SHENENDEHOWA CENTRAL SCHOOL CLIFTON PARK, NEW YORK LIFEGUARD/LEAD LIFEGUARD REQUIREMENTS CERTIFICATION American Red Cross Lifeguard Certificate, is required. PROOF OF IDENTIFICATION Valid passport OR Driver’s license and original Social Security card OR Driver’s license and original birth certificate. MEASLES If born on or after January 1, 1957, applicant must show proof of immunization OR if born before January 1, 1957, must state whether or not they had the measles. IRS AND NYS WITHHOLDING FORMS Applicant must complete Federal and NYS income tax withholding forms. FINGERPRINTING Applicant will be subject to a fingerprint supported criminal history background check in accordance with SAVE Legislation effective July 1, 2001. Current Shenendehowa students are exempt from fingerprinting. All individuals required to be fingerprinted must contact the Office of Human Resources for your NCAC Code prior to scheduling your fingerprint appointment with MorphoTrust. HAZCOM All applicants are required to complete an on-line HAZCOM training session (Right to Know and hazardous materials in the workplace) before their application is processed, and annually thereafter. Please visit the Human Resources page of the District’s website for a direct link to take the on-line HAZCOM training, or go to: http://risk.capregboces.org/OnlineHazcom.htm PLEASE READ THE INSTRUCTIONS THOROUGHLY BEFORE YOU BEGIN. Failure to enter information correctly will result in re-taking the session. In addition, all Lifeguards/Lead Lifeguards will receive bloodborne pathogen information as a group at a later date. LIFEGUARD/LEAD LIFEGUARD PAY RATES Lifeguard (no experience) $9.70/hour Lifeguard (experience) $10.00/hour Lead Lifeguard (8 hour shift) $13.00/hour APPLICATIONS MUST BE PRESENTED IN PERSON Applications must be complete and applicant must have completed on-line HAZCOM training before application will be accepted for processing. Applications are accepted for processing at the Office of Human Resources, 5 Chelsea Place, Clifton Park, New York, by appointment only. Please call Michele Mastrianni at 881-0600, extension 68402 to schedule an appointment. Created 08/09 Revised 01/15, 06/17 mam
Transcript
SHENENDEHOWA CENTRAL SCHOOL CLIFTON PARK, NEW YORK
LIFEGUARD/LEAD LIFEGUARD REQUIREMENTS
CERTIFICATION American Red Cross Lifeguard Certificate, is required.
PROOF OF IDENTIFICATION Valid passport OR Driver’s license and original Social Security card OR Driver’s license and original birth certificate.
MEASLES If born on or after January 1, 1957, applicant must show proof of immunization OR if born before January 1, 1957, must state whether or not they had the measles.
IRS AND NYS WITHHOLDING FORMS Applicant must complete Federal and NYS income tax withholding forms.
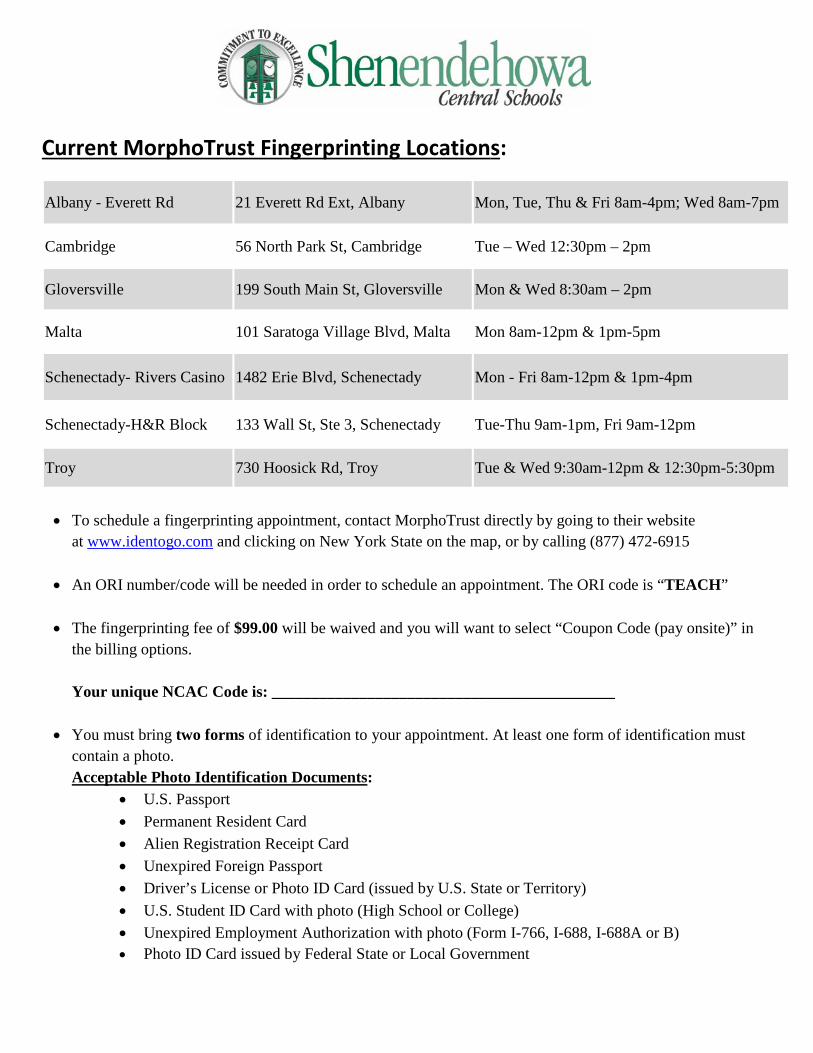
FINGERPRINTING Applicant will be subject to a fingerprint supported criminal history background check in accordance with SAVE Legislation effective July 1, 2001. Current Shenendehowa students are exempt from fingerprinting. All individuals required to be fingerprinted must contact the Office of Human Resources for your NCAC Code prior to scheduling your fingerprint appointment with MorphoTrust.
HAZCOM All applicants are required to complete an on-line HAZCOM training session (Right to Know and hazardous materials in the workplace) before their application is processed, and annually thereafter. Please visit the Human Resources page of the District’s website for a direct link to take the on-line HAZCOM training, or go to: http://risk.capregboces.org/OnlineHazcom.htm PLEASE READ THE INSTRUCTIONS THOROUGHLY BEFORE YOU BEGIN. Failure to enter information correctly will result in re-taking the session. In addition, all Lifeguards/Lead Lifeguards will receive bloodborne pathogen information as a group at a later date.
LIFEGUARD/LEAD LIFEGUARD PAY RATES
Lifeguard (no experience) $9.70/hour
Lifeguard (experience) $10.00/hour
Lead Lifeguard (8 hour shift) $13.00/hour
APPLICATIONS MUST BE PRESENTED IN PERSON
Applications must be complete and applicant must have completed on-line HAZCOM training before application will be accepted for processing. Applications are accepted for processing at the Office of Human Resources, 5 Chelsea Place, Clifton Park, New York, by appointment only. Please call Michele Mastrianni at 881-0600, extension 68402 to schedule an appointment.
• To schedule a fingerprinting appointment, contact MorphoTrust directly by going to their website
at www.identogo.com and clicking on New York State on the map, or by calling (877) 472-6915 • An ORI number/code will be needed in order to schedule an appointment. The ORI code is “TEACH”
• The fingerprinting fee of $99.00 will be waived and you will want to select “Coupon Code (pay onsite)” in
the billing options. Your unique NCAC Code is: ___________________________________________
• You must bring two forms of identification to your appointment. At least one form of identification must contain a photo. Acceptable Photo Identification Documents:
• U.S. Passport • Permanent Resident Card • Alien Registration Receipt Card • Unexpired Foreign Passport • Driver’s License or Photo ID Card (issued by U.S. State or Territory) • U.S. Student ID Card with photo (High School or College) • Unexpired Employment Authorization with photo (Form I-766, I-688, I-688A or B) • Photo ID Card issued by Federal State or Local Government
Date of Board Approval: _______________ Effective Date: _______________
Benefits Eligible Date: _______________ Original Date of Hire/Sub Date of Hire: _______________
Replacing: __________________________
Dual Position: Yes No
10mo 12mo __________ hrs./day
Term Hire _______________ to _______________
Paid Benefits: _____ Sick ______ Family Sick ______ Personal ______ Vacation ______ Professional Development
Aquatics Application
PERSONAL INFORMATION:
Name: Home Phone: Former Name(s): Work Phone: Address: Cell Phone:
e-mail:
Are you legally eligible for employment in this country? Yes No (In accordance with the Immigration Reform and Control Act of 1986, upon employment you will be asked to produce two original forms of identification.)
CERTIFICATION(S)/PROFESSIONAL LICENSE(S):
I hold the Certificate(s) described below: (Provide Copy) Date Issued Exp. Date
Lifeguard Certificate Yes No Lifeguard Instructor Certificate Yes No Water Safety Instructor Certificate Yes No Water Safety Instructor Trainer Certificate Yes No Please list other licenses held and issuing authority: Exp. Date:
EDUCATION:
Name and Location of School Major/Minor Degree College (Undergraduate)
College (Graduate)
Vocational/Technical/Trade
LIFEGUARD EXPERIENCE:
Name and Location of Organization/School Name of Supervisor Telephone Number Dates
RELATED EXPERIENCE:
Have you supervised other lifeguards? Yes No If yes, in what capacity? Have you managed or helped manage a pool? Yes No If yes, in what capacity?
EMERGENCY CONTACT INFORMATION:
Name: Home Phone: Relationship: Work Phone:
Cell Phone:
PLEASE ANSWER THE FOLLOWING QUESTIONS: Yes No
1) Have you ever resigned from a position rather than face disciplinary action?2) Has any disciplinary action been brought against you which resulted in you
being discharged from employment?3) Did you ever receive a discharge from the Armed Forces of the United States
which was other than “honorable” or which was issued under other thanhonorable circumstances?
4) Have you ever been convicted of any crime (felony or misdemeanor)?5) Are you now under charges for any crime (felony or misdemeanor)?6) Have you ever forfeited bail bond posted to guarantee your appearance
in court to answer any charges?7) Have you ever had a teaching or coaching credential revoked, suspended
or annulled?8) Have disciplinary proceedings ever been initiated against you pursuant to
New York State Education Law Section 3020 and/or Section 75 of the CivilService Law?
If you answered YES to any of the questions above, provide, on a separate sheet, the specifics or an explanation for the response. If you elect not to provide specifics, however, or if such an explanation is insufficient, your application may be denied.
AFFIDAVIT
Under penalties of perjury, I declare and affirm the statements made in the foregoing application, including accompanying statements and transcriptions, are true and correct.
Date: _________________________ _________________________________________________________ (signature of applicant)
Mark an X in the box if a newly hired employee or a rehired employee .......First date employee performed services for pay (mmddyyyy) (see instructions):
Are dependent health insurance benefits available for this employee? .............................. Yes No
If Yes, enter the date the employee qualifies (mmddyyyy) : ........
First name and middle initial Last name Social security number
Mailing address (number and street or PO box) Apartment number Date of birth (mmddyyyy)
City, village, or post office State ZIP code
Department of Taxation and Finance
Certificate of Exemption from WithholdingNew York State • New York City • Yonkers
Filing status: Mark an X in only one box
A Single B Married
C Qualifying widow(er) with dependent child, orhead of household withqualifying person ..............
To claim exemption from withholding for New York State personal income tax (and New York City and Yonkers personal income tax, if applicable), you must meet the conditions in either Group A or Group B:Group A
• you must be under age 18, or over age 65, or a full‑time student under age 25; and• you did not have a New York income tax liability for 2016; and• you do not expect to have a New York income tax liability for 2017 (for this purpose, you have a tax liability if your return shows tax
before the allowance of any credit for income tax withheld).Group B
• you meet the conditions set forth under the Servicemembers Civil Relief Act (SCRA), as amended by the Military Spouses Residency Relief Act. See Military spouses.
If you do not meet all of the conditions in either Group A or Group B above, stop; you cannot claim exemption from withholding (see Note below).
IT-2104-E
Instructions
Are you a full-time student?...... Yes No Are you a military spouse exempt under the SCRA? ..... Yes No
I certify that the information on this form is correct and that, for the year 2017, I expect to qualify for exemption from withholding of New York State income tax under section 671(a)(3) of the Tax Law or under the SCRA. I will notify my employer within 10 days of any change requiring revocation of the exemption from withholding as explained in the instructions.
Employer: complete this section only if you must send a copy of this form to the NYS Tax Department (see instructions).Employer name and address Employer identification number
Employee’s signature (give the completed certificate to your employer) Date
EmployeeWho qualifies – To claim exemption from withholding for New York State personal income tax (and New York City and Yonkers personal income tax, if applicable), you must meet the conditions in either Group A or Group B:
Group A• you must be under age 18, or over age 65, or a full‑time student
under age 25; and• you did not have a New York income tax liability for 2016; and• you do not expect to have a New York income tax liability for
2017 (for this purpose, you have a tax liability if your returnshows tax before the allowance of any credit for income taxwithheld).
Group B• you meet the conditions set forth under the Servicemembers
Civil Relief Act (SCRA), as amended by the Military Spouses Residency Relief Act. See Military spouses.
If you meet the conditions in Group A or Group B, file this certificate, Form IT‑2104‑E, with your employer. Otherwise, your employer must withhold New York State income tax (and New York City and
Yonkers personal income tax, if applicable) from your wages. Do not send this certificate to the Tax Department.
Generally, as a resident, you are required to file a New York State income tax return if you are required to file a federal income tax return, or if your federal adjusted gross income plus your New York additions is more than $4,000, regardless of your filing status. However, if you are single and can be claimed as a dependent on another person’s federal return, you must file a New York State return if your federal adjusted gross income plus your New York additions is more than $3,100.
If you are a nonresident and have income from New York sources, you must file a New York return if the sum of your federal adjusted gross income and New York additions to income is more than your New York standard deduction.
A penalty of $500 may be imposed for furnishing false information that decreases your withholding amount.
Note: If you do not qualify for exemption, or you want New York State, New York City, or Yonkers personal income tax withheld from your pay, file Form IT-2104, Employee’s Withholding Allowance Certificate, with your employer. Follow the instructions on Form IT‑2104 to determine the correct number of allowances to claim for withholding tax purposes.
This certificate will expire on April 30, 2018.
IT-2104-E (2017) (back)
When to claim exemption from withholding – File this certificate with your employer if you meet the conditions listed in Group A or Group B above. You must file a new certificate each year if you wish to continue to claim the exemption.
Military spouses – Under the Servicemembers Civil Relief Act (SCRA), as amended by the Military Spouses Residency Relief Act, you may be exempt from New York income tax (and New York City and Yonkers personal income tax, if applicable) on your wages if: 1) your spouse is a member of the armed forces present in NewYork in compliance with military orders; 2) you are present in New York solely to be with your spouse; and 3) you are domiciled in another state.
Liability for estimated tax – If, as a result of this exemption certificate, your employer does not withhold income tax from your wages and you later fail to qualify for exemption from tax, you may be required to pay estimated tax and be subject to penalty if it is not paid. For further information, see Form IT‑2105, Estimated Tax Payment Voucher for Individuals.
Multiple employers – If you have more than one employer, you may claim exemption from withholding with each employer as long as your total expected income will not cause you to incur a New York income tax liability for the year 2017 and you had no liability for 2016.
Revocation by employee – You must revoke this exemption certificate (1) within 10 days from the day you expect to incur a New York income tax liability for the year 2017, (2) on or before December 1, 2017, if you expect to incur a tax liability for 2018, or (3) when you no longer qualify for exemption under the SCRA.
If you are required to revoke this certificate, if you no longer meet the age requirements for claiming exemption, or if you want income tax withheld from your pay (because, for example, you expect your income to exceed $3,100), you must file Form IT-2104, Employee’s Withholding Allowance Certificate, with your employer. Follow the instructions on Form IT‑2104 to determine the correct number of allowances to claim for withholding tax purposes.
Filing status – Mark an X in one box on Form IT‑2104‑E that shows your present filing status for federal purposes.
EmployerKeep this certificate with your records. If an employee who claims exemption from withholding on Form IT‑2104‑E usually earns more than $200 per week, you must send a copy of that employee’s Form IT‑2104‑E to: NYS Tax Department, Income Tax Audit Administrator, Withholding Certificate Coordinator, W A Harriman Campus, Albany NY 12227-0865. See Publication 55, Designated Private Delivery Services, if not using U.S. Mail. If the employee is also a new hire or rehire, see Note below.
The Tax Department will not accept this form if it is incomplete. We will review these certificates and notify you of any adjustments that must be made.
Due dates for sending certificates received from employees who claim exemption and earn more than $200 per week are:Quarter Due date Quarter Due dateJanuary – March April 30 July – September October 31April – June July 31 October – December January 31
Revocation by employer – You must revoke this exemption within 10 days if, on any day during the calendar year, the date of birth stated on the certificate filed by the employee indicates the employee no longer meets the age requirements for exemption. The revocation must be in the form of a written notice to the employee.
New hires and rehires – Mark an X in the box if you are submitting a copy of this form to comply with New York State’s New Hire Reporting Program. A newly hired or rehired employee means an employee previously not employed by you, or previously employed by you but separated from such employment for 60 or more consecutive days. Enter the first day any services are performed for which the employee will be paid wages, commissions, tips and any other type of compensation. For services based solely on commissions, this is the first day an employee working for commissions is eligible to earn commissions. Also, mark an X in the Yes or No box indicating if dependent health insurance benefits are available to this employee. If Yes, enter the date the employee qualifies for coverage. Mail the completed form, within 20 days of hiring, to:
NYS TAX DEPARTMENTNEW HIRE NOTIFICATIONPO BOX 15119ALBANY NY 12212-5119
To report newly hired or rehired employees online go to www.nynewhire.com.
Note: If the newly hired or rehired employee has also claimed exemption from withholding but usually earns more than $200 per week, mail Form IT‑2104‑E to the Tax Department at the New Hire Notification address above.
Privacy notificationSee our website or Publication 54, Privacy Notification.
Need help? • Information and forms are available on the Tax Department’s website (at www.tax.ny.gov).• For help completing this form, employees may call (518) 457‑5181, and employers may call (518) 485‑6654.
First name and middle initial Last name Your social security number
Permanent home address (number and street or rural route) Apartment number
City,village,orpostoffice State ZIPcode
Are you a resident of New York City? ........... Yes NoAre you a resident of Yonkers? ..................... Yes NoComplete the worksheet on page 3 before making any entries.1 TotalnumberofallowancesyouareclaimingforNewYorkStateandYonkers,ifapplicable(from line 17) ........... 12 Total number of allowances for New York City (from line 28) .................................................................................. 2
Use lines 3, 4, and 5 below to have additional withholding per pay period under special agreement with your employer.
3 NewYorkStateamount ........................................................................................................................................ 34 New York City amount ........................................................................................................................................... 45 Yonkers amount .................................................................................................................................................... 5
Department of Taxation and Finance
Employee’s Withholding Allowance CertificateNew York State • New York City • Yonkers
SingleorHeadofhousehold Married
Married, but withhold at higher single rate
Note:Ifmarriedbutlegallyseparated,markanX in the Single or Head of household box.
IcertifythatIamentitledtothenumberofwithholdingallowancesclaimedonthiscertificate.Employee’s signature Date
Employer’s name and address (Employer: complete this section only if you are sending a copy of this form to the NYS Tax Department.) Employeridentificationnumber
Penalty – A penalty of $500 may be imposed for any false statement you make that decreases the amount of money you have withheld from your wages. You may also be subject to criminal penalties.
Employee: detach this page and give it to your employer; keep a copy for your records.
Changes effective for 2017FormIT-2104hasbeenrevisedfortaxyear2017.Theworksheetonpage3andthechartsbeginningonpage4,usedtocomputewithholdingallowancesortoenteranadditionaldollaramountonline(s)3,4,or5,havebeenrevised.IfyoupreviouslyfiledaFormIT-2104andusedtheworksheetorcharts,youshouldcompleteanew2017FormIT-2104andgive it to your employer.
Who should file this form Thiscertificate,FormIT-2104,iscompletedbyanemployeeandgiventotheemployertoinstructtheemployerhowmuchNewYorkState(andNew York City and Yonkers) tax to withhold from the employee’s pay. The more allowances claimed, the lower the amount of tax withheld.
IfyoudonotfileFormIT-2104,youremployermayusethesamenumberofallowancesyouclaimedonfederalFormW-4.Duetodifferencesintax law, this may result in the wrong amount of tax withheld for New York State,NewYorkCity,andYonkers.CompleteFormIT-2104eachyearandfileitwithyouremployerifthenumberofallowancesyoumayclaim
isdifferentfromfederalFormW-4orhaschanged.CommonreasonsforcompletinganewFormIT-2104eachyearincludethefollowing:• You started a new job.• You are no longer a dependent.• Your individual circumstances may have changed (for example, you
were married or have an additional child).• You moved into or out of NYC or Yonkers.• You itemize your deductions on your personal income tax return.• YouclaimallowancesforNewYorkStatecredits.• Youowedtaxorreceivedalargerefundwhenyoufiledyourpersonal
income tax return for the past year.• Yourwageshaveincreasedandyouexpecttoearn$107,650ormore
during the tax year.• Thetotalincomeofyouandyourspousehasincreasedto$107,650or
more for the tax year.• Youhavesignificantlymoreorlessincomefromothersourcesorfrom
another job.• You no longer qualify for exemption from withholding.
Instructions
Employer: Keep this certificate with your records.Mark an XinboxAand/orboxBtoindicatewhyyouaresendingacopyofthisformtoNewYorkState (see instructions):
A Employeeclaimedmorethan14exemptionallowancesforNYS ............ A
B Employee is a new hire or a rehire ... B First date employee performed services for pay (mm-dd-yyyy) (see instr.):
Aredependenthealthinsurancebenefitsavailableforthisemployee? ............. Yes No
• YouhavebeenadvisedbytheInternalRevenueServicethatyouare entitled to fewer allowances than claimed on your original federalFormW-4,andthedisallowedallowanceswereclaimedonyouroriginalFormIT-2104.
Exemption from withholdingYoucannotuseFormIT-2104toclaimexemptionfromwithholding.To claim exemption from income tax withholding, you mustfileFormIT-2104-E,Certificate of Exemption from Withholding, with your employer.Youmustfileanewcertificateeachyearthatyouqualifyforexemption. This exemption from withholding is allowable only if you had no New York income tax liability in the prior year, you expect none in the current year, andyouareover65yearsofage,under18,orafull-timestudentunder25.Youmayalsoclaimexemptionfromwithholdingifyou are a military spouse and meet the conditions set forth under the ServicemembersCivilReliefActasamendedbytheMilitarySpousesResidencyReliefAct.Ifyouareadependentwhoisunder18orafull-timestudent,youmayowetaxifyourincomeismorethan$3,100.
Withholding allowancesYou may not claim a withholding allowance for yourself or, if married, your spouse. Claim the number of withholding allowances you compute inPart1andPart3onpage3ofthisform.Ifyouwantmoretaxwithheld, you may claim fewer allowances. If you claim more than 14 allowances, your employer must send a copy of your Form IT-2104 totheNewYorkStateTaxDepartment.Youmaythenbeaskedtoverifyyourallowances.Ifyouarriveatnegativeallowances(lessthanzero)onlines1or2andyouremployercannotaccommodatenegativeallowances, enter 0 and see Additional dollar amount(s) below.
Income from sources other than wages –Ifyouhavemorethan$1,000ofincomefromsourcesotherthanwages(suchasinterest,dividends, or alimony received), reduce the number of allowances claimedonline1andline2(ifapplicable)oftheIT-2104certificatebyoneforeach$1,000ofnonwageincome.Ifyouarriveatnegativeallowances(less than zero), see Withholding allowances above. You may also considerfilingestimatedtax,especiallyifyouhavesignificantamountsof nonwage income. Estimated tax requires that payments be made by the employee directly to the Tax Department on a quarterly basis. For moreinformation,seetheinstructionsforFormIT-2105,Estimated Tax Payment Voucher for Individuals, or see Need help?onpage6.
Other credits (Worksheetline13) – Ifyouwillbeeligibletoclaimany credits other than the credits listed in the worksheet, such as an investment tax credit, you may claim additional allowances.
FindyourfilingstatusandyourNewYorkadjustedgrossincome(NYAGI)in the chart below, and divide the amount of the expected credit by the number indicated. Enter the result (rounded to the nearest whole number) online13.
Example: You are married and expect your New York adjusted gross income to be less than $323,200. In addition, you expect to receive a flow-through of an investment tax credit from the S corporation of which you are a shareholder. The investment tax credit will be $160. Divide the expected credit by 66. 160/66 = 2.4242. The additional withholding allowance(s) would be 2. Enter 2 on line 13.
Married couples with both spouses working –Ifyouandyourspousebothwork,youshouldeachfileaseparateIT-2104certificatewithyourrespective employers. Your withholding will better match your total tax if thehigherwage-earningspouseclaimsallofthecouple’sallowancesandthelowerwage-earningspouseclaimszeroallowances.Do not claim moretotalallowancesthanyouareentitledto.Ifyourcombinedwagesare:• lessthan$107,650,youshouldeachmarkanX in the box Married,
but withhold at higher single rateonthecertificatefront,anddividethe
totalnumberofallowancesthatyoucomputeonline17andline28(ifapplicable) between you and your working spouse.
• $107,650ormore,usethechart(s)inPart4andentertheadditionalwithholding dollar amount on line 3.
Taxpayers with more than one job –Ifyouhavemorethanonejob,fileaseparateIT-2104certificatewitheachofyouremployers.Besure to claim only the total number of allowances that you are entitled to. Your withholding will better match your total tax if you claim all of yourallowancesatyourhigher-payingjobandzeroallowancesatthelower-payingjob.Inaddition,tomakesurethatyouhaveenoughtax withheld, if you are a single taxpayer or head of household with two or more jobs, and your combined wages from all jobs are under $107,650,reducethenumberofallowancesbysevenonline1andline2(ifapplicable)onthecertificateyoufilewithyourhigher-payingjobemployer.Ifyouarriveatnegativeallowances(lessthanzero),see Withholding allowances above.
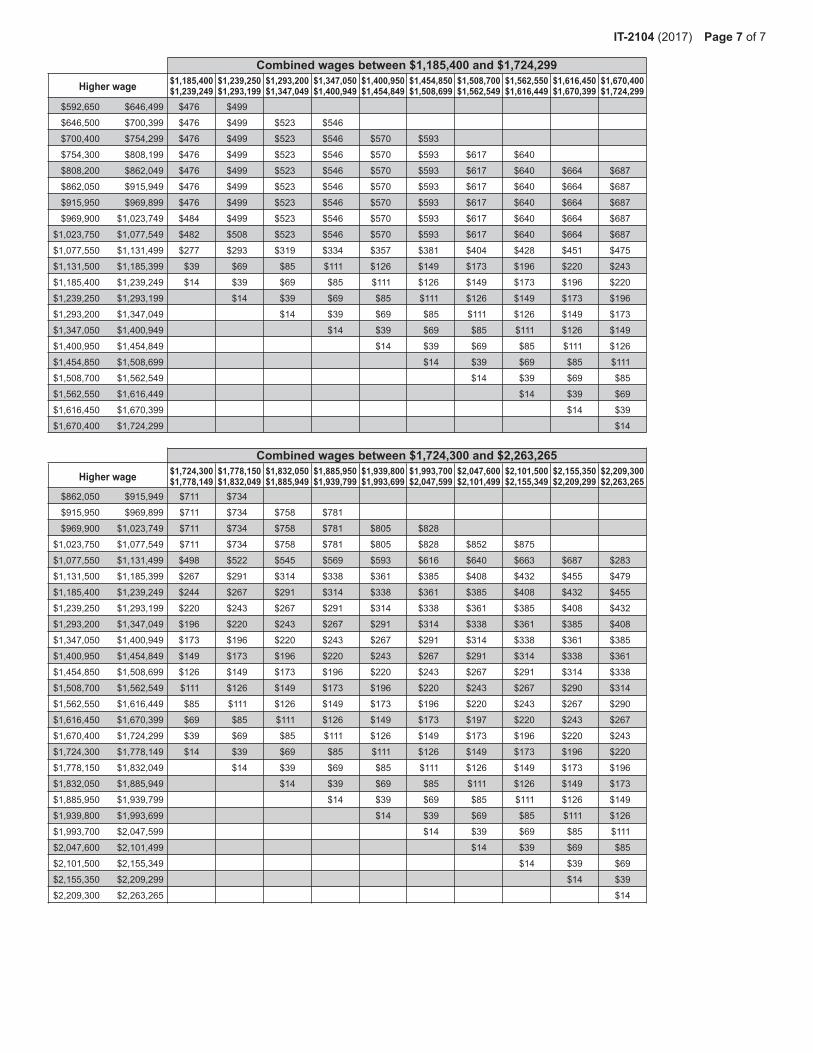
Ifyouareasingleoraheadofhouseholdtaxpayer,andyourcombinedwagesfromallofyourjobsarebetween$107,650and$2,263,265,usethe chart(s) in Part 5 and enter the additional withholding dollar amount from the chart on line 3.
Ifyouareamarriedtaxpayer,andyourcombinedwagesfromallofyourjobsare$107,650ormore,usethechart(s)inPart4andentertheadditionalwithholdingdollaramountfromthechartonline3(Substitutethe words Higher-paying job for Higher earner’s wages within the chart).
Dependents – Ifyouareadependentofanothertaxpayerandexpectyourincometoexceed$3,100,youshouldreduceyourwithholdingallowancesbyoneforeach$1,000ofincomeover$2,500.Thiswillensure that your employer withholds enough tax.
Following the above instructions will help to ensure that you will not owe additionaltaxwhenyoufileyourreturn.
Heads of households with only one job – Ifyouwillusethehead-of-householdfilingstatusonyourstateincometaxreturn,markthe Single or Head of householdboxonthefrontofthecertificate.Ifyouhave only one job, you may also wish to claim two additional withholding allowancesonline14.
Additional dollar amount(s)You may ask your employer to withhold an additional dollar amount each payperiodbycompletinglines3,4,and5onFormIT-2104.Inmostinstances, if you compute a negative number of allowances and your employer cannot accommodate a negative number, for each negative allowanceclaimedyoushouldhaveanadditional$1.85oftaxwithheldperweekforNewYorkStatewithholdingonline3,andanadditional$0.80oftaxwithheldperweekforNewYorkCitywithholdingonline4.Yonkersresidentsshoulduse16.75%(.1675)oftheNewYorkStateamountforadditional withholding for Yonkers on line 5.
Note:Ifyouarerequestingyouremployertowithholdanadditionaldollaramountonlines3,4,or5ofthisallowancecertificate,theadditionaldollar amount, as determined by these instructions or by using the chart(s)inPart4orPart5,isaccurateforaweeklypayroll.Therefore,if you are not paid on a weekly basis, you will need to adjust the dollar amount(s) that you compute. For example, if you are paid biweekly, you must double the dollar amount(s) computed.
Avoid underwithholdingFormIT-2104,togetherwithyouremployer’swithholdingtables,isdesigned to ensure that the correct amount of tax is withheld from your pay. Ifyoufailtohaveenoughtaxwithheldduringtheentireyear,youmayowealargetaxliabilitywhenyoufileyourreturn.TheTaxDepartmentmustassess interest and may impose penalties in certain situations in addition tothetaxliability.Evenifyoudonotfileareturn,wemaydeterminethat you owe personal income tax, and we may assess interest and penalties on the amount of tax that you should have paid during the year.
Single andNYAGI is:
Head of household and NYAGI is:
Married and NYAGI is:
Divide amount of expected credit by:
Less than Less than Less than 66$215,400 $269,300 $323,200Between Between Between$215,400and $269,300and $323,200and 68 $1,077,550 $1,616,450 $2,155,350
Over Over Over 88$1,077,550 $1,616,450 $2,155,350
(continued)
IT-2104 (2017) Page 3 of7
WorksheetSee the instructions before completing this worksheet.
Part 1 – Complete this part to compute your withholding allowances for New York State and Yonkers (line1).
Part 3 – Complete this part to compute your withholding allowances for New York City (line2).
Part 2 – Complete this part only if you expect to itemize deductions on your state return.
18 Enter your estimated federal itemized deductions for the tax year ........................................................................................... 1819 Enteryourestimatedstate,local,andforeignincometaxesorstateandlocalgeneralsalestaxesincludedonline18 ........ 1920 Subtractline19fromline18 .................................................................................................................................................... 2021 Enter your estimated college tuition itemized deduction .......................................................................................................... 2122 Addlines20and21 ................................................................................................................................................................. 2223 Basedonyourfederalfilingstatus,entertheapplicableamountfromthetablebelow ........................................................... 23
24 Subtractline23fromline22(if line 23 is larger than line 22, enter 0 here and on line 16 above) ....................................................... 2425 Divideline24by$1,000.Dropanyfractionandentertheresulthereandonline16above ................................................... 25
6 Enter the number of dependents that you will claim on your state return (do not include yourself or, if married, your spouse) ..... 6 For lines 7, 8, and 9, enter 1 for each credit you expect to claim on your state return. 7 College tuition credit .................................................................................................................................................................. 7 8 NewYorkStatehouseholdcredit ............................................................................................................................................... 8 9 Realpropertytaxcredit .............................................................................................................................................................. 9 For lines 10, 11, and 12, enter 3 for each credit you expect to claim on your state return.
10 Child and dependent care credit ................................................................................................................................................ 1011 Earned income credit ................................................................................................................................................................. 11
12 EmpireStatechildcredit ............................................................................................................................................................ 1213 Other credits (see instructions) ...................................................................................................................................................... 1314 Headofhouseholdstatusand only one job (enter 2 if the situation applies) ................................................................................... 1415 Enter an estimate of your federal adjustments to income, such as alimony you will pay for the tax year
16 Ifyouexpecttoitemizedeductionsonyourstatetaxreturn,completePart2belowandenterthenumberfromline25.All others enter 0 ................................................................................................................................................................... 16
17 Addlines6through16.Entertheresulthereandonline1.Ifyouhavemorethanonejob,orifyouandyourspousebothwork, see instructions for Taxpayers with more than one job or Married couples with both spouses working. ..................... 17
Standard deduction table
EmployersBox A – Ifyouarerequiredtosubmitacopyofanemployee’sFormIT-2104totheTaxDepartmentbecausetheemployeeclaimedmorethan14allowances,markanX in box A and send a copy ofFormIT-2104to:NYS Tax Department, Income Tax Audit Administrator, Withholding Certificate Coordinator, W A Harriman Campus, Albany NY 12227-0865.Iftheemployeeisalsoanewhireorrehire, see Box Binstructions.SeePublication55,Designated Private Delivery Services,ifnotusingU.S.Mail.
Duedatesforsendingcertificatesreceivedfromemployeesclaimingmorethan14allowancesare:Quarter Due date Quarter Due dateJanuary–March April30 July–September October31April–June July31 October–December January31
Box B – IfyouaresubmittingacopyofthisformtocomplywithNewYorkState’sNewHireReportingProgram,markanX in box B. Enter the firstdayanyservicesareperformedforwhichtheemployeewillbepaidwages, commissions, tips and any other type of compensation. For servicesbasedsolelyoncommissions,thisisthefirstdayanemployeeworking for commissions is eligible to earn commissions. Also, mark an X in the Yes or Noboxindicatingifdependenthealthinsurancebenefitsareavailabletothisemployee.IfYes,enterthedatetheemployeequalifiesforcoverage.Mailthecompletedform,within20daysofhiring,to:NYS Tax Department, New Hire Notification, PO Box 15119, Albany NY 12212-5119. Toreportnewly-hiredorrehiredemployeesonlineinsteadofsubmitting this form, go to www.nynewhire.com.
Page 4 of7 IT-2104 (2017)
Part 4 – These charts are only for married couples with both spouses working or married couples with one spouse working more than onejob,andwhosecombinedwagesarebetween$107,650and$2,263,265.
Enter the additional withholding dollar amount on line 3.
Theadditionaldollaramount,asshownbelow,isaccurateforaweeklypayroll.Ifyouarenotpaidonaweeklybasis,youwillneedtoadjust these dollar amount(s). For example, if you are paid biweekly, you must double the dollar amount(s) computed.
Combined wages between $107,650 and $538,749Higher earner’s wages
Ifyouareinoneofthesesituationsandyouwouldliketorequestanadditionaldollaramountofwithholdingfromyourwages,pleasecontacttheTaxDepartment for assistance (see Need help?onpage6).
Part 5 – These charts are only for single taxpayers and head of household taxpayers with more than one job, and whose combined wagesarebetween$107,650and$2,263,265.
Enter the additional withholding dollar amount on line 3.
Theadditionaldollaramount,asshownbelow,isaccurateforaweeklypayroll.Ifyouarenotpaidonaweeklybasis,youwillneedtoadjust these dollar amount(s). For example, if you are paid biweekly, you must double the dollar amount(s) computed.
Employment Eligibility Verification Department of Homeland Security
U.S. Citizenship and Immigration Services
Form I-9 11/14/2016 N Page 1 of 3
►START HERE: Read instructions carefully before completing this form. The instructions must be available, either in paper or electronically,during completion of this form. Employers are liable for errors in the completion of this form.
ANTI-DISCRIMINATION NOTICE: It is illegal to discriminate against work-authorized individuals. Employers CANNOT specify which document(s) an employee may present to establish employment authorization and identity. The refusal to hire or continue to employ an individual because the documentation presented has a future expiration date may also constitute illegal discrimination.
Section 1. Employee Information and Attestation (Employees must complete and sign Section 1 of Form I-9 no laterthan the first day of employment, but not before accepting a job offer.)Last Name (Family Name) First Name (Given Name) Middle Initial Other Last Names Used (if any)
Address (Street Number and Name) Apt. Number City or Town State ZIP Code
Date of Birth (mm/dd/yyyy) U.S. Social Security Number
- -
Employee's E-mail Address Employee's Telephone Number
I am aware that federal law provides for imprisonment and/or fines for false statements or use of false documents in connection with the completion of this form.I attest, under penalty of perjury, that I am (check one of the following boxes):
1. A citizen of the United States
2. A noncitizen national of the United States (See instructions)
3. A lawful permanent resident
4. An alien authorized to work until (See instructions)
(expiration date, if applicable, mm/dd/yyyy):
(Alien Registration Number/USCIS Number):
Some aliens may write "N/A" in the expiration date field.
Aliens authorized to work must provide only one of the following document numbers to complete Form I-9: An Alien Registration Number/USCIS Number OR Form I-94 Admission Number OR Foreign Passport Number.
1. Alien Registration Number/USCIS Number:
2. Form I-94 Admission Number:
3. Foreign Passport Number:
Country of Issuance:
OR
OR
QR Code - Section 1 Do Not Write In This Space
Signature of Employee Today's Date (mm/dd/yyyy)
Preparer and/or Translator Certification (check one): I did not use a preparer or translator. A preparer(s) and/or translator(s) assisted the employee in completing Section 1.(Fields below must be completed and signed when preparers and/or translators assist an employee in completing Section 1.)I attest, under penalty of perjury, that I have assisted in the completion of Section 1 of this form and that to the best of my knowledge the information is true and correct.Signature of Preparer or Translator Today's Date (mm/dd/yyyy)
Last Name (Family Name) First Name (Given Name)
Address (Street Number and Name) City or Town State ZIP Code
Employer Completes Next Page
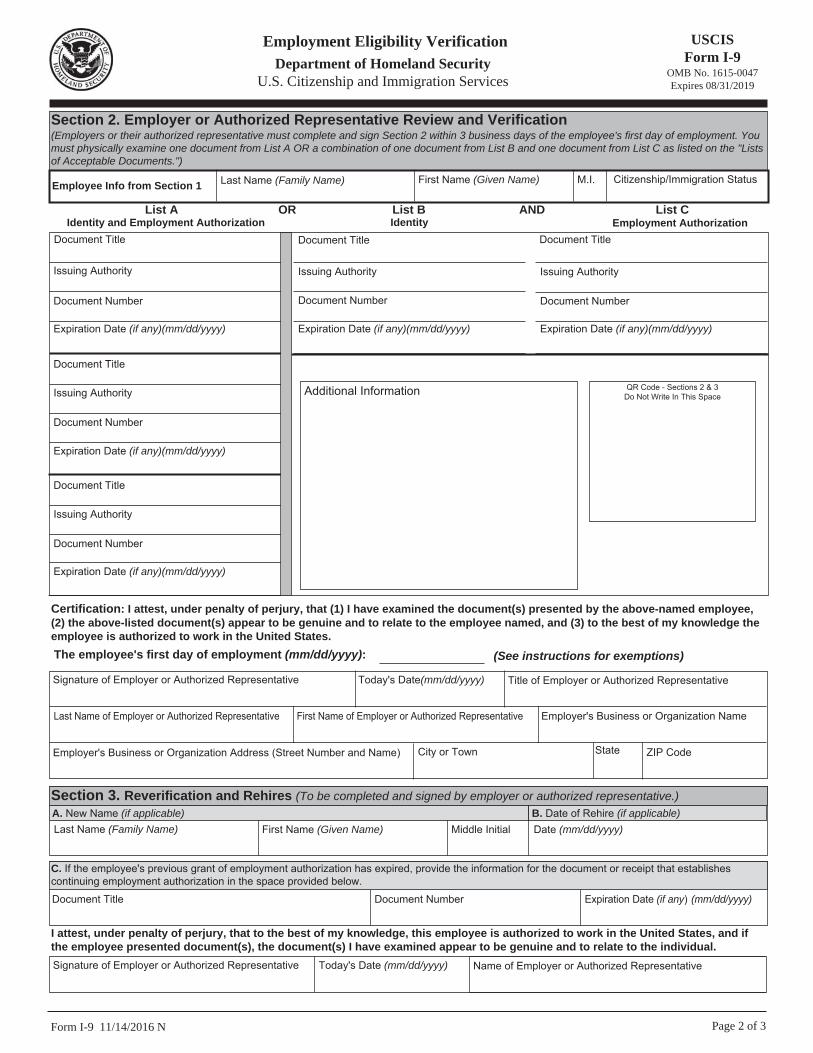
Form I-9 11/14/2016 N Page 2 of 3
USCIS Form I-9
OMB No. 1615-0047 Expires 08/31/2019
Employment Eligibility Verification Department of Homeland Security
U.S. Citizenship and Immigration Services
Section 2. Employer or Authorized Representative Review and Verification (Employers or their authorized representative must complete and sign Section 2 within 3 business days of the employee's first day of employment. You must physically examine one document from List A OR a combination of one document from List B and one document from List C as listed on the "Lists of Acceptable Documents.")
Last Name (Family Name) M.I.First Name (Given Name)Employee Info from Section 1 Citizenship/Immigration Status
List AIdentity and Employment Authorization Identity Employment Authorization
OR List B AND List C
Additional Information QR Code - Sections 2 & 3 Do Not Write In This Space
Document Title
Issuing Authority
Document Number
Expiration Date (if any)(mm/dd/yyyy)
Document Title
Issuing Authority
Document Number
Expiration Date (if any)(mm/dd/yyyy)
Document Title
Issuing Authority
Document Number
Expiration Date (if any)(mm/dd/yyyy)
Document Title
Issuing Authority
Document Number
Expiration Date (if any)(mm/dd/yyyy)
Document Title
Issuing Authority
Document Number
Expiration Date (if any)(mm/dd/yyyy)
Certification: I attest, under penalty of perjury, that (1) I have examined the document(s) presented by the above-named employee, (2) the above-listed document(s) appear to be genuine and to relate to the employee named, and (3) to the best of my knowledge the employee is authorized to work in the United States. The employee's first day of employment (mm/dd/yyyy): (See instructions for exemptions)
Signature of Employer or Authorized Representative Today's Date(mm/dd/yyyy) Title of Employer or Authorized Representative
Last Name of Employer or Authorized Representative First Name of Employer or Authorized Representative Employer's Business or Organization Name
Employer's Business or Organization Address (Street Number and Name) City or Town State ZIP Code
Section 3. Reverification and Rehires (To be completed and signed by employer or authorized representative.)A. New Name (if applicable)Last Name (Family Name) First Name (Given Name) Middle Initial
B. Date of Rehire (if applicable)Date (mm/dd/yyyy)
Document Title Document Number Expiration Date (if any) (mm/dd/yyyy)
C. If the employee's previous grant of employment authorization has expired, provide the information for the document or receipt that establishes continuing employment authorization in the space provided below.
I attest, under penalty of perjury, that to the best of my knowledge, this employee is authorized to work in the United States, and if the employee presented document(s), the document(s) I have examined appear to be genuine and to relate to the individual. Signature of Employer or Authorized Representative Today's Date (mm/dd/yyyy) Name of Employer or Authorized Representative
LISTS OF ACCEPTABLE DOCUMENTSAll documents must be UNEXPIRED
Employees may present one selection from List A or a combination of one selection from List B and one selection from List C.
LIST A
2. Permanent Resident Card or AlienRegistration Receipt Card (Form I-551)
1. U.S. Passport or U.S. Passport Card
3. Foreign passport that contains atemporary I-551 stamp or temporaryI-551 printed notation on a machine-readable immigrant visa
4. Employment Authorization Documentthat contains a photograph (FormI-766)
5. For a nonimmigrant alien authorizedto work for a specific employerbecause of his or her status:
Documents that Establish Both Identity and
Employment Authorization
6. Passport from the Federated States ofMicronesia (FSM) or the Republic ofthe Marshall Islands (RMI) with FormI-94 or Form I-94A indicatingnonimmigrant admission under theCompact of Free Association Betweenthe United States and the FSM or RMI
b. Form I-94 or Form I-94A that hasthe following:(1) The same name as the passport;
and(2) An endorsement of the alien's
nonimmigrant status as long as that period of endorsement has not yet expired and the proposed employment is not in conflict with any restrictions or limitations identified on the form.
a. Foreign passport; and
For persons under age 18 who are unable to present a document
listed above:
1. Driver's license or ID card issued by aState or outlying possession of theUnited States provided it contains aphotograph or information such asname, date of birth, gender, height, eyecolor, and address
9. Driver's license issued by a Canadiangovernment authority
3. School ID card with a photograph
6. Military dependent's ID card
7. U.S. Coast Guard Merchant MarinerCard
8. Native American tribal document
10. School record or report card
11. Clinic, doctor, or hospital record
12. Day-care or nursery school record
2. ID card issued by federal, state or localgovernment agencies or entities,provided it contains a photograph orinformation such as name, date of birth,gender, height, eye color, and address
4. Voter's registration card
5. U.S. Military card or draft record
Documents that Establish Identity
LIST B
OR AND
LIST C
8. Employment authorizationdocument issued by theDepartment of Homeland Security
1. A Social Security Account Numbercard, unless the card includes one ofthe following restrictions:
2. Certification of Birth Abroad issuedby the Department of State (FormFS-545)
3. Certification of Report of Birthissued by the Department of State(Form DS-1350)
4. Original or certified copy of birthcertificate issued by a State,county, municipal authority, orterritory of the United Statesbearing an official seal
5. Native American tribal document
7. Identification Card for Use ofResident Citizen in the UnitedStates (Form I-179)
Documents that Establish Employment Authorization
6. U.S. Citizen ID Card (Form I-197)
(2) VALID FOR WORK ONLY WITHINS AUTHORIZATION
(3) VALID FOR WORK ONLY WITH DHS AUTHORIZATION
(1) NOT VALID FOR EMPLOYMENT
Page 3 of 3Form I-9 11/14/2016 N
Examples of many of these documents appear in Part 8 of the Handbook for Employers (M-274).
Refer to the instructions for more information about acceptable receipts.
Dear New Employee:
In the past, our District has encountered situations pertaining to an outbreak of measles. This has sometimes caused a disruption to the educational programs available to the students at Shenendehowa and has necessitated an employee(s) exclusion from employment for a period of time.
Due to a recommended guideline from the New York State Department of Health and to avoid a disruption to our educational program in the event of an outbreak, we are requesting your cooperation in the completion of the form found at the bottom of this page.
Please return this form, with any required documentation, to the Office of the Assistant Superintendent for Human Resources as soon as possible. Thank you.
Name of Employee _____________________ Date of Birth ___________ (Please Print)
A. I hereby certify that I was born prior to January 1, 1957 and recall that I did/did not (circle one) have a case of measles.
______________________________ ________________________ (Signature of Employee) (Date)
OR
B. Employees born after January 1, 1957 must provide written documentation in one of the following categories which are acceptable proofs of immunity to measles.
1. Live virus measles* vaccine administered after January1, 1967 in an individual one year of age or older, OR
2. Physician-diagnosed history of clinical measles,written by the physician who actually saw and diagnosedthe disease, OR
3. Serologic (blood) evidence of previous measlesinfection.
*Either as single measles shot or combined with rubella (MR) or withrubella and mumps (MMR).
Thank you for your cooperation in this most important matter.
Sincerely,
Anthony Marinello, M.D.
Anthony Marinello, M.D., Ph.D. Chief School Physician
VOLUNTARY SELF-IDENTIFICATION FORM
The Shenendehowa Central School District is committed to the employment and advancement of minorities, females, individuals with disabilities and veterans. Please assist the District by providing the information requested below.
Providing this information is voluntary and providing or refusing to provide it will not subject you to any adverse treatment. The information provided will be held in the strictest confidence, will be maintained in a separate file and will only be used for equal employment/affirmative action recordkeeping and reporting required by law.
Principal Principal’s Aide Assistant Principal Computer Lab Aide/School Technologists/Systems Elementary Teacher Analysts/Sr. AV Tech/Computer Services Program Secondary Teacher Assistant/Microcomputer Systems Coordinator School Counselor Clerical School Psychologist/Social Worker Transportation/Food Service/Facilities & Operations Librarian Building Maintenance Mechanics Professional Development Grounds
Gender: Please check one. Female Male
Race/Ethnic Identification: Please check one. Please refer to federal government definitions below. White (Not of Hispanic origin) Black (Not of Hispanic origin) Hispanic Asian or Pacific Islander American Indian or Alaskan Native Two or more races (Not of Hispanic origin)
______________________________________ __________________________ Signature Date
White (Not of Hispanic origin) – All persons having origins in any of the original peoples of Europe, North Africa or the Middle East.
Black (Not of Hispanic origin) – All persons having origins in any of the black racial groups of Africa.
Hispanic – All persons of Mexican, Puerto Rican, Cuban, Central or South American, or other Spanish culture or origin, regardless of race.
Asian or Pacific Islander – All persons having origins in any of the original peoples of the Far East, Southeast Asia, the Indian subcontinent, or the Pacific Islands. The areas include, for example, China, Japan, Korea, India, the Philippine Islands and Samoa.
American Indian or Alaskan Native – All persons having origins in any of the original peoples of North America, and who maintain cultural identification through tribal affiliation or community recognition.
Retirement System Information This is to advise you that Governor Cuomo signed into Law Chapter 878 of the Laws of 1986. This enactment, which took effect August 2, 1986, provides that individuals eligible for membership in the New York State Employees’ Retirement System, MUST acknowledge the fact that employers have advised them of the right to join the system.
Please read the following statement, then sign and date below:
I hereby acknowledge that I have been informed by Shenendehowa Central School, my employer, that as a classified and/or substitute employee, I may, as a matter of right, join the New York State Employees’ Retirement System. I further acknowledge that I understand under present law if I elect to join the New York State Employees’ Retirement System, I MUST COMPLETE A MEMBERSHIP APPLICATION WHICH MUST BE FILED WITH THE RETIREMENT SYSTEM. I WILL BE REQUIRED TO CONTRIBUTE A SPECIFIC PERCENTAGE OF MY SALARY TO SAID RETIREMENT SYSTEM.*
~ OR ~ RETIRED MEMBER from: (NYSTRS or NYSERS or NYSPF or NYCTRS or NYCERS or NYCPF) Please circle one if you have already retired through any of the above retirement systems.
I am not currently a member of the Employees’ Retirement System.
I understand that I have a right to join the Employees’ Retirement System.
I understand that part time employment (i.e. anything less than full time, 12 month employment for the Employees’ Retirement System) does not require that I join the Retirement System.
I elect not to join at this time. If I choose to join in the future, I will notify the Human Resources Office.
Shenendehowa Central Schools • Human Resources Office • 5 Chelsea Place, Clifton Park, NY 12065 • (518) 881-0600
403(b) UNIVERSAL AVAILABILITY NOTICE
This notice is to inform you that as an employee of the Shenendehowa Central School District, you are eligible to participate in the District-sponsored 403(b) retirement plan.
Who is eligible? Shenendehowa Central School District’s 403(b) Plan allows for all full-time, part-time, and substitute employees to participate in the Plan. If you are currently not a contributing member and wish to become one, you must first open an account with one of the District’s approved Investment Service Providers. You many only select an Investment Service Provider that has been approved by Shenendehowa CSD.
Who is an Approved Investment Service Provider? The OMNI Group is the designated 403(b) Plan Third-Party Administrator (TPA). A list of the Plan’s participating investment providers may be viewed on OMNI’s website (www.omni403b.com) after submitting your Employer’s name and state (Shenendehowa CSD, NY).
How Can I Participate? You can participate in the Plan with pre-tax contributions by submitting a Salary Reduction Agreement (“SRA”) online via OMNI’s website or by submitting a completed SRA form, found on the same website, to OMNI either by facsimile to (585) 672-6194 or by mail to 1099 Jay Street, Building F, Rochester, NY 14611. Prior to contributing you must open an account with an investment provider participating in the Plan.
What If I Do Not Want To Contribute? If you do not want to take advantage of this program, simply submit an SRA with the option “I do not wish to participate at this time” selected. See directions above for on-line and paper submission options.
Questions? If you have any questions, please contact The OMNI Group at 877-544-6664. We recommend that all employees view a brief, 3 minute video presentations called ‘403(b). Why me?’ explaining a 403(b) plan, and how to contribute. The video can be viewed on OMNI’s website at www.omni403b.com.
Confirmation of Notice
I, _______________________________________, as an employee of the Shenendehowa Central School District, was offered the option to participate in the District-sponsored 403(b) retirement plan.
I hereby authorize Shenendehowa CSD to initiate credit entries to my checking and/or savings account (select one or both) at the depository named below.
Employee Name Building
Employee Signature Date
A copy of a voided check or any pre-printed document from your checking account with appropriate bank
information, including employee name, bank name, account number and routing number must be attached.
CHECKING SAVINGS NEW CHANGE ADD TO EXISTING CANCEL
DEPOSITORY/BANK NAME:
ROUTING NUMBER:
ACCOUNT NUMBER:
FLAT AMOUNT OR % OF NET PAY:
CHECKING SAVINGS NEW CHANGE ADD TO EXISTING CANCEL
DEPOSITORY/BANK NAME:
ROUTING NUMBER:
ACCOUNT NUMBER:
FLAT AMOUNT OR % OF NET PAY:
CHECKING SAVINGS NEW CHANGE ADD TO EXISTING CANCEL
DEPOSITORY/BANK NAME:
ROUTING NUMBER:
ACCOUNT NUMBER:
FLAT AMOUNT OR % OF NET PAY:
CHECKING SAVINGS NEW CHANGE ADD TO EXISTING CANCEL
DEPOSITORY/BANK NAME:
ROUTING NUMBER:
ACCOUNT NUMBER:
FLAT AMOUNT OR % OF NET PAY:
This authorization is to remain in effect until Shenendehowa CSD has received written notification from me
of its termination to afford Shenendehowa CSD and DEPOSITORY a reasonable opportunity to act on it.
**The first two pay periods after set up, a pre-note process is initiated, where information regarding your account is sentto the financial institution, but no monies are sent. The next period, the monies will be sent electronically. If you are making a change to the flat dollar amount only, no pre-note will be necessary and no delay in electronic deposits will occur. **
For Payroll office use only
Prenote Checkdate #1: Prenote Checkdate #2: Live Deposit Checkdate: