Urologic Oncology: Seminars and Original Investigations 32 (2014) 135–145 Original article Short telomeres and chromosome instability prior to histologic malignant progression and cytogenetic aneuploidy in papillary urothelial neoplasms Naotaka Izumiyama-Shimomura, M.D. a , Ken-ichi Nakamura, Ph.D. a , Junko Aida, D.D.S., Ph.D. a,i , Naoshi Ishikawa, M.D. a , Mie Kuroiwa, M.D. b , Naoki Hiraishi c , Mutsunori Fujiwara, M.D. d , Yuichi Ishikawa, M.D. e , Naoko Inoshita, M.D. e , Junji Yonese, M.D. f , Masaaki Matsuura, Ph.D. g , Steven S.S. Poon, Ph.D. h , Tomio Arai, M.D. i , Kaiyo Takubo, M.D. a,i,* a Research Team for Geriatric Pathology, Tokyo Metropolitan Institute of Gerontology, Tokyo, Japan b Department of Pathophysiology, Yokohama College of Pharmacy, Yokohama, Japan c Department of Laboratory Medicine, Hadano Red Cross Hospital, Hadano, Kanagawa-ken, Japan d Department of Pathology and Laboratory Medicine, Japanese Red Cross Medical Center, Tokyo, Japan e Division of Pathology, The Cancer Institute, Japanese Foundation for Cancer Research, Tokyo, Japan f Department of Urology, The Cancer Institute Hospital, Tokyo, Japan g Bioinformatics Group, Genome Center and Department of Cancer Genomics, The Cancer Institute, The Japanese Foundation for Cancer Research, Tokyo, Japan h Terry Fox Laboratory, British Columbia Cancer Research Centre, Vancouver, BC, Canada i Department of Pathology, Tokyo Metropolitan Geriatric Hospital, Tokyo, Japan Received 1 November 2012; received in revised form 11 December 2012; accepted 31 December 2012 Abstract Purpose: Evaluation of the relationships existing among 3 histologic types of urothelial tumors, chromosomal instability, and telomere length. Patients and methods: We examined 37 consecutive cases of papillary urothelial neoplasm, from which 26 (70.3%) were suitable for karyotype analysis, comprising 7 papillary urothelial neoplasms of low malignant potential (PUNLMPs), 10 low-grade papillary urothelial carcinomas (PUCs), and 9 high-grade PUCs. We performed karyotype and anaphase bridge analyses, and measured telomere lengths by quantitative fluorescence in situ hybridization. Results: PUNLMPs were always diploid and had anaphase bridges. Low-grade PUCs showed diploidy (n ¼ 2), hypoploidy (n ¼ 4) and polyploidy (n ¼ 4), and high-grade PUCs showed diploidy (n ¼ 1) and polyploidy (n ¼ 8); both had anaphase bridges. The incidence of anaphase bridges did not differ significantly between PUNLMPs and high-grade PUCs (P ¼ 0.105). The telomere lengths of PUNLMP, low-grade PUC, and high-grade PUC, expressed as mean telomere fluorescence units (TFU) SD, were 7906 3197, 4893 1567, and 3299 1406, respectively. The differences among the 3 groups were significant. However, 42.9% of the PUNLMPs had shorter telomeres than the mean value for low-grade PUCs, and 30.0% of the low-grade PUCs had shorter telomeres than those for high-grade PUCs. There was an inverse correlation between telomere length and the incidence of anaphase bridges. Conclusions: PUNLMP appears to progress to low-grade PUC and high-grade PUC in association with telomere shortening and chromosomal instability. Our data suggest that critically shortened telomeres cause chromosomal instability during progression of papillary urothelial neoplasms. r 2014 Elsevier Inc. All rights reserved. Keywords: Telomere; PUNLMP; Urothelial carcinoma; Q-FISH; Chromosomal instability; Anaphase bridge; Karyotype analysis 1078-1439/$ – see front matter r 2014 Elsevier Inc. All rights reserved. http://dx.doi.org/10.1016/j.urolonc.2012.12.005 All of the present authors directly participated in planning, execution, and analysis of the present study. This study was supported by Grants-in-Aid for Scientific Research from the Ministry of Education, Culture, Sports, Science and Technology of Japan (KT, Nos. B17390108, B21390109; KIN: No. C18590354). * Corresponding author. Tel.: þ81-3-3964-3241; fax: þ81-3-3579-4776. E-mail address: [email protected] (K. Takubo).
Transcript
Urologic Oncology: Seminars and Original Investigations 32 (2014) 135–145
1078-1439/$ – see fronthttp://dx.doi.org/10.1016/j
All of the present aut
This study was suppo(KT, Nos. B17390108, B2
* Corresponding authorE-mail address: takubo
Original article
Short telomeres and chromosome instability prior to histologic malignantprogression and cytogenetic aneuploidy in papillary
a Research Team for Geriatric Pathology, Tokyo Metropolitan Institute of Gerontology, Tokyo, Japanb Department of Pathophysiology, Yokohama College of Pharmacy, Yokohama, Japan
c Department of Laboratory Medicine, Hadano Red Cross Hospital, Hadano, Kanagawa-ken, Japand Department of Pathology and Laboratory Medicine, Japanese Red Cross Medical Center, Tokyo, Japane Division of Pathology, The Cancer Institute, Japanese Foundation for Cancer Research, Tokyo, Japan
f Department of Urology, The Cancer Institute Hospital, Tokyo, Japang Bioinformatics Group, Genome Center and Department of Cancer Genomics, The Cancer Institute,
The Japanese Foundation for Cancer Research, Tokyo, Japanh Terry Fox Laboratory, British Columbia Cancer Research Centre, Vancouver, BC, Canada
i Department of Pathology, Tokyo Metropolitan Geriatric Hospital, Tokyo, Japan
Received 1 November 2012; received in revised form 11 December 2012; accepted 31 December 2012
Abstract
Purpose: Evaluation of the relationships existing among 3 histologic types of urothelial tumors, chromosomal instability, and telomere length.Patients and methods: We examined 37 consecutive cases of papillary urothelial neoplasm, from which 26 (70.3%) were suitable for
karyotype analysis, comprising 7 papillary urothelial neoplasms of low malignant potential (PUNLMPs), 10 low-grade papillary urothelialcarcinomas (PUCs), and 9 high-grade PUCs. We performed karyotype and anaphase bridge analyses, and measured telomere lengths byquantitative fluorescence in situ hybridization.
Results: PUNLMPs were always diploid and had anaphase bridges. Low-grade PUCs showed diploidy (n ¼ 2), hypoploidy (n ¼ 4) andpolyploidy (n ¼ 4), and high-grade PUCs showed diploidy (n ¼ 1) and polyploidy (n ¼ 8); both had anaphase bridges. The incidence ofanaphase bridges did not differ significantly between PUNLMPs and high-grade PUCs (P ¼ 0.105). The telomere lengths of PUNLMP,low-grade PUC, and high-grade PUC, expressed as mean telomere fluorescence units (TFU) � SD, were 7906 � 3197, 4893 � 1567, and3299 � 1406, respectively. The differences among the 3 groups were significant. However, 42.9% of the PUNLMPs had shorter telomeresthan the mean value for low-grade PUCs, and 30.0% of the low-grade PUCs had shorter telomeres than those for high-grade PUCs. Therewas an inverse correlation between telomere length and the incidence of anaphase bridges.
Conclusions: PUNLMP appears to progress to low-grade PUC and high-grade PUC in association with telomere shortening andchromosomal instability. Our data suggest that critically shortened telomeres cause chromosomal instability during progression of papillaryurothelial neoplasms. r 2014 Elsevier Inc. All rights reserved.
matter r 2014 Elsevier Inc. All rights reserved..urolonc.2012.12.005
hors directly participated in planning, execution, and analysis of the present study.
rted by Grants-in-Aid for Scientific Research from the Ministry of Education, Culture, Sports, Science and Technology of Japan1390109; KIN: No. C18590354).
N. Izumiyama-Shimomura et al. / Urologic Oncology: Seminars and Original Investigations 32 (2014) 135–145136
1. Introduction
There are 2 independent pathways for the developmentof urothelial carcinoma, although occasional overlapbetween them can occur [1–5]. One pathway is representedby low-grade papillary urothelial neoplasms, includingpapillary urothelial neoplasm of low malignant potential(PUNLMP) and low-grade papillary urothelial carcinoma(PUC), which is characterized by frequent local recurrencewithout distant metastasis, and which only occasionallyprogresses to high-grade PUC or urothelial carcinomawith invasion to the muscular layer [1,6]. PUNLMPhas been defined as a papillary urothelial tumor thatresembles exophytic urothelial papilloma, but showsincreased cellular proliferation exceeding the thickness ofthe normal urothelium [7]. The second pathway is repre-sented by carcinoma in situ and muscle-invasive urothelialcarcinoma [2].
Telomeres play critical roles in the maintenance ofchromosomal stability, as well as in limiting the ultimatereplication capacity of cells [8], and it has been suggestedthat telomere shortening is an important biological factorassociated with cell senescence [9], carcinogenesis, andaging [8–10]. McGrath et al. [11] considered that there wasa need to investigate the associations between telomerelength and histologic grade, but no such study has yet beenreported. Therefore, to clarify the relationships existingamong 3 different histologic types of bladder neoplasm,chromosomal instability, and telomere length, we per-formed karyotype and anaphase bridge analyses [12,13],and measured telomere lengths using quantitative fluores-cence in situ hybridization (Q-FISH) [14,15].
2. Subjects and Methods
2.1. Subjects
The tumor samples studied were obtained, withinformed consent, from 37 consecutive patients withpapillary urothelial neoplasms of the urinary bladder bytransurethral resection (TUR) performed by a singleurologist (JY) at the Cancer Institute Hospital, Tokyo.These neoplasms were histologically divided into 3groups—PUNLMP, low-grade PUCs, and high-gradePUCs—by 2 pathologists (YI, NI), based on the descrip-tion by Epstein et al. [16]. From 26 (70.3%) of the 37neoplasms, we were able to acquire metaphase spreadsthat were suitable for karyotype analysis. Among the 26patients, 7 (4 men and 3 women, aged 53–82 y, mean71.0 y) were diagnosed as having PUNLMP, 10 (10 men,aged 48–74 y, mean 64.0 y) as having low-grade PUC,and 9 (8 men and 1 woman, aged 50–79 y, mean 63.0 y)as having high-grade PUC. Approval for this study wasobtained from the ethics committee of Tokyo Metropoli-tan Institute of Gerontology.
2.2. Estimation of chromosomal instability
2.2.1. The Q-band technique and chromosome numberin FISH samples
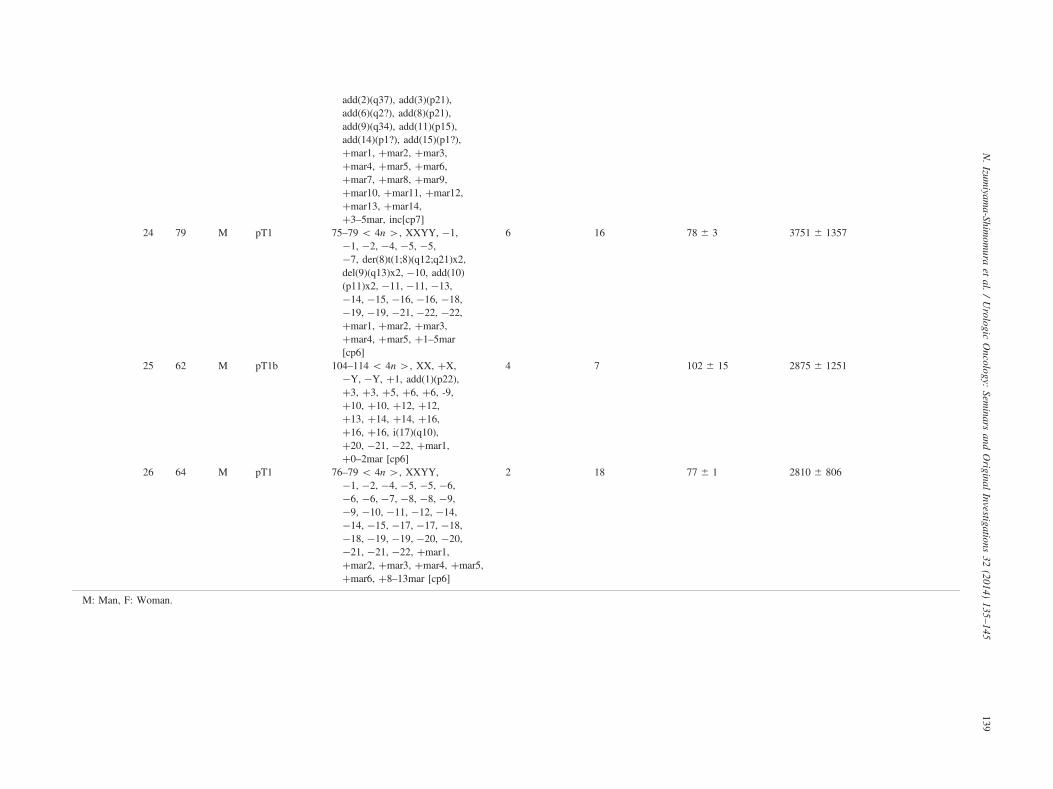
Fresh tumor samples were examined as described else-where [17]. Chromosomes were analyzed using the Q-bandtechnique. Chromosome identification and karyotype des-ignations were performed in accordance with the Interna-tional System for Human Cytogenetic Nomenclature [18].Two of the authors (MF and KIN) tried to examine 10metaphase spreads, if possible, for each case using theQ-band technique. However, in practice, the number ofmetaphase cells analyzed ranged from 2 to 10. For FISHsamples, one of the authors (KIN) recorded the number ofchromosomes in 1 metaphase spread. All of the metaphasespreads obtained for FISH samples were analyzed, and wewere able to obtain 3 to 18 metaphase spreads for each ofthese cases (Table 1).
2.2.2. Anaphase bridge analysisThe presence of anaphase bridges as a possible morpho-
logic indicator of chromosomal instability [12,13] wasexamined by 3 of the authors (KIN, NIS, and NI). Thecarcinoma cells in primary culture were fixed withoutcolcemid treatment, and then cell smears were preparedand analyzed after staining with Giemsa for 30 seconds. Atleast 1000 carcinoma cells were evaluated to estimate therate of occurrence of chromatin bridges in each case. Ananaphase bridge was defined as a filamentous connectionlinking 2 well-separated nuclei [15].
2.3. Telomere measurements by Q-FISH
2.3.1. ProbesThe metaphase chromosomes were hybridized using the
peptide nucleic acid (PNA)-FISH preparation method[14,19]. A Cy3-labeled (CCCTAA)3 peptide nucleic acidprobe (catalog number F1002; Fasmac, Atsugi, Japan) wasused to label the telomeres, and a FITC-labeled CTTCGTT-GGAAACGGGGT peptide nucleic acid probe (a nonspe-cific centromere probe, custom-made; Fasmac) was used forthe centromere. The chromosomes were counterstained with40, 6-diamidino-2-phenylindole(DAPI, Molecular Probes,Eugene, OR, USA).
2.3.2. Q-FISH and image analyses of telomeresQ-FISH and image analyses were performed as
described previously [14,15]. A total of 3 to 18 metaphasespreads for each of the 26 primary-cultured cells wereanalyzed. Telomere intensities of individual arms in themetaphase spreads were measured and expressed as telo-mere fluorescence units (TFUs). Digital images wererecorded with a CCD camera, AxioCam MRm (Zeiss,Oberkochen, Germany) mounted on an Axio Imager MAT(Zeiss) epifluorescence microscope equipped with a tripleband-pass filter for Cy3/FITC/DAPI (61010 Chroma
Table 1Summary of karyotype and anaphase bridge analyses, numbers of chromosomes in FISH samples, and telomere fluorescence units (telomere lengths)
Histology ID Age(yr)
Sex T of TNMclassification
Karyotype by Q-band Incidence ofanaphasebridge(per 1000 cells)
N. Izumiyama-Shimomura et al. / Urologic Oncology: Seminars and Original Investigations 32 (2014) 135–145140
Technology, Corp., Rockingham, VT, USA) and a �63 oilobjective lens (Zeiss EC Plan-NEOFLUAR 63�/1.241/0.17). Microscope control and image acquisition were donewith the ISIS System (Metasystem, GmbH, Altlussheim,Germany). A level of calibration was used to ensure areliable quantitative estimation of telomere length in thevarious samples in each study. So as to correct for dailyvariations in lamp intensity and alignment, images offluorescent beads (orange beads, size 0.2 mm, MolecularProbes Inc.) were acquired just prior to acquisition of theimages from the samples. The fluorescence intensities of thebeads and telomeres were analyzed with the TFL Telo-V2software package (Terry Fox Laboratory, BC CancerResearch Centre, Canada).
2.4. Statistical analysis
Telomere lengths were compared among the 3 groupsusing the unpaired t test. Fisher’s Z test was used forcomparison of relationships. In all comparisons, differencesat P o 0.05 were considered to be significant. Correlationsbetween telomere length and the number of chromosomes,between telomere length and the incidence of anaphasebridges, and between the number of chromosomes and theincidence of anaphase bridges were analyzed in each subject.
Fig. 1. Representative karyotypes in the 3 subject groups. (A) PUNLMPshowing diploidy (ID: 6, TFU ¼ 4398 � 507). (B) Low-grade PUC(ID: 9, TFU ¼ 2313 � 415). (C) High-grade PUC (ID: 23, TFU ¼1410 � 270). Results of karyotype analysis are described in detail inTable 1.
3. Results
Tumor stage (T in the TNM classification [20]) and allresults analyzed are summarized in Table 1.
3.1. Karyotype analysis
UNLMPs always showed diploidy. Low-grade PUCsshowed diploidy (n ¼ 2), hypoploidy (n ¼ 4) andpolyploidy (n ¼ 4), and high-grade PUCs revealeddiploidy (n ¼ 1) and polyploidy (n ¼ 8). Multipleabnormalities were observed in the 17 cases (Fig. 1).
3.2. Numbers of chromosomes in FISH samples
We were able to obtain 3 to 18 metaphase spreads(Fig. 2) in FISH samples, although we collected as manymetaphase spreads as possible. The FISH images ofmetaphase spreads were obtained for all 26 subjects. ThePUNLMPs mostly had 46 chromosomes (45.7 � 0.5). Themean number of chromosomes for low-grade PUCs andhigh-grade PUCs was 55.5 � 17.1 and 69.2 � 17.6,respectively (Fig. 3). PUNLMPs had a significantly smallernumber of chromosomes than high-grade PUCs.
3.3. Anaphase bridge analysis
Typical anaphase bridges were observed in the 3 groups(Fig. 4). Multiple micronuclei were occasionally observed
in the high-grade PUCs. The PUNLMPs, low-grade PUCs,and high-grade PUCs had 2.0 � 1.5 (0.20%), 2.3 � 1.9(0.23%), and 4.4 � 3.8 (0.44%) anaphase bridges per 1000cells, respectively (Fig. 5). However, the differences inincidence among the 3 histologic types were not significant.
3.4. Telomere lengths in the 3 groups
A total of 237 metaphase spreads (PUNLMPs: 39 meta-phase spreads; low-grade PUCs: 100; and high-grade PUCs:
Fig. 2. Representative FISH images of metaphase spreads in the 3 subject groups. (A) PUNLMP (ID: 4). (B) Same case shows diploidy by karyotyping (ID: 4,TFU ¼ 10,756 � 5503). (C) Low-grade PUC (ID: 12, TFU ¼ 5832 � 932). (D) High-grade PUC (ID: 26, TFU ¼ 2810 � 806).
N. Izumiyama-Shimomura et al. / Urologic Oncology: Seminars and Original Investigations 32 (2014) 135–145 141
98) were examined. The median TFU value was defined as arepresentative value for a metaphase spread, and the meanvalue of the median for all karyotypes for a single subject wasdefined as the representative value for that subject. The meanvalue of the median for all subjects within each of the 3 groupswas defined as the representative value for the subject group.
TFUs were very variable on the p-arms and q-arms of thesame chromosome, within the same cell and within the sameindividual. Mean values of the median telomere length � SDfor the 7 PUNLMPs, 10 low-grade PUCs, and 9 high-gradePUCs were 7906 � 3197, 4893 � 1567, and 3299 � 1406TFUs, respectively (Fig. 6), and the intergroup differenceswere all significant. Three (42.9%) of the 7 PUNLMPs had
shorter telomeres than the mean value for the 10 low-gradePUCs. Three (30.0%) of the 10 low-grade PUCs had shortertelomeres than the mean value for the 9 high-grade PUCs.
3.5. Correlations among telomere length, number ofchromosomes, and incidence of anaphase bridges in eachsubject
The correlation between telomere length and the numberof chromosomes in each subject is shown in Fig. 7. Therewas no significant correlation between them (P ¼ 0.089).
The correlation between telomere length and the inci-dence of anaphase bridges in each subject is shown in
Fig. 3. Numbers of chromosomes in FISH materials in the 3 groups. Mostof the PUNLMPs had a diploid pattern (XY, 45.7 � 0.5). Mean numbersof chromosomes in low-grade and high-grade PUCs were 55.5 � 17.1 and69.2 � 17.6, respectively.
Fig. 5. Incidences of anaphase bridges in the 3 groups. PUNLMPs, low-grade PUCs, and high-grade PUCs had 2.0 � 1.5 (0.20%), 2.3 � 1.9(0.23%), and 4.4 � 3.8 (0.44%) anaphase bridges per 1000 cells, respec-tively, but the intergroup differences were not significant.
N. Izumiyama-Shimomura et al. / Urologic Oncology: Seminars and Original Investigations 32 (2014) 135–145142
Fig. 8. A significant correlation was demonstrated betweentelomere length and the incidence of anaphase bridges(P ¼ 0.031). However, for cases within the range 2000to 6000 TFUs (n ¼ 19), no correlation was demonstrated(not shown, y ¼ 0.0016 þ 0.0000002x, r ¼ 0.162,P ¼ 0.508).
The correlation between the number of chromosomesand the incidence of anaphase bridges is shown in Fig. 9.A significant correlation was demonstrated (P ¼ 0.046).
4. Discussion
Most patients with noninvasive G1 tumors (G1 tumors inthe 1973 WHO classification were classified as PUNLMPsand low-grade PUCs in the 2004 WHO classification [21])reportedly have a diploid or nearly diploid chromosomenumber [22]. Here, we confirmed those results, as PUNLMPs
Fig. 4. Representative anaphase bridges in the 3 groups. A very fine chromat4321 � 586); (B) Low-grade PUC (ID: 14, TFU ¼ 5715 � 2279); (C) High-g(ID: 22, TFU ¼ 1817 � 852).
were always cytogenetically diploid and their chromosomeswere relatively stable. Generally, malignant neoplasms,including urothelial carcinomas [23], showing polyploidy onthe basis of cytogenetic analysis have a poor prognosis. It isknown that PUNLMP has a better outcome than PUC [24].In our FISH samples, high-grade PUCs had no less than 46chromosomes, whereas low-grade PUCs had 46 in 2 cases,less than 46 in 4, and more than 46 in 4. These results suggestthat hypoploidy might occur during the process of malignantprogression from PUNLMP to low-grade PUC.
Although in this study the incidence of anaphase bridgesappeared to be related to histology, the relationship was notsignificant. Observation of anaphase bridges providesstrong evidence that chromosomes in the cells are partici-pating in the breakage-fusion-bridge cycle because theyhave inadequate telomere protection against fusions [12,13].
In patients with urothelial carcinoma, telomere measure-ment has been conducted using blood cells, and the
in string connects 2 lobes of a nucleus. (A) PUNLMP (ID: 3, TFU ¼rade PUC. A bleb is located in a string. Multiple micronuclei are evident
Fig. 6. Mean telomere lengths (TFUs) in the 3 groups. Mean telomerelengths in 7 PUNLMPs, 10 low-grade PUCs, and 9 high-grade PUCs were7906 � 3197, 4893 � 1576, and 3299 � 1406 TUFs, respectively, andthe intergroup differences were significant.
N. Izumiyama-Shimomura et al. / Urologic Oncology: Seminars and Original Investigations 32 (2014) 135–145 143
presence of short telomeres appears to be associated with anincreased risk of bladder cancer [25,26]. In patients withbladder cancer, and also in smokers, the buccal epithelium[27] and buffy coat cells [11] are reported to have shortertelomeres than those in the controls. Although the relation-ship between telomere length in the normal urothelium andthe incidence of urothelial carcinoma is still unclear, 1study, in 21 patients with bladder cancer, has reported thattelomere length in bladder cancer and the uninvolvedadjacent nonneoplastic urothelium was 6.6 and 11.5 kilo-base pairs, respectively [28]. However, in the same study,telomere length measured by Southern blotting was sig-nificantly less in superficial than in invasive urothelialcarcinoma [28]. This was not in accord with our presentdata. We previously demonstrated clearly that in humantissues the terminal restriction fragment length measured bySouthern blotting did not represent the telomere length of
Fig. 7. Correlation between TFU and number of chromosomes in FISH samples wTFU and the number of chromosomes in FISH samples within a single individu
the cells investigated [29], because human tissue DNA fromthose cells was usually admixed with that of denseinflammatory cells and stromal cells [30,31]. Therefore,we did not use Southern blotting for telomere measurementin this study, and instead employed Q-FISH to determinethe telomere length of pure urothelial carcinoma cells.
Although we considered it would be informative tocompare telomere lengths between normal urothelium fromhealthy humans and uninvolved urothelium from patients withbladder cancer, we were unable to do so because ethical issuesand autolysis of autopsy samples made it difficult to obtainmetaphase spreads and to measure telomeres in normalurothelium. Also, it was impossible to obtain metaphasespreads solely from uninvolved urothelium adjacent to carci-noma in TUR specimens because distinction between unin-volved urothelium and neoplasms was difficult on the basis ofmacroscopic inspection. We speculate that the uninvolvedurothelium adjacent to carcinoma would have shorter telo-meres than that unassociated with carcinoma, because in ourprevious studies of the esophagus [32] and oral cavity [33], wedemonstrated that nonneoplastic epithelia associated withcarcinoma had shorter telomeres than epithelia withoutcarcinoma. This indicates that, in both tissues, criticallyshortened telomeres cause chromosomal instability early inthe multistep processes of malignant transformation [34], andalso that urothelial carcinoma occurs in urothelium withcritically shortened telomeres and chromosomal instability.
In the present study, PUNLMP had the longest telomeresamong the 3 histologic categories and always showeddiploidy. Critically shortened telomeres cause fusion ofchromosomes, and such fused chromosomes are intrinsi-cally unstable [10,15,34]. Indeed, in urothelial cells, wefound that telomere length was inversely correlated with theanaphase bridge index. Also, low-grade PUCs and high-grade PUCs showed a high incidence of aneuploidy andanaphase bridges, but the differences between them in thisrespect were not significant.
Individual telomere lengths of fibroblasts were distributedover an extremely wide range [15]. Telomere lengths in
ithin a single individual. There was no significant correlation between meanal among the 26 subjects (Fisher’s Z test, P ¼ 0.089).
Fig. 8. Correlation between TFU and the incidence of anaphase bridges within a single individual. There was a significant inverse correlation between meanTFU and the incidence of anaphase bridges within a single individual among the 26 subjects (Fisher’s Z test, P ¼ 0.031).
N. Izumiyama-Shimomura et al. / Urologic Oncology: Seminars and Original Investigations 32 (2014) 135–145144
normal adult bone marrow metaphases are also reportedly veryheterogeneous [35], as was also seen in our present samples,although individual telomeres may mediate important biolo-gical effects, as has been shown in yeast, where loss of asingle telomere results in cell cycle arrest and chromosomeloss [36]. It has been indicated that chromosomes havingexcessively shortened telomeres begin to show features ofinstability such as fusions and anaphase bridges [13,15]. In thepresent study, the incidence of anaphase bridges was notrelated to telomere length in cases having 2000 to 6000 TFUs.Therefore, there is a possibility that the incidence of anaphasebridges may not be related to mean telomere length but to thequantity of excessively shortened telomeres.
Our study involved a relatively small sample. However,although PUNLMPs are known to have mild morphologicatypia [7], and showed cytogenetic diploidy in the presentstudy, 42.9% of them had telomeres that were shorterthan the mean value for low-grade PUCs, and 30.0% of the
Fig. 9. Correlation between incidence of anaphase bridges and the number ofsignificant correlation between the incidences of anaphase bridges and the numbersubjects (Fisher’s Z test, P ¼ 0.046).
low-grade PUCs had telomeres that were shorter than thosein high-grade PUC. There were no significant differences inthe incidence of anaphase bridges among the 3 histologictypes. These results indicate that telomere shortening and anincreased incidence of anaphase bridges might precede thehistologic change from PUNLMP to low-grade PUC, andthe cytogenetic change from diploidy to hypoploidy. Thechange from diploidy to hypoploidy and telomere short-ening occurred during the process of transformation ofPUNLMP to low-grade PUC. Although it is unclearwhether PUNLMP progresses to high-grade PUC via low-grade PUC [2], we consider that PUNLMP changes to low-grade PUC and high-grade PUC with time.
We believe that strict follow-up is needed for patientswith PUNLMPs or low-grade PUCs with shorter telomeres.Also we plan to conduct a prospective study to examine theoutcome of patients with PUNLMPs, low-grade PUCs, andhigh-grade PUCs with shorter telomeres.
chromosomes in FISH samples within a single individual. There was aof chromosomes of FISH samples within a single individual among the 26
N. Izumiyama-Shimomura et al. / Urologic Oncology: Seminars and Original Investigations 32 (2014) 135–145 145
Conflicts of interest
No conflicts of interest are declared.
Acknowledgments
The authors wish to thank Ms. K. Kanno, Mr. S. Nakazawa,and Mr. N. Hosokai for helpful assistance with karyotyping.
References
[1] Castillo-Martin M, Domingo-Domenech J, Karni-Schmidt O, et al.Molecular pathways of urothelial development and bladder tumor-igenesis. Urol Oncol 2010;28(4):401–8.
[2] Goebell PJ, Knowles MA. Bladder cancer or bladder cancers?genetically distinct malignant conditions of the urothelium. UrolOncol 2010;28(4):409–28.
[3] McConkey DJ, Lee S, Choi W, et al. Molecular genetics of bladdercancer: emerging mechanisms of tumor initiation and progression.Urol Oncol 2010;28(4):429–40.
[4] Mitra AP, Cote RJ. Molecular pathogenesis and diagnostics ofbladder cancer. Annu Rev Pathol 2009;4:251–85.
[5] Pollard C, Smith SC, Theodorescu D. Molecular genesis of non-muscle-invasive urothelial carcinoma (NMIUC). Expert Rev MolMed 2010;12:e10.
[6] Juan R. Urothelial (transitional cell) carcinoma. Rosai and Ackerman’ssurgical pathology, 10th ed.. Edinburgh, London, New York, Oxford,Philadelphia, St Louis, Sydney, Toronto: Elsevier: 2011. p. 1257-66.
[7] Lopez-Beltran A, Knowles MA, Sauter G, et al. Tumours of theurinary system. Lyon: IARC Press: 2004.
[8] Greider CW. Telomeres and senescence: the history, the experiment,the future. Curr Biol 1998;8:R178–81.
[9] de Lange T. Telomeres and senescence: ending the debate. Science1998;279:334–5.
[10] Harley CB, Villeponteau B. Telomeres and telomerase in aging andcancer. Curr Opin Genet Dev 1995;5:249–55.
[11] McGrath M, Wong JY, Michaud D, et al. Telomere length, cigarettesmoking, and bladder cancer risk in men and women. CancerEpidemiol Biomarkers Prev 2007;16:815–9.
[12] Rudlph KL, Millard M, Bosenberg MW, et al. Telomere dysfunctionand evolution of intestinal carcinoma in mice and humans. Nat Genet2001;28:155–9.
[13] Gisselsson D, Pettersson L, Hoglund M, et al. Chromosomalbreakage-fusion-bridge events cause genetic intratumor heterogeneity.Proc Natl Acad Sci USA 2000;97:5357–62.
[14] Poon SS, Lansdorp PM. Measurements of telomere length onindividual chromosomes by image cytometry. Darzynkiewicz Z,Crissman HA, Robinson JP, Methods in cell biology, flow cytometry.San Diego, CA: Academic Press: 2001:69–96.
[15] Takubo K, Aida J, Izumiyama N, et al. Chromosomal instability andtelomere lengths of each chromosomal arm measured by Q-FISH inhuman fibroblast strains prior to replicative senescence. Mech AgeingDev 2010;131:614–24.
[16] Epstein JI, Amin MB, Reuter VR, et al. The World HealthOrganization/International Society of Urological Pathology consensusclassification of urothelial (transitional cell) neoplasms of the urinary
bladder. Bladder consensus conference committee. Am J Surg Pathol1998;22:1435–48.
[17] Miura I, Siegfried JM, Resau J, et al. Chromosome alterations in 21non-small cell lung carcinomas. Genes Chromosomes Cancer1990;2:328–38.
[18] Shaffer LG, Slovak ML, Campbell LJ. An international system forhuman cytogenetic nomenclature: recommendations of the interna-tional standing committee on human cytogenetic nomenclature. Basel:S. Karger Co., 2009.
[19] Poon SS, Lansdorp PM. Quantitative fluorescence in situ hybridiza-tion (Q-FISH). Curr Protoc Cell Biol 2001;18:4. Chapter 18 Unit.
[20] Eble JN, Sauter G, Epstein JI, et al. World Health OrganizationClassification of Tumours. Pathology and genetics of tumours of theurinary system and male genital organs. TNM classification ofcarcinomas of the urinary bladder. Lyon: IARC Press: 2004. p. 91.
[21] Montironi R, Lopez-Beltran A. The 2004 WHO classification ofbladder tumors: a summary and commentary. Int J Surg Pathol2005;13:143–53.
[22] Micic S, Micic M, Milasin J. Chromosome analysis in patients withbladder tumor. Urol Int 1988;43(4):201–4.
[23] Bartlett JM, Adie L, Watters AD, et al. Chromosomal aberrations intransitional cell carcinoma that are predictive of disease outcome areindependent of polyploidy. BJU Int 1999;84:775–9.
[24] Malmstrom PU, Busch C, Norlen BJ. Recurrence, progression andsurvival in bladder cancer. A retrospective analysis of 232 patientswith greater than or equal to 5-year follow-up. Scand J Urol Nephrol1987;21:185–95.
[25] Wu X, Amos CI, Zhu Y, et al. Telomere dysfunction: a potentialcancer predisposition factor. J Natl Cancer Inst 2003;95:1211–8.
[26] Gu J, Chen M, Shete S, et al. A genome-wide association studyidentifies a locus on chromosome 14q21 as a predictor of leukocytetelomere length and as a marker of susceptibility for bladder cancer.Cancer Prev Res 2011;4:514–21.
[27] Broberg K, Bjork J, Paulsson K, et al. Constitutional short telomeresare strong genetic susceptibility markers for bladder cancer. Carcino-genesis 2005;26:1263–71.
[28] Kamata S, Kageyama Y, Yonese J, et al. Significant telomerereduction in human superficial transitional cell carcinoma. Br J Urol1996;78:704–8.
[29] Sanada Y, Aida J, Kawano Y, et al. Hepatocellular telomere length inbiliary atresia measured by Q-FISH. World J Surg 2012;36:908–16.
[30] Oexle K. Telomere length distribution and Southern blot analysis.J Theor Biol 1998;190:369–77.
[31] O’Sullivan JN, Bronner MP, Brentnall TA, et al. Chromosomalinstability in ulcerative colitis is related to telomere shortening. NatGenet 2002;32:280–4.
[32] Takubo K, Fujita M, Izumiyama N, et al. Q-FISH analysis of telomereand chromosome instability in the oesophagus with and withoutsquamous cell carcinoma in situ. J Pathol 2010;221:201–9.
[33] Aida J, Izumo T, Shimomura N, et al. Telomere lengths in the oralepithelia with and without carcinoma. Eur J Cancer 2010;46:430–8.
[34] Greider CW. Telomerase activity, cell proliferation, and cancer. ProcNatl Acad Sci USA 1998;95:90–2.
[35] Lansdorp PM, Verwoerd NP, van de Rijke FM, et al. Heterogeneity intelomere length of human chromosomes. Hum Mol Genet 1996;5:685–691.
[36] Sandell LL, Zakian VA. Loss of a yeast telomere: arrest, recovery,and chromosome loss. Cell 1993;75:729–39.