46
Shock in Neonates By: Dr Rupa Banerjee

Shock in Neonates
By: Dr Rupa Banerjee

Shock:
A complex clinical syndrome
caused by an acute failure of
circulatory function and
characterized by inadequate
tissue and organ perfusion

Consequenses of Shock:
•Inadequate oxygen and nutrient substrate delivery
•Compromised metabolic waste removal
•Cellular dysfunction and death
•May involve isolated organs or entire organism

Adequate tissue perfusion requires:
• Cardiac output
• Integrity and maintenance of vasomotor tone of local arterial venous, and capillary vascular beds
• The ability of the blood to deliver oxygen and metabolic substrates and remove metabolic wastes

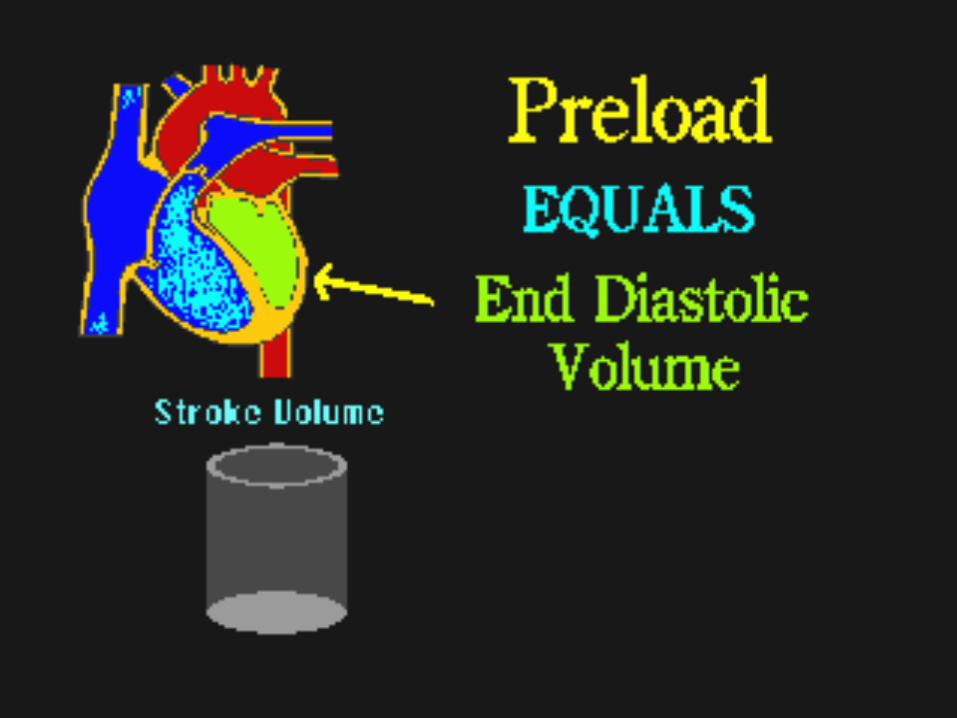
Stroke volume is influenced by:
•Preload
•Afterload
•Myocardial Contractility


Contractility :
• Is a semi-quantitative method of measuring ventricular function
•An increase in contractility will increase the stroke volume provided preload and afterload remain unchanged

Oxygen Delivery to Tissues
Hemoglobin level, CardiacOutputBlood O2 saturation Airway Breathing Rate/Rhythm,FIO2 Stroke volume
Preload,Afterload Contractility
Neonatal Vasoregulation
Blood pressure measures the pressure in the walls of arteries created by the activity of myocardium
This measurement consists of 2 numerical values:
•Systole is the force exerted on the vessel wall during the myocardial contraction
•Diastole is the pressure that remains on the blood vessels when the myocardium relaxes

Blood pressure is effected by following factors:
•The integrity of the myocardium
•The elasticity of the blood vessels
•Blood volume
•Blood viscosity

The neonatal myocardium has unique features:
•It lacks calcium stores in sarcoplasmic reticulum
•It has an increased fibrous non-contractile tissue
•It posses diminished sympathetic intervention

Types of shock
• Hypovolemic shock :caused by acute blood or fluid and electrolyte loss
• Cardiogenic shock :caused by cardiomyopathy, myocardial ischemia, arrhythmias, and heart failure

• Distributive shock :caused by sepsis, vasodilation, myocardial depression, or endothelial injury •Obstructive shock :from tension pneumothorax or cardiac tamponade
• Dissociative shock :from severe anemia or methemoglobinemia
Hypovolemic shock is usually due to:
•Antenatal haemorrhage
•Post-natal blood loss - iatrogenic, or secondary to DIC
•Fluid and electrolyte loss in newborn secondary to gastrointestinal abnormalities, vomiting and diarrhea

Clinical features :
•lethargy •mottling of the skin•cool peripheries•prolonged capillary refill •tachycardia •weak pulse•hypotension •decreased urine output
Cardiogenic shock may be caused by:
• Severe intra-partum asphyxia
• Primary structural heart disease like: HPLV, TA, PA or arrhythmias
• Disturbance of transitionalcirculation due to persistent pulmonary hypertension

The four main clinical features of cardiogenic shock are:
• tachycardia
• tachypnea
• hepatomegaly
• cardiomegaly

Septic shock :
•The commonest form of distributive shock is septic shock that is the major cause of mortality and morbidity in neonates
•Most common organisms causeing neonatal septic shock are E.coli and Group B Streptococcus

Pathophysiology of septic shock

Stages of shock :
•Shock, if not managed competently progresses through 3 phases:
•Compensated
•Uncompensated
•Irreversible

Compensated shock:
•Perfusion to vital organs preserved
•Minimal or absent derangement of vital signs (HR, RR, BP, Temp)
•Increased angiotension, vasopressin, catecholamine release
•Decreased spontaneous activity

Uncompensated shock:
•Decreased oxidative phosphorylation
•Failure of Na+-K+ pump
•Disrupted capillary endothelium
•Plasma protein leak
•Decreased oncotic pressure and shift of intravascualr fluid to extravascular

Irreversible shock:
•Ongoing fluid/blood requirement
despite control of hemorrhage •Persistent hypotension despite
restoration of intravascular volume

• No improvement in parameters
(cardiac output/ blood pressure)
despite inotropic support
•Futile cycle of uncorrectable
hypothermia, hypo-perfusion
acidosis, and coagulopathy

Investigations should determine:
• Type of shock •Cause of shock
• Severity of shock - whether end organ damage is present
•Presence of other complications •Type of management and prognosis

The following tests should be considered: •Complete blood count
•Coagulation tests
•Electrolytes, BUN/creatinine and urinalysis; and hepatic function tests

•Chest x-ray, ECG, echocardiogram
•Serum lactate
•Pro-inflammatory cytokines
•Increase in chemokine IP-10

•More invasive testing is often
required: arterial blood gas for O2/pH;
central venous oxygen saturation (ScvO2) >70%
•If septic shock is suspected, blood, urine, umbilical or wound cultures are advocated with head CT and lumbar puncture

Tests specific for septic shock:
Expected results
Blood culture positive
WBC <4000 OR >30000 (depends on age)
CRP > 2 ng/ml
PCT >2 ng/ml
IL-8 >70 pg/ml

Algorithm for management of shock: Suspected sepsis
Pan culture,urine re/me, CBC CRP, latate , physical examination
Source control, broad spectrum antibiotics
No shock Shock

No shock Reassess CBC, CRP repeat examination and imaging Continue antibiotics
Cultures negative Culture positive No sepsis Sepsis without shock
Stop antibiotics Repeat investigations Tailor antibiotics to culture, complete 7- 14 days antibiotics

Shock Fluid resuscitation 10-20 ml/kg ensure adequate venous access consider arterial access consider intubation
Culture negative Improved perfusion Persistent shock
SIRS(culture Culture positivenegative sepsis)
Serial investigations Septic shockFor alternate causesOf shock Pan culture,urine re/me, CBC CRP, lactate , physical examination complete 7- 14 days complete 7- 14 days antibiotics

Persistent shock after initial fluid rersucsitation Death C x ray, ECHO, cranial USGABG, cortisol level,Glucose, ionised Improved ECMO Calcium level perfusion evaluation
Consider additional fluid,initiate dopamine, Persistent shockAdd vasopressors Brodening of antibiotics InvestigationsReplete calcium for viral and fungal causes
Persistant shock/ Add fluids, add Refractory shock vasopressors,add antifungal add hydrocortisone

Volume and pharmacologic management (vasopressors and inotropes)
•After stable airway is assured, the priority
is volume crystalloid solution replacement
Special attention to ductus arteriosus
•First hour volume replacement limits are
basically determined by the gestational age

•Hemoglobin levels are below 12 g/dL
(Hb < 12 g/dL), packed red blood
cells transfusion is recommended
•The use of 10% glucose solution as
maintenance volume is required

Pharmacological management includes: •Vasopressors as dopamine, norepinephrine
and vasopressin
•Inotropes such as epinephrine
dobutamine and milrinone

Dopamine:• Is the most commonly used vasopressor
•For the initial management a 5-10
mcg/kg/min dose is recommended
•The dose is generally incremented by 2.5
mcg/kg/min steps every 10-15 minutes

Epinephrine: •Improves the heart output, myocardial
perfusion and increases the mesenteric
vascular resistance
•It is indicated for the refractory volume,
dopamine and dobutamine resistant
shock dosed as 0.05 to 0.3 mcg/kg/min

Norepinephrine:• Limited use in neonatal shock, indicated
for “warm” shock (doses 0.05 to 0.5
mcg/kg/min)
Dobutamine:
Frequently associated to dopamine in
the newborn septic shock increasing
both heart contractility and frequency

Milrinone:
•Selective phosphodiesterase inhibitor, with
important inotropic effects while causes
systemic and pulmonary vasodilation
(inodilator)
• dose is 0.75 mcg/kg/min for 3 hours
followed by 0.2 mcg/kg/min

Corticosteroids:
•Hydrocortisone therapy should be reserved for refractory shock patients
•In services missing structure to use inodilators (milrinone)
•In epinephrine-resistant shock
• In suspected relative or absolute adrenal failure (ambiguous genitalia)
Immunomodulator agents:
•IV Immunoglobulin
• Colony-stimulating factors (G-CSF and GM-CSF)
•Activated C protein
•Pentoxifylline, a platelet antiaggregant is recently being used for refractory shock dosed at 5 mg/kg/hour for 6 hours for 5 successive days

Conclusion:The impact of neonatal shock on morbidity
and mortality rates is high, but some
promising strategies have been evaluated
and developed over the years which has
improved the current management trends
and increased survival rates
Thank you…

















