopic retrograde cholangiopancreatography (ERCP), and either a double pigtail biliary stent or a nasobiliary catheter is placed into the gallbladder. Technical success has been achieved in up to 90% of patients, but the technique has not been evaluated in ICU patients. Advantages include the decreased risk of bleeding, bile peritonitis and injury to adjacent organs. Disadvantages include the risk of pancreatitis and associated risks related to ERCP (Johlin & Neil 1994).
2.2.4.4 Antimicrobial therapy
Bile is normally sterile. In AAC, bacterial invasion is not regarded as the triggering etiologic factor, but rather a complication of an already diseased gallbladder (Raunest et al. 1992, Boland et al. 1993). Bacteria can enter the gallbladder hematogeneously or retrogradely from the duodenum. Retrograde bacterial colonization is more important (Subhani et al. 1999). In AAC, bile culture has been positive in 16 - 66 % of patients, and the commonly cultured bacteria have been E.coli, Klebsiella, Enterococcus, Enterobacter species, Staphylococcus, Pseudomonas, Clostridium and Bacteroides fragilis. Fungi and anaerobes are particularly likely in patients with diabetes and advanced age. (Howard
24
1981, Boland et al. 1994, Rady et al. 1998, Wang et al. 2003, Sosna et al. 2004) AAC has also been reported to develop during systemic infection of uncommon pathogens, such as salmonella, cholera, leptospirosis, dengue fever, brucellosis and malaria (McCarron & Love 1997, West et al. 1998, Vilaichone et al. 1999, Andriopoulos et al. 2003, Wu et al. 2003, Saha et al. 2005). Antibiotic treatment does not substitute for purification of the necrotic focus, but remains an important adjunct and should be targeted against the likely organisms covering at least gram-negative rods and enterococci (Barie & Eachempati 2003).
2.3 Tight junctions
The major physiological manifestations in multi-organ dysfunction and severe sepsis are increased vascular and intestinal permeability leading to a loss of cell barrier function and significant oedema formation. Tight junctions (TJ) are important apical intercellular contacts in epithelial and endothelial cell sheets, and they were first described in electron microscopy in 1963 (Farquhar & Palade 1963). Although increased vascular and epithelial permeability is a fundamental feature in the pathophysiology of severe multi-organ failure in critically ill patients, TJ proteins have, however, not yet been studied in critically ill patients. Detailed information of TJ molecular components and structure has only begun to accumulate during the past two decades. The normal function of many organs, such as the lungs, intestines, liver and kidneys depends on the barrier function of epithelial and endothelial cells.
2.3.1 General structure of the tight junctions
In columnar epithelial cells (e.g. those present in the gallbladder wall), TJs clearly subdivide the plasma membrane into apical and basolateral domains, which face the lumen and connective tissue. (Fig.1)
25
Fig. 1. Tight junctions and pathways across cellular sheets. Adopted and modified from Tsukita et al. 2001.
In endothelial cell sheets, TJs separate the membrane into apical and basolateral regions facing blood and the perivascular space, respectively. Tight junctions have two functions; the barrier function and the fence function. The barrier function means that they selectively open and close in response to various signals both inside and outside cells. This allows selective passage of ions, water and various macromolecules (inflammatory cells) and even cancer cells through paracellular spaces and is thus relevant to permeability disorders, such as edema formation and diarrhea (Madara 1998, Schneeberger & Lynch 2004). It also prevents both bacteria and toxins in the intestinal lumen from penetrating deeper into tissues through the paracellular pathway. The fence function maintains cell polarity by restricting the diffusion of lipids and proteins between the apical and basolateral plasma membranes (van Meer & Simons 1986). The adherens junction and desmosome are more basal components of the junctional complex than TJs, and they increase the mechanical strength of the cell-cell contact and maintain intercellular communication (Fig. 2).
26
Fig. 2. Junctional complex between cells. TJ, tight junction; AJ, adherens junction; D, desmosome. Adopted and modified from Tsukita et al. 2001.
The barrier function of epithelial TJs in skin and in the alimentary, respiratory and urinary tracts can vary, and there are “leaky” and “tight” tight junctions. The properties of endothelial TJs also vary in line with the need for permeability. In general, endothelial TJs are quite leaky, permitting a wide variety of substances to be exchanged between blood and organs. In brain, endothelial TJs are well developed, forming the blood-brain barrier (Bazzoni & Dejana 2003).
2.3.2 TJ proteins
Three distinct types of transmembrane proteins have been localized to TJs: occludin, claudins and junctional adhesion molecules (JAMs) (Fig. 2, 3). These proteins are linked to a series of peripheral proteins (including ZO-1, ZO-2, ZO-3) that anchor the integral membrane proteins to the cytoplasm and cytoskeleton by binding to the cytoplasmic tails of these proteins.
27
Fig. 3. Integral membrane proteins localized at tight junction. Adopted and modified from Tsukita et al. 2001.
2.3.2.1 Occludin
Occludin (65 kDa) (522 aminoacids) was the first transmembrane protein identified within tight junctions (Furuse et al. 1993). It has four transmembrane domains with two extracellular loops and a long carboxy-terminal and a short amino-terminal cytoplasmic domain. The extracellular loops are thought to interact in the paracellular space with loops from occludin from the adjacent cell to promote “sealing” of the paracellular space.
Occludin is expressed at high levels in brain endothelial cells and at much lower levels in endothelial cells of non-neural tissues (Hirase et al. 1997). Occludin also has a role in transepithelial migration of leukocytes (Huber et al. 2000). Despite the assumed central role of occludin in TJs in many studies, different results have also been presented; occludin-null mice showed no gross changes in TJ morphology and no alteration in intestinal epithelial barrier function (Saitou et al. 2000). The possibility that other junctional proteins (claudins) could compensate for the deficiency in the expression of occludin has been suggested as an explanation (Turksen & Troy 2004).
2.3.2.2 Claudins
The first members of the claudin family, claudin-1 and claudin-2, were identified from occludin-containing chicken liver junctional fractions in 1998, and so far altogether 24 members of this family have been identified (Furuse et al. 1998, Tsukita et al. 2001). The structural domains of claudins (20-24 kDa) (211 aminoacids) are similar to occludin with
28
four transmembrane domains, two extracellular loops and relatively short cytoplasmic carboxy- and aminoterminal domains. The first extracellular loop of claudins is larger than the second, and the amino acid compositions of the extracellular loops and the cytoplasmic domains vary significantly among the different claudins.
There is marked variation among tissues in the expression of each claudin (Rahner et al. 2001). The composition of different claudins in a tissue and their selective interactions with one another determine the barrier properties of a tissue (Furuse et al. 2001, Kiuchi-Saishin et al. 2002). Claudin-5 is predominantly expressed in endothelial cells (Morita et al. 1999), although it was recently demonstrated in epithelial cells of colonic origin and was suggested to function as a sealing tight junction protein to tighten the epithelial barrier properties (Amasheh et al. 2005).
2.3.2.3 JAMs
Junctional adhesion molecules (JAMs) (36-41 kDa) are also important components of tight junctions regulating permeability. JAM has a short cytoplasmic tail, a single transmembrane domain and a fairly long extracellular portion bearing two immunoglobulin-like loops (Martin-Padura et al. 1998). JAMs are found in epithelial and endothelial tight junctions, and four members of the JAM family have been identified so far.
2.3.2.4 ZO family
Many cytosolic proteins have been reported to associate with the cytoplasmic domains of the tight junction membrane proteins and to regulate the barrier function. ZO-1 was the first protein identified in 1986 (Stevenson et al. 1986), and ZO-2 and ZO-3 were identified a few years later (Jesaitis & Goodenough 1994, Haskins et al. 1998). ZO-1 is found especially in intestinal epithelia and in brain endothelia and arteries. In addition to binding with transmembrane proteins, ZO-1, ZO-2 and ZO-3 interact with each other and with several cytoplasmic signalling molecules and transcription factors (Fanning et al. 1998, Haskins et al. 1998, Balda & Matter 2000).
2.3.2.5 E-cadherin
E-cadherin is one of the transmembrane proteins at the adherens junction (AJ), and it functions as an adhesion molecule. It also interacts with the actin cytoskeleton to stabilize TJ and AJ (Tunggal et al. 2005).
29
2.3.3 Tight junctions and diseases
Increased tissue permeability is a common characteristic of, for instance, pulmonary edema, acute lung injury, pancreatitis, multi-organ dysfunction syndrome, inflammatory bowel disease and pseudomembranous colitis (Doig et al.1998, Dudek & Garcia 2001). Aberrant TJ expression and function are feasible explanations for the pathophysiology of these clinical manifestations (Kucharzik et al. 2001, Sawada et al. 2003, Lee et al. 2006).
One mechanism for action is that tight junctions can be direct or indirect targets of pathogens. Claudin-3 and -4 have been shown to be receptors for Clostridium perfringens enterotoxins and JAM a receptor for reovirus (Katahira et al. 1997, Fujita et al. 2000, Barton et al. 2001). After binding to receptors, these toxins cause TJ dysfunction. Bacteroides fragilis causes disruption of tight junctions by digesting E-cadherin (Wu et al. 1998). Enterobacteria can cause zonulin secretion from the small intestine, and zonulin is an endogenous modulator of intestinal tight junctions (Di Pierro et al. 2001).
Inflammatory mediators can regulate the expression of TJ proteins. Tumour necrosis factor alpha and interferon gamma downregulate the expression of occludin in human intestinal cell culture (Mankertz et al. 2000) and cause redistribution of JAM in endothelial cells (Ozaki et al. 1999). Endotoxemia has been shown to cause a marked decrease in the expression of occludin in the liver, lungs and intestine in mice (Han et al. 2004a, Han et al. 2004b, Han et al. 2004c).
The combined effect of trauma and severe infection on the expression of occludin and claudin-3 has been studied in rats (Samonte et al. 2004). Burn injury and Enterococcus fecalis infection together caused a significant increase in intestinal permeability and a decrease in the expression of intestinal occludin but not in the expression of claudin-3.
In human inflammatory bowel disease (IBD), diffuse global down-regulation of occludin has been found together with intense over-expression of claudin-2 along the inflamed colon epithelium (Prasad et al. 2005). Decreased claudin-1, -3 and -4, ZO-1, JAM and E-cadherin expressions have also been observed in epithelial cells immediately adjacent to transmigrating neutrophils in the diseased part of the colon (Kucharzik et al. 2001).
Human mutations of claudin-16, a specific claudin found in kidney epithelial cells, show abnormal paracellular passage of Mg2+ ions, resulting in excessive loss of Mg2+ in urine and in hypomagnesemia (Simon et al. 1999), and mutations in the claudin-14 gene result in an inability to maintain the special ionic environments in the cochlear duct, causing deafness (Wilcox et al. 2001).
Tight junctions are also considered to be deeply involved in tumorigenesis and metastasis. Altered expressions of claudin-1, -3 and -4 have been observed in human colorectal cancer (de Oliveira et al. 2005), while claudin-4 expression has been altered in pancreatic (Michl et al. 2001) and claudin-3 and claudin-4 in ovarian cancers (Hough et al. 2000).
3 Aims of the study
The aim of this study was to clarify the clinical and histological picture of surgically treated AAC and its association with multiple organ failure in critically ill patients. The following issues were of particular interest:
1. Incidence, admission diagnoses, diagnostic findings, associated organ system dysfunction and outcome of surgically treated AAC in mixed medical-surgical ICU patients (I, II).
2. Effect of cholecystectomy on organ system dysfunction in AAC patients (II). 3. Differences in gallbladder histology between AAC and ACC (III). 4. Expression of tight junction proteins in normal gallbladders and in the gallbladders of
patients with AAC and ACC (IV).
4 Patients and methods
This study consists of four different substudies, which have previously been reported in publications hereafter referred to as the studies I-IV. The studies I, III, IV were approved by The Ethics Committee of Oulu University Hospital and the use of the tissue specimens in the studies III and IV was approved by The National Authority for Medicolegal Affairs. No approval for study II from an ethical review committee was required because the data had already been collected for clinical purposes, and no additional interventions were done. The studies were conducted in the Intensive Care Unit, Department of Anesthesiology, Oulu University Hospital, and the studies III and IV in the collaboration with the Department of Pathology, University of Oulu.
4.1 Patients
In the studies I and II, the medical records of all ICU patients who had operatively treated AAC between 1 January 2000 and 31 December 2001 (I) and between 1 January 2003 and 31 December 2004 (II) were retrospectively examined. A total of 39 patients were included in study I and 24 patients in study II. All patients found to have AAC at laparotomy were included in study I regardless of other intra-abdominal pathology. Study II was conducted to find out the effect of cholecystectomy on organ dysfunctions in AAC patients, and all the patients who had additional intra-abdominal pathology, e.g. intestinal ischemia or perforation (10 patients), were excluded.
The indication for open cholecystectomy was a suspicion of AAC based on a pathologic ultrasound and/or CT finding together with clinical signs and symptoms of sepsis or deteriorating multiple organ dysfunction without other obvious foci. The decision to operate was made by the ICU team, which consisted of intensivists, a gi-surgeon and an infectious disease specialist. The patients were considered to have AAC if no gallstones were found, but necrosis and gangrene or distension and thickening of their gallbladder wall were seen at operation. During the same time periods, altogether 5 ICU patients (3 after cardiac surgery, 1 patient with pneumonia and 1 with sepsis) underwent cholecystectomy because of acute calculous cholecystitis 5 to 15 days after admission into ICU.
32
In study III, altogether 84 patients were included in three different study groups. The AAC group consisted of the same 39 AAC patients as study I. The ACC group consisted of 30 consecutively operated ACC patients admitted during the same time period as the 39 AAC patients. They were admitted into hospital because of primary acute gallbladder disease, were treated on a normal ward and did not have severe sepsis or multiple organ dysfunction. They had no signs of other intra-abdominal pathology than ACC at operation and no history of inflammatory bowel disease. The median (25th, 75th percentile) time from the onset of symptoms to the operation was 3 days (2, 5) and the median (25th, 75th percentile) time from the admission into hospital to the operation was 1 (1, 2) day. Their median (25th, 75th percentile) C-reactive protein value on the day of cholecystectomy was 173 mg/L (59, 212), and the median (25th, 75th percentile) white blood cell (WBC) count was 9.7 (8.2, 12.6) x 109/L. The control group consisted of 15 patients who had their macroscopically normal gallbladder removed during pancreatic tumour surgery. Five of the AAC samples, two of the ACC samples and one of the control samples could not be analyzed due to extensive autolysis of the samples, and the final numbers of samples were 76 samples, 34 in the AAC group, 28 in the ACC group and 14 in the control group.
In study IV, tight junction proteins were analyzed in 60 gallbladders. These gallbladders were selected from the 76 gallbladders in study III by a laboratory nurse blinded to any clinical data. This study included 30 samples of AAC patients, 21 samples of ACC patients and 9 samples of control patients.
4.2 Clinical data (I, II)
In the studies I and II, the following patient data were collected from the hospital records and the intensive care unit’s data management system (Deio-Ohmeda®, Helsinki, Finland in study I, Centricity Critical Care Clinisoft®, GE Healthcare, Helsinki, Finland in study II): age, sex, body mass index (BMI) (I), admission diagnosis, Acute Physiology and Chronic Health Evaluation (APACHE) II score, Simplified Acute Physiology Score (SAPS) II, appearance of the gallbladder at operation, length of ICU stay in days (calculated as hours divided by 24), parenteral/enteral nutrition, ICU and hospital outcome and cause of death.
In study I, the following data were also collected as “yes” or “no” responses on admission: presence of coronary heart disease, universal arteriosclerosis or diabetes mellitus and abuse of alcohol. Data on the use of opioids, corticosteroids, antibiotics, vasoactive and sedative drugs during the ICU stay before cholecystectomy were also collected from the data management system. The highest body temperature, the results of bilirubin and liver function tests, C-reactive protein and white blood cell count on the day of cholecystectomy were recorded as well. The results of blood (taken one to eight days before cholecystectomy) and bile cultures (taken prior to cholecystectomy via US-guided puncture or during cholecystectomy) as well as the findings of preoperative radiologic imaging (CT, US) were also recorded.
33
4.3 SOFA score (I, II)
The SOFA scores were collected from the intensive care unit’s data management system. In study I, the scores were collected for the first 24 hours in the ICU and for the 24 hours before cholecystectomy. In study II, the SOFA scores were collected on the admission day, three days before cholecystectomy, on the day of cholecystectomy and on the first, second, third and seventh postoperative days after cholecystectomy. The SOFA score is composed of scores for six organ system functions, graded from 0 (normal) to 4 (most severe dysfunction). These organ systems are: the respiratory, cardiovascular, renal, haematological, neurological and hepatic systems (Vincent et al. 1996, Vincent et al. 1998) (Table 1). Arterial blood gas analysis, platelet count and serum creatinine measurement were made at least once daily, and serum bilirubin was measured twice or three times a week at the physician’s discretion. The worst physiologic value for each day was recorded. If a value was missing (most frequently serum bilirubin), the previous value was used, and if that was not available, the next value was substituted. If both values were missing, the value was considered missing data and calculated as normal.
Table 1. Sequential Organ Failure Assessment (SOFA) score. Adopted and modified from Vincent et al. 1996.
Organ system 0 1 2 3 4 Respiration
PaO2/FiO2 (mmHg) (kPa)
> 400 >53.3
≤ 400 ≤ 53.3
≤ 300 ≤ 40
≤ 200a
≤ 26.7
≤ 100a
< 13.3 Coagulation
Platelets (x109/l)
>150
≤ 150
≤ 100
≤ 50
≤ 20 Liver
Bilirubin (μmol/l)
< 20
20-32
33-101
102-204
> 204 Cardiovascular
Hypotension
MAP ≥ 70 mmHg
MAP < 70
mmHg
Dopa ≤ 5 or
dobu (any dose)b
Dopa > 5 or epi ≤ 0.1 or
norepi ≤ 0.1 b
Dopa > 15 or epi > 0.1 or
norepi > 0.1b CNS
Glasgow Coma Score
15
13-14
10-12
6-9
< 6 Renal
Creatinine (μmol/L) urine output (ml/day)
< 110
110-170
171-299
300-440
< 500
> 440 < 200
a with respiratory support; b adrenergic agents administered at least for one hour (doses given are μg/kg/min); MAP, mean arterial pressure; dopa, dopamine; dobu, dobutamine; epi, epinephrine; norepi, norepinephrine; CNS, central nervous system
34
4.4 ICU treatment
Our ICU is a “closed unit”, and the treatment during the study period was managed by three to five full-time intensivists (anesthesiologists) in close co-operation with cardiac, neuro- and GI surgeons and specialists in infectious diseases, cardiology and radiology. All patients were treated according to the same general principles. Arterial blood gas analyses, lactate measurement and mixed venous oxygen saturation were used in addition to clinical assessment for routine tissue oxygenation monitoring. Pulmonary artery catheter was used to monitor the circulation whenever there was uncertainty of cardiac function or volume status and if vasoconstrictors or inotropes were used. Dobutamine was the first-line inotrope and noradrenaline the first-line vasoconstrictor. Levosimendan and milrinone were used as second-line inotropes.
Pressure control ventilation (Pplat < 30 H20) was used as the routine mode of mechanical ventilation, and continuous veno-venous hemodiafiltration was the primary method of renal replacement therapy.
Strict blood glucose control (< 8.0 mmol/l) with insulin infusion and intravenous hydrocortisone (200 -300 mg daily for 5 to 7 days) in septic shock not responding to adequate fluid replacement were used (Van den Berghe et al. 2001, Annane et al. 2002). Nutrition routines included initiation of enteral nutrition (1 kcal/ml) within 24-48 hours from admission at 10-20 ml /hour, followed by an increase in 3-4 days up to 1000-1500 ml per day. If the patient was intolerant of enteral nutrition, the rate was decreased and supplemental parenteral nutrition was provided. In the case of gastroparesis, a jejunal feeding tube was inserted endoscopically.
Propofol and midazolam were used for patient sedation and oxycodone and fentanyl for opioid analgesia.
The algorithm for the diagnosis and treatment of critically ill patients with suspected AAC or other intra-abdominal complications is presented in Figure 4.
35
Fig. 4. Algorithm for the diagnosis and treatment of AAC.
36
4.5 Blinding (III, IV)
Histological and immunohistochemical analyses were performed blindly without any clinical information, including patient category. All assessments were made by two investigators, JL and TK in study III and JL and either TK or YS in study IV.
4.6 Histological examination (III)
The gallbladder samples in study III had been taken for routine histopathological analysis during cholecystectomy. The samples were fixed in neutral buffered formalin and were embedded in paraffin. The sections were stained with haematoxylin and eosin.
The extent of changes in the surface epithelium was estimated, including the proportion (%) of surface area showing erosion (epithelial detachment) and the proportion of surface epithelium showing signs of degeneration or necrosis. The criteria for degeneration included cytoplasmic vacuolization or partial detachment. Necrotic epithelial cells were recognized based on either a pyknotic or karyorrhectic nucleus with or without deeply eosinophilic cytoplasm. Epithelial degenerative changes were separately estimated in the upper and lower halves of the mucosa.
The amounts of inflammatory cells, including neutrophilic and eosinophilic granulocytes, and mononuclear inflammatory cells (lymphocytes and plasma cells) were scored separately in the surface epithelium, lamina propria, subserosal fat and peritoneal surface. The latter included 20-50 μm of submesothelial connective tissue. Scoring was based on visual analogue scales. In each case, the score was determined according to the dominant pattern as ranging from absent (score 0) through slight (score 1) and moderate (score 2) to heavy increase (score 3) (see the original manuscript III).
The numbers of lymphatic follicles with germinal centres were counted and presented as counts/four high-power (40 x objective) fields (total area 3.2 mm2). The dilatation of lymphatic vessels was scored as being absent or present. The presence of leukocyte margination and thrombosis in blood vessels were also noted.
In some cases, eroded surface was covered by yellowish brown bile-like material, which occasionally infiltrated into the adjacent degenerated tissue. This type of mucosal bile penetration associated with destruction of mucosal surface was designated as bile infiltration, and the proportion (%) of surface with this change was estimated and recorded together with the maximum penetration into the gallbladder wall structures.
The proportion (%) of mucosal area showing Rokitansky-Aschoff sinuses (herniation of epithelium into lamina propria, smooth muscle or subserosal connective tissue) was estimated, and the presence of inflammatory cells in the sinus region was scored as absent (0) or mildly (1), moderately (2) or heavily (3) increased.
The presence of necrosis in the muscle layer and the proportion (%) of necrotic muscle area and depth were evaluated. The depth of necrosis was estimated by using the proportion of thickness showing necrotic change. The percentage of subserosal fat tissue showing necrosis was similarly estimated.
37
4.7 Immunohistochemical examination (IV)
In study IV, the gallbladder samples had been fixed in neutral buffered formalin and embedded in paraffin. The expression of the epithelial tight junction proteins claudin-1, -2, -3 and -4, occludin, ZO-1 and E-cadherin were studied by immunohistochemistry. The primary antibodies were purchased from Zymed Laboratories Inc. (South San Fransisco, CA, USA). The antibodies were used according to the manufacturer’s recommendations, and they consisted of polyclonal rabbit anti-claudin-1, monoclonal mouse anti-claudin-2, polyclonal rabbit anti-claudin-3, monoclonal mouse anti-claudin-4, polyclonal rabbit anti-occludin, polyclonal rabbit anti-ZO-1 and monoclonal mouse anti-E-cadherin. The sections were pretreated with TRIS/EDTA, except in the case of occludin, for which the sections were pretreated with pronase. The sections for ZO-1 immunohistochemistry were heated in a microwave oven for 15 minutes before the application of the primary antibodies. After incubation with the primary antibodies, a secondary antibody and the PowerVision+ Poly-HRP IHC kit (ImmunoVision Technologies, Brisbane, CA, USA) were applied. The colour was developed by diaminobenzidine using the DAKO EnVision Detection kit (DakoCytomation, Denmark). Negative control stainings were carried out by substituting non-immune rabbit or mouse serum and PBS for the primary antibodies. There were some individual specimens missing for technical reasons in each group, and the final amount of studied specimen was therefore 26-30/30 in the AAC group, 19-21/21 in the ACC group and 8-9/9 in the control group.
The results are presented as proportions (percentage) of epithelial cells expressing the studied antigens. Membrane-bound and cytoplasmic immunoreactivities were separately assessed. Staining intensity was categorized into four classes for analysis (0=absent, 1= weak, 2=moderate, 3=strong). Immunoreactivity in the vascular endothelial cells in the gallbladder wall was analyzed separately. Distinctive findings in the samples were recorded as well.
4.8 Statistical methods
The data are expressed as percentage, mean and standard deviation (SD), median and interquartile range (IQR, 25th, 75th percentiles) or as median with minimal and maximal values.
The statistical analyses were performed using the SPSS® for Windows software (versions 10.0-12.0.1, SPSS Inc., Chicago, IL). Categorical data were analyzed using X2
or Fisher’s exact test, as appropriate. Unpaired Student’s t-test was used to compare continuous data in study I. The assessment of changes within the total SOFA scores and within the individual organ system SOFA in study II was performed using Friedman’s test. If significant changes were found, comparisons within scores were performed using Wilcoxon’s test for paired comparisons. Kruskall-Wallis test was used to describe the histological and immunohistochemical differences between the AAC, ACC and control groups in study III and IV, while Mann-Whitney U-test was applied when comparing the parameters between the AAC and ACC groups. P < 0.05 was considered significant.
5 Results
5.1 Patients
Altogether 3984 (I) and 4200 (II) patients were treated in the ICU of Oulu University Hospital between 1.1.2000-31.12.2001 and 1.1.2003-31.12.2004, respectively. Forty percent of the patients were admitted after cardiac surgery, and the rest were general surgical, neurosurgical or medical patients. Seventy-three patients had operatively treated AAC during these time periods. There were 39 patients during 2000-2001 (study I) and 34 during 2003-2004 (study II). Ten of the patients in the years 2003-2004 had additional intestinal ischemia or perforation during the laparotomy. These ten patients were excluded, to recruit merely the AAC patients included in study II. Two-thirds of the studied AAC patients were men. The gallbladder was ischemic and gangrenous in 44 % and 54 % of the cases, respectively.
In study III, five of the AAC samples, two of the ACC samples and one of the control samples could not be analyzed due to extensive autolysis of the samples, and the final numbers of samples were 34 in the AAC group, 28 in the ACC group and 14 in the control group.
Patient characteristics are presented in Table 2. Less than half of the patients had ischemic heart disease (41%), universal arteriosclerosis (23%), alcohol abuse (20%) or diabetes (10%) as underlying chronic diseases (I). Preoperatively, more than half (56%) of the patients were on enteral feeding and, and 90 % of the patients received propofol and oxycodone infusions for sedation and pain relief. Fifty-four percent of the patients received steroid medication (54%) either for chronic disease or for sepsis (I).
39
Table 2. Patient characteristics in study groups I-IV, mean (SD) or median [IQR].
adm, admission; surg, surgery; LOS, length of stay. AAC patients in study IV are subgroup of AAC patients in study III. ACC patients in study IV are subgroup of ACC patients in study III.
5.2 Incidence of AAC (I, II)
A total of 73 patients out of 8184 had operatively treated AAC during the study periods 2000-2001 (39) and 2003-2004 (34), giving an incidence rate of 0.9 % (0.8 % and 1.0 %, p=0.481) and 6.7 %. among long-stayers (> 5 days) . The incidence of mere AAC without other intra-abdominal pathology in study II was 0.6%.
5.3 Admission diagnoses (I, II)
The most common admission diagnoses were sepsis (41-42%) followed by cardiovascular surgery (23-30%). The admission diagnoses are presented in Table 3.
Table 3. Admission diagnoses of patients with AAC in studies I and II, n (%).
The diagnostic findings are presented in table 4. The sensitivity of US was 80 and 72 % in the studies I and II. Two of the eleven patients with normal or undiagnostic US findings had necrosis in their gallbladder. Computed tomography had sensitivity of 58 and 50 % in the studies I and II. Five of the eight patients with normal or undiagnostic CT findings had necrosis in their gallbladder.
Table 4. Diagnostic findings of AAC patients in the studies I and II.
Study US CT Pain, tenderness Study I
positive/negative sensitivity
24/6 80%
7/5
58%
21/18 54%
Study II positive/negative sensitivity
13/5 72%
3/3
50%
10/14 42%
Fever was an uncommon symptom in AAC patients, half of the patients had normal WBC counts, and the median (25th, 75th percentiles) C-reactive protein value on the day of cholecystectomy was 169 mg/L (68, 245). In study II, the liver function tests on the day of cholecystectomy did not differ from the test results of all ICU patients during the study period 2003-2004 (Table5). Positive bile cultures were found in 12.8 and 12.5 % of the patients in the studies I and II.
Table 5. Median (25th, 75th percentile) values of liver function tests of AAC patients on the day of cholecystectomy (AAC(II)) and median (25th, 75th percentile) values of all liver function tests of all patients during years 2003-04.
Patients ALAT ASAT Bilirubin AFOS AAC (II) 43 (24, 68)
Ninety percent of the patients in study I had respiratory failure on the day of cholecystectomy. Cardiovascular (64%), renal (41%) and coagulation (36%) dysfunction were also common. There was significantly less cardiovascular dysfunction on the day of cholecystectomy than on admission, while renal dysfunction showed an opposite trend. Figure 5.
41
Fig. 5. Percentage of patients with associated organ failures on admission and on the day of cholecystectomy, study I.
5.5.1 Total SOFA scores
In study I, the median (IQR) total SOFA scores on admission and on the day of surgery were 11 (8-14) and 12 (8-14), respectively. In study II, the median (IQR) total SOFA score three days before cholecystectomy was 7.5 (1.3-8.0), and it significantly increased to 10.5 (8.3-13.0) by the day of cholecystectomy (see Figure 6). After the operation, the score decreased to 5.5 (3.3-10.8) by the seventh postoperative day.
42
Fig. 6. Median (IQR) total SOFA scores 3 (D-3), 2 days (D-2) and 1 day (D-1) before cholecystectomy, on the day of cholecystectomy (D0) and 1 (D+1), 2 (D+2), 3 (D+3) and 7 days (D+7) after cholecystectomy, study II.
5.5.2 Organ-specific SOFA scores
Cardiovascular and respiratory scores increased significantly from the third preoperative day to the day of surgery (II). After the operation, these organ system dysfunctions decreased. A significant increase was also seen in the renal and coagulation SOFA scores preoperatively. After the operation, renal dysfunction did not reach significant improvement until the 7th postoperative day. Coagulation disorder had a tendency to improve after the operation. Hepatic and neurologic dysfunctions did not show any remarkable changes before or after cholecystectomy. (Figure 7).
In study I, the median (IQR) values of the cardiovascular, respiratory and neurologic SOFA scores on the day of surgery were 3 (1-4), 3 (3-3) and 1 (0-2), respectively. The values for renal, hepatic and coagulation disorders were 2 (0-3), 1 (0-2) and 2 (0-3), respectively. The median values for cardiovascular, respiratory and neurological dysfunctions were the same, while the renal, hepatic and coagulation SOFA scores were higher than in study II.
0
4
8
12
16
20
24
P=0.004P<0.0001
D+7D+3D+2D+1D 0D-1D-2D-3
Tota
l Sof
a sc
ore
43
Fig. 7. Median (IQR) SOFA scores for individual organ systems 3 (D-3), 2 (D-2) and 1 day (D-1) before cholecystectomy, on the day of cholecystectomy (D0) and 1 (D+1), 2 (D+2), 3 (D+3) and 7 days (D+7) after cholecystectomy, study II.
0
1
2
3
4 P<0.0001P=0.001
D+7D+3D+2D+1D 0D-1D-2D-3
Card
iova
scul
ar S
OFA
sco
re
0
1
2
3
4P<0.0001P=0.001
D+7D+3D+2D+1D 0D-1D-2D-3
Resp
irato
ry S
OFA
sco
re
0
1
2
3
4 P=0.206P=0.015
D+7D+3D+2D+1D 0D-1D-2D-3
Rena
l SO
FA s
core
0
1
2
3
4
D+7D+3D+2D+1D 0D-1D-2D-3
P=N.S.
Hepa
tic S
OFA
sco
re
0
1
2
3
4
P=0.09P=0.01
D+7D+3D+2D+1D 0D-1D-2D-3
Coa
gula
tion
SOFA
sco
re
0
1
2
3
4
D+7D+3D+2D+1D 0D-1D-2D-3
P=N.S.
Neur
olog
ic S
OFA
sco
re
44
5.6 Mortality (I, II)
Nine out of 39 patients (23%, I) and three out of 24 (13%, II) patients died during their ICU stay after cholecystectomy. The hospital mortality rate was 43 % (I,II). Multiple organ failure (MOF) was the most common cause of death (65 % in study I, 80 % in study II). There was no statistically significant difference in age, gender, BMI, length of ICU stay or admission APACHE II, SAPS II and SOFA scores between the survivors and non-survivors (I). The non-survivors had, however, significantly higher SOFA scores on the day of surgery than the survivors (12.9 vs.9.5, P=0.007).
The median (IQR) survival of the non-survivors after cholecystectomy was 9 (2.5-17) days in study I. In study II, all deaths occurred later than during the first post-operative week, the median (IQR) being 33 days (12-50).
5.7 Histological findings (III)
5.7.1 Epithelial changes
There were significantly fewer degenerated epithelial cells in AAC than in ACC, and the extent of epithelial defect (erosion) was significantly less in AAC than in ACC (Table 6). Epithelial necrosis was present in 52.9 % (18/34) of the AAC and in 70.4 % (19/27) of the ACC samples (P=0.196) without any difference in the extent of necrosis. The control samples showed no epithelial degenerative changes or necrosis (Fig 8 A,B).
Table 6. Epithelial changes in the AAC, ACC and control groups. Both the occurrence (number of cases, % in parentheses) of cases showing an abnormality and the extent of this abnormality (median (min-max)) are indicated.
Epithelial change AAC ACC Controls P P AAC vs. ACC Degeneration,
Neutrophils were detectable less frequently in AAC than in ACC in all layers, with the exception of subserosal fat, where the difference did not reach statistical difference (Fig 8 C-F). Neutrophils were not present in any of the control samples. Mononuclear inflammatory cells were also less frequently found in AAC than in ACC in subserosal fat and the mesothelial surface, while eosinophilic granulocytes were seen significantly less only in subserosal fat. No significant differences between the AAC, ACC and control groups were seen in mononuclear and eosinophilic granulocytes in the gallbladder epithelium and lamina propria. (See Table 2 in the original paper III, page 490.)
5.7.3 Lymphatic follicles and vascular changes
There were no differences in the presence of capillary thromboses between the AAC and ACC groups. In contrast, leukocyte margination as well as lymphatic vessel dilatation were significantly more common in AAC compared to ACC (Fig 8 H). No capillary thrombosis, leucocyte margination or lymphatic dilatation was found in the control samples.
5.7.4 Bile infiltration and Rokitansky-Aschoff sinuses
Bile infiltration into the gallbladder mucosa was a significantly more common phenomenon in the AAC than in the ACC samples (50 % vs. 14 %, P=0.004), and the extent of mucosal surface covered with bile infiltration was also larger in AAC (7 % vs. 0.9 %, P=0.004) (Fig 8 E,F). Bile infiltration reached into the muscular layer in 35% of the samples in the AAC group, while in the ACC group bile infiltration was always restricted to the mucosal layer (P= 0.002). No bile infiltration was seen in the control samples. Rokitansky-Aschoff sinuses were found similarly in the AAC, ACC and control samples, and inflammatory cells in these sinuses were detected to the same extent in the AAC and ACC samples (12% and 15 %, respectively), while there were no inflammatory cells in the sinuses of the control samples.
5.7.5 Necrosis in the muscle layer and subserosal adipose tissue
The occurrence, extent and depth of smooth muscle necrosis were less marked in AAC than in ACC. Necrosis in adipose tissue seemed to be a more common phenomenon in ACC, but the difference did not reach statistical significance. No necrosis was seen in the control samples either in smooth muscle or in the adipose layer. (Table 7).
46
Table 7. Gallbladder wall necrosis in the AAC, ACC and control groups. Both the occurrence of necrosis (number of cases, % in parentheses) and the estimated extent (% of surface area) and depth (% of total thickness) of necrosis are indicated (median (min-max)).
Site of necrosis AAC ACC Controls P P AAC vs. ACC Muscle layer
Fig. 8. Photomicrographs showing the histology of normal gallbladder and that of AAC and ACC. A, B, Histologically normal gallbladder. C, D, ACC with purulent inflammation destroying the mucosa (arrowheads) and the muscle layer (arrows). E, F, AAC with brownish bile impregnation of the eroded mucosa (arrowheads) and muscle layer (arrows). G, Detail of the mucosal surface in AAC showing an epithelial defect with a few necrotic (arrowheads) or degenerate (arrows) epithelial cells. H, mucosa in AAC showing a dilated lymphatic vessel (L) and a venule (V) with margination of leucocytes.
48
5.8 Immunohistochemistry (IV)
We found both membrane-bound and cytoplasmic immunoreactivity for all studied TJ proteins in our gallbladder samples. The percentages of epithelial cells with positive staining in the different groups are presented in the Figures 9A, 9B, 10A and 10B, and the distribution of staining intensity in Table 8 and 9. In endothelial cells, marked immunoreactivity was detectable for ZO-1 and occludin.
5.8.1 Claudins
The immunoreactivity for the claudins -1, -3 and -4 was mainly membranous (Fig. 9A). Cytoplasmic staining was also detectable, and there was some granular staining in the apical regions of the cytoplasms, especially for the claudins -1, -2 and -3. The immunoreactivity for claudin-4 in epithelial cells seemed more heterogenous than that for the other claudins.
The membrane-bound staining for the claudins -1, -3 and -4 was present in practically all epithelial cells in the AAC and the control samples, but was less extensive in ACC (Fig. 9A). The cytoplasmic staining for claudin-1, -3 and -4 was clearly less extensive than membrane-bound staining in all groups (Fig. 9B). In ACC the intensity of cytoplasmic staining was weaker than in AAC for claudin-3 and -4 and weaker than in the control group for claudin-1 and -4.
The expression of claudin-2 differed from the other claudins; in the control and AAC groups, only about half of the cells showed membrane-bound or cytoplasmic staining, but a significantly greater part of cells stained positively in ACC (Fig. 8), and the intensity of staining was also stronger in ACC than in AAC or in the controls (Table 8).
49
Fig. 9. Median (IQR) percentages of cells staining positively for claudins. A membrane-bound staining, B cytoplasmic staining. CL 1 = claudin-1, CL 2 = claudin-2, CL 3 = claudin-3, CL 4 = claudin-4.
Table 8. Intensity of membranous and cytoplasmic staining of the claudins 1-4 (CL 1-4) assessed as the number of patients having each intensity score (0/1/2/3).
The extent of membrane-bound positivity for occludin was similar in the control and AAC groups but significantly diminished in the ACC group (Fig. 10A). The cytoplasmic positivity for occludin was significantly less extensive both in AAC and in ACC compared to the control group (Fig. 10B). There were no differences in the intensity of staining for occludin between the groups (Table 9).
ZO-1 expression was most evident in the apical regions of epithelial cells. The control group had an intensive membrane-bound immunoreaction for ZO-1, while positively stained cells were less abundant in AAC and especially in ACC (Fig. 10A). The intensity of the membrane-bound immunostaining of ZO-1 was stronger in AAC than in ACC. Cytoplasmic ZO-1 positivity was present in half of the cells in all groups, and there were no significant differences between the groups (Fig. 10B). Staining for E-cadherin was widespread both as membrane-bound and as cytoplasmic, and there were no remarkable differences between the groups.
51
Fig. 10. Median (IQR) percentages of cells staining positively for occludin, ZO-1 and E-cadherin. A membrane-bound staining, B cytoplasmic staining. OCCL = occludin, ECAD = E-cadherin.
0
10
20
30
40
50
60
70
80
90
100
P=0.015
P=0.001
P=0.001
ECADZO-1OCCL
Perc
enta
ge o
f pos
itive
cel
ls
Control AAC ACC
0
10
20
30
40
50
60
70
80
90
100
P=0.005
P=0.004
ECADZO-1OCCL
Perc
enta
ge o
f pos
itive
cel
ls
Control AAC ACC
B
A
52
Table 9. Intensity of membranous, cytoplasmic and endothelial staining of the occludin, ZO-1 and E-cadherin assessed as the number of patients having each intensity score (0/1/2/3).
Endothelial cells had extensive immunoreaction for ZO-1 in all groups, and the median (25th, 75th percentile) percentage of positive cells was 100 (95, 100) in the control group, 100 (100, 100) in AAC and 100 (90, 100) in ACC. The corresponding figures for occludin were 35 (30, 60) in the control group, 30 (20, 40) in AAC and 20 (10, 40) in ACC. The differences between the groups were not statistically significant.
6 Discussion
6.1 General discussion
The study population of 73 AAC patients was relatively small, but it is still one of the biggest series of AAC in ICU patients ever reported. A multi-centre study would have yielded a higher number of patients, but the single-centre approach allowed a more uniform treatment protocol.
The histopathological and immunohistological investigations were blinded by using normal gallbladders as controls. All slides were examined by at least two investigators, one of whom was an experienced pathologist.
It is not certain that we found and treated all AAC patients during this period. There might have been some patients with milder disease who recovered following conservative treatment. Systematic retrospective analysis of gallbladders of all patients who died during their ICU stay was not possible because the gallbladder was not routinely studied or stored at autopsy.
6.2 Incidence and concomitant factors of AAC
The incidence of AAC in our medical-surgical ICU patients was 0.9 %. This figure is in concordance with the earlier reports, where incidence rates have varied from 0.2 % to 4 % depending on the type of the ICU population (Savino et al. 1985, Kallifas et al. 1998, Rady et al. 1998 Mariat et al. 2000). However, the incidence among long-stayers was higher than has earlier been reported in cardiovascular surgery patients (6.7% vs. 3 %) (Rady et al. 1998). Infection was the most common admission diagnosis in our patients, and only one-third of the patients were postoperative or trauma patients. This shows that the occurrence of AAC is not limited to cardiovascular and postoperative patients, but is also possible in any critically ill patients, and that sepsis as such is an important predisposing factor.
Contrary to earlier reports, total parenteral nutrition, diabetes or alcohol abuse were not predominant concomitant factor in our patient series. The high proportion of patients
54
with mechanical ventilation probably reflected the severity of the underlying illness rather than the relationship of AAC with mechanical ventilation.
6.3 Diagnostic and treatment challenges
Only half of our patients presented with pain and tenderness in the right upper abdominal quadrant, and only 13 % of them had fever. None of the commonly used laboratory tests were good markers of AAC. In harmony with the earlier reports, US or CT were unable to reliably identify AAC (Fidler et al. 1996, Molenat et al.1996, Boland et al. 2000, Puc et al. 2002). Eleven out of 48 patients had no ultrasonographic findings of AAC, though the disease was diagnosed at surgery. Eight out of 18 examined patients did not have CT findings of AAC, and yet five of them had a necrotic gallbladder. However, US continues to be the basic diagnostic tool in AAC because it is non-invasive, inexpensive and portable, and follow-up scans are easy to obtain.
In practice, thorough clinical assessment, US findings (repeated if not diagnostic), arterial and mixed venous blood gas analysis, lactate measurement and trends in cardiovascular, respiratory, renal, hematologic, hepatic and central nervous system functions are the basic tools for the diagnosis of AAC.
Splanchnic hypoperfusion and ischemia probably have a pivotal role in the pathogenesis of AAC. In spite of the huge interest in splanchnic circulation during the past two decades, we still lack practical methods to monitor splanchnic perfusion or oxygenation. Gastric tonometry was developed to assess splanhnic perfusion by measuring gastric intramucosal pHi or the mucosal–arterial pCO2 gap, and it has been widely used in research and also clinically (Kuttila et al. 1994, Parviainen 1997, Juvonen et al. 1999). There are, however, problems in the interpretation of the findings, and the prognostic value of tonometry is not clear (Boldt 2002). In addition, enteral feeding, which is recommended to be started early in the case of critically ill patients, may disturb its reliability (Ala-Kokko & Laurila 1999).
If there is a suspicion of severe AAC with exacerbation of multiple organ dysfunction and rising SOFA scores without any other obvious focus with or without abdominal pain and distention, cholecystectomy should be considered. Before operation, if additional intra-abdominal or thoracic pathology is suspected, CT is the preferred radiologic imaging method instead of US.
There is currently some controversy as to the treatment of choice of AAC (Melin et al. 1995, Boggi et al. 1999, Shapiro 1999, McChesney et al. 2003). To date, there are no prospective controlled studies available to compare the conservative, percutaneous and surgical treatments of AAC. Percutaneous cholecystostomy has yielded good results in primary calculous disease, but the results have been poorer in ICU long-stayers with multiple organ dysfunction and SIRS (Melin et al. 1995, Hamy et al. 1997, Boggi et al. 1999, Davis et al. 1999, Spira et al. 2002, Sosna et al. 2004). Five of our patients initially underwent US-guided percutaneous cholecystostomy, but all of them later required operative treatment.
It is generally accepted that AAC complicated by gangrene or perforation is a definite indication for cholecystectomy and cannot be treated by percutaneous drainage. In our
55
series, gangrene and ischemic lesions of the gallbladder were present in half of the patients. Similar results have been reported earlier, with gangrene and necrosis of the gallbladder in 59 % and 63 % of critically ill AAC patients (Shapiro et al. 1994, Kalliafas et al. 1998). Because of the high incidence of gangrenous gallbladder and a lack of correlation between symptomatology and gangrene, we strongly agree with the opinion that cholecystectomy is the definitive treatment of severe AAC (Shapiro 1999). In our series, surgery was well tolerated, and no mortality was associated with cholecystectomy.
6.4 Multiple organ failure and outcome
Multiple organ dysfunction syndrome refers to the progressive impairment of two or more organ systems as a response to a severe illness or injury, and it is the most important factor contributing to mortality and prolongation of intensive care (Beal & Cerra 1994, Moreno et al. 1999). The sequential organ failure assessment score (SOFA) was developed to describe objectively the severity of multiorgan dysfunction (Vincent et al. 1996, Vincent et al. 1998). Individual organ functions (respiratory, cardiovascular, renal, coagulation, hepatic and neurological) are graded from normal (grade 0) through mild dysfunction to severe organ failure (grade 4). The higher the SOFA score, the more severe the organ dysfunction (Moreno et al. 1999). Although the SOFA score was not developed to predict hospital mortality, the ability of the daily maximum SOFA score and the total maximum SOFA score to distinguish between survivors and non-survivors is relatively good, i.e. comparable to APACHE III (Pettilä et al. 2002).
Multiple organ failure was common among the present AAC patients. The patients were severely ill on admission into ICU, the mean (SD) APACHE II being 25.5 (6.4) and the mean (SD) total SOFA score 10.2 (3.5). At this stage, 90 % of the patients had respiratory and 79 % cardiovascular dysfunction, and coagulation dysfunction was also quite common. Multiple organ dysfunction continued to progress during the ICU treatment before cholecystectomy. The mean total, cardiovascular, respiratory, renal and coagulation SOFA scores increased as a marker of multiple organ failure. On the day of cholecystectomy, most patients had three or more organ failures.
The choice of the surgical approach as treatment of AAC is supported by our finding that removal of the diseased gallbladder was followed by remarkable improvement in individual and total SOFA scores by the seventh postoperative day. The cardiovascular and respiratory functions were the most sensitive organ functions to be disturbed and also the first functions to improve. Renal dysfunction both developed and improved more slowly than the cardiovascular or respiratory functions. Coagulation disorder also increased and decreased before and after cholecystectomy, respectively, while the hepatic and neurologic organ systems did not show any significant change.
The hospital mortality of AAC patients was high (43%), which reflects high severity of the underlying illnesses. Our mortality was quite similar to that reported by Kalliafas et al. (1998), but our patients were more severely ill according to the APACHE II scores (25 vs. 17).
56
6.5 Histological findings
Although AAC and ACC have previously been considered similar diseases with or without stones (Glenn 1979, Myers et al. 1988, Jessurun & Albores-Saavedra 2002), we found differences in the histologic characteristics of these two types of cholecystitis.
Leucocyte margination of blood vessels and lymphatic dilatation were significantly more common in AAC than in ACC, which suggests involvement of ischemia- and reperfusion-mediated injury (Savoca et al. 1990a, Taoka 1991). However, we could not confirm the earlier observations that capillary thromboses are typical of AAC (Warren 1992, Hakala et al. 1997). Interestingly, a possible sign of increased interstitial oedema, i.e. the presence of focal lymphatic dilatation, was clearly associated with AAC in our series. Collectively, these findings suggest that circulatory disturbances could play a role in the pathogenesis of AAC.
Bile infiltration into the gallbladder mucosa was significantly more abundant and extended deeper in AAC than in ACC. Epithelial defects in the gallbladder mucosa were more extensive in ACC, indicating that factors other than epithelial ulceration explain the development of bile infiltration in AAC. Increased epithelial permeability might explain this finding.
Mucosal infiltration of mononuclear inflammatory cells was similar in AAC, ACC and control gallbladders, suggesting that some mucosal infiltration of chronic inflammatory cells can be considered physiological. However, the presence of mucosal neutrophils and inflammation in the deeper parts of the gallbladder mucosa clearly showed differences between cholecystitis patients and controls and, more importantly, between AAC and ACC. Extensive epithelial degeneration and detachment were accompanied by an intensive mucosal neutrophil reaction in ACC and, to a significantly lesser extent, in AAC. Similarly, in the muscle layer, necrosis up to half of its thickness was seen in the cases with ACC, while muscle necrosis in AAC was rare and less extensive. Our study suggests that, although necrosis is present in both types of cholecystitis, it is less severe in AAC. A similar difference was apparent in subserosal adipose tissue and the peritoneal surface, where an acute inflammatory reaction was predominantly present in ACC and, to a lesser extent, in AAC. All these differences in the patterns of inflammation and necrosis further suggest that AAC and ACC are pathogenetically different. These results suggest that AAC is a manifestation of systemic critical illness, whereas ACC is typically a local, predominantly purulent and necrotic inflammatory disease of the gallbladder.
6.6 Tight junction proteins in AAC and ACC
The expression of tight junctions has not been previously investigated in critically ill patients or in normal gallbladders. In the present study, TJ proteins were widely expressed in the membrane of the epithelial cells of normal gallbladders, with the exception of claudin-2, which was detectable only in half of the cells. Cytoplasmic expression of all studied TJ proteins was lower than membranous expression.
There were qualitative and quantitative differences in TJ protein stainings between the AAC, ACC and normal gallbladders. In AAC, significant down-expression of
57
cytoplasmic occludin and claudin-1 was seen in the gallbladder epithelium. Earlier, it has been shown that proinflammatory cytokines, tumor necrosis factor alpha and interferon gamma down-regulated the expression of occludin in human intestinal cell culture, and that endotoxemia caused a marked decrease in the expression of occludin in intestine, liver and lung in mice (Mankertz et al. 2000, Han et al. 2004a-c). In an animal study, two-hit injury of burn and infection has been shown to decrease the expression of intestinal occludin concomitantly with an increase in intestinal permeability (Samonte et al. 2004).
ACC was characterised by more extensive down-regulation of the claudin-1, -3, -4, occludin and ZO-1 proteins and up-regulation of claudin-2. Similar results have been reported for intense local purulent inflammation in IBD and colitis ulcerosa, and claudin-2 up-regulation seems to be a typical response in inflammatory reactions involving neutrophilic leucocytes (Kucharzik et al. 2001, Prasad et al. 2005). In comparison with AAC, the more intensive and partly divergent reaction in ACC could be caused by high concentrations of local proinflammatory factors and local microbial invasion, which contrast with the presumably lower concentrations of systemic proinflammatory mediators with vascular entry into the gallbladder mucosa in AAC. Additionally, hypoxic conditions in AAC might further modify the gallbladder response.
7 Conclusions
1. The incidence of surgically treated AAC was 0.9% in the whole ICU patient series and 6.7 % among the long-stayers (>5 days). Infection was the most common admission diagnosis, followed by cardiovascular surgery. The sensitivity of US in diagnosing AAC was 80 and 72 % in the studies I and II, and that of CT was remarkably poorer, being 58% and 50 %, respectively. Liver function tests, WBC count and C-reactive protein were not reliable tests in diagnosing AAC. AAC was associated with multiple organ dysfunction. Sixty-four percent of the patients had three or more failing organs on the day of cholecystectomy. The hospital mortality of these patients was 43 %.
2. Open cholecystectomy improved the deteriorating multiple organ dysfunction. The change was most obvious in the cardiovascular and respiratory functions.
3. AAC and ACC were histopathologically different. Typical features in AAC were bile infiltration, lymphatic dilatation and leucocyte margination of blood vessels, while epithelial degeneration and defects, widespread occurrence of inflammatory cells and extensive and deep muscle layer necrosis were typical features in calculous cholecystitis.
4. Tight junction proteins (claudin -1, -2, -3, -4, occludin, ZO-1, E-cadherin) were widely expressed in normal and diseased gallbladder. There were remarkable qualitative and quantitative differences in the expression of these TJ proteins in AAC and ACC.
References
Akhan O, Akinci D & Özmen MN (2001) Percutaneous cholecystectomy. Eur J Radiol 43:229-236. Ala-Kokko TI & Laurila J (1999) Continuous gastric mucosal capnometry is affected by enteral
nutrition. Potential for misinterpretation of tissue oxygenation. Chest 115:1482-1483. Almeida J, Sleeman D, Sosa JL, Puente I, McKenney M & Martin L (1995) Acalculous
cholecystitis:the use of diagnostic laparoscopy. J Laparoendosc Surg 5:227-231. Amasheh S, Schmidt T, Mahn M, Florian P, Mankertz J, Tavalali S, Gitter AH, Schulzke JD &
Fromm M (2005) Contribution of claudin-5 to barrier properties in tight junctions of epithelial cells. Cell Tissue Res 321:89-96.
Andriopoulos P, Tsironi M & Asimakopoulos G (2003) Acute abdomen due to brucella melitensis. Scand J Inf Dis 35:204-205.
Annane D, Belissant E & Cavaillon JM (2005) Septic shock. Lancet 365:63-78. Annane D, Sebille V, Charpentier C, Bollaert PE, Francois B, Korach JM, Capellier G, Cohen Y,
Azoulay E, Troche G, Chaumet-Riffaut P & Belissant E (2002) Effect of treatment with low doses of hydrocortisone and fludrocortisone on mortality in patients with septic shock. JAMA 288:862-871.
Balda MS & Matter K (2000) The tight junction protein ZO-1 and an interacting transcription factor regulate ErB-2 expression. EMBO J 19:2024-2033.
Barie PS & Eachempati SR (2003) Acute acalculous cholecystitis. Curr Gastroent Rep 5:302-309. Barnes SL, Clark DM & Schwartz RW (2004) Biliary dyskinesia: A brief review. Curr Surg
61:428-434. Barton ES, Forrest JC, Connolly JL, Chappell JD, Liu Y, Schnell FJ, Nusrat A, Parkos CA &
Dermody TS (2001) Junction adhesion molecule is a receptor for reovirus. Cell 104:441-451. Bazzoni G & Dejana E (2003) Endothelial cell-to-cell junctions: Molecular organization and role in
vascular homeostasis. Physiol Rev 84: 869-901. Beal AL & Cerra FB (1994) Multiple organ failure syndrome in the 1990s: Systemic inflammatory
response and organ dysfunction. JAMA 271:226-233. Becker CG, Dubin T & Glenn F (1980) Induction of acute cholecystitis by activation of factor XII.
J Exp Med 151:81-90. Bennett GL, Rusinek H, Lisi V, Israel GM, Krinsky GA, Slywotzky CH & Megibow A (2002) CT
findings in acute gangrenous cholecystitis. Am J Roentgenol 178:275-281. Boggi U, Di Candio G, Campatelli A, Oleggini M, Pietrabissa A, Filipponi F, Bellini R, Mazzotta
D & Mosca F (1999) Percutaneous cholecystectomy for acute cholecystitis in critically patients. Hepato-Gastroenterol 46:121-125.
60
Boland G, Lee MJ & Mueller PR (1993) Acute acalculous cholecystitis in the intensive care unit. New Horizons 1:246-260.
Boland G, Slater G, Lu DSK, Eisenberg P, Lee MJ & Mueller PR (2000) Prevalence and significance of gallbladder abnormalities seen on sonography in intensive care unit patients. Am J Roentgenol 174:973-977.
Boldt J (2002) Hemodynamic monitoring in intensive care unit. Crit Care 6:52-59. Bone RC, Balk RA, Cerra FB, Dellinger RP, Fein AM, Knaus WA, Shein RM & Sibbald WJ
(1992) Definition for sepsis and organ failure and guidelines for use of innovative therapies in sepsis. The ACCP/SCCM Consensus Conference Committee. American College of Chest Physicians/Society of Critical Care Medicine. Chest 101:1644-1655.
Brandt CP, Priebe PP & Jacobs DG (1994) Value of laparoscopy in trauma ICU patients with suspected acute acalculous cholecystitis. Surg Endosc 8:361-364.
Crawford JM (1999) The liver and the biliary tract. In Cotran RS, Kumar V, Collins T (eds) Robbins pathologic basis of disease. WB Sounders Company, Philadelphia, 895-897.
Cullen JJ, Maes EB, Aggrawal S, Conklin JL, Ephgrave KS & Mitros FA (2000) Effect of endotoxin on opossum gallbladder motility: A model of acalculous cholecystitis. Ann Surg 232:202-207.
Dahn MS, Lange P, Lobdell K, Hans B, Jacobs LA & Mitchell RA (1987) Splanchnic and total body oxygen consumption differences in septic and injured patients. Surgery 101:69-80.
Davis CA, Landercasper J, Gundersen LH & Lambert PJ (1999) Effective use of percutaneous cholecystectomy in high-risk surgical patients: techniques, tube management, and results. Arch Surg 134:727-732.
De Backer D, Creuter J, Silva E & Vincent JL (2003) Effects of dopamine, norepinephrine, and epinephrine on splanchnic circulation is septic shock: Which is best ? Crit Care Med 31:1659-1667.
de Oliveira SS, de Oliveira IM, de Souza W & Morgado-Diaz JA (2005) Claudins upregulation in human colorectal cancer. FEBS Letters 579:6179-6185.
Di Pierro M, Lu R, Uzzau S, Wang W, Margaretten K, Pazzani C, Maimone F & Fasano A ( (2001) Zonula occludens toxin structure-function analysis. Identification of the fragment biologically active on tight junctions and of the zonulin receptor binding domain. J Biol Chem 276:19160-19165.
Doig CJ, Sutherland LR, Sandham JD, Fick GH, Verhoef M & Meddings JB (1998) Increased intestinal permeability is associated with the development of multiple organ dysfunction syndrome in critically ill patients. Am J Respir Crit Care Med 158:444-451.
Draghi F, Ferrozzi G, Calliada F, Solcia M, Madonia L & Campani R (2000) Power Doppler ultrasound of gallbladder wall vascularization in inflammation: clinical implications. Eur Radiol 10:1587-1590.
Dudek SM & Garcia JGN (2001) Cytoskeletal regulation of pulmonary vascular permeability. J Appl Physiol 91:1487-1500.
Duncan J (1844) Femoral hernia; gangrene of the gallbladder; extravasation of bile; peritonitis; death. North J Med: 151-153.
DuPriest RW, Khaneja SC & Cowley RA (1979) Acute cholecystitis complicating trauma. Ann Surg 189:84-89.
Fanning AS, Jameson BJ, Jesaitis LA & Anderson JM (1998) The tight junction protein ZO-1 establishes a link between the transmembrane protein occludin and actin cytoskeleton. J Biol Chem 273:29745-29753.
Farquhar MG & Palade GE (1963) Junctional complexes in various epithelia. J Cell Biol 17:375-412.
Fidler J, Paulson EK & Layfield L (1996) CT evaluation of acute cholecystitis: Findings and usefulness in diagnosis. Am J Roentgenol 166:1085-1088.
61
Fink MP & Delude RL (2005) Epithelial barrier dysfunction: a unifying theme to explain the pathogenesis of multiple organ dysfunction at the cellular level. Crit Care Clin 21:177-196.
Flancbaum L & Choban PS (1995) Use of morphine cholescintigraphy in the diagnosis of acute cholecystitis in critically ill patients. Intensive Care Med 21:120-124.
Flancbaum L, Majerus TC & Cox EF (1985) Acute posttraumatic acalculous cholecystitis. Am J Surg 150:252-256.
Frierson HF Jr (1992) Gallbladder and the extrahepatic biliary system. In: Sternberg SS (ed) Histology for pathologists. Raven Press, New York, 639-655.
Fujita K, Katahira J, Horiguchi Y, Sonoda N, Furuse M & Tsukita S (2000) Clostridium perfringens enterotoxin binds to the second extracellular loop of claudin-3, a tight junction integral membrane protein. FEBS Lett 476:258-261.
Furuse M, Fujita K, Hiiragi T, Fujimoto K & Tsukita S (1998) Claudin-1 and -2: novel integral membrane proteins localizing at tight junctions with no sequence similarity to occludin. J Cell Biol 141: 1539-1550.
Furuse M, Furuse K, Sasaki H & Tsukita S (2001) Conversion of zonula occludentes from tight to leaky strand typeby introducing claudin-2 into Madin-Dardy canine kidney I cells. J Cell Biol 153: 263-272.
Furuse M, Hirase T, Itoh M, Nagafuchi A, Yonemura S, Tsukita S & Tsukita S (1993) Ocludin: a novel integral membrane protein localizing at tight junctions. J Cell Biol 123:1777-1788.
Glenn F (1947) Acute cholecystitis following the surgical treatment of unrelated disease. Ann Surg 126:411-420.
Glenn F (1979) Acute acalculous cholecystitis. Ann Surg 189:458-465. Glenn F & Becker CG (1982) Acute acalculous cholecystitis. Ann Surg 195:131-136. Gomez-Pinilla PJ, Morales S, Camello-Almaraz C, Moreno R, Pozo MJ & Camello PJ (2005)
Changes in guinea pig gallbladder smooth muscle Ca 2+ homeostasis by acute acalculous cholecystitis. Am J Physiol Gastrointest Liver Physiol 290:G14-G22.
Hagino RT, Valentine RJ & Clagett GP (1997) Acalculous cholecystitis after aortic reconstruction. J Am Coll Surg 184:245-248.
Hakala T, Nuutinen PJO, Ruokonen ET & Alhava E (1997) Microangiopathy in acute acalculous cholecystitis. Br J Surg 84:1249-1252.
Hamy A, Visset J, Likholatnikov D, Lerat F, Gibaud H, Savigny B & Paineau J (1997) Percutaneous cholecystectomy for acute cholecystitis in critically ill patients. Surgery 121:398-401.
Han X, Fink MP, Uchiyama T, Yang R & Delude RL (2004a) Increased iNOS activity is essential for hepatic epithelial tight junction dysfunction in endotoxemic mice. Am J Physiol Gastrointest Liver Physiol 284:G126-136.
Han X, Fink MP, Uchiyama T, Yang R & Delude RL (2004b) Increased iNOS activity is essential for pulmonary epithelial tight junction dysfunction in endotoxemic mice. Am J Physiol Lung Cell Mol Physiol 286:L259-267.
Han X, Fink MP, Yang R & Delude RL (2004 c) Increased iNOS activity is essential for intestinal epithelial tight junction dysfunction in endotoxemic mice. Shock 21:261-270.
Harvey RT & Miller WT Jr (1999) Acute biliary disease: initial CT and follow-up US versus initial US and follow-up CT. Radiology 213:831-836.
Haskins J, Gu L, Wittchen ES, Hibbard J & Stevenson BR (1998) ZO-3, a novel member of the MAGUK protein family found at the tight junction, interacts with ZO-1 and occludin. J Cell Biol 141:199-208.
Hassoun HT, Kone BC, Mercer DW, Moody FG, Weisbrodt NW & Moore FA (2001) Post-injury multiple organ failure: the role of the gut. Shock 15:1-10
62
Hirase T, Staddon JM, Saitou M, Anod-Akatsuka Y, Itoh M, Furuse M, Fujimoto K, Tsukita S & Rubin LL (1997) Ocludin as a possible determinant of tight junction permeability in endothelial cells. J Cell Sci 110:1603-1613.
Hotchkiss RS & Karl IE (2003) The pathophysiology and treatment of sepsis. N Engl J Med 348:138-150.
Hough CD, Sherman-Baust CA, Pizer ES, Montz FJ, Im DD, Rosenshein NB, Cho KR, Riggens GJ & Morin PJ (2000) Large-scale serial analysis of gene expression reveals genes differentially expressedin ovarian cancer. Cancer Recearch 60:6281-6287.
Howard RJ (1981) Acute acalculous cholecystitis. Am J Surg 141:194-198. Howard JM, Milford MT & DeBakey ME (1952) The significance of the sympathetic nervous
system in acute cholecystitis. Surgery 32:251-258. Huber D, Balda MS & Matter K (2000) Occludin modulates transepithelial migration of
neutrophils. J Biol Chem 275: 5773-5778. Imamoglu M, Sarihan H, Sari A & Ahmetoglu A (2002) Acute acalculous cholecystitis in children:
diagnosis and treatment. J Pediatr Surg 37:36-39. Inoue T & Mishima Y (1988) Postoperative acute cholecystitis: a collective review of 494 cases in
Japan. Jpn J Surg 18:35-42. Jeffrey Jr RB, Nino-Murcia M, Ralls PW, Jain KA & Davidson HC (1995) Color Doppler
sonography of the cystic artery: comparison of normal controls and patients with acute cholecystitis. J Ultrasound Med 14:33-36.
Jesaitis LA & Goodenough DA (1994) Molecular characterization and tissue distribution of ZO-2, a tight junction protein homologous to ZO-1 and the Drosophiladisc-large tumor suppressor protein. J Cell Biol 124:949-961.
Jessurun J & Albores-Saavedra J (2001) Diseases of the gallbladder. In: MacSween RNM, Burt AD, Portman BC, Scheuer PJ, Anthony PP (eds) Pathology of the liver, 4th edition. Churchill Livingstone, London, 507-538.
Joehl RJ, Koch KL & Nahrwold DL (1984) Opioid drugs cause bile duct obstruction during hepatobiliary scans. Am J Surg 147:134-138.
Johanning JM & Gruenberg JC (1998) The changing face of cholecystectomy. Am Surg 64: 643-648.
Johlin FC Jr & Neil GA (1994) Drainage of the gallbladder in patients with acute acalculous cholecystitis by transpapillary andoscopic cholecystotomy. Gastrointest Endosc 39:645-651.
Johnson LB (1987) The importance of early diagnosis of acute acalculous cholecystitis. Surg Gynecol Obstet 164:197-203.
Johnson EE & Hedley-Whyte J (1975) Continuous positive pressure ventilation and choledochoduodenal flow resistance. J Appl Physiol 39:937-942.
Juvonen PO, Tenhunen JJ, Heino AA, Merasto M, Paajanen HEK, Alhava EM & Takala J (1999) Splanchnic tissue perfusion in acute experimental pancreatitis. Scand J Gastroenterol 34:308-314.
Kalliafas S, Ziegler DW, Flancbaum L & Choban PS (1998) Acute acalculous cholecystitis: incidence, risk factors, diagnosis, and outcome. Am Surg 64: 471-475.
Kamimura T, Mimori A, Takeda A, Masuyama J, Yoshio T, Okazaki H, Kano S & Minota S (1998) Acute acalculous cholecystitis in systemic lupus erythematosus: a case report and review of literature. Lupus 7:361-363.
Kaminski DL, Amir G, Deshpande YG, Beck D & Li AP (1994) Studies on the etiology of acute acalculous cholecystitis: The effect of lipopolysaccharide on human gallbladder mucosal cells. Prostaglandins 47:319-330.
Kaminski DL, Andrus CH, German D & Deshpande YG (1990) The role of prostanoids in the production of acute acalculous cholecystitis by platelet-activating factor. Ann Surg 212:455-461.
63
Katahira J, Sugiyama H, Inoue H, Horiguchi Y, Matsuda M & Sugimoto N (1997) Clostridium perfringens enterotoxin utilizes two structurally related membrane proteins as functional receptors in vivo. J Biol Chem 272:26652-26658.
Kiuchi-Saishin Y, Gotoh S, Furuse M, Takasuga A, Tano Y & Tsukita S (2002) Differential expression patterns of claudins, tight junction membrane proteins, in mouse nephron segments. J Am Soc Nephrol 13: 875-886.
Ko CW, Sekijima JH & Lee PS (1999) Biliary sludge. Ann Intern Med 130:301-311. Kucharzik T, Walsh SV, Chen J, Parkos CA & Nusrat A (2001) Neutrophil transmigration in
inflammatory bowel disease is associated with differential expression of epithelial intercellular junction proteins. Am J Pathol 159:2001-2009.
Kuttila K, Perttilä J, Vänttinen E & Niinikoski J (1994) Tonometric assessment of sigmoid perfusion during aortobifemoral reconstruction for arteriosclerosis. Eur J Surg 160:491-495.
Lee SP (1990) Pathogenesis of biliary sludge. Hepatology 12:200S-203S. Lee RD, Choe E, Flint L & Steinberg S (1998) Neither dopamine nor dobutamine corrects
mesenteric blood flow depression caused by positive end-expiratory pressure an a rat model of acute lung injury. Crit Care Med 26:1875-1880.
Lee DBN, Huang E & Ward HJ (2006) Tight junction biology and kidney dysfunction. Am J Physiol Renal Physiol 290:F20-F34.
Lee SP, Nicholls JF & Park HZ (1992) Biliary sludge as a cause of acute pancreatitis. N Engl J Med 326:589-593.
Levy MM, Fink MP, Marshall JC, Abraham E, Angus D, Cook D, Cohen J, Opal SM, Vincent JL & Ramsay G (2003) International sepsis definitions conference. Intensive Care Med 29:530-538.
Lindberg E, Grinnan G & Smith L (1970) Acalculous cholecystitis in Viet Nam casualties. Ann Surg 171: 152-157.
Long TN, Heimbach DM & Carrico CJ (1978) Acalculous cholecystitis in critically ill patients. Am J Surg 136:31-36.
Madara JL (1998) Regulation of the movement of solutes across tight junctions. Annu Rev Physiol 60:143-159.
Mankertz J, Tavalali S, Schmitz H, Mankertz A, Riecken EO, Fromm M & Schulzke JD (2000) Expression from the human occludin promoter is affected by tumor necrosis factor α and interferon γ. J Cell Sci 113:2085-2090.
Mariat G, Mahul P, Prevot N, De Filippis JP, Cuilleron M, Dubois F & Auboyer C (2000) Contribution of ultrasonography and cholescintigraphy to the diagnosis of acute acalculous cholecystitis in intensive care unit patients. Intensive Care Med 26:1658-1663.
Martikainen TJ, Tenhunen JJ, Uusaro A & Ruokonen E (2003) The effects of vasopressin on systemic and splanchnic hemodynamics and metabolism in endotoxin shock. Anesth Analg 97:1756-1763.
Martin-Padura I, Lostaglio S, Schneemann M, Williams L, Romano M, Fruscella P, Panzeri C, Stoppacciaro A, Ruco L, Villa A, Simmons D & Dejana E (1998) Junctional adhesion molecule, a novel member of the immunoglobulin superfamily that distributesat intercellular junctions and modulates monocyte transmigration. J Cell Biol 142:117-127.
McCarron B & Love WC (1997) Acalculous nontyphoidal salmonellal cholecystitis requiring surgical intervention despite ciprofloxacin therapy: report of three cases. Clin Infect Dis 24:707-709.
McChesney JA, Northup PG & Bickston SJ (2003) Acute acalculous cholecystitis associated with systemic sepsis and visceral arterial hypoperfusion: a case series and review of pathophysiology. Dig Dis Sci 48:1960-1967.
McClain T, Gilmore BT & Peetz M (1997) Laparoscopic cholecystectomy in the treatment of acalculous cholecystitis in patients after thermal injury. J Burn Care Rehabil 18:141-146.
64
McConnell KW & Coopersmith CM (2005) Epithelial cells. Crit Care Med 33:S520-S522. McDermott MW, Scudamore CH, Boileau LO, Snelling CF & Kramer TA (1985) Acalculous
cholecystitis: its role as a complication of major burn injury. Can J Surg 28:529-533. Melin MM, Sarr MG, Bender CE & Van Heerden JA (1995) Percutaneous cholecystectomy: a
valuable technique in high-risk patients with presumed acute cholecystitis. Br J Surg 82:1274-1277.
Michl P, Buchholz M, Rolke M, Kunsch S, Lohr M, McClane B, Tsukita S, Leder G, Adler G & Gress TM (2001) Claudin-4: a new target for pancreatic cancer treatment using Clostridium perfringens enterotoxin. Gastroenterology 121:678-684.
Mirvis SE, Vainright JR, Nelson AW, Johnston GS, Shorr R, Rodriguez A & Whitley NO (1986) The diagnosis of acute acalculous cholecystitis: A comparison of sonography, scintigraphy and CT. Am J Roentgenol 147:1171-1175.
Molenat F, Boussugas A, Valantin V & Sainty JM (1996) Gallbladder abnormalities in medical ICU patients: an ultrasonographic study. Intensive Care Med 22:356-358.
Moreno R, Vincent JL, Matos R, Mendoca A, Cantraine F, Thijs L, Takala J, Sprung C, Antonelli M, Bruining H & Willatts S (1999) The use of maximum SOFA score to quantify organ dysfunction/failure in intensive care. Results of a prospective, multicentre study. Intensive Care Med 25:686-696.
Morita K, Sasaki H, Furuse M & Tsukita S (1999) Endothelial claudin: claudin-5/TMVCF constitutes tight junction strands in endothelial cells. J Cell Biol 147:185-194.
Mutlu GM, Mutlu EA & Factor P (2001) GI complications in patients receiving mechanical ventilation. Chest 119:1222-1241.
Myers SI, Haley-Russel D, Parks L & Husband K (1988) Common bile duct ligation in rabbit: a new model of acute cholecystitis description of histology and bile analysis. J Surg Res 45:556-564.
Orlando R, Gleason E & Drezner AD (1983) Acute acalculous cholecystitis in critically ill patient. Am J Surg 145:472-476.
Ouriel K, Green RM, Ricotta JJ, DeWeese JA & Adams JT (1984) Acute acalculous cholecystitis complicating abdominal aortic aneurysm resection. J Vasc Surg 1:646-648.
Ozaki H, Ishii K, Horiuchi H, Arai H, Kawamoto T, Okawa K, iwamatsu A & Kita T (1999) Cutting edge: combined treatment of TNF-α and IFN-γ causes redistribution of junctional adhesion molecule in human endothelial cells. J Immunol 163:553-557.
Parkman HP, James AN, Bogar LJ, Bartula LLThomas RM, Ryan JP & Myers SI (2000) Effect of acalculous cholecystitis on gallbladder neuromuscular transmission and contractility. J Surg Res 88:182-192.
Parviainen I (1997) Gastric tonometry in the assessment of splanchnic perfusion. Methodological aspects and evaluation of simultaneous regional blood flow measurements and gastric tonometry after coronary artery bypass grafting surgery. Kuopio University Publications D. Medical Sciences 123.
Paull DE (2001) Acute cholecystitis in the immediate postoperative period following esophagogastrectomy. Am Surg 67:97-99.
Pelinka LE, Schmidhammer R, Hamid L, Mauritz W & Redl H (2003) Acute acalculous cholecystitis after trauma: A prospective study. J Trauma 55:323-329.
Petersen SR & Sheldon GF (1979) Acute acalculous cholecystitis: a complication of hyperalimentation. Am J Surg 138:814-817.
Perttilä J, Salo M, Vuori A & Heikelä A (1989) Effects of various ventilation modes on immunocompetence in surgical patients. Acta Anaesthesiol Scand 33:348-352.
Pettilä V, Pettilä M, Sarna S, Voutilainen P & Takkunen O (2002) Comparison of multiple organ dysfunction scores in the prediction of hospital mortality in the critically ill. Crit Care Med 30:1705-1711.
65
Prasad S, Mingrino R, Kaukinen K, Hayes KL, Powell RM, MacDonald TT & Collins JE (2005) Inflammatory processes have differential effects on claudins 2, 3, and 4 in colonic epithelial cells. Lab Invest 85:1139-1162.
Prevot N, Mariat G, Mahul P, Granjon D, Cuilleron M, Tiffet O, De Filipis JP, Jospe R, Auboyer C & Dubois F (1999) Contribution of cholescintigraphy to the early diagnosis of acute acalculous cholecystitis in intensive-care-unit patients. Eur J Nucl Med 26:1317-1325.
Puc MM, Tran HS, Wry PW & Ross SE (2002) Ultrasound is not a useful screening tool for acute acalculous cholecystitis in critically ill trauma patients. Am Surg 68:65-69.
Rady MY, Kodavatiganti R & Rayan T (1998) Perioperative predictors of acute cholecystitis after cardiovascular surgery. Chest 114:76-84.
Rahner C, Mitic LL & Anderson JM (2001) Heterogeneity in expression and subcellular localization of claudins 2, 3, 4 and 5 in the rat liver, pancreas and gut. Gastroenterology 120:411-422.
Ranieri VM, Suter PM, Tortorella C, De Tullio R, Dayer JM, Brienza A, Bruno F & Slutsky AS (1999) Effect of mechanical ventilation on inflammatory mediators in patients with acute respiratory distress syndrome. JAMA 282:54-61.
Raunest J, Imhof M, Rauen U, Ohmann CH, Thon KP & Burrig KF (1992) Acute cholecystitis: A complication in severely injured intensive care patients. J Trauma 32:433-440.
Rautanen M, Kuttila K, Gullichsen E, Perttilä J, Nelimarkka O & Niinikoski J (1996) Splanchnic and peripheral tissue perfusion in experimental fat embolism. Crit Care Med 24:1018-1024.
Roslyn JJ, Pitt HA, Mann LL, Ament ME & DenBesten L (1983) Gallbladder disease in patients on long-term parenteral nutrition. Gastroenterology 84:148-154.
Ryu JK, Ryu KH & Kim KH (2003) Clinical features of acute acalculous cholecystitis. J Clin Gastroenterol 36:166-169.
Saha A, Batra P, Vilhekar KY & Chaturvedi P (2005) Acute acalculous cholecystitis in a child with plasmodium falciparum malaria. Ann Trop Pediatr 25:141-142.
Saitou M, Furuse M, Sasaki H, Schulzke JD, Fromm M, Takano H, Noda T & Tsukita S (2000) Complex phenotype of mice lacking occludin, a component of tight junction strands. Mol Biol Cell 11:4131-4142.
Samonte VA, Goto M, Ravindranath TM, Fazal N, Holloway VM, Goyal A, Gamelli RL & Sayeed MM (2004) Exacerbation of intestinal permeability in rats after a two-hit injury: Burn and Enterococcus faecalis infection. Crit Care Med 32:2267-2273.
Savino JA, Scalea TM & Del Guercio LR (1985) Factors encouraging laparotomy in acalculous cholecystitis. Crit Care Med 13:377-380.
Savoca PE, Longo WE, Pasternak B & Gusberg RJ (1990a) Does visceral ischemia play a role in the pathogenesis of acute acalculous cholecystitis ? J Clin Gastroenterol 12:33-36.
Savoca PE, Longo WE, Zucker KA, McMillen MM & Modlin IM (1990b) The increasing prevalence of acalculous cholecystitis in outpatients. Results of a 7-year study. Ann Surg 211:433-437.
Sawada N, Murata M, Kikuchi K, Osanai M, Tobioka H, Kojima T & Chiba H (2003) Tight junctions and human diseases. Med Electron Microsc 36:147-156.
Schneeberger EE & Lynch RD (2004) The tight junction: a multifunctional complex. Am J Physiol Cell Physiol 286:C1213-C1228.
Sessions SC, Scoma RS, Sheikh FA, McGeehin WH & Smink RD Jr (1993) Acute acalculous cholecystitis following open heart surgery. Am Surg 59:74-77.
Shapiro MJ (1999) Acute acalculous cholecystitis. In: Webb R, Shapiro MJ, Singer M, Suter PM (eds) Oxford textbook of critical care. Oxford University Press, New York, 322-323.
Shapiro MJ, Luchtenfeld WB, Kurzweil S, Kaminski DL, Durham RM & Mazuski JE (1994) Acute acalculous cholecystitis in the critically ill. Am Surg 60:335-339.
66
Shea JA, Berlin JA, Escarce JJ, Clarke JR, Kinosian BP, Cabana MD, Tsai WW, Horangic N, Malet PF & Schwartz JS (1994) Revised estimates of diagnostic test sensitivity and specificity in suspected biliary tract disease. Arch Int Med 154:2573-2581.
Simon DB, Lu Y, Choate KA, Velazquez H, Al-Sabban E, Praga M, Casari G, Bettinelli A, Colussi G, Rodriguez-Soriano J, McCredie D, Milford D, Sanjad S & Lifton RP (1999) Paracellin-1, a renal tight junction protein required for paracellular Mg2++
resorption. Science 285:103-106. Sosna J, Kruskal JB, Copel L, Goldberg SN & Kane RA (2004) US-guided percutaneous
cholecystectomy: features predicting culture-positive bile and clinical outcome. Radiology 230:785-791.
Spira RM, Nissan A, Zamir O, Cohen T, Fields SI & Freund HR (2002) Percutaneous transhepatic cholecystectomy and delayed laparoscopic cholecystectomy in critically ill patients with acute calculus cholecystitis. Am J Surg 183:62-66.
Stevens PE, Harrison NA & Rainford DJ (1988) Acute acalculous cholecystitis in acute renal failure. Intensive Care Med 14:411-416.
Stevenson BR, Siliciano JD, Mooseker MS & Goodenough DA (1986) Identification of ZO-1: A high molecular weight polypeptide associated with the tight junction (zonula occludens) in a variety of epithelial. J Cell Biol 103:755-766.
Tabata M (1994) Experimental study of the pathogenesis of acute acalculous cholecystitis: Role of autonomic denervation. J Gastroenterol 29:320-331.
Taoka H (1991) Experimental study on the pathogenesis of acute acalculous cholecystitis, with special reference to the roles of microcirculatory disturbances, free radicals and membrane-bound phospholipase A2. Gastroenterol Jpn 26:633-644.
Tenhunen JJ, Uusaro A, Kärjä V, Oksala N, Jakob SM & Ruokonen E (2003) Apparent heterogeneity of regional blood flow and metabolic changes within splanchnic tissues during experimental endotoxin shock. Anesth Analg 97:555-563.
Thompson JW, Ferris DO & Baggenstoss AH (1962) Acute cholecystitis complicating operation for other diseases. Ann Surg 155:489-494.
Topeli A, Demiroglu H & Dundar S (1996) Acute acalculous cholecystitis in patients with acute leukaemia. Br J Clin Pract 50:224-245.
Toung T, Reilly PM, Fuh KC, Ferris R & Bulkley GB (2000) Mesenteric vasoconstriction in response to hemorrhagic shock. Shock 13:267-273.
Trowbridge RL, Rutkowski NK & Kaveh GS (2003) Does this patient have acute cholecystitis? JAMA 289:80-86.
Tsakayannis DE, Kozakewich HPW & Liilehei CV (1996) Acalculous cholecystitis in children. J Pediatr Surg 31:127-131.
Tsukita S, Furuse M & Itoh M (2001) Multifunctional strands in tight junctions. Nature Reviews 2:285-293.
Tunggal JA, Helfrich I, Schmitz A, Schwarz H, Gunzel D, Fromm M, Kemler R, Krieg T & Niessen CM (2005) E-cadherin is essential for in vivo epidermal barrier function by regulating tight junctions. EMBO J 24:1146-1156.
Turksen K & Troy TC (2004) Barriers built on claudins. J Cell Sci 117: 2435-2447. Van den Berghe G, Wouters P, Weekers F, Verwaest C, Bruyninckx F, Schietz M, Vlasselaers D,
Ferdinande P, Lauwers P & Bouillon R (2001) Intensive insulin therapy in critically ill patients. N Engl J Med 345:1359-1367.
van Meer G & Simons K (1986) The function of tight junctions in maintaining differences in lipid composition between the apical and basolateral cell surface domains of MDCK cells. EMBO J 5: 1454-1455.
67
van Sonnenberg E, D’Agostino HB, Goodacre BW, Sanchez RB & Casola G (1992) Percutaneous gallbladder puncture and cholecystostomy: results, complications, and caveats for safety. Radiology 183:167-170.
Vilaichone RK, Mahachai V & Wilde H (1999) Acute acalculous cholecystitis in leptospirosis. J Clin Gastroenterol 29:280-283.
Vincent JL, de Mendoca A, Cantraine F, Moreno R, Takala J, Suter PM, Sprung CL, Colardyn F & Blecher S (1998) Use of the SOFA score to assess the incidence of organ dysfunction/failure in intensive care units: results of a multicenter, prospective study. Crit Care Med 26:1793-800.
Vincent JL, Moreno R, Takala J, Wallatts S, De Mendoca A, Bruining H, Reinhart CK, Suter PM & Thjis LG (1996) The SOFA (sepsis-related organ failure assessment) score to describe organ dysfunction/failure. Intensive Care Med 22:707-710.
Wang AJ, Wang TE, Lin CC, Lin SC & Shih SC (2003) Clinical predictors of severe complications in acute acalculous cholecystitis. World J Gastroenterol 9:2821-2823.
Warren BL (1992) Small vessel occlusion in acute acalculous cholecystitis. Surgery 111:163-168. West BC, Silberman R & Otterson WN (1998) Acalculous cholecystitis and septicaemia caused by
non-O1 vibrio cholerae: first reported case and review of biliary infections with vibrio cholerae. Diagn Microbiol Infect Dis 30:187-191.
Wiboltt KS & Jeffrey RB Jr (1997) Acalculous cholecystitis in patients undergoing bone marrow transplantation. Eur J Surg 163:519-524.
Wilcox ER, Burton QL, Naz S, Riazuddin S, Smith TN, Ploplis B, Belyantseva I, Ben-Yosef T, Liburd NA, Morell RJ, Kachar B, Wu DK, Griffith AJ, Riazuddin S & Friedman TB (2001) Mutations in the gene encoding tight junction claudin-14 cause autosomal recessive deafness DFNB29. Cell 104:165-172.
Wu KL, Changhien CS, Kuo CM, Chuah SK, Lu SN, Eng HL & Kuo CH (2003) Dengue fever with acalculous cholecystitis. Am J Trop Med Hyg 68:657-660.
Wu SD, Zhang ZH, Jin JZ, Kong J, Wang W, Zhang Q, Li DY & Wang MF(2004) Effects of narcotic analgesic drugs on human Oddi’s sphincter motility. World J Gastroenterol 10:2901-2904.
Original publications
I Laurila J, Syrjälä H, Laurila PA, Saarnio J & Ala-Kokko TI (2004) Acute acalculous cholecystitis in critically ill patients. Acta Anaesthesiol Scand 48: 986-991.
II Laurila J, Laurila PA, Saarnio J, Koivukangas V, Syrjälä H & Ala-Kokko TI (2006) Organ system dysfunction following open cholecystectomy for acute acalculous cholecystitis in critically ill patients. Acta Anaesthesiol Scand 50: 173-179.
III Laurila JJ, Ala-Kokko TI, Laurila PA, Saarnio J, Koivukangas V, Syrjälä H & Karttunen TJ (2005) Histopathology of acute acalculous cholecystitis in critically ill patients. Histopathology 47: 485-492.
IV Laurila JJ, Karttunen TJ, Koivukangas V, Laurila PA, Syrjälä H, Saarnio J, Soini Y & Ala-Kokko TI. Expression of tight junction proteins in acute acalculous and calculous cholecystitis. (Submitted).
Articles I-III are reprinted with the permission of Acta Anaesthesiologica Scandinavica and Histopathology.
Original papers are not included in the electronic version of the dissertation.
A C T A U N I V E R S I T A T I S O U L U E N S I S
Distributed byOULU UNIVERSITY LIBRARY
P.O. Box 7500, FI-90014University of Oulu, Finland
Book orders:OULU UNIVERSITY PRESSP.O. Box 8200, FI-90014University of Oulu, Finland
S E R I E S D M E D I C A
863. Karihtala, Peeter (2005) Oxidative damage and counteracting mechanisms inbreast carcinoma
864. Penttilä, Hannu (2005) Myocardial and cerebral preservation during off-pumpcoronary artery surgery
865. Törmäkangas, Liisa (2005) Experimental Chlamydia pneumoniae infection model:effects of repeated inoculations and treatment
866. Willig, Reeta (2006) Hip fracture—aspects of background factors and outcome
867. Pönkkö, Maija-Leena (2005) Erityisoppilaan psykiatrinen hoitoketju. Hoitoketjuntarpeen ja toiminnan monitahoarviointi
868. Leppilampi, Mari (2006) Functional and immunohistological studies on cancer-associated carbonic anhydrase IX
869. Nurmenniemi, Petri (2006) Inflammatory cells and mitotic activity ofkeratinocytes in gingival overgrowth induced by immunosuppressive- andnifedipine medication
870. Hinkula, Marianne (2006) Incidence of gynaecological cancers and overall andcause specific mortality of grand multiparous women in Finland
871. Syrjäpalo, Kyllikki (2006) Arvot ja arvostukset psykiatrisessa hoidossa.Henkilökunnan ja potilaiden näkemyksiä hoidon nykytilasta
872. Karinen, Liisa (2006) Chronic chlamydial infection: impact on human reproductivehealth. Reproductive health research in the Northern Finland 1966 Birth Cohort(NFBC 1966)
873. Silvennoinen, Laura (2006) ERp57—Characterization of its domains anddetermination of solution structures of the catalytic domains
874. Sorppanen, Sanna (2006) Kliinisen radiografiatieteen tutkimuskohde.Käsiteanalyyttinen tutkimus kliinisen radiografiatieteen tutkimuskohdettamäärittävistä käsitteistä ja käsitteiden välisistä yhteyksistä
875. Erola, Tuomo (2006) Deep brain stimulation of the subthalamic nucleus inParkinson's disease. A clinical study
876. Mäkinen, Tiina M. (2006) Human cold exposure, adaptation and performance in anorthern climate
877. Autio, Reijo (2006) MRI of herniated nucleus pulposus. Correlation with clinicalfindings, determinants of spontaneous resorption and effects of anti-inflammatorytreatments on spontaneous resorption
D878etukansi.kesken.fm Page 2 Tuesday, May 2, 2006 10:22 AM
ABCDEFG
UNIVERS ITY OF OULU P .O . Box 7500 F I -90014 UNIVERS ITY OF OULU F INLAND
A C T A U N I V E R S I T A T I S O U L U E N S I S
S E R I E S E D I T O R S
SCIENTIAE RERUM NATURALIUM
HUMANIORA
TECHNICA
MEDICA
SCIENTIAE RERUM SOCIALIUM
SCRIPTA ACADEMICA
OECONOMICA
EDITOR IN CHIEF
EDITORIAL SECRETARY
Professor Mikko Siponen
Professor Harri Mantila
Professor Juha Kostamovaara
Professor Olli Vuolteenaho
Senior assistant Timo Latomaa
Communications Officer Elna Stjerna
Senior Lecturer Seppo Eriksson
Professor Olli Vuolteenaho
Publication Editor Kirsti Nurkkala
ISBN 951-42-8097-0 (Paperback)ISBN 951-42-8098-9 (PDF)ISSN 0355-3221 (Print)ISSN 1796-2234 (Online)
FACULTY OF MEDICINE, DEPARTMENT OF ANAESTHESIOLOGY, DEPARTMENT OF SURGERY, DEPARTMENT OF PATHOLOGY,UNIVERSITY OF OULU;DEPARTMENT OF INFECTION CONTROL,OULU UNIVERSITY HOSPITAL
D 878
AC
TA Jouko Laurila
D878etukansi.kesken.fm Page 1 Tuesday, May 2, 2006 10:22 AM