Drug and Alcohol Dependence, 17 (1986) 331-338 Elsevier Scientific Publishers Ireland Ltd. 331 SERUM PROLACTIN CORRELATES WITH DEPRESSED MOOD DURING ALCOHOL WITHDRAWAL FRANK MILLER*, ALAN BARASCH, MICHAEL SACKS, JANE LEVITAN and LOIS ASHCROFT Department of Psychiatry, The Payne Whitney Clinic, New York Hospital-Cornell University Medical Center, 525 East 68th Street, New York, NY 10021 (U.S.A.) (Received July 24th, 1985) SUMMARY Alterations in central dopamine function have been identified in de- pression and in alcohol withdrawal. Attempts to determine the magnitude and direction of the central dopamine alteration in alcohol withdrawal have produced conflicting results. In this study serum prolactin (PRL) was used as an indicator of central dopamine activity since dopamine is the most important factor in the control of prolactin secretion from the pitu- itary. Increased serum PRL levels were found during alcohol withdrawal and they correlated significantly with high scores on the Hamilton Depres- sion Rating Scale (HDRS). No significant correlations were identified with The Brief Psychiatric Rating Scale (BPRS), the ‘Mini-Mental State’ of Fol- stein (MMS), The Beck Depression Inventory (BDI) or The Modified Gross Alcohol Withdrawal Selective Severity Assessment Scale (GAWSSA). The authors concluded that the transient depressive symptomatology typically found in detoxifying alcoholic patients may be, in part, the result of a central hypodopaminergic state. Key words: Alcohol - Alcoholism - Depression - Prolactin INTRODUCTION Increasing evidence implicates a role for altered cen_tral dopamine func- tion in the pathophysiology of alcohol withdrawal syndromes. Fujimoto *To whom requests for reprints should be addressed. 0376~8716/86/$03.50 Elsevier Scientific Publishers Ireland Ltd. Printed and Published in Ireland
Transcript
Drug and Alcohol Dependence, 17 (1986) 331-338 Elsevier Scientific Publishers Ireland Ltd.
331
SERUM PROLACTIN CORRELATES WITH DEPRESSED MOOD DURING ALCOHOL WITHDRAWAL
FRANK MILLER*, ALAN BARASCH, MICHAEL SACKS, JANE LEVITAN and LOIS ASHCROFT
Department of Psychiatry, The Payne Whitney Clinic, New York Hospital-Cornell
University Medical Center, 525 East 68th Street, New York, NY 10021 (U.S.A.)
(Received July 24th, 1985)
SUMMARY
Alterations in central dopamine function have been identified in de- pression and in alcohol withdrawal. Attempts to determine the magnitude and direction of the central dopamine alteration in alcohol withdrawal have produced conflicting results. In this study serum prolactin (PRL) was used as an indicator of central dopamine activity since dopamine is the most important factor in the control of prolactin secretion from the pitu- itary. Increased serum PRL levels were found during alcohol withdrawal and they correlated significantly with high scores on the Hamilton Depres- sion Rating Scale (HDRS). No significant correlations were identified with The Brief Psychiatric Rating Scale (BPRS), the ‘Mini-Mental State’ of Fol- stein (MMS), The Beck Depression Inventory (BDI) or The Modified Gross Alcohol Withdrawal Selective Severity Assessment Scale (GAWSSA). The authors concluded that the transient depressive symptomatology typically found in detoxifying alcoholic patients may be, in part, the result of a central hypodopaminergic state.
Increasing evidence implicates a role for altered cen_tral dopamine func- tion in the pathophysiology of alcohol withdrawal syndromes. Fujimoto
*To whom requests for reprints should be addressed.
0376~8716/86/$03.50 Elsevier Scientific Publishers Ireland Ltd. Printed and Published in Ireland
332
et al. [ 11 observed that the cerebrospinal fluid major dopamine metabolite homovanillic acid (CSF-HVA) decreased during alcohol withdrawal delirium and returned to normal when the delirium resolved. In a similar vein, Major et al. [2] reported that CSF-HVA concentration in patients with alcohol withdrawal symptoms was decreased compared to the post-withdrawal state.
Borg and Weinholdt [ 3,4] reported that alcohol withdrawal is associated with significantly elevated serum prolactin (PRL) and advised the use of dopamine agonists in the treatment of alcohol withdrawal. Secretion of PRL is predominantly under the inhibitory control of the hypothalamus, mediated by the release of dopamine into the hypothalamic-hypophyseal portal system. [5-S]. Since dopamine can act directly on pituitary gland mammotrophs to decrease the secretion of PRL, it is theorized that dop- amine is either a constituent of prolactin inhibiting factor (PIF) or is PIF itself (9-101. Accordingly, Borg and Weinholdt’s finding of elevated serum PRL in acute alcohol withdrawal can be taken as evidence of a central hypodopaminergic state in this condition. However, not all laboratories have concluded that alcohol withdrawal is associated with decreased dop- amine. Loosen et al. [ll] reported that men in acute alcohol withdrawal demonstrated significantly lower serum PRL levels, than did men in the post-withdrawal state and normal subjects. They concluded that the most parsimonious explanation for the lowered serum PRL levels when compared to baseline levels, was the postulation of a central hyperdopaminergic state.
With this divergence in the literature as our point of departure, the present study addressed the following questions: (1) does alcohol withdrawal result in elevated or reduced serum PRL? (2) do signs and symptoms of alcohol withdrawal and specifically depressed mood correlate with various levels of serum PRL? and (3) are some of the contradictions in the literature an outcome resulting from the study of different patient populations? For the purpose of this study, serum PRL is presumed to be a measure of central dopamine activity.
METHODS
Fifteen male patients (age 40.9 t 12.0) admitted to the Payne Whitney Clinic of the New York Hospital with a diagnosis of alcohol addiction were studied. Patients were included if they were between the ages of 18 and 65, without a history of primary mood disorder; if they did not require a medical regimen; and if they had not taken opiates, sedatives, hypnotics, analgesics, other than aspirin and acetominophen, hormones, or any psycho- active drug during the 30 days preceding the hospitalization. Only patients who were detoxified with chlordiazepoxide and received no medication other than vitamins, bowel softeners, and antacids were included. While severely limiting the number of subjects, this approach was necessary to reduce the factors which are known or suspected to influence the release of PRL.
333
On the first hospital day informed consent and demographic data were acquired. In addition, time of last drink and total alcohol consumed during the preceding 24 h, 7 days, and 30 days were estimated. All drugs used during the preceding 90 days were determined. A Diagnostic and Statistical Manual III (DSM III) diagnosis of alcohol addiction was confirmed [ 121. On days 1, 3, 5, and 8, following overnight fast and bedrest two blood samples were drawn approx. 30 min apart, 1-3 h after awakening, and generally between 0800 and 1000. The coefficients of variation for the paired serum PRL samples were determined and analyzed with 2-tailed variance ratio tests. No significant differences were identified. Therefore, the averages of the paired samples were used in all calculations. Serum PRL determinations were made using a commercially prepared assay kit em- ploying a double-antibody 125 I radioimmunoassay method and human serum-based calibrators [ 131. For our laboratory the mean serum PRL level for 45 normal men was 6.9 + 3.3 ng/ml (mean + S.D.).
On days 1, 3, 5, and 8 the following rating scales were completed: (1) BPRS [14]; (2) MMS [15]; (3) HDRS [16]; (4) GAWSSA [17]; and (5) BDI [ 181. Each patient was evaluated by two interviewers and the average score was recorded and used in all calculations. The average of the paired serum PRL levels acquired on days 1, 3, 5 and 8 were correlated with the scores of the rating scales acquired on the corresponding days.
TABLE I
SERUM PROLACTIN (in ng/ml) FOR 15 DETOXIFYING ALCOHOLIC PATIENTS
aOne sample only. bAnalysis of variance for repeated measures: non-significant.
28 19 12a 28
4 6 5 8 5 6 9
17 9
25a 5
12 +gb
334
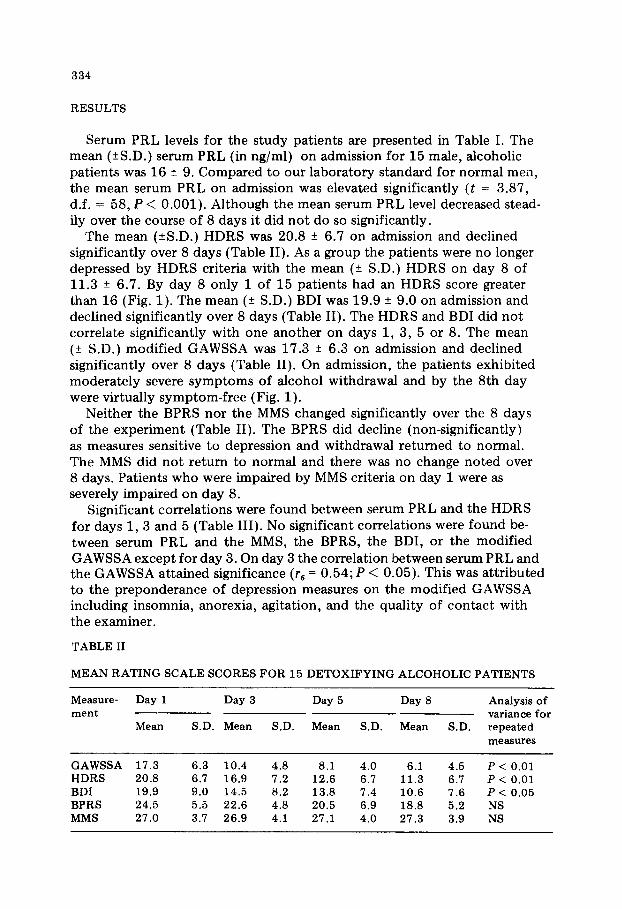
RESULTS
Serum PRL levels for the study patients are presented in Table I. The mean (2S.D.) serum PRL (in ng/ml) on admission for 15 male, alcoholic patients was 16 f 9. Compared to our laboratory standard for normal men, the mean serum PRL on admission was elevated significantly (t = 3.87, d.f. = 58, P < 0.001). Although the mean serum PRL level decreased stead- ily over the course of 8 days it did not do so significantly.
The mean (*SD.) HDRS was 20.8 + 6.7 on admission and declined significantly over 8 days (Table II). As a group the patients were no longer depressed by HDRS criteria with the mean (k S.D.) HDRS on day 8 of 11.3 k 6.7. By day 8 only 1 of 15 patients had an HDRS score greater than 16 (Fig. 1). The mean (it: S.D.) BDI was 19.9 k 9.0 on admission and declined significantly over 8 days (Table II). The HDRS and BDI did not correlate significantly with one another on days 1, 3, 5 or 8. The mean (k S.D.) modified GAWSSA was 17.3 + 6.3 on admission and declined significantly over 8 days (Table II). On admission, the patients exhibited moderately severe symptoms of alcohol withdrawal and by the 8th day were virtually symptom-free (Fig. 1).
Neither the BPRS nor the MMS changed significantly over the 8 days of the experiment (Table II). The BPRS did decline (non-significantly) as measures sensitive to depression and withdrawal returned to normal. The MMS did not return to normal and there was no change noted over 8 days. Patients who were impaired by MMS criteria on day 1 were as severely impaired on day 8.
Significant correlations were found between serum PRL and the HDRS for days 1, 3 and 5 (Table III). No significant correlations were found be- tween serum PRL and the MMS, the BPRS, the BDI, or the modified GAWSSA except for day 3. On day 3 the correlation between serum PRL and the GAWSSA attained significance (r, = 0.54; P < 0.05). This was attributed to the preponderance of depression measures on the modified GAWSSA including insomnia, anorexia, agitation, and the quality of contact with the examiner.
TABLE II
MEAN RATING SCALE SCORES FOR 15 DETOXIFYING ALCOHOLIC PATIENTS
Measure- Day 1 Day 3 Day 5 Day 8 Analysis of ment variance for
Mean S.D. Mean S.D. Mean S.D. Mean S.D. repeated measures
Fig. 1. Scatter plots of individual rating scale scores for 15 detoxifying alcoholic patients.
Serum PRL did not correlate significantly with age, total years of addic- tion or abuse, or with the amount of alcohol consumed during the preceding 24 h, 7 days or 30 days. Serum PRL did not correlate significantly with total bilirubin, with transaminase levels, (SGOT, SGPT) or with alkaline phosphatase.
336
TABLE III
CORRELATIONS BETWEEN SERUM PROLACTIN AND THE HAMILTON RATING SCALE FOR 15 DETOXIFYING ALCOHOLIC PATIENTS
Day Spearman rank order correlation
Significance
1 rs = 0.68 P < 0.02 3 rs = 0.72 P < 0.01 5 rs = 0.65 P < 0.02 8 rs = 0.51 NS
DISCUSSION
A chart review conducted in preparation for this study revealed that 31 of 44 alcoholic patients admitted for detoxification met DSM III criteria for major depression. However, as this study documents, for the majority of patients without a history of primary mood disorder, depression resolves during the detoxification period. Therefore, abstinence alone appears to be all that is required to ameliorate the condition. The significant correlations between the HDRS and serum PRL for days 1, 3 and 5 suggest that the symptoms of depression observed during alcohol detoxification may relate to altered dopamine function. This hypothesis is supported by evidence implicating a role for altered dopamine function in the pathophysiology of depression [ 19-251. However, the synthesis, release and metabolism of PRL are not solely under the control of dopamine; and, even though it would be parsimonious to integrate dopamine’s inhibition of PRL release into a model which explained alcoholic depression, to do so at the present time would be premature.
Loosen et al’s [ll] contradictory observation that acute alcohol with- drawal is hyperdopaminergic may be the result of their patient selection. Their patients were described as being in ‘impending delirium tremens’ (p. 540) while no patient in our study was so characterized. Fujimoto et al. [l] and Major et al. [2] established that a correlation between CSF- HVA and alcohol withdrawal delirium does exist, but determined that delirium was associated with a decrease in CSF-HVA. This finding does not support Loosen et al’s observation. Clarification must await further study.
Serum PRL did not decrease significantly over 8 days. Whether a decline to normal levels actually occurred subsequently is not known. Possibly a study design which measured serum PRL after several weeks of abstinence would have revealed significant declines.
The insignificant decrease in serum PRL may have been the result of
3 37
factors mitigating against decline. Sleep is known to influence early morning serum PRL levels significantly. Serum levels of PRL increase during undis- turbed sleep, peaking between 0400 and 0600 and rarely exceeding 30 ng/ml during those hours [ 261. This late nocturnal rise is followed by a decline soon after awakening and the lowest levels are reached 1-3 h later. Insomnia was a factor in all study patients. All patients complained of disturbed sleep and many of early morning awakening, especially on the first and third study days. Insomnia would tend to lower serum PRL, while improving sleep would tend to raise serum PRL. All patients reported improved sleep over the 8 study days. Improved sleep would increase late nocturnal levels of serum PRL and since the plasma half-life of PRL is relatively long the levels 1-3 h after awakening would tend to be higher [27]. A decline in serum PRL resulting from hypothalamic-pituitary recovery, occurring during alcohol withdrawal, would be counteracted by the enhanced PRL release resulting from improved sleep. Therefore, a statistically insignificant decline in serum PRL, may reflect a clinically significant recovery of hypo- thalamic-hypophyseal function.
The distribution of serum PRL levels observed in this study, while sup- porting the hypothesis that alcohol withdrawal, complicated by depression, is associated with elevated serum PRL levels; does not support the con- clusion that elevated serum PRL will be observed in all cases of alcohol withdrawal. The absence of repeated significant correlations between the modified GAWSSA and serum PRL demonstrates that such a conclusion is unwarranted. Patients with moderately several alcohol withdrawal were as likely to have serum PRL within normal limits as they were to have elevated serum PRL. We concluded, therefore, that alcohol withdrawal is associated with a spectrum of serum PRL levels.
In this study we were unable to collect a sample of delusional, hallucin- ated, or delirious patients who were not depressed by HDRS criteria. This group may comprise those patients who have lowered serum PRL resulting from a central hyperdopaminergic state. This finding would be of theoretical and clinical interest; for a significant correlation between hallucinosis or delusional mood, on the one hand, and increased central dopamine activity, on the other, would fit well with the dopamine theory of psychosis. This hypothesis requires study.
REFERENCES
1 A. Fujimoto et al., Biol. Psychiatry, 18 (1983) 1141. 2 L. Major et al., Biol. Psychiatry, 12 (1977) 635. 3 V. Borg and T. Weinholdt, Acta Psychiatr. Stand., 65 (1982) 101. 4 V. Borg and T. Weinholdt, Curr. Ther. Res., 27 (1980) 170. 5 d. Takahara, A. Arimura and A. Schally, Endocrinology, 95 (1974) 1490. 6 A. Boyd and S. Reichlin, Psychoneuroendocrinology, 3 (1978) 113. 7 ‘L. Ferland et al., Role of the tuberoinfundibular dopaminergic system in the control
338
of prolactin secretion, in: M. Motta (Ed.) Endocrine Functions of the Brain, Raven Press, New York, 1980, pp. 271-296.
8 G. Gudelsky, Psychoneuroendocrinology, 6 (1981) 3. 9 H. Leblanc et al., J. Clin. Endocrinol. Metab., 43 (1976) 668.
IO A. Schally et al., Acta Endocrinol., 82 (1976) 1. 11 P. Loosen, A. Prange and I. Wilson, Arch. Gen. Psychiatry, 36 (1979) 540. I2 American Psychiatric Association, Committee on Nomenclature and Statistics:
Diagnostic and Statistical Manual of Mental Disorder, 3rd Edn, Washington, DC, American Psychiatric Association, 1980.
13 Prolactin Double Antibody with Human Serum Calibrators, Protocol: Diagnostic Products Corporation, Los Angeles, CA, 1984.
I4 J. Overall and D. Gorham, The Brief Psychiatric Rating Scale. Psychol. Rep., 10 (1962) 799.
15 M. Folstein, S. Folstein and P. McHugh, J. Psychiatr. Res., 12 (1975) 189. 16 M. Hamilton, J. Neurol. Neurosurg. Psychiatry, 23 (1960) 56. 17 M. Gross, E. Lewis and J. Hastey, Acute alcohol withdrawal syndrome, in: B. Kissin
and H. Begleiter (Eds.), The Biology of Alcoholism, Vol. 3, Plenum Press, New York, 1974, pp. 191-263.
18 A. Beck et al., Arch. Gen. Psychiatry, 26 (1981) 57. 19 R. Post, J. Ballenger and F. Goodwin, Cerebrospinal fluid studies of neurotrans-
mitter function in manic and depressive illness, in: J. Wood (Ed.), Neurobiology of Cerebrospinal Fluid, Vol. 1, Plenum Press, New York, 1980, pp. 685-717.
20 L. Colonna, M. Petit and J. Lepine, J. Affect. Disorders, 1 (1979) 173. 21 C. Nordin, B. Siwers, L. Bert&son, Acta Psychiatr. Stand., 64 (1981) 25. 22 E. Silberman et al., Am. J. Psychiatry, 138 (1981) 1302. 23 A. Halaris, K. Belendiuk and D. Freedman, Biochem. Pharmacol., 24 (1975) 1896. 24 G. Serra et al., Life Sci., 25 (1979) 415. 25 A. Randrup and C. Braestrup, Psychopharmacology, 53 (1977) 309. 26 J. De La Fuente and A. Rosebaum, Psychopharmacology, 53 (1981) 309. 27 D. Jimerson et al., Psychiatry Res., 13 (1984) 1.








![Dnr for Depressed Psychiatric Patients[1]](https://static.documents.pub/doc/80x56/5535edb1550346d5788b483b/dnr-for-depressed-psychiatric-patients1.jpg)















