PL 18190/0011-12 UKPAR Egis Pharmaceutical, Sertraline 50mg and 100mg Tablets 1 Public Assessment Report Sertraline 50mg Tablets Sertraline 100mg Tablets Sertraline hydrochloride PL 18190/0011 PL 18190/0012 Egis Pharmaceutical UK Limited Table of Contents Page Lay Summary 2 Scientific Discussion 3 Overall Conclusion And Risk Benefit/Analysis 12 Steps Taken During Assessment 13 Summary of Product Characteristics 14 Labels and Leaflet 27
Transcript
PL 18190/0011-12
UKPAR Egis Pharmaceutical, Sertraline 50mg and 100mg Tablets
1
Public Assessment Report
Sertraline 50mg Tablets Sertraline 100mg Tablets
Sertraline hydrochloride
PL 18190/0011 PL 18190/0012
Egis Pharmaceutical UK Limited
Table of Contents Page Lay Summary 2 Scientific Discussion 3 Overall Conclusion And Risk Benefit/Analysis 12 Steps Taken During Assessment 13 Summary of Product Characteristics 14 Labels and Leaflet 27
PL 18190/0011-12
Lay Summary The MHRA granted a National Marketing Authorisation (licence) to Egis Pharmaceutical UK Ltd for the medicinal products for Sertraline 50mg and 100mg Tablets on 6th December 2006. Sertaline is used in the treatment of depression. No new or unexpected safety concerns arose from this application and it was, therefore, judged that the benefits of taking this product outweigh the risks, hence a Marketing Authorisation has been granted.
UKPAR Egis Pharmaceutical, Sertraline 50mg and 100mg Tablets
2
PL 18190/0011-12
Scientific Discussion
INTRODUCTION This Public Assessment Report is based on the Assessment Reports for an abridged complex and abridged standard application for a Marketing Authorisation for Sertraline 50mg and 100mg Tablets. The application was submitted, by Egis Pharmaceutical UK Ltd, under article 10.1 (a) (iii) of Directive 2001/83/EC (first paragraph), claiming essential similarity to the innovator product, Lustral (Pfizer Ltd) which were first authorised in the UK on November 19th 1990 (PL 00057/0308-39). A Marketing Authorisation was granted to Egis Pharmaceuticals on 6th December 2006. The active, Sertraline, is a naphthaleneamine derivative, is a selective serotonin re-uptake inhibitor with actions and uses similar to those of fluoxetine. It is administered by mouth and in the treatment of depression, the usual initial dose is 50 mg daily increased, if necessary, in increments of 50 mg at intervals of at least a week to a maximum of 200 mg daily
PHARMACEUTICAL ASSESSMENT DRUG SUBSTANCE The drug substance is the subject of a Drug Master File (DMF). A satisfactory letter of access was provided and the latest version of the DMF has been assessed and accepted. A declaration was provided that the Market Authorisation holder would be notified of any changes in the manufacturing process of the active.
General information Sertraline Hydrochloride is a white crystalline powder, slightly soluble in water. There are no pharmacopoeia monograph (PhEur, BP or USP) for this active, and the active is controlled using an in-house specification which is acceptable. Control of Active Ingredient The Certificates of Analysis and results of the in-house testing for three typical batches are provided demonstrating compliance with the proposed specification. The methods used for assay, related substances and residual solvents are in-house methods and are validated. Satisfactory Certificates of Analysis are provided for the reference standards used in the development and validation of these methods. Stability of Active Ingredient The material is packed in polybags and placed in fiber drum/container. Stability data is provided on a number of batches of active stored at 25C/60% RH. Stability results presented indicate that the assay values and related substances (No significant change in the level of known or unknown impurities. Total impurities below 0.2%) are within the in-house proposed specifications. The polymorphic stability of the drug substance is confirmed during storage by IR.
UKPAR Egis Pharmaceutical, Sertraline 50mg and 100mg Tablets
3
PL 18190/0011-12
DRUG PRODUCT Composition Tablets are white, oval shape, biconvex, coated, with a score line on one side and E271 or 272 on the other side. The 100 mg tablets are punched at double weight prior to coating, therefore, the composition of the core is identical to that of the 50 mg tablets. The qualitative composition of the tablets is shown below;
3.2. CONTAINER The tablets are in PVC/PVdC/Aluminium (250 µm/60g/m2/ 20micron) blister strips. The blister strips are packed in cardboard cartons containing a total of 28 tablets. Two blister strips of 14 tablets. 3.3. CLINICAL TRIAL FORMULA The batch used for the conduct of the PK study was manufactured using the same formulation proposed for marketing. 3.4. DEVELOPMENT PHARMACEUTICS The tablets were developed as a generic equivalent to the brand leader marketed by Pfizer. It is stated that the properties (physical and chemical properties, as well as the list of excipients) the brand leader manufactured and marketed in Europe by Pfizer, were investigated. The applicant was asked to provide further data on dissolution profiles and comparative impurity profiles. This was provided, and together with the results of the bioequivalence study, support the claim of essential similarity.
UKPAR Egis Pharmaceutical, Sertraline 50mg and 100mg Tablets
4
PL 18190/0011-12
Manufacture The manufacturing site has been inspected by a PECA authority and is GMP compliant. Satisfactory manufacturing licences were provided for active, finished product and assembly. The manufacturing process was adequately summarised and a flow diagram was provided. Excipients The excipients are PhEur grade. Satisfactory in-house specification and Certificates of Analysis are provided for typical batches of excipients and are satisfactory. Supplier’s Certificates of Analysis for typical batches of the excipients have been provided. Control of Finished Product Detail of the batch data, in- process controls, sampling plans, the tests carried out and the results obtained were presented. After tightening of some parameters after assessment of batch data a satisfactory finished product specification was provided. Results of the chemical and physical testing of the validation batches are satisfactory and show consistency and control in the manufacturing process. Stability The stability data provided are on batches of 50-mg tablets and batches of 100-mg tablets. Data provided supports the shelf-life of 60 months. Photostability data was also provided demonstrating that the product was not light-sensitive. BIOAVAILABILITY/BIOEQUIVALENCE For the bioequivalence study please see medical assessment. TSE and BSE The applicant declares that magnesium stearate is of animal origin, and an acceptable TSE Certificate of Suitability is provided. Declarations are provided from Egis regarding other excipients and activated carbon used in the purification of active substance. Egis states that based on the information received from each supplier, it is declared that the product contains no material of animal origin except magnesium stearate.
UKPAR Egis Pharmaceutical, Sertraline 50mg and 100mg Tablets
5
PL 18190/0011-12
Summary of Product Characteristics SPC), Patient Information Leaflet (PIL) and packaging Minor amendments were made to the SPC, PIL and full colour mock-ups of the packaging provided. The revised SPC can be found on page 14 of this report and the PIL on page of this report. Expert Report The pharmaceutical expert is suitably qualified and the report was satisfactory.
ASSESSOR’S OVERALL CONCLUSIONS ON QUALITY AND ADVICE A Marketing Authorisation was granted.
UKPAR Egis Pharmaceutical, Sertraline 50mg and 100mg Tablets
6
PL 18190/0011-12
MEDICAL ASSESSMENT
1. INTRODUCTION This national abridged application claims essential similarity to Lustral tablets Pfizer PL 0057/0308. 2. INDICATIONS The indication for Obsessive Compulsive Disorder was included during assessment and the indications were amended so that they are fully consistent with the current cross-reference SPC. 3. DOSE & DOSE SCHEDULE This section was amended to be fully consistent with the cross-reference SPC, particularly with respect to the dosage regime in children during assessment. 4. TOXICOLOGY No new data 5. CLINICAL PHARMACOLOGY The applicant has conducted a randomised single dose 2-way cross-over comparative bioavailability study of 2x50 mg test product against the Italian cross-reference product Zoloft 50mg tablet (Pfizer) in 22 healthy male volunteers. Pharmacokinetics of Actives Sertraline is slowly absorbed from the GI tract with peak plasma concentrations occurring about 4.5 to 8.5 hours after ingestion and elimination half-life of 24 to 26 hours (Martindale).It undergoes extensive first-pass metabolism in the liver. The main pathway is demethylation to N-desmethylsertraline which is inactive. Sertraline is highly bound (98%) to plasma proteins. The metabolites are excreted in faeces and urine at almost equal extent. Certificates of Analysis are provided for both batches used in the study. The study conducted was 2 periods of single dose administration, separated by 28 days between doses. Blood samples were collected immediately before and at 1.0, 2.0, 3.0, 4.0, 5.0, 5.5, 6.0, 6.5, 7.0, 7.5, 8.0, 9.0, 10.0, , 12.0, 16.0, 24.0, 48,.0, 72.0, 96.0,120.0 , 144.0, 192.0, 240 hours after study drug administration. The frequency and total number of blood collections per study period is sufficient for actives with the above reported half-lives. 19 of the volunteers completed the study (Volunteer NO 15 and 16 did not complete the study). Sertraline and N-desmethylsertraline were analysed using a validated GC/MS method with LODs of 0.50ng/ml for Sertraline and for N-desmethylsertraline. Standard curve
UKPAR Egis Pharmaceutical, Sertraline 50mg and 100mg Tablets
7
PL 18190/0011-12
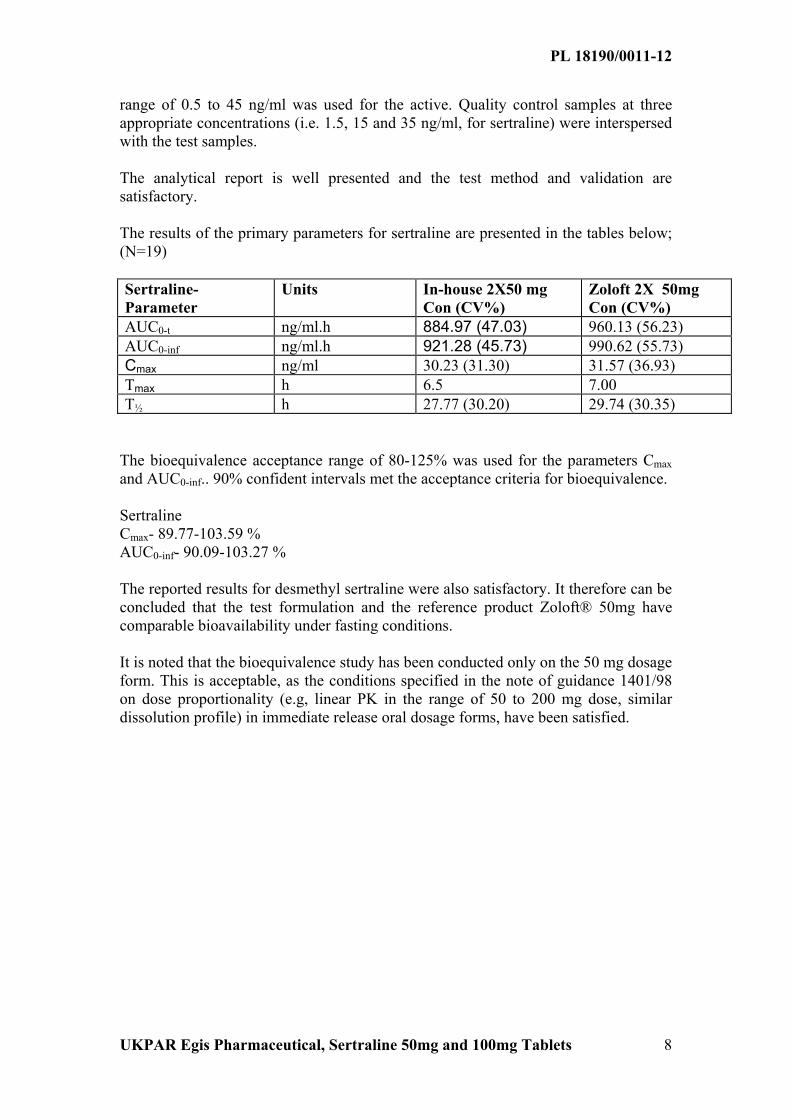
range of 0.5 to 45 ng/ml was used for the active. Quality control samples at three appropriate concentrations (i.e. 1.5, 15 and 35 ng/ml, for sertraline) were interspersed with the test samples. The analytical report is well presented and the test method and validation are satisfactory. The results of the primary parameters for sertraline are presented in the tables below; (N=19) Sertraline-Parameter
The bioequivalence acceptance range of 80-125% was used for the parameters Cmax and AUC0-inf.. 90% confident intervals met the acceptance criteria for bioequivalence. Sertraline Cmax- 89.77-103.59 % AUC0-inf- 90.09-103.27 % The reported results for desmethyl sertraline were also satisfactory. It therefore can be concluded that the test formulation and the reference product Zoloft® 50mg have comparable bioavailability under fasting conditions. It is noted that the bioequivalence study has been conducted only on the 50 mg dosage form. This is acceptable, as the conditions specified in the note of guidance 1401/98 on dose proportionality (e.g, linear PK in the range of 50 to 200 mg dose, similar dissolution profile) in immediate release oral dosage forms, have been satisfied.
UKPAR Egis Pharmaceutical, Sertraline 50mg and 100mg Tablets
8
PL 18190/0011-12
6. EFFICACY No new data 7. SAFETY No new data 8. EXPERT REPORTS The clinical expert report is satisfactory and from a suitably qualified expert. 9. PATIENT INFORMATION LEAFLET (PIL) The PIL was redrafted in accordance with the amendments to the SPC 10. LABELLING Medically satisfactory 11. APPLICATION FORM (MAA) Satisfactory 12. SUMMARY OF PRODUCT CHARACTERISTICS (SPC) A number of amendments to the SPC were made during assessment including; Interactions: The potential interaction with pimozide was added. Undesirable effects: This section was altered to include the side effect profile in children with OCD and be fully consistent with the current cross-reference SPC. 13. DISCUSSION The 90% CI for ratios of AUC and Cmax for both sertraline an its active metabolite desmethyl sertraline were within the acceptable guideline ranges of 80 - 125% and 70 - 143% respectively. 14. MEDICAL CONCLUSION A Marketing authorisation was granted.
UKPAR Egis Pharmaceutical, Sertraline 50mg and 100mg Tablets
9
PL 18190/0011-12
Overall Conclusion and Risk/Benefit Analysis
Quality The quality aspects of Sertraline 50mg and 100mg Tablets are well defined and controlled. The specifications and batch analytical results indicate consistency from batch to batch. There are no outstanding quality issues that would have a negative impact on the benefit/risk balance. Pre-Clinical No new pre-clinical data were presented or were required for this type of application.
Clinical No formal data on clinical efficacy or safety were presented for this application and none were required. A satisfactory bioequivalence study was carried out. Changes were made to the Summary of Product Characteristics, PIL and packaging to satisfy current requirements.
Risk/Benefit Analysis The quality of the products, Sertraline 50mg and 100mg Tablets, is acceptable and the products are essentially similar to the reference product which has a positive risk/benefit assessment. A Marketing Authorisation was granted.
UKPAR Egis Pharmaceutical, Sertraline 50mg and 100mg Tablets
10
PL 18190/0011-12
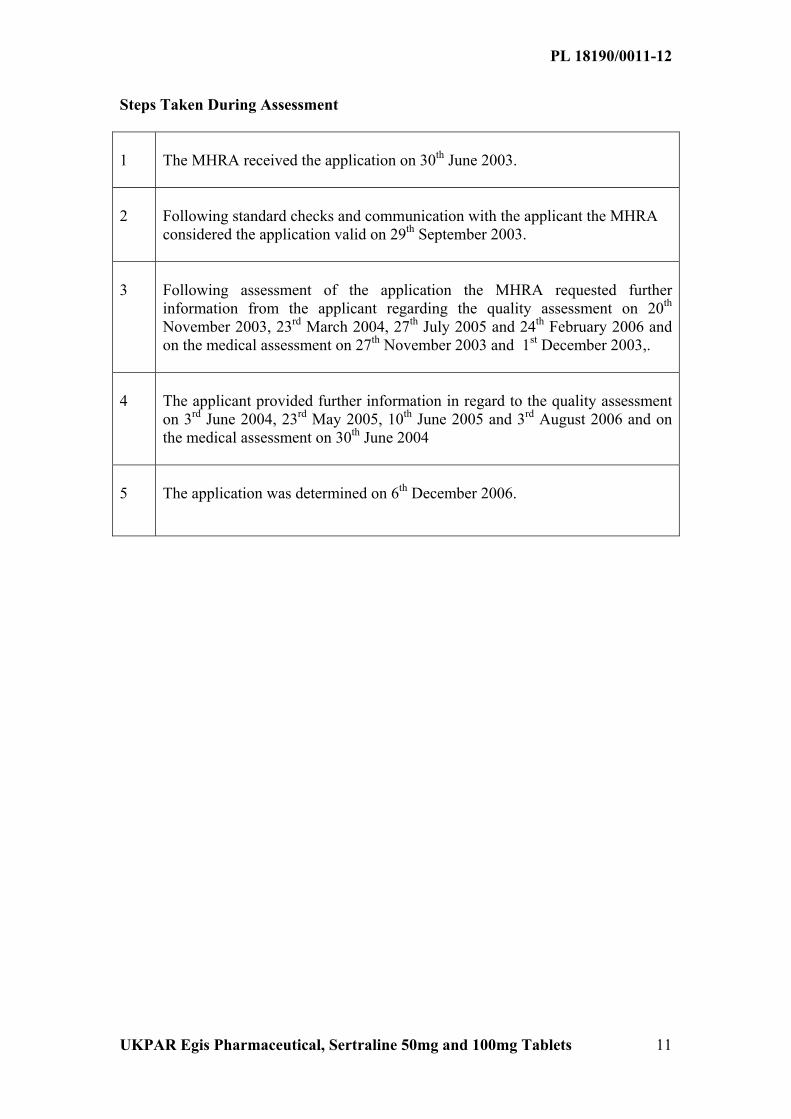
Steps Taken During Assessment 1
The MHRA received the application on 30th June 2003.
2
Following standard checks and communication with the applicant the MHRA considered the application valid on 29th September 2003.
3
Following assessment of the application the MHRA requested further information from the applicant regarding the quality assessment on 20th November 2003, 23rd March 2004, 27th July 2005 and 24th February 2006 and on the medical assessment on 27th November 2003 and 1st December 2003,.
4
The applicant provided further information in regard to the quality assessment on 3rd June 2004, 23rd May 2005, 10th June 2005 and 3rd August 2006 and on the medical assessment on 30th June 2004
5
The application was determined on 6th December 2006.
UKPAR Egis Pharmaceutical, Sertraline 50mg and 100mg Tablets
11
PL 18190/0011-12
SUMMARY OF PRODUCT CHARACTERISTICS
1 NAME OF THE MEDICINAL PRODUCT Sertraline 50mg film-coated Tablets
2 QUALITATIVE AND QUANTITATIVE COMPOSITION Each tablet contains sertraline hydrochloride equivalent to 50mg sertraline. For excipients, see section 6.1
3 PHARMACEUTICAL FORM Film-coated tablet
White or almost white, odourless, oval shaped, biconvex film-coated tablets, having stylised E and 271 mark on one side and halving line on the other side.
The halving line, or breakline on one face of the tablet allows the tablet to be broken to give a unit dose of 25 mg of sertraline.
4 CLINICAL PARTICULARS
4.1 Therapeutic indications Sertraline 50mg film-coated Tablets are indicated for the treatment of symptoms of depressive illness, including accompanying symptoms of anxiety. Following satisfactory response, continuation with Sertraline 50mg film-coated Tablets therapy is effective in preventing relapse of the initial episode of depression or recurrence of further episodes, including accompanying symptoms of anxiety. Sertraline is also indicated for the treatment of obsessive compulsive disorder (OCD). Following initial response, sertraline has been associated with sustained efficacy, safety and tolerability in up to two years treatment of OCD. Sertraline is also indicated for the treatment of paediatric patients with OCD. Clinical trials in PTSD (post-traumatic stress disorder) demonstrated efficacy in female patients but no evidence of efficacy was seen in males. Treatment with sertraline cannot normally therefore be recommended for male patients with PTSD. A therapeutic trial in males might on occasion be justified, but treatment should subsequently be withdrawn unless there is clear evidence of therapeutic benefit.
UKPAR Egis Pharmaceutical, Sertraline 50mg and 100mg Tablets
12
PL 18190/0011-12
Sertraline is not indicated for use in children and adolescents under the age of 18 years with Major Depressive Disorder. In particular, controlled clinical studies failed to demonstrate efficacy and do not support the use of sertraline in the treatment of children and adolescents with Major Depressive Disorder. (See sections 4.3 Contraindications and 4.8 Undesirable effects).
4.2 Posology and method of administration Sertraline 50mg film-coated Tablets should be given as a single daily dose. Sertraline 50mg film-coated Tablets can be administered with or without food.
Adults Depression (including accompanying symptoms of anxiety): The starting dose is 50mg daily and the usual antidepressant dose is 50mg daily. In some patients, doses higher than 50mg may be required.
Obsessive Compulsive Disorder: The starting dose is 50mg daily, and the therapeutic dose range is 50-200mg daily.
Post-Traumatic Stress Disorder: Treatment for PTSD should be initiated at 25 mg/day. After one week, the dose should be increased to 50mg once daily. PTSD is a heterogeneous illness and some patient groups fulfilling the criteria for PTSD do not appear to be responsive to treatment with Sertraline 50mg film-coated Tablets. Dosing should be reviewed periodically by the prescribing physician to determine response to therapy and treatment should be withdrawn if there is no clear evidence of efficacy.
Depression (including accompanying symptoms of anxiety), OCD and PTSD: In some patients doses higher than 50mg daily may be required. In patients with incomplete response but good toleration at lower doses, dosage adjustments should be made in 50mg increments over a period of weeks to a maximum of 200mg daily.
Once optimal therapeutic response is achieved the dose should be reduced, depending on therapeutic response, to the lowest effective level. Dosage during prolonged maintenance therapy should be kept at the lowest effective level, with subsequent adjustments depending on therapeutic response. The onset of therapeutic effect may be seen within 7 days, although 2-4 weeks (and even longer in OCD) are usually necessary for full activity. A longer treatment period, even beyond 12 weeks in some cases, may be required in the case of a therapeutic trial in PTSD. Use in children aged 6-17 years Treatment should only be initiated by specialists. The safety and efficacy of sertraline has been established in paediatric OCD patients (aged 6-17). The administration of sertraline to paediatric OCD patients (aged 13-17) should commence at 50mg/day. Therapy for paediatric OCD patients (aged 6-12) should commence at 25mg/day increasing to 50mg/day after 1 week. Subsequent doses may be increased in case of lack of response in 50mg/day increments up to 200mg/day as needed. However, the generally lower body weights of children compared to adults should be taken into consideration in advancing the dose from 50mg, in order to avoid excessive dosing. Given the 24 hour elimination half-life of sertraline, dose changes should not occur at intervals of less than 1 week.
UKPAR Egis Pharmaceutical, Sertraline 50mg and 100mg Tablets
13
PL 18190/0011-12
The efficacy and safety of sertraline in children and adolescents under the age of 18 years with Major Depressive Disorder have not been established. Controlled clinical studies failed to demonstrate efficacy and do not support the use of sertraline in the treatment of children and adolescents with Major Depressive Disorder (See sections 4.3 Contraindications and 4.8 Undesirable effects.) Children aged less than six years Sertraline is not recommended in children under six years of age since safety and efficacy have not been established. (See also 5.1 ‘Pharmacological Properties’). Use in the elderly No special precautions are required. The usual adult dose is recommended. Several hundred elderly patients have participated in clinical studies with sertraline. The pattern and incidence of adverse reactions in the elderly is similar to that in younger patients. Withdrawal symptoms seen on discontinuation of sertraline Abrupt discontinuation should be avoided. When stopping treatment with sertraline the dose should be gradually reduced over a period of at least one to two weeks in order to reduce the risk of withdrawal reactions (see section 4.4 Special warnings and special precautions for use and section 4.8 Undesirable effects). If intolerable symptoms occur following a decrease in the dose or upon discontinuation of treatment, then resuming the previously prescribed dose may be considered. Subsequently, the physician may continue decreasing the dose, but at a more gradual rate.
Sertraline 50mg film-coated Tablets are for oral administration only. 4.3 Contraindications Sertraline 50mg film-coated Tablets are contra-indicated in patients with a known hypersensitivity to sertraline. Monoamine oxidase inhibitors: Cases of serious and sometimes fatal reactions have been reported in patients receiving an SSRI in combination with a monoamine oxidase inhibitor (MAOI), including the selective MAOI selegiline and reversible MAOI (RIMA) moclobemide and in patients who have recently discontinued an SSRI and have been started on a MAOI. Some cases presented with features resembling serotonin syndrome. Symptoms of a drug interaction with a MAOI include: hyperthermia, rigidity, myoclonus, autonomic instability with possible rapid fluctuations of vital signs, mental status changes that include confusion, irritability and extreme agitation progressing to delirium and coma. Sertraline 50mg film-coated Tablets should not be used in combination with a MAOI. Sertraline 50mg film-coated Tablets may be started 14 days after discontinuing treatment with an irreversible MAOI and at least one day after discontinuing treatment with the reversible MAOI (RIMA), moclobemide. At least 14 days should elapse after discontinuing Sertraline 50mg film-coated Tablets treatment before starting a MAOI or RIMA.
UKPAR Egis Pharmaceutical, Sertraline 50mg and 100mg Tablets
14
PL 18190/0011-12
Use in hepatic impairment: There is insufficient clinical experience in patients with significant hepatic dysfunction and accordingly Sertraline 50mg film-coated Tablets should not be used in such patients. Concomitant use in patients taking pimozide is contra-indicated (see section 4.5 Interaction with other medicinal products and other forms of interaction). Sertraline should not be used in children and adolescents under the age of 18 years with Major Depressive Disorder. (See section 4.8 Undesirable effects.) 4.4 Special warnings and special precautions for use Monoamine oxidase inhibitors See 4.3 ‘Contraindications’.
Use in patients with renal or hepatic impairment As with many other medications, sertraline should be used with caution in patients with renal and hepatic impairment (see 4.3 ‘Contraindications’).
Since sertraline is extensively metabolised, excretion of unchanged drug in urine is a minor route of elimination. In patients with mild to moderate renal impairment (creatinine clearance 20-50 ml/min) or severe renal impairment (creatinine clearance <20 ml/min), single dose pharmacokinetic parameters were not significantly different compared with controls. However, steady state pharmacokinetics of sertraline have not been adequately studied in this patient population and caution is advised when treating patients with renal impairment.
Sertraline is extensively metabolised by the liver. A multiple dose pharmacokinetic study in subjects with mild, stable cirrhosis demonstrated a prolonged elimination half-life and approximately three-fold greater AUC and Cmax in comparison with normal subjects. There were no significant differences in plasma protein binding observed between the two groups. The use of sertraline in patients with hepatic disease should be approached with caution. A lower or less frequent dose should be used in patients with hepatic impairment.
Diabetes In patients with diabetes, treatment with an SSRI may alter glycaemic control, possibly due to improvement of depressive symptoms. Insulin and/or oral hypoglycaemic dosage may be needed to be adjusted. Seizures Seizures are a potential risk with antidepressant or antiobsessional drugs. The drug should be discontinued in any patient who develops seizures. Sertraline 50mg film-coated Tablets should be avoided in patients with unstable epilepsy and patients with controlled epilepsy should be carefully monitored. Sertraline 50mg film-coated Tablets should be discontinued if there is an increase in seizure frequency. Electroconvulsive therapy (ECT) Since there is little clinical experience of concurrent administration of sertraline and ECT, caution is advisable.
Mania Sertraline 50mg film-coated Tablets should be used with caution in patients with a history of mania/hypomania. Sertraline 50mg film-coated Tablets should be discontinued in any patient entering a manic phase.
UKPAR Egis Pharmaceutical, Sertraline 50mg and 100mg Tablets
15
PL 18190/0011-12
Suicide/suicidal thoughts Depression is associated with an increased risk of suicidal thoughts, self harm and suicide (suicide-related events). This risk persists until significant remission occurs. As improvement may not occur during the first few weeks or more of treatment, patients should be closely monitored until such improvement occurs. It is general clinical experience that the risk of self harm is highest shortly after presentation and the risk of suicide may increase again in the early stages of recovery. Furthermore, there is evidence that in a small group of people, antidepressants may increase the risk of suicidal thoughts and self-harm. Other psychiatric conditions for which sertraline is prescribed can also be associated with an increased risk of suicide-related events. In addition, these conditions may be co-morbid with major depressive disorder. The same precautions observed when treating patients with major depressive disorder should therefore be observed when treating patients with other psychiatric disorders. Patients with a history of suicide-related events, those exhibiting a significant degree of suicidal ideation prior to commencement of treatment, and young adults, are at a greater risk of suicidal thoughts or suicide attempts, and should receive careful monitoring during treatment. Patients, (and caregivers of patients) should be alerted about the need to monitor for the emergence of suicidal thoughts and to seek medical advice immediately if these symptoms present. Haemorrhage There have been reports of cutaneous bleeding abnormalities such as ecchymoses and purpura with SSRIs.
Caution is advised in patients taking SSRIs, particularly in concomitant use with drugs known to affect platelet function (e.g. atypical antipsychotics and phenothiazines, most tricyclic antidepressants, aspirin and non-steroidal anti-inflammatory drugs (NSAIDs) as well as in patients with a history of bleeding disorders.
Psychomotor restlessness The use of sertraline has been associated with the development of psychomotor restlessness, which clinically may be very similar to akathisia, characterised by a subjectively unpleasant or distressing restlessness and need to move often accompanied by an inability to sit or stand still. This is most likely to occur within the first few weeks of treatment. In patients who develop these symptoms, increasing the dose may be detrimental and it may be necessary to review the use of sertraline. Use in the elderly Several hundred elderly patients have participated in clinical studies with sertraline. The pattern and incidence of adverse reactions in the elderly is similar to that in younger patients. Use in Children and adolescents under 18 years of age Sertraline 50mg film-coated Tablets should not be used in the treatment of children and adolescents under the age of 18 years, except for patients with Obsessive Compulsive Disorder. Suicide-related behaviours (suicide attempt and suicidal thoughts), and hostility (predominantly aggression, oppositional behaviour and anger) were more frequently observed in clinical trials and adolescents treated with antidepressants compared to those treated with placebo. If, based on clinical need, a decision to treat is nevertheless taken, the patient should be carefully monitored for the appearance of suicidal symptoms. In
UKPAR Egis Pharmaceutical, Sertraline 50mg and 100mg Tablets
16
PL 18190/0011-12
addition, long-term safety data in children and adolescents concerning growth, maturation and cognitive and behavioural development are lacking. The efficacy of sertraline in paediatric patients with depression or panic disorder has not been demonstrated in controlled trials. Safety and effectiveness in paediatric patients below the age of 6 have not been established.
There is limited knowledge with respect to an effect on sexual development in children.
Withdrawal symptoms seen on discontinuation of sertraline treatment Withdrawal symptoms when treatment is discontinued are common, particularly if discontinuation is abrupt (see section 4.8 Undesirable effects).
Discontinuation of SSRIs There is no evidence that SSRIs cause dependence. However, abrupt discontinuation may cause dizziness, paresthesiae, insomnia, headache, nausea, anxiety, sweating and stress, which are mild and transient. Discontinuation should be gradual and under close medical surveillance. The risk of withdrawal symptoms may be dependent on several factors including the duration and dose of therapy and the rate of dose reduction. Dizziness, sensory disturbances (including paraesthesia), sleep disturbances (including insomnia and intense dreams), agitation or anxiety, nausea and/or vomiting, tremor and headache are the most commonly reported reactions. Generally these symptoms are mild to moderate, however, in some patients they may be severe in intensity. They usually occur within the first few days of discontinuing treatment, but there have been very rare reports of such symptoms in patients who have inadvertently missed a dose. Generally these symptoms are self-limiting and usually resolve within 2 weeks, though in some individuals they may be prolonged (2-3 months or more). It is therefore advised that sertraline should be gradually tapered when discontinuing treatment over a period of several weeks or months, according to the patient’s needs (see "Withdrawal symptoms seen on discontinuation of sertraline ", section 4.2 Posology and method of administration). 4.5 Interaction with other medicinal products and other forms of interaction Monoamine oxidase inhibitors See 4.3 ‘Contraindications’.
Centrally active medication Caution is advised if Sertraline 50mg film-coated Tablets are administered with other centrally active medication. In particular, SSRIs have the potential to interact with tricyclic antidepressants leading to an increase in plasma levels of the tricyclic antidepressant. A possible mechanism for this interaction is the inhibitory effect of SSRIs on the CYP2D6 isoenzyme. There is variability among the SSRIs in the extent to which they inhibit the activity of CYP2D6. The clinical significance of this depends on the extent of inhibition and the therapeutic index of the co-administered drug. In formal interaction studies, chronic dosing with sertraline 50mg daily showed minimal elevation (mean 23-37%) of steady state plasma desipramine levels (a marker of CYP2D6 isoenzyme activity). Pimozide – Increased pimozide levels have been demonstrated in a study of a single low dose pimozide (2mg) with sertraline coadministration. These increased levels
UKPAR Egis Pharmaceutical, Sertraline 50mg and 100mg Tablets
17
PL 18190/0011-12
were not associated with any changes in ECG. While the mechanism of this interaction is unknown, due to the narrow therapeutic index of pimozide, concomitant administration of pimozide and sertraline is contra-indicated. Alcohol In 11 healthy subjects administered sertraline (200mg daily) for 9 days, there was no adverse effect on cognitive or psychomotor performance relative to placebo, following a single dose of 500mg/kg alcohol. However, the concomitant use of Sertraline 50mg film-coated Tablets and alcohol in depressed patients is not recommended. Lithium and Tryptophan In placebo-controlled trials in normal volunteers, the co-administration of sertraline and lithium did not significantly alter lithium pharmacokinetics.
Co-administration of sertraline with lithium did result in an increase in tremor relative to placebo, indicating a possible pharmacodynamic interaction. There have been other reports of enhanced effects when SSRIs have been given with lithium or tryptophan and therefore the concomitant use of SSRIs with these drugs should be undertaken with caution. Serotonergic drugs There is limited controlled experience regarding the optimal timing of switching from other antidepressant or antiobsessional drugs to sertraline. Care and prudent medical judgement should be exercised when switching, particularly from long-acting agents. The duration of washout period which should intervene before switching from one selective serotonin re-uptake inhibitor (SSRI) to another has not been established.
Until further data are available, serotonergic drugs, such as tramadol, sumatriptan or fenfluramine, should not be used concomitantly with Sertraline 50mg film-coated Tablets, due to a possible enhancement of 5-HT associated effects. St John's Wort Concomitant use of the herbal remedy St John's wort (Hypericum perforatum) in patients receiving SSRIs should be avoided since there is a possibility of serotonergic potentiation. Drugs that affect platelet function, such as NSAIDs See 4.4 Special warnings and special precautions for use (Haemorrhage). Other drug interactions Since sertraline is bound to plasma proteins, the potential of Sertraline 50mg film-coated Tablets to interact with other plasma protein bound drugs should be borne in mind.
Formal drug interaction studies have been performed with sertraline. Co-administration of sertraline (200mg daily) with diazepam or tolbutamide resulted in small, statistically significant changes in some pharmacokinetic parameters. Co-administration with cimetidine caused a substantial decrease in sertraline clearance. The clinical significance of these changes in unknown. Sertraline had no effect on the beta-adrenergic blocking ability of atenolol. No interaction with sertraline (200mg daily) was observed with glibenclamide or digoxin.
Co-administration of sertraline (200mg daily) with warfarin resulted in a small but statistically significant increase in prothrombin time, the clinical significance of
UKPAR Egis Pharmaceutical, Sertraline 50mg and 100mg Tablets
18
PL 18190/0011-12
which is unknown. Accordingly, prothrombin time should be carefully monitored when Sertraline 50mg film-coated Tablet therapy is initiated or stopped.
Sertraline (200mg daily), did not potentiate the effects of carbamazepine, haloperidol or phenytoin on cognitive and psychomotor performance in healthy subjects. 4.6 Pregnancy and lactation Pregnancy Although animal studies did not provide any evidence of teratogenicity, the safety of sertraline during human pregnancy has not been established. As with all drugs Sertraline 50mg Tablets should only be used in pregnancy if the potential benefits of treatment to the mother outweigh the possible risks to the developing foetus. Lactation Sertraline is known to be excreted in breast milk. Its effects on the nursing infant have not yet been established. If treatment with Sertraline 50mg film-coated Tablets is considered necessary, discontinuation of breast feeding should be considered. 4.7 Effects on ability to drive and use machines Clinical pharmacology studies have shown that sertraline has no effect on psychomotor performance. However, since antidepressant or antiobsessional drugs may impair the abilities required to perform potentially hazardous tasks such as driving a car or operating machinery, the patient should be cautioned accordingly. Sertraline 50mg film-coated Tablets should not be administered with benzodiazepines or other tranquillizers in patients who drive or operate machinery. 4.8 Undesirable effects Side-effects which occurred significantly more frequently with sertraline than placebo in multiple dose studies were: nausea, diarrhoea/loose stools, anorexia, dyspepsia, tremor, dizziness, insomnia, somnolence, increased sweating, dry mouth and sexual dysfunction (mainly ejaculatory delay in males). The side-effect profile commonly observed in double-blind, placebo-controlled studies in patients with OCD and PTSD was similar to that observed in patients with depression. In paediatric OCD patients, side-effects which occurred significantly more frequently with sertraline than placebo were: headache, insomnia, agitation, anorexia, tremor. Most were of mild to moderate severity. Post-marketing spontaneous reports include the following: Cardiovascular Blood pressure disturbances including postural hypotension, tachycardia.
Eye disorders Abnormal vision.
Gastro-intestinal Vomiting, abdominal pain.
UKPAR Egis Pharmaceutical, Sertraline 50mg and 100mg Tablets
19
PL 18190/0011-12
Nervous system Amnesia, headache, drowsiness, movement disorders, paraesthesia, hypoaesthesia, depressive symptoms, hallucinations, aggressive reaction, agitation, anxiety, psychosis, depersonalisation, nervousness, panic reaction and signs and symptoms associated with serotonin syndrome which include fever, rigidity, confusion, agitation, diaphoresis, tachycardia, hypertension and diarrhoea. Rare Psychomotor restlessness/akathisia (see section 4.4 Special warnings and special precautions for use).
There have also been reports of manic reaction, although this phenomenon may be part of the underlying disease.
Convulsions (Seizures) Sertraline 50mg film-coated Tablets should be discontinued in any patient who develops seizures. (See 4.4 ‘Special warnings and special precautions for use’). Musculoskeletal Arthralgia, myalgia. Hepatic/pancreatic Rarely, pancreatitis and serious liver events (including hepatitis, jaundice and liver failure) could occur. Asymptomatic elevation in serum transaminases (SGOT and SGPT) have been reported in association with sertraline administration (0.8-1.3%), with an increased risk associated with the 200mg daily dose. The abnormalities usually occurred within the first 1 to 9 weeks of drug treatment and promptly diminished upon drug discontinuation. Renal and urinary disorders Urinary retention. Reproductive Hyperprolactinaemia, galactorrhoea, menstrual irregularities, anorgasmy. Skin and allergic reactions Rash (including rare reports of erythema multiforme, photosensitivity), angioedema, ecchymoses, pruritus and anaphylactoid reactions. Metabolic Rare cases of hyponatremia have been reported and appeared to be reversible when sertraline was discontinued. Some cases were possibly due to the syndrome of inappropriate antidiuretic hormone secretion. The majority of reports were associated with older patients, and patients taking diuretics or other medications. Haematologic There have been rare reports of altered platelet function and/or abnormal clinical laboratory results in patients taking sertraline. While there have been reports of thrombocytopenia, abnormal bleeding or purpura in several patients taking sertraline, it is unclear whether sertraline had a causative role. (See also 4.4 ‘Special warning and special precautions for use’.) General Malaise. Withdrawal symptoms seen on discontinuation of sertraline treatment Discontinuation of sertraline (particularly when abrupt) commonly leads to withdrawal symptoms. Dizziness, sensory disturbances (including paraesthesia), sleep disturbances (including insomnia and intense dreams), agitation or anxiety, nausea and/or vomiting, tremor and headache are the most commonly reported reactions. Generally these events are mild to moderate and are self-limiting, however, in some
UKPAR Egis Pharmaceutical, Sertraline 50mg and 100mg Tablets
20
PL 18190/0011-12
patients they may be severe and/or prolonged. It is therefore advised that when sertraline treatment is no longer required, gradual discontinuation by dose tapering should be carried out (see section 4.2 Posology and method of administration and section 4.4 Special warnings and special precautions for use). Adverse events from paediatric clinical trials In paediatric clinical trials in depression the following adverse events were reported at a frequency of at least 2% of patients and occurred at a rate of at least twice that of placebo: dry mouth (2.1% vs 0.5 %), hyperkinesia (2.6% vs 0.5%), tremor (2.1% vs 0%), diarrhoea (9.5% vs 1.6%), vomiting (4.2% vs 1.1%) agitation (6.3% vs 1.1%), anorexia (5.3% vs 1.1%) and urinary incontinence (2.1% vs 0%). Suicidal thoughts and suicide attempts were mainly observed in clinical trials with Major Depressive Disorder. 4.9 Overdose On the evidence available, sertraline has a wide margin of safety in overdose. Overdoses of sertraline alone of up to 8g have been reported. Deaths involving overdoses of sertraline in combination with other drugs and/or alcohol have been reported. Therefore, any overdosage should be treated aggressively. Symptoms of overdose include serotonin-mediated side-effects such as somnolence, gastrointestinal disturbances (such as nausea and vomiting), tachycardia, tremor, agitation and dizziness. Less frequently reported was coma. No specific therapy is recommended and there are no specific antidotes to sertraline. Establish and maintain an airway, ensure adequate oxygenation and ventilation. Activated charcoal, which may be used with sorbitol, may be as or more effective than emesis or lavage, and should be considered in treating overdose. Cardiac and vital signs monitoring is recommended along with general symptomatic and supportive measures. Due to the large volume of distribution of sertraline, forced diuresis, dialysis, haemoperfusion and exchange transfusion are unlikely to be of benefit. 5. PHARMACOLOGICAL PROPERTIES 5.1 Pharmacodynamic properties Pharmacotherapeutic group: Selective serotonin reuptake inhibitors ATC Code: N06AB Sertraline is a potent and specific inhibitor of neuronal serotonin (5-HT) uptake both in vitro and in vivo, but is without affinity for muscarinic, serotonergic, dopaminergic, adrenergic, histaminergic, GABA or benzodiazepine receptors. Sertraline is devoid of stimulant, sedative, anticholinergic activity or cardiotoxicity in animals.
UKPAR Egis Pharmaceutical, Sertraline 50mg and 100mg Tablets
21
PL 18190/0011-12
Unlike tricyclic antidepressants, no weight gain is observed with sertraline treatment for depression. Sertraline has not been observed to produce physical or psychological dependence. Sertraline has been evaluated in paediatric OCD patients aged 6 to 17 in a 12-week placebo-controlled study. Therapy for paediatric OCD patients (aged 6-12) commenced at 25mg/day increasing to 50mg/day after 1 week. Side-effects which occurred significantly more frequently with sertraline than placebo were: headache, insomnia, agitation (6-12 years), insomnia, anorexia, tremor (13-17 years). There is limited evidence of efficacy and safety beyond 12 weeks of treatment. 5.2 Pharmacokinetic properties Sertraline exhibits dose proportional pharmacokinetics over a range of 50-200mg. After oral administration of sertraline in man, peak blood levels occur at about 4.5-8.4 hours. Daily doses of sertraline achieve steady-state after one week. Sertraline has a plasma half-life of approximately 26 hours with a mean half-life for young and elderly adults ranging from 22-36 hours. Sertraline is approximately 98% bound to plasma proteins. The principal metabolite, N-desmethylsertraline is inactive in in vivo models of depression and has a half-life of approximately 62-104 hours. Sertraline and N-desmethylsertraline are both extensively metabolised in man and the resultant metabolites excreted in faeces and urine in equal amounts. Only a small amount (<0.2%) of unchanged sertraline is excreted in the urine. The pharmacokinetics of sertraline in paediatric OCD patients have been shown to be comparable with adults (although paediatric patients metabolise sertraline with slightly greater efficiency). However, lower doses may be advisable for paediatric patients given their lower body weights (especially 6-12 years), in order to avoid excessive plasma levels. A clear relationship between sertraline concentration and the magnitude of therapeutic response has not been established. The pharmacokinetics of sertraline in elderly patients are similar to younger adults. Food does not significantly change the bioavailability of sertraline. 5.3 Preclinical safety data Extensive chronic safety evaluation studies in animals show that sertraline is generally well tolerated at doses that are appreciable multiples of those that are clinically effective.
UKPAR Egis Pharmaceutical, Sertraline 50mg and 100mg Tablets
22
PL 18190/0011-12
6. PHARMACEUTICAL PARTICULARS 6.1 List of excipients Sertraline 50mg film-coated Tablets include the following inert ingredients:
Film coating: hypromellose macrogol 6000 titanium dioxide (E171) 6.2 Incompatibilities None known. 6.3 Shelf life 5 years 6.4 Special precautions for storage This medicinal product does not require any special storage conditions.
6.5 Nature and contents of container PVC/PVDC aluminium foil opaque blisters in a cardboard carton containing 28 tablets.
6.6 Special precautions for disposal No special requirements.
UKPAR Egis Pharmaceutical, Sertraline 50mg and 100mg Tablets
23
PL 18190/0011-12
9 DATE OF FIRST AUTHORISATION/RENEWAL OF THE AUTHORISATION
06/12/2006 10 DATE OF REVISION OF THE TEXT
06/12/2006
UKPAR Egis Pharmaceutical, Sertraline 50mg and 100mg Tablets
24
PL 18190/0011-12
SUMMARY OF PRODUCT CHARACTERISTICS
1 NAME OF THE MEDICINAL PRODUCT Sertraline 100mg film-coated Tablets
2 QUALITATIVE AND QUANTITATIVE COMPOSITION Each tablet contains sertraline hydrochloride equivalent to 100mg sertraline. For excipients, see section 6.1
3 PHARMACEUTICAL FORM Film-coated tablet White or almost white, odourless, oval shaped, biconvex film-coated tablets, having stylized E and 272 mark on one side and halving line on the other side. The halving line, or breakline on one face of the tablet allows the tablet to be broken to give a unit dose of 50 mg of sertraline.
4 CLINICAL PARTICULARS
4.1 Therapeutic indications Sertraline 100mg film-coated Tablets are indicated for the treatment of symptoms of depressive illness, including accompanying symptoms of anxiety. Following satisfactory response, continuation with Sertraline 100mg film-coated Tablets therapy is effective in preventing relapse of the initial episode of depression or recurrence of further episodes, including accompanying symptoms of anxiety. Sertraline is also indicated for the treatment of obsessive compulsive disorder (OCD). Following initial response, sertraline has been associated with sustained efficacy, safety and tolerability in up to two years treatment of OCD. Sertraline is also indicated for the treatment of paediatric patients with OCD. Clinical trials in PTSD (post-traumatic stress disorder) demonstrated efficacy in female patients but no evidence of efficacy was seen in males. Treatment with sertraline cannot normally therefore be recommended for male patients with PTSD. A
UKPAR Egis Pharmaceutical, Sertraline 50mg and 100mg Tablets
25
PL 18190/0011-12
therapeutic trial in males might on occasion be justified, but treatment should subsequently be withdrawn unless there is clear evidence of therapeutic benefit. Sertraline is not indicated for use in children and adolescents under the age of 18 years with Major Depressive Disorder. In particular, controlled clinical studies failed to demonstrate efficacy and do not support the use of sertraline in the treatment of children and adolescents with Major Depressive Disorder. (See sections 4.3 Contraindications and 4.8 Undesirable effects).
4.2 Posology and method of administration Sertraline 100mg film-coated Tablets should be given as a single daily dose. Sertraline 100mg film-coated Tablets can be administered with or without food. Adults Depression (including accompanying symptoms of anxiety): The starting dose is 50mg daily and the usual antidepressant dose is 50mg daily. In some patients, doses higher than 50mg may be required. Obsessive Compulsive Disorder: The starting dose is 50mg daily, and the therapeutic dose range is 50-200mg daily.
Post-Traumatic Stress Disorder: Treatment for PTSD should be initiated at 25 mg/day. After one week, the dose should be increased to 50mg once daily. PTSD is a heterogeneous illness and some patient groups fulfilling the criteria for PTSD do not appear to be responsive to treatment with Sertraline 100mg film-coated Tablets. Dosing should be reviewed periodically by the prescribing physician to determine response to therapy and treatment should be withdrawn if there is no clear evidence of efficacy.
Depression (including accompanying symptoms of anxiety), OCD and PTSD: In some patients doses higher than 50mg daily may be required. In patients with incomplete response but good toleration at lower doses, dosage adjustments should be made in 50mg increments over a period of weeks to a maximum of 200mg daily.
Once optimal therapeutic response is achieved the dose should be reduced, depending on therapeutic response, to the lowest effective level. Dosage during prolonged maintenance therapy should be kept at the lowest effective level, with subsequent adjustments depending on therapeutic response. The onset of therapeutic effect may be seen within 7 days, although 2-4 weeks (and even longer in OCD) are usually necessary for full activity. A longer treatment period, even beyond 12 weeks in some cases, may be required in the case of a therapeutic trial in PTSD. Use in children aged 6-17 years Treatment should only be initiated by specialists. The safety and efficacy of sertraline has been established in paediatric OCD patients (aged 6-17). The administration of sertraline to paediatric OCD patients (aged 13-17) should commence at 50mg/day. Therapy for paediatric OCD patients (aged 6-12) should commence at 25mg/day increasing to 50mg/day after 1 week. Subsequent doses may be increased in case of lack of response in 50mg/day increments up to
UKPAR Egis Pharmaceutical, Sertraline 50mg and 100mg Tablets
26
PL 18190/0011-12
200mg/day as needed. However, the generally lower body weights of children compared to adults should be taken into consideration in advancing the dose from 50mg, in order to avoid excessive dosing. Given the 24 hour elimination half-life of sertraline, dose changes should not occur at intervals of less than 1 week. The efficacy and safety of sertraline in children and adolescents under the age of 18 years with Major Depressive Disorder have not been established. Controlled clinical studies failed to demonstrate efficacy and do not support the use of sertraline in the treatment of children and adolescents with Major Depressive Disorder (See sections 4.3 Contraindications and 4.8 Undesirable effects.) Children aged less than six years Sertraline is not recommended in children under six years of age since safety and efficacy have not been established. See also 5.1 'Pharmacological Properties'. Use in the elderly No special precautions are required. The usual adult dose is recommended. Several hundred elderly patients have participated in clinical studies with sertraline. The pattern and incidence of adverse reactions in the elderly is similar to that in younger patients. Withdrawal symptoms seen on discontinuation of sertraline Abrupt discontinuation should be avoided. When stopping treatment with sertraline the dose should be gradually reduced over a period of at least one to two weeks in order to reduce the risk of withdrawal reactions (see section 4.4 Special warnings and special precautions for use and section 4.8 Undesirable Effects). If intolerable symptoms occur following a decrease in the dose or upon discontinuation of treatment, then resuming the previously prescribed dose may be considered. Subsequently, the physician may continue decreasing the dose, but at a more gradual rate.
Sertraline 100mg film-coated Tablets are for oral administration only.
4.3 Contraindications Sertraline 100mg film-coated tablets are contra-indicated in patients with a known hypersensitivity to sertraline. Monoamine oxidase inhibitors: Cases of serious and sometimes fatal reactions have been reported in patients receiving an SSRI in combination with a monoamine oxidase inhibitor (MAOI), including the selective MAOI selegiline and reversible MAOI (RIMA) moclobemide and in patients who have recently discontinued an SSRI and have been started on a MAOI. Some cases presented with features resembling serotonin syndrome. Symptoms of a drug interaction with a MAOI include: hyperthermia, rigidity, myoclonus, autonomic instability with possible rapid fluctuations of vital signs, mental status changes that include confusion, irritability and extreme agitation progressing to delirium and coma. Sertraline 100mg film-coated Tablets should not be used in combination with a MAOI. Sertraline 100mg film-coated Tablets may be started 14 days after discontinuing treatment with an irreversible MAOI and at least one day after
UKPAR Egis Pharmaceutical, Sertraline 50mg and 100mg Tablets
27
PL 18190/0011-12
discontinuing treatment with the reversible MAOI (RIMA), moclobemide. At least 14 days should elapse after discontinuing Sertraline 100mg film-coated Tablets treatment before starting a MAOI or RIMA. Use in hepatic impairment There is insufficient clinical experience in patients with significant hepatic dysfunction and accordingly Sertraline 100mg film-coated Tablets should not be used in such patients. Concomitant use in patients taking pimozide is contra-indicated (see section 4.5 Interaction with other medicinal products and other forms of interaction). Sertraline should not be used in children and adolescents under the age of 18 years with Major Depressive Disorder. (See section 4.8 Undesirable effects.)
4.4 Special warnings and precautions for use Monoamine oxidase inhibitors See 4.3 ‘Contraindications’.
Use in patients with renal or hepatic impairment As with many other medications, sertraline should be used with caution in patients with renal and hepatic impairment (see 4.3 ‘Contraindications’).
Since sertraline is extensively metabolised, excretion of unchanged drug in urine is a minor route of elimination. In patients with mild to moderate renal impairment (creatinine clearance 20-50 ml/min) or severe renal impairment (creatinine clearance <20 ml/min), single dose pharmacokinetic parameters were not significantly different compared with controls. However, steady state pharmacokinetics of sertraline have not been adequately studied in this patient population and caution is advised when treating patients with renal impairment.
Sertraline is extensively metabolised by the liver. A multiple dose pharmacokinetic study in subjects with mild, stable cirrhosis demonstrated a prolonged elimination half-life and approximately three-fold greater AUC and Cmax in comparison with normal subjects. There were no significant differences in plasma protein binding observed between the two groups. The use of sertraline in patients with hepatic disease should be approached with caution. A lower or less frequent dose should be used in patients with hepatic impairment.
Diabetes In patients with diabetes, treatment with an SSRI may alter glycaemic control, possibly due to improvement of depressive symptoms. Insulin and/or oral hypoglycaemic dosage may be needed to be adjusted. Seizures Seizures are a potential risk with antidepressant or antiobsessional drugs. The drug should be discontinued in any patient who develops seizures. Sertraline 100mg film-coated Tablets should be avoided in patients with unstable epilepsy and patients with controlled epilepsy should be carefully monitored. Sertraline 100mg film-coated Tablets should be discontinued if there is an increase in seizure frequency. Electroconvulsive therapy (ECT) Since there is little clinical experience of concurrent administration of sertraline and ECT, caution is advisable.
UKPAR Egis Pharmaceutical, Sertraline 50mg and 100mg Tablets
28
PL 18190/0011-12
Mania Sertraline 100mg film-coated Tablets should be used with caution in patients with a history of mania/hypomania. Sertraline 100mg film-coated Tablets should be discontinued in any patient entering a manic phase. Suicide/suicidal thoughts Depression is associated with an increased risk of suicidal thoughts, self harm and suicide (suicide-related events). This risk persists until significant remission occurs. As improvement may not occur during the first few weeks or more of treatment, patients should be closely monitored until such improvement occurs. It is general clinical experience that the risk of self harm is highest shortly after presentation and the risk of suicide may increase again in the early stages of recovery. Furthermore, there is evidence that in a small group of people, antidepressants may increase the risk of suicidal thoughts and self-harm. Other psychiatric conditions for which sertraline is prescribed can also be associated with an increased risk of suicide-related events. In addition, these conditions may be co-morbid with major depressive disorder. The same precautions observed when treating patients with major depressive disorder should therefore be observed when treating patients with other psychiatric disorders. Patients with a history of suicide-related events, those exhibiting a significant degree of suicidal ideation prior to commencement of treatment, and young adults, are at a greater risk of suicidal thoughts or suicide attempts, and should receive careful monitoring during treatment. Patients, (and caregivers of patients) should be alerted about the need to monitor for the emergence of suicidal thoughts and to seek medical advice immediately if these symptoms present. Haemorrhage There have been reports of cutaneous bleeding abnormalities such as ecchyimoses and purpura with SSRIs.
Caution is advised in patients taking SSRIs, particularly in concomitant use with drugs known to affect platelet function (e.g. atypical antipsychotics and phenothiazines, most tricyclic antidepressants, aspirin and non-steroidal anti-inflammatory drugs (NSAIDs) as well as in patients with a history of bleeding disorders.
Psychomotor restlessness The use of sertraline has been associated with the development of psychomotor restlessness, which clinically may be very similar to akathisia, characterised by a subjectively unpleasant or distressing restlessness and need to move often accompanied by an inability to sit or stand still. This is most likely to occur within the first few weeks of treatment. In patients who develop these symptoms, increasing the dose may be detrimental and it may be necessary to review the use of sertraline. Use in the elderly Several hundred elderly patients have participated in clinical studies with sertraline. The pattern and incidence of adverse reactions in the elderly is similar to that in younger patients. Use in Children and adolescents under 18 years of age Sertraline 100mg film-coated Tablets should not be used in the treatment of children and adolescents under the age of 18 years, except for patients with Obsessive Compulsive Disorder. Suicide-related behaviours (suicide attempt and suicidal thoughts), and hostility
UKPAR Egis Pharmaceutical, Sertraline 50mg and 100mg Tablets
29
PL 18190/0011-12
(predominantly aggression, oppositional behaviour and anger) were more frequently observed in clinical trials and adolescents treated with antidepressants compared to those treated with placebo. If, based on clinical need, a decision to treat is nevertheless taken, the patient should be carefully monitored for the appearance of suicidal symptoms. In addition, long-term safety data in children and adolescents concerning growth, maturation and cognitive and behavioural development are lacking. The efficacy of sertraline in paediatric patients with depression or panic disorder has not been demonstrated in controlled trials. Safety and effectiveness in paediatric patients below the age of 6 have not been established.
There is limited knowledge with respect to an effect on sexual development in children.
Withdrawal symptoms seen on discontinuation of sertraline treatment Withdrawal symptoms when treatment is discontinued are common, particularly if discontinuation is abrupt (see section 4.8 Undesirable effects). Discontinuation of SSRIs There is no evidence that SSRIs cause dependence. However, abrupt discontinuation may cause dizziness, paresthesiae, insomnia, headache, nausea, anxiety, sweating and stress, which are mild and transient. Discontinuation should be gradual and under close medical surveillance. The risk of withdrawal symptoms may be dependent on several factors including the duration and dose of therapy and the rate of dose reduction. Dizziness, sensory disturbances (including paraesthesia), sleep disturbances (including insomnia and intense dreams), agitation or anxiety, nausea and/or vomiting, tremor and headache are the most commonly reported reactions. Generally these symptoms are mild to moderate, however, in some patients they may be severe in intensity. They usually occur within the first few days of discontinuing treatment, but there have been very rare reports of such symptoms in patients who have inadvertently missed a dose. Generally these symptoms are self-limiting and usually resolve within 2 weeks, though in some individuals they may be prolonged (2-3 months or more). It is therefore advised that sertraline should be gradually tapered when discontinuing treatment over a period of several weeks or months, according to the patient’s needs (see "Withdrawal symptoms seen on discontinuation of sertraline ", section 4.2 Posology and method of administration).
4.5 Interaction with other medicinal products and other forms of interaction Monoamine oxidase inhibitors See 4.3 ‘Contraindications’. Centrally active medication Caution is advised if Sertraline 100mg film-coated Tablets are administered with other centrally active medication. In particular, SSRIs have the potential to interact with tricyclic antidepressants leading to an increase in plasma levels of the tricyclic antidepressant. A possible mechanism for this interaction is the inhibitory effect of SSRIs on the CYP2D6 izoenzyme. There is variability among the SSRIs in the extent to which they inhibit the activity of CYP2D6. The clinical significance of this depends on the extent of inhibition and the
UKPAR Egis Pharmaceutical, Sertraline 50mg and 100mg Tablets
30
PL 18190/0011-12
therapeutic index of the co-administered drug. In formal interaction studies, chronic dosing with sertraline 50mg daily showed minimal elevation (mean 23-37%) of steady state plasma desipramine levels (a marker of CYP2D6 isoenzyme activity). Pimozide – Increased pimozide levels have been demonstrated in a study of a single low dose pimozide (2mg) with sertraline coadministration. These increased levels were not associated with any changes in ECG. While the mechanism of this interaction is unknown, due to the narrow therapeutic index of pimozide, concomitant administration of pimozide and sertraline is contra-indicated. Alcohol In 11 healthy subjects administered sertraline (200mg daily) for 9 days, there was no adverse effect on cognitive or psychomotor performance relative to placebo, following a single dose of 500mg/kg alcohol. However, the concomitant use of Sertraline 100mg film-coated Tablets and alcohol in depressed patients is not recommended. Lithium and Tryptophan In placebo-controlled trials in normal volunteers, the co-administration of sertraline and lithium did not significantly alter lithium pharmacokinetics.
Co-administration of sertraline with lithium did result in an increase in tremor relative to placebo, indicating a possible pharmacodynamic interaction. There have been other reports of enhanced effects when SSRIs have been given with lithium or tryptophan and therefore the concomitant use of SSRIs with these drugs should be undertaken with caution. Serotonergic drugs There is limited controlled experience regarding the optimal timing of switching from other antidepressant or antiobsessional drugs to sertraline. Care and prudent medical judgement should be exercised when switching, particularly from long-acting agents. The duration of washout period which should intervene before switching from one selective serotonin re-uptake inhibitor (SSRI) to another has not been established.
Until further data are available, serotonergic drugs, such as tramadol, sumatriptan or fenfluramine, should not be used concomitantly with Sertraline 100mg film-coated Tablets, due to a possible enhancement of 5-HT associated effects. St John's Wort Concomitant use of the herbal remedy St John's wort (Hypericum perforatum) in patients receiving SSRIs should be avoided since there is a possibility of serotonergic potentiation. Drugs that affect platelet function, such as NSAIDs See 4.4 Special warnings and special precautions for use (Haemorrhage). Other drug interactions Since sertraline is bound to plasma proteins, the potential of Sertraline 100mg film-coated Tablets to interact with other plasma protein bound drugs should be borne in mind.
Formal drug interaction studies have been performed with sertraline. Co-administration of sertraline (200mg daily) with diazepam or tolbutamide resulted in small, statistically significant changes in some pharmacokinetic parameters. Co-administration with cimetidine caused a substantial decrease in sertraline clearance.
UKPAR Egis Pharmaceutical, Sertraline 50mg and 100mg Tablets
31
PL 18190/0011-12
The clinical significance of these changes in unknown. Sertraline had no effect on the beta-adrenergic blocking ability of atenolol. No interaction with sertraline (200mg daily) was observed with glibenclamide or digoxin.
Co-administration of sertraline (200mg daily) with warfarin resulted in a small but statistically significant increase in prothrombin time, the clinical significance of which is unknown. Accordingly, prothrombin time should be carefully monitored when Sertraline 100mg film-coated Tablet therapy is initiated or stopped.
Sertraline (200mg daily), did not potentiate the effects of carbamazepine, haloperidol or phenytoin on cognitive and psychomotor performance in healthy subjects.
4.6 Pregnancy and lactation Pregnancy Although animal studies did not provide any evidence of teratogenicity, the safety of sertraline during human pregnancy has not been established. As with all drugs Sertraline 100mg Tablets should only be used in pregnancy if the potential benefits of treatment to the mother outweigh the possible risks to the developing foetus. Lactation Sertraline is known to be excreted in breast milk. Its effects on the nursing infant have not yet been established. If treatment with Sertraline 100mg film-coated Tablets is considered necessary, discontinuation of breast feeding should be considered.
4.7 Effects on ability to drive and use machines Clinical pharmacology studies have shown that sertraline has no effect on psychomotor performance. However, since antidepressant or antiobsessional drugs may impair the abilities required to perform potentially hazardous tasks such as driving a car or operating machinery, the patient should be cautioned accordingly. Sertraline 100mg film-coated Tablets should not be administered with benzodiazepines or other tranquillizers in patients who drive or operate machinery.
4.8 Undesirable effects Side-effects which occurred significantly more frequently with sertraline than placebo in multiple dose studies were: nausea, diarrhoea/loose stools, anorexia, dyspepsia, tremor, dizziness, insomnia, somnolence, increased sweating, dry mouth and sexual dysfunction (mainly ejaculatory delay in males). The side-effect profile commonly observed in double-blind, placebo-controlled studies in patients with OCD and PTSD was similar to that observed in patients with depression. In paediatric OCD patients, side-effects which occurred significantly more frequently with sertraline than placebo were: headache, insomnia, agitation, anorexia, tremor. Most were of mild to moderate severity. Post-marketing spontaneous reports include the following:
UKPAR Egis Pharmaceutical, Sertraline 50mg and 100mg Tablets
32
PL 18190/0011-12
Cardiovascular Blood pressure disturbances including postural hypotension, tachycardia.
Eye disorders Abnormal vision.
Gastro-intestinal Vomiting, abdominal pain.
Nervous system Amnesia, headache, drowsiness, movement disorders, paraesthesia, hypoaesthesia, depressive symptoms, hallucinations, aggressive reaction, agitation, anxiety, psychosis, depersonalisation, nervousness, panic reaction and signs and symptoms associated with serotonin syndrome which include fever, rigidity, confusion, agitation, diaphoresis, tachycardia, hypertension and diarrhoea. Rare Psychomotor restlessness/akathisia (see section 4.4 Special warnings and special precautions for use)
There have also been reports of manic reaction, although this phenomenon may be part of the underlying disease.
Convulsions (Seizures) Sertraline 100mg film-coated Tablets should be discontinued in any patient who develops seizures. (See 4.4 ‘Special warnings and special precautions for use’). Musculoskeletal Arthralgia, myalgia. Hepatic/pancreatic Rarely, pancreatitis and serious liver events (including hepatitis, jaundice and liver failure) could occur. Asymptomatic elevation of in serum transaminases (SGOT and SGPT) have been reported in association with sertraline administration (0.8-1.3%), with an increased risk associated with the 200mg daily dose. The abnormalities usually occurred within the first 1 to 9 weeks of drug treatment and promptly diminished upon drug discontinuation. Renal and urinary disorders Urinary retention. Reproductive Hyperprolactinaemia, galactorrhoea, menstrual irregularities, anorgasmy. Skin and allergic reactions Rash (including rare reports of erythema multiforme, photosensitivity), angioedema, ecchymoses, pruritus and anaphylactoid reactions. Metabolic Rare cases of hyponatremia have been reported and appeared to be reversible when sertraline was discontinued. Some cases were possibly due to the syndrome of inappropriate antidiuretic hormone secretion. The majority of reports were associated with older patients, and patients taking diuretics or other medications. Haematologic There have been rare reports of altered platelet function and/or abnormal clinical laboratory results in patients taking sertraline. While there have been reports of thrombocytopenia, abnormal bleeding or purpura in several patients taking sertraline, it is unclear whether sertraline had a causative role. See also 4.4 ‘Special warning and special precautions for use’. General Malaise. Withdrawal symptoms seen on discontinuation of sertraline treatment Discontinuation of sertraline (particularly when abrupt) commonly leads to
UKPAR Egis Pharmaceutical, Sertraline 50mg and 100mg Tablets
33
PL 18190/0011-12
withdrawal symptoms. Dizziness, sensory disturbances (including paraesthesia), sleep disturbances (including insomnia and intense dreams), agitation or anxiety, nausea and/or vomiting, tremor and headache are the most commonly reported reactions. Generally these events are mild to moderate and are self-limiting, however, in some patients they may be severe and/or prolonged. It is therefore advised that when sertraline treatment is no longer required, gradual discontinuation by dose tapering should be carried out (see section 4.2 Posology and method of administration and section 4.4 Special warnings and special precautions for use). Adverse events from paediatric clinical trials In paediatric clinical trials in depression the following adverse events were reported at a frequency of at least 2% of patients and occurred at a rate of at least twice that of placebo: dry mouth (2.1% vs 0.5 %), hyperkinesia (2.6% vs 0.5%), tremor (2.1% vs 0%), diarrhoea (9.5% vs 1.6%), vomiting (4.2% vs 1.1%) agitation (6.3% vs 1.1%), anorexia (5.3% vs 1.1%) and urinary incontinence (2.1% vs 0%). Suicidal thoughts and suicide attempts were mainly observed in clinical trials with Major Depressive Disorder.
4.9 Overdose On the evidence available, sertraline has a wide margin of safety in overdose. Overdoses of sertraline alone of up to 8g have been reported. Deaths involving overdoses of sertraline in combination with other drugs and/or alcohol have been reported. Therefore, any overdosage should be treated aggressively. Symptoms of overdose include serotonin-mediated side-effects such as somnolence, gastrointestinal disturbances (such as nausea and vomiting), tachycardia, tremor, agitation and dizziness. Less frequently reported was coma. No specific therapy is recommended and there are no specific antidotes to sertraline. Establish and maintain an airway, ensure adequate oxygenation and ventilation. Activated charcoal, which may be used with sorbitol, may be as or more effective than emesis or lavage, and should be considered in treating overdose. Cardiac and vital signs monitoring is recommended along with general symptomatic and supportive measures. Due to the large volume of distribution of sertraline, forced diuresis, dialysis, haemoperfusion and exchange transfusion are unlikely to be of benefit.
5 PHARMACOLOGICAL PROPERTIES
5.1 Pharmacodynamic properties Pharmacotherapeutic group: Selective serotonin reuptake inhibitors ATC Code: N06AB Sertraline is a potent and specific inhibitor of neuronal serotonin (5-HT) uptake both in vitro and in vivo, but is without affinity for muscarinic, serotonergic, dopaminergic, adrenergic, histaminergic, GABA or benzodiazepine receptors.
UKPAR Egis Pharmaceutical, Sertraline 50mg and 100mg Tablets
34
PL 18190/0011-12
Sertraline is devoid of stimulant, sedative, anticholinergic activity or cardiotoxicity in animals. Unlike tricyclic antidepressants, no weight gain is observed with sertraline treatment for depression. Sertraline has not been observed to produce physical or psychological dependence. Sertraline has been evaluated in paediatric OCD patients aged 6 to 17 in a 12-week placebo-controlled study. Therapy for paediatric OCD patients (aged 6-12) commenced at 25mg/day increasing to 50mg/day after 1 week. Side-effects which occurred significantly more frequently with sertraline than placebo were: headache, insomnia, agitation (6-12 years), insomnia, anorexia, tremor (13-17 years). There is limited evidence of efficacy and safety beyond 12 weeks of treatment.
5.2 Pharmacokinetic properties Sertraline exhibits dose proportional pharmacokinetics over a range of 50-200mg. After oral administration of sertraline in man, peak blood levels occur at about 4.5-8.4 hours. Daily doses of sertraline achieve steady-state after one week. Sertraline has a plasma half-life of approximately 26 hours with a mean half-life for young and elderly adults ranging from 22-36 hours. Sertraline is approximately 98% bound to plasma proteins. The principal metabolite, N-desmethylsertraline is inactive in in vivo models of depression and has a half-life of approximately 62-104 hours. Sertraline and N-desmethylsertraline are both extensively metabolised in man and the resultant metabolites excreted in faeces and urine in equal amounts. Only a small amount (<0.2%) of unchanged sertraline is excreted in the urine. The pharmacokinetics of sertraline in paediatric OCD patients have been shown to be comparable with adults (although paediatric patients metabolise sertraline with slightly greater efficiency). However, lower doses may be advisable for paediatric patients given their lower body weights (especially 6-12 years), in order to avoid excessive plasma levels. A clear relationship between sertraline concentration and the magnitude of therapeutic response has not been established. The pharmacokinetics of sertraline in elderly patients are similar to younger adults. Food does not significantly change the bioavailability of sertraline.
5.3 Preclinical safety data Extensive chronic safety evaluation studies in animals show that sertraline is generally well tolerated at doses that are appreciable multiples of those that are clinically effective.
6 PHARMACEUTICAL PARTICULARS
UKPAR Egis Pharmaceutical, Sertraline 50mg and 100mg Tablets
35
PL 18190/0011-12
6.1 List of excipients Sertraline 100mg film-coated Tablets include the following inert ingredients: