Shoulder Pain: Shoulder Pain: Evidence Based Evidence Based Evaluation & Evaluation & Management Management Frank J. Domino, M.D. Frank J. Domino, M.D. Professor Professor Department Family Medicine & Community Department Family Medicine & Community Health Health University of Massachusetts Medical University of Massachusetts Medical School School
Transcript
Shoulder Pain:Shoulder Pain:Evidence Based Evidence Based
Evaluation & ManagementEvaluation & Management
Frank J. Domino, M.D.Frank J. Domino, M.D.
ProfessorProfessor
Department Family Medicine & Community HealthDepartment Family Medicine & Community Health
University of Massachusetts Medical School University of Massachusetts Medical School
By the end of this session, you By the end of this session, you will:will:
1 Understand the normal and abnormal anatomy 1 Understand the normal and abnormal anatomy of the shoulderof the shoulder
2. Learn to use the 2. Learn to use the historyhistory and physical and physical examination to narrow the differential diagnosisexamination to narrow the differential diagnosis
3. Develop an evidence based diagnostic and 3. Develop an evidence based diagnostic and
treatment algorithm for usetreatment algorithm for use
Causes of Shoulder Pain in the Causes of Shoulder Pain in the Primary Care Setting:Primary Care Setting:
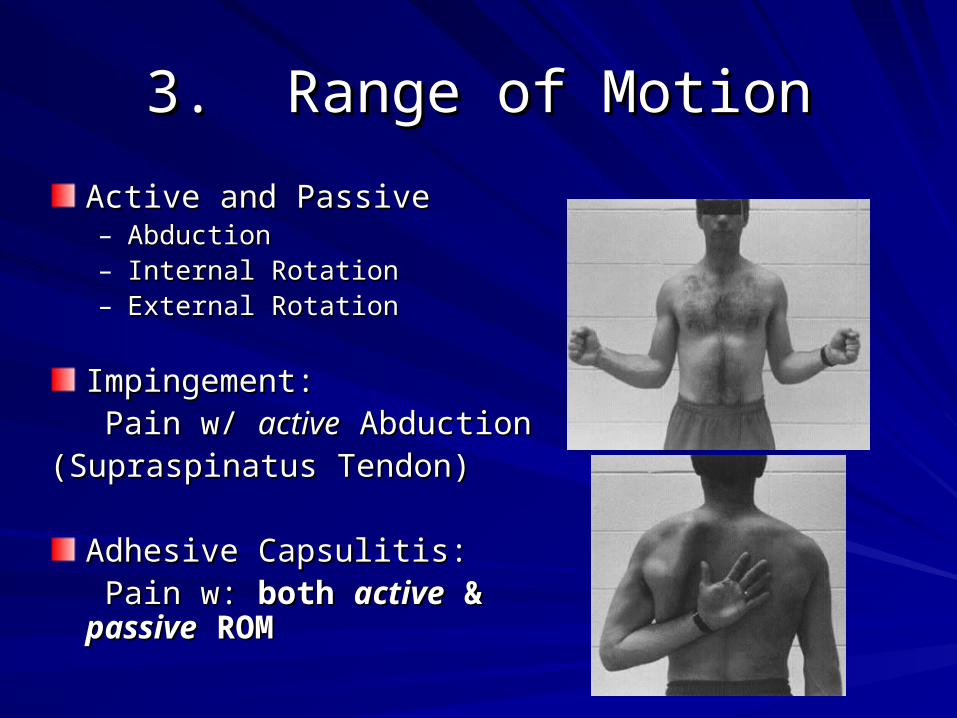
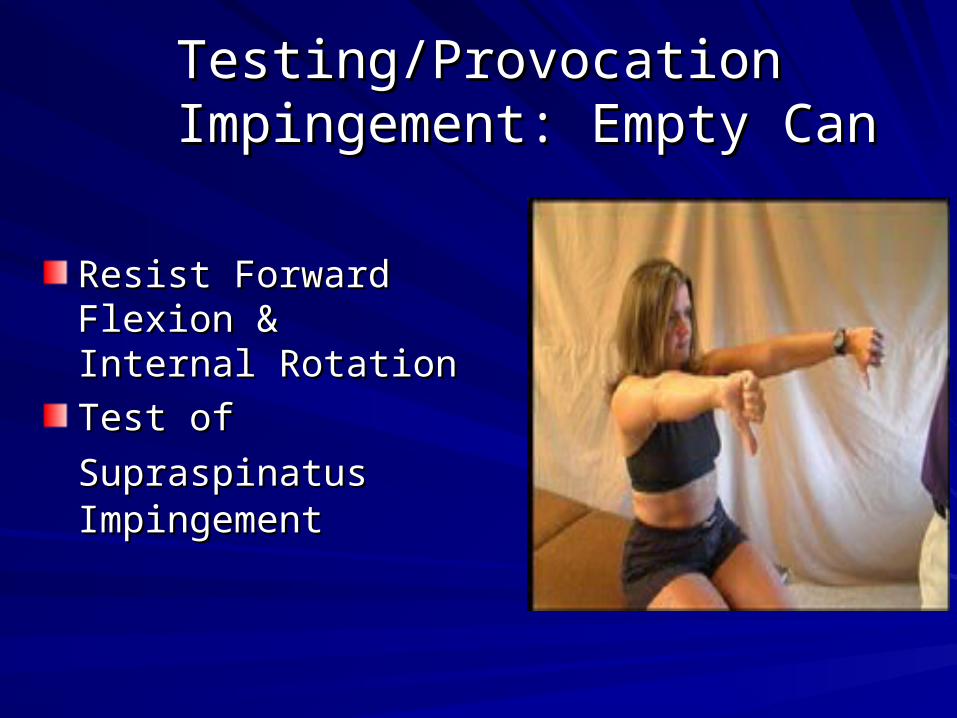
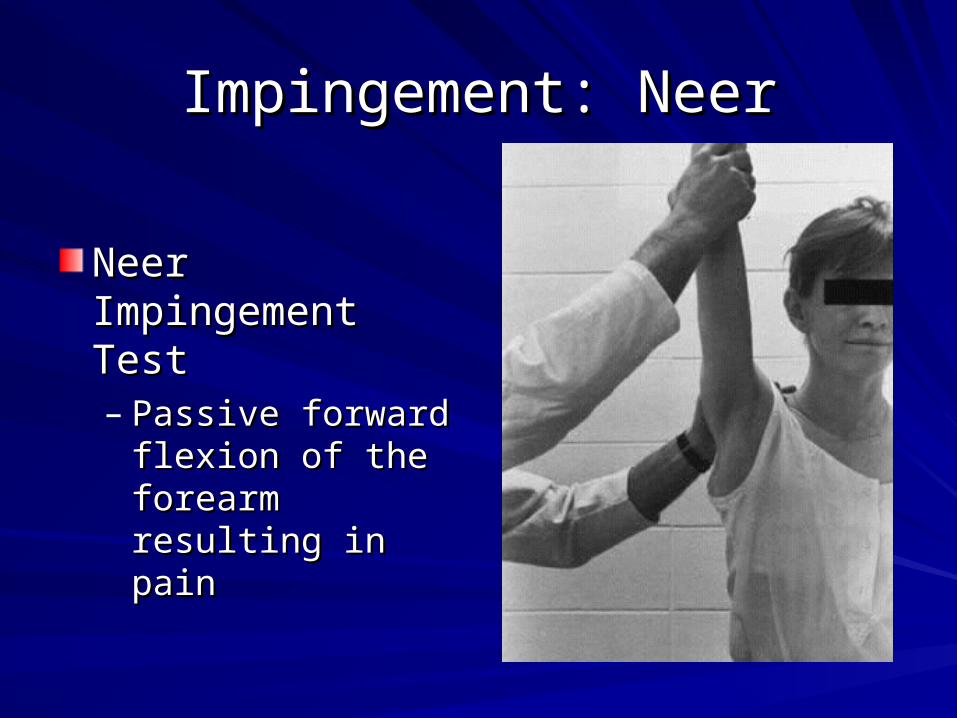
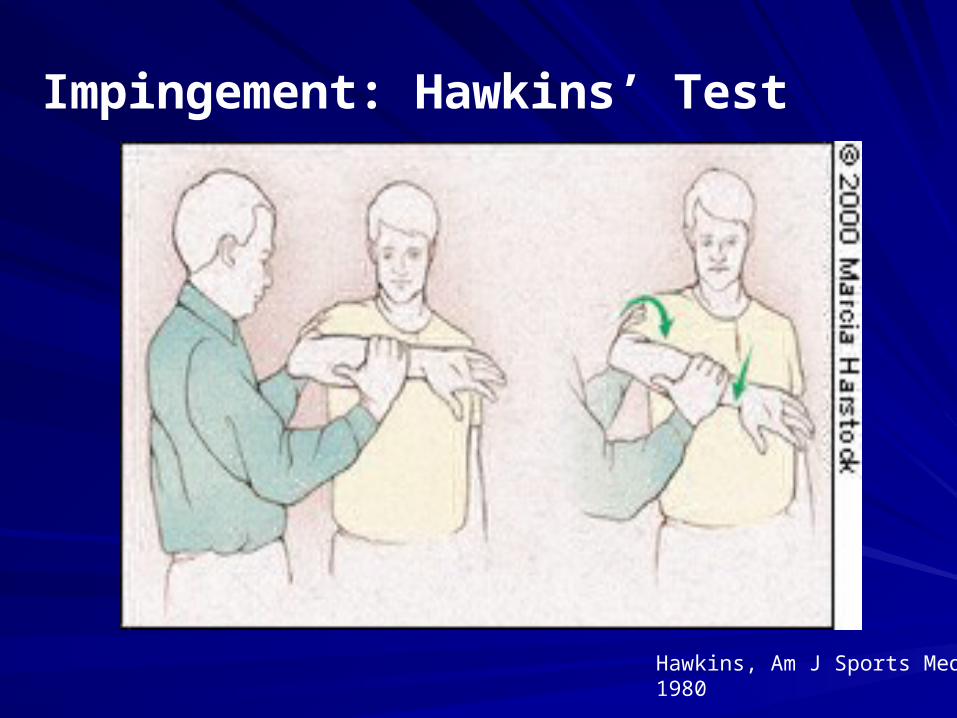
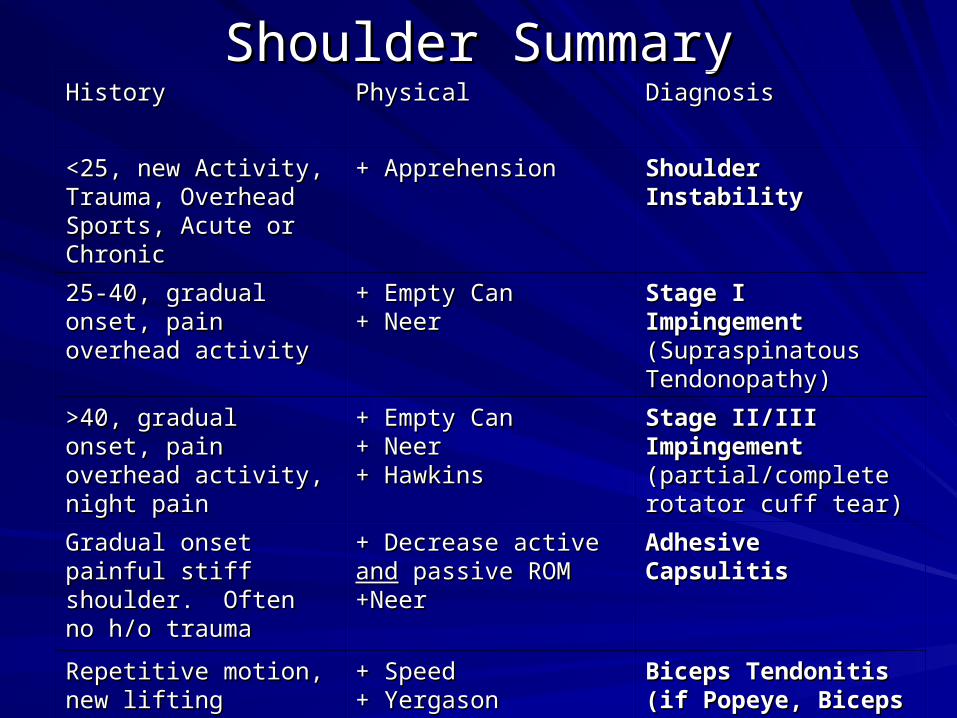
Impingement Syndrome >70%
Adhesive Capsulitis 12%
Bicipital Tendonitis 4%
A/C Joint OA 7%
Other (Instability, Infection) 7%
Smith, J Gen Intern Med 1992
Stats 101Stats 101
SensitivitySensitivity: : % of % of PeoplePeople with with Disease who Test + Disease who Test +
SpecificitySpecificity: : % of % of PeoplePeople without Disease who test Negative without Disease who test Negative (TN/(TN+FN) = b/(b+d)(TN/(TN+FN) = b/(b+d)
PPVPPV: : Percent of + Percent of + Test ResultsTest Results that are truly positive that are truly positive
RCT Pain -> RCT Pain -> ↓ ROM ↓ ROM ---> Contracture of joint capsule ---> Contracture of joint capsule
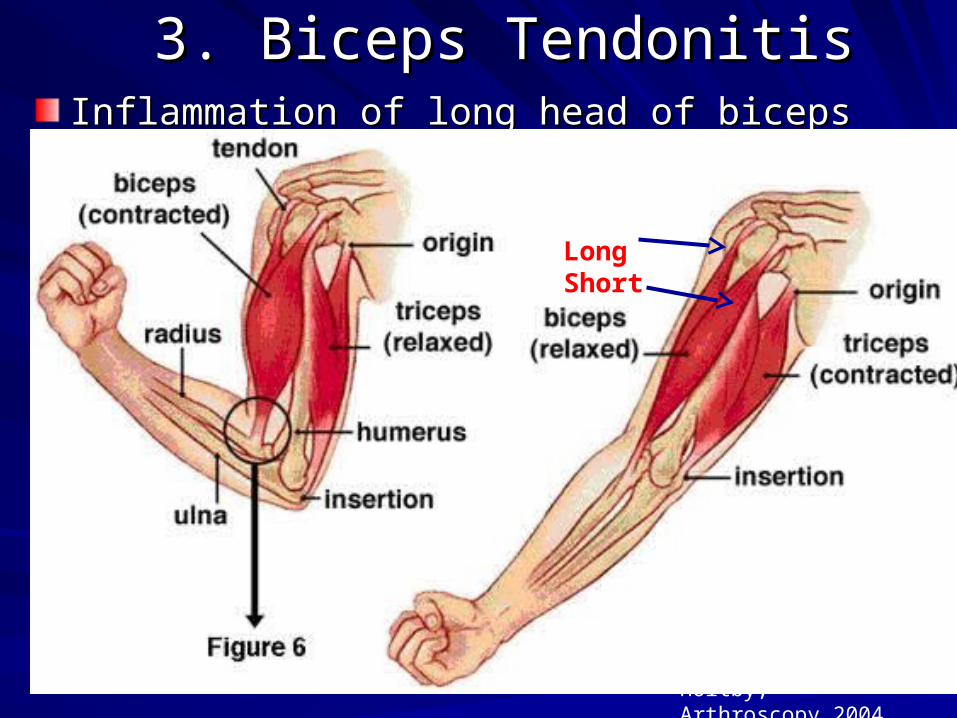
3. Biceps Tendonitis3. Biceps TendonitisInflammation of long head of biceps tendonInflammation of long head of biceps tendonRepetitive lifting, overhead reaching or supinationRepetitive lifting, overhead reaching or supinationAnterior humeral pain; tenderness bicipital grooveAnterior humeral pain; tenderness bicipital groove
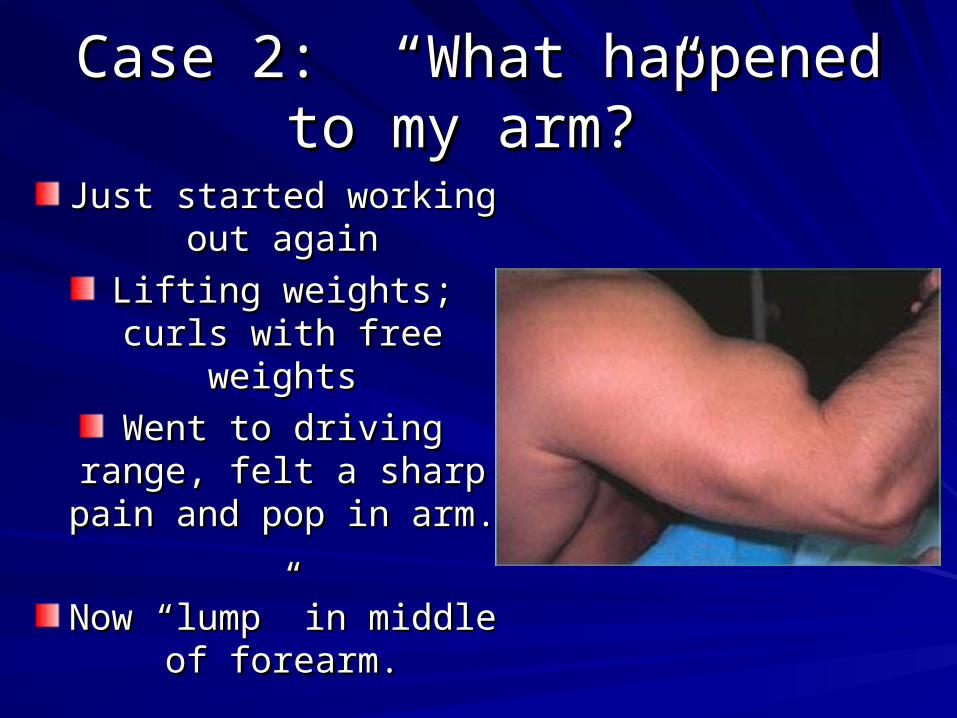
Tear of Biceps Tendon:Tear of Biceps Tendon:Chronically inflamed tendonChronically inflamed tendonLoss of flexion/supinationLoss of flexion/supination““Popeye Sign”—proximal to Popeye Sign”—proximal to antecubital fossaantecubital fossa
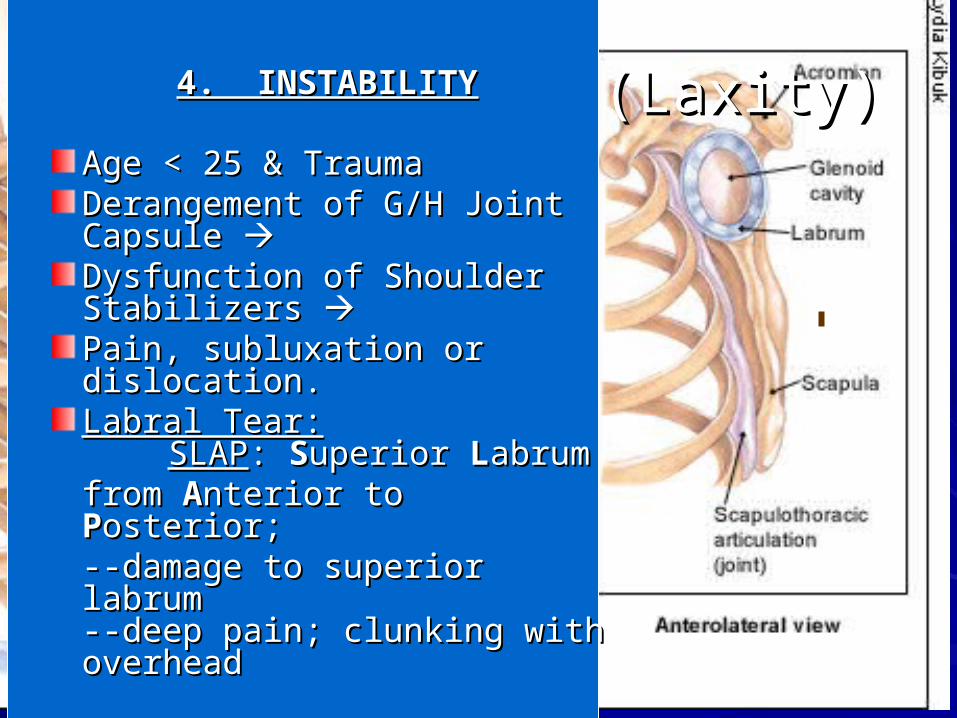
Age < 25 & TraumaAge < 25 & TraumaDerangement of G/H Joint Derangement of G/H Joint Capsule Capsule Dysfunction of Shoulder Dysfunction of Shoulder Stabilizers Stabilizers Pain, subluxation or Pain, subluxation or dislocation.dislocation.Labral Tear:Labral Tear:
SLAPSLAP: : SSuperior uperior LLabrum abrum from from AAnterior to nterior to PPosterior; osterior; --damage to superior labrum --damage to superior labrum --deep pain; clunking with --deep pain; clunking with overheadoverhead
7% Other7% Other
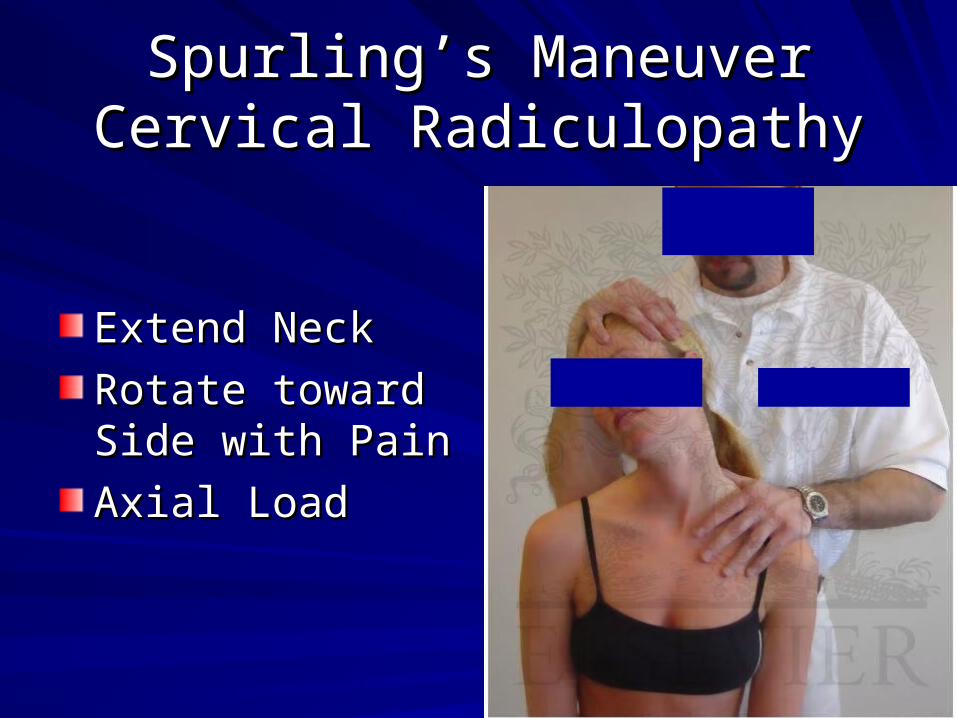
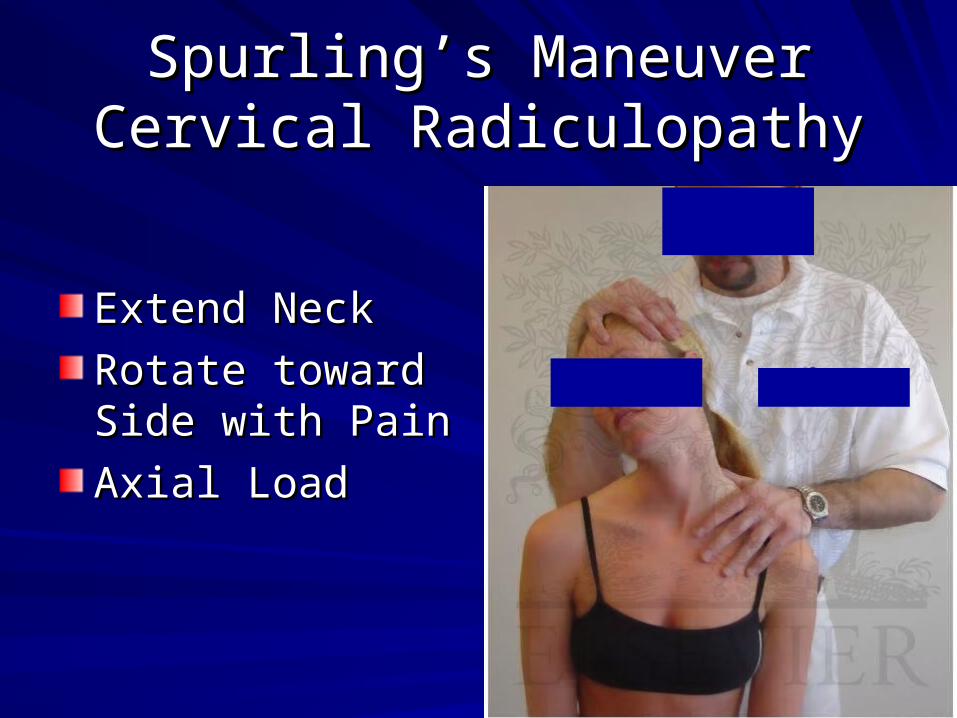
Cervical Radiculopathy Cervical Radiculopathy (neck pain, pain that (neck pain, pain that radiates to the elbow)radiates to the elbow)
Infection (G/N, Lyme)Infection (G/N, Lyme)
Left Sided: CVD/Anginal Left Sided: CVD/Anginal EquivalentEquivalent
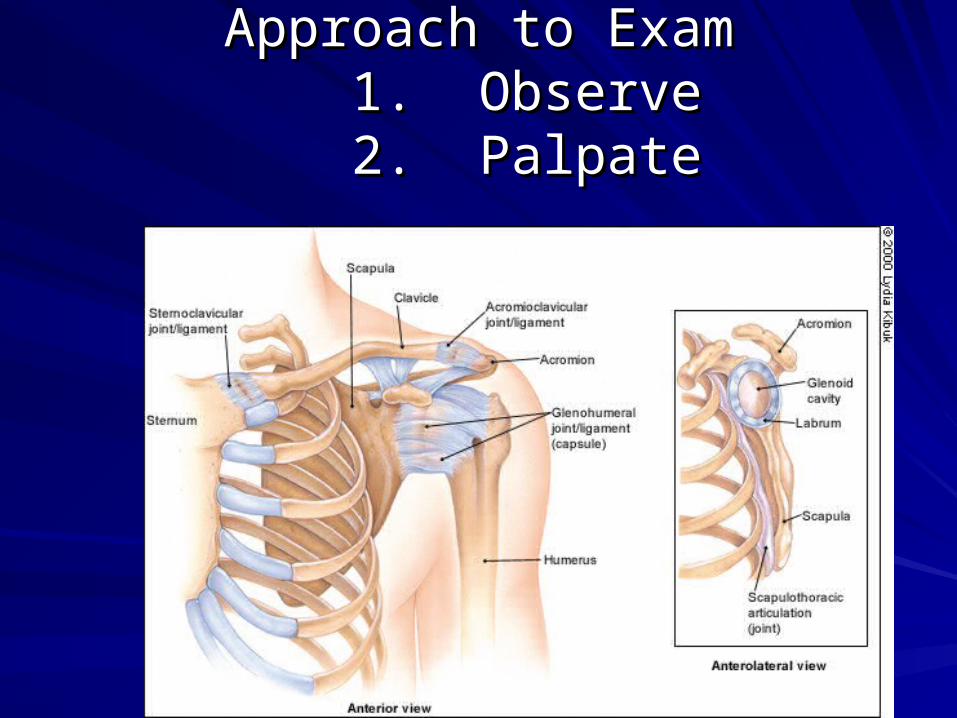
Introduction to ExaminationIntroduction to Examination
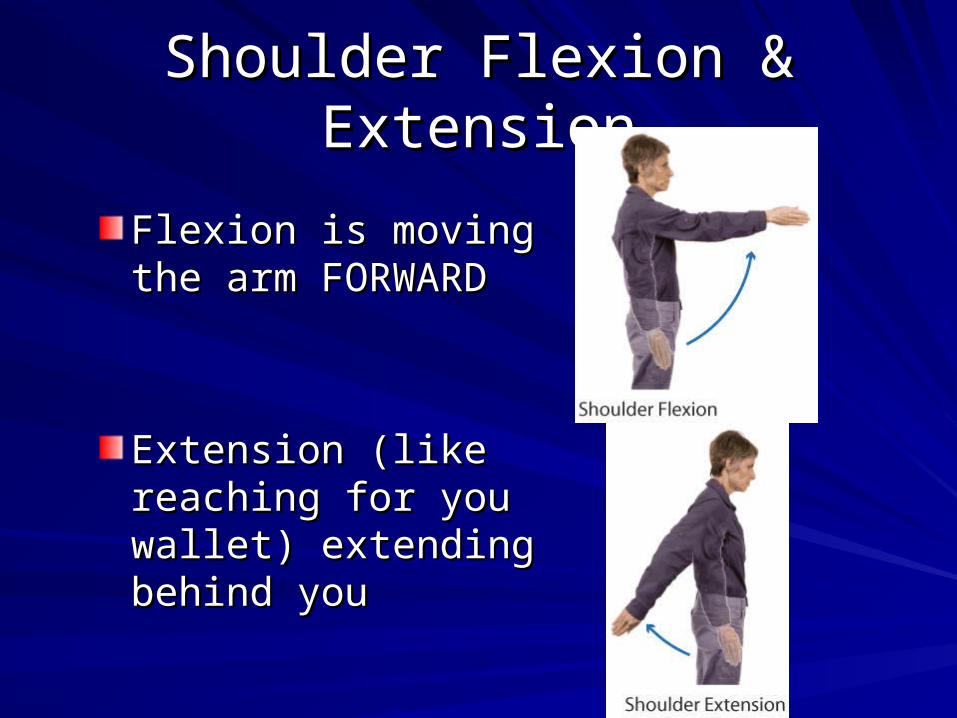
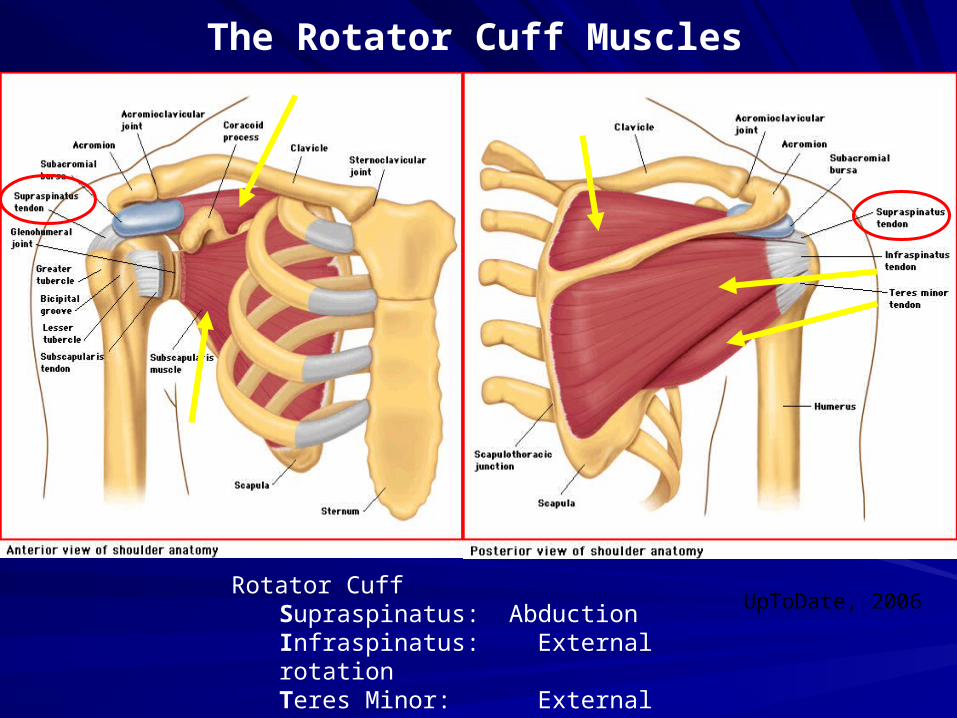
The shoulder is a The shoulder is a multiaxial ball-and-multiaxial ball-and-socket synovial jointsocket synovial joint
Depends on muscles Depends on muscles and ligaments rather and ligaments rather than bones for than bones for support and stabilitysupport and stability
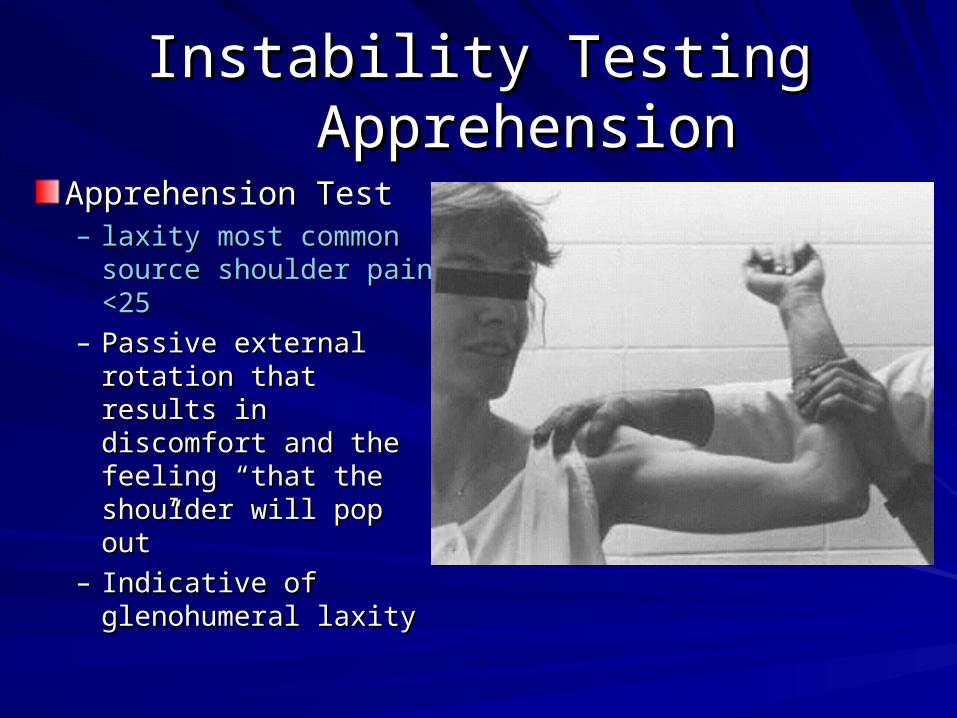
Apprehension TestApprehension Test– laxity most common laxity most common
source shoulder pain source shoulder pain <25<25
– Passive external Passive external rotation that results in rotation that results in discomfort and the discomfort and the feeling “that the feeling “that the shoulder will pop out”shoulder will pop out”
– Indicative of Indicative of glenohumeral laxity glenohumeral laxity
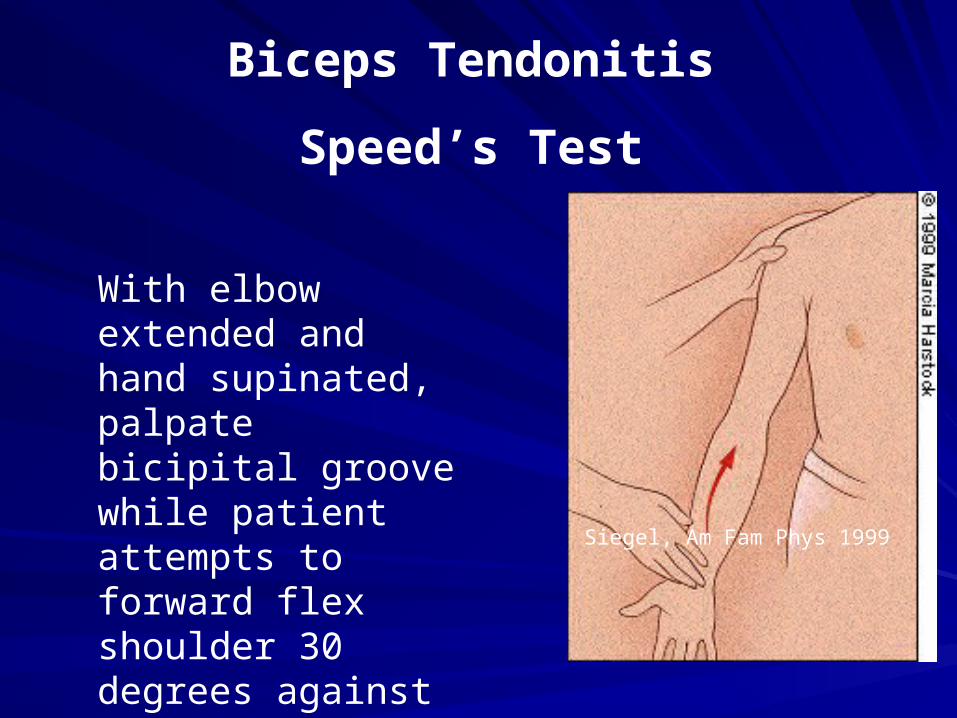
Biceps Tendonitis
Speed’s Test
With elbow extended and hand supinated, palpate bicipital groove while patient attempts to forward flex shoulder 30 degrees against resistance
Case 1. Doc, why does my Case 1. Doc, why does my shoulder hurt?shoulder hurt?
55 year old carpenter presents with 3 55 year old carpenter presents with 3 month history of right shoulder pain. month history of right shoulder pain. Gradual onset without h/o trauma. Gradual onset without h/o trauma. Pain at night when he lies on affected side Pain at night when he lies on affected side Pain with overhead activityPain with overhead activity
Reduce offending activitiesReduce offending activitiesPhysical TherapyPhysical TherapyNSAIDs or subacromial steroid injectionNSAIDs or subacromial steroid injection– Each is better than placeboEach is better than placebo– Little long term differenceLittle long term difference– No benefit in combination treatmentNo benefit in combination treatment
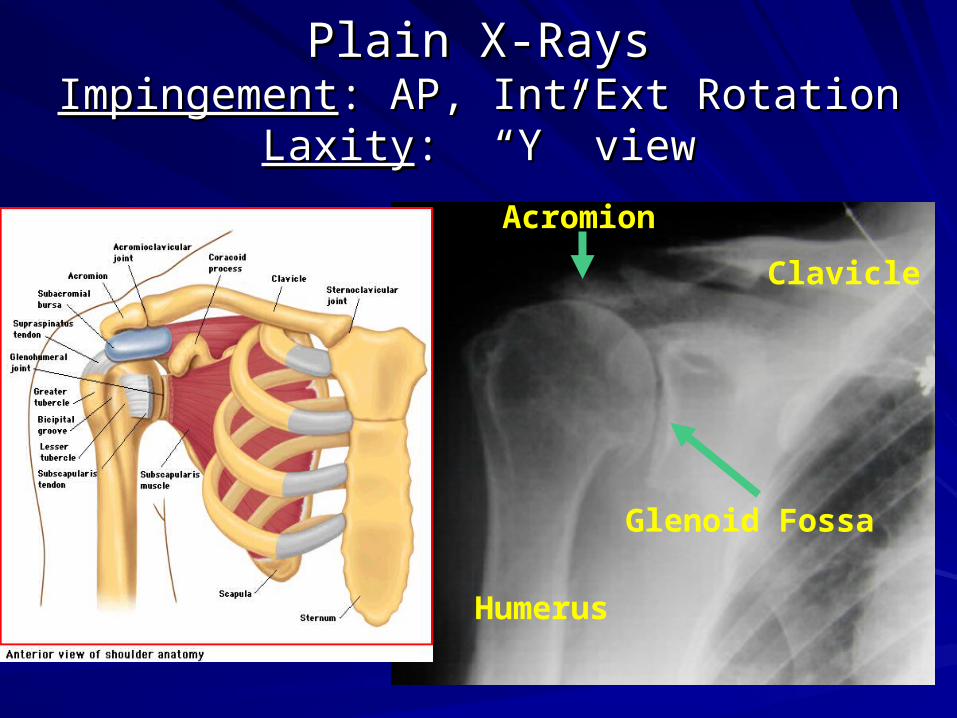
Obtain X-rays: AP w/Internal & External Obtain X-rays: AP w/Internal & External RotationRotation
Materials for Glenohumeral Materials for Glenohumeral Joint injectionJoint injection
5-10 cc Syringe5-10 cc Syringe
22 or 25 g 1 ½ needle22 or 25 g 1 ½ needle
3-5 ml of 1% or 2% Lidocaine w/o Epi.3-5 ml of 1% or 2% Lidocaine w/o Epi.
1-2 ml of1-2 ml of– 1 to 2 mL Triamcinolone (Kenalog) 40 mg/mL 1 to 2 mL Triamcinolone (Kenalog) 40 mg/mL
oror– betamethasone sodium phosphate and betamethasone sodium phosphate and
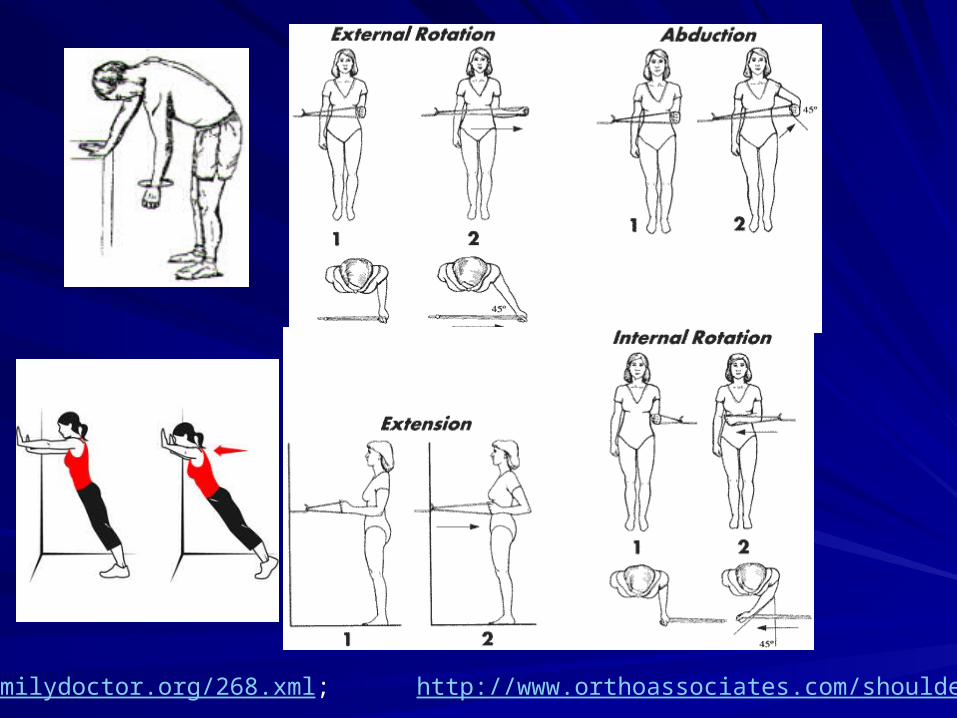
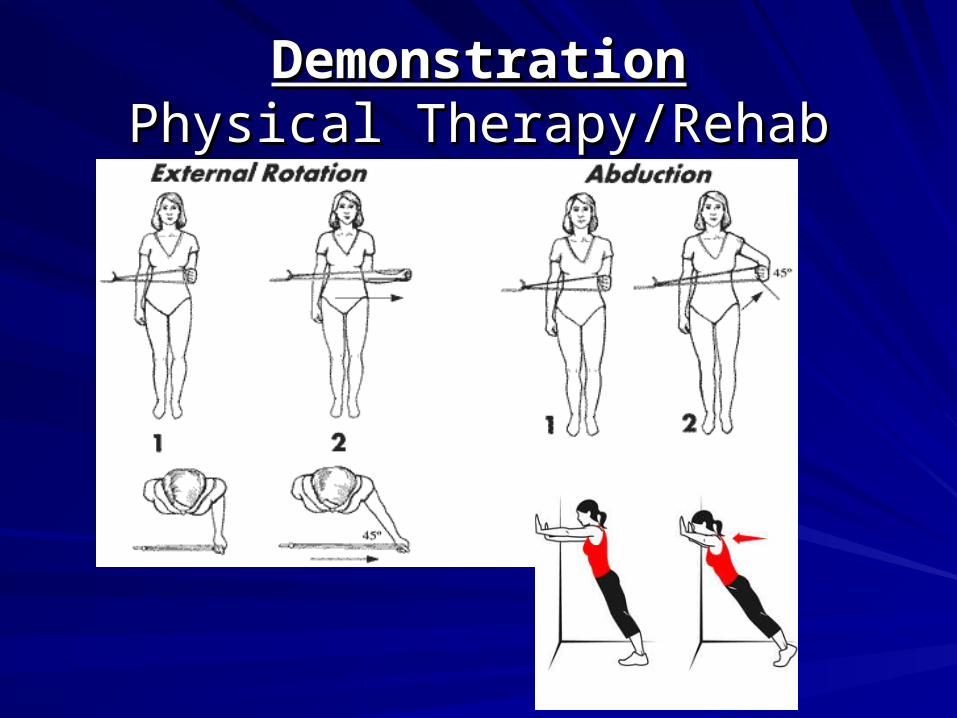
Physical TherapyPhysical TherapyNSAIDs or subacromial steroid injectionNSAIDs or subacromial steroid injection
– Most resolve with conservative treatment: Most resolve with conservative treatment: Stretching/Exercises x 18 monthsStretching/Exercises x 18 months; ;
– Orthopedic ReferralOrthopedic Referral
Case 2: “What happened to my Case 2: “What happened to my arm?”arm?”
Just started working Just started working out againout again
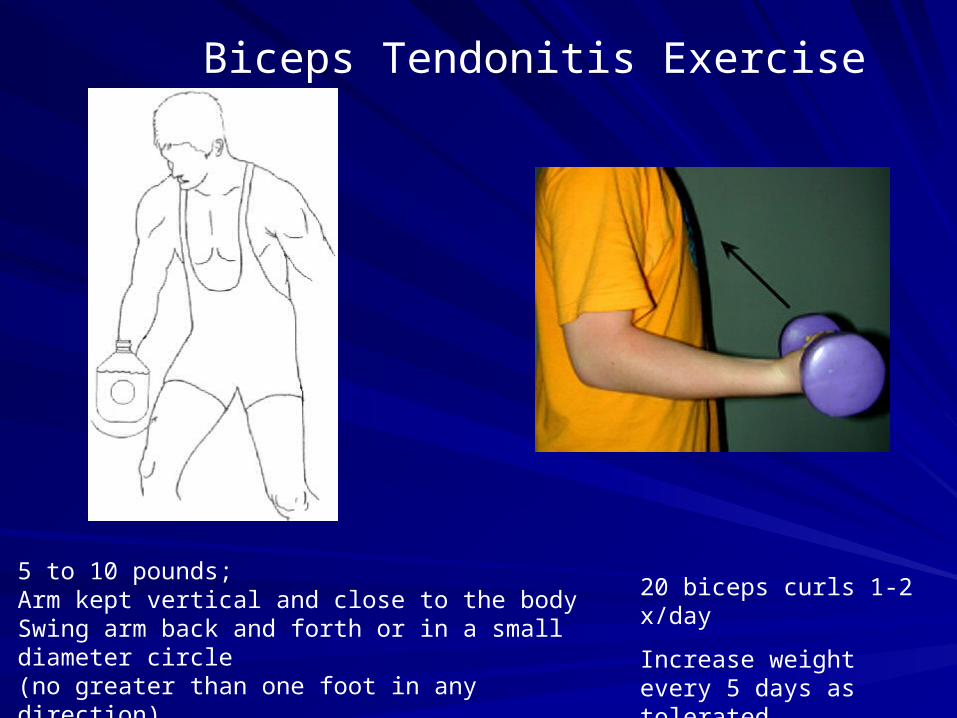
5 to 10 pounds; Arm kept vertical and close to the body Swing arm back and forth or in a small diameter circle (no greater than one foot in any direction).