Serum Calcitonin-Lowering Effect of Magnesium in Patients with Medullary Carcinoma of the Thyroid CONSTANTINE ANAST, Louis DAVID, JOHN WINNAcKER, ROBERT GLASS, WILLIAM BASKIN, LEONARD BRUBAKER, and THOMAS BURNS From the Division of Endocrinology, Departments of Child Health and Medicine, School of Medicine, University of Missouri and Veterans Administration Hospital, Columbia, Missouri 65201 A B S T R A C T The effect of magnesium chloride or magnesium sulfate infusion on circulating levels of im- munoreactive calcitonin (iCT) was evaluated on nine occasions in three patients with metastatic medullary carcinoma of the thyroid. One patient was normocal- cemic and had normal circulating levels of immunoreac- tive parathyroid hormone (iPTH), one patient was hy- pocalcemic and had surgical hypoparathyroidism, and one patient had mild to moderate hypercalcemia associ- ated with bone metastases. The basal serum iPTH lev- els were undetectable in the latter two patients. In every instance magnesium administration produced a rapid and striking fall in circulating iCT and usually a de- tectable fall in serum calcium. During the hypermag- nesemic state, serum iPTH fell from normal to un- detectable in the patient with normal parathyroid func- tion, while serum iPTH levels remained undetectable in the hypoparathyroid patient and in the patient with hypercalcemia associated with bone metastases. The re- sults of these studies indicate that: (a) contrary to what has been reported in normal experimental animals, magnesium administration lowers circulating iCT in human subjects with thyroid medullary carcinoma and (b) the calcium-lowering effect produced by magnesium in patients with medullary carcinoma may, in part at least, be due to a redistribution of body calcium that is not mediated by the actions of either parathyroid hor- mone or calcitonin. INTRODUCTION It has been well established that the secretion of calci- tonin is under the control of the blood calcium level A preliminary report of this research was presented at the 48th Annual Meeting of the Central Society for Clinical Research, November 1974. Received for publication 10 June 1975 and in revised form 18 August 1975. with hypercalcemia stimulating the release of this hor- mone from the thyroid gland. There are many similari- ties, both biological and chemical, between magnesium and calcium and the possibility that magnesium might influence calcitonin secretion has, therefore, been stud- ied in experimental animals by several investigators. The reports of in vitro, in situ, and in vivo animal stud- ies all indicate that magnesium, like calcium, stimulates the release of calcitonin from the thyroid gland (1-4). Moreover, on the basis of the results of the in vivo stud- ies, it has been suggested that the characteristic hypo- calcemic effect produced by magnesium administration is the result of magnesium-induced release of calcitonin. In normal man, the serum concentration of calcitonin is low and, because of methodologic problems, difficult to quantify. Therefore, the secretion of calcitonin in human subjects has been most extensively studied in pa- tients with medullary carcinoma of the thyroid, who characteristically have high circulating levels of the hormone. Similar to what has been observed in normal experimental animals, the administration of calcium in- creases the serum calcitonin concentration in these patients. However, there is little information concerning the possible interrelationship of magnesium and calci- tonin in man. The purpose of the present investigation was to study the effect of magnesium administration on circulating levels of calcitonin in patients with medullary carcinoma of the thyroid. Much to our surprise and in direct contrast to the reported studies in normal labora- tory animals, we found that experimentally-induced hy- permagnesemia consistently produced a rapid and strik- ing fall in the serum calcitonin concentration in these patients. METHODS Laboratory methods Serum and urine calcium and magnesium were deter- mined by atomic absorption spectrophotometry (model 303 The Journal of Clinical Investigation Volume 56 December 1975-1615-1621 1615
Transcript
Serum Calcitonin-Lowering Effect of Magnesium in Patients
with Medullary Carcinoma of the Thyroid
CONSTANTINEANAST, Louis DAVID, JOHNWINNAcKER, ROBERTGLASS,WILLIAM BASKIN, LEONARDBRUBAKER,and THOMASBURNS
From the Division of Endocrinology, Departments of Child Health andMedicine, School of Medicine, University of Missouri and VeteransAdministration Hospital, Columbia, Missouri 65201
A B S T R A C T The effect of magnesium chloride ormagnesium sulfate infusion on circulating levels of im-munoreactive calcitonin (iCT) was evaluated on nineoccasions in three patients with metastatic medullarycarcinoma of the thyroid. One patient was normocal-cemic and had normal circulating levels of immunoreac-tive parathyroid hormone (iPTH), one patient was hy-pocalcemic and had surgical hypoparathyroidism, andone patient had mild to moderate hypercalcemia associ-ated with bone metastases. The basal serum iPTH lev-els were undetectable in the latter two patients. In everyinstance magnesium administration produced a rapidand striking fall in circulating iCT and usually a de-tectable fall in serum calcium. During the hypermag-nesemic state, serum iPTH fell from normal to un-detectable in the patient with normal parathyroid func-tion, while serum iPTH levels remained undetectablein the hypoparathyroid patient and in the patient withhypercalcemia associated with bone metastases. The re-sults of these studies indicate that: (a) contrary towhat has been reported in normal experimental animals,magnesium administration lowers circulating iCT inhuman subjects with thyroid medullary carcinoma and(b) the calcium-lowering effect produced by magnesiumin patients with medullary carcinoma may, in part atleast, be due to a redistribution of body calcium that isnot mediated by the actions of either parathyroid hor-mone or calcitonin.
INTRODUCTIONIt has been well established that the secretion of calci-tonin is under the control of the blood calcium level
A preliminary report of this research was presented atthe 48th Annual Meeting of the Central Society for ClinicalResearch, November 1974.
Received for publication 10 June 1975 and in revised form18 August 1975.
with hypercalcemia stimulating the release of this hor-mone from the thyroid gland. There are many similari-ties, both biological and chemical, between magnesiumand calcium and the possibility that magnesium mightinfluence calcitonin secretion has, therefore, been stud-ied in experimental animals by several investigators.The reports of in vitro, in situ, and in vivo animal stud-ies all indicate that magnesium, like calcium, stimulatesthe release of calcitonin from the thyroid gland (1-4).Moreover, on the basis of the results of the in vivo stud-ies, it has been suggested that the characteristic hypo-calcemic effect produced by magnesium administration isthe result of magnesium-induced release of calcitonin.
In normal man, the serum concentration of calcitoninis low and, because of methodologic problems, difficultto quantify. Therefore, the secretion of calcitonin inhuman subjects has been most extensively studied in pa-tients with medullary carcinoma of the thyroid, whocharacteristically have high circulating levels of thehormone. Similar to what has been observed in normalexperimental animals, the administration of calcium in-creases the serum calcitonin concentration in thesepatients. However, there is little information concerningthe possible interrelationship of magnesium and calci-tonin in man. The purpose of the present investigationwas to study the effect of magnesium administration oncirculating levels of calcitonin in patients with medullarycarcinoma of the thyroid. Much to our surprise and indirect contrast to the reported studies in normal labora-tory animals, we found that experimentally-induced hy-permagnesemia consistently produced a rapid and strik-ing fall in the serum calcitonin concentration in thesepatients.
METHODS
Laboratory methods
Serum and urine calcium and magnesium were deter-mined by atomic absorption spectrophotometry (model 303
The Journal of Clinical Investigation Volume 56 December 1975-1615-1621 1615
spectrophotomieter, Perkin-Elnmer Corp., Norwalk, Coini.)anid inorganic phosphorus by thec metlhod of Fiske and(I Sub-barow adapted to the Technico n AnutoA\nalyzer (TechlniconInstruments Corp., Tarrytown, N. Y.) (5). Seruiml levelsof immunoreactive parathvroidl horiimonie (iPTH) ' were(letermined by a double-antihody radlioinmmunoassay teclh-niq(ute develol)edl in our laboratory (6). IhuImiani hyperpara-tllyroi(l seruiml is used as a referenice stanl(lar(d in the assayand( the coinceintrationl of iPTH in unlk;nown serumil samlplesis expressed as microliter equivalents of stanidard hyper-parathyroid serum per milliliter (jt eq/mil) ; normlal valuesrange from undetectable to 10 Al eq/mIil.
Serum immunoreactive calcitoniin (iCT) was measuredby an immunoassay procedure develope(d in our laboratory.Synthetic human calcitonini 'M is labeled with "II at specificradioactivities of 250-500 jsCi/,ug and purified hy adsorbingto Quso G 32 (Philadelphia Quartz Co., Philadelphia, Pa.)followed by elution with a solution of 20% acetone-1%acetic acid. The incubation buffer is Tris buffer 0.5 'M atpH 7.8. The final incubation mixture is 500 Ml and coni-tains 100 ,ul of either standard or unkniow-ni serumi, anti-serum at a final concentratioin of 1: 20,000, 33I-labeled cal-citonin, and buffer. The antiserum to humani calcitoninii wasmade by injecting rabbits with syntlhetic lhumani calcitoninM1. A nonequilibrium incubation systeml is used in whichthe unlabeled standard humiiani calcitonini or unkniown serumiisamples are preincubated at 4°C with antiserum for 3 daysand then with labeled calcitoninl for an additional 3-4 days.After incubation, free and bound calcitonin 1311 are sepa-rated by dextran-charcoal. The supernate and precipitateof each standard and unkniown sample are counted in agamma counter and a bound-to-free ratio is calculated.
It has been demonstrated that serum samples can pro-duce nonspecific displacement of tracer from antibody inthe calcitonin immunoassay procedure (7). Therefore, toeliminate or minimize this artifact, calcitonin concenitrationwas determined in the serum samples before and aftercharcoal adsorption, according to the procedure describedby Deftos (7). In the serum samples obtained in thisstudy the calculated iCT conlcentrationis wvere 2-18%o low-erafter thle addition of charcoal. Quantitatively, the effect pro-(Iiced by the apparent interferinig sulbstanices on the im-munoassay determinationi of calcitonin x-as relatively coIn-stant in variouis serumil samples obtained from ani- onepatient.
With our immiiunioassay procedure the concenitrationi ofserum iCT in normiial clildreni an(l a(dults ranges fromundetectable in most subjects (< 0.1 ng/miil) to less than 0.2ng/ml. The intraassay variation is less tllan 8% whlile theinterassay variation is less thanl 157c. Sequential serumsamples obtained in each of the study periods to be de-scribed were always analyzed in the same assay, thus elimi-nating the effect of interassay variation.
Paticent 1, a 64-yr-old (60-kg) white male librarian, hada total thyroidectomy and radical neck dissection 3 yr be-fore the study. Histological studies revealed medullary car-cinoma of the thyroid with cervical lymph node metastases.In addition, there was evidence of liver and pulmonarymetastases. Postoperatively he developed hypocalcemia andthe diagnosis of surgical hypoparathyroidism was made.The serum iCT concentration on admission was 11.6 ng/ml.The serum calcium level was 7.0 mg/100 ml, serum mag-nesium 1.8 mg/100 ml, and serum phosphorus 5.9 mg/100ml. The serum iPTH was undetectable.
'Abbrcviationis utsed in this paper: iCT, immunoreactivecalcitonint; iPTH, immunoreactive parathyroid hormone.
PatiCezt 2, a 74-yr-old (44-kg) white lhousewife, lhad a
total thyroilectomy ani( radical neck (lissectioni 18 mo beforethe study. Histological studies revealed medullarv carcinoimiaof the thyroid wxitlh cerxvical lymph i no(le metastases. Tlher-ewas evidence of liver imietastases as well as mietastatic boiill(lisease as rexvealed b1 lvtic lesiolns of tIle calvatriumn all(lX-ray clhaniges in the (lorsal and( lumbar spine. The serumiCT level On a(illliss:oll was 138 ng/nll. The serunll calcium
level was 11.2 img/100 mil, serumii iulagliesiunll 1.8 mig/100 m1l,and serunl phllospllorus 3.4 mg/10( n1l. TLhe serum i PTH wasun(letectable.
Pttlwiot 3, a 50-yr-old (65-klg) white housewife, Iladmedullary carciniomiia of tIle thyroid with cervical lymph
node metastases. The left lobe of the tllyroid was removed3 yr anil the rigllt lobe 1 year before the study. On ad-IlmissioIn the sernii iCT was 0.89 ilg/ill, serunil calcium9.50 mg/100 nil, serumn magnesium 2.1 mg/100 ml, aiidserum phospllorus 3.8 illg/100 ml. Tile serum iPTH levelwas 9.0 ,ul eq/ml.
In sumnmary, the three patients of tllis study wvere similarill that eacll hlad hlad a dllyroidectomy follow ed by clinicalevidence of metastases andcl persistellce of elevated serumiCT levels. In eacll the seruimi sodium, potassium, bicarbon-ate. clllori(le, and bloodl urea nitrogen were within normallimits. TIle patients differed in the following respects:(a) patienit 1 developed hlypocalcemnia with un(letectablelevels of serunl iPTH after thyroid surgery alld xvas coil-sidered to have surgical hypoparathyroidism; (b) patient 2lhad hypercalcemia associated witlh the radiologic evidenceof metastatic boile disease and undetectable levels of serumiPTH and (c) patieilt 3 x-as nornllocalcemic aild base-linieiPTH levels wvere within the nornl-lal ranige.
Magnesium infusion procedureAll subjects studie(d were lhospitalized OIn the ward of
the Clinical Research Center. The protocols followed wereapproved by the institution's Committee for Projects Ini-volvinig Human Subjects. The study was explained to each
sul)ject and written conseilt obtained.The IpatienIts receivedl a regular (iet and the inifusioni
procedures were carriecl out after aln overnight fast. Mag-ilesiunl sulfate or magniesium clhlori(le w-as adminiistere( in-travenously in 5% (lextrose water during tinle intervalsthat ranged from 1, to 6 h. The rate of infusion was adjustedIill each stuidy to achie-e serum magnesiunm levels of alp-proximately 4-6 mg/100 ml as (letermined by frequenitperiodic magnesium determinations. During the infusionprocedure a physician was in constant atten(laince and, inaddition to frequenit serum magnesiumn determinations, thepatients were carefully evaluated by a cardiac monitor an(l
by testing of deep teildon reflexes. Except for a nild
flushing sensation, the patients explerienced no side effects
clurinig the inlfusioIns.RESULTS
Paticnt 1 (hlpocalccut ic-hvifpoparatlir.1oid'). Fig. 1Ashow-s the effect in patienit 1 of the infusion of 520 nmgof magnesium as illagllesium sulfate over a 2-h periodoil serum magnesium, iCT, calcium, phosplhorus, aindiPTH. As the serum magnesium increased there w-as a
rapid fall in serum iCT, and as tile serum magnesiumdecreased after discontinuation of the infusion there was
a rise in serum iCT toward base-line levels. There was
little chainge in the serum calciumni during magniesitill
1 01( Atna.st, David, WVinnaker, Glass, Baskin, Brubaker, and Burns
Ni(S04 Infusion
4 -
2
P.%frngflfflmO\
12
iCT I
(ngiml\ 10 a II
!\~~~~~r-~
i
8,
7 - >1oB- -------I &,-S
Ca \(rgllOOmlS
6 \ ,
5 L
iPTH(pi eq,'mlI
4 1
oI; t __2K
i 2 3 4 24
..nCI Infusion
E
p4 /mqg!oofOnj
c'- - -J
TlIME (h)
FIGURE 1 (A) The effect of the infusion of 520 mg of magnesium as magnesium sulfate overa 2-h period on serum magnesium, iCT, calcium, phosphorus, and iPTH in patient 1. Theshaded area in the lower panel in this and subsequent figures indicates limits of detectabilityof parathyroid hormone immunoassay. (B) The effect of the infusion of 2.250 mg of mag-nesium as magnesium chloride over a 6-h period on serum magnesium, iCT, calcium, phos-phorus, and iPTH in patient 2.
infusion, although a modest increase was observed afterthe infusion was discontinued. A fall in serum phos-phorus was observed during magnesium infusion, whilethe serum iPTH remained undetectable throughout theentire period of study.
Patient 2 (hypercalcemnic-bonte metastases). The ef-fect of a relatively long-term infusion of magnesium inpatient 2 is shown in Fig. 1B. 2,250 mg of magnesiumas magnesium chloride was infused over a 6-h period.The serum magnesium level increased to a high of 6.4mg/100 ml during the infusion and then declined slowlyto a level of 3.8 mg/100 ml over the 17-h period follow-ing the discontinuation of the infusion. The serum iCTdeclined rapidly during the infusion to a lowv point thatwas less than 50% of control values. As the serum mag-nesium concentration declined after the discontinuationof the infusion, the serum iCT slowly increased, but wasstill below base-line levels 17 h after the end of theinfusion, when the serum magnesium concentration was3.8 mg/100 ml. In general, the changes in serum calciumparalleled the changes in serum iCT. Thus, the initialfall in serum iCT was accompanied by a fall in serumcalcium and the rise in serum iCT that occurred afterthe infusion was accompanied by a rise in serum calcium.
No distinct pattern in serumi phosplhorus Nvas ob-served although there was a slight and transient de-crease during the 1st h of the magnesium infusion. Theserum iPTH remained undetectable throughout the pe-riod of study.
Patient 3 (normocalcemic-normital detectable serumniPTH). The effect of the infusion of 1,190 mg of mag-nesium as magnesium chloride over a 3-h period in pa-tient 3 is seen in Fig. 2A. During the infusion periodthe serum iCT decreased rapidly and was accompaniedby a fall in serum calcium, a rise in serum phosphorus,and a progressive decrease in serum iPTH to an un-detectable level. Within an hour after the discontinua-tion of the infusion, when the serum magnesium wasslowly returning toward baseline and the serum calciumwas continuing to fall, the serum iPTH increased andsubsequently reached base-line levels 2 h after discontinu-ation of the infusion.
The effect of the infusion of 480 mg of magnesium asmagnesium sulfate over a 1-h period in patient 3 isshown in Fig. 2B. The pattern of response was similarto that produced by magnesium chloride (Fig. 2A) ex-cept that the serum phosphorus decreased rather thanincreased.
Calcitonin-Lowering Effect of Magnesium 1617
NMgC12 Infusion
6,
AIgimg OOmb
4,
A B
1. 21
0.0icrlng ml)
0. 4,.
10,. - __
0-o ___o~°' -- SX
Ca ° -4 4
tmg4IO mil 9- </ ~ ° - 8-op
,1< / ~~~~~~~~~~~~~~~~~~~~imglOOmll8L -]- / ~~~~~~~~~~~~~~~~~~~~2o,0~~ _____.__ r2 O
iPTHjal eq ml)
2 4 6 8 10 12 24 1 2 3TIME Ih)
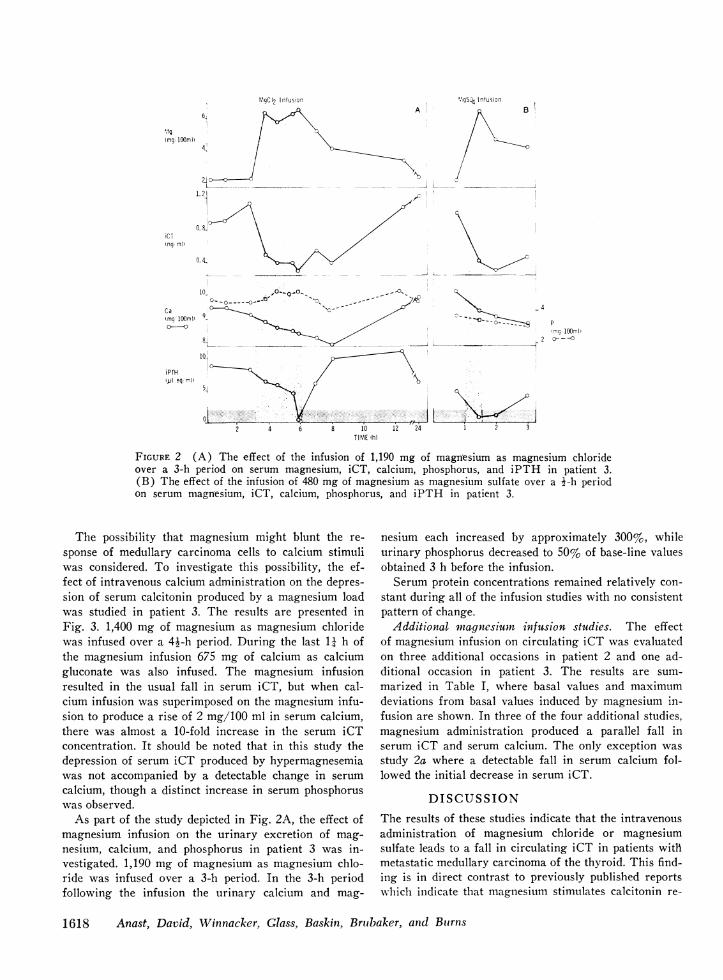
FIGURE 2 (A) The effect of the infusion of 1,190 mg of magnesium as magnesium chlorideover a 3-h period on serum magnesium, iCT, calcium, phosphorus, and iPTH in patient 3.(B) The effect of the infusion of 480 mg of magnesium as magnesium sulfate over a 1-h periodon serum magnesium, iCT, calcium, phosphorus, and iPTH in patient 3.
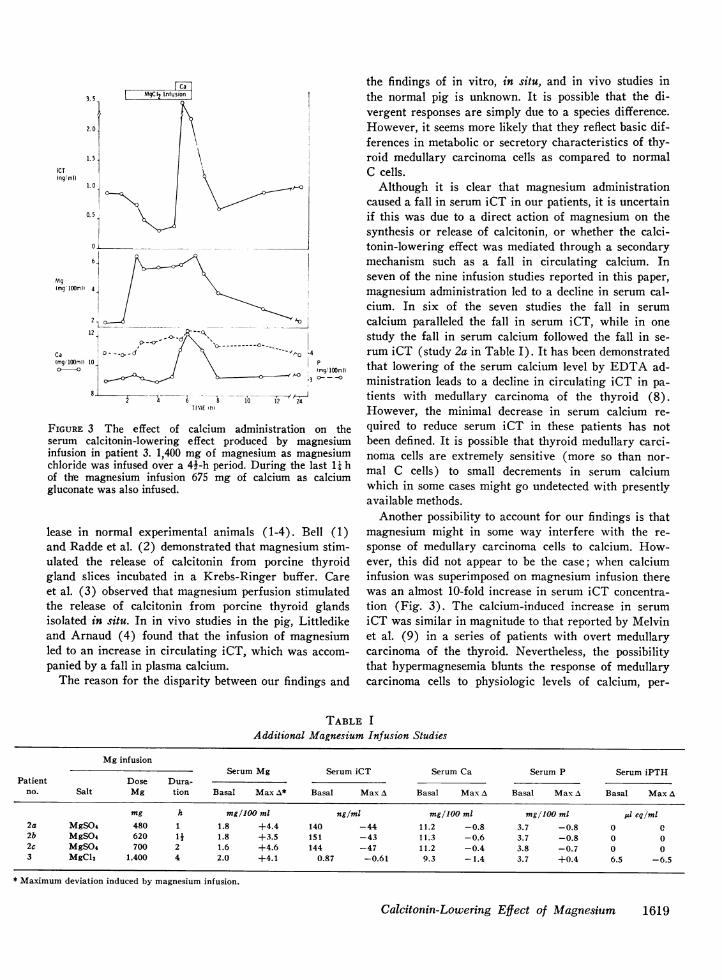
The possibility that magnesium might blunt the re-sponse of medullary carcinoma cells to calcium stimuliwas considered. To investigate this possibility, the ef-fect of intravenous calcium administration on the depres-sion of serum calcitonin produced by a magnesium loadwas studied in patient 3. The results are presented inFig. 3. 1,400 mg of magnesium as magnesium chloridewas infused over a 4k-h period. During the last 11 h ofthe magnesium infusion 675 mg of calcium as calciumgluconate was also infused. The magnesium infusionresulted in the usual fall in serum iCT, but when cal-cium infusion was superimposed on the magnesium infu-sion to produce a rise of 2 mg/100 ml in serum calcium,there was almost a 10-fold increase in the serum iCTconcentration. It should be noted that in this study thedepression of serum iCT produced by hypermagnesemiawas not accompanied by a detectable change in serumcalcium, though a distinct increase in serum phosphoruswas observed.
As part of the study depicted in Fig. 2A, the effect ofmagnesium infusion on the urinary excretion of mag-nesium, calcium, and phosphorus in patient 3 was in-vestigated. 1,190 mg of magnesium as magnesium chlo-ride was infused over a 3-h period. In the 3-h periodfollowing the infusion the urinary calcium and mag-
nesium each increased by approximately 300%, whileurinary phosphorus decreased to 50% of base-line valuesobtained 3 h before the infusion.
Serum protein concentrations remained relatively con-stant during all of the infusion studies with no consistentpattern of change.
Additional miagnesium infusion studies. The effectof magnesium infusion on circulating iCT was evaluatedon three additional occasions in patient 2 and one ad-ditional occasion in patient 3. The results are sum-marized in Table I, where basal values and maximumdeviations from basal values induced by magnesium in-fusion are shown. In three of the four additional studies,magnesium administration produced a parallel fall inserum iCT and serum calcium. The only exception wasstudy 2a where a detectable fall in serum calcium fol-lowed the initial decrease in serum iCT.
DISCUSSIONThe results of these studies indicate that the intravenousadministration of magnesium chloride or magnesiumsulfate leads to a fall in circulating iCT in patients witlhmetastatic medullary carcinoma of the thyroid. This find-ing is in direct contrast to previously published reportswlhich indicate that magnesium stimulates calcitonin re-
1618 Anast, David, Winnacker, Glass, Baskin, Brubaker, and Buirns
%IgSO4 Infusion
__
3.5
2.10
iCT(ngl m1)
1.5
1.0
0.5
6.-
Mg(mg'1IOOmI) 4
2.112
CaImgl0l0ml\ 10
o-
pW~~~~~~~~1C ---- --c- - -
\mg/ lOOml)3 0
6 12 24TIME th)
FIGuRE 3 The effect of calcium administration on theserum calcitonin-lowering effect produced by magnesiuminfusion in patient 3. 1,400 mg of magnesium as magnesiumchloride was infused over a 4i-h period. During the last 11 hof the magnesium infusion 675 mg of calcium as calciumgluconate was also infused.
lease in normal experimental animals (1-4). Bell (1)and Radde et al. (2) demonstrated that magnesium stim-ulated the release of calcitonin from porcine thyroidgland slices incubated in a Krebs-Ringer buffer. Careet al. (3) observed that magnesium perfusion stimulatedthe release of calcitonin from porcine thyroid glandsisolated in situ. In in vivo studies in the pig, Littledikeand Arnaud (4) found that the infusion of magnesiumled to an increase in circulating iCT, which was accom-panied by a fall in plasma calcium.
The reason for the disparity between our findings and
the findings of in vitro, in situ, and in vivo studies inthe normal pig is unknown. It is possible that the di-vergent responses are simply due to a species difference.However, it seems more likely that they reflect basic dif-ferences in metabolic or secretory characteristics of thy-roid medullary carcinoma cells as compared to normalC cells.
Although it is clear that magnesium administrationcaused a fall in serum iCT in our patients, it is uncertainif this was due to a direct action of magnesium on thesynthesis or release of calcitonin, or whether the calci-tonin-lowering effect was mediated through a secondarymechanism such as a fall in circulating calcium. Inseven of the nine infusion studies reported in this paper,magnesium administration led to a decline in serum cal-cium. In six of the seven studies the fall in serumcalcium paralleled the fall in serum iCT, while in onestudy the fall in serum calcium followed the fall in se-rum iCT (study 2a in Table I). It has been demonstratedthat lowering of the serum calcium level by EDTA ad-ministration leads to a decline in circulating iCT in pa-tients with medullary carcinoma of the thyroid (8).However, the minimal decrease in serum calcium re-quired to reduce serum iCT in these patients has notbeen defined. It is possible that thyroid medullary carci-noma cells are extremely sensitive (more so than nor-mal C cells) to small decrements in serum calciumwhich in some cases might go undetected with presentlyavailable methods.
Another possibility to account for our findings is thatmagnesium might in some way interfere with the re-sponse of medullary carcinoma cells to calcium. How-ever, this did not appear to be the case; when calciuminfusion was superimposed on magnesium infusion therewas an almost 10-fold increase in serum iCT concentra-tion (Fig. 3). The calcium-induced increase in serumiCT was similar in magnitude to that reported by Melvinet al. (9) in a series of patients with overt medullarycarcinoma of the thyroid. Nevertheless, the possibilitythat hypermagnesemia blunts the response of medullarycarcinoma cells to physiologic levels of calcium, per-
TABLE IAdditional Magnesium Infusion Studies
Mg infusionSerum Mg Serum iCT Serum Ca Serum P Serum iPTH
Patient Dose Dura-no. Salt Mg tion Basal Max A* Basal Max A Basal Max A Basal Max A Basal Max A
* Maximum deviation induced by magnesium infusion.
Calcitonin-Lowering Effect of Magnesium 1619
haps by competinig for binding sites, has not been defi-nitely ruled out.
Littledike and Arnaud (4) observed that the responseof intact pigs to magnesium clhloride infusioni was char-acterized by a rise in serum iCT and a fall in serumcalcium, while magnesium infusion in a thyroparathy-roidectomized pig led to a rise in serum calcium N-ithno detectable change in serum iCT. On the basis of thesefindings, the investigators suggested that the major fac-tor responsible for the hypocalcemic effect of magnesiumis calcitonin. This possibility is consistent w-ith previousreports which indicate that magniesitum administrationlowers the serum calcium level in intact, but not thy-roidectomized, cats and rats (10, 11). In our studies ofpatients with medullary carcinoma the fall in serumcalcium produced by the administration of magnesitumchloride or magnesium sulfate (observed in seven of ninestudies) was accompanied by a fall, rather than a rise,in serum iCT. Therefore, the calcium-low-erinig effectproduced by magnesium in these patients cannot be at-tributed to a calcitonin effect as was postulated in ani-imlal studies.
The fall in serumil iPTH produced by magnesium ad-ministration in patient 3 is consistent with previouslypublished observations that magnesium inhibits para-thyroid hormone secretion (12, 13), except in certainpatients with magnesium deficiency where magnesiummay actually stimulate the release of parathyroid hor-mone (14, 15). The fall in serumil calcium (Fig. 2) andin urine phosphorus in patient 3 could be secondary tothe fall in serum iPTH produced by magnesium. How-ever, in patient 2 with hvpercalcemia and bone meta-stases, a fall in serum calcium was observed in the pres-ence of a consistently undetectable serum iPTH level.Thus, in this patient the calcium-lowN-ering effect pro-duced by magnesium caninot be attribtuted to either arise in circulating iCT or a detectable fall in circulatingiPTH. This observation suggests that the calcium-lowering effect produced by mnagniesitunm is, in part atleast, due to a redistribution of body calciumii that is notmediated through the actions of eitlher paratlhvroid hor-mone or calcitonin.
The hypocalcenmic effect produiced by magniesitum infu-sioIn could be related to the calcituric effect of magnlesitum(16, 1/7), which lhas been attributed to competitive in-hiibition of tubular calciumni reabsorptioni. WVe observeda calciuric effect secondary to magniesitum infusion inpatient 3, while urinary excretion studies were not car-ried out in the other two patielnts.
The chalnges in serumn phosplhortus levels induced bymagnesium infusion in our patienits are of interest. Insome of our studies the adminiistration of magnesium re-suilted in a fall in serumni phosphorus while in other stuid-ies there wras either no change or a modest increase in
serum phosplhorus. Analysis of our data indicates thatthe responise of sertlm plhosphorus appeared to be re-lated to the anion that was infused with magnesium,
ithl the low-ering of the serumi phosplhortus being associ-ated N-ith sulfate inftusion. A hypophosphatemic effectof soditum sulfate has been previously noted and in onestudy wvas associated w-itlh a modest inicrease in turiniaryphlosphate excretion (18. 19).
Recently Gaut-vik and Tasljilan (20) reported sttudiesof calcitoniin release in a lhuman medullarv carcinolmianmaintainied in tissue culture. In this in vitro studxv mag-nesiumii alonie or in combiniatioin with calciulm did notinfluence the release of calcitonin. However, an tun-physiologically higlh calcium colncentration (20 nmM)was necessary to stimulate calcitonin release in cultuirewhile low calcitum concentratioins (0.5 mM\) did not af-fect hormonie release. The significance of this single illvitro study relative to in vivo studies in patients Nitlhmedtullarv thyroid car-cinonma is unlcertaini.
Altlhotlgh the nmechanism lhas not been eluicidated, itis clear that magnesiuim loxwers circulating iCT in pa-tienits N-itlh medullary carcinoma of the tlhvroid. Althotughlwe hlave attribtuted tllis finding to a direct or ilndirecteffect of nmagnesiumii on the release and,'or synthesis ofcalcitonin, it is possible that nmagnesium in some wvayalters the degradation of calcitonin in patients withmedullary thvroid carcinomiia. Further studies are neededto clarify this possibility.
Under basal conditions patient 1 lhad loose stoolsapproximatelv every half lhour and marked borborvgmi.It is of interest that for several hours duiring and aftermagnesium infusion there was distinct abatement inthese symptonms. It is possible that this improvement w-asrelated to the fall in circulating calcitonin since it lhasbeen suiggested that the diarrhea occurring in associa-tion wvith medullarv carcinoma of the thyvroid may bedue to calcitonin inhlibition of sodium cand water absorp-tion bv the intestine (21). On the otlher hand, hlighcontenits of serotonin and( prostaglandins lhav e been fotundin some thyroid medullarv carcinomas and both of thesecompounds are knoxvni to stimulate smooth muscle (22-24). The possibility that, in addition to its effect oncalcitonin, magniesiumil might influence the secretion orsy-nthesis of other bioactive substances produced by tllh-roid medullary carcinomas, including prostaglandi ns,serotonin, ACTH, and histaminase, is currently tunderinvestigationi.
ACKNOWNLEDGMENTSWe wish to express gratitude for the expert technical as-sistance of -Mrs. 'Marcia Schweiss, 'Mrs. SammyLangeluttig,and Dr. Arsenia Rodrigues and also for the excellent sec-retarial assistance of NMrs. Fern 'McClanahan in the prepa-ration of this manuscript.
This research was supported in part by Public HealthService Research Grants HD-02756 and FR-00287.
REFERENCES1. Bell, N. H. 1970. Effects of glucagon, dibutyryl cyclic
3',5'-adenosine moniophosphate, anid theophylline oni cal-citonin secretion in vitro. J. Clin. Invest. 49: 1368-1373.
2. Radde, I. C., D. K. Parkinson, E. R. Witterman, andB. Hoffken. 1969. Magnesium and calcium as stimulito in vitro release of calcitonin from thyroid slices.In Calcitonin 1969, Proceedings of the Second Inter-national Symposium. S. Taylor and G. Foster, editors.William Heinemann (Medical Books), Ltd., London.376-380.
3. Care, A. D., N. H. Bell, and R. F. L. Bates. 1971.The effect of hypermagnesaemia on calcitonin secretionin vivo. J. Endocrinol. 51: 381-386.
4. Littledike, E. T., and C. D. Arnaud. 1971. The influenceof plasma magnesium concentrations on calcitonin secre-tion in the pig. Proc. Soc. Exp. Med. Biol. 136: 1000-1006.
5. Fiske, C. H., and Y. Subbarow. 1926. The colorimetricdetermination of phosphorus. J. Biol. Chem. 66: 375-400.
6. Conaway, H. H., and C. S. Anast. 1974. Double-anti-body radioimmunoassay for parathyroid hormone. J.Lab. Clin. Med. 83: 129-138.
7. Deftos, L. J. 1971. Immunoassay for human calcitonin.I. Method. Metab. Clin. Exp. 20: 1122-1128.
8. Deftos, L. J., A. D. Goodman, K. Engelman, and J. T.Potts, Jr. 1971. Suppression and stimulation of calci-tonin secretion in medullary thyroid carcinoma. Metab.Clin. Exp. 20: 428-431.
9. Melvin, K. E. W., A. H. Tashjian, Jr., and H. H.Miller. 1972. Studies in familial (medullary) thyroidcarcinoma. Recent Prog. Horm. Res. 28: 399-470.
10. Radde, I. C., E. R. Witterman, and S. Pensuwan. 1968.Effect of thyroid and parathyroid on hypocalcemia oc-curring after a magnesium load. Endocrinology. 83:1285-1292.
11. Nielsen, S. P. 1970. Abolition of magnesium-inducedhypocalcaemia by acute thyro-parathyroidectomy in thecat. Acta Endocrinol. 64: 150-158.
12. Buckle, R. M., A. D. Care, C. W. Cooper, and H. J.Gitelman. 1968. The influence of plasma magnesiumconcentration on parathyroid hormone secretion. J. En-docrinol. 42: 529-534.
13. Pletka, P., D. S. Bernstein, C. L. Hampers, J. P.MIerrill, and L. M. Sherwood. 1971. Effects of mag-nesium on paratlhyroid hormone secretion durinig chronichaemodialysis. Lancet. 2: 462-463.
14. Anast, C. S., J. M. Mohs, S. L. Kaplan, and T. W.Burns. 1972. Evidence for parathyroid failure in mag-nesium deficiency. Scienice (W'ash. D. C.). 177: 606-608.
15. Suh, S. M., A. H. Tashjian, Jr., N. Matsuo, D. K.Parkinson, and D. Fraser. 1973. Pathogenesis of hypo-calcemia in primary hypomagnesemia: normal end-organ responsiveness to parathyroid hormone, impairedparathyroid gland function. J. Clin. Invest. 52: 153-160.
16. Mendel, L. B., and S. R. Benedict. 1909. The paths ofexcretion for inorganic compounds. IV. The excretionof magnesium. Am. J. Physiol. 25: 1-22.
17. Jones, K. H.. and P. Fourman. 1966. Effects of in-fusions of magnesium and of calcium in parathyroidinsufficiency. Clin. Sci. (Oxf.). 30: 139-150.
18. Chakmakjian, Z. H., and J. E. Bethune. 1966. Sodiumsulfate treatment of hypercalcemia. N. Engl. J. Med.275: 862-869.
19. Fulmer, D. H., A. B. Dimich, E. 0. Rothchild, andW. P. L. Myers. 1972. Treatment of hypercalcemia.Comparison of intravenously administered phosphate,sulfate, and hydrocortisone. Arch. Intern. Med. 129:923-930.
20. Gautvik, K. M., and A. H. Tashjian, Jr. 1974. Humanmedullary thyroid carcinoma: control of calcitonin se-cretion in vivo and in tissue culture. Horm. Metab. Res.6: 70-73.
21. Gray, T. K., F. A. Bieberdorf, and J. S. Fordtran.1973. Thyrocalcitonin and the jejunal absorption of cal-cium, water, and electrolytes in normal subjects. J. Clin.Invest. 52: 3084-3088.
22. Cope, C. S., and E. D. Williams. 1967. Clinicopathologi-cal conference: a case of diarrhea and goiter. Br. Med.J. 3: 293-297.
23. Ibanez, M. L., V. W. Cole, W. 0. Russel, and R. L.Clark. 1967. Solid carcinoma of the thyroid Analyses of53 cases. Cancer. 20: 706-723.
24. Williams, E. D., S. M. M. Karim, and M. Sandler.1968. Prostaglandin secretion by medullary carcinomaof the thyroid. A possible case of associated diarrhoea.Laiwcet. 1: 22-23.