33
SHOCK! SHOCK RECOGNITION AND FIRST STEPS CHRISTOPHER S. AMATO, MD, FACEP, FAAP MORRISTOWN MEDICAL / GORYEB CHILDREN’S HOSPITAL MORRISTOWN, NJ ENVISION PHYSICIANS GROUP

SHOCK!SHOCK RECOGNITION AND FIRST
STEPS
CHRISTOPHER S. AMATO, MD, FACEP, FAAP
MORRISTOWN MEDICAL / GORYEB CHILDREN’S HOSPITAL
MORRISTOWN, NJ
ENVISION PHYSICIANS GROUP

OBJECTIVES
Discuss myths and advantages/complications of standard peripheral line placement vs. IO placement vs. ultrasound guided line placement vs. UVC line in the neonate.
Discuss the use of goal-directed therapy in pediatrics.
Describe the assessment, treatment, and resuscitation of the pediatric patient in shock.
Illustrate new literature and the use of goal-directed therapy in pediatrics.
Review the thoughtful use of fluids in sepsis management.

READY…
…..Set….…IDENTIFY!!!
PUMP
TANK PIPES

LETS MAKE THIS SIMPLE
Insufficient circulating blood volume (preload)
Changes in vascular resistance (afterload)
Heart failure (contractility)
Obstruction to blood flow

IDENTIFICATION
https://www.google.com/search?biw=1600&bih=789&tbm=isch&sa=1&ei=JbRZXJLKLcGs5wKEnp7IBA&q=gif%2C+weakness%2C+disney&oq=gif%2C+weakness%2C+disney&gs_l=img.3...21715.26559..26941...1.0..0.153.945.5j4......1....1..gws-wiz-img.......0i8i30.N4g2qjBdOU0#imgrc=xkdqE-KfAP1PNM:
https://www.google.com/search?q=gif,+fatigue&tbm=isch&source=hp&sa=X&ved=2ahUKEwj-6ZOL_KTgAhVNzlkKHe2WBUoQsAR6BAgAEAE&biw=1600&bih=789#imgrc=VD8oPlRdVj1_YM:tps://www.google.com/search?q=gif,+fatigue&tbm=isch&source=iu&ictx=1&fir
nwYUQ76rciNGzM%253A%252CsNjZl9XJ9HNJ9M%252C_&usg=AI4_-QzeN81Ers0q4SIQrBoKcmtxMFDjQ&sa=X&ved=2ahUKEwj-ZOL_KTgAhVNzlkKHe2WBUoQ9QEwAXoECAAQBg#imgrc=nwYUQ76rciGzM:
https://www.google.com/search?tbm=isch&sa=1&ei=ZbVZXNvbE-qb5wLBxKWIBA&q=dizziness+gif%2C+donald+duck&oq=dizziness+gif%2C+donald+duck&gs_l=img.3...35479.41511..41797...2.0..0.174.1620.1j12......1....1..gws-wiz-img.ioSW96YMPUY#imgdii=SMnkSbCDZip7KM:&imgrc=UHP9gmE5hOpJIM:
https://www.google.com/search?tbm=isch&sa=1&ei=kLVZXLH6C4mc5wKe_7q4BA&q=shock+gif%2C+minnie+mouse&oq=shock+gif%2C+minnie+mouse&gs_l=img.3...158851.168810..169217...1.0..0.188.3344.13j16......1....1..gws-wiz-img.......0i8i7i30j0j0i8i30.Pkszx5NOpLA#imgrc=vdgFTSZUAZ2eXM:
FATIGUEMALAISE
WEAKNESS
DIZZINESS
AMS/ Syncope
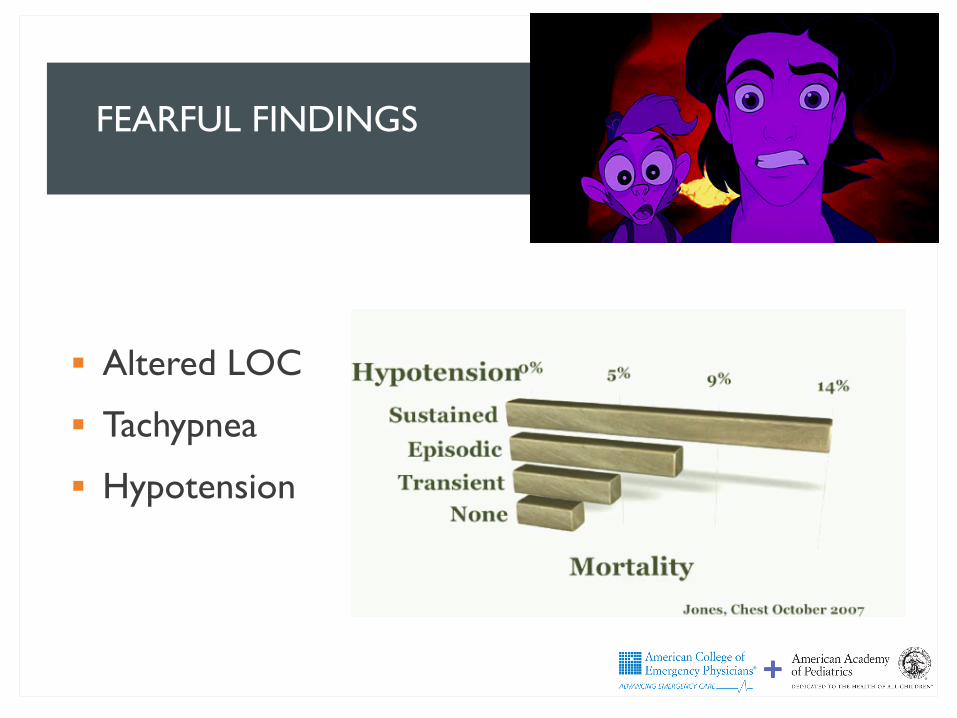
FEARFUL FINDINGS
Altered LOC
Tachypnea
Hypotension

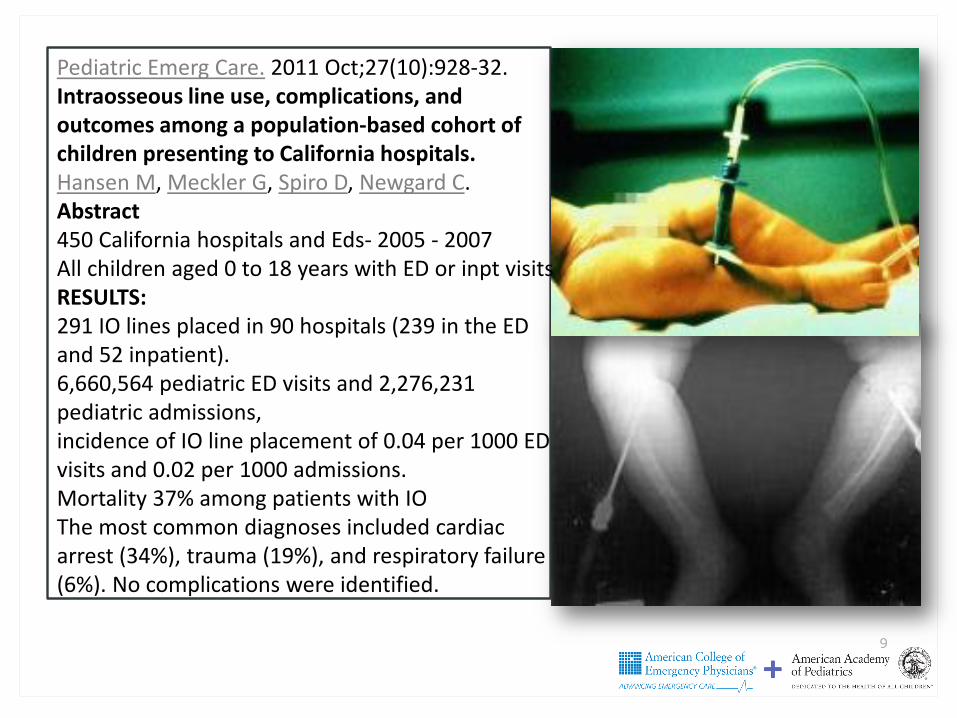
INTRAOSSEOUS9
Pediatric Emerg Care. 2011 Oct;27(10):928-32.Intraosseous line use, complications, and outcomes among a population-based cohort of children presenting to California hospitals.Hansen M, Meckler G, Spiro D, Newgard C.Abstract450 California hospitals and Eds- 2005 - 2007All children aged 0 to 18 years with ED or inpt visits RESULTS: 291 IO lines placed in 90 hospitals (239 in the ED and 52 inpatient). 6,660,564 pediatric ED visits and 2,276,231 pediatric admissions, incidence of IO line placement of 0.04 per 1000 ED visits and 0.02 per 1000 admissions. Mortality 37% among patients with IOThe most common diagnoses included cardiac arrest (34%), trauma (19%), and respiratory failure (6%). No complications were identified.

INTRAOSSEOUS
STERNUM>>>>Proximal Humerus >>> FEMUR>>>>> Tibia
A comparison of proximal tibia, distal femur, and proximal Humerus infusion rates using the EZ-IO intraosseous device on the adult swine (Sus scrofa) model.Julio R Lairet, Vikhyat S Bebarta, +5 authors James KingPublished 2013 in Prehospital emergency care: official journal of the National Association of EMS Physicians and the National Association of State EMS Director

UMBILICAL VEIN??
https://www.google.com/search?biw=1600&bih=789&tbm=isch&sa=1&ei=mKZhXNWxAsGIggeBoojgDA&q=umbilical+line+placement+pediatric&oq=umbilical+line+placement+pediatric&gs_l=img.3...519184.524055..524343...0.0..0.200.1672.5j8j1......1....1..gws-wiz-img.3NpJ3P-GNV0#imgrc=eKyHXdWKsASbfM:

ACCESS
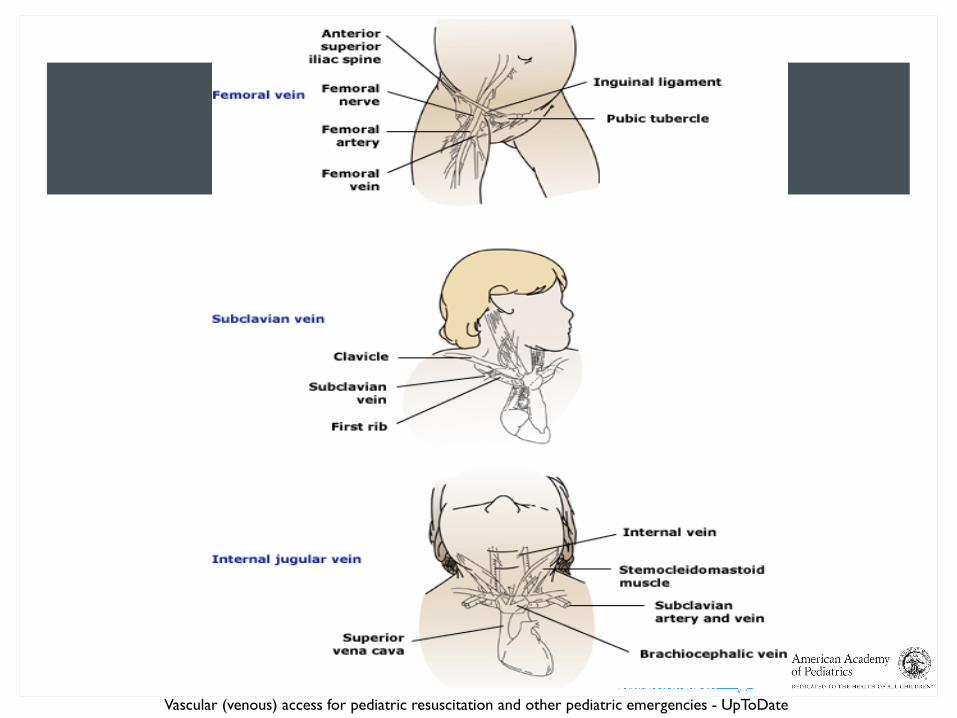
Vascular (venous) access for pediatric resuscitation and other pediatric emergencies - UpToDate

INTERNAL JUGULAR POSITIONING
Trendelenburg 15-30 degrees
Shoulder roll
Head turned away from side of insertion
INTERNAL JUGULAR
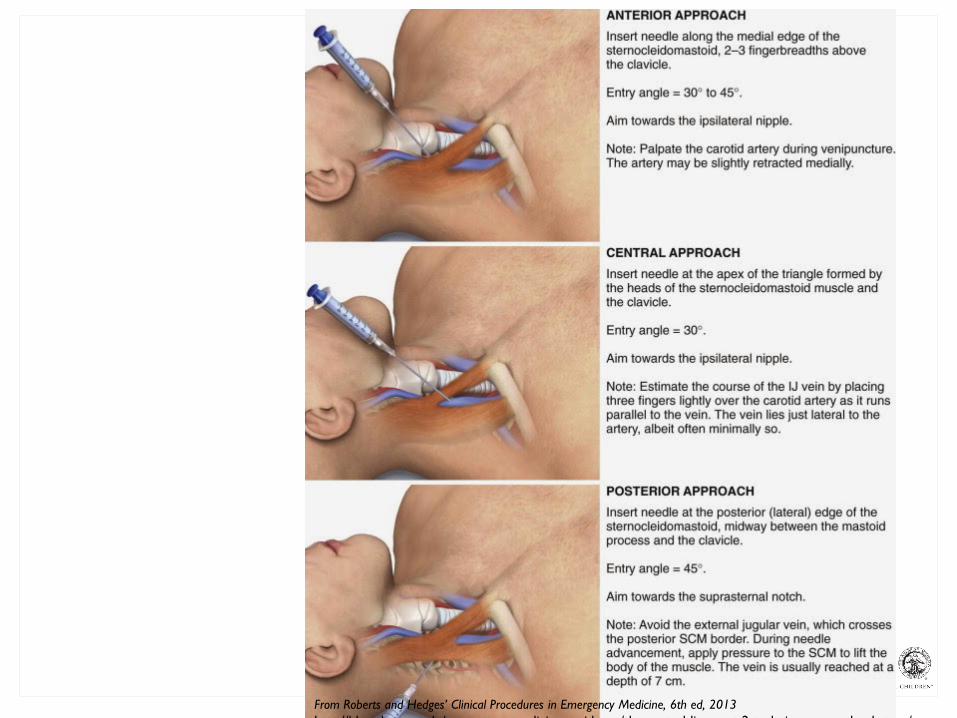
PROCEDURE
From Roberts and Hedges’ Clinical Procedures in Emergency Medicine, 6th ed, 2013htt //bl b d / di i id /th t l li t 2 t h i d l t /
95% of people have some overlap of the femoral vein by femoral artery
By positioning the leg in an ABDUCTED & EXTERNALLY ROTATED Amount of overlap is reduced and
Diameter of the vein is increased
Maximizing the percentage of the vein available for cannulation

FEMORAL IJ/ Supraclavicular
PROS • Large Vessel = ↑ flow rate• Ease of placement• No risk of pneumothorax
• Tip placement in right atrium decreases recirculation
CONS • Risk for infection• ↓ flow if (+) ascites/increased
abdominal pressure
• Superior vena cava syndrome
• Risk of PTX esp. with high PEEP

WORK UP
Bio-Markers:
Lactate
Blood Glucose
Electrolytes
VBG vs. ABG
Sepsis pathways
RNA Biosignatures ?
CRP
Procalcitonin
IL-18
CD-64

Update on pediatric sepsis: a review. Tatsuya KawasakiEmail authorView ORCID ID profile. Journal of Intensive Care20175:47 https://doi.org/10.1186/s40560-017-0240-1 © The Author(s). 2017 Published: 20 July 2017

GOAL DIRECTED THERAPY
Hypotensive hypovolemic or distributive shock 20 mL/kg per bolus of isotonic crystalloid over 5 to 10
minutes
Repeat 4 times in patients without improvement and no signs of fluid overload
Blood products?

GOAL DIRECTED THERAPY
Median volume of fluid delivered over five minutes
Gravity 6.2 mL/kg
“Push-pull" 20.2 mL/kg

GOAL DIRECTED THERAPY
Median volume of fluid delivered over five minutes
“Push-pull" 20.2 mL/kg
Pressure bag 20.9 mL/kg
TO MUCH OF A GOOD THING
Cardiogenic shock
DKA
SIADH
Severe malnutrition

NORMAL SALINE
Saline Potential hyperchloremic non-gap acidosis
Balanced fluids Higher rates of renal injury – ADULTS
NNT 94
Lactated Ringers
Plasmalyte – another option

TARGETED END-POINTS
Improving quality of pulses
Improving blood pressure
Improving Skin perfusion
Improving level of consciousness
Urine output?? >1ml/kg/hour

VASOACTIVE MEDS
Major Traumatic Brain injury
Peri-intubation Hypotension
Post-arrest hypotension
The Use of Bolus-Dose Vasopressors in the Emergency DepartmentHolden D. et al. Ann Emerg Med 2018

REFRACTORY?
Antibiotics for sepsis (early in course)
Corticosteroids
Hydrocortisone bolus, using a dose of 50 to 100 mg/m2
Age-based dosing may be used as follows:
Infants and toddlers 0 to 3 years old: 25 mg IV
Children 3 to 12 years: 50 mg IV
Children and adolescents 12 years and older: 100 mg IV

STABILIZATION
A / B: Administer Oxygen but be cautions Titrate between 92-97% (after ROSC)
C: Get accessHumeral IO may be better then Tibia
Administer isotonic crystalloid - consider balanced solutions
Consider peripheral pressor until central access available

SUMMARY
Determine shock as quick as possibleVitals: Tachycardia, tachypnea, HYPOTENSION
Altered Mental status,
Urine output
Labs – Lactate – ensure 20% decreased within 2 hrs.
SUMMARY
Treat shock as quick as possible Fluids - Crystalloid
Peripheral pressor – likely start with Nor-epi
TARGETS
Improved perfusion / vitals
Improved pulses/ skin / cap refill <3
Decreasing lactate

QUESTIONS???

ACKNOWLEDGEMENTS
Michael Winters, MD, MBA
Timothy E Bunchman; Professor & Director; Helen DeVos Children’s Hospital, Grand Rapids, MI
Jennifer D. Walthall, MD, MPH














![SHOCK[1] - Hypovolemic Shock](https://static.documents.pub/doc/80x56/58edc1bc1a28abae538b4711/shock1-hypovolemic-shock.jpg)


