43
Siddhartha S. Nadkarni, M.D. F.A.C.E.S. Conference May 5, 2013 DIAGNOSIS AND TREATMENT OF MOOD DISORDERS IN EPILEPSY
| Date post: | 23-Dec-2015 |
| Category: |
Documents |
| Upload: | andra-walters |
| View: | 215 times |
| Download: | 1 times |

Siddhartha S. Nadkarni, M.D.
F.A.C.E.S. Conference
May 5, 2013
DIAGNOSIS AND TREATMENT OF MOOD DISORDERS IN EPILEPSY




WHAT IS MOOD?• Emotional State or Frame of Mind
• Not an Emotion, less specific
• A Weather
• Not Temperament or Personality (which are more like a climate)

• Dysthymia
• Major Depression
• Bipolar Disorder
• Mania
• Depression
• Mixed States
• Bipolar I, Bipolar II
HOW TO DIAGNOSE MOOD DISORDERS


DYSTHYMIA• Chronic Depression
• More days than not for at least 2 years
• In kids can be irritability for at least 1 year
• Never goes more than 2 months without experiencing:
• Poor appetite or overeating
• Insomnia or hypersomnia
• Low energy or fatigue
• Low self esteem
• Poor concentration or difficulty making decisions
• Feelings of hopelessness

DEPRESSION• 5 Symptoms for at least 2 weeks:
• Depressed Mood*
• Sleep Disturbance
• Interest Loss (“Anhedonia”)*
• Guilty Ruminations
• Energy loss
• Concentration Loss
• Appetite Changes
• Psychomotor Changes
• Suicidal Thinking
• * One has to be depressed mood or loss of pleasure

MANIA• 1 Week of persistently elevated, expansive, or irritable mood (or any duration if
hospitalization required)
• During this time at least 3 of the following:
• Inflated self-esteem or grandiosity
• Decreased need for sleep
• More talkative or pressured speech
• Flight of ideas or racing thoughts
• Distractibility
• Increased goal-directed activity or psychomotor agitation
• Excessive involvement in pleasurable activities that have a high potential for painful consequences

BIPOLARITY AND DYSTHYMIA• Bipolar I is diagnosed by the presence of a manic episode
• Bipolar II is diagnosed by the presence of depression and hypomania
• Mixed state is when one meets criteria for both a depressive and manic episode
• Schizoaffective Disorder is characterized by psychosis between mood episodes
• Outside post-ictal or prodromal mood states, Depression is far and away the most common mood disorder in Epilepsy

DEPRESSION AND EPILEPSY
• Up to 80% of Epilepsy patients have depression (50% - 80%).
• Suicide attempts may be 4 times that of a control group with chronic neurologic illnesses.
• Depression was the only correlating factor in a recent study in terms of quality of life for a wide range of seizure patients (Boylan, 2004) including sz type/frequency/location/medications, etc.

DEPRESSION AND EPILEPSY
• Increased Suicide attempts related to interictal psychopathology (borderline p.d., psychosis) rather than sz frequency, medications, psychosocial stressors (Mathews and Barabas, 1981; Medez et al., 1989)
• Biological Factors contributing to interictal depression:• Family History of Mood Disorders• Left Sided Sz focus• Bilateral Frontal Hypometabolism

DEPRESSION AND EPILEPSY
• WAY UNDERRECOGNIZED AND UNDERTREATED (BOYLAN, 2004).
• May be different than “major depression.”
TREATMENTS FOR DEPRESSION IN EPILEPSY• Antidepressants
• Anti-Epileptic Drugs
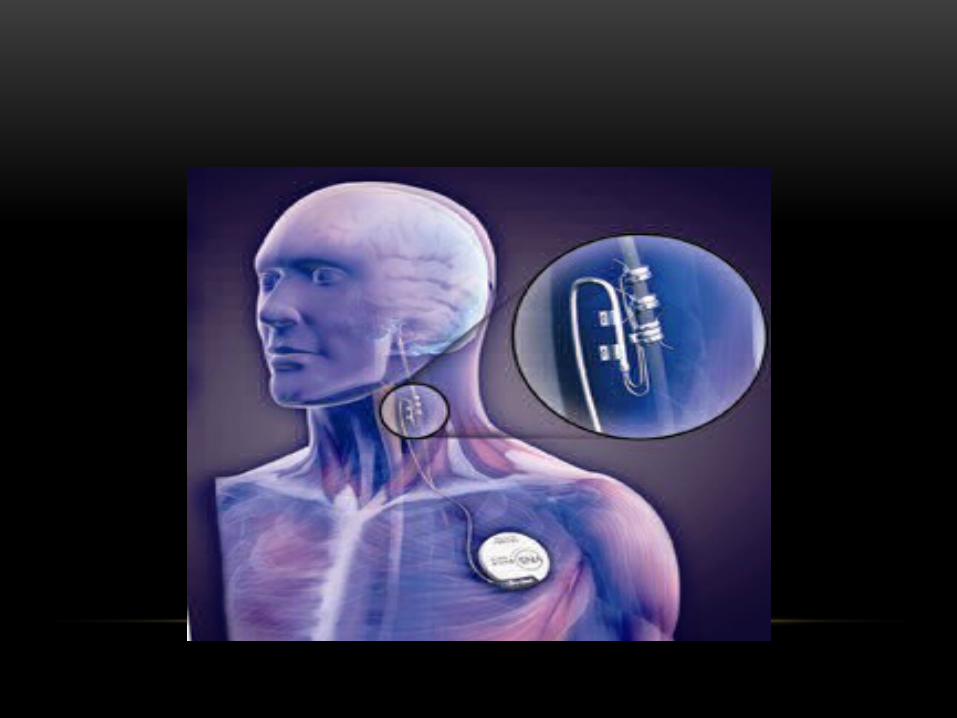
• Vagus Nerve Stimulation
• Cognitive Behavioral Therapy
• Transcranial Magnetic Stimulation
• Future Directions and Alternative Treatments

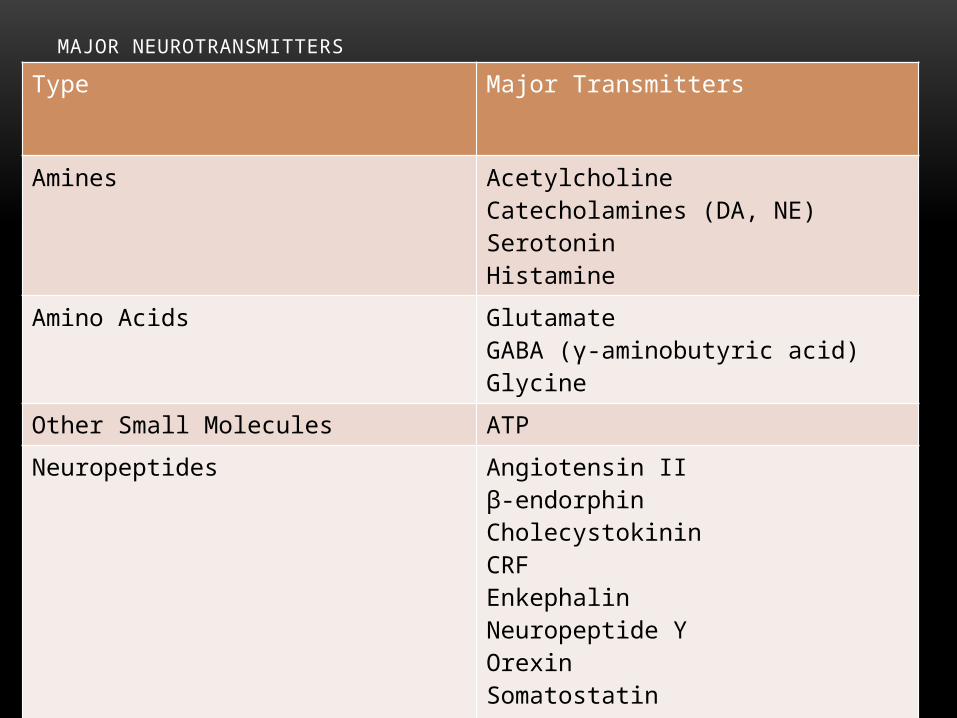
MAJOR NEUROTRANSMITTERSType Major Transmitters
Amines AcetylcholineCatecholamines (DA, NE)SerotoninHistamine
Amino Acids GlutamateGABA (γ-aminobutyric acid)Glycine
Other Small Molecules ATP
Neuropeptides Angiotensin IIβ-endorphinCholecystokininCRFEnkephalinNeuropeptide YOrexinSomatostatinSubstance PMany others

NOREPINEPHRINE

SEROTONIN

ANTIDEPRESSANTS



RISPERDAL
Karen Blair has Schizophrenia. “The magnificent Circus”

SIDE EFFECTS
• All Anti-Epileptic Drugs (AED’s) have side effects.
• In a given patient these effects may be problematic or helpful.
• The Goal of Epilepsy treatment is to obtain seizure freedom without untoward side effects.
• A note about the PDR.

AED’S
• Depression
• Phenobarbital
• Zonegran
• Depakote
• Dilantin
• Keppra
• Anxiety
• Keppra
• Lamictal
• Felbatol

ZYPREXA
“She Likes You”

POSITIVE SIDE EFFECTS
• Mood Stabilization:
• Tegretol
• Depakote
• Lamictal
• Antidepressant
• Lamictal
• Stimulant
• Lamictal
• Anxiolytic
• N eurontin
• Phenobarbital
SEROQUEL
“What Jack Saw”



Neuropsychopharmacology, April 2001

• Open Pilot Study of 60 patients with treatment resistent depression
• 2 weeks single blind recovery (no stimulation) followed by 10 weeks of VNS
• 59 completers because one person improved during recovery period (no stim)
• Conclusions:
• 30.5% responder rate for HRSD
• 30% responder rate for the MADRS
• 37.3% responder rate for the Clinical Global Impression-Improvement Score
• Of those who had received 7 or more antidepressants, none responded
• 39% of the rest responded
• Those who never had ECT were 3.9 X more likely to respond
• Most Common Side Effect was Hoarseness in 55%
• Good for low to moderate antidepressant resistence
Biological Psychiatry 2005

• 222 patients
• 15% responded in active treatment
• 10% responded in sham arm
• 1% dropped out for non-tolerabilty
• No evidence of short term efficacy


ELECTROCONVULSIVE THERAPY
• ECT is likley the most effective treatment we have for Depression
• ECT is not contraindicated in Epilepsy
• In fact ECT came into use due to “forced normalization.”
• ECT can be used to abort Status Epilepticus

TREATMENT TIPS• First step is diagnosis. We don’t do as good a job as we should in asking
about these symptoms. You may need to tell us.
• Remove inciting AED’s.
• Antidepressants, may respond to lower doses in this population.
• Antipsychotics as needed or in low doses.
• Stimulants.
• Anti-anxiety medications may treat both seizrues and anxiety but tolerance and withdrawal are worries.

















