8 10 Brief Communications March 1992 American Heart Journal cians were alert to the existence of this entity. Further- more, recognition of this phenomenon may have profound clinical implications. Although experience with this condi- tion is of course limited, prudence dictates that measures be taken to avoid exacerbating the subaortic stenosis. Va- sodilator therapy should be avoided. HD regimens should be modified so as to minimize the magnitude of associated changes in preload and afterload. Patients should be mon- itored closely for signs of cardiovascular instability during HD, and alternative treatment modalities such as perito- neal dialysis or early transplantation should be considered. Wider appreciation of the potential impact of HD upon the hemodynamics of renal patients with ASH may permit the true incidence of HD-induced subaortic obstruction to be ascertained and allow the optimal management of this dis- order to be established. REFERENCES 1. 2. 3. 4. 5. 6. Drukker A, Urbach J, Glaser J. Hypertrophic cardiomyopathy in children with end stage renal disease and hypertension. Proc EDTA 1981;18:542-7. Huting J, Kramer W, Schutterle G, Wizemann V. Analysis of left ventricular changes associated with chronic hemodialysis. Nephron 1988;49:284-90. Bernardi D, Bernini L, Cini G, Geri AB, Urti DA, Bonechi I. Asymmetric septal hypertrophy in uremic-normotensive pa- tients on regular hemodialysis. Nephron 1985;39:30-5. Abbasi AS, Slaughter JC, Allen MW. Asymmetric septal hy- pertrophy in patients on long-term hemodialysia. Chest 1978;74:548-51. Ireland MA, Mehta BR, Shiu MF. Acute effects of haemodi- alysis on left heart dimensions and left ventricular function: an echocardiographic study. Nephron 1981;29:73-9. Wynne J, Braunwald E. Hypertrophic cardiomyopathy. In: Braunwald E, ed. Heart disease. 3rd ed. Philadelphia: WB Saunders, 19881418-30. Severe subpulmonic outflow obstruction caused by aneurysm of the membranous ventricular septum: Diagnosis by transesophageal echocardiography Ashok Sharma, MD, Morton J. Kern, MD, Paul Callicoat, MD, Frank Aguirre, MD, Arthur Labovitz, MD, and Vallee L. Willman, MD. St. Louis. MO. An aneurysm of the membranous portion of the ventricu- lar septum is a rare congenital anomaly, occurring alone or From the Cardiology Division, St. Louis University Hospital. Reprint requests: Morton J. Kern, MD, J. G. Mudd Cardiac Catheterization Laboratory, St. Louis University Hospital, 3635 Vista Ave. at Grand Blvd., St. Louis, MO 63110-0250. 414134611 B Fig. 1. A, Frame from transesophageal two-dimensional echocardiography. B, Diagram of echocardiogram. A, An- eurysm; IVS, intraventricular septum; LA, left atrium; LV, left ventricle; RV, right ventricle. The aneurysm was seen only in systole. in combination with other cardiac lesions, and is usually of no clinical significance. l. 2 Large aneurysms may produce arrhythmias or significant hemodynamic changes by ob- structing the right ventricular outflow tract or by extend- ing into and distorting or replacing the septal leaflets of the tricuspid valve. 3-5 We report a patient with symptomatic right ventricular outflow tract obstruction caused by large ventricular septal aneurysm diagnosed by transesophageal echocardiography, confirmed by angiography, and repaired surgically. Although the clinical, hemodynamic, and cin- eangiographic features have been previously described,5-15
Transcript
8 10 Brief Communications March 1992
American Heart Journal
cians were alert to the existence of this entity. Further- more, recognition of this phenomenon may have profound clinical implications. Although experience with this condi- tion is of course limited, prudence dictates that measures be taken to avoid exacerbating the subaortic stenosis. Va- sodilator therapy should be avoided. HD regimens should be modified so as to minimize the magnitude of associated changes in preload and afterload. Patients should be mon- itored closely for signs of cardiovascular instability during HD, and alternative treatment modalities such as perito- neal dialysis or early transplantation should be considered.
Wider appreciation of the potential impact of HD upon the hemodynamics of renal patients with ASH may permit the true incidence of HD-induced subaortic obstruction to be ascertained and allow the optimal management of this dis- order to be established.
REFERENCES
1.
2.
3.
4.
5.
6.
Drukker A, Urbach J, Glaser J. Hypertrophic cardiomyopathy in children with end stage renal disease and hypertension. Proc EDTA 1981;18:542-7. Huting J, Kramer W, Schutterle G, Wizemann V. Analysis of left ventricular changes associated with chronic hemodialysis. Nephron 1988;49:284-90. Bernardi D, Bernini L, Cini G, Geri AB, Urti DA, Bonechi I. Asymmetric septal hypertrophy in uremic-normotensive pa- tients on regular hemodialysis. Nephron 1985;39:30-5. Abbasi AS, Slaughter JC, Allen MW. Asymmetric septal hy- pertrophy in patients on long-term hemodialysia. Chest 1978;74:548-51. Ireland MA, Mehta BR, Shiu MF. Acute effects of haemodi- alysis on left heart dimensions and left ventricular function: an echocardiographic study. Nephron 1981;29:73-9. Wynne J, Braunwald E. Hypertrophic cardiomyopathy. In: Braunwald E, ed. Heart disease. 3rd ed. Philadelphia: WB Saunders, 19881418-30.
Severe subpulmonic outflow obstruction caused by aneurysm of the membranous ventricular septum: Diagnosis by transesophageal echocardiography
Ashok Sharma, MD, Morton J. Kern, MD, Paul Callicoat, MD, Frank Aguirre, MD, Arthur Labovitz, MD, and Vallee L. Willman, MD. St. Louis. MO.
An aneurysm of the membranous portion of the ventricu- lar septum is a rare congenital anomaly, occurring alone or
From the Cardiology Division, St. Louis University Hospital.
Reprint requests: Morton J. Kern, MD, J. G. Mudd Cardiac Catheterization Laboratory, St. Louis University Hospital, 3635 Vista Ave. at Grand Blvd., St. Louis, MO 63110-0250.
414134611
B
Fig. 1. A, Frame from transesophageal two-dimensional echocardiography. B, Diagram of echocardiogram. A, An- eurysm; IVS, intraventricular septum; LA, left atrium; LV, left ventricle; RV, right ventricle. The aneurysm was seen only in systole.
in combination with other cardiac lesions, and is usually of no clinical significance. l. 2 Large aneurysms may produce arrhythmias or significant hemodynamic changes by ob- structing the right ventricular outflow tract or by extend- ing into and distorting or replacing the septal leaflets of the tricuspid valve. 3-5 We report a patient with symptomatic
right ventricular outflow tract obstruction caused by large ventricular septal aneurysm diagnosed by transesophageal echocardiography, confirmed by angiography, and repaired surgically. Although the clinical, hemodynamic, and cin- eangiographic features have been previously described,5-15
Volume 123
Number 3 Brief Communications 811
1 set
ECG ECG
RA RV Outflow tract g50 mmHg)
1 set
ww
RV+PA (O-l 00 mmHg)
Fig. 2. Right heart hemodynamics. Note the right ventricular (RV) outflow tract and pulmonary artery (PA) pressures show no gradient (0 to 50 mm Hg scale). The body of the right ventricle below the obstruc- tion showed a striking systolic gradient (0 to 100 mm Hg scale).
this case is the first report employing transesophageal echocardiography for diagnosis.
A 39-year-old white man was referred for evaluation of palpitations and progressively worsening shortness of breath associated with dizziness. A heart murmur had been detected in his childhood, but he was asymptomatic until 1 year before, when he noted a decrease in exercise toler- ance. His physical development in childhood was normal. The patient smoked cigarettes and was taking no medica- tions. Physical examination revealed a well-developed man with a blood pressure of 140/80 mm Hg and a pulse of 54/ min and regular. The cardiac examination revealed a nor- mal S1 and soft, single Ss with no pulmonic closing sound, and a grade III/VI ejection murmur along the third left in- tercostal space radiating to the axilla. The chest, abdomen, and extremity examinations were normal. The chest roent- genogram was normal. The electrocardiogram showed sinus bradycardia with a normal axis. Transthoracic two- dimensional echocardiography revealed normal left ven- tricular and atrioventricular valvular function. Color flow and Doppler showed subpulmonic stenosis. Transesoph- ageal echocardiography demonstrated a bulging membra- nous ventricular septum into the right ventricular outflow tract seen only in systole (Fig. 1). Increased pulmonary flow velocities of 4 m/set were detected at the ventricular side of the pulmonic valve, consistent with subpulmonic steno- sis. Right and left heart catheterization, selective coronary angiography, and ventriculography were performed. The right atria1 pressure was 6 mm Hg with large A waves. Right ventricular pressure below the subpulmonic chamber was 80/5 mm Hg, with a 60 mm Hg gradient across the right ventricular outflow tract (Fig. 2). Pulmonary artery pres- sure was 20/10 mm Hg. Aortic pressure was 118/70 mm Hg. Left ventricular end-diastolic and pulmonary capillary wedge pressures were 12 mm Hg. Serial oximetry failed to demonstrate left-to-right shunting. Cardiac output (Fick method) was 4.7 L/min. Coronary arteriography was nor- mal and left ventriculography showed normal contraction.
During systolic contraction, the left ventriculogram re- vealed a bulging, contrast-filled aneurysm extending from the membranous septum into the right ventricular outflow tract (Fig. 3). The systolic frames of the right ventriculo- gram also showed a negative shadow of the aneurysm fill- ing the right ventricular outflow tract. The aortic root an- giogram was normal without valvular regurgitation. At surgery, the pulmonary artery was normal in size with a prominent thrill. Through a small right ventriculotomy below the pulmonary anulus and extending toward the apex, a large saccular aneurysm arising from the membra- nous septum was seen and was excised (Fig. 4). This mem- branous sac was associated with a small ventricular septal defect and involved the base of the tricuspid valve. After the major portion of the sac was excised, the ventricular septal defect was obliterated. The postoperative course was uneventful and the patient was discharged home in an am- bulatory condition and without symptoms.
Aneurysms of the membranous ventricular septum were first described in 1826 by Laennec.i6 More recently, there have been more than 200 cases reported in the world liter- ature,l-15 with the largest series of 80 cases reported by Steinberg in 1957.r Ventricular septal defects in the mem- branous septum may be reduced or even closed by fre- quently associated fibrous tissue tags resulting from fibrin proliferation and/or an adhesion of tricuspid valve tissue to edges of the defect. l7 Although perimembranous ventricu- lar septal defects have the potential to develop into aneu- rysms, this transformation is more frequently found in those that extend into the inlet or trabecular portion of the septum, postulated to occur because of the localization and proximity to the tricuspid septal leaflet. In 1912, Mall3 de- scribed aneurysms of the membranous septum tangential to the root of the aorta and proposed that a structural weakness could propagate minor degrees of rightward dis- placement of the ventricular septum. After birth high pressures in the left ventricle would progressively distend the aneurysmal sac. Lev and Saphir4 amplified this conjec-
812 Brief Communications March IS92
American Heart .Journe,
Fig. 3. A, Left ventriculogram (30-degree right anterior oblique projection) in diastole and (B) in systole. Arrow denotes aneurysm appearing in the right ventricular outflow tract. C, Left ventriculography (45-de- gree left anterior oblique projection with 20-degree cranial projection) in systole showing large aneurysm in the right ventricular outflow tract. D, Right ventriculogram (30-degree right anterior oblique projection) with negative contrast shadow confirming location of septal aneurysm. E, Right ventriculography (45-de- gree left anterior oblique projection with 20-degree cranial projection).
ture, concluding that congenital aneurysmal formation of the membranous septum is a mild form of transposition, resulting from defective fusion of bulbar swelling. Another explanation is that the aneurysm develops in relation to spontaneous closure of the ventricular septal defect. The current case has findings that would fit either theory.
Aneurysms of the membranous ventricular septum may be an isolated finding or may occur with other cardiac mal- formations, particularly with primum type atria1 septal defect, ventricular septal defect, malformations of aortic or
pulmonary valves, subaortic stenosis, or aneurysms of the sinus of Valsalva.* Although aneurysms of the ventricular septum are usually asymptomatic, associated systemic emboli, cardiac arrhythmias, rupture or perforation of the aneurysm with a left-right shunt, and obstruction of the left ventricular outflow tract with hemodynamic distur- bance have been reported. 5-15 With the advent of ventric- ulography, the incidence of aneurysm of the ventricular septal defect in the last three decades is higher than that reported by Steinberg.’ The clinical diagnosis may be dif-
Volume 123
Number 3 Brief Communications 8 i 3
Fig. 4. A, Photograph at time of surgery showing large aneurysm. 6, Diagram of photograph shown in A.
ficult and indistinguishable from pulmonic or subpulmonic obstruction. Although this anomaly had been clearly dem- onstrated by angiography and transthoracic two-dimen- sional echocardiography, this case highlights the severe hemodynamic effects of the aneurysm, which resulted in significant and symptomatic right ventricular outflow tract obstruction, with the correct diagnosis established with both two-dimensional surface and, for the first time, transesophageal echocardiography prior to corrective sur- gery. In summary, aneurysms of the membranous septum are rare congenital lesions. Commonly asymptomatic, some aneurysms cause right ventricular outflow tract obstruc- tion or rupture and may be associated with septal defects. The presence of a septal aneurysm can be diagnosed by angiography, two-dimensional echocardiography and, most recently, transesophageal echocardiography. REFERENCES
1. Steinberg I. Diagnosis of congenital aneurysm of ventricular septum during life. Br Heart J 1957;19:8-12.
2.
3.
4.
5.
6.
7.
8.
9.
10.
Lev M, Saphir 0. Congenital aneurysm of the interventricular septum. J Tech Methods 1936;16:51-61. Mall FP. Aneurysm of the membranous septum projecting into right atrium. Anat Ret 1912;6:291. Lev M, Saphir 0. Congenital aneurysm of membranous sep- tum. Arch Path01 1938;25:819-24. Clarke RJ, White PD. Congenital aneurysmal defect of mem- branous portion of ventricular septum associated with heart block, ventricular Autter, Adam-Stokes syndrome and death. Circulation 1952;5:725-30. Rogers HM, Evaps IC, Dobmeier LH. Congenital aneurysm of membranous portion of the ventricular septum: report of two cases. AM HEART J 1952;43:781-90. Yarom R, Griffel B. Aneurysm of interventricular septum with subaortic stenosis. J Path01 Bacterial 1964;88:93-5. Varghese PJ, Izukerra T, Celermajer J, et al. Aneurvsms of the membranous ventricular septum: a method of spontaneous closure of small VSD. Am J Cardiol 1969:24:531-6. Das SK, Jahnke EJ, Walker WJ. Aneurysm of the membra- nous septum with interventricular septal defect producing right outflow tract obstruction. Circulation 1964;30:420-33. Persalo 0, Halonen PI, Pyorala K, et al. Aneurysm of the membranous ventricular septum causing obstruction of right
8 14 Brief Communications March 1992
American Heart Journal
ventricular outflow tract in case of VSD. Acta Chir Stand 1962;283:123-8.
11. Falsetti H, Anderson M. Aneurysm of membranous ventricu- lar septum producing right ventricular outflow tract obstruc- tion and left ventricular failure. Chest 1971;59:578-80.
12. Bonvicini G, Piovaccari G, Picchio FM. Severe subpulmonary obstruction caused by an aneurysmal tissue tag complicating an infundibular perimembranous ventricular septal defect. Br Heart J 1982;48:189-91.
13. Shumacker HB Jr, Glover J. Congenital aneurysms of the ventricular septum. AM HEART J 1963;66:405-8.
14. Canale JM, Sahn DJ, Valdes-Cruz LM, Allen HD, Goldberg SJ, Ovitt TW. Accuracy of two-dimensional echocardiography in detection of aneurysms of ventricular septum. AM HEART J 1981;101:255-9.
15. Yiannikas J, et al. Intravenous digital subtraction angiography to access aneurysms of ventricular and atria1 septum. Am J Cardiol 1984;53:383-5.
16. Laennec RTH. Traite de Pauscultation mediate et des mala- dies des poumons es du coeur. ed. 2. vol. 2. Paris: J.S. Chaude, 1865:547.
17. Mall FP. On the development of the human heart. Am J Anat 1912;13:249-54.
Hypertrophic cardiomyopathy progressing to a dilated cardiomyopathy-like feature in Noonan’s syndrome
Akihiko Shimizu, MD, Yasuhiko Oku, MD, Kiyotaka Matsuo, MD, and Kunitake Hashiba, MD. Nagasaki, Japan
The association of congenital heart disease with Noonan’s syndrome has been reported. Valvular pulmonary stenosis is the most common cardiac abnormality. Left-sided car-
From The Third Department of Internal Medicine, Nagasaki University School of Medicine.
Reprint requests: Akihiko Shimizu MD, The Third Department of Internal Medicine, Nagasaki University School of Medicine, Nagasaki University Hospital, 7-l Sakamoto-cho, Nagasaki, Japan 852. 414134498
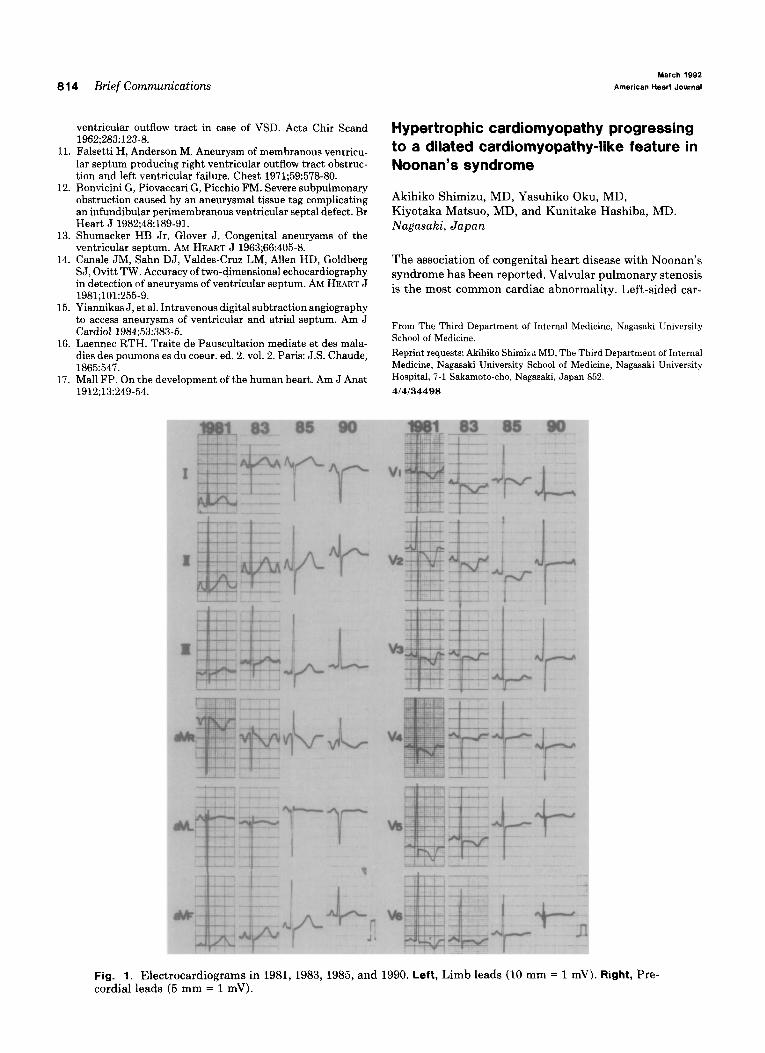
Fig. 1. Electrocardiograms in 1981,1983,1985, and 1990. Left, Limb leads (10 mm = 1 mV). cordial I eads (5 mm = 1 mV).