270
0 Simmons College Dietetic Internship Program Student Handbook 2012-2013 Simmons College Department of Nutrition Boston, MA Preparing the Future Leaders of Healthcare
| Date post: | 21-Mar-2018 |
| Category: |
Documents |
| Upload: | truongcong |
| View: | 225 times |
| Download: | 4 times |
0
Simmons College Dietetic Internship Program
Student Handbook 2012-2013
Simmons College Department of Nutrition
Boston, MA Preparing the Future Leaders of Healthcare

1
TABLE OF CONTENTS
Topic/Section Page
General Information/Policy and Procedures
Simmons College Dietetic Internship Mission Statement and Goals 3-5
Simmons College Dietetic Internship Rotation and Affiliation Descriptions 6-10
Simmons College Dietetic Internship Policies and Procedures 11-17
Simmons College Nutrition Department CORI Policy 18-19
The Code of Ethics for the Profession of Dietetics 20-27
Simmons College Policy on Non-Discrimination and Grievance Procedures 28-36
Competency Statements for the Supervised Practice Component of Entry-Level Dietitian Education Programs
37-41
Allocation of the General and Community-focused Competencies to the Simmons College Dietetic Internship Rotations
42-43
Evaluation Forms
Simmons College Dietetic Internship Student Performance Evaluation Sheet Instructions
44-46
Rotation Evaluation: Clinical/Acute Care Competencies and Planned Experiences
47-54
Rotation Evaluation: Community Health Center Competencies and Planned Experiences
55-63
Rotation Evaluation: Department of Public Health Competencies and Planned Experiences
64-69
Rotation Evaluation: State Government Nutrition Initiative Competencies and Planned Experiences
70-77
Rotation Evaluation: Counseling and Education Competencies and Planned Experiences
78-85
Rotation Evaluation: Food Service Competencies and Planned Experiences 86-94
Rotation Evaluation: Research and Professional Practice Planned Experiences
95-98
Student’s Evaluation of Their Clinical Education Experience 99-106
Simmons College Dietetic Internship Evaluation of the Joint Dietetic
Internship Class Days
107-109
2
Clinical and Acute Care Worksheets
Medical Terminology Worksheets 110-117
Therapeutic and Mechanically Altered Diet Worksheets 118-120
Formulary Overview 121-122
Review of Common Lab Values 123-132
Review of Common Drug-Nutrient Interactions 133-139
Enteral Nutrition Worksheets 140-157
Parenteral Nutrition Worksheets 158-179
Counseling and Education Worksheets
Counseling and Education Tips 180-189
Nutrition Care Process (NCP) Worksheets 190-196
Pregnancy and Lactation Worksheets 197-206
Diabetes Worksheets 207-221
Anemia Worksheets 222-227
Community Health Center and Department of Public Health Worksheets
Public Policy and Legislation Information 228-234
CHC Demographic and Data Collection 235-238
Nutrition Programs and Services Worksheets 239-242
SNAP Worksheets 243-244
CHC Case Study 245
Food Service Worksheets 246-270

3
SIMMONS COLLEGE DIETETIC INTERNSHIP PROGRAM
Mission Statement and Goals The Mission of the Simmons College Dietetic Internship Program
The Simmons College Dietetic Internship Program and the Department of Nutrition upholds the mission, goals and objectives of the College. Simmons College Mission: Simmons College exists to educate, empower and transform the lives of its students, preparing them for leadership in the professions, in their communities and in the world. Department of Nutrition Mission The Mission of the Simmons College Department of Nutrition is twofold. The first is to educate students to:
Foster an appreciation of lifelong learning in preparation for success in advanced
nutrition or dietetics education or employment. Be effective in a profession that works to affect the eating behaviors and
subsequent health and quality of life of a multicultural and diverse population. Add to the scientific investigation about food and health, and one that fosters an
appreciation of food’s relationship to other sciences.
Secondly, the nutrition mission is to provide the entire College community with the intellectual basis and professional expertise for achieving and/or maintaining health through food habits. The mission of the Department of Nutrition embraces the broad mission of the College, where academic and real world experiences prepares undergraduate women and graduate students for rewarding lives and careers. The College reflects beliefs that professional education is not enough to equip graduates for the lives they may expect to lead; a Simmons education embodies the principles of a liberal arts and sciences education with professional education within the context of a multicultural society. The Department of Nutrition philosophy supports the concept that nutrition is a science governed by the rigorous rules of scientific investigation. It is a biological science because its elements, nutrients, are chemicals and chemical compounds which participate in the regulation of homeostasis and, thus, the continuity of life. Nutrition is further a social science, because its elements are consumed, primarily, in the form of food on a regular basis. How and why food is chosen is determined by a set of human behaviors that are constantly refined by such diverse forces as biology, environment, economics, politics, culture and the effect of the media. Since the faculty further believes that the practice of Dietetics is predicated, in large part, on the science of Nutrition, the Department of Nutrition’s contribution to the education of dietetic practitioners is philosophically consistent with the mission of the College and in harmony with societal expectations of professional health care workers.
4
Simmons College Dietetic Internship Mission: is to graduate competent, ethical entry level practitioners who build on evidence-based research and standards of practice and standards of professional performance to provide nutritional care, health promotion and disease prevention that is culturally and economically sensitive. Our graduates will develop an appreciation for life-long learning to increase knowledge and enhance professional development. The program’s mission is consistent with the standards of practice and the standards of professional performance. The mission statement for the dietetic internship can also be found in the School of Nursing and Health Sciences Nutrition catalog. The commonalities among the three mission statements are the acquisition of knowledge and education and professional practice. The College, department and internship program work to integrate quality education into preparation for professional practice among our graduates. The Simmons College Dietetic Internship Program supports the Department of Nutrition mission, goals and objectives and supports the mission and vision statements of the College. The ongoing objectives of a Simmons education include preparing women and men to be well informed, open minded, and sensitive to values; committed to learning as a continuing experience; thoughtful, analytical, and flexible in their approach to new information and new intellectual challenges; competent in at least one area of concentration or specialization, but responsive to the variety of opportunities open to them; knowledgeable in at least one area related to their career objective; and successful in integrating their education with their personal and professional lives. The program’s mission is consistent with the standards of practice and the standards of professional performance. The students participating in our dietetic internship program have committed to a degree in the field of dietetics. It is through the Simmons College dietetic internship program that our students will gain quality hands-on education as it relates to the interdisciplinary art and science of nutrition and dietetics. The program recognizes that the education of dietitians in health-care settings other than the hospital has taken on more significance with the need for cost containment and the advent of preventive medicine. As a result, the program curriculum supports the current trend away from acute hospital-based care towards, wellness, health promotion and disease prevention. The Dietetic internship supports the Department of Nutrition statements:
To foster the development of skills in critical analysis. To foster a creative and effective approach to problem solving. To provide opportunity for the direct application of didactic material. To encourage students to recognize the importance of continuous learning for
enrichment of their personal and professional lives. To provide an environment which encourages and contributes to an understanding
of the psychological, social, cultural, and economic factors that influence food consumption in various populations.
To provide students with the skills which will enable an objective and competent interpretation of the scientific literature in order to better understand the relationship of nutrition to health promotion, wellness and disease prevention, and

5
the involvement of adequate nutrition in human development and in the aging processes.
Simmons College Dietetic Internship Program Goals and Objectives Simmons College Dietetic Internship Program Goals Since the profession of dietetics is built on a conceptual framework that is constantly changing as a result of the discovery of new operational principles, evidenced based research, and standards of practice, the dietetic internship’s goals are: Simmons College Program Goal #1 Prepare dietetic professionals for a career using their intellectual and clinical skills to function within a community nutrition health promotion and wellness setting, acute care setting, and food service management setting as an entry level practitioner. Program Goal #1 Outcome Measures
Over a five year period, 70% or more of DI graduates who seek employment in dietetics will be employed within three months of completing internship.
80% of employers will rate graduates as strong or superior in nutritional knowledge and professional skills compared with other entry level practitioners.
100% of interns enrolled in the DI program will complete the program requirements within 50 weeks, or, 150% of the time planned for completion.
Simmons College Program Goal #2 Prepare entry-level dietitians who participate in continuous learning and professional development activities. Program Goal #2 Outcome Measures
Over a five-year period, the pass rate for DI graduates taking the registration examination for the first time will be at least 80%.
80% of graduates seeking acceptance to graduate programs in place of employment will enroll within 5 months of program completion.
80% of graduates will indicate they participate in continuing education and professional development activities.
6
SIMMONS COLLEGE DIETETIC INTERNSHIP PROGRAM
Rotation and Affiliation Descriptions
Description of the Simmons College Dietetic Internship Program
The Simmons College dietetic internship program is a full-time, 33-week community-oriented internship experience for students who would like to become registered dietitians. The program’s goal is to provide students with both the attitude and skills necessary to continue learning in a dynamic discipline. Students will develop the intellectual and clinical skills of a successful professional so as to function efficiently and effectively within a healthcare or community setting. The emphasis of the program reflects the current trend away from acute hospital-based care towards health promotion and disease prevention. Upon completion of the program the student is expected to be properly prepared, from a hands-on practical standpoint, to complete the examination to gain registered dietitian status in accordance with the Commission on Dietetic Registration. The program consists of seven supervised practice rotations that take place annually between the months of September and April. Currently, the program enrolls nine students. The rotations are as follows:
Ten weeks at an acute care hospital. Four weeks at a community health center Four weeks at a state or local department of public health. Four weeks at a state government-based nutrition initiative such as a state program which
directs or provides services to elders though federal and state funding. Four weeks in a counseling and education setting (corporate fitness programs, outpatient
programs offered by acute care hospitals or a renal dialysis unit, to name a few) or with a private practice dietitian focusing on individual and group nutrition education and counseling.
Six weeks at a long term care facility, community hospital, school foodservice or other related facility concentrating on food service-related experiences and gaining exposure to the role a dietitian in the assigned setting.
One week in a research and professional practice rotation directed by the Internship Director and Coordinator.
The remainder of this document will briefly describe each of the rotations that students will attend during their experience as a means of satisfying the program’s completion requirements, including meeting the thirty-eight core competencies and four community competencies set forth by the American Dietetic Association. Furthermore, information will be provided on what types of facilities and preceptors are utilized for each of the rotations.

7
Preceptor/Faculty Selection The Simmons College Nutrition Department selects affiliations that support the mission and goals of the Program. Preliminary discussions are conducted with all new affiliating preceptors to ensure that students obtain the type of experience expected and supervision required, and to assess the affiliating faculty’s willingness to complete written student evaluations. Throughout the internship program written and oral communication is made with affiliating faculty to ensure that they are providing entry level dietetic skills as determined by the competencies set forth by the American Dietetic Association. Furthermore, recruitment of affiliations is based on the ability of the sites to provide a variety of community-oriented experiences that encompass diverse ethnic, cultural, economic, political, and age-specific populations. This will ensure that students are prepared for the multitude of community-based employment opportunities available to dietitians. The internship is designed to prepare interns for entry-level positions in the dietetics field. For this reason, Simmons arranges fieldwork sites for students, which provide maximum educational benefits to interns this includes fieldwork sites at which students will not be used to replace employees. If an intern feels that he/she is continually being used to replace employees, then the intern is asked to discuss this with the internship director or coordinator.
Preceptor Requirements The primary supervisor at each site must be a registered dietitian, appropriately credentialed or have equivalent experience, such as food service managers, and also must be employed by the affiliating institution. It is also highly encouraged that the faculty to student ratio at the affiliations is one to one, although exceptions may be made if it is determined that the experience is conducive to two interns completing the same rotation in tandem. A copy of all the preceptors resumes are kept on file in the Nutrition Department. Preceptors are contacted and provided with the competencies and sample experiences appropriate to the rotation. Preceptors review with the coordinator responsibilities for providing appropriate experiences. Preceptors must agree to supervise students and give formative and summative feedback in a timely manner. If a preceptor agrees to meet these expectations a contract is sent to the preceptor for review and is signed by the appropriate individual within the organization. Throughout the internship program written and oral communication will be made with affiliating preceptors to ensure that they are providing entry-level dietetic skills as determined by the competencies set forth by the American Dietetic Association. Furthermore, it is a policy of the Simmons College Dietetic Internship Program to obtain sites that can provide a variety of community-oriented experiences that encompass diverse ethnic, cultural, economic, political, and age-specific populations. This will ensure that students are prepared for the multitude of community-based employment opportunities available to dietitians. Contractual agreements between Simmons College and the affiliating sites are required and are managed by the Graduate School for Nursing and Health Sciences. The current contract has been

8
approved by the Associate Provost after consultation with appointed lawyers. The contracts will be kept on file in the Nutrition Department. Both Simmons College and the affiliating sites will have an originally signed copy of the contract. The following is a list of acceptable types of facilities for each of the six offsite rotations: Acute Care/Clinical Rotation (10 weeks) Students will be placed in a hospital setting, preferably a community teaching hospital. The hospital should offer a variety of services to ensure a well-rounded and varied experience. Students are expected to gain experience in nutrition screening, charting, developing nutrition care plans, enteral and parenteral nutrition, and interacting with patients and health care professionals. They should aim to start their experience by working on simpler tasks and advancing to more complex tasks as their experience proceeds. In addition to a strong inpatient component, most affiliating agencies offer a wide variety of outpatient preventative health and educational programs on topics such as weight management, healthy heart, bone health, women’s health, pregnancy, lactation and childcare and alternative medicine. Current Facilities Used in the Greater Boston Area: Cambridge Hospital, Caritas Carney Hospital, Faulkner Hospital, Lemuel-Shattuck Hospital, Melrose-Wakefield Hospital, Milton Hospital, Whidden Hospital. Preceptor: The preceptor must be a registered dietitian. The preceptor must be available to the student during the time that they are at the facility. In other words, there must be at least one full time dietitian available to the student at all times. It is also valuable if the facility has diet technicians so the student can supervise their work. Food Service Rotation (6 weeks) Students are assigned to a community-based food service location to complete their food service requirements. The location may be a school food service, community hospital, long term care food service, or any other appropriate community-based organization that will provide an appropriate experience. Students will learn how a foodservice operation functions and will begin to develop managerial skills through observation and practice. Students will also become familiar with the nutritional procedures and forms that are required by state and federal mandates in various facilities. Students may be placed in a long term care facility if they indicate that they would like to gain experience in this sector. Placement in a long term care facility is beneficial since a large segment of the population is aging and the demand for dietetic professionals in long term care is expected to rise dramatically. Ideally, the students will be able to complete their food service requirements and gain considerable experience with a consulting dietitian. The benefit of obtaining these two experiences at one site is that the student can acquire a strong working knowledge of how food service systems and medical nutrition therapy are coordinated to ensure provision of quality dietary care. Students may also be placed in a K-12 school food service program or at a public or private school, college or university. Here students will learn the in’s and out’s of feeding larger groups of people in a specialized setting, and in the primary school setting will be exposed to school

9
feeding programs such as the school breakfast and lunch programs. In these settings, students will perform virtually all food service tasks, provide education and counseling to students and employees, and assist in any healthy initiatives within the school. Current Facilities Used in the Greater Boston Area: Caritas Carney Hospital, Lemuel Shattuck Hospital, The German Centre for Long Term Care, Simmons College Food Service, Manchester Essex School Food Service, Medford Public Schools, Berkley College of Music Food Service. Preceptor: The preceptor must be a registered dietitian, food service director and/or food service supervisor. Public Health Rotation (4 weeks) Students are to spend time at the local department of public health so that they can observe and participate in policy development, education and training, program development and implementation, the legislative process, and research and epidemiology as it relates to nutrition and physical activity. The programs should emphasize development of strategies and programs for health promotion and disease prevention for children, adolescents, adults, elderly and families. Some of the nutrition-specific programs administered by the local department of public health could include maternal and child health education, healthy start, W.I.C., diabetes control, food stamp outreach, growth and nutrition, women’s health, fitness and physical activity promotion, and osteoporosis prevention. Current Facilities Used in the Greater Boston Area: Massachusetts Department of Public Health, United State Department of Agriculture (USDA) North East Regional Office. Preceptor: It is preferred that the main preceptor for this rotation is a registered dietitian. However, it is expected that students will spend time with other health care professionals during this rotation. Community Health Center Rotation (4 weeks) Interns rotate at a Boston area community health center which will provide a multi-ethnic supervised practice experience. The assigned community health center will generally be a non-profit, community-based organization that provides primary and preventive health care services to their communities, particularly the vulnerable and underserved populations. Students will gain proficiency in providing nutrition counseling and education in an outpatient or community setting, with both individuals and groups, and become active participants in public health initiatives such as W.I.C. (Women, Infants and Children), Maternal and Child Health (MCH), and special programs that assist elders in leading independent lives. During this rotation, students can also work with community hunger agencies such as soup kitchens, food pantries and food banks, to name a few. Current Community Health Centers Used in the Greater Boston Area: East Boston Neighborhood Health Center, Roxbury Comprehensive Community Health Center, Dimock Street Community Health Center, and Manet Community Health Center, Cambridge Health Alliance Community Health Centers. Preceptor: It is preferred that the main preceptor for this rotation is a registered dietitian. The preceptor may also be a WIC supervisor or social service director in charge of public health

10
initiatives for the health center. However, it is expected that students will spend time with multiple health care professionals during this rotation. State Government/Non-Profit Nutrition Initiative Program Rotation (4 weeks) Students are assigned to a 4-week experience in which they will observe and participate in various activities involved in a federal and/or state funded nutrition-related programs. Examples of appropriate programs include food banks or kitchens, congregate meal programs, home-delivered meal programs, AIDS clinics, and other nutrition-based programs for the homeless, pregnant women and their families, and the elderly. Statewide or local programs focusing on childhood and adult obesity are another possibility or an elderly nutrition program supported by federal and state funds. Student are placed in a site where they will be involved in observing and participating in the implementation of key nutrition services and policies including provision of nourishing meals to all individuals throughout the lifespan, nutrition screening, assessment, education, and counseling to ensure that individuals achieve and maintain optimal nutritional status. Current Facilities Used in the Greater Boston Area: Executive Office of Elder Affairs, Boston Public Health Commission, the Greater Boston Food Bank, and the Massachusetts Department of Agricultural Resources. Preceptor: It is preferred that the main preceptor for this rotation is a registered dietitian. However, it is expected that students will spend time with other health care professionals during this rotation. Nutrition Counseling and Education Rotation (4 weeks) Students are assigned to a four week experience in which they will observe and participate in client and patient nutrition education and counseling. Students can spend their time with a private practice dietitian, a fitness or wellness facility with a nutrition component run by a registered dietitian, a corporate wellness program, a medical practice, dialysis center, eating disorder program, diabetes management program or any other site that focuses on preventative medicine, disease management, and overall health and wellness. Activities in this rotation include developing and presenting educational seminars, participating in community education programs, developing educational tools, and writing nutrition and exercise-related articles for the lay public. Current Facilities Used in the Greater Boston Area: Walden Behavioral Care, Jan Hangan Nutrition, The Weymouth Club, NourishRx/North Shore Medical Center Outpatient, Faulkner Hospital Outpatient, Community Servings, Susan Frates Nutrition, and Harvard Vanguard Medical Associates. Preceptor: It is preferred that the main preceptor for this rotation is a registered dietitian. However, it is expected that students will spend time with other health care professionals during this rotation.

11
SIMMONS COLLEGE DIETETIC INTERNSHIP PROGRAM
Policies and Procedures PROGRAM POLICIES AND PROCEDURES
1. Credentialing for Dietetic Practitioners
The Simmons College Dietetic Internship Program, accredited by Accreditation Council for Education in Nutrition and Dietetics (ACEND), is designed for students who hold a baccalaureate degree and meet the didactic program in dietetics (DPD) requirements. The program provides over 1,200 hours of fieldwork experience concentrating on the use of medical nutrition therapy in the community setting. Students completing the program are considered graduates of an accredited program and are eligible to complete the registration examination. Upon doing so, the faculty anticipates that graduates will be capable of practicing in a variety of settings performing nutrition-related professional activities.
The Accreditation Council for Education in Nutrition and Dietetics (ACEND) can be contacted by mail at 120 South Riverside Plaza, Suite 2000, Chicago Illinois, 60606-6995 or by phone at 800-877-1600 extension 5400 or by fax at 312-899-4817 (4772). The CADE web site can also be accessed on the internet at www.eatright.org/acend .
2. Program Completion Requirements
Completion of seven required rotations including related projects and assignments and make-up of any days missed or sick days.
Completion of all core competencies and program community emphasis competencies required by the Academy of Nutrition and Dietetics.
A ‘B’ or better in the required graduate level course Nutrition 452: Nutrition Program Planning, Implementation, and Evaluation.
Attendance at all scheduled Monday afternoon internship meetings at Simmons College. Completion of a formal evaluation by the student’s primary preceptor at each rotation. Completion of a formal evaluation by the student of each rotation. Completion of clinical worksheets provided in the Student Handbook for each rotation,
and submission to the Program Director at the end of the program. Participation in and evaluation of each of the joint dietetic internship class days. Collection and submission of projects completed during each rotation, and submission to
the Program Director at the end of the program. Participation in exit interviews at the completion of the 33 week internship experience. Complete a sample RD exam administered after participation in the RD exam review
sessions required during the final week of the internship program.
The dietetic internship director and coordinator, in conjunction with the preceptor, will review progression of all interns. If an intern does not meet the criteria for progressing in the program, then the intern may be asked to remain past the 33 weeks until performance meets the criteria. If an intern’s work including projects and homework does not meet criteria then the intern may be asked to revise his/her work for resubmission. No prior learning credit will be awarded towards completion of any rotation or class time

12
including Nutrition 452: Program Planning, Implementation, and Evaluation with the exception of exemption from Nutrition 452 for students who have taken the course at Simmons College within 10 years of beginning the internship. Note: A student may be asked to stay beyond the 33 weeks if, in the opinion of the program director, the student has not reached entry-level competence. Scheduled supervised practice experiences must be completed within a two-year period. This two year period begins when the students start their supervised practice experiences. If it is determined that a student needs to take a leave of absence, they must complete appropriate paperwork required by the School of Nursing and Health Sciences. Factors that will be considered in determining if a student’s experience must be lengthened include the following:
Recommendations from a preceptor(s) involved in the student’s experience. Recommendations from the program coordinator or program director. Student concerns about not being adequately prepared for an entry-level position in
the field of dietetics. Incomplete or unsatisfactory student evaluations indicating sub-optimal entry level
competence. Inability of a facility or internship site to provide an adequate experience due to
unforeseen circumstances. Personal circumstances that interfere and delay the completion of the internship
experience in the allotted 33-week period.
Upon completion of all dietetic internship requirements as listed above, information for all interns will be submitted to CDR for eligibility to sit for the RD examination. Verification statements of dietetic internship completion will be given out in person during the review days at the end of the program after the director and coordinator have verified that all completion requirements have been met. Each intern will be provided 5 signed verification statement, but may request more at any time if they have a specific need. Paper copies of verification statements are stored in a permanent file in the Simmons College Department of Nutrition, as well as, electronically as a PDF format in a locked computer file. The Department keeps former intern files on site in accessible locked storage indefinitely. If the intern has not completed all requirements by the review days, the director and coordinator will continue to work with the intern until all requirements are met and will issue verification statements once the intern has turned in all documentation. Interns who are not able to receive verification statements during the review days may pick up their verification statements in person from the Simmons College Department of Nutrition (300 The Fenway, Boston MA 02115), or request that the verification statements sent via The US Postal Service. Such requests must be in writing, email is acceptable. Former interns requiring reissued verification statements must do so either in person or in writing, giving specific instructions on how they would like the reissued statements to be delivered.
13
3. Program Estimated Costs: Application Fee:
A non-refundable fee of $50 must accompany the application when applying to the dietetic internship program.
Enrollment Fee: A non-refundable $500 enrollment fee is required of students accepted into the
program to confirm their willingness to participate in the program for the selected time period. Deposits will be applied to the first semester bill.
Tuition Fee: The students are required to pay a tuition fee equivalent to 12 semester hours of
field work (9 credits) and graduate course work (3 credits) at Simmons College. For the 2012-2013 school year, the cost per semester hour for graduate programs offered in the School of Health Sciences is $1,082 and therefore, a cost of $12,984 is required for enrollment in the 12 program credits required by the dietetic internship program. More information can be found at: http://www.simmons.edu/snhs/finaid/index.php.
Student Activity Fee: An activity fee of $100 per semester must be paid by all students participating in
the dietetic internship program. This fee supports student activities and other program-related events.
Criminal Offense Record Information (CORI): The Simmons College Nutrition Program requires that all students enrolled in the
Simmons College Dietetic Internship Program have a CORI (Criminal Offender Record Information) check performed prior to beginning their clinical experiences. The CORI check allows the Simmons College Nutrition Department to access conviction and pending criminal case data for the purpose of screening students participating in clinical programs where there is the potential for unmonitored access to vulnerable populations, including, but not limited to, children, the elderly, patients or disabled persons. The students must pay $55.50 for this check. Please see the end of this section for official policy and appeals information.
Drug Testing:
Drug testing is not mandatory for the Simmons dietetic internship, but may be required by a specific site. If this is the case, that site will be responsible for administering the test.
Health Insurance:
Students enrolled in the School for Health Studies for six or more semester hours are required by Massachusetts state law to have health insurance coverage. Students must either purchase health insurance offered by Simmons or waive participation in the Simmons plan by demonstrating that they will be covered for the year by privately purchased insurance that is comparable to a Qualifying Student Health Insurance Plan (QSHIP). Student health insurance for the 2012-2013 school year is $3449. Questions about medical insurance can be addressed to the Office of Student Accounts at (617) 521-2009.
14
Health/Medical Services:
Graduate students living on the residence campus are required to pay the Health Center Fee (2012-2013: $375 for each semester for a total of $750 per year). Other students not covered by the Health Center Fee may elect as well to use the Health Center by paying the Health Fee or on a fee-for-service basis. For additional information, students can call the Health Center at (617) 521-1002.
Medical Clearance: All students accepted into the dietetic internship program are required to complete
a recent physical exam and must have all of their vaccinations up-to-date prior to the start of their first rotation. Accepted dietetic interns will be provided with a medical clearance form soon after they are accepted to the internship program which must be completed prior to the start of their rotations.
Cost of Living Considerations: Simmons College Graduate Housing: Room/Board (19 meal plan): 2012-2013 = $
7,360 per semester; $14,720 per year. Apartments for Rent Around Simmons College:
1 Bedroom Apartment: ~$1000-1600 2 Bedroom Apartment: ~$1,700-1,900 3 Bedroom Apartment: ~$2,000-2,300 4 Bedroom Apartment: ~$2,400-2,600
Local Public Transportation: Students may purchase the MBTA Semester Transit Pass. This Fall Semester package includes 4 monthly passes (Sept-Dec). This Spring Semester Pass includes 4 monthly passes (Feb-May). Order forms for the discount Semester Pass are available at the Student Life Office or online at: http://my.simmons.edu/services/business/parking/mbta-passes.shtml . For additional information on public transportation see the Massachusetts Bay Transit Authority (mbta) web site at www.mbta.com .
Monthly Garage Parking: $150-$250 Parking Meters: ~$0.25 per 15 minutes Gasoline: $3.00-$4.00/gallon, self-serve, regular unleaded Laundromat: Wash: ~$1.00; Dry: ~$0.25 per 10 min Sales Tax: No tax on groceries and clothing, 6.25% on all nonessentials.
4. Financial Aid:
Financial aid is available for all students based on need and merit. Need-based awards consist primarily of low-interest loans, grant money, and Federal Work-Study. There are also outside loan programs to help supplement need-based assistance. State and National scholarship information is also available.
The TERI Continuing Education Loan is available for those students enrolled only in the Dietetic Internship Program or the MEFA Loan for those concurrently enrolled in the Master’s Nutrition Program.
Students requesting aid must file a Free Application for Federal Student Aid (FAFSA), and a Simmons Application for Graduate Financial Aid. These forms can be obtained by
15
contacting the financial aid office at (617) 521-2036 or by accessing the Simmons College Web site at http://my.simmons.edu/services/sfs/apply/graduate.shtml
Applicants for financial aid are advised to submit all application materials by March 1 for the upcoming summer and fall semesters. Since students are not matched with a dietetic internship program until mid-April, it is advised that they submit their financial aid forms as soon as they can after committing to the dietetic internship program.
5. Withdrawal from the Program:
If a student withdraws from the Dietetic Internship Program after acceptance, they will lose their $500 acceptance fee. All College expenses incurred by the student before withdrawal from the College must be paid in full prior to the release of an official transcript. Graduate students wishing to withdrawal from the Dietetic Internship Program should complete a “Notice of Withdrawal from the College” form which is available from the Program Director (Nancie Herbold, Dietetic Internship Program Director) or the Office of the Dean of the College. Students with loans and grants must write their intentions to withdrawal and submit them to the Office of Financial Aid. Students are urged to review the College’s refund policy before making a final decision. Refund of Tuition and Fees:
The College’s general policy regarding fall and spring semester tuition refunds to students is as follows:
1. The College provides all instruction (to be paid for prior to the beginning of each semester) on an academic-semester basis. Tuition refunds are granted based upon the refund dates listed on the Fact Sheet in the Graduate Schedule of Classes for each semester which can be reviewed at: http://www.simmons.edu/academics/calendar/ . The date that appears on the official Add/Drop Form filed with the Registrar is used to determine refund amounts. Refunds are granted on a prorated basis only after add/drop forms are filed.
2. Students receiving federal financial assistance who withdraw from all their course work are subject to different rules. The philosophy of financial assistance programs is that the student is primarily responsible for paying college costs. Assistance is meant to bridge the gap between what the student can pay and the total cost of an education program. With this in mind, any credit to the student’s account resulting from withdrawal from course work will be refunded to the financial aid programs first, then to the student if funds remain after all aid is repaid. If funds remain after all aid is repaid and the student has no outstanding financial obligation, any excess monies will be refunded to the student.
3. The Application Fee, Tuition Deposit, Activity and Health Fees, and other fees are non-refundable. Questions regarding refunds should be directed to the Office of Student Financial Services, Room W-207, Main College Building, 300 The Fenway, Boston. Telephone: (617) 521-2001.
6. Liability for Safety in Transit to or from Assigned Areas and Professional Liability The student is expected to provide her/his own transportation to and from clinical practice sites.

16
Liability is assigned to the individual student and is not the responsibility of the College. The student is covered under Simmons College's policy for Professional Liability. 7. Vacation, Holiday and Sick Time The program consists of seven supervised practice rotations that take place annually between the months of September and April. Interns follow a schedule laid out by the internship director and coordinator and do not follow the official Simmons College Academic Calendar. The start and end dates, as well as, the winter break schedule is provided to all interns in the “Welcome Letter” sent out annually in May. The final rotation schedule is provided to each intern on the first day of orientation. There is a one-week vacation between Christmas and the New Year. In 2012-2013, vacation will begin at the end of the work day on Friday, December 21, 2012. You will restart your rotations on Wednesday, January 2, 2013. This week is not included in the 33-week period allotted to the program.
For all other holidays, students will observe the holiday schedule for their assigned rotations. Students who are ill must notify their preceptor and the dietetic internship program director (Nancie Herbold) or dietetic internship coordinator (Lisa Brown). All sick time must be made up by the student. Additionally, please note that some preceptors will have you make-up Monday class days or early release days. 8. Injury or Illness Policy The Affiliation Agreement with the student internship sites states that the affiliations shall have no responsibility for providing health services for the student interns. The only exception is that the affiliations shall provide emergency medical care to the interns in the event that the need arises, but shall not be obligated to furnish medical and surgical services in the absence of an emergency. It is agreed that the charges for any treatment provided by the affiliations will be billed to the appropriate health insurance company covering the involved intern.
In instances when a student’s physical health may be considered life threatening, the college will require that a student be evaluated by a physician or another appropriate medical professional. If the student refuses to be evaluated, the student will not be allowed to stay in residence or attend classes and their clinical sites. The student’s parent/guardian/emergency contact person will be notified that the student is in a potentially dangerous situation.
In the case of non-life threatening illness or injury, the student will have to make a rational decision as to whether they should attend their clinical site. Generally, site directors will ask that students remain at home until their major symptoms have resolved. The site director and the dietetic internship program director must be notified of all absences and the reason for the absence. The absences will be made up at a later date as determined by the site director and the student.
9. Disciplinary/Termination Procedures

17
The program faculty will review the records of any students progressing unsatisfactorily and may take any of the following actions:
Exclusion from the Program: ‘Exclusion’ shall mean the student is required to withdraw from the program.
Probation: ‘Probation’ shall mean that the student may remain in the Program, under warning for one month, with review and further action by the Program Director at the end of that month. The student’s file shall bear the notation of probation only while the student is in probation.
Letter of Warning: A ‘Letter of Warning’ may be sent to a student whose progress is marginal.
No Action: The term ‘No Action’ indicates that a student remains in good standing.
10. Time on Duty
A forty-hour week is planned for each affiliation. The selected time on duty varies depending upon the rotation. Hence, occasional weekends or non-traditional hours (for example, 11 a.m. to 7 p.m. or 6 a.m. to 2 p.m.) may be expected of you during your rotations.
11. Dress Code
Professional dress is expected. For women a reasonable length skirt (not mini-skirt) or full-length trousers of a non-jeans material combined with a top (such as a dress shirt, polo, or sweater set) is considered acceptable. An informal dress with appropriate skirt length is also acceptable. For men, a shirt and tie is required. It is advisable to ask each of your preceptors if there are any attire requirements prior to the initiation of your rotation. Please make sure your clothing is not tight fitting and that cleavage, midriffs, and underwear are not exposed. Additionally, it is recommended that you possess at least one full-length white laboratory coat for those rotations that require laboratory coats.
12. Requirements for Initiation of Rotations Prior to START of internship rotations, ALL interns must have on file with the Simmons College Department of Nutrition:
An official DPD Verification Statement, signed by the DPD director of your DPD institution
Final transcript with specification of degree awarded Health Center Clearance from the Simmons College Health Center CORI clearance HIPAA certificate Bloodborne pathogen OSHA certificate

18
Simmons College Nutrition Department CORI Policy
Where Criminal Offender Record Information (CORI) checks are part of a general background check for employment, volunteer work or licensing purposes, the following practices and procedures will generally be followed. I. CORI checks will only be conducted as authorized by CHSB. All applicants will be notified that a CORI check will be conducted. If requested, the applicant will be provided with a copy of the CORI policy. II. An informed review of a criminal record requires adequate training. Accordingly, all personnel authorized to review CORI in the decision-making process will be thoroughly familiar with the educational materials made available by CHSB. III. Unless otherwise provided by law, a criminal record will not automatically disqualify an applicant. Rather, determinations of suitability based on CORI checks will be made consistent with this policy and any applicable law or regulations. IV. If a criminal record is received from CHSB, the authorized individual will closely compare the record provided by CHSB with the information on the CORI request form and any other identifying information provided by the applicant, to ensure the record relates to the applicant. V. If the Simmons College Nutrition Department is inclined to make an adverse decision based on the results of the CORI check, the applicant will be notified immediately. The applicant shall be provided with a copy of the criminal record and the organization's CORI policy, advised of the part(s) of the record that make the individual unsuitable for the position or license, and given an opportunity to dispute the accuracy and relevance of the CORI record. VI. Applicants challenging the accuracy of the policy shall be provided a copy of CHSB’s Information Concerning the Process in Correcting a Criminal Record. If the CORI record provided does not exactly match the identification information provided by the applicant, Simmons College Nutrition Department will make a determination based on a comparison of the CORI record and documents provided by the applicant. The Simmons College Nutrition Department may contact CHSB and request a detailed search consistent with CHSB policy. VII. If the Simmons College Nutrition Department reasonably believes the record belongs to the applicant and is accurate, based on the information as provided in section IV on this policy, then the determination of suitability for the position or license will be made. Unless otherwise provided by law, factors considered in determining suitability may include, but not be limited to the following: (a) Relevance of the crime to the position sought; (b) The nature of the work to be performed; (c) Time since the conviction; (d) Age of the candidate at the time of the offense; (e) Seriousness and specific circumstances of the offense; (f) The number of offenses; (g) Whether the applicant has pending charges;
Department of Nutrition School of Health Sciences Simmons College 300 The Fenway Telephone – 617-521-2718 Boston, MA 02115 Facsimile – 617-521-3002
19
(h) Any relevant evidence of rehabilitation or lack thereof; (i) Any other relevant information, including information submitted by the candidate or requested by the hiring authority VIII. Simmons College Nutrition Department will notify the applicant of the decision and the basis of the decision in a timely manner.
CORI Appeals Process for Employees (Students): Before making a finding of unsuitability to review CORI based on an employee’s criminal history, the Administrator shall provide the individual with the opportunity to dispute the accuracy and relevance of the CORI. The Administrator will notify said employee of the potential adverse decision and provide the individual with the following: (a) A copy of the CORI; (b) A copy of this policy; (c) The CHSB's Information Concerning the Process for Correcting a Criminal Record and the CHSB’s Information Concerning the Process on How to Establish Yourself as a Victim of Identity Theft for CORI Purposes; (d) The Administrator will identify the parts of the criminal record that appear to make him/her ineligible; and (e) An opportunity to dispute the accuracy and relevance of the CORI. An employee seeking to exercise the opportunity to dispute the accuracy of the CORI may submit a statement to the Administrator specifying the information he or she believes is inaccurate. The statement must include any documentation the individual has to support the claim. The administrator may contact the CHSB for assistance with disputes as to accuracy. An employee seeking to exercise the opportunity to dispute the relevance of the CORI must submit a statement to the Administrator describing why he or she believes the CORI does not affect his or her ability to effectively administer the CORI process in compliance with all applicable laws and regulations. The administrator may request additional information from the individual and/or assistance from the CHSB in this process. Upon receipt of all information, the administrator will review the request and inform the individual of the final decision in writing. The administrator shall document all steps taken to comply with this process and must be able to provide this information to the CHSB upon request. Documentation must be maintained for a period of two years.
From: Criminal History Systems Board Policy for Administrator's conducting CORI checks of Agency Submitters
20
SIMMONS COLLEGE DIETETIC INTERNSHIP PROGRAM
Code of Ethics for the Profession of Dietetics CODE OF ETHICS FOR THE PROFESSION OF DIETETICS The American Dietetic Association and its Commission on Dietetic Registration have adopted a voluntary, enforceable code of ethics. This code, entitled the Code of Ethics for the Profession of Dietetics, challenges all members, registered dietitians, and dietetic technicians, registered, to uphold ethical principles. The enforcement process for the Code of Ethics establishes a fair system to deal with complaints about members and credentialed practitioners from peers or the public. The House of Delegates adopted the first code of ethics in October 1982; enforcement began in 1985. The code applied to members of The American Dietetic Association only. A second code was adopted by the House of Delegates in October 1987 and applied to all members and Commission on Dietetic Registration credentialed practitioners. A third revision of the code was adopted by the House of Delegates on October 18, 1998, and enforced as of June 1, 1999, for all members and Commission on Dietetic Registration credentialed practitioners. The current code was adopted in 2009 and was in effect as of January 1, 2010. A link to the original article and more information can be found at: http://www.eatright.org/HealthProfessionals/content.aspx?id=6868. The Ethics Committee is responsible for reviewing, promoting, and enforcing the Code. The Committee also educates members, credentialed practitioners, students, and the public about the ethical principles contained in the Code. Support of the Code of Ethics by members and credentialed practitioners is vital to guiding the profession’s actions and to strengthening its credibility. The Ethics Committee is responsible for reviewing, promoting, and enforcing the Code. The Committee also educates members, credentialed practitioners, students, and the public about the ethical principles contained in the Code. Support of the Code of Ethics by members and credentialed practitioners is vital to guiding the profession’s actions and to strengthening its credibility. PREAMBLE The American Dietetic Association and its credentialing agency, the Commission of Dietetic Registration, believe it is in the best interest of the profession and the public it serves to have a Code of Ethics in place that provides guidance to dietetics practitioners in their professional practice and conduct. Dietetics practitioners have voluntarily adopted a Code of Ethics to reflect the values and ethical principles guiding the dietetics profession and to outline commitments and obligations of the dietetics practitioner to client, society, self and the profession. The Ethics Code applies in its entirety to members of The American Dietetic Association who are Registered Dietitians (RDs) or Dietetic Technicians, Registered (DTRs). Except for sections solely dealing with the credential, the Code applies to all members of The American Dietetic Association who are not RDs or DTRs. Except for aspects solely dealing with membership0, the Code applies to all RDs and DTRs who are not members of The American Dietetic Association. The entire aforementioned are referred to in the Code a “dietetics practitioners.” By accepting membership in The American Dietetic Association and/or accepting and maintaining Commission of Dietetic Registration credentials, members of The American Dietetic Association and Commission on Dietetic Registration credentialed dietetics practitioners agree to abide by the Code.
1. The student conducts himself/herself with honesty, integrity, and fairness. 2. The student practices dietetics based on scientific principles and current information. 3. The student presents substantiated information and interprets controversial information without personal
bias, recognizing that legitimate differences of opinion exist. 4. The student assumes responsibility and accountability for personal competence in practice, continually
striving to increase professional knowledge and skills and to apply them in practice.

21
5. The student recognizes and exercises professional judgment within the limits of his/her qualifications and collaborates with others, seeks counsel, or makes referrals as appropriate.
6. The student provides sufficient information to enable clients and others to make their own informed decisions.
7. The student protects confidential information and makes full disclosure about any limitations on his/her ability to guarantee full confidentiality.
8. The student provides professional services with objectivity and with respect for the unique needs and values of individuals.
9. The student provides professional services in a manner that is sensitive to cultural differences and does not discriminate against others on the basis of race, ethnicity, creed, religion, disability, sex, age, sexual orientation or national origin.
10. The student does not engage in sexual harassment in connection with professional practice. 11. The student permits the use of his/her name for the purpose of certifying that dietetics services have been
rendered only if he/she has provided or supervised the provision of those services. 12. The student accurately presents professional qualifications and credentials. 13. The student withdraws from the program under the following circumstances:
a. The student has engaged in any substance abuse that could affect his/her practice; b. The student has been adjudged by a court to be mentally incompetent; c. The student has an emotional or mental disability that affects his/her practice in a manner that
could harm the client or others. 14. The student complies with all applicable laws and regulations concerning the profession and is subject to
disciplinary action under the following circumstances: a. The student has been convicted of a crime under the laws of the United States that is a felony or a
misdemeanor, an essential element of which is dishonesty, and which is related to the practice of the profession.
b. The student has been disciplined by a state, and at least one of the grounds for the discipline is the same or substantially equivalent to these principles.
c. The student has committed an act of misfeasance or malfeasance which is directly related to the practice of the profession as determined by a court of competent jurisdiction, a licensing board, or an agency of a governmental body.
CONSIDERATION OF ETHICS ISSUES A 3-person committee, comprised of members of The American Dietetic Association and/or Commission on Dietetic Registration credentialed practitioners, will be appointed to handle all ethics matters. One person will be appointed each by the president of The American Dietetic Association, the Chairperson of the Commission on Dietetic Registration, and the Speaker of the House of Delegates. Terms of office will be for 3 years. Initial terms will be staggered to allow for continuity. The American Dietetic Association President’s initial appointment will serve for 3 years; the Chairperson of the Commission on Dietetic Registration’s initial appointment will serve for 2 years; and the Speaker of the House of Delegates’ initial appointment will serve for 1 year. Thereafter, each appointee will serve for 3 years. The chairmanship will rotate among the 3 Committee members. The American Dietetic Association President’s appointment will serve first as chair followed in sequence by the Commission on Dietetic Registration Chairperson’s and the HOD Speaker’s appointments. The Committee will have authority to consult with subject experts as necessary to conduct its business. The Committee may perform such other educational activities as might be necessary to assist members and credentialed individuals to understand the Code of Ethics. Ethics Opinions The Committee may issue opinions on ethics issues under the Code on its own initiative or in response to a member’s or credentialed practitioner’s request. These opinions will be available to members and credentialed practitioners to guide their conduct and to the public. Situations may be factual or hypothetical, but no names will be disclosed. Ethics Cases

22
Preamble: The enforcement procedures are intended to permit a fair resolution of disputes on ethical practices in a manner that protects the rights of individuals while promoting understanding and ethical practice. The Ethics Committee has the authority and flexibility to determine the best way to resolve a dispute, including educational means where appropriate.
1. Complaint A complaint that a member or credentialed practitioner has allegedly violated the Code of Ethics for the Profession of Dietetics must be submitted in writing on the appropriate form to the Ethics Committee. The complaint must be made within 1 year of the date that the complainant (person making complaint) first became aware of the alleged violation or within 1 year from the issuance of a final decision in an administrative, licensure board, or judicial action involving the facts asserted in the complaint. The complainant need not be a member of The American Dietetic Association or a practitioner credentialed by the Commission of Dietetic Registration. The complaint must contain details on the activities complained of; the basis for complainant’s knowledge of these activities; names, addresses and telephone numbers of all persons involved or who might have knowledge of the activities; and whether the complaint has been submitted to a court, an administrative body, or a state licensure board. The complaint must also cite the section(s) of the Code of Ethics for the Profession of Dietetics allegedly violated. The complaint must be signed and sworn to by the complainant(s).
2. Preliminary Review of Complaint The chair of the Ethics Committee, legal counsel for The American Dietetic Association, and appropriate staff will review the complaint to determine if the complainant has submitted all the required information and whether an ethics question is involved. If a complaint is made regarding an alleged violation of the Code of Ethics for the Profession of Dietetics and a similar complaint is already under consideration regarding the same individual by a state licensure board of examiners, an administrative body, or a court of law, the Ethics Committee will not process the complaint until final decision had been issued.
3. Response If the persons making the preliminary review determine that the process should proceed, the chair of the Ethics Committee will notify the respondent (person against whom the complaint is made) that a complaint has been made. The notice will be sent from the staff via certified mail, return-receipt requested. The respondent will be sent a copy of the complaint, the Code of Ethics for the Profession of Dietetics, the Review Process and Response to Complaint form. The respondent will have thirty (30) days from receipt of the notification in which to submit a response. The response must be signed and sworn to by the respondent(s). If the Ethics Committee does not receive a response, the chair of the Ethics Committee or his/her designee will contact the respondent by telephone. If contact with the respondent is still not made, a written notice will be sent. Failure to reach the respondent will not prevent the Committee from proceeding with the investigation.
4. Ethics Committee Review If the chair of the Ethics Committee deems it appropriate, after consultation with legal counsel and appropriate staff, he/she will submit the complaint and the response to the Ethics Committee for review.

23
The Committee has broad discretion to determine how to proceed, including, but not limited to, dismissing the complaint, requesting further information from the parties, resolving the case through educational activities, holding a hearing as specified hereafter, or in any other way deemed advisable. The Committee may use experts to assist it in reviewing the complaint and response and determining further action. At the appropriate time, the Ethics Committee will notify the complainant and the respondent of its decision, which may include the Committee’s preliminary opinion with a request that the respondent take certain actions, including, but not limited to, successful completion of continuing professional education in designated areas, or supervised practice on terms to be set forth by the Committee. The Ethics Committee may also recommend appropriate remedial action to the parties, which if undertaken, would resolve the matter. The Ethics Committee may recommend, in its discretion, that a hearing be held subject to the other provisions of these procedures.
5. Licensure Board Action or Final Judicial or Administrative Action When the Ethics Committee is informed by a state licensure body that a person subject to the Code of Ethics for the Profession of Dietetics has had his/her license suspended or revoked for reasons covered by the Code, the Committee may take appropriate disciplinary action without a formal hearing. When a person has been finally adjudged or has admitted to committing a misdemeanor or felony as specified in Principle 18 of the Code, the Committee may take appropriate disciplinary action without a formal hearing.
6. Hearings a. General b. Hearings shall be held as determined by the Ethics Committee under the following guidelines. The chairman of the Ethics Committee will establish hearing dates. All hearings will be held in Chicago.
The Ethics Committee will notify the respondent and the complainant by certified mail, return-receipt requested, of the date, time and place of the hearing. The respondent may request a copy of the file on the case and will be allowed at least one postponement, provided the request for postponement is received by The American Dietetic Association at least fourteen (14) days before the hearing date.
c. Conduct of Hearings The chair of the Ethics Committee will conduct a hearing with appropriate staff and legal counsel present. Individuals who have no conflict of interest will be appointed. In the event that any Ethics Committee member cannot serve on the hearing panel for any reason, a replacement will be appointed by the representative of the original body that made the appointment, either the American Dietetic Association President, the Commission of Dietetic Registration Chairperson, or the Speaker of the House of Delegates as appropriate. The parties shall have the right to appear; to present witnesses and evidence; to cross-examine the opposing party and adverse witnesses; and to have legal counsel present. Legal counsel for the parties may advise their clients, but may only participate in the hearings with the permission of the chair. The hearing is the sole opportunity for the participants to present their positions. Three members of the Ethics Committee shall constitute a quorum. Affirmative vote of two-thirds (2/3) of the members voting will be required to reach a decision.

24
A transcript will be prepared and will be available to the parties at cost.
d. Costs The American Dietetic Association will bear the costs for the Ethics Committee, legal counsel, staff, and any other parties called by The American Dietetic Association. The American Dietetic Association will bear the travel and one night’s hotel expenses for the complainant and respondent and one person that each chooses to bring, provided that such person is necessary to the conduct of the hearing as determined by the Chair of the Ethics Committee. The Ethics Committee shall issue regulations to govern the payment of these expenses which shall be incorporated and made part of these procedures. The respondent and the complainant will be responsible for all costs and fees incurred in their preparation for and attendance at the hearing, except expenses for travel and hotel as stated above.
e. Decision The Ethics Committee will render a written decision specifying the reasons therefore and citing the provision(s) of the Code of Ethics for the Profession of Dietetics that may have been violated. The Committee will decide that:
1. The respondent be acquitted; 2. Educational opportunities be pursued; 3. The respondent be censured, placed on probation, suspended, or expelled from The
American Dietetic Association and/or 4. The credential of the respondent be suspended or revoked by the Commission on
Dietetic Registration of The American Dietetic Association.
The decision of the Ethics Committee will be sent to the respondent and the complainant as soon as practicable after the hearing.
7. Definitions of Disciplinary Action Censure: A written reprimand expressing disapproval of conduct. It carries no loss of membership or registration status, but may result in removal from office at the national, state, and district levels and from committee membership. Time frame – not applicable. Probation: A directive to allow for correction of behavior specified in Principle 17 of the Code of Ethics for the Profession of Dietetics. It may include mandatory participation in remedial programs (e.g., education, professional counseling, and peer assistance). Failure to successfully complete these programs may result in other disciplinary action being taken. It carries no loss of membership or registration status, but may result in removal from office at the national, state and district levels and from committee membership. Time frame – specified time to be decided on a case-by-case basis. Suspension: Temporary loss of membership and all membership benefits and privileges for a specified time with the exception of retention of coverage under health and disability insurance. The American Dietetic Association group malpractice insurance will not be available and will not be renewed during the suspension period. Time frame – specified time to be decided on a case-by-case basis. Suspension of Registration: Temporary loss of credential and all benefits and privileges for a specified period of time. It may include mandatory participation in remedial programs (e.g., education, professional counseling, and peer assistance). At the end of the specified suspension period, membership and registration benefits and privileges are automatically restored. Time frame – specified time to be decided on a case-by-case basis. Expulsion: Removal from membership and a loss of all benefits and privileges. Time frame – may apply for reinstatement after a 5-year period has elapsed or sooner if the basis for the expulsion has been
25
removed, with payment of a reinstatement fee. Must meet membership requirements in effect at the time of application for reinstatement. Revocation of Credential: Loss of registration status and removal from registry; loss of all benefits and privileges. Upon revocation, the former credentialed practitioner shall return the registration identification card to the Commission on Dietetic Registration. Time frame –Specified time for reapplication to be decided on a case-by-case basis, but, at a minimum, current re-certification requirements would need to be met. A credential will not be issued until the Commission on Dietetic Registration determines that the reasons for revocation have been removed.
8. Appeals a. General
Only the respondent may appeal an adverse decision to The American Dietetic Association. During the appeals process, the membership and registration status of the respondent remains unchanged. The American Dietetic Association President, the Chairperson of the Commission on Dietetic Registration, and the Speaker of the House of Delegates shall each appoint one person to hear the appeal. These individuals shall constitute the Appeals Committee for that particular case. Individuals who have no conflict of interest will be appointed.
b. Recourse to the Appeals Committee To request a hearing before the Appeals committee, the respondent/appellant shall nifty the appropriate staff at The American Dietetic Association headquarters, by certified mail, return-receipt requested, that the respondent wishes to appeal the decision. This notification must by receive within thirty (30) days after receipt of the letter advising the respondent/appellant of the Ethics Committee’s decision.
c. Contents The appeal must comply with the following:
1. The appeal must be in writing and contain, at a minimum, the following information: 1. The decision being appealed 2. The date of the decision 3. Why the individual feels the decision is wrong or was improperly rendered (See
8, E, “Scope of Review, “ below) 4. The redress sought by the individual 5. The appeal will be signed and sworn to
If the appeal does not contain the information listed above, it will be returned to the individual who will be given ten (10) calendar days to resubmit. Failure to furnish the required information within ten (10) calendar days will result in the appeal being waived.
d. Procedures Upon receipt of this notification, appropriate staff shall promptly notify the chair of the Appeals Committee that the respondent/appellant is appealing a decision made by the Ethics Committee. The Appeals Committee chair shall acknowledge the appeal and request a copy of the relevant written information on the case from appropriate staff.
1. Location and participants 1. All appeals hearings will be held in Chicago.
26
2. The complainant/appellee, the respondent/appellant, and the chair of the Ethics Committee will have the opportunity to participate in the appeals hearing.
3. The parties may have legal counsel present, who may advise their clients, but may only participate in the hearings with the permission of the chair.
4. Attendance at the hearing will be limited to persons determined by the chair to have a direct connection with the appeal and appropriate staff and legal counsel.
2. Conduct of the hearing
The three parties involved in the appeal will be given the opportunity to state why the decision and/or disciplinary action of the Ethics Committee should be upheld, modified, or reversed.
e. Scope of Review The Appeals Committee will determine whether the Ethics Committee committed procedural error that affected its decision, whether the Ethics Committee’s decision was contrary to the weight of the evidence presented to it, or whether there is new and substantial evidence that would likely have affected the Ethics Committee’s decision that was unavailable to the parties at the time of the Ethics Committee’s hearing for reasons beyond their control. In reviewing the decision of the Ethics Committee, the Appeals Committee shall consider only the transcript of the hearing and the evidence presented to the Ethics Committee.
f. Record of Hearing A transcript will be prepared and will be maintained in the case file.
g. Decision of Appeals Committee 1. The Appeals Committee shall prepare a written decision stating the reasons therefore.
The decision shall be to affirm, modify, or reject the decision and/or disciplinary action of the Ethics Committee or to remand the case to the Ethics Committee with instructions for further proceedings.
2. Decisions of the Appeals Committee will be final.
h. Costs The American Dietetic Association will bear the costs for the Appeals Committee, staff and legal counsel, and any parties called by The American Dietetic Association. The American Dietetic Association will bear the travel and one night’s hotel expenses for the respondent/appellant, the complainant/appellee, and the chair of the Ethics Committee. The Ethics Committee shall issue regulations to govern the payment of these expenses, which shall be incorporated and made part of this procedure. The respondent/appellant and the complainant/appellee will be responsible for all costs and fees incurred in their preparation for and attendance at the heading, except expenses for travel and hotel as stated above.
9. Notification of Adverse Action If the respondent is disciplined by the Ethics Committee and does not appeal the decision, the chair of the Ethics Committee will notify the appropriate American Dietetic Association organizational units, Commission on Dietetic Registration, the affiliate dietetic association, appropriate licensure boards, and governmental and private bodies within thirty (30) days after notification of the final decision. In the event the respondent appeals a decision to discipline him/her and the Ethics Committee decision is affirmed or modified, similar notification will be made by the chair of the Ethics Committee. In response to an inquiry about registration status, the Office on Dietetic Credentialing will state only whether a person is currently registered.

27
10. Record Keeping
a. Records will be kept for a period of time after the disposition of the case in accordance with The American Dietetic Association’s record retention policy.
b. Information will be provided only upon written request and affirmative response from The American Dietetic Association’s legal counsel.
11. Confidentiality Procedures
The following procedures have been developed to protect the confidentiality of both the complainant and the respondent in the investigation of a complaint of an alleged violation of the Code of Ethics for the Profession of Dietetics:
a. The need for confidentiality will be stressed in initial communications with all parties. b. Committee members will refrain from discussing the complaint and hearing outside of official
committee business pertaining to the complaint and hearing. c. If the hearing on a complaint carries over to the next Committee, the complaint will be heard by
the original Committee to hear the complaint. d. Communication with American Dietetic Association witnesses will be the responsibility of the
Committee chair or staff liaison. e. Witnesses who testify on behalf of The American Dietetic Association will be informed of the
confidentiality requirements and agree to abide by them. f. The Committee chair will stress the importance of confidentiality at the time of the hearing. g. To ensure confidentiality, the only record of the hearing will be the official transcript and
accompanying materials that will be kept at The American Dietetic Association offices. All other materials that were mailed or distributed to committee members should be returned to The American Dietetic Association staff, along with any notes taken by Committee members.
h. The transcript will be available if there is an appeal of the Ethics Committee’s decision and only to the parties, Ethics Committee members, Appeals Committee members, The American Dietetic Association legal counsel, and staff directly involved with the appeal.
Reprinted with permission: The Journal of the American Dietetic Association, Aug 2009.
28
SIMMONS COLLEGE DIETETIC INTERNSHIP PROGRAM
Policy of Non-Discrimination, Grievance Procedures, and Student Privacy
Notice of Non-Discrimination and Grievance Procedures
Chartered in 1899 and opened in 1902, Simmons College is first and foremost an academic community whose primary goals are to prepare women and men to be well informed, open-minded, and sensitive to values. To attain these goals we seek to create an atmosphere within which students may learn to become actively engaged members of society and to develop the resources to lead rich personal lives. We hope to achieve these goals through an active and continuing exchange of ideas among students and faculty and the general College community.
To ensure that these goals are attained, Simmons has committed itself to the following principles:
Simmons College supports the principle and spirit of equal employment opportunity for all persons, based on each individual's qualifications and fitness. In accordance with applicable law, the College administers its employment and personnel policies without regard to race, color, religion, disability, national origin, ancestry, age, sex, sexual orientation, or veteran's status.
Simmons College administers its educational programs and activities in accordance with the requirements and implementing regulations of Title VI of the Civil Rights Act of 1964, Title IX of the Educational Amendments of 1972, the Age Discrimination Act of 1975, Section 504 of the Rehabilitation Act of 1973, and Title III of the Americans with Disabilities Act of 1990.
Simmons College strives to ensure that all decisions concerning hiring and promotion of faculty and staff, or the educational process of students, are based on considerations appropriate to an academic institution and not on factors such as race, color, sex, sexual orientation, religion, age, national origin, ancestry, disability, or veteran's status.
Furthermore, Simmons College is committed to creating an atmosphere within which the diversity of its members' individual roles meets with understanding, respect, and encouragement, and where discrimination and harassment by any member of the faculty, staff, or student body against any other will be condemned and redressed. The College does not tolerate sexual harassment of employees or students.
If you have a complaint about unlawful discrimination or harassment and if you are a student, you should bring your concerns to the dean of your school or to the dean for student life. If you have a complaint about unlawful discrimination or harassment and you are an employee, you should bring your concern to the attention of the director of human resources. Complaints or inquiries concerning the College's policies and compliance with applicable laws, statutes, and regulations may also be directed to the College president's office, or to the College's General Counsel, in (Office to be announced) or 617-521-2276. Your complaint should contain your name and address so that we can contact you and give a brief description of the actions you

29
believe to be unlawful. You should bring your complaint in a timely manner, usually no later than 60 days after you become aware of the alleged violation. The president or appropriate College officer (or his or her designee) will conduct an investigation and issue a written decision on the complaint, ordinarily within 45 days.
If you have a complaint regarding the operation of the Simmons College Dietetic Internship program in relation to the program’s compliance with the accreditation/approval standards you should contact the Accreditation Council for Education in Nutrition and Dietetics (ACEND). The Commission is interested in the sustained quality and continued improvement of dietetics education and programs but does not intervene on behalf of individuals or act as a court of appeal for individuals in matters of admission, appointment, promotion, or dismissal of faculty, staff or students.
A copy of the accreditation/approval standards and/or the Council’s policy and procedure for submission of complaints may be obtained by contacting the Education staff at The Academy of Nutrition and Dietetics, 120 South Riverside Plaza, Suite 2000, Chicago, IL 60606-6995 or calling 800/877-1600 ext. 4872.

30
College Policies & Procedures
Student Emergencies
In instances when a student's physical health may be considered life threatening, the College will require that a student be evaluated by a physician or other appropriate medical personnel.
If the student refuses to be evaluated, the student will not be allowed to stay in residence or attend classes. The student's parent/guardian/emergency contact person will be notified that the student is in a potentially dangerous situation.
College Response to Endangering Behavior/ Involuntary Leaves of Absence
Simmons College is committed to the safety and well-being of its community members and to the integrity of the learning environment. Our goals therefore are to maintain the health and safety of each individual in our community and to enable all enrolled students to participate fully in the life of the College. We recognize that from time to time, students may take a voluntary leave of absence from their studies as a result of medical or mental health issues or other personal matters that compromise their ability to continue in an academic program. However, in instances in which a student whose mental/emotional or medical health condition poses a threat to themselves and/or others, or cause significant disruption to the educational activities of the College community and they have not taken a voluntary leave, such students may be required to take a leave of absence from the College.
In such circumstances, the Associate Dean for Student Life or designee may require a student to undergo a psychological and/or medical evaluation in order to make an informed assessment regarding the student's fitness required for college life. This evaluation can be conducted by a member of the College's clinical staff, or by a student's external health care provider who is providing ongoing healthcare to the student. If an external provider is used, the student will be required to sign a release giving permission to the College's designated clinical personnel to speak with her/his evaluating health care provider and to allow for the release of any relevant medical reports as part of the evaluation process.
If the student chooses not to submit to an evaluation or to allow for a release of information following an evaluation, this may result in a required leave of absence and if applicable, an immediate removal from the residence halls. If, following the evaluation, a leave is deemed unnecessary the Associate Dean for Student Life or designee may impose other conditions and/or requirements which the student would be required to comply with as a condition of continued enrollment at the College.
Examples of behaviors that may necessitate such an evaluation include but are not limited to:
unresolved, ongoing or serious suicidal threats, or behavior indicating a student's inability to care for oneself
disordered eating including self-starvation, binging or purging which may be life-threatening in nature and/or adversely affects the surrounding community

31
evidence of chronic and/or serious alcohol or drug involvement serious threats made to others or articulating serious threats to others within or external to
the Simmons community instances in which a student engages in inappropriate behavior where a contributing
factor is failure to follow a prescribed medical or psychological treatment plan, which may include a prescription regime
instances of inappropriate behavior that cause a chronic, inordinate use of college resources, including but not limited to staff time, psychological services, medical services, and/or emergency services, thereby causing an undue burden to the College
In instances when an involuntary leave is considered, wherever possible the College will encourage the student to take a voluntary leave of absence, thereby aiding in the preservation of the student's privacy and confidentiality. In any instance in which a leave is required, the Associate Dean for Student Life or designee will provide written notice to the student, including the specific requirements that must be met as a condition of eligibility for re-enrollment. In most instances, the parent(s) or guardian(s) of the student will be included in this notice. Students are strongly encouraged to discuss the need for a voluntary or involuntary leave with their parent(s) or guardian(s) prior to and during the leave process.
The duration of the leave is typically no fewer than two semesters, although the specific length of the leave will be determined by the Associate Dean or designee on a case-by-case basis. When a student takes a leave before the end of a semester, whether voluntary or involuntary, Simmons' usual tuition and residence hall refund schedule applies.
Policy for Return to College for Students Hospitalized for Mental Health Reasons
Simmons College students who are not on leave and have been hospitalized for mental health reasons are required to have a clearance interview with the consulting psychiatrist for the College Counseling Center, prior to their return to the College. They are also required to sign an authorization form that enables the hospital or treatment facility to release information necessary for the clearance interview. Following the interview, the consulting psychiatrist will make a recommendation to the Associate Dean for Student Life or designee regarding the student's readiness to return.
As a condition of continued enrollment and, if applicable, as a condition of re-admittance to the residence halls, the following criteria must be met:
1) The consulting psychiatrist must find that the student is sufficiently stable to meet academic requirements and, if applicable, capable of observing the community standards of residential life.
2) The student must commit to follow a recommended and established treatment plan.
32
3) The student and the consulting psychiatrist in conjunction with all relevant health care providers must establish and agree upon a plan for continuing safety after return to College.
In the event that the student chooses to leave the hospital against medical advice without extenuating circumstances which are communicated to the Associate Dean or designee, or has not met the above mentioned criteria, it is possible that she/he may be compromising her/his health and subsequent re-entry to the College. As a result, the student may be required to take a leave of absence for a period of time deemed appropriate by the College.
If the student chooses to take a leave of absence as a result of a hospitalization for mental health reasons, the Associate Dean or designee will assist with processing the leave, and the student will be required to meet with the consulting psychiatrist for a re-entry/clearance interview as a condition of returning to the College. Following a successful clearance interview, the student will meet with the Associate Dean for Student Life or designee to establish a plan for return to the College and to identify community resources as appropriate.
Missing Person's Policy
http://my.simmons.edu/services/business/public-safety/docs/missing_persons.pdf
Procedure to Respond to Bias-Related Incidents
Bias-related harassment may be defined as conduct that has the purpose or effect of unreasonably interfering with an individual's or group's performance or environment or creating an intimidating, hostile, or offensive working, learning, or living environment. Bias-related harassment is based on an individual's or group's religion, ethnicity, race, color, nationality, sex, sexual orientation, disability, or age.
Simmons College is committed to maintaining a respectful and welcoming living and learning environment for all students, faculty, and staff. Any individual found engaging in acts of harassment or bias will be held accountable to the fullest extent possible.
Students are encouraged to report a bias-related incident immediately. Students may report such incidents to any representative of the College but are encouraged to report such incidents to the Office of the Dean for Student Life, the Office of Residence Life, or the Office of Public Safety. Any student life staff member who receives a report of an incident of bias must inform her/his supervisor who will inform public safety, the Dean of Student Life, and the Associate Dean for Student Life. Such matters will be investigated thoroughly. This investigation will include, when appropriate, the photographing and removal of any graffiti or physical evidence related to the act. Any student who is found to have committed a bias-related act will be brought before either the Residence Campus Judicial Board or the Honor Board depending on the location and nature of the incident. Please refer to pages 197-202 of this handbook for the description of the Residence Campus Judicial Board procedures and to pages 195-197 of this handbook for Honor Board procedures.

33
In any bias-related situation, College staff members and public safety officers will take appropriate steps to maintain confidentiality of the student(s) involved; however the law requires any staff member responding to an incident of this nature to file a report describing the basic details of the incident without including the names of students involved.
Any bias-related incident affects both the students who are directly involved and the entire Simmons community. Such matters will be addressed on a community level through various educational means to help create and maintain a respectful and welcoming living and learning environment for all members of the Simmons College community.
Family Educational Rights and Privacy Act of 1974
The College's practice in regard to student record-keeping is based on the provisions of the Family Educational Rights and Privacy Act (FERPA) of 1974 (the Buckley Amendment), and is intended to be a safeguard against the unauthorized release of information. This act applies to all enrolled students, former students, and alumni. It does not apply to applicants seeking admission into an institution.
Under the provisions of the act, it is the right of the student to view her/his official educational records. Educational records are defined as records regarding a student that are maintained by an educational institution. Such records are kept in the Office of the Dean for Student Life, the Office of the Registrar, faculty advisors' offices, and the Center for Academic Achievement. Not included in this category of records are the following:
records containing confidential information written before January 1, 1975 financial records submitted to the College by the parents of a student medical and counseling records records containing information on more than one student private records intended for use of an individual law enforcement records student employment records records to which a student has waived her right of access as required by a judicial order
or a lawful subpoena
In order to view her/his record, a student must make a request in writing to the appropriate office. The office has 45 days in which to fulfill the request. If requested, copies of a student's record are available to the student for a slight charge to cover the cost of duplicating. Any information in a student's record found to be "inaccurate, misleading, or [that] violates the privacy or other rights of the student" may be challenged by the student. Only the accuracy of the information may be challenged.
For example, a grade received may not be questioned, only the accuracy of its recording. In order to contest the information in her/his record, the student must submit a written statement to the person responsible for the content of the record and request that she/he receive a written response. If no written response is forthcoming or if an unsatisfactory response is received by a

34
student, she/he may appeal to the chairperson or appropriate supervisory person. In the event that no resolution is made, it is the student's right to request a hearing, to be presided over by the dean for student life or a designee.
The College has the right to publish a directory listing all enrolled students and containing the following information:
student's name address telephone number place and date of birth concentration digital photo year of graduation and dates of attendance awards and degrees received membership in organizations educational institution most recently attended
A student who wishes to be omitted from the directory must so indicate by writing to the Office of the Registrar.
A student's record is not accessible to anyone outside the College without the written authorization from the student.
Exceptions to this regulation are as follows:
officials at an institution where the student is applying for admission officials disbursing financial aid parents of a dependent student (for tax purposes) accrediting and educational testing organizations federal officials officials complying with a judicial order appropriate officials in the event of an emergency (only if necessary to safeguard the
health or well-being of the student or other individuals) The alleged victim of a crime of violence may receive results of any disciplinary
proceedings conducted by the College against the alleged perpetrator of that crime in reference to that crime. Student records are available to the above with the stipulation that this information is only for the use of the above unless written consent is secured from the student.
Student records may not be distributed to other parties. It is the responsibility of each office maintaining records to keep a log that verifies the name and date of each person who has viewed the record and for what reason. Students have the right to see this log.
35
A student may sign a waiver of access to confidential recommendations for graduate school or for employment purposes. However, the student must be kept informed of those people providing recommendations.
The College does not ordinarily notify a student's parents or guardians of academic and social problems she/he encounters as a Simmons student without her/his consent. However, if a student's behavior places her/his continuance at Simmons or in residence in jeopardy, or if the student's behavior indicates she/he may be harmful to herself/himself or others, the College may deem it to be in her/his best interest to notify, without consent, her/his parents, guardians, or other appropriate persons.
Depending upon the nature and seriousness of the student's behavior she/he may be asked to leave the Residence Campus and/or the College immediately.
Prior to asking a student to leave residence and/or school, the College may deem it necessary to enter into a contractual agreement with a student around the student's behavior in residence and/or the College community, particularly in situations where the student's behavior has become an issue for the larger community. Should a contractual agreement be entered into between a student and the College, the College maintains the right to handle any violations of the contractual agreement administratively rather than through the student judicial process. A student may appeal administrative decisions about violations of her contractual agreement to the Dean for Student Life within seven business days of the decision that has been communicated to her. The appeal must be made in writing.
Further questions about the Buckley Amendment should be directed to the Office of the Dean for Student Life.
Simmons College Grievance Procedures
In the event of a perceived disagreement with program personnel, a student should first make the effort to resolve the disagreement with the particular faculty. If resolution is not forthcoming, the student may then discuss the issue with the Program Director. In the rare instance where the problem is still unresolved to the satisfaction of the student, the matter may be referred to the Office of the Associate Dean of the School for Health Studies by either the student of the Program Director. In the event of a perceived disagreement with a student’s education records (i.e. evaluation of the Buckley Amendment), the individual has the right to readdress her concerns in the following manner: The hearing panel for undergraduate and graduate students will be composed of the Associate Dean of the College, who will act as the chairperson, and two other officials (one faculty member and one administrator to be appointed by the President). The hearing panel for graduate students shall be similarly composed with presidential appointments from the graduate division.
36
A student’s request for a formal hearing must be made in writing to the Associate Dean of the College who, within a reasonable time period, must inform the student of the date, place and time of the hearing. Due process, as outlined in the Simmons College Honor System, will be afforded the student during the hearing. The decision of the hearing panel will be final and written notification will be forwarded to all parties concerned.
If the decision is in favor of the student, the office maintaining the student record will be instructed to correct or amend the appropriate portions of the student record.
If the decision is unfavorable to the student, the chairperson of the panel must include in the notification of the decision a statement of the reasons for the decision and inform the student that she may place with the education record a statement commenting on the information in question, or a statement of disagreement with the decision of the Hearing Panel. This statement becomes part of the student’s permanent record and will be disclosed to all authorized parties.
All college personnel who work with student education records are reminded to avoid placing irrelevant or injudicious comments in student records. However, no portion of a student’s record may be destroyed if a request for access or review is outstanding. In the event of a perceived violation of the Honor Code, the following procedures should be utilized:
Members of the community who violate the Code of Responsibility are obliged to report themselves immediately to the Chairperson of the Honor Board. A student who observes another student violating the Code of Responsibility is obligated to inform her of the violation and urge her to report herself to the Chairperson of the Honor Board. The observing student is encouraged to report the case to the Board, if the offending student does not do so herself.
Faculty and administrators who observe or suspect a student of violating the Code of Responsibility are obliged to first discuss the matter with the student and then to report the incident to the Chairperson of the Honor Board.
Should a member of the faculty or the administration be suspected of violating the Code of Responsibility, she/he should be so informed by the person or persons observing the violation and urged to report herself/himself to the Chairperson of the Honor Board. The observing party is encouraged to report the case to the Chairperson of the Honor Board if the offending party does not do so.
Mutual responsibility is a very important strength of the Honor System, and abiding by the system is each person’s inherent responsibility to the community as a whole. This is a difficult obligation; without it, however, the integrity of the Honor System cannot be maintained.

37
SIMMONS COLLEGE DIETETIC INTERNSHIP PROGRAM
Competency Statements for the Supervised Practice Component of Entry-Level Dietitian Education Programs
Competency statements specify what every dietitian should be able to so at the beginning of his or her practice career. The core competency statements build on appropriate knowledge and skills necessary for the entry-level practitioner to perform reliably at the verb level indicated. Also, since Simmons College has chosen to offer an internship program with community-emphasis, there are nine additional community-oriented competencies that must be met by students participating in the Simmons College dietetic internship program. Therefore, there are fifty-six competencies that are to be acquired by students by the end of the 30-week experience. The minimum performance level for the competency is indicated by the action verb used at the beginning of the statement. The action verbs reflect four levels of performance as outlined below. The higher level of performance assumes the ability to perform at the lower level:
assist - independent performance under supervision, or participate - take part in team activities;
perform - able to initiate activities without direct supervision, or conduct - activities performed independently;
consult - able to perform specialized functions that are discrete delegated activities intended to improve the work of others, or supervise - able to oversee daily operations of a unit including personnel, resource utilization, and environmental issues; or coordinate and direct the activities of a team or project workgroup;
manage - able to plan, organize, and direct an organization unit through actual or simulated experiences, including knowing what questions to ask
It is recommended that you use these definitions above to develop planned experiences if they differ from the ones stated on the evaluation form.

38
Competencies/Learning Outcomes for Dietetic Internship Programs Upon completion of the supervised practice component of dietitian education, all graduates will be able to do the following:
Competencies/Learning Outcomes for Dietetic Internship Programs
Competency Number
Description of the Competency
CRD 1.1 Select indicators of program quality and/or customer service and measure achievement of objectives. (Tip: Outcomes may include clinical, programmatic, quality, productivity, economic, or other outcomes in wellness, management, sports, clinical settings, etc.)
CRD 1.2 Apply evidence-based guidelines, systematic reviews, and scientific literature (such as the Academy’s Evidence Analysis Library and Evidence-based Nutrition Practice Guidelines, the Cochrane Database of Systematic Reviews, and the U.S. Department of Health and Human Services, Agency for Healthcare Research and Quality, and National Guideline Clearinghouse websites) in nutrition care process and model and other areas of dietetic practice.
CRD 1.3 Justify programs, products, services and care using appropriate evidence or data.
CRD 1.4 Evaluate emerging research for application in dietetics practice.
CRD 1.5 Conduct projects using appropriate research methods, ethical procedures, and data analysis.
CRD 2.1 Practice in compliance with current federal regulations and state statutes and rules, as applicable and in accordance with accreditation standards and the Scope of Dietetic Practice and Code of Ethics for the Profession of Dietetics.
CRD 2.2 Demonstrate professional writing skills in preparing professional communications. (Tip: Examples include research manuscripts, project proposals, education materials, policies, and procedures.)
CRD 2.3 Design, implement, and evaluate presentations to a target audience. (Tip: A quality presentation considers life experiences, cultural diversity, and educational background of the target audience.)
CRD 2.4 Use effective education and counseling skills to facilitate behavior change.
CRD 2.5 Demonstrate active participation, teamwork, and contributions in group settings.
CRD 2.6 Assign appropriate patient care activities to DTRs and/or support personnel as appropriate. (Tip: In completing the task, the student/intern should consider the needs of the patient/client or situation, the ability of the support personnel, jurisdictional law, practice guidelines, and policies within the facility.)
CRD 2.7 Refer clients and patients to other professionals and services when needs are beyond individual scope of practice.

39
CRD 2.8 Apply leadership skills to achieve desired outcomes.
CRD 2.9 Participate in professional and community organizations (see tip, below).
CRD 2.10 Establish collaborative relationships with other health professionals and support personnel to deliver effective nutrition services. (Tip: Other health professionals include physicians, nurses, pharmacists, etc.)
CRD 2.11 Demonstrate professional attributes within organizational cultures. (Tip: Professional attributes include initiative and proactively developing solutions, advocacy, customer focus, risk taking, critical thinking, flexibility, time management, work prioritization, and work ethic.)
CRD 2.12 Perform self-assessment, develop goals and objectives, and prepare a draft portfolio for professional development as defined by the Commission on Dietetic Registration.
CRD 2.13 Develop negotiation skills. (Tip: Demonstrating negotiating skills includes showing assertiveness when needed while respecting the life experiences, cultural diversity, and educational background of the other parties.)
CRD 3.1 Perform the Nutrition Care Process (a through e below) and use standardized nutrition language for individuals, group, and populations of differing ages and health status, in a variety of settings.
CRD 3.1a Assess the nutritional status of individuals, groups, and populations in a variety of settings where nutrition care is or can be delivered.
CRD 3.1b Diagnose nutrition problems and create problem, etiology, signs, and symptoms (PES) statements.
CRD 3.1c Plan and implement nutrition interventions to include prioritizing the nutrition diagnosis, formulating a nutrition prescription, establishing goals, and selecting and managing intervention.
CRD 3.1d Monitor and evaluate problems, etiologies, signs, symptoms and the impact of interventions on the nutrition diagnosis.
CRD 3.1e Complete documentation that follows professional guidelines, guidelines required by health care systems, and guidelines required by the practice setting.
CRD 3.2 Demonstrate effective communication skills for clinical and customer services in a variety of formats. (Tip: Formats include oral, print, visual, electronic, and mass media methods for maximizing client education, employee training, and marketing.)
CRD 3.3 Develop and deliver products, programs, or services that promote consumer health, wellness, and lifestyle management. (Tip: Students/interns should consider health messages and interventions that integrate the consumer’s desire for taste, convenience, and economy with the need for nutrition and food safety.)
CRD 3.4 Deliver respectful, science-based answers to consumer questions concerning emerging trends.

40
CRD 3.5 Coordinate procurement, production, distribution, and service of goods and services. (Tip: Students/interns should demonstrate and promote responsible use of resources including employees, money, time, water, energy, food, and disposable goods.)
CRD 3.6 Develop and evaluate recipes, formulas, and menus for acceptability and affordability that accommodates cultural diversity and health needs of various populations, groups, and individuals.
CRD 4.1 Participate in management of human resources.
CRD 4.2 Perform management functions related to safety, security, and sanitation that affect employees, customers, patients, facilities, and food.
CRD 4.3 Participate in public policy activities, including both legislative and regulatory initiatives.
CRD 4.4 Conduct clinical and customer service quality management activities.
CRD 4.5 Use current informatics technology to develop, store, retrieve, and disseminate information and data.
CRD 4.6 Analyze quality, financial, or productivity data and develop a plan for intervention.
CRD 4.7 Propose and use procedures as appropriate to the practice setting to reduce waste and protect the environment. (Tip: Students/interns are encouraged to promote environmentally-friendly practices so that future generations have the water, materials, and resources to protect human health and life on the planet. Practical steps include using local ingredients; not wasting food and resources; using efficacious, non-toxic products when available; properly disposing of toxic material; reusing containers and products; recycling when possible; purchasing products with recycled content; and teaching others the value of sustainability.)
CRD 4.8 Conduct feasibility studies for products, programs, or services with consideration of costs and benefits.
CRD 4.9 Analyze financial data to assess utilization of resources.
CRD 4.10 Develop a plan to provide or develop a product, program, or service that includes budget, staffing needs, equipment, and supplies.
CRD 4.11 Code and bill for dietetic/nutrition services to obtain reimbursement from public or private insurers.
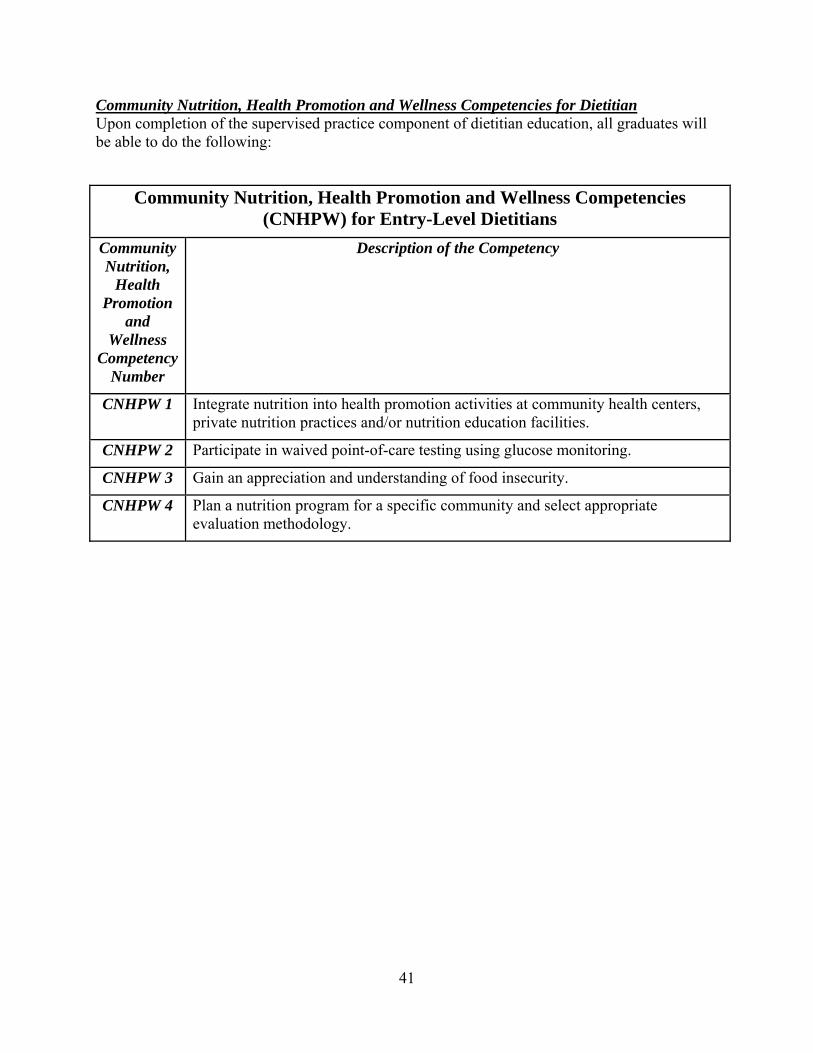
41
Community Nutrition, Health Promotion and Wellness Competencies for Dietitian Upon completion of the supervised practice component of dietitian education, all graduates will be able to do the following:
Community Nutrition, Health Promotion and Wellness Competencies (CNHPW) for Entry-Level Dietitians
Community Nutrition,
Health Promotion
and Wellness
Competency Number
Description of the Competency
CNHPW 1 Integrate nutrition into health promotion activities at community health centers, private nutrition practices and/or nutrition education facilities.
CNHPW 2 Participate in waived point-of-care testing using glucose monitoring.
CNHPW 3 Gain an appreciation and understanding of food insecurity.
CNHPW 4 Plan a nutrition program for a specific community and select appropriate evaluation methodology.

42
SIMMONS COLLEGE DIETETIC INTERNSHIP PROGRAM
Allocation of the Core and Community-Focused Competencies of the Simmons College Dietetic Internship Rotations
***** = The competency must be met during the particular rotation, meeting or graduate class. Competency Counseling &
Education Acute/
Clinical Care LTC/FS DPH Community
Health Center Exec Office of Elder Affairs
Research and Professional
Practice Week
Nutrition 452 and Simmons
Classes
CRD 1.1 * * * * * * CRD 1.2 ***** CRD 1.3 * * * * CRD 1.4 * * * CRD 1.5 ***** CRD 2.1 * * * * * * CRD 2.2 * * * * * CRD 2.3 * * * CRD 2.4 * * * CRD 2.5 * * * * * * * CRD 2.6 * * CRD 2.7 * * * CRD 2.8 * * * * * * CRD 2.9 ***** CRD 2.10 * * * * * * CRD 2.11 * * * * CRD 2.12 * * * * * * * CRD 2.13 * * * * * CRD 3.1 * * * CRD 3.1.a * * * CRD 3.1.b * * * CRD 3.1.c * * * CRD 3.1.d * * * CRD 3.1e * * * CRD 3.2 * * * * * * CRD 3.3 * * * * * CRD 3.4 * * * * CRD 3.5 ***** CRD 3.6 * * * * * * CRD 4.1 ***** CRD 4.2 ***** * CRD 4.3 * * * CRD 4.4 * * *
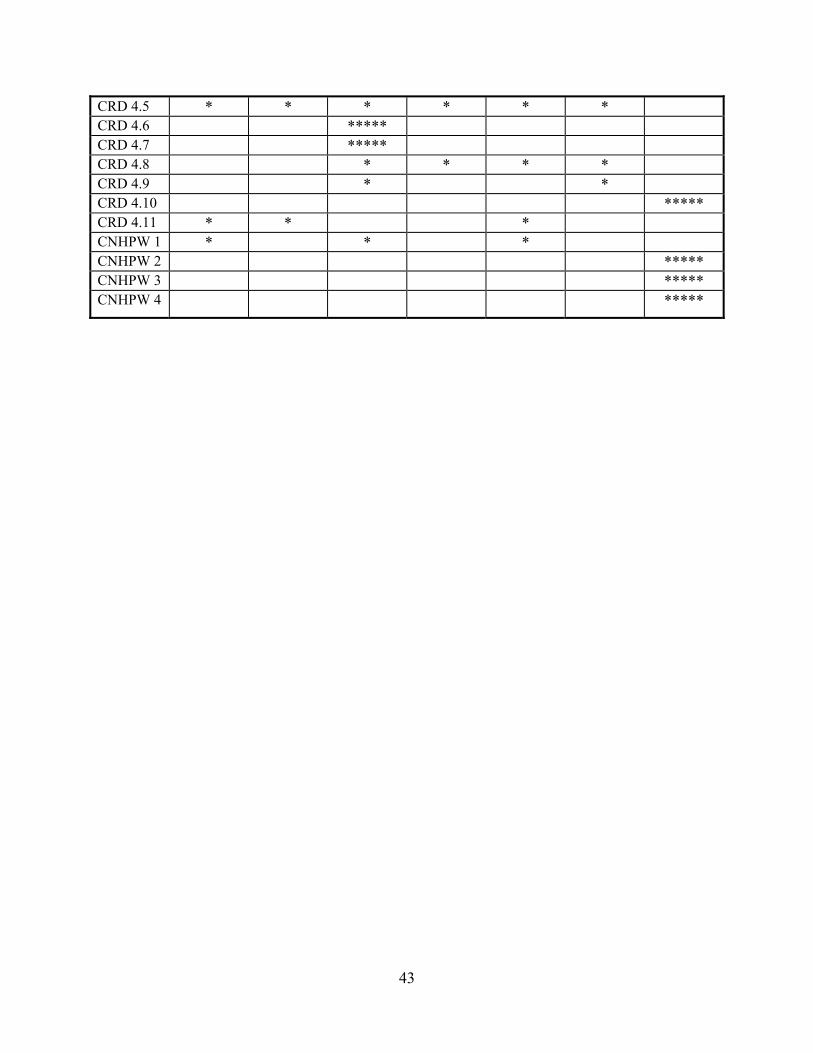
43
CRD 4.5 * * * * * * CRD 4.6 ***** CRD 4.7 ***** CRD 4.8 * * * * CRD 4.9 * * CRD 4.10 ***** CRD 4.11 * * * CNHPW 1 * * * CNHPW 2 ***** CNHPW 3 ***** CNHPW 4 *****

44
SIMMONS COLLEGE DIETETIC INTERNSHIP PROGRAM
Student Performance Evaluation Instructions
The process of periodically evaluating dietetic interns is essential for ensuring that they achieve entry-level competence by the end of their internship experience. The evaluation forms created for the Simmons College Dietetic Internship Program are based on the Academy of Nutrition and Dietetics’ forty core competency statements developed for the supervised practice component for gaining registered dietitian status. Additionally, since Simmons College offers a community-emphasis internship program, students enrolled in the program are required to meet four additional community-oriented competencies. In sum, there are forty-four competencies that must be met by the Simmons College dietetic interns by the end of their 33-week experience.
A separate Student Performance Evaluation Form has been created for each of the seven rotations offered by the Simmons College Dietetic Internship Program (DIP):
1. Clinical/Acute Care Rotation 2. Community Health Center Rotation 3. Department of Public Health Rotation 4. Counseling and Education Rotation 5. Foodservice Rotation 6. State Government-based Nutrition Initiative Rotation 7. Research and Professional Practice/Class Days/Nutrition 452
The competencies have been assigned to different rotations based on the experiences that students are expected to encounter within each of the rotations. Some competencies can only be met at one rotation while other competencies have been assigned to multiple rotations and can be met at any time. The following will describe how to properly complete the Student Performance Evaluation Form. 1. Column 1: Competency Statements
The first column introduces the Academy of Nutrition and Dietetics’ competency statements. CRD 1.1 through CRD 4.11 are the core competencies and CNHPW 1 through CNHPW 4 are the community-emphasis competencies. Not all competencies will appear on each evaluation form.
The minimum performance level for the competency is indicated by the action verb used at the beginning of the statement. The action verbs reflect four levels of performance beginning with introductory (1) and progressing through entry level competence (4). Ranking the competencies in this manner allows the student and preceptor to plan experiences that will gradually and logically advance the student from an introductory level of competence (1) to entry level competence (4) by the end of their experience. As the student and preceptor formulate a list of experiences for a rotation, the competencies marked as ‘1’ (introductory) should be met first and progress from ‘2’ to ‘3’ and ultimately to level 4 (entry level). Also, keep in mind that the higher level of performance assumes the ability to perform at the lower level. Action Verb Definition:
45
1. assist - independent performance under supervision, or participate - take part in team activities;
2. perform - able to initiate activities without direct supervision, or conduct - activities performed independently;
3. consult - able to perform specialized functions that are discrete delegated activities intended to improve the work of others, or supervise - able to oversee daily operations of a unit including personnel, resource utilization, and environmental issues; or coordinate and direct the activities of a team or project workgroup;
4. manage - able to plan, organize, and direct an organization unit through actual or simulated experiences, including knowing what questions to ask.
Important Notes: Specific competencies have been chosen for specific rotations. The competencies
that begin with five stars (*****) indicate that the competency can only be met in the particular rotation and therefore must be given priority.
Only those competencies that students have attempted to acquire at a rotation should be scored and all others left blank.
As mentioned above, not all competencies will appear on each evaluation form. If a student meets a competency that is not listed on the evaluation form intended for the given rotation, the preceptor can sign off on the competency on any other evaluation form that lists the competency of interest.
2. Column 2: Planned Experience
The second column lists planned experiences that would be appropriate for meeting the competencies listed in column one.
The planned experiences for each competency start with introductory experiences and progress to higher levels of difficulty based on the level of expertise the competency requires for the student to acquire.
Note: These experiences can be changed, but substitute experiences must adequately meet the competency described in column one. It is recommended that you use the action verbs mentioned above to develop planned experiences if they differ from the ones stated on the evaluation form.
3. Column 3: Actual Activities
Students must summarize the actual activities they have completed to satisfy the competency listed in the first column. This section is to be completed by the student before the supervisor evaluates whether or not the student has satisfied the competency during the given rotation.
The description of the actual activities should be specific. For example, if the planned experience is to ‘Create and evaluate one nutrition education handout intended for the target population served at a community health center’ then the

46
actual activity statement should be similar to the following: ‘Developed a one-sided nutrition handout entitled ‘Are You Getting Enough Calcium?’ for the African American population at a community health center. Evaluated the effectiveness of the handout by asking five health center members to answer a short questionnaire inquiring about what they learned from the handout’.
Keep in mind that the planned experiences and activities are performed as a means for meeting the competencies.
4. Column 4: Evaluation
Both the student and supervisor are required to evaluate the student. The student must complete the ‘actual activities’ column and score themselves prior to giving the evaluation form to their supervisor.
The score is based on a scale of 1 to 3. The following provides descriptions of the one through three continuum:
1. Student requires constant supervision and assistance to demonstrate skills or knowledge. Cannot meet stated criteria.
2. Needs occasional guidance to demonstrate skills or knowledge. May seek consultation prior to completion of activity.
3. Consistently demonstrates skills or knowledge with no guidance. Supervisor needs only to respond to student questions or requests upon completion of activity.
A score of two or better indicates that the student has adequately met the entry-level competency via the planned experience.
The supervisor is responsible for circling the ‘met’ or ‘exceeds’ statement in the ‘Final Evaluation’ portion of the form only when the competency has been completed in the rotation during which they were the primary supervisor. Please also have the student’s preceptor sign next to ‘Evaluation’ column for each competency met during the rotation.
The ‘not met’ column is circled when the student did not satisfactorily meet the stated competency by the end of the rotation.
The ‘met’ column is circled when the student needs occasional guidance to demonstrate skills or knowledge. May seek consultation prior to completion of activity.
The ‘exceeds’ column is circled when the student consistently demonstrates skills or knowledge with no guidance. Supervisor needs only to respond to student questions or requests upon completion of activity.
The ‘N.O. = not observed’ column is checked when the supervisor has not had the opportunity to observe the student demonstrate skills that demonstrate that they have met the competency.

47
SIMMONS COLLEGE DIETETIC INTERNSHIP PROGRAM
Clinical/Acute Care Rotation Program Competencies and Planned Experiences
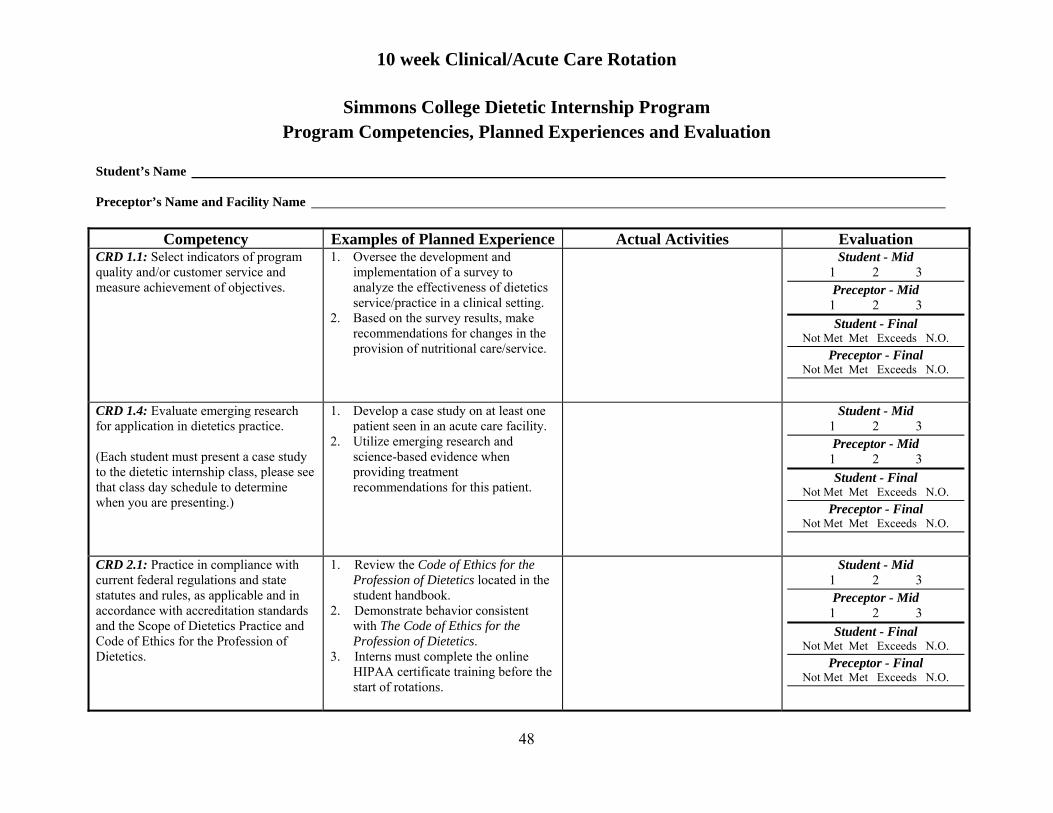
10 week Clinical/Acute Care Rotation
48
Simmons College Dietetic Internship Program Program Competencies, Planned Experiences and Evaluation
Student’s Name Preceptor’s Name and Facility Name
Competency Examples of Planned Experience Actual Activities Evaluation CRD 1.1: Select indicators of program quality and/or customer service and measure achievement of objectives.
1. Oversee the development and implementation of a survey to analyze the effectiveness of dietetics service/practice in a clinical setting.
2. Based on the survey results, make recommendations for changes in the provision of nutritional care/service.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 1.4: Evaluate emerging research for application in dietetics practice. (Each student must present a case study to the dietetic internship class, please see that class day schedule to determine when you are presenting.)
1. Develop a case study on at least one patient seen in an acute care facility.
2. Utilize emerging research and science-based evidence when providing treatment recommendations for this patient.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 2.1: Practice in compliance with current federal regulations and state statutes and rules, as applicable and in accordance with accreditation standards and the Scope of Dietetics Practice and Code of Ethics for the Profession of Dietetics.
1. Review the Code of Ethics for the Profession of Dietetics located in the student handbook.
2. Demonstrate behavior consistent with The Code of Ethics for the Profession of Dietetics.
3. Interns must complete the online HIPAA certificate training before the start of rotations.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.

10 week Clinical/Acute Care Rotation
49
CRD 2.4: Use effective education and counseling skills to facilitate behavior change.
1. Formulate medical nutrition therapy recommendations for at least three patients/clients with complex medical conditions.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 2.5: Demonstrate active participation, teamwork and contributions in group settings.
1. Participate in grand rounds or an interdisciplinary care plan meeting on an assigned medical unit.
2. Present and discuss nutritional recommendations for one patient at interdisciplinary rounds for an assigned hospital unit.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 2.6: Assign appropriate patient care activities to DTRs and/or support personnel as appropriate.
1. Assign diet office staff/diet aids to deliver nutrition supplements and trays to patients.
2. Assign diet office employees to monitor tray delivery to patients and food consumption.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 2.7: Refer clients and patients to other professionals and services when needs are beyond individual scope of practice.
1. Refer at least one patient/client to a dietetic or other health care professional within an acute care facility.
2. Refer at least one patient/client to PT, OT, SLP, social work, or psychology.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
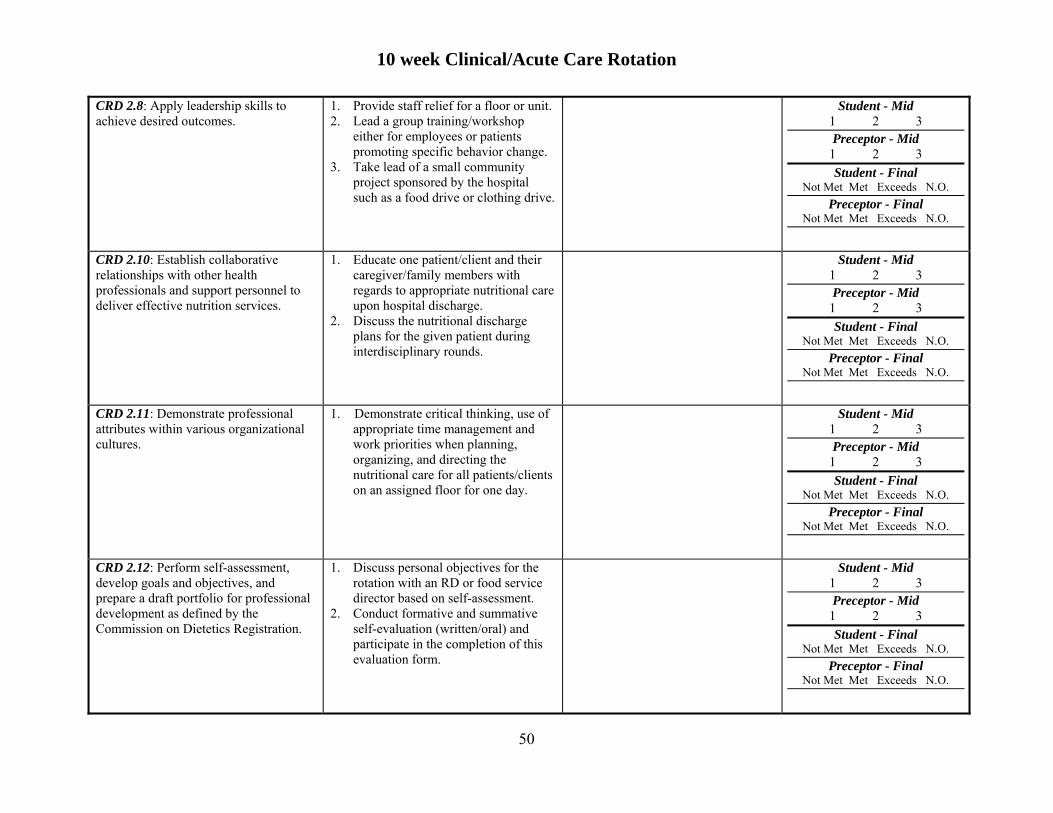
10 week Clinical/Acute Care Rotation
50
CRD 2.8: Apply leadership skills to achieve desired outcomes.
1. Provide staff relief for a floor or unit. 2. Lead a group training/workshop
either for employees or patients promoting specific behavior change.
3. Take lead of a small community project sponsored by the hospital such as a food drive or clothing drive.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 2.10: Establish collaborative relationships with other health professionals and support personnel to deliver effective nutrition services.
1. Educate one patient/client and their caregiver/family members with regards to appropriate nutritional care upon hospital discharge.
2. Discuss the nutritional discharge plans for the given patient during interdisciplinary rounds.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 2.11: Demonstrate professional attributes within various organizational cultures.
1. Demonstrate critical thinking, use of appropriate time management and work priorities when planning, organizing, and directing the nutritional care for all patients/clients on an assigned floor for one day.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 2.12: Perform self-assessment, develop goals and objectives, and prepare a draft portfolio for professional development as defined by the Commission on Dietetics Registration.
1. Discuss personal objectives for the rotation with an RD or food service director based on self-assessment.
2. Conduct formative and summative self-evaluation (written/oral) and participate in the completion of this evaluation form.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
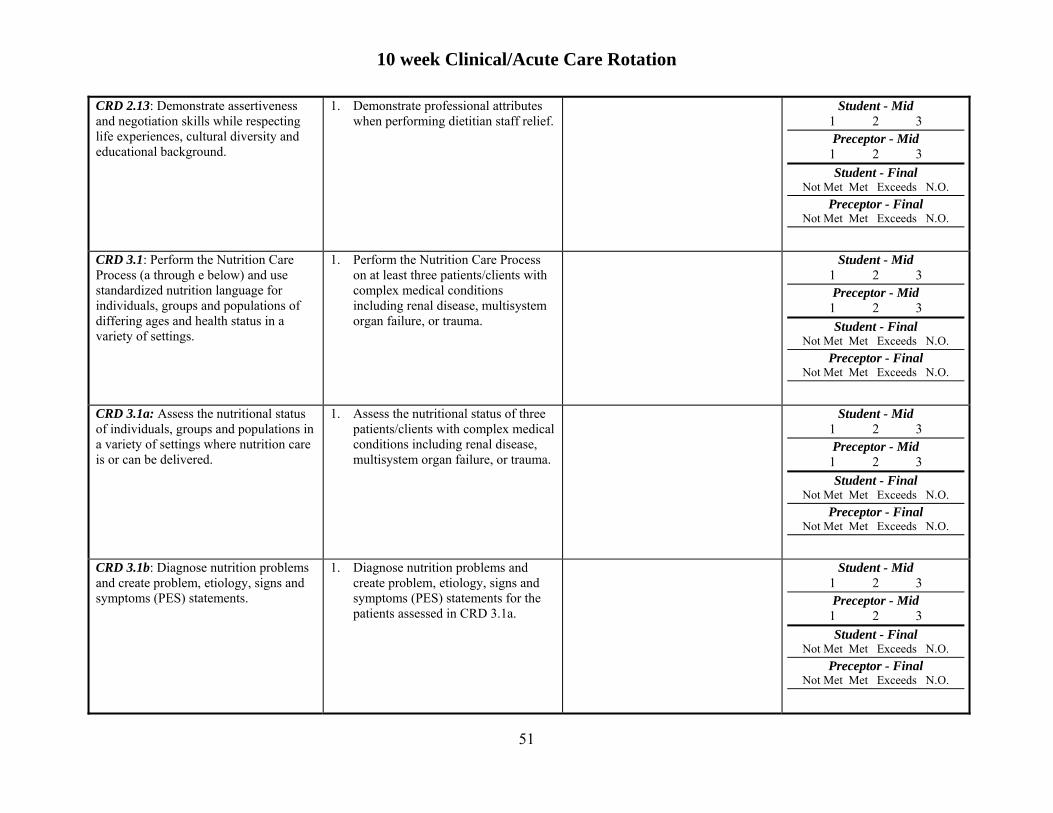
10 week Clinical/Acute Care Rotation
51
CRD 2.13: Demonstrate assertiveness and negotiation skills while respecting life experiences, cultural diversity and educational background.
1. Demonstrate professional attributes when performing dietitian staff relief.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 3.1: Perform the Nutrition Care Process (a through e below) and use standardized nutrition language for individuals, groups and populations of differing ages and health status in a variety of settings.
1. Perform the Nutrition Care Process on at least three patients/clients with complex medical conditions including renal disease, multisystem organ failure, or trauma.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 3.1a: Assess the nutritional status of individuals, groups and populations in a variety of settings where nutrition care is or can be delivered.
1. Assess the nutritional status of three patients/clients with complex medical conditions including renal disease, multisystem organ failure, or trauma.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 3.1b: Diagnose nutrition problems and create problem, etiology, signs and symptoms (PES) statements.
1. Diagnose nutrition problems and create problem, etiology, signs and symptoms (PES) statements for the patients assessed in CRD 3.1a.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
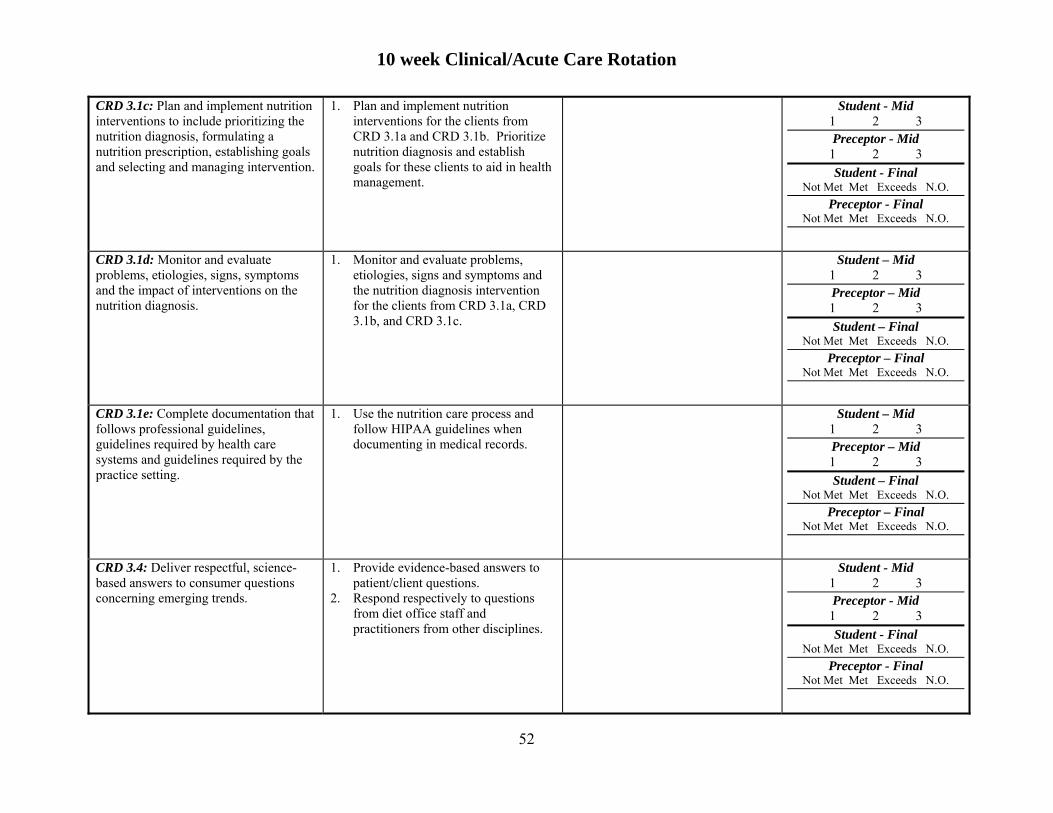
10 week Clinical/Acute Care Rotation
52
CRD 3.1c: Plan and implement nutrition interventions to include prioritizing the nutrition diagnosis, formulating a nutrition prescription, establishing goals and selecting and managing intervention.
1. Plan and implement nutrition interventions for the clients from CRD 3.1a and CRD 3.1b. Prioritize nutrition diagnosis and establish goals for these clients to aid in health management.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 3.1d: Monitor and evaluate problems, etiologies, signs, symptoms and the impact of interventions on the nutrition diagnosis.
1. Monitor and evaluate problems, etiologies, signs and symptoms and the nutrition diagnosis intervention for the clients from CRD 3.1a, CRD 3.1b, and CRD 3.1c.
Student – Mid 1 2 3
Preceptor – Mid
1 2 3
Student – Final Not Met Met Exceeds N.O.
Preceptor – Final Not Met Met Exceeds N.O.
CRD 3.1e: Complete documentation that follows professional guidelines, guidelines required by health care systems and guidelines required by the practice setting.
1. Use the nutrition care process and follow HIPAA guidelines when documenting in medical records.
Student – Mid 1 2 3
Preceptor – Mid
1 2 3
Student – Final Not Met Met Exceeds N.O.
Preceptor – Final Not Met Met Exceeds N.O.
CRD 3.4: Deliver respectful, science-based answers to consumer questions concerning emerging trends.
1. Provide evidence-based answers to patient/client questions.
2. Respond respectively to questions from diet office staff and practitioners from other disciplines.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.

10 week Clinical/Acute Care Rotation
53
CRD 3.6: Develop and evaluate recipes, formulas and menus for acceptability and affordability that accommodate the cultural diversity and health needs of various populations, groups and individuals.
1. Screen and assess at least one patient receiving enteral and/or parenteral nutrition as their primary source of nourishment.
2. Calculate calorie, protein, carbohydrate, fat, and water needs of the specified patient incorporating these requirements into enteral/parenteral feeding regimes.
3. Evaluate enteral/parenteral recommendations within 48 hours after initiated.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 4.4: Conduct clinical and customer service quality management activities.
1. Perform tray audits. 2. Participate in meal rounds.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 4.5: Use current informatics technology to develop, store, retrieve, and disseminate information and data.
1. Use technology when creating, storing, or retrieving client education materials.
2. Utilize computerized medical records when reviewing care plans or documenting in patient charts.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 4.11: Code and bill for dietetic/nutrition services to obtain reimbursement from public or private insurers.
1. Participate in the coding and billing of dietetics/nutrition services for at least one client provided with nutrition services at the facility.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
10 week Clinical/Acute Care Rotation
54
Additional Comments Regarding the Student’s Performance and Abilities:
Strengths Weaknesses
Preceptor Signature: Date:

55
SIMMONS COLLEGE DIETETIC INTERNSHIP PROGRAM
Community Health Center (CHC) Rotation Program Competencies and Planned Experiences
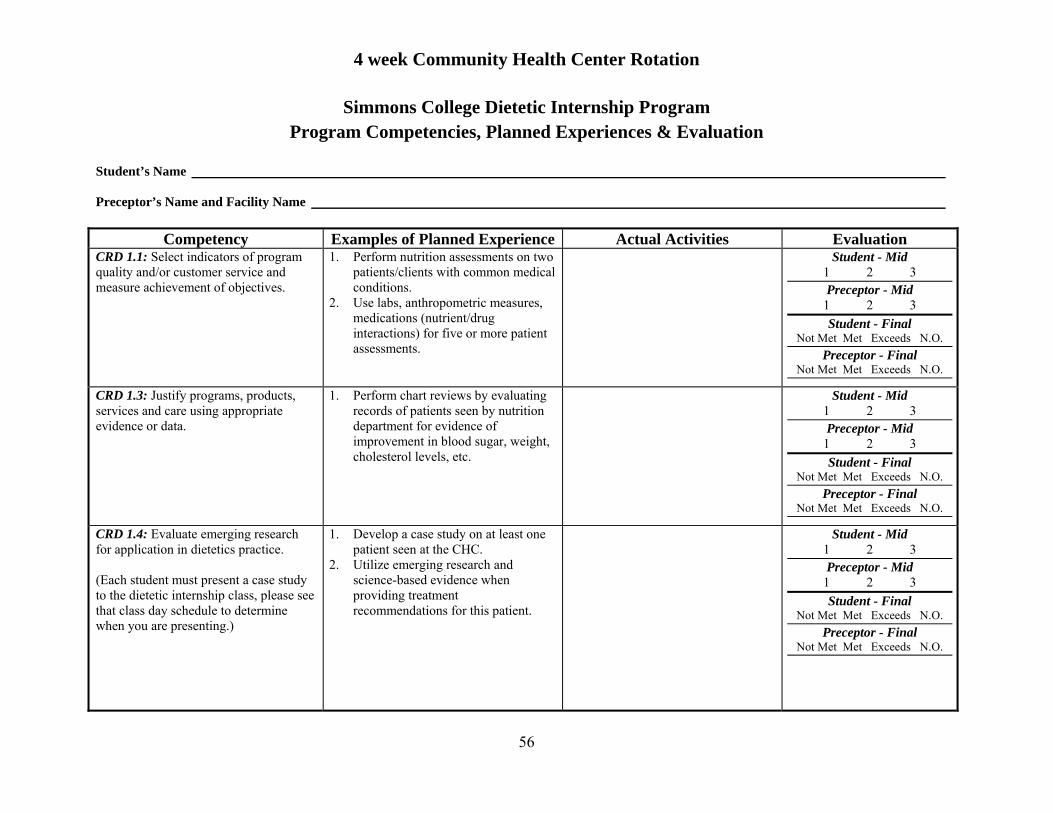
4 week Community Health Center Rotation
56
Simmons College Dietetic Internship Program Program Competencies, Planned Experiences & Evaluation
Student’s Name Preceptor’s Name and Facility Name
Competency Examples of Planned Experience Actual Activities Evaluation CRD 1.1: Select indicators of program quality and/or customer service and measure achievement of objectives.
1. Perform nutrition assessments on two patients/clients with common medical conditions.
2. Use labs, anthropometric measures, medications (nutrient/drug interactions) for five or more patient assessments.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 1.3: Justify programs, products, services and care using appropriate evidence or data.
1. Perform chart reviews by evaluating records of patients seen by nutrition department for evidence of improvement in blood sugar, weight, cholesterol levels, etc.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 1.4: Evaluate emerging research for application in dietetics practice. (Each student must present a case study to the dietetic internship class, please see that class day schedule to determine when you are presenting.)
1. Develop a case study on at least one patient seen at the CHC.
2. Utilize emerging research and science-based evidence when providing treatment recommendations for this patient.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
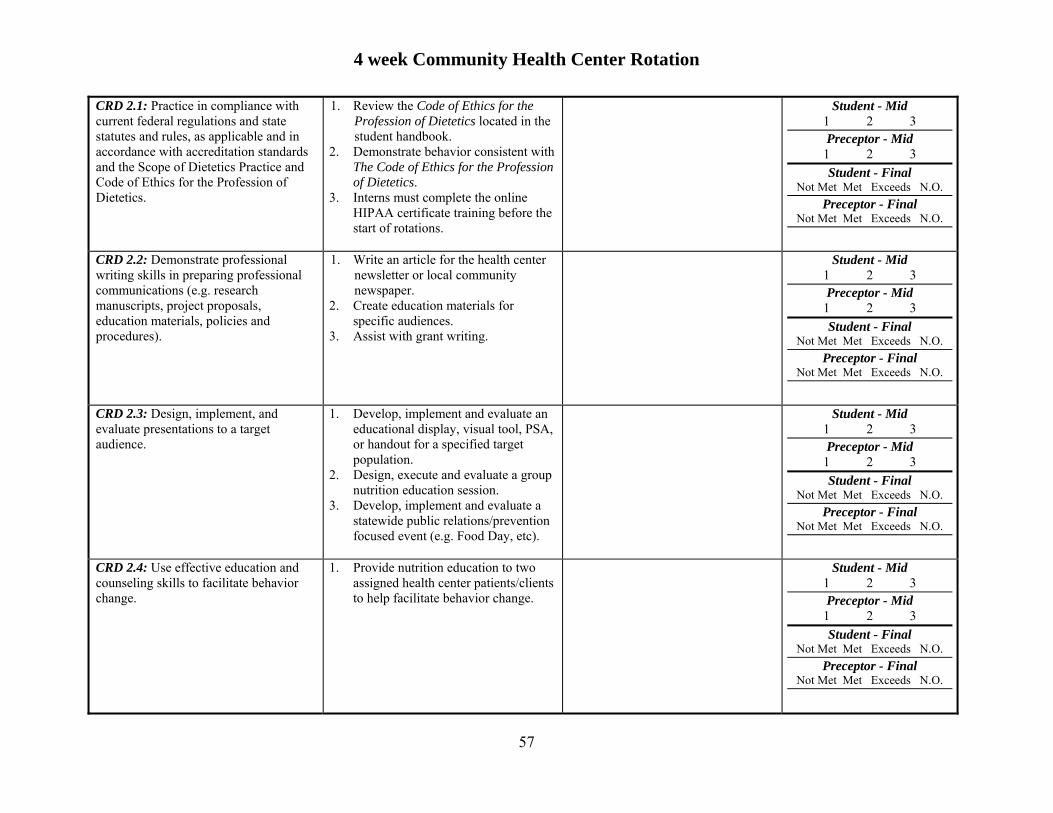
4 week Community Health Center Rotation
57
CRD 2.1: Practice in compliance with current federal regulations and state statutes and rules, as applicable and in accordance with accreditation standards and the Scope of Dietetics Practice and Code of Ethics for the Profession of Dietetics.
1. Review the Code of Ethics for the Profession of Dietetics located in the student handbook.
2. Demonstrate behavior consistent with The Code of Ethics for the Profession of Dietetics.
3. Interns must complete the online HIPAA certificate training before the start of rotations.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 2.2: Demonstrate professional writing skills in preparing professional communications (e.g. research manuscripts, project proposals, education materials, policies and procedures).
1. Write an article for the health center newsletter or local community newspaper.
2. Create education materials for specific audiences.
3. Assist with grant writing.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 2.3: Design, implement, and evaluate presentations to a target audience.
1. Develop, implement and evaluate an educational display, visual tool, PSA, or handout for a specified target population.
2. Design, execute and evaluate a group nutrition education session.
3. Develop, implement and evaluate a statewide public relations/prevention focused event (e.g. Food Day, etc).
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 2.4: Use effective education and counseling skills to facilitate behavior change.
1. Provide nutrition education to two assigned health center patients/clients to help facilitate behavior change.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.

4 week Community Health Center Rotation
58
CRD 2.5: Demonstrate active participation, teamwork, and contributions in group settings.
1. Participate in an interdisciplinary health center staff meeting or case conference.
2. Assist with group education sessions or workshops.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 2.7: Refer clients and patients to other professionals and services when needs are beyond individual scope of practice.
1. Refer at least one patient/client to a dietetic or other health care professional in the community CHC.
2. Refer at least one patient/client to PT, OT, SLP, social work, or psychology.
3. Refer at least one patient/client to community services such as food banks/pantry, smoking cessation services, WIC, fuel assistance, etc.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 2.8: Apply leadership skills to achieve desired outcomes.
1. Lead a group training/workshop either for employees or patients of the CHC promoting specific behavior change.
2. Take lead of a small community project sponsored by the health center such as a food drive or clothing drive.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 2.10: Establish collaborative relationships with other health professionals and support personnel to deliver effective nutrition services.
1. Work collaboratively with health professionals and caregivers to meet the nutritional needs of clients.
2. Participate in a staff meeting that involves employees of the health center other than the nutrition staff.
3. Consult with another health professional in the CHC, such as the CDE, a doctor, nurse, or WIC staff to better tailor treatment.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.

4 week Community Health Center Rotation
59
CRD 2.11: Demonstrate professional attributes such as advocacy, customer focus, risk taking, critical thinking, flexibility, time management, work prioritization, and work ethic within various organizational cultures.
1. Demonstrate a client focus and use of appropriate time management and work priorities when initiating the activities necessary to conduct a community-based health promotion/disease prevention program to address the most common nutritional needs/risks of clients frequenting the CHC.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 2.12: Perform self-assessment, develop goals and objectives, and prepare a draft portfolio for professional development as defined by the Commission on Dietetics Registration.
1. Discuss personal objectives for the rotation with an RD or food service director based on self-assessment.
2. Conduct formative and summative self-evaluation (written/oral) and participate in the completion of this evaluation form.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 2.13: Demonstrate assertiveness and negotiation skills while respecting life experiences, cultural diversity, and educational background.
1. Demonstrate assertiveness when making dietary recommendations to healthcare professionals from other disciplines.
2. Consider cultural diversity and socioeconomic status of clients when making dietary recommendations.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 3.1: Perform the Nutrition Care Process (a through e below) and use standardized nutrition language for individuals, groups, and populations of differing ages and health status in a variety of settings.
1. Perform the Nutrition Care Process on at least two clients including pregnant women, children, or other clients with unique health conditions (overweight, obesity, diabetes, cholesterol management, women’s health, etc).
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
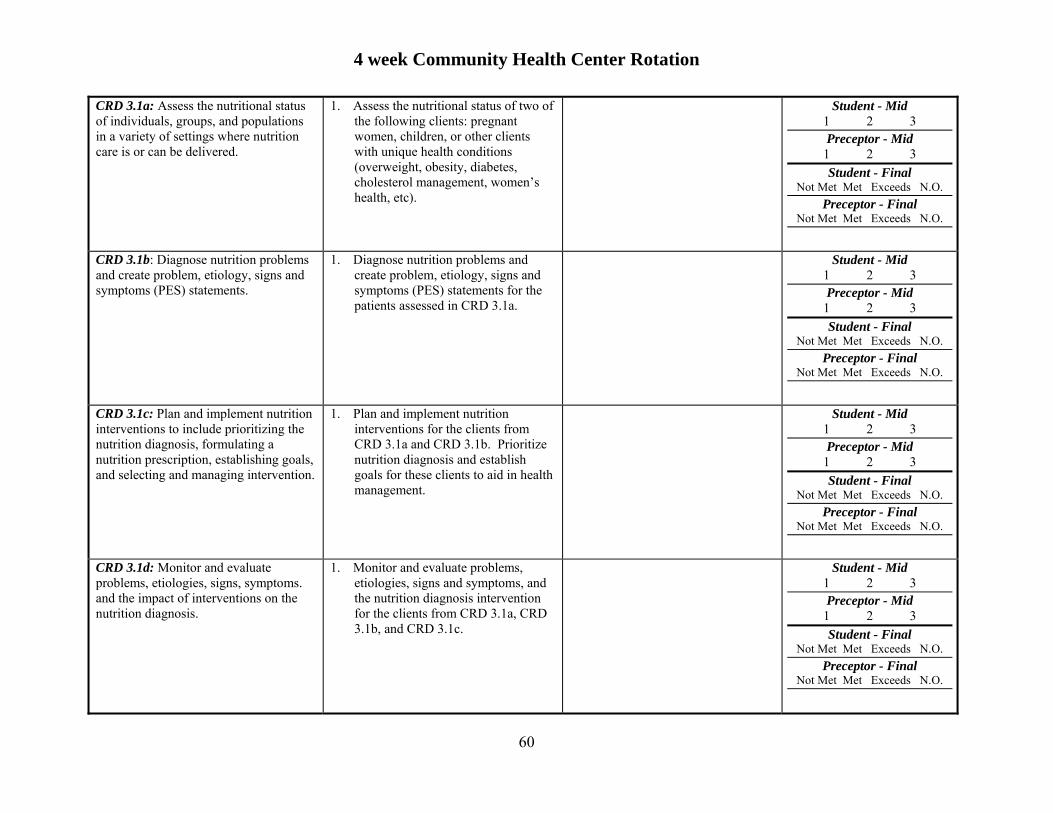
4 week Community Health Center Rotation
60
CRD 3.1a: Assess the nutritional status of individuals, groups, and populations in a variety of settings where nutrition care is or can be delivered.
1. Assess the nutritional status of two of the following clients: pregnant women, children, or other clients with unique health conditions (overweight, obesity, diabetes, cholesterol management, women’s health, etc).
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 3.1b: Diagnose nutrition problems and create problem, etiology, signs and symptoms (PES) statements.
1. Diagnose nutrition problems and create problem, etiology, signs and symptoms (PES) statements for the patients assessed in CRD 3.1a.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 3.1c: Plan and implement nutrition interventions to include prioritizing the nutrition diagnosis, formulating a nutrition prescription, establishing goals, and selecting and managing intervention.
1. Plan and implement nutrition interventions for the clients from CRD 3.1a and CRD 3.1b. Prioritize nutrition diagnosis and establish goals for these clients to aid in health management.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 3.1d: Monitor and evaluate problems, etiologies, signs, symptoms. and the impact of interventions on the nutrition diagnosis.
1. Monitor and evaluate problems, etiologies, signs and symptoms, and the nutrition diagnosis intervention for the clients from CRD 3.1a, CRD 3.1b, and CRD 3.1c.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.

4 week Community Health Center Rotation
61
CRD 3.1e: Complete documentation that follows professional guidelines, guidelines required by health care systems, and guidelines required by the practice setting.
1. Use the nutrition care process and follow HIPAA guidelines when documenting in medical records.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 3.2: Demonstrate effective communications skills for clinical and customer services in a variety of formats.
1. Develop a marketing plan for an upcoming nutrition workshop or lecture (i.e. brochures, flyers, posters, etc).
2. Use web-based or social media to communicate with patients/clients (only if the health center already has a platform for this).
3.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 3.3: Develop and deliver products, programs, or services that promote consumer health, wellness, and lifestyle management.
1. Develop a program (such as food day) that directly targets consumers.
2. Develop an employee wellness program or service.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 3.4: Deliver respectful, science-based answers to consumer questions concerning emerging trends.
1. Provide evidence-based answers to patient questions during a nutrition session.
2. Implement an “Ask the Dietitian” information booth in the lobby/waiting room of a CHC. Answer all consumer questions using science-based information and with consideration of emerging trends.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
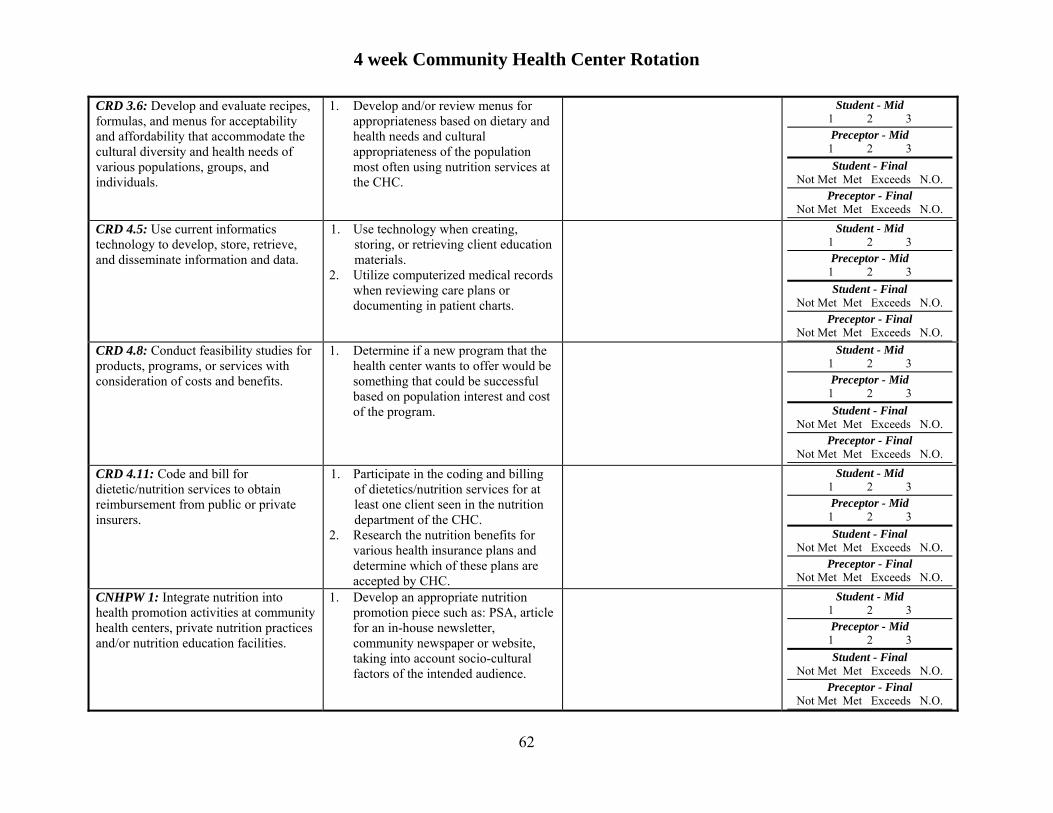
4 week Community Health Center Rotation
62
CRD 3.6: Develop and evaluate recipes, formulas, and menus for acceptability and affordability that accommodate the cultural diversity and health needs of various populations, groups, and individuals.
1. Develop and/or review menus for appropriateness based on dietary and health needs and cultural appropriateness of the population most often using nutrition services at the CHC.
Student - Mid 1 2 3 Preceptor - Mid 1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 4.5: Use current informatics technology to develop, store, retrieve, and disseminate information and data.
1. Use technology when creating, storing, or retrieving client education materials.
2. Utilize computerized medical records when reviewing care plans or documenting in patient charts.
Student - Mid 1 2 3 Preceptor - Mid 1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 4.8: Conduct feasibility studies for products, programs, or services with consideration of costs and benefits.
1. Determine if a new program that the health center wants to offer would be something that could be successful based on population interest and cost of the program.
Student - Mid 1 2 3 Preceptor - Mid 1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 4.11: Code and bill for dietetic/nutrition services to obtain reimbursement from public or private insurers.
1. Participate in the coding and billing of dietetics/nutrition services for at least one client seen in the nutrition department of the CHC.
2. Research the nutrition benefits for various health insurance plans and determine which of these plans are accepted by CHC.
Student - Mid 1 2 3 Preceptor - Mid 1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CNHPW 1: Integrate nutrition into health promotion activities at community health centers, private nutrition practices and/or nutrition education facilities.
1. Develop an appropriate nutrition promotion piece such as: PSA, article for an in-house newsletter, community newspaper or website, taking into account socio-cultural factors of the intended audience.
Student - Mid 1 2 3 Preceptor - Mid 1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
4 week Community Health Center Rotation
63
Additional Comments Regarding the Student’s Performance and Abilities:
Strengths Weaknesses
Preceptor Signature: Date:

64
SIMMONS COLLEGE DIETETIC INTERNSHIP PROGRAM Department of Public Health Rotation
Program Competencies and Planned Experiences
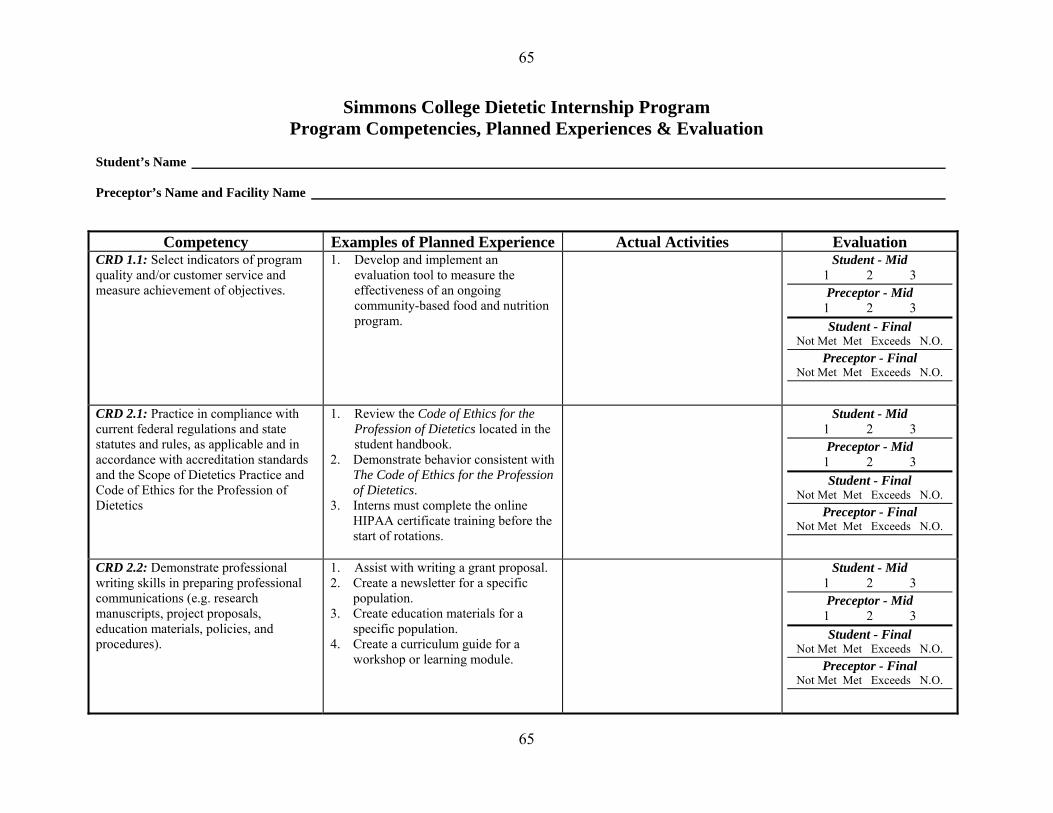
65
65
Simmons College Dietetic Internship Program Program Competencies, Planned Experiences & Evaluation
Student’s Name Preceptor’s Name and Facility Name
Competency Examples of Planned Experience Actual Activities Evaluation CRD 1.1: Select indicators of program quality and/or customer service and measure achievement of objectives.
1. Develop and implement an evaluation tool to measure the effectiveness of an ongoing community-based food and nutrition program.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 2.1: Practice in compliance with current federal regulations and state statutes and rules, as applicable and in accordance with accreditation standards and the Scope of Dietetics Practice and Code of Ethics for the Profession of Dietetics
1. Review the Code of Ethics for the Profession of Dietetics located in the student handbook.
2. Demonstrate behavior consistent with The Code of Ethics for the Profession of Dietetics.
3. Interns must complete the online HIPAA certificate training before the start of rotations.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 2.2: Demonstrate professional writing skills in preparing professional communications (e.g. research manuscripts, project proposals, education materials, policies, and procedures).
1. Assist with writing a grant proposal. 2. Create a newsletter for a specific
population. 3. Create education materials for a
specific population. 4. Create a curriculum guide for a
workshop or learning module.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
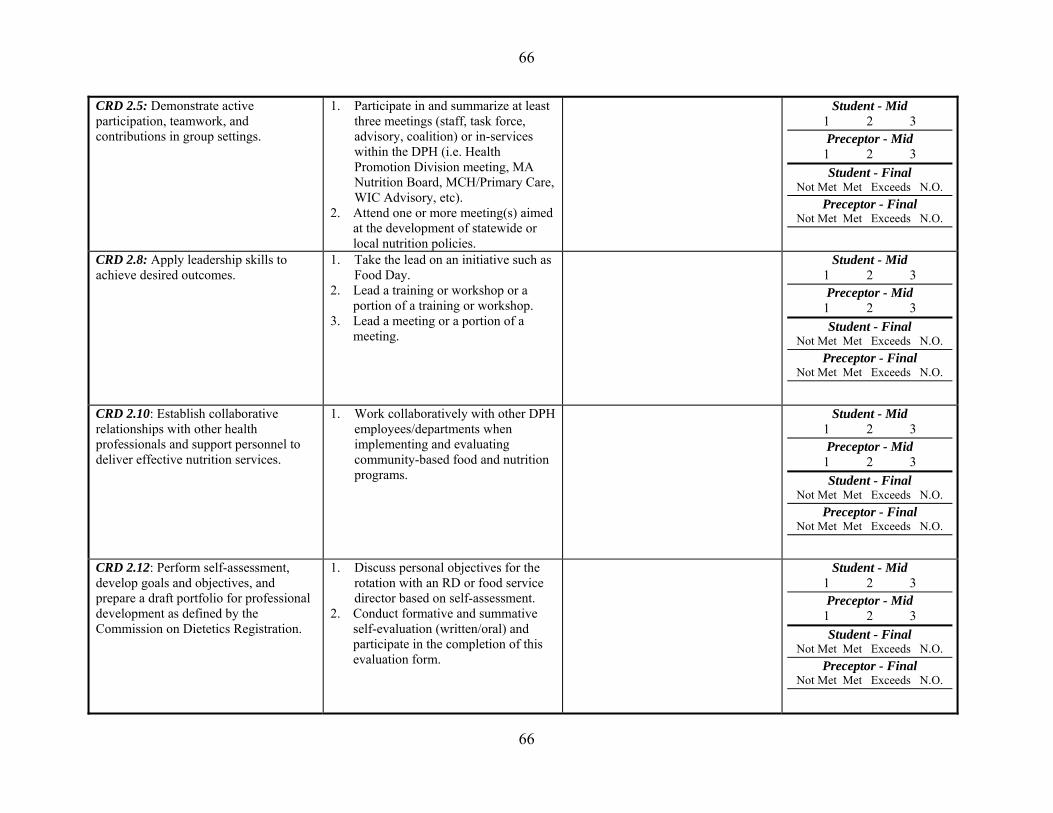
66
66
CRD 2.5: Demonstrate active participation, teamwork, and contributions in group settings.
1. Participate in and summarize at least three meetings (staff, task force, advisory, coalition) or in-services within the DPH (i.e. Health Promotion Division meeting, MA Nutrition Board, MCH/Primary Care, WIC Advisory, etc).
2. Attend one or more meeting(s) aimed at the development of statewide or local nutrition policies.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 2.8: Apply leadership skills to achieve desired outcomes.
1. Take the lead on an initiative such as Food Day.
2. Lead a training or workshop or a portion of a training or workshop.
3. Lead a meeting or a portion of a meeting.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 2.10: Establish collaborative relationships with other health professionals and support personnel to deliver effective nutrition services.
1. Work collaboratively with other DPH employees/departments when implementing and evaluating community-based food and nutrition programs.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 2.12: Perform self-assessment, develop goals and objectives, and prepare a draft portfolio for professional development as defined by the Commission on Dietetics Registration.
1. Discuss personal objectives for the rotation with an RD or food service director based on self-assessment.
2. Conduct formative and summative self-evaluation (written/oral) and participate in the completion of this evaluation form.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.

67
67
CRD 3.2: Demonstrate effective communications skills for clinical and customer services in a variety of formats.
1. Demonstrate effective communication skills when conferring with providers of nutrition services in federal, state, or community-based programs.
2. Demonstrate effective communication skills when performing activities related to a new or ongoing health promotion/disease prevention program for the DPH.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 3.3: Develop and deliver products, programs, or services that promote consumer health, wellness, and lifestyle management.
1. Develop a program (such as food day) that directly targets consumers.
2. Develop an employee wellness program or service.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 3.6: Develop and evaluate recipes, formulas and menus for acceptability and affordability that accommodate the cultural diversity and health needs of various populations, groups, and individuals.
1. Assist with creating and analyzing recipes for an education program or handout.
2. Assist with the development of a cookbook.
3. Assist with menu development for a site.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 4.3: Participate in public policy activities, including both legislative and regulatory initiatives.
1. Participate in the activities associated with a nutrition-related bill, write testimony, and/or attend and report on a legislative hearing.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
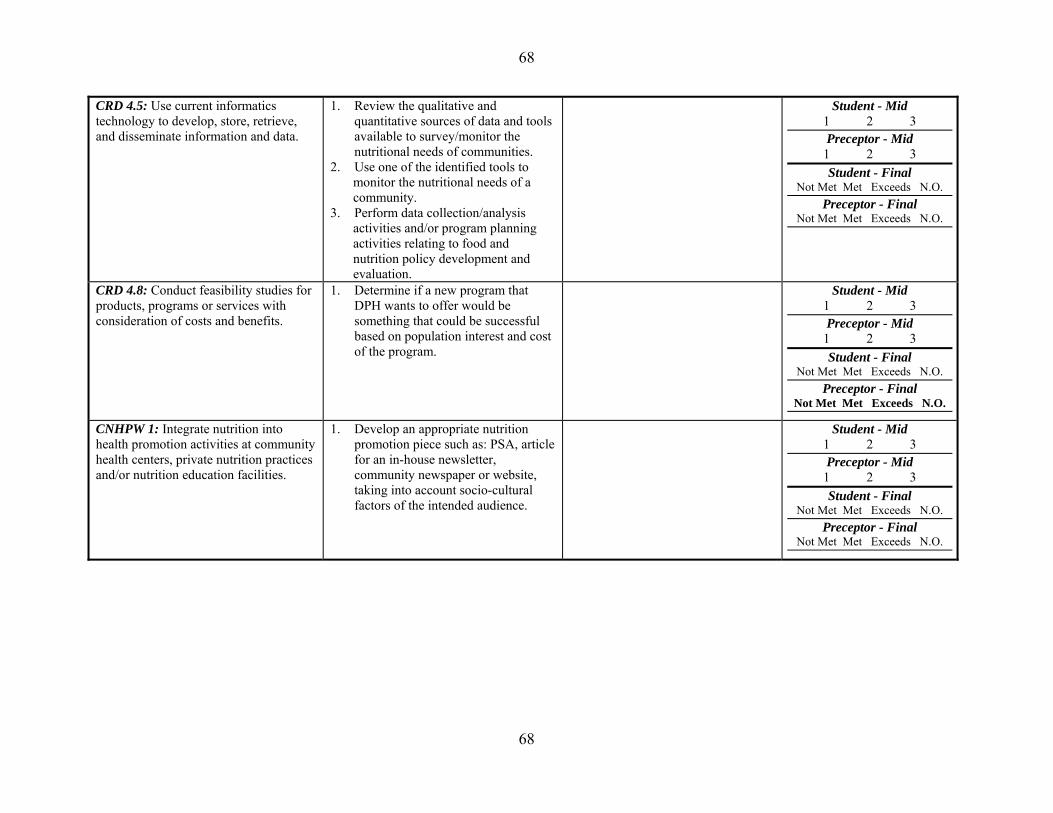
68
68
CRD 4.5: Use current informatics technology to develop, store, retrieve, and disseminate information and data.
1. Review the qualitative and quantitative sources of data and tools available to survey/monitor the nutritional needs of communities.
2. Use one of the identified tools to monitor the nutritional needs of a community.
3. Perform data collection/analysis activities and/or program planning activities relating to food and nutrition policy development and evaluation.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 4.8: Conduct feasibility studies for products, programs or services with consideration of costs and benefits.
1. Determine if a new program that DPH wants to offer would be something that could be successful based on population interest and cost of the program.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CNHPW 1: Integrate nutrition into health promotion activities at community health centers, private nutrition practices and/or nutrition education facilities.
1. Develop an appropriate nutrition promotion piece such as: PSA, article for an in-house newsletter, community newspaper or website, taking into account socio-cultural factors of the intended audience.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.

69
69
Additional Comments Regarding the Student’s Performance and Abilities:
Strengths Weaknesses
Preceptor Signature: Date:

70
70
SIMMONS COLLEGE DIETETIC INTERNSHIP PROGRAM
State Government-Based Nutrition Initiative Rotation Program Competencies and Planned Experiences

4 week State Government-Based Nutrition Initiative Rotation
71
Simmons College Dietetic Internship Program Program Competencies, Planned Experiences & Evaluation
Student’s Name Preceptor’s Name and Facility Name
Competency Examples of Planned Experience Actual Activities Evaluation CRD 1.1: Select indicators of program quality and/or customer service and measure achievement of objectives.
1. Complete a plate waste assessment at congregate meal site.
2. Oversee the development and implementation of a survey to analyze the effectiveness of nutrition service/practice in a community setting.
3. Based on the survey results, make recommendations for changes in the provision of nutritional care/service.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 2.1: Practice in compliance with current federal regulations and state statutes and rules, as applicable and in accordance with accreditation standards and the Scope of Dietetic Practice and Code of Ethics for the Profession of Dietetics.
1. Review the Code of Ethics for the Profession of Dietetics located in the student handbook.
2. Demonstrate behavior consistent with The Code of Ethics for the Profession of Dietetics.
3. Interns must complete the online HIPAA certificate training before the start of rotations.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 2.2: Demonstrate professional writing skills in preparing professional communications (e.g. research manuscripts, project proposals, educations materials, policies, and procedures).
1. Develop a nutrition education lesson plan to be used in the government-based nutrition program to which you have been assigned.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
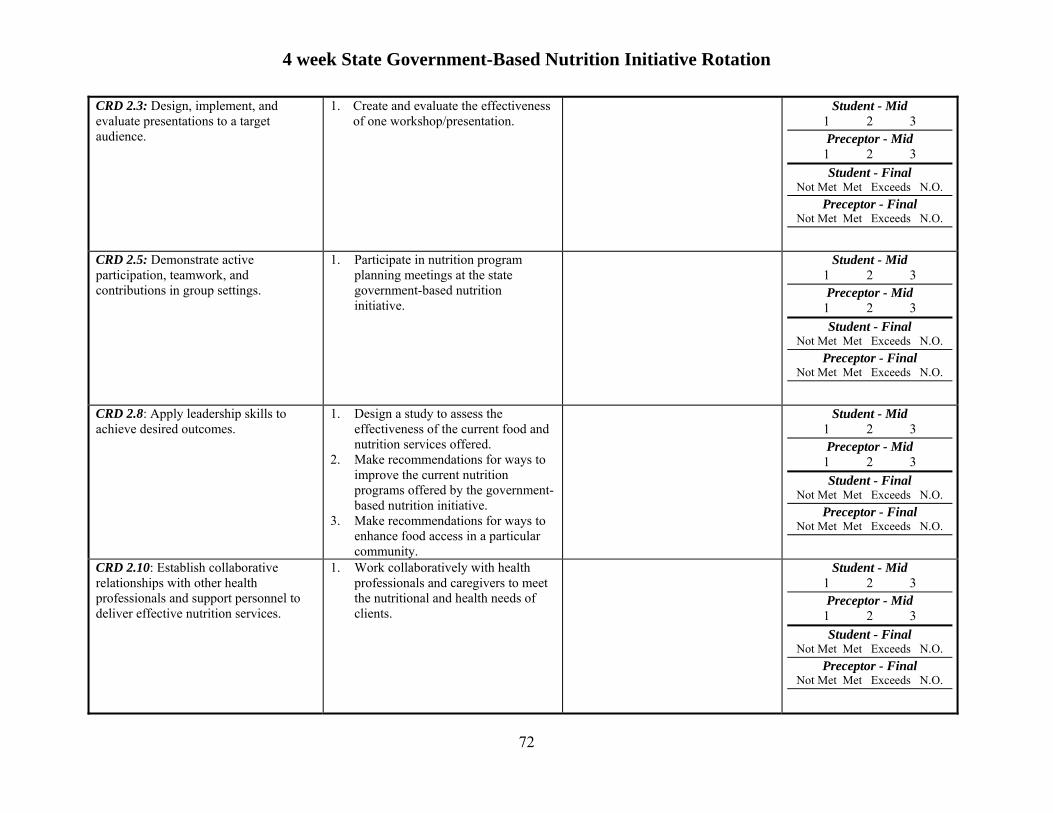
4 week State Government-Based Nutrition Initiative Rotation
72
CRD 2.3: Design, implement, and evaluate presentations to a target audience.
1. Create and evaluate the effectiveness of one workshop/presentation.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 2.5: Demonstrate active participation, teamwork, and contributions in group settings.
1. Participate in nutrition program planning meetings at the state government-based nutrition initiative.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 2.8: Apply leadership skills to achieve desired outcomes.
1. Design a study to assess the effectiveness of the current food and nutrition services offered.
2. Make recommendations for ways to improve the current nutrition programs offered by the government-based nutrition initiative.
3. Make recommendations for ways to enhance food access in a particular community.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 2.10: Establish collaborative relationships with other health professionals and support personnel to deliver effective nutrition services.
1. Work collaboratively with health professionals and caregivers to meet the nutritional and health needs of clients.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.

4 week State Government-Based Nutrition Initiative Rotation
73
Demonstrate professional attributes within organizational cultures (Tip: Professional attributes include showing initiative and proactively developing solutions, advocacy, customer focus, risk taking, critical thinking, flexibility, time management, work prioritization and work ethic)
1. Participate in educating local government agencies and pertinent professionals on the policies and procedures for new or existing nutrition programs.
2. Manage a project demonstrating good ability to prioritize needs and time management.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 2.12: Perform self-assessment, develop goals and objectives, and prepare a draft portfolio for professional development as defined by the Commission on Dietetics Registration.
1. Discuss personal objectives for the rotation with an RD or food service director based on self-assessment.
2. Conduct formative and summative self-evaluation (written/oral) and participate in the completion of this evaluation form.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 3.2: Demonstrate effective communication skills for clinical and customer services in a variety of formats. Examples include communication skills using oral, print, visual, electronic, and mass media methods for maximizing client education, employee training, and marketing.
1. Demonstrate effective communication skills when providing nutrition education to a group of individuals receiving services from the state based nutrition initiative program.
2. Demonstrate effective communication skills when in-servicing a case manager, non-registered dietitian, or other professional.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
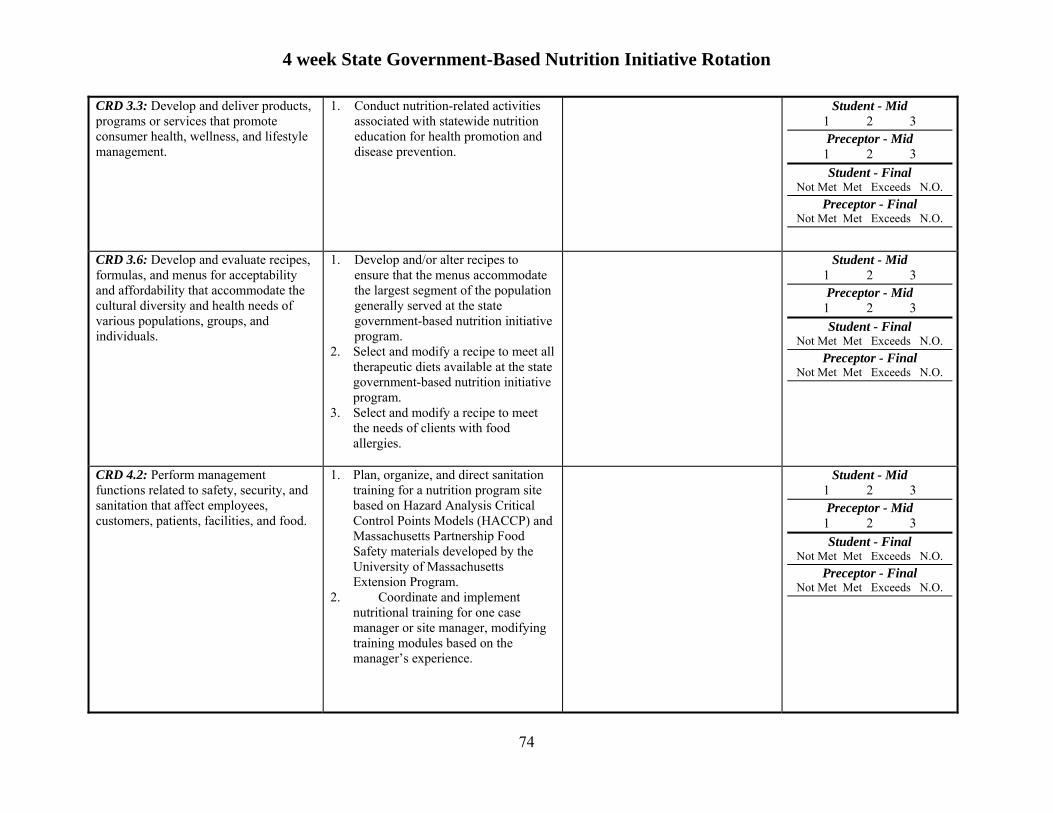
4 week State Government-Based Nutrition Initiative Rotation
74
CRD 3.3: Develop and deliver products, programs or services that promote consumer health, wellness, and lifestyle management.
1. Conduct nutrition-related activities associated with statewide nutrition education for health promotion and disease prevention.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 3.6: Develop and evaluate recipes, formulas, and menus for acceptability and affordability that accommodate the cultural diversity and health needs of various populations, groups, and individuals.
1. Develop and/or alter recipes to ensure that the menus accommodate the largest segment of the population generally served at the state government-based nutrition initiative program.
2. Select and modify a recipe to meet all therapeutic diets available at the state government-based nutrition initiative program.
3. Select and modify a recipe to meet the needs of clients with food allergies.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 4.2: Perform management functions related to safety, security, and sanitation that affect employees, customers, patients, facilities, and food.
1. Plan, organize, and direct sanitation training for a nutrition program site based on Hazard Analysis Critical Control Points Models (HACCP) and Massachusetts Partnership Food Safety materials developed by the University of Massachusetts Extension Program.
2. Coordinate and implement nutritional training for one case manager or site manager, modifying training modules based on the manager’s experience.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
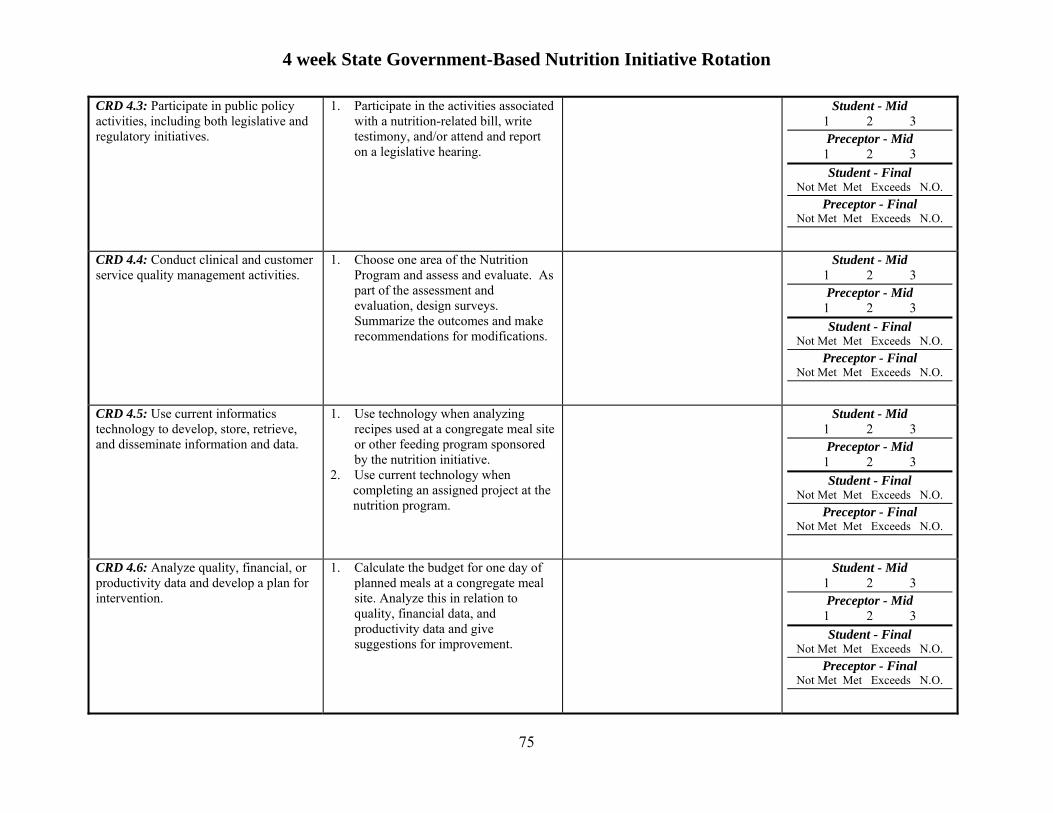
4 week State Government-Based Nutrition Initiative Rotation
75
CRD 4.3: Participate in public policy activities, including both legislative and regulatory initiatives.
1. Participate in the activities associated with a nutrition-related bill, write testimony, and/or attend and report on a legislative hearing.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 4.4: Conduct clinical and customer service quality management activities.
1. Choose one area of the Nutrition Program and assess and evaluate. As part of the assessment and evaluation, design surveys. Summarize the outcomes and make recommendations for modifications.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 4.5: Use current informatics technology to develop, store, retrieve, and disseminate information and data.
1. Use technology when analyzing recipes used at a congregate meal site or other feeding program sponsored by the nutrition initiative.
2. Use current technology when completing an assigned project at the nutrition program.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 4.6: Analyze quality, financial, or productivity data and develop a plan for intervention.
1. Calculate the budget for one day of planned meals at a congregate meal site. Analyze this in relation to quality, financial data, and productivity data and give suggestions for improvement.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
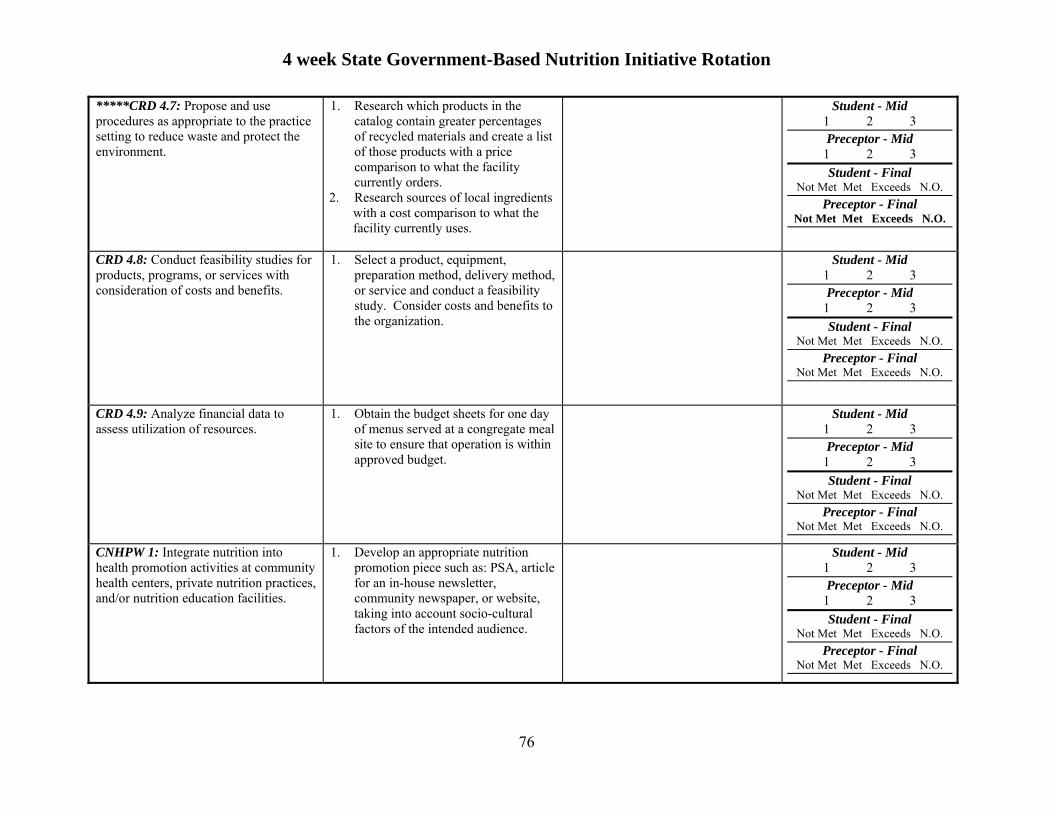
4 week State Government-Based Nutrition Initiative Rotation
76
*****CRD 4.7: Propose and use procedures as appropriate to the practice setting to reduce waste and protect the environment.
1. Research which products in the catalog contain greater percentages of recycled materials and create a list of those products with a price comparison to what the facility currently orders.
2. Research sources of local ingredients with a cost comparison to what the facility currently uses.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 4.8: Conduct feasibility studies for products, programs, or services with consideration of costs and benefits.
1. Select a product, equipment, preparation method, delivery method, or service and conduct a feasibility study. Consider costs and benefits to the organization.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 4.9: Analyze financial data to assess utilization of resources.
1. Obtain the budget sheets for one day of menus served at a congregate meal site to ensure that operation is within approved budget.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CNHPW 1: Integrate nutrition into health promotion activities at community health centers, private nutrition practices, and/or nutrition education facilities.
1. Develop an appropriate nutrition promotion piece such as: PSA, article for an in-house newsletter, community newspaper, or website, taking into account socio-cultural factors of the intended audience.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
4 week State Government-Based Nutrition Initiative Rotation
77
Additional Comments Regarding the Student’s Performance and Abilities:
Strengths Weaknesses
Preceptor Signature: Date:

78
SIMMONS COLLEGE DIETETIC INTERNSHIP PROGRAM
Counseling and Education Rotation Program Competencies and Planned Experiences

4 week Counseling and Education Rotation
*****=These competencies take priority as they have the best chance of being met in this rotation. Revised 4/2010 79
Simmons College Dietetic Internship Program Program Competencies, Planned Experiences and Evaluation
Student’s Name Preceptor’s Name and Facility Name
Competency Examples of Planned Experience Actual Activities Evaluation CRD 1.3: Justify programs, products, services, and care using appropriate evidence or data.
1. Assist with billing clients for insurance reimbursement.
2. Justify patients seen in relation to reimbursement request.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 2.1: Practice in compliance with current federal regulations and state statutes and rules, as applicable and in accordance with accreditation standards and the Scope of Dietetics Practice and Code of Ethics for the Profession of Dietetics.
1. Review the Code of Ethics for the Profession of Dietetics located in the student handbook.
2. Demonstrate behavior consistent with The Code of Ethics for the Profession of Dietetics.
3. Interns must complete the online HIPAA certificate training before the start of rotations.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 2.2: Demonstrate professional writing skills in preparing professional communications (e.g. research manuscripts, project proposals, education materials, policies and procedures).
1. Create a newsletter or press release to promote an event.
2. Develop nutrition education materials on an assigned topic or topic of interest.
3. Create a promotion campaign for a program or event.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
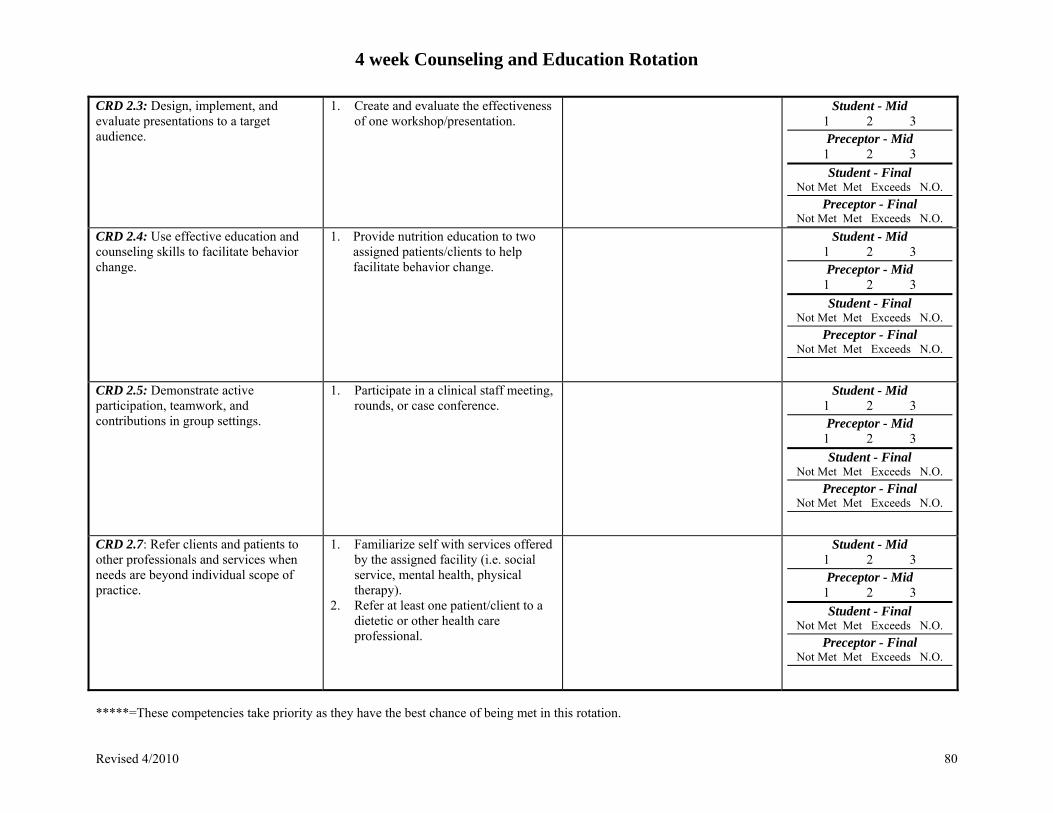
4 week Counseling and Education Rotation
*****=These competencies take priority as they have the best chance of being met in this rotation. Revised 4/2010 80
CRD 2.3: Design, implement, and evaluate presentations to a target audience.
1. Create and evaluate the effectiveness of one workshop/presentation.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 2.4: Use effective education and counseling skills to facilitate behavior change.
1. Provide nutrition education to two assigned patients/clients to help facilitate behavior change.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 2.5: Demonstrate active participation, teamwork, and contributions in group settings.
1. Participate in a clinical staff meeting, rounds, or case conference.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 2.7: Refer clients and patients to other professionals and services when needs are beyond individual scope of practice.
1. Familiarize self with services offered by the assigned facility (i.e. social service, mental health, physical therapy).
2. Refer at least one patient/client to a dietetic or other health care professional.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.

4 week Counseling and Education Rotation
*****=These competencies take priority as they have the best chance of being met in this rotation. Revised 4/2010 81
CRD 2.8: Apply leadership skills to achieve desired outcomes.
1. Lead a group training/workshop either for employees or clients promoting specific behavior change.
2. Take lead of a small project or workshop sponsored by the site.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 2.10: Establish collaborative relationships with other health professionals and support personnel to deliver effective nutrition services.
1. Work collaboratively with health professionals and caregivers to meet the nutritional and health needs of clients.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 2.12: Perform self-assessment, develop goals and objectives, and prepare a draft portfolio for professional development as defined by the Commission on Dietetics Registration.
1. Discuss personal objectives for the rotation with an RD or food service director based on self-assessment.
2. Conduct formative and summative self-evaluation (written/oral) and participate in the completion of this evaluation form.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 2.13: Demonstrate negotiation skills and assertiveness when needed while respecting life experiences, cultural diversity, and educational background.
1. Demonstrate assertiveness when making dietary recommendations to healthcare professionals from other disciplines.
2. Consider cultural diversity and socioeconomic status of clients when making dietary recommendations.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
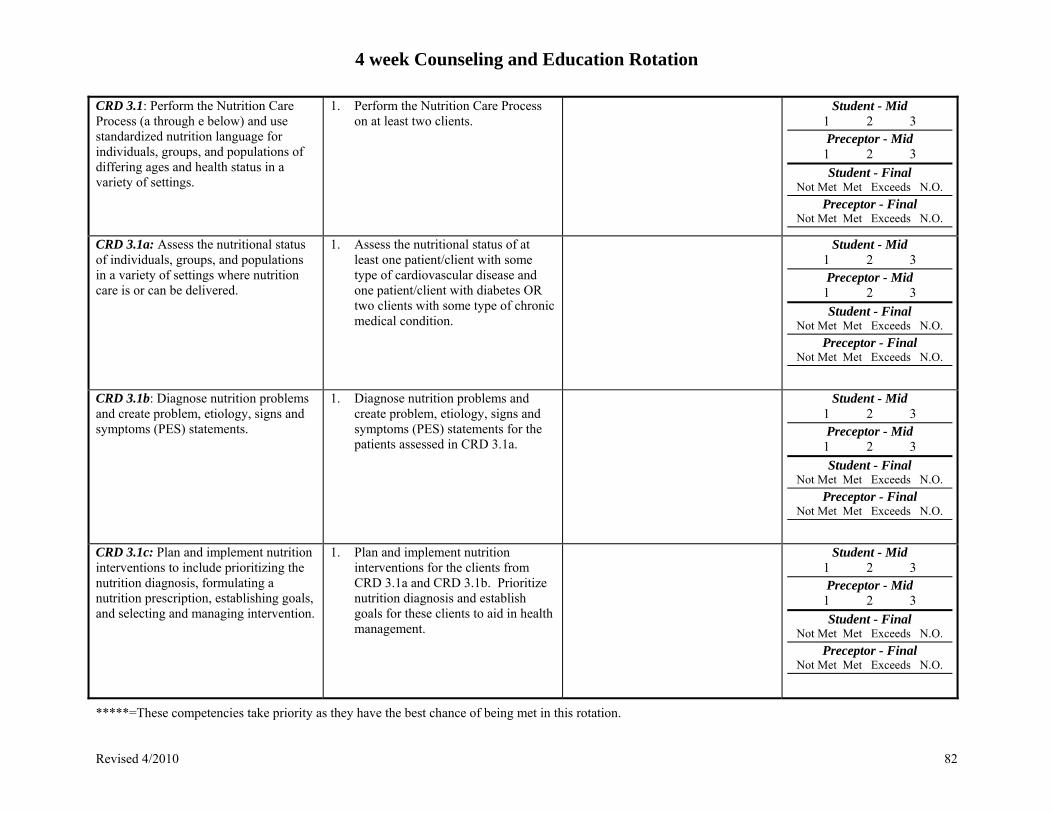
4 week Counseling and Education Rotation
*****=These competencies take priority as they have the best chance of being met in this rotation. Revised 4/2010 82
CRD 3.1: Perform the Nutrition Care Process (a through e below) and use standardized nutrition language for individuals, groups, and populations of differing ages and health status in a variety of settings.
1. Perform the Nutrition Care Process on at least two clients.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 3.1a: Assess the nutritional status of individuals, groups, and populations in a variety of settings where nutrition care is or can be delivered.
1. Assess the nutritional status of at least one patient/client with some type of cardiovascular disease and one patient/client with diabetes OR two clients with some type of chronic medical condition.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 3.1b: Diagnose nutrition problems and create problem, etiology, signs and symptoms (PES) statements.
1. Diagnose nutrition problems and create problem, etiology, signs and symptoms (PES) statements for the patients assessed in CRD 3.1a.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 3.1c: Plan and implement nutrition interventions to include prioritizing the nutrition diagnosis, formulating a nutrition prescription, establishing goals, and selecting and managing intervention.
1. Plan and implement nutrition interventions for the clients from CRD 3.1a and CRD 3.1b. Prioritize nutrition diagnosis and establish goals for these clients to aid in health management.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
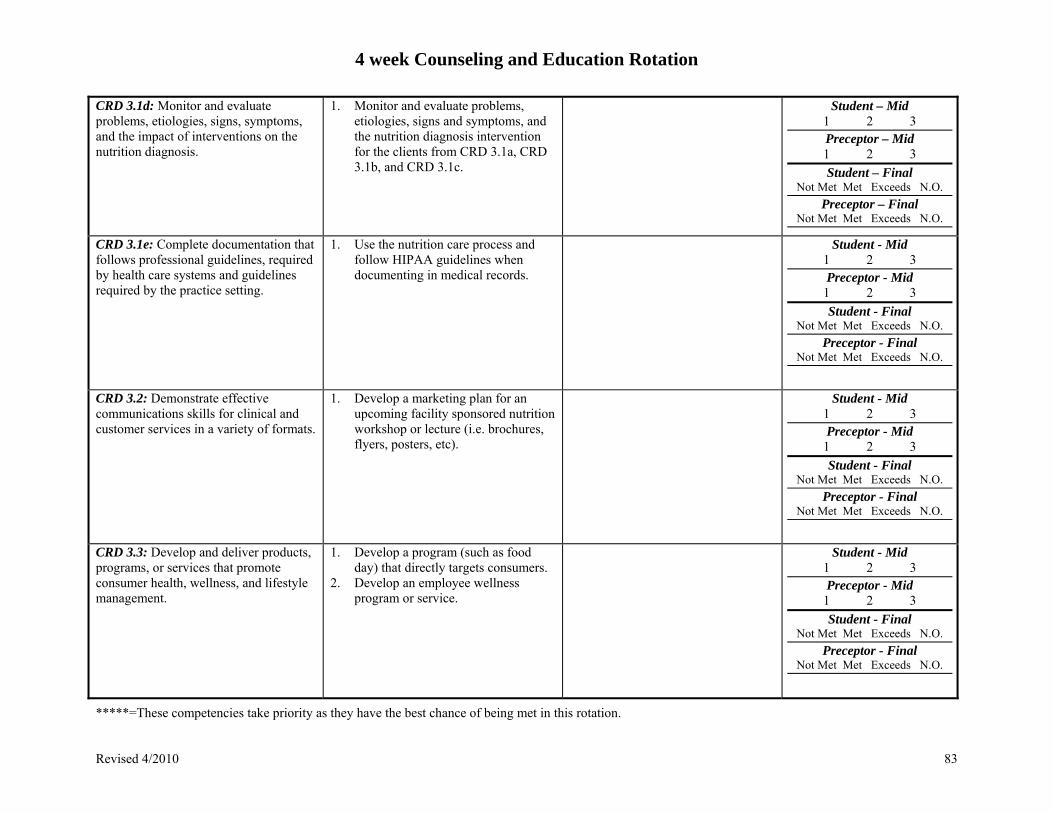
4 week Counseling and Education Rotation
*****=These competencies take priority as they have the best chance of being met in this rotation. Revised 4/2010 83
CRD 3.1d: Monitor and evaluate problems, etiologies, signs, symptoms, and the impact of interventions on the nutrition diagnosis.
1. Monitor and evaluate problems, etiologies, signs and symptoms, and the nutrition diagnosis intervention for the clients from CRD 3.1a, CRD 3.1b, and CRD 3.1c.
Student – Mid 1 2 3
Preceptor – Mid
1 2 3
Student – Final Not Met Met Exceeds N.O.
Preceptor – Final Not Met Met Exceeds N.O.
CRD 3.1e: Complete documentation that follows professional guidelines, required by health care systems and guidelines required by the practice setting.
1. Use the nutrition care process and follow HIPAA guidelines when documenting in medical records.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 3.2: Demonstrate effective communications skills for clinical and customer services in a variety of formats.
1. Develop a marketing plan for an upcoming facility sponsored nutrition workshop or lecture (i.e. brochures, flyers, posters, etc).
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 3.3: Develop and deliver products, programs, or services that promote consumer health, wellness, and lifestyle management.
1. Develop a program (such as food day) that directly targets consumers.
2. Develop an employee wellness program or service.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
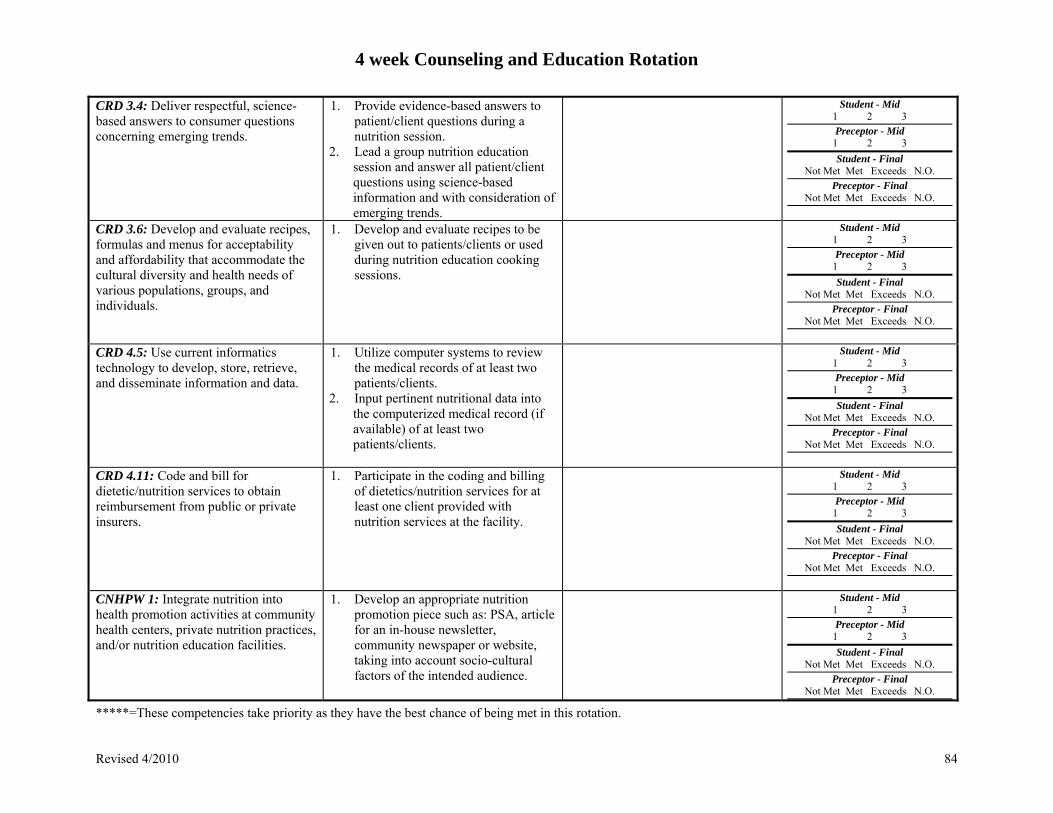
4 week Counseling and Education Rotation
*****=These competencies take priority as they have the best chance of being met in this rotation. Revised 4/2010 84
CRD 3.4: Deliver respectful, science-based answers to consumer questions concerning emerging trends.
1. Provide evidence-based answers to patient/client questions during a nutrition session.
2. Lead a group nutrition education session and answer all patient/client questions using science-based information and with consideration of emerging trends.
Student - Mid 1 2 3
Preceptor - Mid 1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 3.6: Develop and evaluate recipes, formulas and menus for acceptability and affordability that accommodate the cultural diversity and health needs of various populations, groups, and individuals.
1. Develop and evaluate recipes to be given out to patients/clients or used during nutrition education cooking sessions.
Student - Mid 1 2 3
Preceptor - Mid 1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 4.5: Use current informatics technology to develop, store, retrieve, and disseminate information and data.
1. Utilize computer systems to review the medical records of at least two patients/clients.
2. Input pertinent nutritional data into the computerized medical record (if available) of at least two patients/clients.
Student - Mid 1 2 3 Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 4.11: Code and bill for dietetic/nutrition services to obtain reimbursement from public or private insurers.
1. Participate in the coding and billing of dietetics/nutrition services for at least one client provided with nutrition services at the facility.
Student - Mid 1 2 3
Preceptor - Mid 1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CNHPW 1: Integrate nutrition into health promotion activities at community health centers, private nutrition practices, and/or nutrition education facilities.
1. Develop an appropriate nutrition promotion piece such as: PSA, article for an in-house newsletter, community newspaper or website, taking into account socio-cultural factors of the intended audience.
Student - Mid 1 2 3
Preceptor - Mid 1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
4 week Counseling and Education Rotation
*****=These competencies take priority as they have the best chance of being met in this rotation. Revised 4/2010 85
Additional Comments Regarding the Student’s Performance and Abilities:
Strengths Weaknesses
Preceptor Signature: Date:

86
SIMMONS COLLEGE DIETETIC INTERNSHIP PROGRAM
Food Service Rotation Program Competencies and Planned Experiences
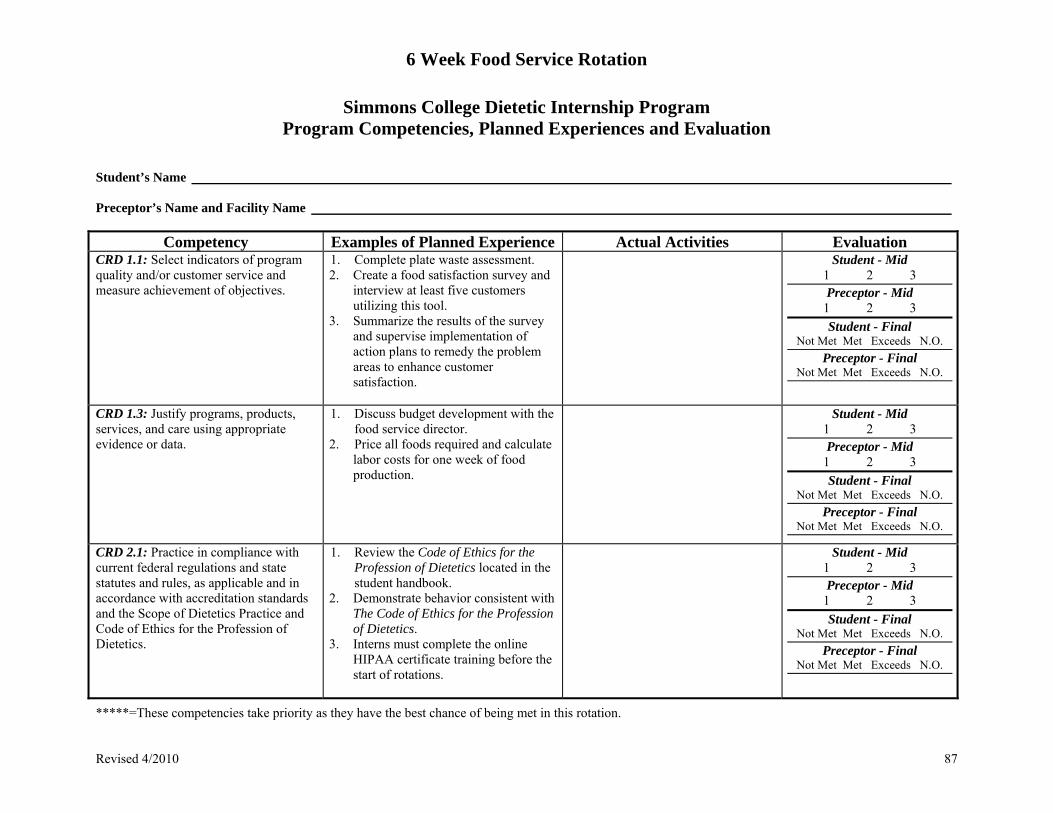
6 Week Food Service Rotation
*****=These competencies take priority as they have the best chance of being met in this rotation. Revised 4/2010 87
Simmons College Dietetic Internship Program Program Competencies, Planned Experiences and Evaluation
Student’s Name Preceptor’s Name and Facility Name
Competency Examples of Planned Experience Actual Activities Evaluation CRD 1.1: Select indicators of program quality and/or customer service and measure achievement of objectives.
1. Complete plate waste assessment. 2. Create a food satisfaction survey and
interview at least five customers utilizing this tool.
3. Summarize the results of the survey and supervise implementation of action plans to remedy the problem areas to enhance customer satisfaction.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 1.3: Justify programs, products, services, and care using appropriate evidence or data.
1. Discuss budget development with the food service director.
2. Price all foods required and calculate labor costs for one week of food production.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 2.1: Practice in compliance with current federal regulations and state statutes and rules, as applicable and in accordance with accreditation standards and the Scope of Dietetics Practice and Code of Ethics for the Profession of Dietetics.
1. Review the Code of Ethics for the Profession of Dietetics located in the student handbook.
2. Demonstrate behavior consistent with The Code of Ethics for the Profession of Dietetics.
3. Interns must complete the online HIPAA certificate training before the start of rotations.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.

6 Week Food Service Rotation
*****=These competencies take priority as they have the best chance of being met in this rotation. Revised 4/2010 88
CRD 2.2: Demonstrate professional writing skills in preparing professional communications (e.g. research manuscripts, project proposals, education materials, policies and procedures).
1. Develop a job description for one position in the food service department.
2. Write a policy about the dress code in the food service department.
3. Write a newsletter for the employees or clients/patients/residents highlighting important news about the food service program.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 2.5: Demonstrate active participation, teamwork and contributions in group settings.
Participate in one of the following: 1. Food service organizational meeting 2. Menu planning meeting 3. QA meeting discussing food/nutrition
related topics 4. Department staff meeting
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 2.6: Assign appropriate patient care activities to DTRs and/or support personnel as appropriate.
1. Assign appropriate employee to cover positions during employee illness, holidays, vacation, and family leave.
2. Assign employees to cover activities for special events based on employee skills and strengths.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 2.8: Apply leadership skills to achieve desired outcomes.
1. Plan and supervise the service of all meals for one meal in a food service facility.
2. Plan and supervise the service of food/meals for a special event or program.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.

6 Week Food Service Rotation
*****=These competencies take priority as they have the best chance of being met in this rotation. Revised 4/2010 89
CRD 2.10 Establish collaborative relationships with other health professionals and support personnel to deliver effective nutrition services.
1. Work collaboratively with customers (i.e. students, patients, employees) to meet the nutritional needs and preferences of customers.
2. Work with food service employees to ensure that meals are meeting needs of customers.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 2.11: Demonstrate professional attributes within various organizational cultures.
1. Demonstrate critical thinking, use of appropriate time management, and work priorities when planning, organizing, and directing the food service operation for a meal or a special program.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 2.12: Perform self-assessment, develop goals and objectives, and prepare a draft portfolio for professional development as defined by the Commission on Dietetics Registration.
1. Discuss personal objectives for the rotation with an RD or food service director based on self-assessment.
2. Conduct formative and summative self-evaluation (written/oral) and participate in the completion of this evaluation form.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 2.13: Demonstrate negotiation skills. (Tip: Demonstrating negotiating skills includes showing assertiveness when needed while respecting the life experiences, cultural diversity, and educational background of the other parties)
1. Negotiate with a vendor regarding a purchase or return.
2. Negotiate with a patient/client/resident to ensure that food provided meets their needs within the limitations of the food service operation.
3. Negotiate with other staff within the facility to solve a problem.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.

6 Week Food Service Rotation
*****=These competencies take priority as they have the best chance of being met in this rotation. Revised 4/2010 90
CRD 3.2: Demonstrate effective communications skills for clinical and customer services in a variety of formats. (Tip: Formats include oral, print, visual, electronic, and mass media methods for maximizing client education, employee training and marketing.)
1. Prepare, implement, and evaluate an employee in-service on an appropriate topic as determined by the dietetic intern and the food service manager.
2. Create a marketing campaign for a special feature of the food service operation (e.g. the salad bar) or for a special meal or program.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 3.3: Develop and deliver products, programs or services that promote consumer health, wellness and lifestyle management. (Tip: Students/interns should consider health messages and interventions that integrate the consumer’s desire for taste, convenience, and economy with the need for nutrition and food safety)
1. Prepare and implement a cost appropriate production plan for a day in a food service system including labor costs, employee needs, and energy.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 3.4: Deliver respectful, science-based answers to consumer questions concerning emerging trends.
1. Respond respectively to customer suggestion box comments.
2. Use science-based answers to reply to customer emails.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
*****CRD 3.5: Coordinate procurement, production, distribution and service of goods and services. (Tip: Students/interns should demonstrate and promote responsible use of resources including employees, money, time, water, energy, food, and disposable goods)
1. Oversee the procurement, distribution and service of food within a food service facility for a day.
2. Oversee the procurement, distribution and service of food within the facility for a special program or meal.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.

6 Week Food Service Rotation
*****=These competencies take priority as they have the best chance of being met in this rotation. Revised 4/2010 91
CRD 3.6: Develop and evaluate recipes, formulas and menus for acceptability and affordability that accommodate the cultural diversity and health needs of various populations, groups, and individuals.
1. Coordinate and direct menu planning meetings to ensure that the menus accommodate the largest segment of the population generally served at the food service facility.
2. Select and modify a recipe to meet all therapeutic diets available at the food service facility.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
*****CRD 4.1: Participate in management of human resources.
1. Assist in development of a performance-based employee evaluation.
2. Utilize the performance evaluation tool to assess two employees in a mock-type situation.
3. Using the institution’s employee evaluation assessment form, complete an evaluation on a selected employee (not actually given to the employee) to be discussed with the food service manager.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
****CRD 4.2: Perform management functions related to safety, security, and sanitation that affect employees, customers, patients, facilities, and food.
1. Oversee and coordinate a safety and sanitation inspection by the food service staff in accordance with local health regulations.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 4.4: Conduct clinical and customer service quality management activities.
1. Develop a sensory tool to evaluate foods prior to their distribution to customers.
2. Participate in a plate waste analysis.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
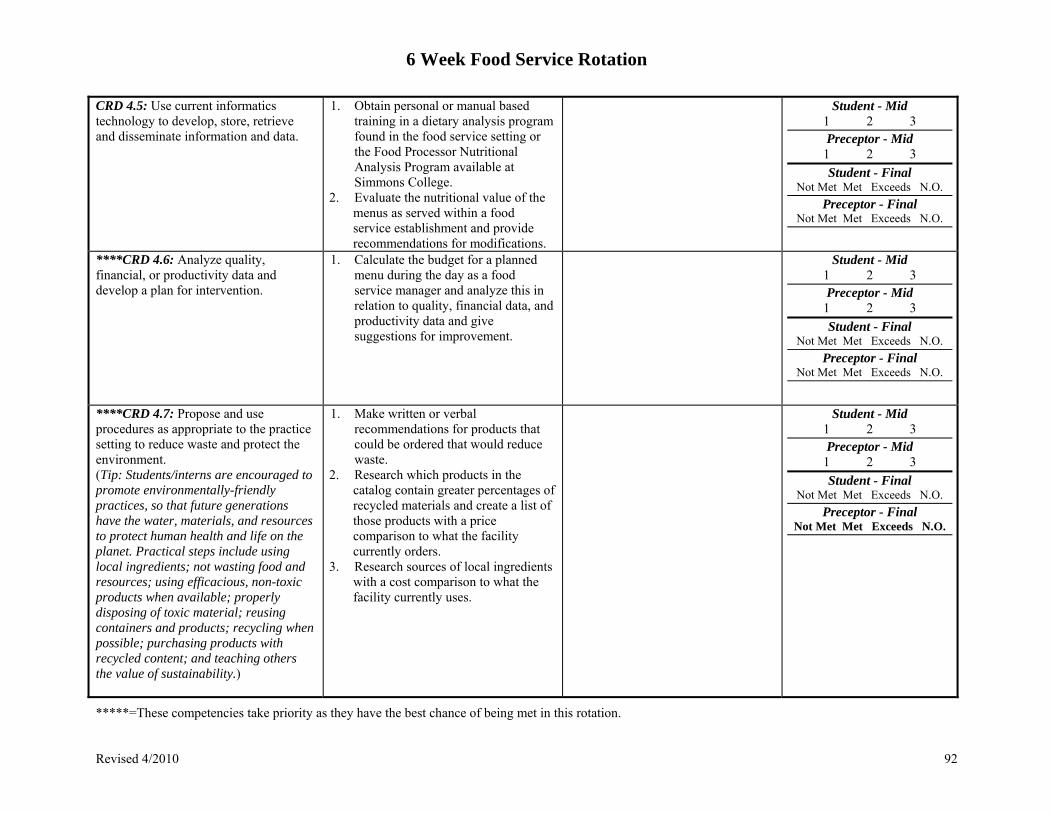
6 Week Food Service Rotation
*****=These competencies take priority as they have the best chance of being met in this rotation. Revised 4/2010 92
CRD 4.5: Use current informatics technology to develop, store, retrieve and disseminate information and data.
1. Obtain personal or manual based training in a dietary analysis program found in the food service setting or the Food Processor Nutritional Analysis Program available at Simmons College.
2. Evaluate the nutritional value of the menus as served within a food service establishment and provide recommendations for modifications.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
****CRD 4.6: Analyze quality, financial, or productivity data and develop a plan for intervention.
1. Calculate the budget for a planned menu during the day as a food service manager and analyze this in relation to quality, financial data, and productivity data and give suggestions for improvement.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
****CRD 4.7: Propose and use procedures as appropriate to the practice setting to reduce waste and protect the environment. (Tip: Students/interns are encouraged to promote environmentally-friendly practices, so that future generations have the water, materials, and resources to protect human health and life on the planet. Practical steps include using local ingredients; not wasting food and resources; using efficacious, non-toxic products when available; properly disposing of toxic material; reusing containers and products; recycling when possible; purchasing products with recycled content; and teaching others the value of sustainability.)
1. Make written or verbal recommendations for products that could be ordered that would reduce waste.
2. Research which products in the catalog contain greater percentages of recycled materials and create a list of those products with a price comparison to what the facility currently orders.
3. Research sources of local ingredients with a cost comparison to what the facility currently uses.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.

6 Week Food Service Rotation
*****=These competencies take priority as they have the best chance of being met in this rotation. Revised 4/2010 93
CRD 4.8: Conduct feasibility studies for products, programs, or services with consideration of the costs and benefits.
1. Select a product, equipment, preparation method, delivery method, or service and conduct a feasibility study. Consider costs and benefits to the organization.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CRD 4.9: Analyze financial data to assess utilization of resources.
1. Calculate the budget for a planned menu during the day as a food service manager to ensure that revenues are covering costs.
2. Obtain budget sheets to ensure that operation is within global parameters.
Student - Mid 1 2 3
Preceptor - Mid
1 2 3
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
6 Week Food Service Rotation
*****=These competencies take priority as they have the best chance of being met in this rotation. Revised 4/2010 94
Additional Comments Regarding the Student’s Performance and Abilities: Strengths Weaknesses
Preceptor Signature: Date:

95
SIMMONS COLLEGE DIETETIC INTERNSHIP PROGRAM
Research and Professional Practice Rotation Program Competencies and Planned Experiences

1 Week Professional Practice and Research Rotation
*****=These competencies take priority as they have the best chance of being met in this rotation. Revised 4/2010 96
Simmons College Dietetic Internship Program Program Competencies, Planned Experiences and Evaluation
1 week / Research and Professional Practice Rotation Student’s Name_______________________________________________________________________________________ Preceptor’s Name and Facility Name_____________________________________________________________________
Competency Examples of Planned Experience Actual Activities Evaluation* CNHPW1: Interns will integrate nutrition into health promotion and wellness activities at community health centers, private nutrition practices and/or nutrition education facilities.
1. Based on student’s interests, they can arrange additional experiences beyond the community health center rotation during this week.
2. Interns will plan their own goals and objectives to meet.
Student - Mid n/a
Preceptor - Mid
n/a
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CNHPW2: Interns will participate in waived point of care testing using glucose monitoring.
1. Demonstration of how to use glucose monitoring system during intern class meetings.
2. Develop plans of care for results obtained from glucose monitoring results.
Student - Mid n/a
Preceptor - Mid
n/a
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
CNHPW3: Interns will gain an appreciation and understanding of food insecurity.
1. Interns will read and discuss The Working Poor during orientation
2. The thrifty food plan assignment-students will plan diet for themselves and follow, using the thrifty food plan money allowance. Interns will analyze 3 days of their planned meals to make sure that they meet nutrient adequacy.
Student - Mid n/a
Preceptor - Mid
n/a
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
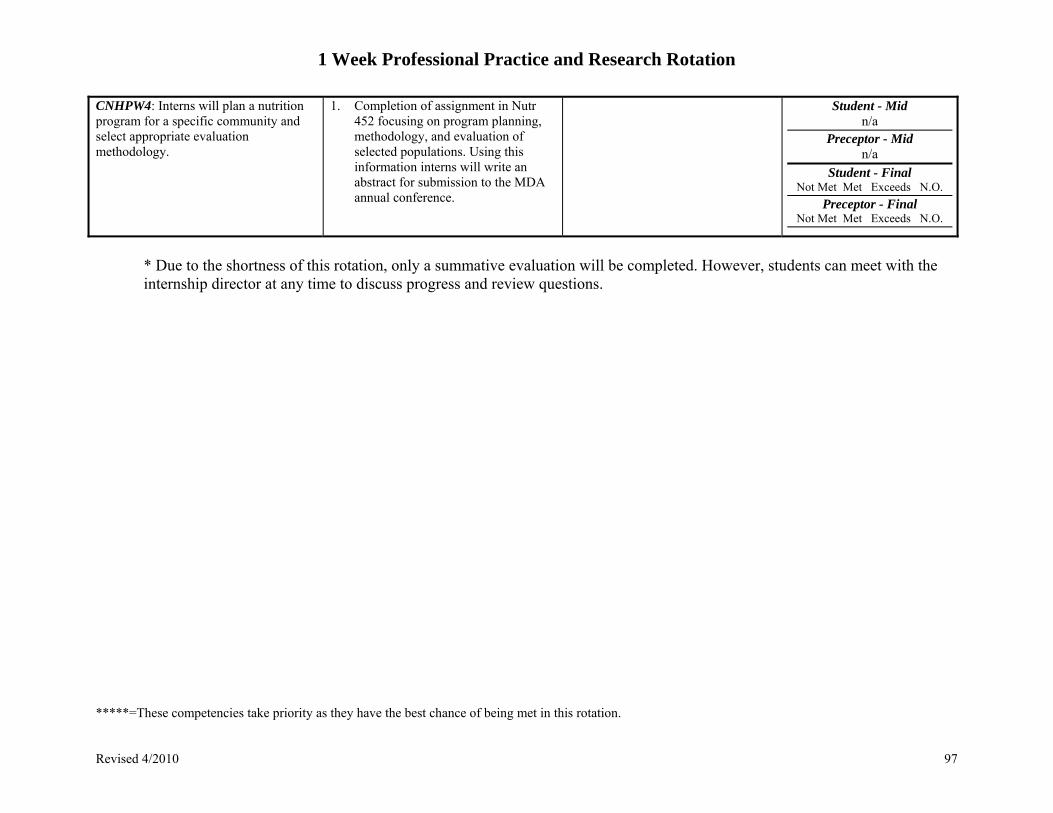
1 Week Professional Practice and Research Rotation
*****=These competencies take priority as they have the best chance of being met in this rotation. Revised 4/2010 97
CNHPW4: Interns will plan a nutrition program for a specific community and select appropriate evaluation methodology.
1. Completion of assignment in Nutr 452 focusing on program planning, methodology, and evaluation of selected populations. Using this information interns will write an abstract for submission to the MDA annual conference.
Student - Mid n/a
Preceptor - Mid
n/a
Student - Final Not Met Met Exceeds N.O.
Preceptor - Final Not Met Met Exceeds N.O.
* Due to the shortness of this rotation, only a summative evaluation will be completed. However, students can meet with the internship director at any time to discuss progress and review questions.
1 Week Professional Practice and Research Rotation
*****=These competencies take priority as they have the best chance of being met in this rotation. Revised 4/2010 98
Additional Comments Regarding the Student’s Performance and Abilities: Strengths Weaknesses
Preceptor Signature: Date:
99
Other Dietetic Internship Evaluation Forms: Student Evaluation of Internship Rotation
Student Evaluation of Joint Class Day

100
SIMMONS COLLEGE DIETETIC INTERNSHIP PROGRAM
Student Evaluation of Their Supervised Practice Experiences Student’s Evaluation of their Supervised Practice Experiences
Purpose After each of the six external rotations, students are asked to evaluate the pro’s and con’s of their rotation. This information is helpful for the sites sponsoring our students, and for the program director and coordinator of the Simmons College internship program so that they can make any necessary modifications in the program with the aim of providing a positive experience for all parties involved. We ask that you please be as constructive as possible.
Instructions Please complete this evaluation at the end of each of your clinical experiences. Some questions may not apply to your experience because of the type of rotation or the length of time you spent at the particular rotation. In these instances please use the not applicable (NA) response. We ask that you please share the completed evaluation with your clinical instructor(s) at the particular rotation before returning the evaluation to the Simmons College Dietetic Internship Program Director or Coordinator.
Student’s Name (please print) and Signature Preceptor’s Name (please print) and Signature Name of the Affiliating Site Dates of Clinical Education Experience

101
Student Evaluation of Their Supervised Practice Experiences 1. Initial Orientation to the Rotation/Facility o Were you provided with an orientation to the facility, staff and other important resources? Yes_______ No_______ Comments: o During orientation, did you and your preceptor(s) develop a general plan for your rotation? Yes_______ No_______
Comments: o After the orientation, did you, as well as your clinical instructors, have a clear understanding as to what was expected of you? Yes_______ No_______
Comments: o Do you have any suggestions for improving your orientation experience to better prepare you for the rotation?

102
2. Preceptor Assessment o How many dietitians did you work with? Please provide their names, title and credentials. 3. Other Staffing Experiences o Were you able to interact with individuals without registered dietitian status, including diet technicians, doctors, food service staff, physical therapists, nurses or speech therapists, for consultation, discussion, conferences, rounds, or lectures? Yes_______ No_______
Comments:
o How would you describe your experience with these individuals?
4. Supervision and Support Assessment o Do you feel you were provided with enough quality supervision and support to meet the pertinent competencies and to maximize the amount you learned from this rotation? Yes_______ No_______ Comments:
103
o Do you feel the learning experiences you were provided with were modified based on your previous experiences and level of knowledge?
Yes_______ No_______ Comments:
o After your preceptor(s) became familiar with your level of proficiency, were you given adequate opportunity to provide staff relief and feel like you were really wearing the shoes of your preceptor(s)? Yes_______ No_______
Comments:
5. Evaluation Sheets and Competency Assessment o Do you feel the evaluation sheets and competencies assigned to this rotation were realistic in the time frame and setting provided? Yes_______ No_______ Comments:

104
o Did you and your preceptor meet mid-way through your experience to evaluate your progress and make new goals for the remaining time at the rotation? Yes_______ No_______
Comments:
o How would you describe the final evaluation/comments of your performance? Did your preceptor(s) make your strengths and weaknesses clear throughout your rotation so there were no major surprises at the end?
6. Student Experience Assessment o Please list the various projects, presentations, in-service education programs or other nutrition-related programs that you contributed to during this rotation.

105
o Were these valuable experiences? Which would you like more experience with and which did you feel were unnecessary?
o How would you describe your workload during this rotation?
_______Too much _______Too little _______Just right
7. Rotation Strengths o Please list the strengths of this rotation. 8. Rotation Weaknesses o Please list the weaknesses of this rotation.

106
9. Assessment of Your Overall Experience o How would you best describe your overall experience at this rotation?
o Based on your past experience in clinical education, and your concept of the “ideal” clinical education experience, how would you rate your clinical education experience at this rotation on a scale of 1 (‘I did not learn as much as I would like’) to 5 (‘I learned a great deal and believe this was a very positive experience’).
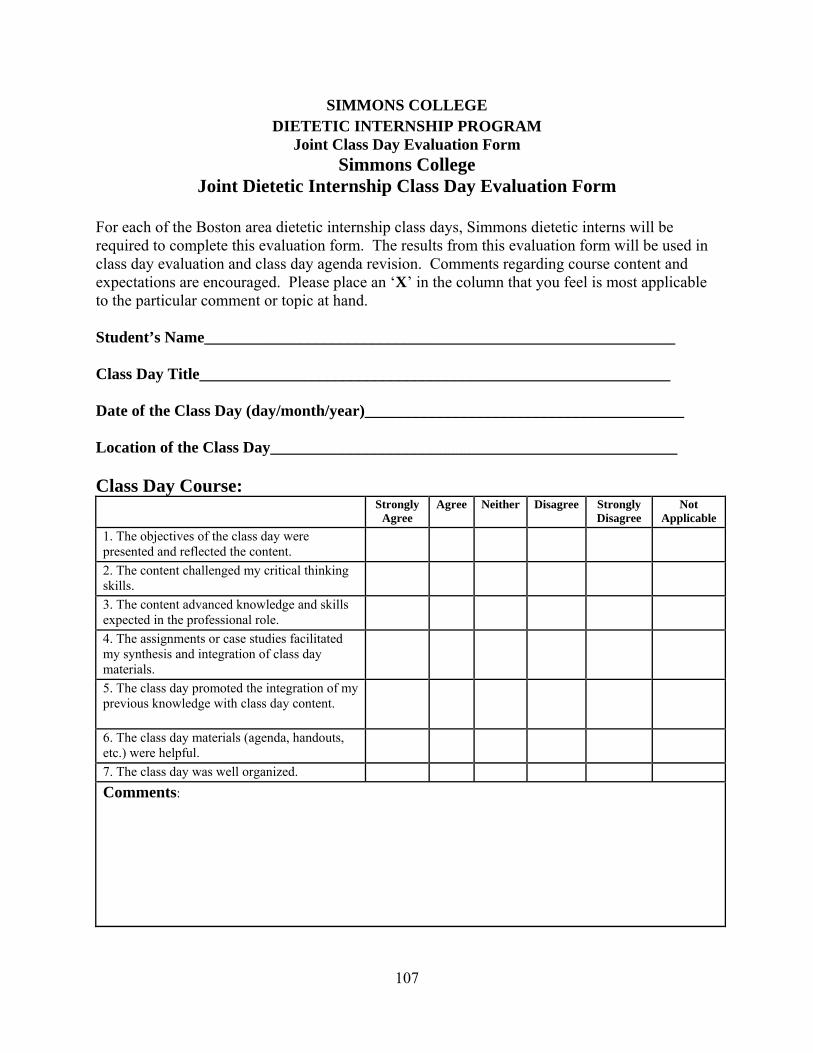
107
SIMMONS COLLEGE DIETETIC INTERNSHIP PROGRAM
Joint Class Day Evaluation Form Simmons College
Joint Dietetic Internship Class Day Evaluation Form
For each of the Boston area dietetic internship class days, Simmons dietetic interns will be required to complete this evaluation form. The results from this evaluation form will be used in class day evaluation and class day agenda revision. Comments regarding course content and expectations are encouraged. Please place an ‘X’ in the column that you feel is most applicable to the particular comment or topic at hand. Student’s Name___________________________________________________________ Class Day Title___________________________________________________________ Date of the Class Day (day/month/year)________________________________________ Location of the Class Day___________________________________________________ Class Day Course:
Strongly Agree
Agree Neither Disagree Strongly Disagree
Not Applicable
1. The objectives of the class day were presented and reflected the content.
2. The content challenged my critical thinking skills.
3. The content advanced knowledge and skills expected in the professional role.
4. The assignments or case studies facilitated my synthesis and integration of class day materials.
5. The class day promoted the integration of my previous knowledge with class day content.
6. The class day materials (agenda, handouts, etc.) were helpful.
7. The class day was well organized.
Comments:
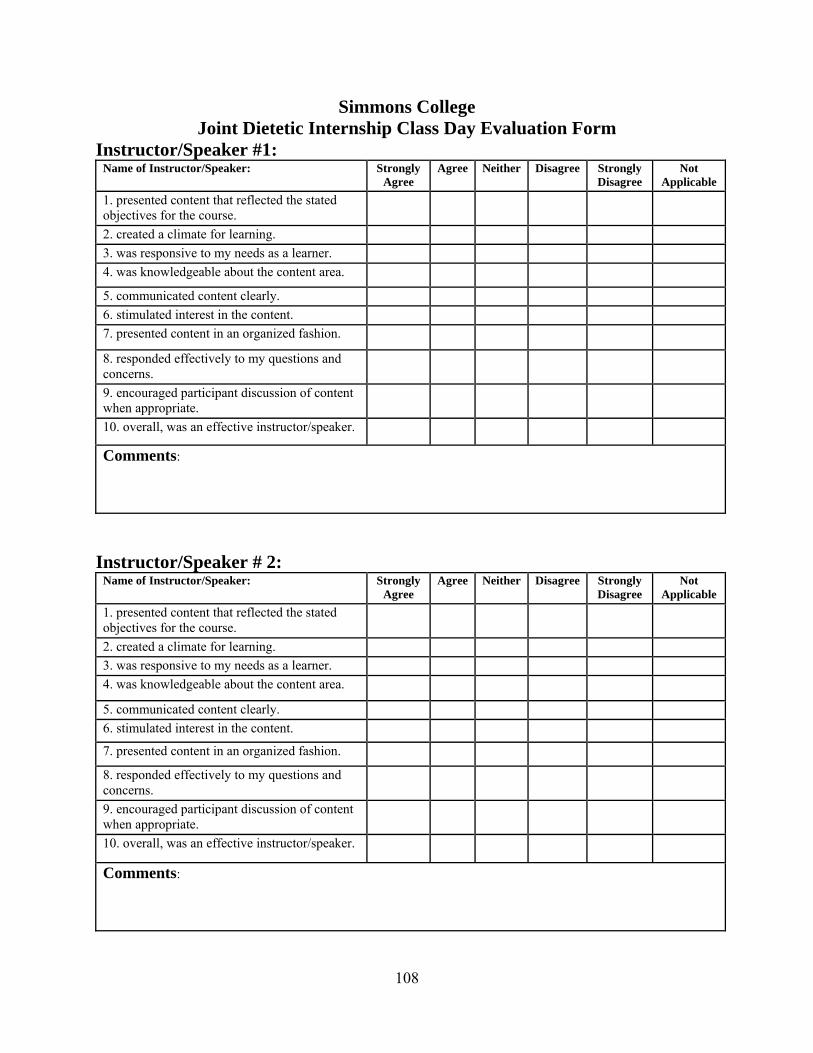
108
Simmons College Joint Dietetic Internship Class Day Evaluation Form
Instructor/Speaker #1: Name of Instructor/Speaker: Strongly
Agree Agree Neither Disagree Strongly
Disagree Not
Applicable
1. presented content that reflected the stated objectives for the course.
2. created a climate for learning.
3. was responsive to my needs as a learner.
4. was knowledgeable about the content area.
5. communicated content clearly.
6. stimulated interest in the content.
7. presented content in an organized fashion.
8. responded effectively to my questions and concerns.
9. encouraged participant discussion of content when appropriate.
10. overall, was an effective instructor/speaker.
Comments:
Instructor/Speaker # 2:
Name of Instructor/Speaker: Strongly Agree
Agree Neither Disagree Strongly Disagree
Not Applicable
1. presented content that reflected the stated objectives for the course.
2. created a climate for learning.
3. was responsive to my needs as a learner.
4. was knowledgeable about the content area.
5. communicated content clearly.
6. stimulated interest in the content.
7. presented content in an organized fashion.
8. responded effectively to my questions and concerns.
9. encouraged participant discussion of content when appropriate.
10. overall, was an effective instructor/speaker.
Comments:

109
Instructor/Speaker #3: Name of Instructor/Speaker: Strongly
Agree Agree Neither Disagree Strongly
Disagree Not
Applicable
1. presented content that reflected the stated objectives for the course.
2. created a climate for learning.
3. was responsive to my needs as a learner.
4. was knowledgeable about the content area.
5. communicated content clearly.
6. stimulated interest in the content.
7. presented content in an organized fashion.
8. responded effectively to my questions and concerns.
9. encouraged participant discussion of content when appropriate.
10. overall, was an effective instructor/speaker.
Comments:
Instructor/Speaker # 4:
Name of Instructor/Speaker: Strongly Agree
Agree Neither Disagree Strongly Disagree
Not Applicable
1. presented content that reflected the stated objectives for the course.
2. created a climate for learning.
3. was responsive to my needs as a learner.
4. was knowledgeable about the content area.
5. communicated content clearly.
6. stimulated interest in the content.
7. presented content in an organized fashion.
8. responded effectively to my questions and concerns.
9. encouraged participant discussion of content when appropriate.
10. overall, was an effective instructor/speaker.
Comments:

110
Worksheets and Other Resources

111
SIMMONS COLLEGE DIETETIC INTERNSHIP PROGRAM
Clinical and Acute Care Worksheets Medical Terminology Worksheets
Therapeutic and Mechanically Altered Diet Worksheets Formulary Review
Review of Common Drug – Nutrient Interaction Enteral Nutrition Worksheets
Parenteral Worksheets Clinical Rotation
Medical Nutrition Therapy for
Various Chronic Diseases & Conditions
The following list of common chronic diseases and medical conditions are well known to the world of medical nutrition therapy. You may encounter a number of these conditions throughout your career in the field of dietetics. Hence, it is recommended that you become familiar with the basic nutritional recommendations for these conditions. Two great references include:
Rapid Reference for Nurses – Nutrition (1st edition) by Nancie Herbold and Sari
Edelstein is a quick, portable, and convenient reference for students and professionals in various clinical settings. A PDA version is also available. For more information visit the Jones and Bartlett website at: http://nursing.jbpub.com .
Manual of Clinical Dietetics (6th
edition) which can be ordered from the American Dietetic Association (ADA) by calling (800) 877-1600 ext 5000 or via their web site at www.eatright.org . If you are interested in pediatric nutrition, there is also a Pediatric Manual of
Clinical Dietetics (2nd
edition) by Nancy Nevin-Folino which can also be obtained from the ADA. ADA Pocket Guide to Nutrition Assessment by Pamela Charney, MS, RD and Ainsley Malone, MS, RD (2004) is a pocket guide which provides convenient, reliable information on the tools and techniques of nutrition assessment. From nutrition screening to physical assessment, laboratory assessment, anthropometrics and determining protein and energy requirements, this guide emphasizes interpretation and application of the findings to individual patient situations. This book can also be obtained by contacting the ADA at (800) 877-1600 ext 5000 or via their web site at www.eatright.org . Medical Terminology: The Language of Health Care by Marjorie Willis (1996, Williams and Wilkens). Again, there are great prices on this textbook on http://half.ebay.com . Nutrition and Diagnosis-Related Care by Sylvia Escott-Stump (2002). You can find this book in a local medical/hospital bookstore or at the following web site: http://www.fetchbook.info/search_Sylvia_Escott-Stump/searchBy_Author.html . There is also a version of the manual for A PDA which was published in 2004. Essentially, any book covering medical nutrition therapy for major chronic diseases is recommended to have as a reference for you internship and for your future in dietetics.

112
Concepts to Consider When Applying Medical Nutrition Therapy To Chronic Disease: Knowledge of the etiology and physiology of the disease or condition. Side effects or complications that can influence the nutritional status of individuals
possessing a particular condition. Potential side effects from drugs commonly used for a particular disease or condition. Medical nutrition therapy recommendations for the disease (i.e. Adjustments in calorie,
carbohydrate, protein, fat, and vitamin and mineral recommendations). Common Chronic Diseases & Conditions
Acquired Immunodeficiency Syndrome / HIV Infection Food Allergies Burns Cancer (all types) Cardiovascular Accident (Stroke) Celiac Disease Chronic Obstructive Pulmonary Disease Congestive Heart Failure (CHF) Coronary Artery Disease (CAD) / Arteriosclerosis / Atherosclerosis Crohn’s Disease Cystic Fibrosis Diabetes Diverticular Disease Eating Disorders; Anorexia and Bulimia Nervosa Gastrectomy Nutritional Implications of Gastric Bypass Surgery Gastroesophageal Reflux Disease (GERD) Hepatic Cirrhosis Hepatitis Hypercholesterolemia / Hyperlipidemia Hypertension (HTN) Hyperthyroidism / Hypothyroidism Lactose Intolerance Metabolic Syndrome (Syndrome X) Myocardial Infarction (MI) Obesity Osteoporosis Pancreatitis Peripheral Vascular Disease (PVD) Renal Disease, acute, chronic, end-stage Short Bowel Syndrome (SBS) Trauma Ulcerative Colitis
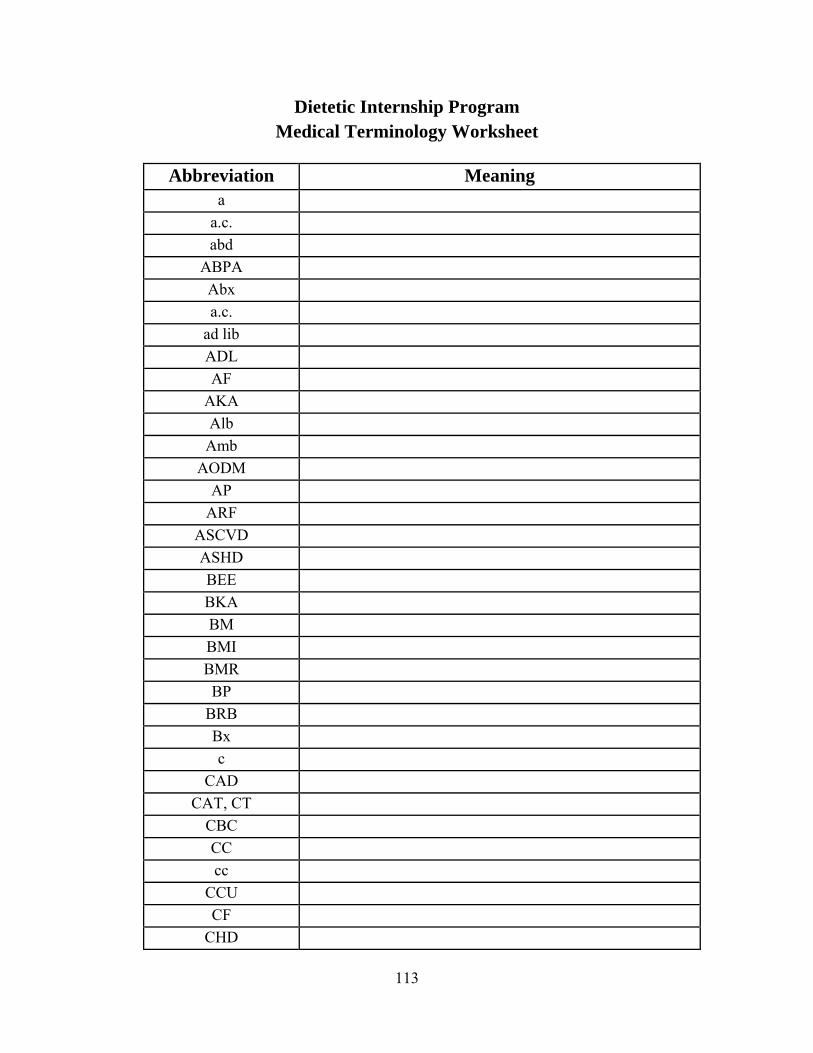
113
Dietetic Internship Program Medical Terminology Worksheet
Abbreviation Meaning
a
a.c.
abd
ABPA
Abx
a.c.
ad lib
ADL
AF
AKA
Alb
Amb
AODM
AP
ARF
ASCVD
ASHD
BEE
BKA
BM
BMI
BMR
BP
BRB
Bx
c
CAD
CAT, CT
CBC
CC
cc
CCU
CF
CHD
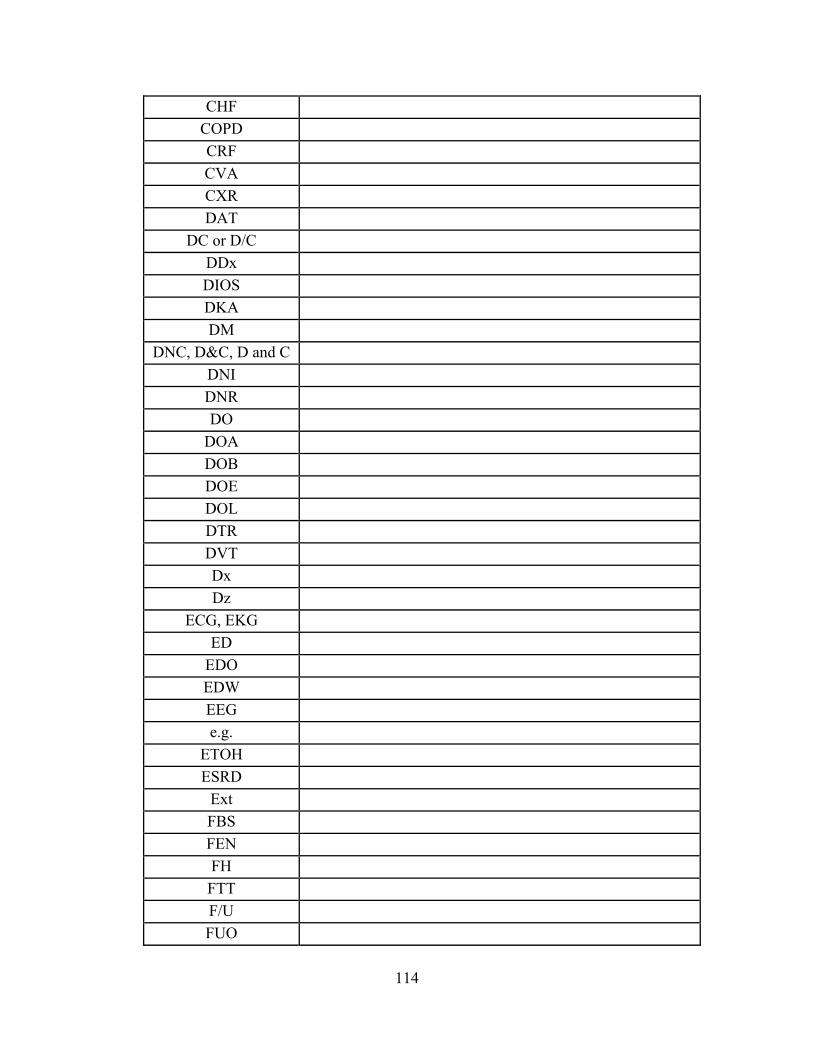
114
CHF
COPD
CRF
CVA
CXR
DAT
DC or D/C
DDx
DIOS
DKA
DM
DNC, D&C, D and C
DNI
DNR
DO
DOA
DOB
DOE
DOL
DTR
DVT
Dx
Dz
ECG, EKG
ED
EDO
EDW
EEG
e.g.
ETOH
ESRD
Ext
FBS
FEN
FH
FTT
F/U
FUO
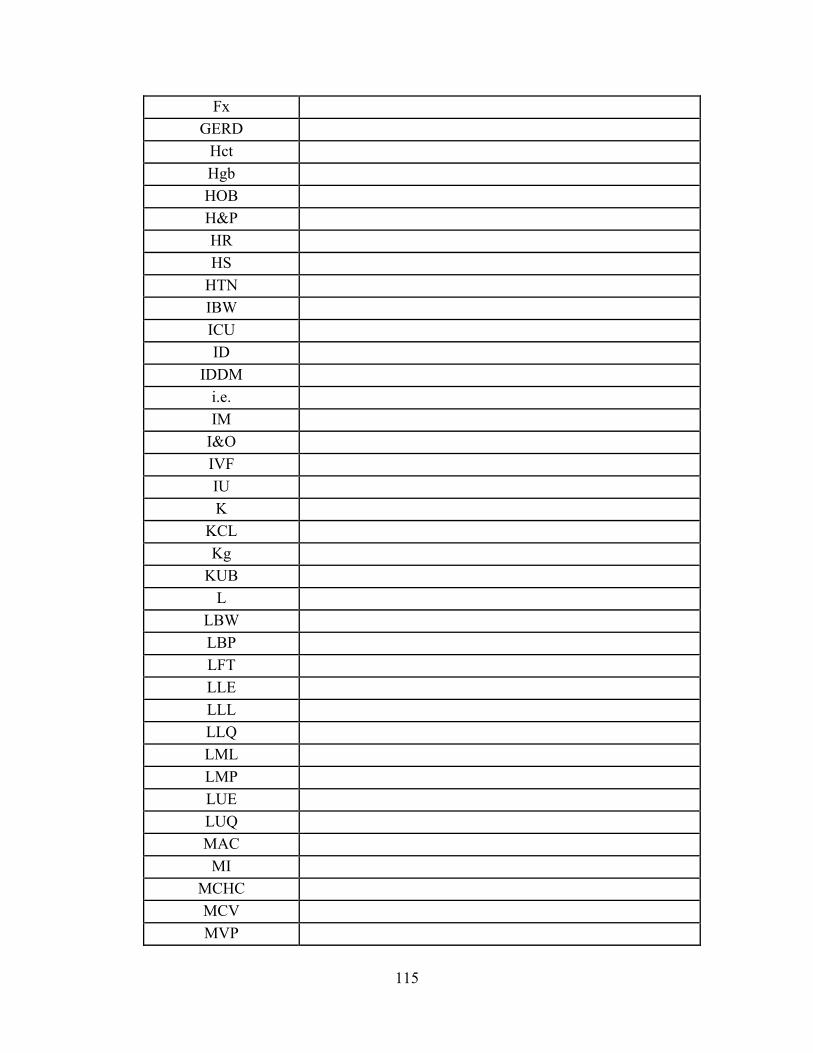
115
Fx
GERD
Hct
Hgb
HOB
H&P
HR
HS
HTN
IBW
ICU
ID
IDDM
i.e.
IM
I&O
IVF
IU
K
KCL
Kg
KUB
L
LBW
LBP
LFT
LLE
LLL
LLQ
LML
LMP
LUE
LUQ
MAC
MI
MCHC
MCV
MVP
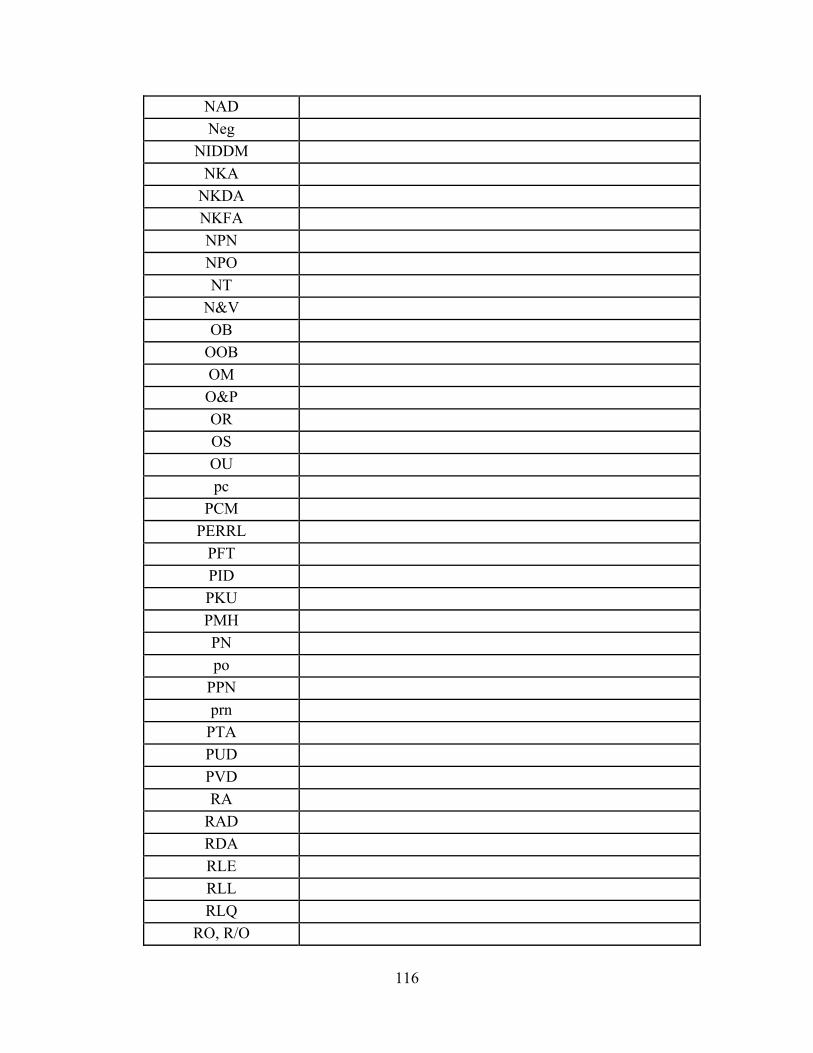
116
NAD
Neg
NIDDM
NKA
NKDA
NKFA
NPN
NPO
NT
N&V
OB
OOB
OM
O&P
OR
OS
OU
pc
PCM
PERRL
PFT
PID
PKU
PMH
PN
po
PPN
prn
PTA
PUD
PVD
RA
RAD
RDA
RLE
RLL
RLQ
RO, R/O
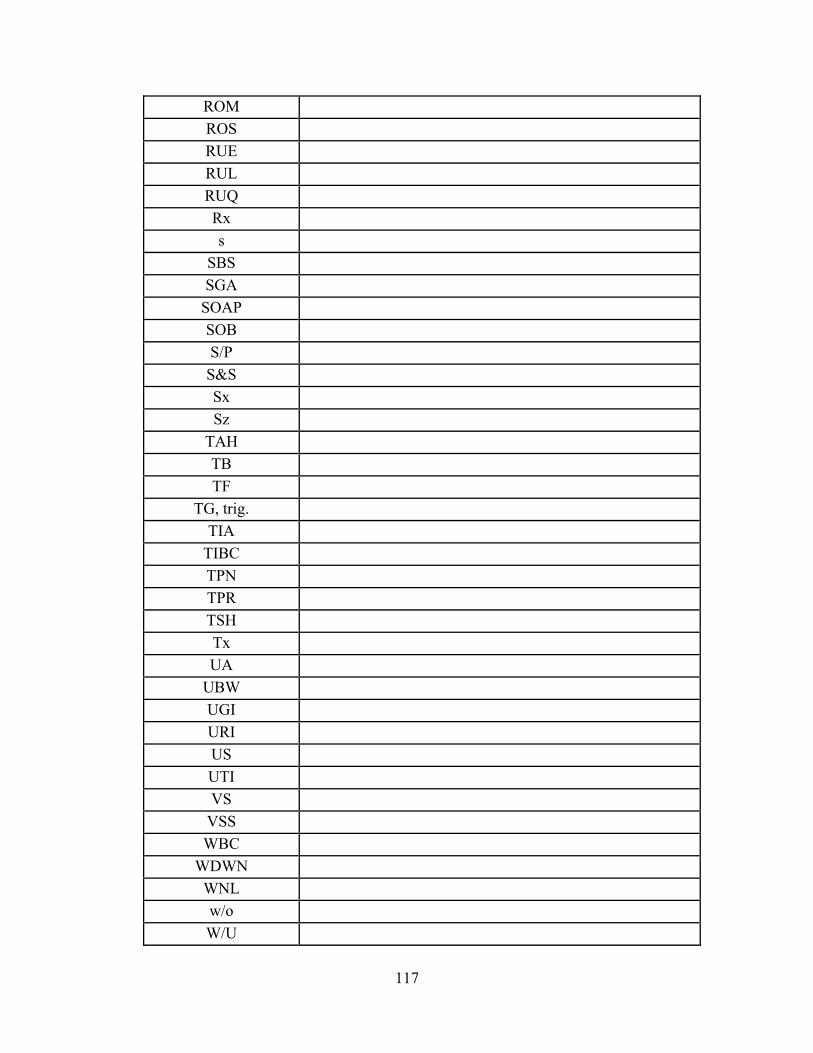
117
ROM
ROS
RUE
RUL
RUQ
Rx
s
SBS
SGA
SOAP
SOB
S/P
S&S
Sx
Sz
TAH
TB
TF
TG, trig.
TIA
TIBC
TPN
TPR
TSH
Tx
UA
UBW
UGI
URI
US
UTI
VS
VSS
WBC
WDWN
WNL
w/o
W/U
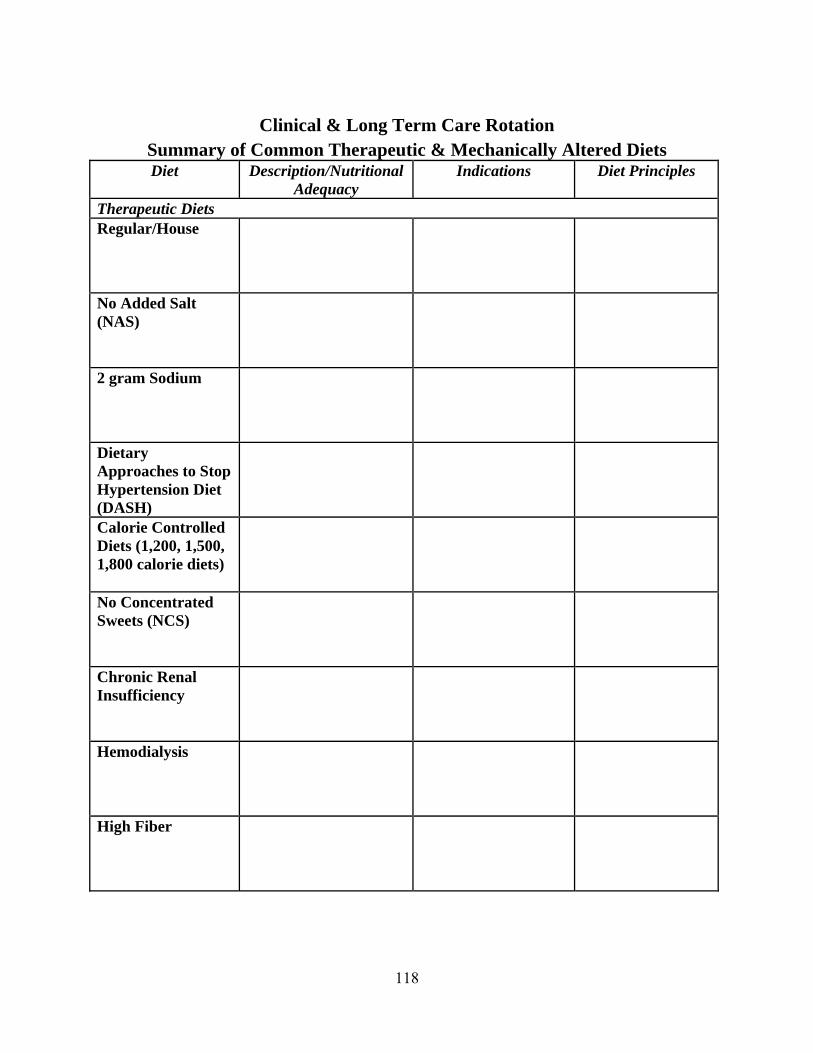
118
Clinical & Long Term Care Rotation
Summary of Common Therapeutic & Mechanically Altered Diets Diet Description/Nutritional
Adequacy Indications Diet Principles
Therapeutic Diets Regular/House
No Added Salt (NAS) 2 gram Sodium
Dietary Approaches to Stop Hypertension Diet (DASH)
Calorie Controlled Diets (1,200, 1,500, 1,800 calorie diets) No Concentrated Sweets (NCS) Chronic Renal Insufficiency Hemodialysis
High Fiber

119
Low Fiber/Low Residue National Cholesterol Education Program’s Therapeutic Lifestyle Changes Diet
Lactose Restricted/Lactose Free High Calorie, High Protein Phenylalanine Restricted Gluten Free
Transitional Diets Clear Liquid
Mechanical Soft
Soft
Texture Modified Diets Mechanical Soft/Ground
120
Dysphagia (Dysphagia Regular, Dysphagia Ground, Dysphagia Puree)
Pureed
121
Clinical Rotation Formula Analysis
Find at least one formula that fits within each of the following formula classes. Identify the name of the product, its indication for use, and its calorie, carbohydrate, protein and fat content.
Product Indications for Use Caloric Density
(kcal/cc)#
Carbo (g/1000
cc)
Protein (g/1000
cc)
Fat (g/1000
cc) General Purpose – Intact (Polymeric) Product: ___________
Defined-Partially Hydrolyzed Product: ___________
Fiber-enriched Product: ___________
Hepatic Product: ___________
Renal Product: ___________
Pulmonary Product: ___________

122
Glucose Intolerance Product: ___________
Trauma Product: ___________
Modular, Carbohydrate Product: ___________
Modular, Protein Product: ___________
Modular, Fat Product: ___________
Other Available Formulas
Indication: ___________ Product: ___________
Indication: ___________ Product: ___________
# Remember when calculating grams per ‘cc’ that 1,000 cc = 1,000 ml = 1 liter; 1oz = 30 cc or 30 ml; 120 cc = 4 oz; 240 cc = 8 oz.

123
Clinical Rotation A Review of Common Lab Values
The following chart presents common lab values that you will encounter during your internship experience. Please record the significance of the particular lab measurement, the normal lab value range, and what may be the problem when these labs are above or below the norm.
Laboratory Measurement
Significance of the Measurement
Normal Lab Value
Range
Conditions Related with
Elevated Readings
Conditions Related with
Low Readings
Albumin
B-Carotene
Blood Urea Nitrogen (BUN)
Calcium, Total
124
Ceruloplasmin
Chloride
Cholesterol, Total
Copper
Creatinine
Disaccharide Absorption Test

125
Erythrocyte Count
Fat, Fecal
Ferritin
Folate
Glucose
Glucose Tolerance Test (GTT)
126
Growth Hormone (hGH)
HDL-Cholesterol (HDLC)
Glycosylated Hemoglobin (HbA1C)
Hematocrit (Hct)
Hemoglobin (Hb)
Iron

127
Iron-Binding Capacity, Total
LDL Cholesterol
Lead
Mean Corpuscular
Mean Corpuscular Hemoglobin
Mean Corpuscular Hemoglobin Concentration
128
Niacin (nicotine acid)
Phenylalanine
Phosphatase, Alkaline
Phosphorus, Inorganic
Potassium
Prealbumin
129
Protein, Total
Prothrombin Time (PT)
Retinol-Binding Protein (RBP)
Riboflavin (vitamin B2)
Sodium
Somatomedin C
130
Thiamine (vitamin B1)
Thyroid Stimulating Hormone (TSH)
Thyroxine (T4)
Transferrin
Triglycerides (TG)
Tyrosine

131
Urea Nitrogen
Vitamin A
Vitamin B6
Vitamin B12
Vitamin C
Vitamin D2, 25 Hydroxy
132
Vitamin D3, 1,25-Dihydroxy
Vitamin E
Zinc

133
Clinical Rotation A Review of Common Medications
* It is highly recommended that you purchase the most recent edition of Food-Medication Interactions. It costs ~$21.95 plus S & H and can be ordered by calling (800) 746-2324.
Medication Intended Use Common Side Effects Drug-nutrient Interactions or
Dietary Considerations
ACE Inhibitors
Aldactone (spironolactone) Antifungals
Aricept
Ativan
Atenolol
AZT (zidovudine)

134
Buspar
Calcijex/Calcitriol
Cephalosporins
Cholestyramine
Cimetidine
Cipro
Codeine
Colchicine
Cozaar
Corticosteroids (prednisone)
135
Coumadin (Warfarin) Digoxin
Diabeta Elavil
Eldepryl
Erythromycin
Ferrous Sulfate, Fumerate & Gluconate Flagyl
Glipizide
Glucophage

136
Haldol
Hydrochlorothiazide (HCTZ Insulin (novolin, humulin) Isoniazid
Klonopin
Lasix (Furosemide) Levodopa
Lipitor
Macrolides
Methotrexate

137
Micronase
Monoamine Oxidase Inhibitors Monopril
Oral Contraceptives Ofloxacin
Paxil
Penicillin
Phenobarbital
Phenytoin (dilantin) Phos-Lo

138
Prilosec
Probenecid
Propranolol
Prozac
Quinolones
Remeron
Synthroid
Tegretol
Tetracycline (doxycycline, minocycline) Theophylline Medications
139
Thiazide Diuretics
Valium
Vasotec
Wellbutrin
Xanax
Zoloft

140
INTRODUCTION TO NUTRITION SUPPORT
The metabolic needs of the ill, hospitalized patient become increased due to stress and other physical factors, often complicating the patient's feeding and nutritional status. Alternative techniques have been developed for feeding patients whose nutritional status has been compromised. These alternative feeding methods include total parenteral nutrition, peripheral parenteral nutrition, and commercial enteral nutritional products. Enteral nutrition is indicated when the patient's gastrointestinal tract is functioning. Although oral feedings are preferable, tube feedings may be essential in patients who have mechanical difficulties in chewing and swallowing, who are comatose, or who have impaired function of their digestive tracts. Commercial formulas offer a variety of standardized products that can be adapted to meet individual needs. Modular tube feeding products are also now available to allow tube feeding regimens to be adapted to the nutrient needs of the patient. Enteral feedings can now be accomplished in the home setting when the appropriate support is available. Total parenteral nutrition and peripheral parenteral nutrition utilize the venous system as a means of providing nutrients to meet the patient's metabolic needs. By assessing the patient's nutritional status, a parenteral solution can be formulated to meet the patient's requirements. Careful monitoring of parenteral solutions is essential to prevent complications and assess for changes in nutrient needs. Parenteral feedings can also be provided in the home when the patient is metabolically and clinically stable and if the appropriate support is available.

141
Enteral Nutrition Worksheets
1. List and discuss indications for initiating enteral nutrition.
2. List and discuss contraindications for initiating enteral nutrition.
3. Briefly discuss the major properties of enteral solutions (osmolality, compos-tion,
etc.). How are they differentiated and how the level of GI tract function effects your selection of an enteral product?
4. Describe the effect of a hyperosmolar solution in the gastrointestinal tract (i.e., greater than 300 m0sm). Compare the effect of osmolality as it relates to the stomach, duodenum, and jejunum. Identify which nutrients make the greatest contribution to the osmolality of a solution.

142
5. Discuss nutrition assessment parameters used in monitoring tube feeding tolerance
(include subjective and objective data).
6. Compare and contrast the following delivery routes. a. Nasogastric (NG) Route
b. Nasoduodenal (ND) or Nasojejunal (NJ) Route
c. Percutaneous Endoscopic Gastrostomy (PEG)
d. Endoscopic Jejunostomy/PEJ
143
e. Percutaneous Gastrojejunostomy (PGJ)
7. Compare and contrast the following tube sizes, including pros and cons of each tube size.
a. Small-bore
b. Large-bore
8. Compare and contrast the following delivery systems.
a. Administration Pumps
b. Open Systems
144
c. Closed Systems
9. Differentiate between the following feeding schedules: bolus feeding, intermittent
drip and continuous drip.
10. List important parameters (i.e. weight, edema, etc.) that must be regularly monitored to prevent and correct complications and ensure proper amount of ingested formula to ensure meeting nutritional needs. Provide the number of times per week that these parameters should be monitored.
145
11. List and describe preventative measures that can be followed to prevent tube
clogging and maintain tube patency.
12. Define gastric residual and how it is measured. Describe why gastric residual is undesirable. How often must gastric residual be monitored in patients receiving enteral nutrition?
13. List and describe at least five complications (aspiration, diarrhea, constipation, etc.) associated with tube feeding, and discuss appropriate treatments.

146
14. Briefly describe ways nursing can care for insertion sites so to prevent skin irritation and dislodgement of the tube.
15. Develop a decision tree for determining methods of nutritional support, including product selection.

147
Enteral Nutrition Case Study 1
A 65-year-old black female suffered a CVA and is comatose. A nasogastric tube was placed immediately upon admission. A tube feeding regimen using Osmolite 1.2 (Abbott Nutrition http://www.abbottnutrition.com) was started at 15cc/hr and increased to a goal of 60cc/hr and within 36 hours was advanced to FS Vital 1.5 at 85 cc/hr (Abbott Nutrition http://abbottnutrition.com). On day 3 of the tube feeding, the patient developed diarrhea. The feeding was consequently stopped, and a nutrition consult was ordered. PMH: Seizure disorder, HTN Medication: Dilantin, Ampicillin, Gentamycin, Colace, IV D5 1/2 NS at 85 cc/hr Laboratory Data: DAY 1 DAY 3 DAY 6 ALBUMIN 3.5 2.4 2.2 Hct 48 32 32 MCV 90 85 85 Na 149 135 135 K+ 3.7 3.2 3.4 BUN 48 18 18 Creat 1.6 1.4 1.4 Phos n/a 1.9 1.0 Height: 5'10" Weight: 130 lb. UBW: 150 lb. (all information per family) Tmax: Day 1 102.6F I/O pt. inc. Day 3 100.6F IV D/C'd day 2

148
Questions Enteral Nutrition Case Study 1
1. Assess patient's energy, protein, and fluid needs. 2. Identify at least four possible causes of diarrhea in the tube-fed patient. 3. Discuss the appropriateness of the initial tube feeding, including nutrient content, volume
and formula selection. 4. What alternative product(s) might be suggested for this patient? Justify your answers. 5. If the patient remains comatose and is at risk for aspiration, what adjustments could be
made in the delivery of the formula to reduce the risk to the patient? 6. Discuss the patient's medications and their impact on the tube feeding.
7. What is your response to the nutrition consult received on HD 3? Include your
recommendations. 8. Your recommendations were followed and tube feed restarted on day 3, with the patient
reaching her goal rate by day 5. On day 6 albumin and phosphorus levels were checked and were in critical range. What are possible reasons for these abnormal levels? Would your recommendations change? If so, how?

149
Enteral Nutrition
Case Study 2 A 69-year-old white female presented at the Emergency Department with a chief complaint of difficulty swallowing. The patient was admitted, and a swallowing workup revealed she had a functional abnormality. She was placed on a puree diet with Resource 2.0 supplements b.i.d (Novartis Medical Nutrition: http://www.novartisnutrition.com/us/home). Following a 17 day trial period, family members complained that the patient was taking minimal p.o.'s. A few days later a PEG tube was placed, and a nutrition consult ordered. PMH: MVR (mitral valve repair), scoliosis, depression Medication: Digoxin, Procan SR, Verapamil, FeSo
4 Elixir, Coumadin
Laboratory Data Alb Hct Chol PO
4
Day 1 2.8 31.2 166 - Day 11 2.6 32.7 - - Day 17 2.5 - - 2.4 Day 26 2.6 - - 3.4 Height: 5'7" Weight: On admission - 100 lb. On day 17 - 96 lb. UBW (1 month PTA): 108 lb.
1. Complete a nutritional assessment for this patient, including TF recommendations.
2. Discuss any possible interactions with current medications.

150
3. Feeding is implemented per your recommendations. What parameters would you follow while establishing tolerance to enteral feeding?
4. On day 26 another nutrition consult was ordered for recommendations on bolus feeding. How would you make the transition to bolus feedings? Prepare a schedule for the transition. How would you monitor tolerance?
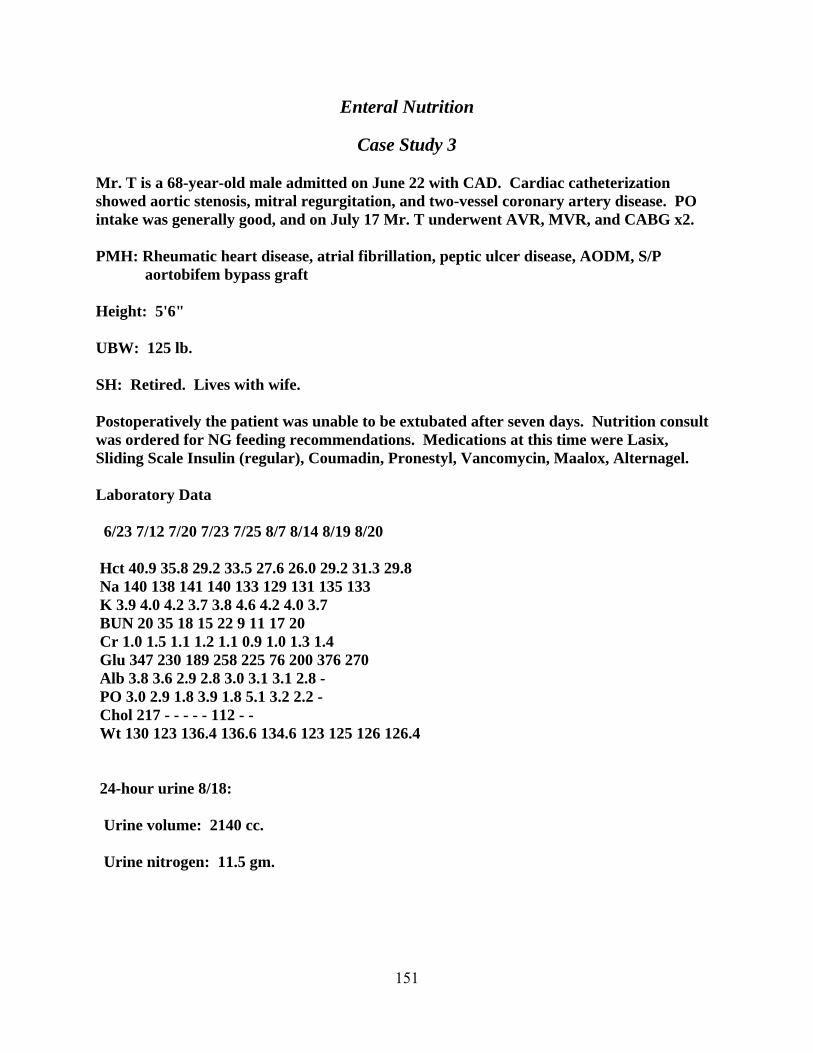
151
Enteral Nutrition
Case Study 3 Mr. T is a 68-year-old male admitted on June 22 with CAD. Cardiac catheterization showed aortic stenosis, mitral regurgitation, and two-vessel coronary artery disease. PO intake was generally good, and on July 17 Mr. T underwent AVR, MVR, and CABG x2. PMH: Rheumatic heart disease, atrial fibrillation, peptic ulcer disease, AODM, S/P
aortobifem bypass graft Height: 5'6" UBW: 125 lb. SH: Retired. Lives with wife. Postoperatively the patient was unable to be extubated after seven days. Nutrition consult was ordered for NG feeding recommendations. Medications at this time were Lasix, Sliding Scale Insulin (regular), Coumadin, Pronestyl, Vancomycin, Maalox, Alternagel. Laboratory Data 6/23 7/12 7/20 7/23 7/25 8/7 8/14 8/19 8/20 Hct 40.9 35.8 29.2 33.5 27.6 26.0 29.2 31.3 29.8 Na 140 138 141 140 133 129 131 135 133 K 3.9 4.0 4.2 3.7 3.8 4.6 4.2 4.0 3.7 BUN 20 35 18 15 22 9 11 17 20 Cr 1.0 1.5 1.1 1.2 1.1 0.9 1.0 1.3 1.4 Glu 347 230 189 258 225 76 200 376 270 Alb 3.8 3.6 2.9 2.8 3.0 3.1 3.1 2.8 - PO 3.0 2.9 1.8 3.9 1.8 5.1 3.2 2.2 - Chol 217 - - - - - 112 - - Wt 130 123 136.4 136.6 134.6 123 125 126 126.4 24-hour urine 8/18: Urine volume: 2140 cc. Urine nitrogen: 11.5 gm.

152
1. Write your consult reply and recommendations for feeding. 2. On 7/25 serum phosphorus dropped and neutrophos was added to medications. What are
possible causes of low serum phosphorus and implications of hypophos-phatemia in this patient's condition?
3. On 8/11 the patient was below preoperative weight and became hypotensive, with decreased urine output. The physician felt he needed more fluid and changed the tube feeding to 1/2 strength Resource 2.0 (Novartis Medical Nutrition: http://www.novartisnutrition.com/us/home) at 80 cc/hr (diluted with normal saline). Is this formula adequate for Mr. T's requirements? Please calculate nutrients provided, including sodium and H
2O as well as pro, CHO, fat, and vitamins/minerals. Would you recommend any
changes at this time?

153
4. Mr. T continued to have difficulty weaning, and on 8/20 you receive a nutrition consult requesting a high protein, high fat (at least 50% of calories) formula. He continues to require approximately 2 liters of fluid and 5 grams of sodium daily. Write a SOAP note detailing your recommendations and consult reply.
Medications at this time were sucralfate, Regular Humulin S/S, Neutrophos, Inderal,
Coumadin, K-dur, Valium, NPH, Digoxin, FeSO4, Folate, MVI, Vancomycin, and
Haldol.
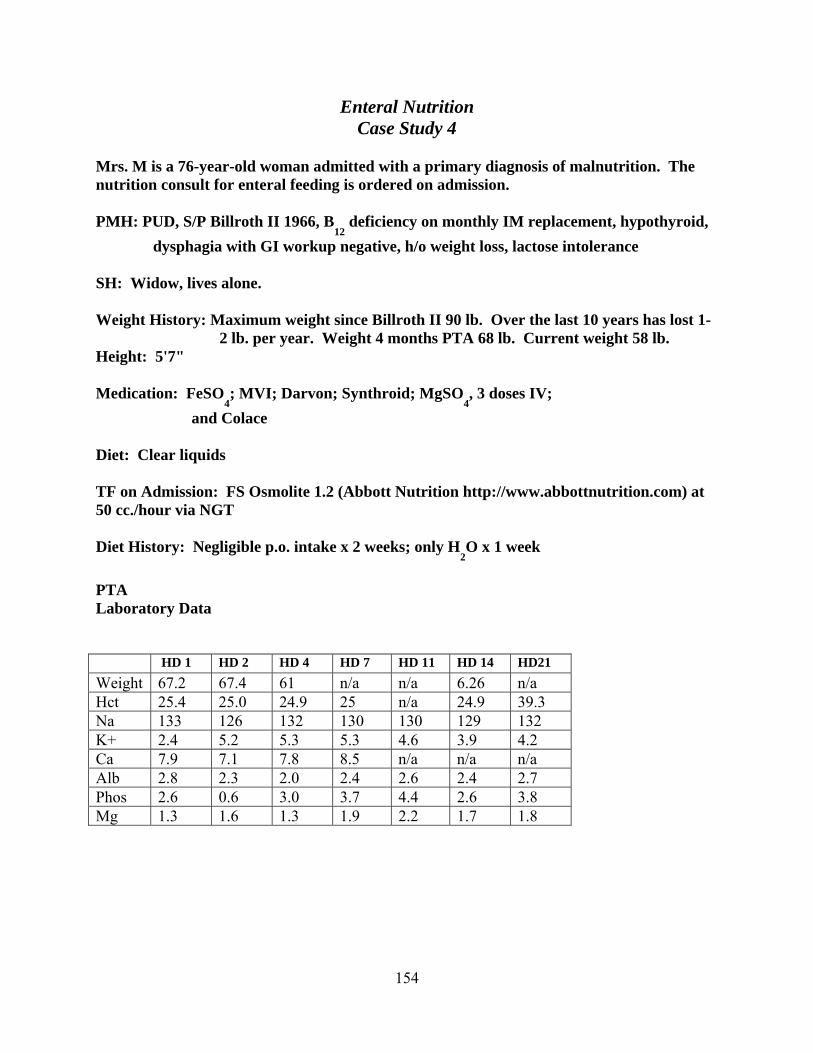
154
Enteral Nutrition Case Study 4
Mrs. M is a 76-year-old woman admitted with a primary diagnosis of malnutrition. The nutrition consult for enteral feeding is ordered on admission. PMH: PUD, S/P Billroth II 1966, B
12 deficiency on monthly IM replacement, hypothyroid,
dysphagia with GI workup negative, h/o weight loss, lactose intolerance SH: Widow, lives alone. Weight History: Maximum weight since Billroth II 90 lb. Over the last 10 years has lost 1-
2 lb. per year. Weight 4 months PTA 68 lb. Current weight 58 lb. Height: 5'7" Medication: FeSO
4; MVI; Darvon; Synthroid; MgSO
4, 3 doses IV;
and Colace Diet: Clear liquids TF on Admission: FS Osmolite 1.2 (Abbott Nutrition http://www.abbottnutrition.com) at 50 cc./hour via NGT Diet History: Negligible p.o. intake x 2 weeks; only H
2O x 1 week
PTA Laboratory Data HD 1 HD 2 HD 4 HD 7 HD 11 HD 14 HD21
Weight 67.2 67.4 61 n/a n/a 6.26 n/a Hct 25.4 25.0 24.9 25 n/a 24.9 39.3 Na 133 126 132 130 130 129 132 K+ 2.4 5.2 5.3 5.3 4.6 3.9 4.2 Ca 7.9 7.1 7.8 8.5 n/a n/a n/a Alb 2.8 2.3 2.0 2.4 2.6 2.4 2.7 Phos 2.6 0.6 3.0 3.7 4.4 2.6 3.8 Mg 1.3 1.6 1.3 1.9 2.2 1.7 1.8

155
Questions Enteral Nutrition
Case Study 4
1. Please discuss your recommendations for feeding this patient. Include a discussion of pertinent laboratory data and meds. What parameters would you monitor?
2. On HD 2 the patient developed diarrhea. Alb and phos as well as Na had decreased.
Discuss possible causes of diarrhea and decreasing laboratory values. What recommendations would you make at this time?
3. On HD 4 TF was FS Osmolite 1.2 (Abbott Nutrition http://www.abbottnutrition.com) at 35 cc/hr. The patient was becoming interested in eating. What are your recommendations for diet progression?
4. Medications: FeSO
4, MVI without minerals, Darvon, Synthroid, Neutraphos, Mg Oxide,
CaCO3.
By HD 11, TF is FS Osmolite 1.2 @ 35 cc/hr (Abbott Nutrition http://www.abbottnutrition.com), and p.o. intake was improving. The patient c/o fullness with PO plus TF. A percutaneous J-tube was scheduled for HD 13. Diarrhea was resolved. What plans would you suggest for combining p.o. plus TF after the J-tube? 5. By HD 14 p.o.'s had increased and were averaging 1,000 calories and 30 gm. protein daily.
You are asked to alter the TF regimen to supplement p.o.'s. Long-term goal is night TF, with p.o.'s during daytime. Discuss your plan for changing to night TF. What volume of TF will be required?
Run the enteral feeding at 35 cc/hr for 12 hours as po intake is improving. Recommend to follow prealbumin levels every 3 to monitor protein improvement.

156
6. By HD 21 weight was slowly improving. Phos and Mg had stabilized, and supplemental
phos, Mg, and calcium were discontinued. The patient is being transferred to a nursing home. Please write a nutrition referral outlining nutrition plan and goals.
7. What is refeeding syndrome? What are potential complications? How should this be
managed?

157
Enteral Nutrition
Case Study 5 A 27-year-old male was admitted S/P a motorcycle accident, with a basilar skull fracture, bilateral mandibular fractures, and diffuse cerebral edema. His Glasgow Coma Scale was 6. He had a Richmond ICP monitor placed on the day of admission and returned to the operating room two days later for open reduction and internal fixation of his mandibular fractures and G- and J-tube placement for suction and feeding respectively. J-tube feedings are to start immediately. The patient is 185 cm. tall and weighs 81 kg. on admission. 1. What are the patient's kcal and protein requirements? 2. What tube feeding would you recommend for this patient, and why? 3. What would you recommend for initiating and advancing a J-tube feeding?

158
Parenteral Nutrition Calculations
Complete the following chart of sample parenteral nutrition products. Use 3.4 kcal/g for CHO, 4 cal/g for protein, and the appropriate calories/cc with lipids. Show calculations (show % of total kcal also).
Product Non-Protein Total Calories
Calories CHO (g) Fat (g) Protein (g)
2LD15A5+ 40 g lipid
3LD15A5
2LA3 D5+ 40 g lipid
2.5LA3 D6
159
Parenteral Nutrition Worksheets
Note: All answers must be from a nutrition support perspective. Part A: Terminology 1. Define or explain the following terms: a. Total Parenteral Nutrition (TPN) b. Peripheral Parenteral Nutrition (PPN) c. Branch-Chain Amino Acids d. Expanded Food and Nutrition Education Program (EFNEP) e. Women Infants and Children Program (WIC) f. Glycerol g. Essential Fatty Acid h. Essential Amino Acid
160
i. Aromatic Amino Acid k. Maternal and Infant Care Projects l. Admixture m. Stress Response n. Subclavian Vein o. Respiratory Quotient (equation and explanation) p. Starvation Adaptation q. "Refeeding" Syndrome r. Glucagon

161
s. Catecholamines t. Kwashiorkor u. Marasmus v. Nitrogen Balance w. Early Enteral Feeding x. Indirect Calorimetry y. Ileus

162
Part B: Estimating Energy and Macronutrient Needs
1. There are many methods of estimating energy and protein needs for the stressed patient. Discuss the use of the BEE with stress factors vs. The Body Surface Area normogram. Which method do you prefer and why?
2. Which weight do you use--IBW, UBW, or current body weight--for the obese patient?
The cachectic patient? The fluid overloaded patient? 3. What are the maximum levels of macronutrients (glucose/dextrose, amino acids, lipids
and fluids) that should be used in PN formulation? 4. Disease-specific amino acid solutions are currently available. Discuss the indications
and contraindications.
163
Part C: Vitamin and Mineral Supplementation
1. Discuss the use of vitamin and mineral supplementation in parenteral nutrition. How do the parenteral requirements differ from the oral requirements? Why?
2. Why is iron not included in PPN or TPN solutions? 3. List and describe what micronutrient should be added to PPN and TPN solutions that
will be administered indefinitely?
Part D: Managing Possible Parenteral Nutrition Side Effects and Problems 1. List the major causes of the following and guidelines for troubleshooting each problem.
a. Elevated Blood Glucose
b. Elevated Blood Triglycerides
164
c. Air Embolism
d. Clogged Catheter
e. Catheter Infection
f. Refeeding Syndrome
g. Dehydration
h. Fluid Overload
i. Hypersensitvity
j. Drug/Nutrient Interactions
165
k. Sudden Weight Change
l. Electrolyte depletion
Part E: Branched Chain Amino Acids 1. Discuss the indications and theory for use of branched chain amino acid solutions. Part F: Essential Amino Acids 1. Discuss the indications for use of essential amino acid solutions.

166
Part G: Overfeeding Syndrome 1. Discuss the concerns in "overfeeding" the stressed patient. What pertinent laboratory
values or other clinical tests are altered with overfeeding?
Part H: Respiratory Failure 1. How does respiratory failure alter parenteral nutrition substrate utilization? Identify
any pertinent calculations.
Part I: Gut Translocation 1. Discuss the concept of gut translocation of bacteria, and the roles, if any, of enteral and
parenteral nutrition.

167
Part J: Cost Effectiveness of Enteral and Parenteral Nutrition 1. Discuss why aggressive enteral or parenteral nutritional support is cost effective. 2. How can a nutrition support service help an institution to control costs? Part K: Home Parenteral Nutrition 1. Discuss the indications for home total parenteral nutrition. 2. Discuss why psychological support is important for the patient on home nutritional
support (enteral or parenteral), especially if the patient is NPO.

168
Part L: Multi-System Organ Failure 1. Multi-system organ failure is a complex cumulative progression of organ dysfunc-tion
and failure. Discuss the role of nutritional support as this process progresses. What role does early parenteral or enteral nutrition play?
Part M: Ethical Implications of Parenteral and Enteral Nutrition 1. Ethical decision making is an ongoing process with all hospitalized patients who have
terminal illnesses. a. Why are some patients who are DNR candidates for nutrition support?
b. Discuss the significance of withdrawing versus withholding nutritional support in the terminally ill patient.
Part N: Cycling TPN Solutions 1. Explain at least two of the rationales for cycling TPN solutions.

169
Part O: Parenteral Nutrition Calculations
1. What TPN formulas would you choose for each case scenario given below? Include fluid volume, rate, dextrose, amino acids, and lipids (if appropriate).
a. A 30-year-old male with a history of heavy ETOH abuse was admitted with a diagnosis of acute pancreatitis. He was at low weight for height, with an albumin of 2.7. He has been NPO x 7 days and is to start TPN today. His triglyceride level is 150; all his electrolytes, BUN, and creatinine are normal. His requirements are 2,700 kcal. with 95 gm. protein/day.
b. An 80-year-old female is admitted to the MICA in congestive heart failure. Tube feedings are attempted, but the patient has several episodes of nausea and vomiting. TPN is to be started. Her kcal/protein requirements are 1,950 kcal. with 75 gm. protein. The patient has been granted less than 1,400 cc/day. Her triglyceride level is 105.
c. A 25-year-old male is admitted S/P a fall from a five-story building. He has bilateral tibia and fibula fractures, a pelvic fracture with a huge retroperitoneal hematoma by CT scan, and traumatic pancreatitis necessi-tating TPN initiation. His requirements are 3,200 kcal. with 150 gm. protein/day. His amylase is 650 and triglyceride level is 125.

170
d. A 35-year-old male is admitted with ulcerative colitis and 8 to 10 bloody stools per day. He has failed medical treatment and is preoperative for a total colectomy. He is to receive 14 days of preoperative TPN. His kcal/protein requirements are 2,750 kcal. with 140 gm. protein/day. His electrolytes are normal, albumin is 2.3, and triglyceride level is 360.

171
Nutrition Support
Case Study 1
Mr. S is a 68-year-old male admitted on 10/7/07 with intractable diarrhea for two weeks (↑ volume with a BM q.2 hr.), dehydration, and anemia. His final diagnosis is Whipple's disease (intestinal lipodystrophy) - see Harrison's Principles of Internal Medicine. Tests: 24-hour urine for protein Normal Fecal fat test Abnormal Erythrocyte sedimentation rate High D-xylose Abnormal Biopsy of duodenum positive for Whipple's disease. Admission Weight: 116 lbs. Height: 5' 8" Abnormal Admission Labs: Ca++ 7.0 mg/dl Alb 1.5 gm/dl Chol 59 mg/dl Phos 2 mg/dl During the acute phase of his disease, Mr. S was started on CPN and clear liquid. Do the following: 1. Code for malnutrition and discuss reasons for abnormal labs. 2. Design a CPN solution using a 3:1 system. 70% dextrose, 11.4% AA, 40 gm fat emulsion are the max stock solutions available. 3. Discuss what additional lytes/additives he will need and give reasons why.

172
4. Discuss why you may also want to enterally feed the patient.
5. Explain the role of a D-xylose test in maldigestion vs. malabsorption. 6. What do you think was the fat content of his feces (high, moderate, low)? 7. Would you give additional protein to this patient? Explain. 8. After biopsy and diagnosis for Whipple's disease, Mr. S was started on antibiotic (Bactrim)
and his diarrhea resolved. He is ready for transitional feeding to solid food. Choose one of the following and explain you choice:
o House diet with Carnation Instant Breakfast o Low Fat diet with Liposorb o Low lactose diet with Ensure
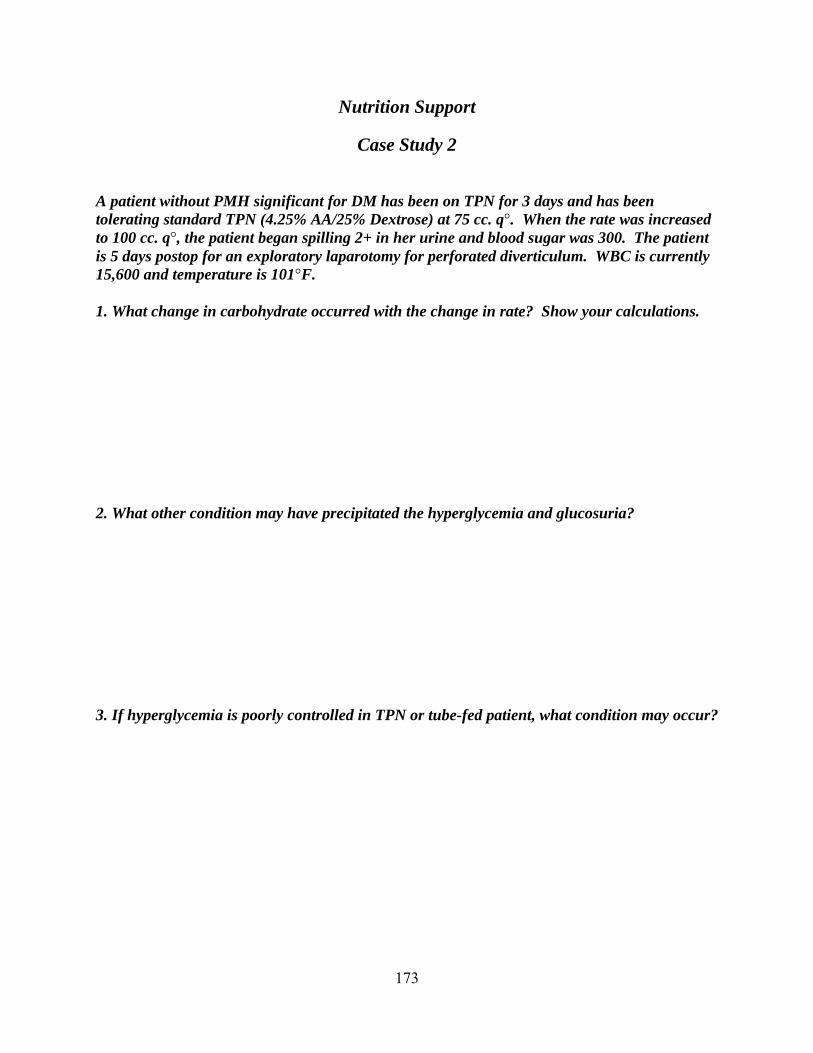
173
Nutrition Support
Case Study 2 A patient without PMH significant for DM has been on TPN for 3 days and has been tolerating standard TPN (4.25% AA/25% Dextrose) at 75 cc. q°. When the rate was increased to 100 cc. q°, the patient began spilling 2+ in her urine and blood sugar was 300. The patient is 5 days postop for an exploratory laparotomy for perforated diverticulum. WBC is currently 15,600 and temperature is 101°F. 1. What change in carbohydrate occurred with the change in rate? Show your calculations. 2. What other condition may have precipitated the hyperglycemia and glucosuria? 3. If hyperglycemia is poorly controlled in TPN or tube-fed patient, what condition may occur?
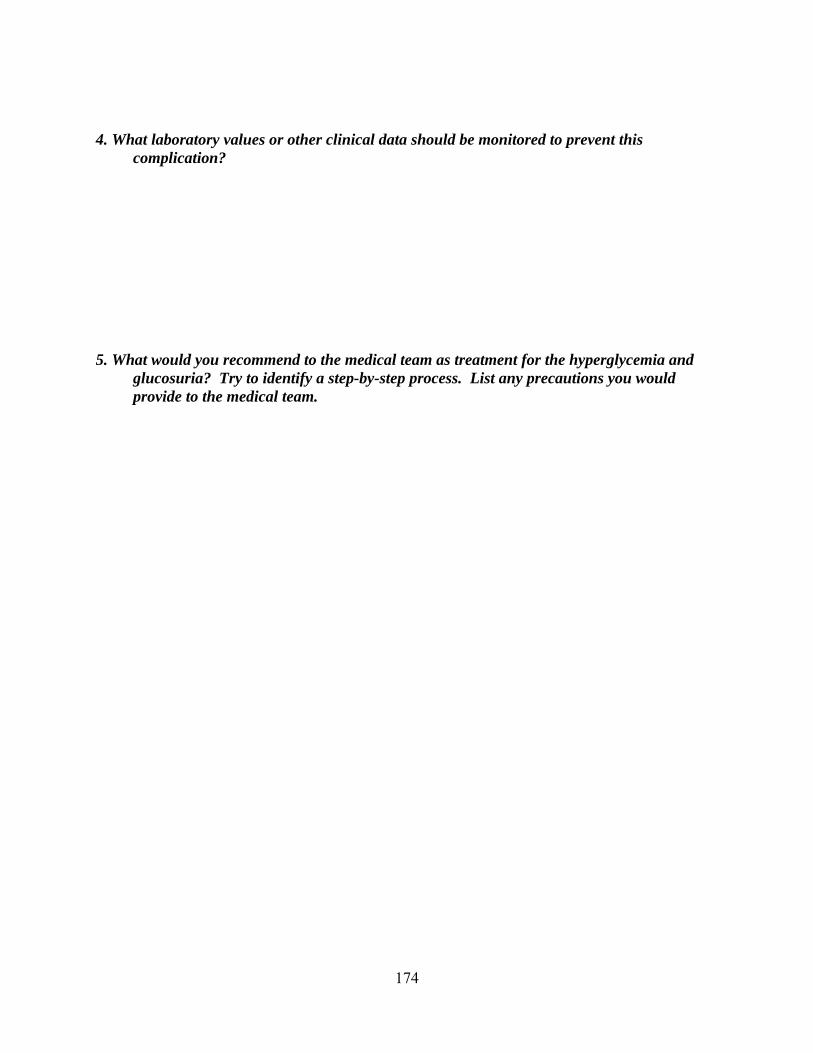
174
4. What laboratory values or other clinical data should be monitored to prevent this complication?
5. What would you recommend to the medical team as treatment for the hyperglycemia and
glucosuria? Try to identify a step-by-step process. List any precautions you would provide to the medical team.
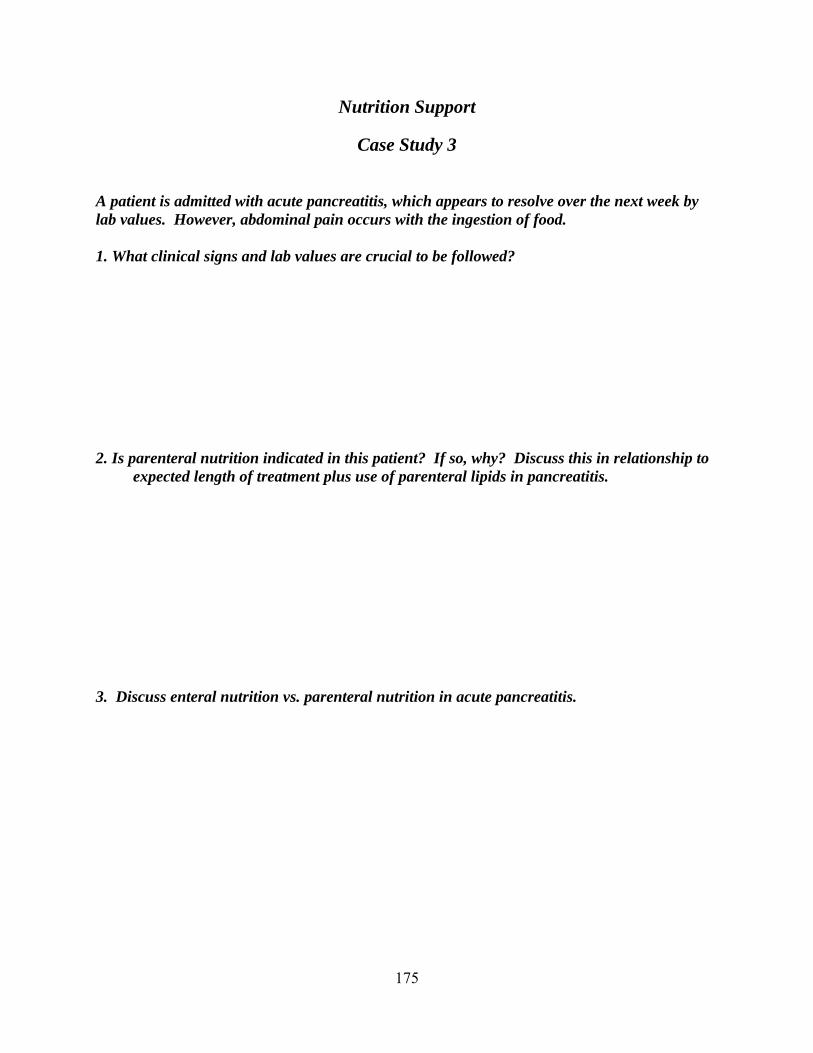
175
Nutrition Support
Case Study 3 A patient is admitted with acute pancreatitis, which appears to resolve over the next week by lab values. However, abdominal pain occurs with the ingestion of food. 1. What clinical signs and lab values are crucial to be followed? 2. Is parenteral nutrition indicated in this patient? If so, why? Discuss this in relationship to
expected length of treatment plus use of parenteral lipids in pancreatitis. 3. Discuss enteral nutrition vs. parenteral nutrition in acute pancreatitis.

176
Nutrition Support
Case Study 4 Mrs. Player is a 50 year old female admitted emergently to the hospital yesterday with a large gastrointestinal bleed. She has a history of a 20 lb weight loss over the last three months so it was decided to initiate TPN.. A central venous line was inserted for TPN. She is considered to be moderately stressed. Plan an appropriate parenteral nutrition formula.
o Sex: Female o Age: 50 o Height: 5’ 7’ o Weight: 120 lbs o Weight History: 20 lb weight loss over preceding 3 months
HINTS
Calculate her fluid requirements first so that you know what volume of formula you will need. Show calculations.
Calculate her calorie and protein requirements. Her normal RMR, is increased by 20%. Her activity factor is considered to be 1.2. The formula must include carbohydrate, fat, and protein from amino acids. Show calculations.
Show your calculations for the total grams of carbohydrate and calories from glucose; total grams of protein and calories from amino acids and total amount of fat calories from 20% fat emulsion (fat calories should not exceed 30% of her total calories.
Note: It will be helpful to calculate total calories required first then calculate calories contributed by her protein requirement. Subtract the protein calories from the total calories and use this as the non-protein calorie contribution (CHO + fat).
Now you have her total CHO gm, gm of amino acids (protein), and fat calories. Distribute these equally into the total volume you plan to provide (round to within the 1/2 liter). [e.g. 500 gm CHO divided by 3.5L would give you 143 gm CHO/L].
Translate this into percentage of CHO and protein/ L [e.g. in this example it is 14.3% CHO]. Do protein the same way, express fat as calories only.

177
Nutrition Support
Case Study 5 Mrs. Juicer is a 50 yo female with a 50% burn due to her nightclothes catching fire from the gas stove. Enteral feedings have been attempted, however it has been unsuccessful due to a persistent ileus. She has a triple lumen catheter in place, one port has been saved for feeding. Plan a parenteral nutrition formula to meet her requirements. Plan a parenteral nutrition formula to meet her requirements.
Height: 5’ 4” Admission weight: 130 lbs

178
Nutrition Support
Case Study 6
Mrs. Smith was admitted emergently to the hospital yesterday. She has a permanent Hickman catheter IV access which has been used for chemotherapy and any fluid/medication she may need. She is in the ICU and is requiring ventilator support. They were unable to pass an NG tube for feeding. Her Hickman catheter is the only IV access she will have. Plan an appropriate nutrition formulation. Consider the fact that the IV line she will be using for PN has been used for multiple types of infusions.
Height: 5’ 7” Admission weight: 120 lbs

179
Enteral and Parenteral Nutrition References
Bloch, A.S., & Mueller, C. “Chapter 23: Enteral and Parenteral Nutrition Support.” Mahan, L.K.,
& Escott-Stump, S. (Eds). Krause’s Food, Nutrition and Diet Therapy (11th
ed.). Philadelphia, PA: W.B. Saunders. 2004. 533-553. Matarese, L.E., & Gottschlich, M.M. Contemporary Nutrition Support Practice: A Clinical
Guide (2nd
ed.). Philadelphia, PA: W.B. Saunders. 2003. Parrish, C.R., & Malone, A. “Enteral Formula Selection: A Review of Selected Product Categories.” Practical Gastroenterology. June 2005. 44-74. http://www.healthsystem.virginia.edu/internet/digestive-health/nutritionarticles/MaloneArticle.pdf . Parrish, C. R., & McCray, S. “Enteral Feeding: Dispelling Myths.” Practical Gastroenterology. Sept 2003. 33-50. http://www.healthsystem.virginia.edu/internet/digestive-health/nutritionarticles/practicalgastrosept03.pdf . Worthington, P.H. Practical Aspects of Nutritional Support: An Advanced Practice Guide. Philadelphia, PA: W.B. Saunders. 2004. 265-341.

180
SIMMONS COLLEGE DIETETIC INTERNSHIP PROGRAM
• Counseling and Education Tips • Nutrition Care Process Worksheets
• Pregnancy and Lactation Worksheets • Diabetes Worksheets • Anemia Worksheets
Patient Education & Counseling Tips
Chief Assessment Factors
1. Socioeconomic factors 2. Cultural, religious beliefs and background 3. Age & sex of patient & significant others 4. Birth order and family involvement of the patient 5. Occupation 6. Medical status and medical history 7. Marital status; number and ages of children 8. Cognitive status; educational level 9. Readiness to learn and staging:
precontemplation contemplation preparation action
maintenance 10. Emotional status (stress, acceptance of illness, chronic disease, or condition) 11. Instructor’s ability to teach; awareness of use of teaching/learning principles
Principles of Learning
1. Information must be valued by the recipient. 2. The pace should be adequate for the learner (i.e. small steps). 3. The environment should be conducive to learning (free of distractions & stress) and the
patient should be ready to learn (free of pain). 4. Information must be meaningful, relevant and organized. The material should be logical
in sequence. 5. The counselor must be truly interested in sharing the information. 6. Adequate follow-up should be available for reinforcement of facts and principles. 7. For adult learners, information that is useful in the present is more meaningful that facts
learned for the “future”.
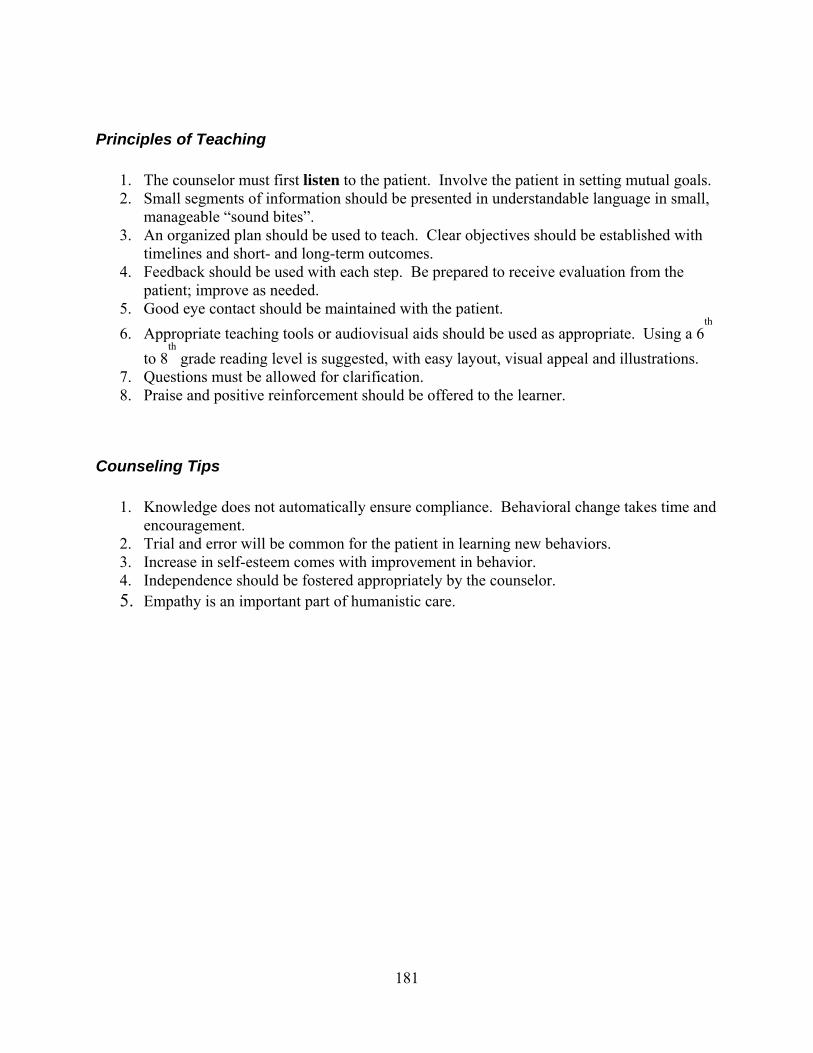
181
Principles of Teaching
1. The counselor must first listen to the patient. Involve the patient in setting mutual goals. 2. Small segments of information should be presented in understandable language in small,
manageable “sound bites”. 3. An organized plan should be used to teach. Clear objectives should be established with
timelines and short- and long-term outcomes. 4. Feedback should be used with each step. Be prepared to receive evaluation from the
patient; improve as needed. 5. Good eye contact should be maintained with the patient.
6. Appropriate teaching tools or audiovisual aids should be used as appropriate. Using a 6th
to 8th
grade reading level is suggested, with easy layout, visual appeal and illustrations. 7. Questions must be allowed for clarification. 8. Praise and positive reinforcement should be offered to the learner.
Counseling Tips
1. Knowledge does not automatically ensure compliance. Behavioral change takes time and encouragement.
2. Trial and error will be common for the patient in learning new behaviors. 3. Increase in self-esteem comes with improvement in behavior. 4. Independence should be fostered appropriately by the counselor. 5. Empathy is an important part of humanistic care.

182
Individual Nutrition Counseling in the Outpatient Setting
Introduction Individual diet counseling is the backbone of the outpatient setting. It is the antithesis of the standardized diet pattern where the client must tailor his life to a preformed intake. Central to its use is the recognition that each person's food pattern is as individual as his fingerprint and that modification of this intake should be equally individualized. NOBODY EATS THE SAME WAY Inpatient vs. Outpatient Counseling The optimum setting for discussion of long-term dietary change is in an outpatient setting. The client can focus on the role of food in his usual life pattern and can negotiate realistic changes. These can be tested and renegotiated on following visits. Environmental influences can be defined and approached. Support systems can be established and strengthened. While dietary planning in an inpatient setting is important, it can be disrupted by a crisis in the client's life. It also competes with other medical information and teaching and lacks the time and home setting to test out the plans made. The Interview In diet counseling, the setting, type and quality of interaction are as important as the content of the information provided. Setting and Atmosphere It is important that the counseling setting be physically comfortable. The room should be at a comfortable temperature, adequately ventilated, well lit, large enough for comfortable seating, with comfortable chairs and note-taking surface. The area should be relatively quiet, or be able to be shut off from noise. The emotional atmosphere should encourage the client to be at ease. Enough time should be scheduled so that the counselor need not feel or make the client feel rushed. Interruptions should be held to a minimum. If fees are a concern to the client, this should be discussed and the interview time limited to that which the client feels he can afford, allowing him to move his attention on to other issues. Interaction and Communication Food habits and patterns often have strong emotional and psychological components, and are

183
sensitive areas for many people to discuss. The interview will be seriously hampered if the client is worried that what he says will not be acceptable or will be judged. Interaction should indicate positive regard for the client and be non-judgmental in response to information given. The client needs to feel that no matter what he says, he will not be opening himself to criticism or negative comments. ("Six candy bars! No wonder you're so fat!") Questions, too, should not be leading or indicate value or a preferred response. ("You don't eat ham, do you?") Clients may be more at ease if the anticipated progression and content of the interview are described at the onset. As the client provides information, verbal and nonverbal cues from the interviewer should indicate attention, comprehension and acceptance. Verbal and nonverbal cues of attention - eye contact, body turned toward the client, nods, or "I see" - will help the client feel that what he has to say is worthwhile. Active listening - rephrasing or reflecting the ideas the client puts forth - shows comprehension and allows the counselor to check the accuracy of his understanding. Stated neutrally or supportively, reflection of the client's thoughts and feelings encourages the client to continue and be open in his communication. If the client seems to digress from the topic, he may be gently brought back on track by a question that acknowledges the importance of the information and asks how it is related to eating patterns. ("That must be a frustrating situation for you. Do you find that frustration affects your appetite?") If the situation or information presented cannot be related in any way to dietary patterns, a nod of acknowledgement or a brief reflective statement followed by a question bringing the conversation back to dietary patterns is appropriate. In this way, the client finds what he says accepted and understood and can move back to a dietary focus without feeling cut off. Occasionally, a client may be highly anxious or involved in a non-diet-related topic. In this case, dealing with dietary issues is probably not realistic. The counselor should listen to enough of the situation to make an appropriate referral or suggestion for help in dealing with the problem and suggest that dietary issues be dealt with at a later date. Although dietary planning may not take place, the visit and discussion should be recorded in the medical record. There may be instances when communication with a client may seem to be missing the mark or happening at cross-purposes. While it may be important to get specific information across, it may be more helpful to step back from the content of the communication and try to understand the process. The client may talk about unrelated things, joke about dietary measures, ignore information provided by the counselor, or in other ways seem to be hindering communication. While this seems frustrating and unproductive to the counselor, it may be very productive for the client if he wishes to avoid the topic, deny the importance of dietary measures, or simply state unwillingness to make changes. If one of these seems to be the case, it should be checked out with the client. ("From the way you joke about it, diet doesn't seem to be a priority for you at this time. Is that an accurate interpretation of what's going on here?") If the client's intent is not clear, a statement

184
such as the following may be made: "I need to back away from specifics for a moment and talk about what this visit is all about. My understanding was that we were going to plan dietary measures to help control your diabetes, but that doesn't seem to be of interest to you. What are your reasons for coming here today?" Nonverbal communication may be as important to read as a client's verbal communi-cation. Although a client may report eating a picture-perfect diet, nonverbal signals of anxiety or eagerness to please may lead you to distrust this recall. A client who says "Just give me a diet and I'll follow it," yet who sits stony-faced, arms and legs crossed, may be indicating more strongly his resistance to any externally imposed "invasion" or change. If there seems to be a discrepancy between verbal and nonverbal communi-cation, this should be explored more thoroughly. Interview Content Much of the early stages of the dietary interview are spent in data gathering. This includes details of food intake, weight history, previous dietary restrictions, the client's understanding of his disorder and the relationship of diet, and social, cultural, emotional and environmental determinants of the client's eating pattern. During this time, when the anticipated progress of the interview is being described, it is appropriate to provide or complete the patient's knowledge of the relationship of diet to his disorder and state the general goals of diet therapy. In this period, the counselor seeks not only to quantify nutritional intake, but also to understand what the experience of eating is like for the client. Since eating is a universal activity, it may be easy for the counselor to assume that the client's experience is similar to his own. This should be avoided, however, and the client encouraged to describe his experiences to a point where the counselor understands what it is like for the client. Similarly, solutions that have worked for the counselor should be shared guarded-ly, with the understanding that each person's solutions will be different. If the counselor is looked upon as an authority, clients may be quick to adopt the counselor's solution, even though it may not be the best one for their situation. It may be better to present this solution, if at all, along with others as in: "_____ has worked for some people in situations similar to yours; _____ has worked for others." The more the counselor can come to understand food and eating as the client sees it, the more realistic the suggestions that are made can be. Goal Setting Once food patterns are defined, goal setting can begin. It is probably less threatening to the client if the counselor can begin by pointing out aspects of his patterns that are already well suited to the diet to be planned. The aspects that need to be changed can then be discussed. It is important to present these changes as a means for the client to reach a goal rather than rules
185
established by the counselor. For example, a client will probably respond more positively to: "We'll probably be able to control your blood sugar better if we look for some plain desserts you would enjoy in limited amounts to replace the concentrated ones" than to "Diabetics can't eat sweets, so you'll have to cut them out. All you can have are plain cakes or cookies, and not much of them." Many clients assume that "a diet has to hurt to work," and anticipate severe restrictions. It is advisable to discuss this concept and the difference between "diets" and behavior or habit change. The long-term advantage of the latter may be stressed as well as the stepwise progression of manageable changes. Finally, it should be emphasized that since it is the patient who must live with the changes, it is only the client who can know what steps are more or less feasible and realistic and make the choices, understanding that changes that "hurt" are rarely maintained long-term. As planning is begun, unrealistic goals will be encountered. These should be discussed, and even if the client chooses to try to meet them, he should be encouraged not to think of himself as a failure if it is not met. Clients in search of "perfection" - always making the right choice, using diet foods only, never snacking, etc. - will find learning to problem solve more difficult since they are limiting their options severely and accept no compromise. As they find themselves making occasional "wrong" choices, however, the results can be assessed and the action may come into better perspective. Eventually, they may even come to accept "limiting the damage" as a good choice within a given situation. In setting any goal for change, the statement of the expected change should be specific and measurable so that the client can be certain what is expected of him. For example: "Try to eat more slowly" may be the intent but is frustratingly vague. Better stated, this goal might read: "Try putting your fork down between bites to slow your eating speed. In the first week, try to use this behavior during three meals and try to increase use by two meals each week." The second half of this goal indicates the expected rate of adaptation to the change, important in setting the stage for long-term rather than immediate adjustment. Making Decisions for Change The counselor is a facilitator, a provider of information and advice, but not the ultimate decision maker of what the client will do. Even clients who remain passive in the interview become decision makers in practice by using or not using the advice they have been given. The concept of the client as a decision maker can be introduced early in the interview in describing the anticipated course of the interview. It can be stated that, once information is gathered on the client's food patterns, the counselor will propose several ways that the dietary goals of the interview can be reached and ask the client to participate in choosing among them. It is important to remember that the client has the right to choose not to change, and that this is always one of the options open to him. This trend can be continued when the client states his reason and goals for the visit. The client's weight goal, for example, may be different from his physician's goal for him or from standard
186
weight for height from a table. This can be discussed, the client's opinion acknowledged, reasons for the discrepancy discussed, and compromise goals set. Each client's willingness and ability to change varies, not only in the physical sense but also in emotional and psychosocial areas. Clients undergoing a great deal of stress or change in other areas of their lives may not have much emotional strength left for dietary change. Priorities may need to be discussed and dietary goals postponed for a more favorable time if stressors seem temporary. If stressors seem more long-term, dietary goals may need to be broken down into small steps and planned over a long-term intervention period. While some clients may resist decision making, their investment in carrying out plans made will be greater if they can state how the dietary changes can be put into effect for themselves. They will also be more likely to make the changes if they see what they are gaining for themselves with it. It is helpful to have more than one reinforcer for the change so that no one reinforcer is depended on too greatly. It is also more productive to draw on the clients' strengths to develop strategies rather than to try and alter their weaknesses. Past successes can be explored for their common denominator, as can past failures, and the client can learn to put himself in situations that nurture success. This may help him alter common attitudes that it is "lack of will power" or "weakness" that keeps him from succeeding. If the client seems unsure how to choose from among options presented to him, this can be prompted using observations made during the interview. For example: "From what you said about really enjoying bread at night, I'd guess that it would be easier for you to cut down on potato than on bread. Is this so?" Learning Style and Teaching Tools As specific diet management steps are being negotiated, the type of tool that will be most appropriate should also be discussed. People who need structure will want a structured teaching tool such as an exchange list. Those whose sent having structure imposed upon them, or who have had difficulty in the past with such diets, may do better with specific guidelines stating changes that will bring their intake in line with the stated goals. For example, a diabetic who eats three meals, snacks on sweets, and eats 2,200 calories per day can be given a structured 1,500 calorie diet pattern or guidelines that eliminate concentrated sweets, replace them with other snacks, and outline steps to eliminate 700 calories per day. Such guidelines must be specific - one cannot assume that clients will be able to apply general principles to their own situations. Food records are a tool that may be useful. They are commonly used for clients whose eating patterns are so erratic that they are poorly defined by diet history, for those who are unaware of what their patterns or portions really are, or for those who want to explore behavioral and intake patterns to look for associations. In some instances, food records per se have led to increased awareness, concomitant decreased intake, and weight reduction. More often, they are a data-
187
gathering tool from which decisions for change can be made. Another type of tool that is useful is a specific behavioral change. If a client describes being overfull or uncomfortable at the end of a meal, and also describes eating rapidly, good results may be gained by working on techniques to decrease the speed of eating. In many instances, it will decrease caloric intake and therefore weight. It is important that the client sees how the technique will benefit him, and use it to attain specific results rather than "on faith." He will then be able to see and measure the positive result, and will be more likely to continue to use the technique. Behavioral techniques may be used in combination with other types of dietary intervention. Discussion of these techniques often seems to be more a part of "life management" than dietary management, but are nonetheless important for dietary behavior change. Common topics include controlling the eating environment (such as keeping problem foods unavailable or hidden), altering response to food cues (taking a walk at a usual snack time), planning ahead (choosing a restaurant with appropriate food choices), dealing with others (eliciting support, anticipating and dealing with sabotage, assertiveness), and supportive life skills (physical activity, relaxation, time management.) Follow-Up In planning for tools and approach with the client, feasibility of follow-up is an important factor. If the client can and will come in as often as seems necessary, follow-up can be tailored to the approach. If the client lives far enough away to be able to come in only once each month or six weeks, consideration needs to be given to this in choosing an approach. Follow-up per se is planned by what is geographically, financially, and psychologically best for the client. Some clients seek regular and frequent follow-up for support and encouragement. Others prefer to work independently and come back to "report in." In such cases, follow-up is usually much less closely spaced. These factors should be discussed and a mutually agreeable decision reached. Regularity of follow-up, however, is often associated with a high degree of success. The Client-Counselor Relationship The ultimate goal for clients is for them to "take charge"; to learn to anticipate situations and develop their own problem solving skills. Clients often expect initial visits to be fairly structured or counselor-oriented. Initially, even though the counselor encourages client participation, suggestions and potential solutions to problems may come more from the counselor. Gradually, however, the client is encouraged to develop his own solutions, checking them out with the counselor or drawing on the counselor's knowledge base for data with which to make

188
decisions. The client's role is to become the problem solver, the counselor's to use his expertise to help the client check out the feasibility of solutions. It is more useful to problem solve around anticipated rather than past events, since the solutions can be used or checked out. The goal of each situation is to make good choices within a given set of circumstances. It becomes easier if clients learn to anticipate what is coming and set the situation up to be on their side. Brainstorming can be used to list all possible solutions; then the most realistic ones be discussed. Self-Praise One of the hardest things for many people to learn is to give themselves credit for what they have done. Clients should be encouraged to take pride in any change they make and draw on their success to encourage further success. This goes hand in hand with helping clients learn to treat themselves as valuable and worthwhile, take time and make efforts for themselves, and learn to ask others for what they need. Internal and external support systems are very important to long-term success. Family Interaction At times, a client's spouse or other family member will come to the interview with him. This should be encouraged, since family support is extremely valuable. The interaction between the two during the visit, however, may indicate that the existing methods of interaction are counter-productive. It is not unusual for family members to "help" a person on a diet with controlling comments such as: "You know you shouldn't eat that" or "You shouldn't be taking seconds!" A fairly common response to this is for the client to eat whatever he is told not to, and sometimes more. It is a way of indicating his independence and control over his own intake. When interaction in an interview indicates that this kind of conflict is occurring (Spouse: "I tell him not to eat that, but he goes ahead and eats it anyway!) the counselor needs to step in. He must try to diffuse the conflict, maintain the emotional "safety" of the setting for the client, and help the couple establish more productive patterns of interaction. The counselor should acknowledge the good intentions of the family member's comments, noting that they express concern for the client's health and well-being. She can then safely point out the need in all of us to control our own actions and the natural rebellion that occurs when external forces try to control us. This, then, explains the actions of the client who, though understanding the concern, must often react to maintain control. He may find himself doing the opposite of what he otherwise would have. It can be suggested that the family member only comment on the client's intake when he sees him doing something positive and can praise and reinforce this. Occasionally, family members may seem to sabotage the client's success. This may be out of fear of changing the status quo, or misunderstanding of what the client is trying to do. This can be explored individually with the client in seeking ways for him to face the saboteur. If preferred

189
and feasible, the counselor may choose to talk to the couple or family together. Documentation The primary method of communicating with other health professionals is through the consultation report that is sent to the referring physician, and to the patient's primary care physician if referral was from a specialist. Since the plan of action is based not only on estimated nutrient intake but also on data concerning food habits and patterns, environ-mental influences, activity patterns, and client attitudes, this is all documented in the medical record. While nutrition notes on hospitalized clients are kept concise, notes in the outpatient section must often stand alone and need to supply more detail. As the basis for a long-term plan of action, the note of the initial interview is typically one to two pages long, reflecting the information obtained and given, the discussion, and planning of the hour-plus meeting with the client. Follow-up notes, which often reflect a shorter time of discussion, are similarly shorter in length.
190
The Nutrition Care Process and Model
The Nutrition Care Process (NCP) is a systematic problem solving method that dietetics professionals use to critically think and make decisions to address nutrition-related problems and provide safe, effective, high-quality nutrition care. Two great resources to assist in better understanding the NCP include:
Lacey K, Pritchett E. Nutrition Care Process and Model: ADA adopts road map to quality care and outcomes management. J Am Diet Assoc. 2003; 103: 1061-1072.
Nutrition Diagnosis and Intervention: Standardized Language for the Nutrition Care Process: http://www.eatright.org/ada/files/Nutr_Diag_and_Intervention_Publication_Fall_2006.pdf (you must be a member to access this document).
1. Describe the difference between Medical Nutrition Therapy (MNT) and the NCP.
2. Identify and define the four steps in the Nutrition Care Process and model: (1) nutrition screening and assessment; (2) nutrition diagnosis; (3) nutrition intervention; and (4) nutrition monitoring and evaluation.
191
3. List and describe what critical thinking skills are required in the Nutrition Screening and Assessment step of the NCP.
4. Provide a list of the types of documentation that should be included in the Nutrition
Screening and Assessment portion of the NCP?
5. Describe the population studied and the type of information that the following nutritional
status and nutrition-related health measurements aim to obtain, and how this information can assist in the nutrition screening and assessment steps of the NCP.
Pediatric Nutrition Surveillance System (PedNSS) Pregnancy Nutrition Surveillance System (PNSS) National Health and Nutrition Examination Survey (NHANES) USDA Nationwide Food Consumption Surveys (NFCS) Five a Day for Better Health Survey (NCI, National Cancer Institute, NIH)

192
6. Describe the population studied and the type of information that the following knowledge, attitudes, and behavior assessments gather, and how this information can assist in the nutrition screening and assessment steps of the NCP.
Behavioral Risk Factor Surveillance System (BRFSS) Youth Risk Behavior Survey (YBRS) Weight Loss Practice Survey (WLPS) Diet and Health Knowledge Survey (DHKS) Feeding Infants and Toddlers Study 2002 (FITS)
7. Distinguish between a nutrition diagnosis and a medical diagnosis.
193
8. Define the three domains – Clinical, Intake and Behavioral-Environmental – within
which nutrition diagnoses/problems may fall. Provide examples of diagnoses within each domain, and how the unique characteristics of each domain contribute to nutritional health.
9. Describe the three components of the nutrition diagnosis statement and how this statement is derived: (1) problem; (2) etiology; and (3) signs and symptoms.

194
10. Identify the Problem, Etiology, and Signs and Symptoms in the following statements.
Overweight related to intake of high fat foods resulting in more than 300 extra calories per day as evidenced by a BMI of 30.
Impaired ability to prepare foods related to fatigue as evidenced by patient only
eating 1 meal each day. Chewing difficulty related to oral surgery as evidenced by missing teeth.
Inadequate vitamin A intake related to knowledge deficit of food sources of vitamin A as evidenced by night blindness.
11. List and describe what critical thinking skills are required in the Nutrition Diagnosis step of the NCP.
12. Distinguish between the two interrelated components of the Nutrition Intervention step of
the NCP – planning and implementation.

195
13. Distinguish between and provide examples of the four main classes of Nutrition
Interventions: (1) Food and/or Nutrient Provisions; (2) Nutrition Education; (3) Nutrition Counseling, and (4) Coordination of Care.
14. List and describe what critical thinking skills are required in the Nutrition Intervention
step of the NCP.
15. Describe the difference between Nutrition Monitoring and Nutrition Evaluation.

196
16. List and describe what critical thinking skills are required in the Nutrition Monitoring
and Evaluation steps of the NCP.
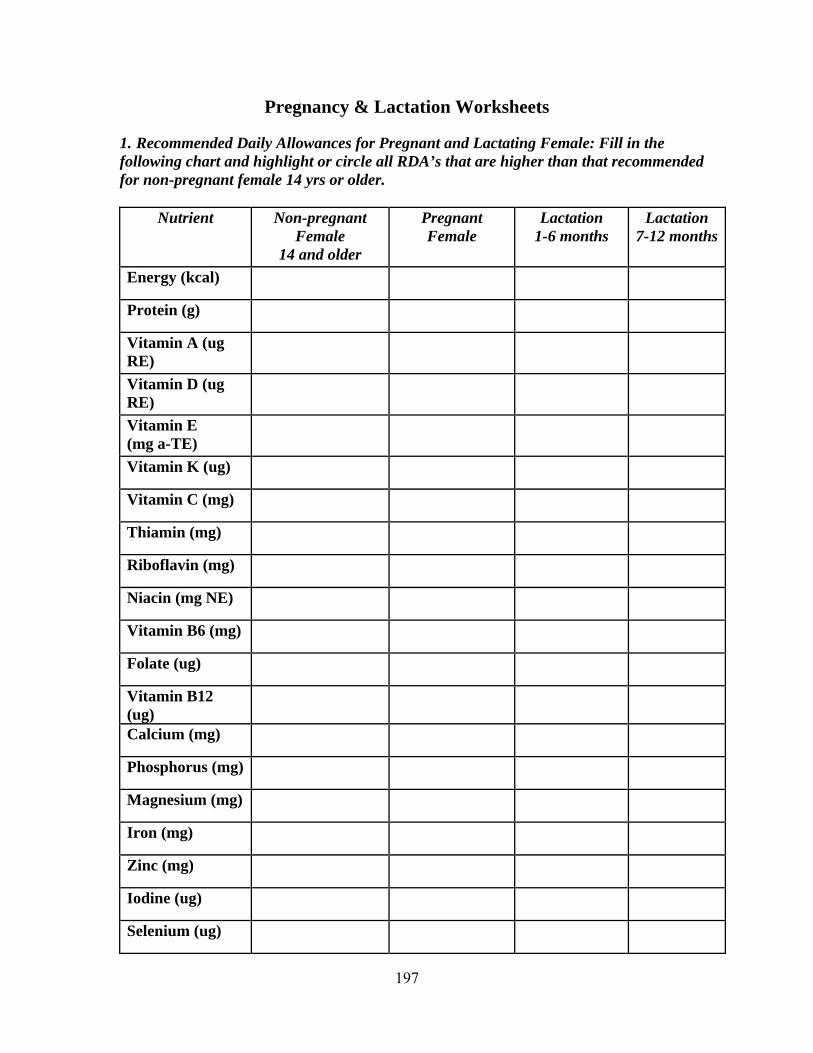
197
Pregnancy & Lactation Worksheets
1. Recommended Daily Allowances for Pregnant and Lactating Female: Fill in the following chart and highlight or circle all RDA’s that are higher than that recommended for non-pregnant female 14 yrs or older.
Nutrient Non-pregnant
Female 14 and older
Pregnant Female
Lactation 1-6 months
Lactation 7-12 months
Energy (kcal) Protein (g) Vitamin A (ug RE)
Vitamin D (ug RE)
Vitamin E (mg a-TE)
Vitamin K (ug) Vitamin C (mg) Thiamin (mg) Riboflavin (mg) Niacin (mg NE) Vitamin B6 (mg) Folate (ug) Vitamin B12 (ug)
Calcium (mg) Phosphorus (mg) Magnesium (mg) Iron (mg) Zinc (mg) Iodine (ug) Selenium (ug)
198
2. Provide user-friendly dietary recommendations for ways to increase dietary calcium,
iron and folic acid intake, including why pregnant women require extra quantities of each of these micronutrients.
Calcium:
Iron:
Folic Acid: 3. Briefly describe what nutritional recommendations you would provide for a newly
pregnant women whose pre-pregnancy weight is within normal limits. Include calorie recommendations, specific nutrients this individual should emphasize in her diet, foods to avoid during pregnancy, etc.
199
4. How do nutritional needs differ during pregnancy versus lactation? 5. Why are each of the following substances not recommended during pregnancy and
lactation: Alcohol:
Tobacco:
Artificial Sweeteners:
Caffeine:

200
Recommended Weight Gain:
Pre-pregnancy Weight Recommended Weight Gain
Underweight (<85 IBW) Normal Body Weight Overweight (>120% IBW) Twin Pregnancy
7. Nutritional Remedies for Conditions Common to Pregnancy:
Symptom/Condition Description/Cause Nutritional Intervention
Constipation
Fluid Retention/Edema
Gestational Diabetes (Hyperglycemia)
Hypoglycemia
Heartburn
Hyperemesis
201
Iron Deficiency Anemia
Leg Cramps
Nutritional Remedies for Conditions Common to Pregnancy:
Symptom/Condition Description/Cause Nutritional Intervention
Nausea and Vomiting
Pica
Pregnancy-induced Hypertension (PIH)
8. Common Tests Performed During Pregnancy:
Test Description, Time Frame and Indications
Amniocentisis
Blood Type and Rh Status and Antibody Screen

202
Chorionic Villi Sampling (CVS)
Expanded Alpha-Fetoprotein Screening (AFP)
Fetal Heart Rate Monitoring
Genetic Screening
Common Tests Performed During Pregnancy:
Test Description, Time Frame and Indications
Glucose Tolerance Test
Group B Strep Culture (GBS)
Hematocrit (Hct)
Hemoglobin (Hgb)

203
Nuchal Translucency Screening (NT)
Ultrasound
Urine Screen
Describe the advantages of breast feeding versus bottle feeding, especially during an infants
first 4 to 6 months. What are common barriers to initiation and continuation of breast feeding? What are solutions to these barriers?
Infant Formula Comparison
Standard Infant Formulas
Formula Indications Similac with Iron (Ross)
Enfamil with Iron (Mead Johnson)
Carnation Good Start (Nestle)
Parents Choice with Iron (Wyeth-Ayerst)
204
Soy Infant Formulas Isomil (Ross)
Prosobee (Mead Johnson)
Essentials Soy (Nestle)
Parents Choice Soy (Wyeth-Ayerst)
Protein Hydrolysate Infant Formulas Nutramigen (Mead Johnson)
Pregestimil (Mead Johnson)
Alimentum Advance (Ross)
Amino Acid-Based Infant Formulas Elecare (Ross)
Neocate (Scientific Hosp. Supplies)
Standard Follow-Up Infant Formulas Similac 2 Advance (Ross)
Enfamil Next Step Lipil (Mead Johnson)
205
Good Start 2 Essentials (Nestle)
Parents Choice 2 w/ Lipids (Wyeth-Ayerst)
11. Pregnancy and Lactation Medical Terminology
Abbreviation/Term Meaning AFP
BF
Colostrum
DOB
Eclampsia
EDC
FTT
G
Gest
GYN
HOG
Hyperemesis
LBW
LMP
Mature Milk
NICU
OB
Parity

206
PIH
Post Partum
Preeclampsia
SGA
SRM
Toxemia
VLBW
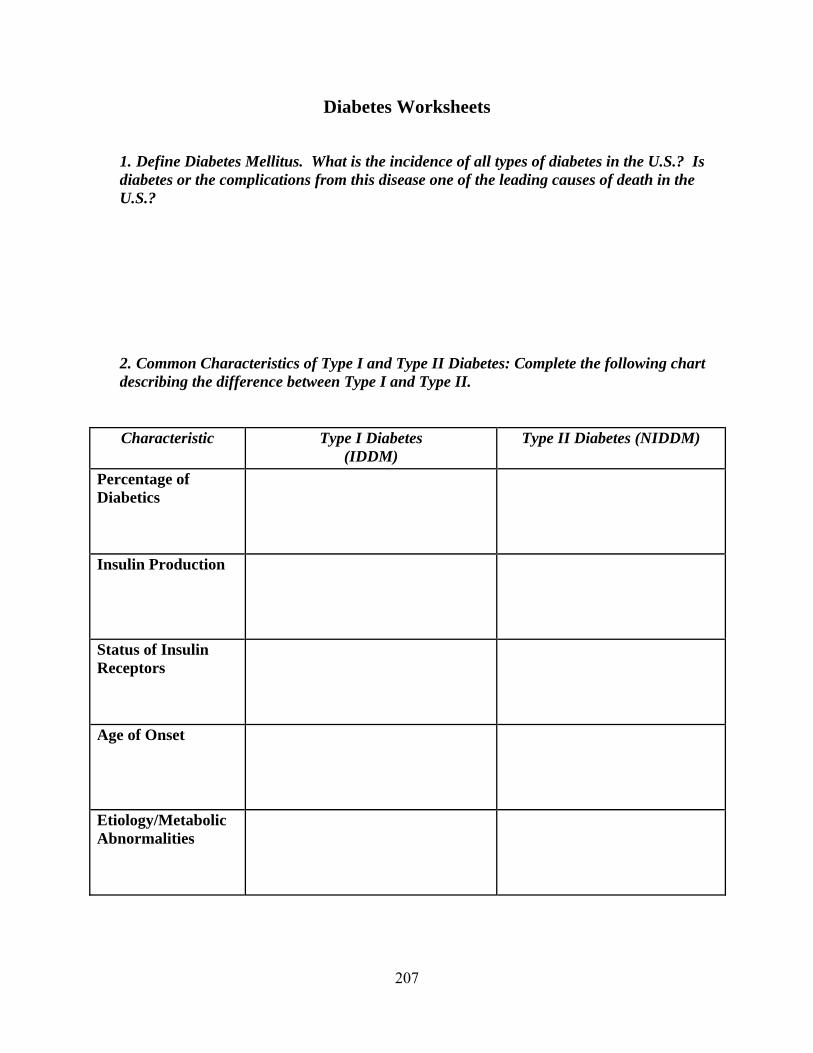
207
Diabetes Worksheets
1. Define Diabetes Mellitus. What is the incidence of all types of diabetes in the U.S.? Is
diabetes or the complications from this disease one of the leading causes of death in the U.S.?
2. Common Characteristics of Type I and Type II Diabetes: Complete the following chart
describing the difference between Type I and Type II.
Characteristic Type I Diabetes (IDDM)
Type II Diabetes (NIDDM)
Percentage of Diabetics
Insulin Production
Status of Insulin Receptors
Age of Onset
Etiology/Metabolic Abnormalities

208
Genetic Influences on Disease Development
Common Disease-related Symptoms
Rate at which Symptoms Appear
Associated Conditions
Risk of Metabolic Ketoacidosis
Possibility of Elimination of the Disease from One’s Life
Medications
Primary Dietary Objectives

209
3. Labs Important to the Diagnosis and Management of Diabetes Mellitus: Describe the following labs, including acceptable ranges for the lab measurement.
Laboratory Measurement Description & Significance Accepted Lab
Value RangeBlood Urea Nitrogen (BUN)
Creatinine
Fasting Blood Glucose
Fingerstick Blood Sugar Evaluations
Glucose Tolerance Test (GTT)
Glycosolated Hemoglobin (Hgb A1C)
Total Cholesterol, including HDL and LDL components
Triglycerides

210
Urine Glucose Tests
Urine Ketone Tests
4. Diabetes-related Complications and Symptoms: Describe the following potential
complications related to diabetes mellitus and provide solutions for each dilemma.
Diabetes-Related Symptoms
Symptoms & Causes Dietary and Medical Solutions
Chronic Renal Failure
Constipation
Diabetic Coma
Dyslipidemia
Gastroparesis
Glycosuria
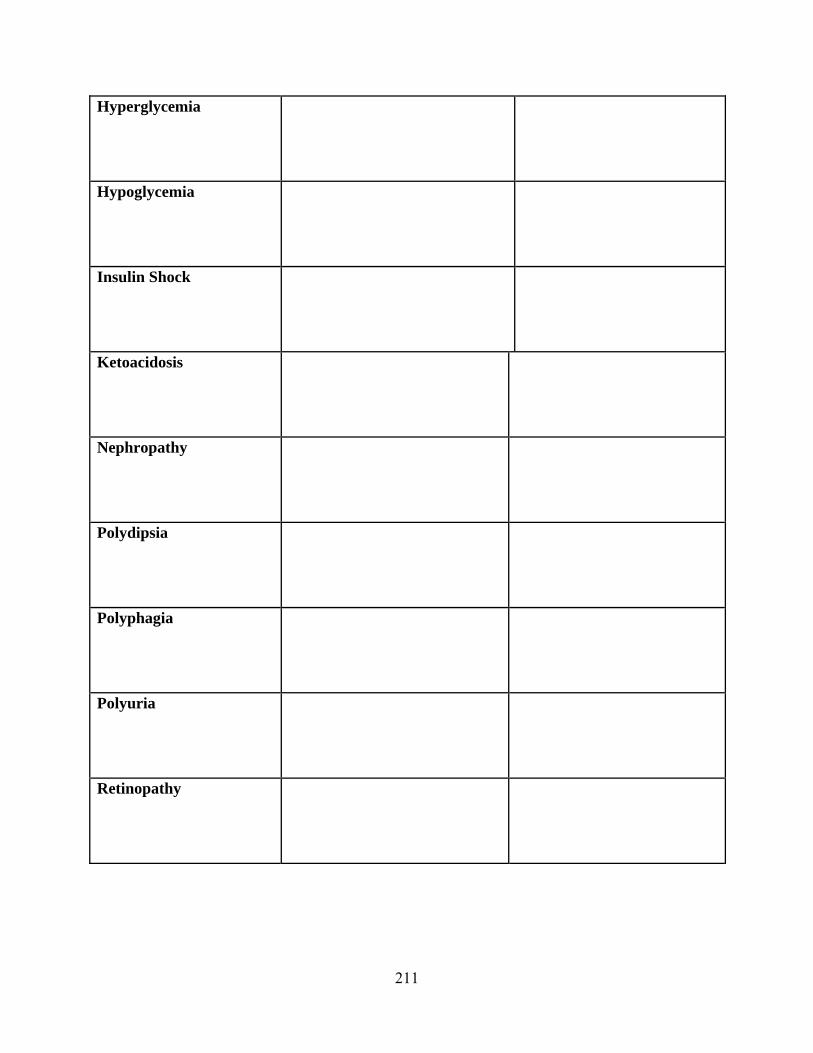
211
Hyperglycemia
Hypoglycemia
Insulin Shock
Ketoacidosis
Nephropathy
Polydipsia
Polyphagia
Polyuria
Retinopathy
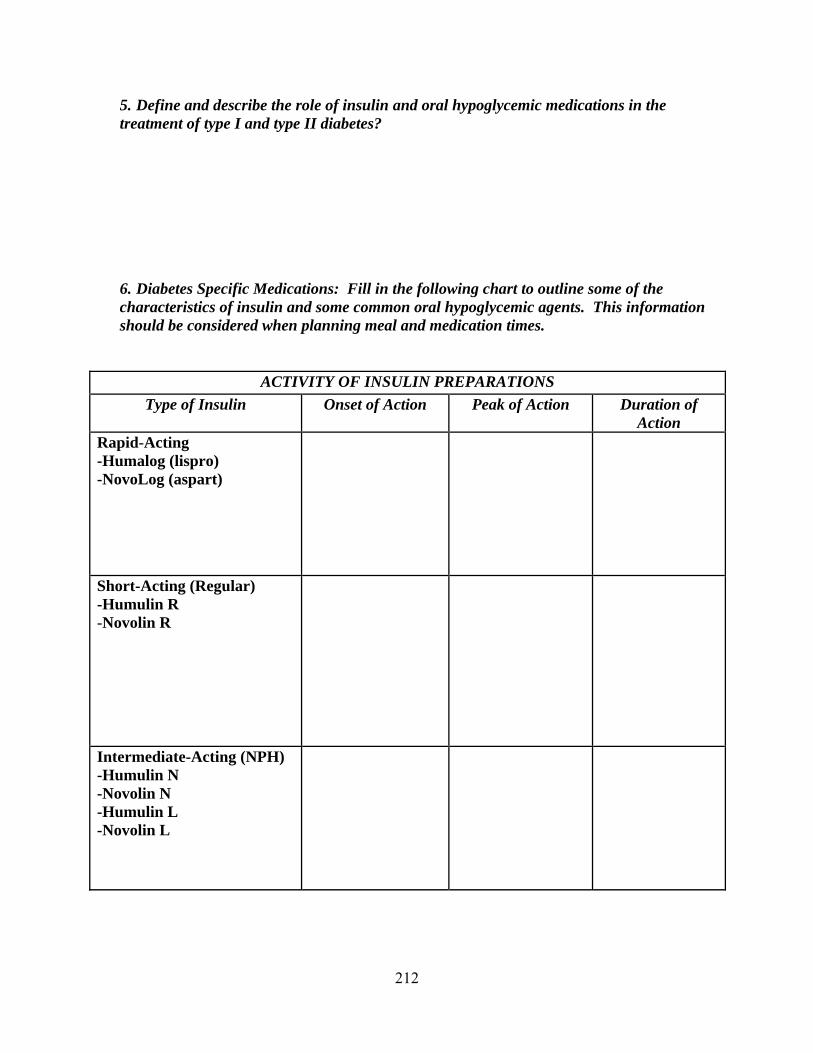
212
5. Define and describe the role of insulin and oral hypoglycemic medications in the treatment of type I and type II diabetes?
6. Diabetes Specific Medications: Fill in the following chart to outline some of the
characteristics of insulin and some common oral hypoglycemic agents. This information should be considered when planning meal and medication times.
ACTIVITY OF INSULIN PREPARATIONS
Type of Insulin Onset of Action Peak of Action Duration of Action
Rapid-Acting -Humalog (lispro) -NovoLog (aspart)
Short-Acting (Regular) -Humulin R -Novolin R
Intermediate-Acting (NPH) -Humulin N -Novolin N -Humulin L -Novolin L
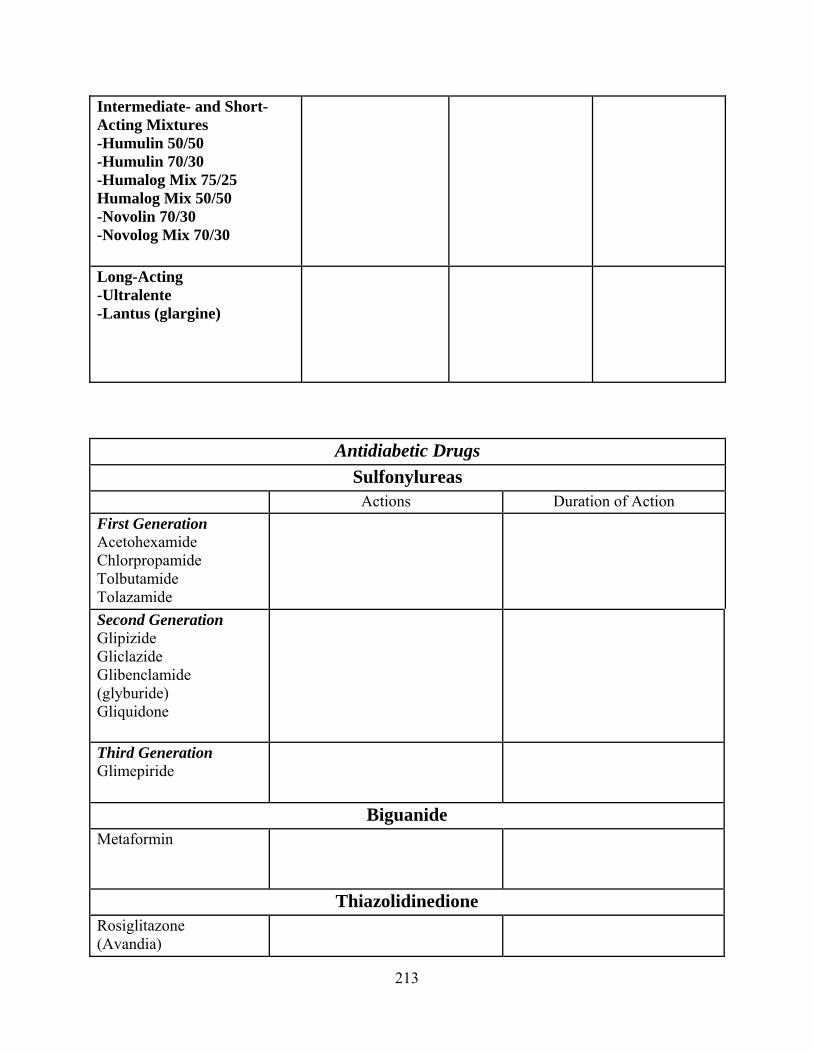
213
Intermediate- and Short-Acting Mixtures -Humulin 50/50 -Humulin 70/30 -Humalog Mix 75/25 Humalog Mix 50/50 -Novolin 70/30 -Novolog Mix 70/30
Long-Acting -Ultralente -Lantus (glargine)
Antidiabetic Drugs
Sulfonylureas Actions Duration of Action
First Generation Acetohexamide Chlorpropamide Tolbutamide Tolazamide
Second Generation Glipizide Gliclazide Glibenclamide (glyburide) Gliquidone
Third Generation Glimepiride
Biguanide Metaformin
Thiazolidinedione Rosiglitazone (Avandia)
214
Pioglitazone (Actos)
Alpha-Glucosidase Inhibitors Acarbose
Miglitol
Meglitinide Nateglinide
Repaglinide
Dipeptidyl Peptidase-4 Inhibitors Actions Duration of Action
Saxagliptin
Sitagliptin
Vildagliptin
215
7. Briefly describe the rationale for use of insulin pumps, intensive insulin therapy and multiple daily insulin injections.
8. Explain the importance and/or provide solutions for the following issues commonly
addressed as part of the dietary management of type I and type II diabetes.
a. Timing and frequency of meals and snacks
b. Managing sick days
c. Necessary changes to medication administration and food choices when physical activity is added to the equation

216
d. Alcohol’s consumption and its’ influence on the diabetic condition
e. The use of artificial sweeteners in the dietary treatment of diabetes
217
DIABETIC WORKSHEETS
The nutritional management of diabetes guides the person with diabetes in making appropriate food choices and behavioral changes that will result in improved glucose levels, improved nutritional status and self management of diabetes. Diabetic diets are intended for individuals with abnormal glucose levels due to insulin resistance or the lack of insulin. Medical nutrition therapy approaches to the dietary management of diabetes include diabetic meal patterns and carbohydrate counting. The goal of the following worksheets is to assist the dietetic intern in gaining a better understanding of these dietary approaches. NUTRIENT BREAKDOWN OF THE EXCHANGE LISTS:
Food Group Portion Size* Carbohydrate (g)
Protein (g)
Fat (g)
Energy (Kcal)
Starch/Bread Meat Lean Medium-Fat High-Fat
Vegetable Fruit Milk Skim Low-fat Whole
Fat * A more extensive list of portions sizes can be found in the appendix of most basic nutrition textbooks or ordered from the American Dietetic Association by calling (800) 877-1600 ext 5000 and asking for the booklet entitled “Exchange Lists for Meal Planning”.
218
DIET PLANNING WITH THE EXCHANGE SYSTEM: Fill in the number of servings that you would recommend from each food group for each calorie level. Use the following guidelines to calculate the following meal patterns: (1) Determine caloric needs based on usual eating habits, medications, medical condition(s),
and activity level. (2) Distribute calories as follows: Carbohydrate (g) = 55-60% total calories, 4 kcal/g, Protein
(g) = 10-20% total calories, 4 kcal/g; Fat (g) = 25-30% total calories, 9 kcal/g. (3) Convert carbohydrate, protein and fat into exchanges according to individual
preferences. (4) Distribute exchanges into meals and snacks according to medication and lifestyle.
Food Group 1,200 calories
1,500 calories
1,800 calories
2,000 calories
2,200 calories
2,600 calories
3,000 calories
Starch/Bread Vegetable Fruit Meat Milk Fat

219
Diabetes Worksheets Carbohydrate Counting
1. Describe the concept of carbohydrate counting used in diabetes management. What is
the rationale for this method? What are the advantages and disadvantages of this method versus the exchange system?
2. Determine how many carbohydrates you need using the following equations and then
make up a meal plan according to the results.
A. First determine your desired weight in pounds:
• If you are overweight, a 10% loss from your current weight is ideal.
• Desired weight = _________#
• Or base your ideal weight on this formula: • Women: 100# + (5 x ________” inches over 5 ft) = ________ goal wt • Men: 106# + (6 x ________” inches over 5 ft) = ________ goal wt
• Use this weight if you have an average frame. • For a light frame, subtract 10% = ________# • For a heavy frame, add 10% = ________#

220
B. Choose a calorie factor that best determines your activity level:
Men Women Very Sedentary 13 11.5 Sedentary 14 12.5 Moderately Active 15 13.5 Active 16 14.5 Super Active 17 15.5
C. Determine your total daily caloric need: Desired wt________# x Calorie Factor________ = ________Calories/day
D. Then divide by 8 ( ½ of calories as carbohydrate and ¼ gram per calorie) to determine how many grams of carbohydrate you need a day.
Calories/day________ / 8 = ________Grams carbos/day
E. Decide how you want to split up your carbohydrate grams for the day into different meals.
• Breakfast ________ grams • AM snack ________ grams • Lunch ________ grams • PM snack ________ grams • Dinner ________ grams • Eve. Snack ________ grams
F. Make up a sample meal plan for the day.

221
3. How would you tell your client to count their carbohydrates once you have determined their appropriate gram amount for the day?

222
Anemia Worksheets
1. What are the two main nutrients required for RBC maturation, other than protein?
2. How does a lack of folic acid lead to anemia?
3. What is the name for this type of anemia?
4. What other nutrient deficiency can cause this type of anemia?
5. What are the best sources of folic acid?
223
6. Why is there an expanded need for folate during pregnancy?
7. What is the RDA for folic acid during pregnancy? How does this compare to the RDA for a 30 year old, non-pregnant women? Why do folic acid needs increase during pregnancy?
8. Women who have prolonged use of oral contraceptives before pregnancy may be
likely to have low serums levels of folate. Why?
9. Vitamin B12
deficiency is rare, why?
10. ________________ is necessary for the absorption of Vit B12
its absence can be
inherited or acquired by two main reasons:
• ________________
• ________________

224
11. What is more commonly deficient, Vitamin B12
or Folic Acid?
12. Maternal iron deficiency does not usually result in an infant who is anemic at birth, why?
13. If the infant is not at risk, then why is iron deficiency anemia a risk during pregnancy?
14. What roll does hemoglobin play in the body?
15. Around 3-5 months, lower levels of hemoglobin are normal in the pregnant women. Why?
225
16. During which trimester does the fetus accumulate most of its iron?
17. What are acceptable levels of hematocrit and hemoglobin in pregnancy? In non-pregnant women?
18. What is the recommended level of iron supplementation during pregnancy?
19. How much iron is typically found in breast milk?
20. To diagnose anemia, you would look at the concentration of Hct and HgB, as well as the appearance of RBC. What would RBC look like in various cases of anemia (i.e. iron, B12 and folate deficiency)?
226
21. Identify the following laboratory measurements and their importance in the diagnosis of the various anemias.
a. Differential CBC
b. Platelet count
c. Mean corpuscular volume (MCV)
d. Serum ferritin
e. Reticulocyte count
f. TIBC
g. Serum iron

227
h. Serum B12
i. Serum folate
j. Schilling test
22. How long does it take for a woman to replace iron stores after pregnancy?
23. What stimulates increased blood production in pregnancy?
A. _________________
B. _________________
24. List in order the 3 most common causes of anemia.

228
SIMMONS COLLEGE DIETETIC INTERNSHIP PROGRAM
Community Health Center and Department of Public Health Worksheets Public Policy and Legislation Information
Nutrition Programs and Services Food Stamp Worksheets
Public Policy and Legislation
Nutrition policy exerts an overarching influence on the types of programs and services offered by dietitians and nutritionists in the community. It is essential that dietitians and nutritionists be familiar with the issues and the public policy process in order to provide leadership and direction to both nutrition programs and practice.
One of your core competencies (DI 4.4) requires that you “Participate in public policy activities, including both legislative and regulatory initiatives.” To meet this competency, you must participate in the activities associated with a nutrition-related bill, write testimony and/or attend and report on a legislative hearing. To find out what is going on in the nutrition world in terms of public policy and legislation, check out the following web sites:
o www.congress.org and under the Issues and Actions heading choose Health: www.congress.org/congressorg/home/ o Nutrition.gov: www.nutrition.gov/home/index.php3 o Massachusetts Public Health Association’s web site: www.mphaweb.org; o American Dietetic Association’s web site: www.eatright.org/Public/GovernmentAffairs/98_9015.cfm o FNIC’s Nutrition and Food Information Center: www.nal.usda.gov/fnic/etext/000033.html#xtocid2381827
How a Bill Becomes a Law When a senator or a representative introduces a bill, he or she sends it to the clerk of his house, who gives it a number and title. This is the first reading, and the bill is referred to the proper committee. The committee may decide the bill is unwise or unnecessary and table it, thus killing it at once. Or it may decide the bill is worthwhile and hold hearings to listen to facts and opinions presented by experts and other interested persons. After members of the committee have debated the bill and perhaps offered amendments, a vote is taken; and if the vote is favorable, the bill is sent back to the floor of the house. The clerk reads the bill sentence by sentence to the house, and this is known as the second reading. Members may then debate the bill and offer amendments. In the House of

229
Representatives, the time for debate is limited by a cloture rule, but there is no such restriction in the Senate for cloture, where 60 votes are required. This makes possible a filibuster, in which one or more opponents hold the floor to defeat the bill. The third reading is by title only, and the bill is put to a vote, which may be by voice or roll call, depending on the circumstances and parliamentary rules. Members who must be absent at the time but who wish to record their vote may be paired if each negative vote has a balancing affirmative one. The bill then goes to the other house of Congress, where it may be defeated, or passed with or without amendments. If the bill is defeated, it dies. If it is passed with amendments, a joint congressional committee must be appointed by both houses to iron out the differences. After its final passage by both houses, the bill is sent to the president. If he approves, he signs it, and the bill becomes a law. However, if he disapproves, he vetoes the bill by refusing to sign it and sending it back to the house of origin with his reasons for the veto. The objections are read and debated, and a roll-call vote is taken. If the bill receives less than a two-thirds vote, it is defeated and goes no further. But if it receives a two-thirds vote or greater, it is sent to the other house for a vote. If that house also passes it by a two-thirds vote, the president's veto is overridden, and the bill becomes a law. Should the president desire neither to sign nor to veto the bill, he may retain it for ten days, Sundays excepted, after which time it automatically becomes a law without signature. However, if Congress has adjourned within those ten days, the bill is automatically killed, that process of indirect rejection being known as a pocket veto.
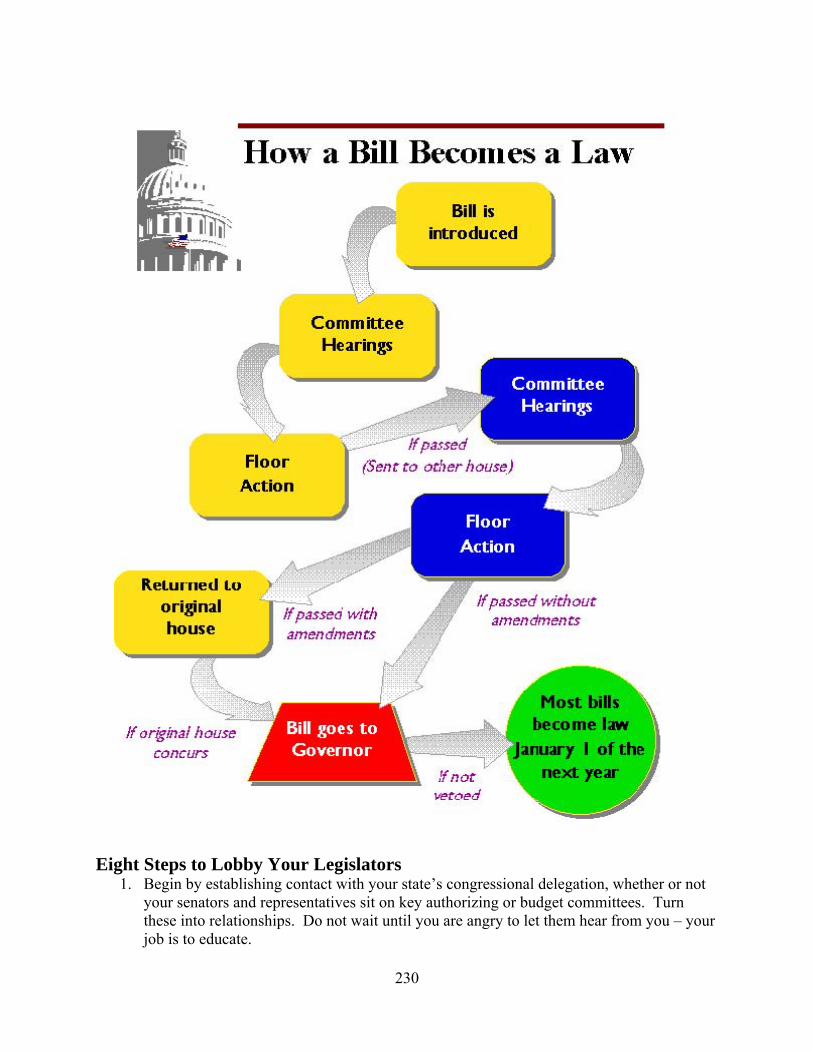
230
Eight Steps to Lobby Your Legislators
1. Begin by establishing contact with your state’s congressional delegation, whether or not your senators and representatives sit on key authorizing or budget committees. Turn these into relationships. Do not wait until you are angry to let them hear from you – your job is to educate.
231
2. Find out which members of the staff handle such issues as food, nutrition, trade,
environment and consumer affairs. Very often only one or two people will be in charge of all these issues.
3. Write to the appropriate members or staff; introduce yourself, explain your interest and the services you provide, and let them know what a vital role you or your interest plays in your community.
4. Follow up with a telephone call to make sure that the appropriate staff member received your letter and to answer any questions they might have.
5. Make an appointment to meet either the staff or your legislator - or both.
6. Prepare for that meeting. If you plan to discuss a particular piece of legislation, learn the vocabulary of that legislation and where it stands in committee (a call to the staff of the relevant committee can help here). You will also need to educate the member about your interest. Promote your agenda in a manner that leaves the member with a feeling that he wants to help. Once you are in the workplace, invite the member to tour your workplace to see firsthand the societal benefits your interest foster.
7. Prepare some brief written materials – written in lay language – to distribute at your meeting.
8. After your visit, be sure to send a thank you note summarizing the key points of your visit. Keep in touch with the office on a regular basis.
How to Write Your Representative
1. Use personal stationary with a return address on the letter as well as the envelope. 2. The purpose of your letter should be clearly stated in the first paragraph. When the letter
pertains to a specific piece of legislation, state the name of the bill. Its number, your position, and a time frame, if known.
3. Be factual and direct. Making your point in one page is desirable. Never looks like you
are writing a form letter. 4. Whenever possible, include data and sources of information to support your position.
Offer to provide additional information if necessary and thank them for considering your views.
5. Be courteous. Never be righteous, demanding or rude. Your role is to help them
understand, not to make them angry. 6. Feel free to use your own words, your own phrases, your own experience. Brief,

232
anecdotal accounts from your own experience can be very powerful if used appropriately. 7. Request the member to take a specific action: for example, report the bill favorably out of
committee, vote in favor of the bill on the floor, etc. The specific actions required are outlined on the MDA legislative alerts on their web page www.massnutrition.org .
8. Always cc the MDA office on any correspondence. 9. For a state senator, address correspondence to The Honorable (insert full name), State
House, Boston, MA. “Dear Senator (insert last name).” To a state representative, address correspondence to Representative (insert full name), State House, Boston, MA. “Dear Representative (insert last name).” For the Governor, address correspondence to “His Excellency (insert full name), State House, Boston, MA. “Dear Governor (insert last name).”
10. Remember, government officials work for you. Members and their staff are strongly
influenced by the correspondence they receive. How to Contact Your Legislator by Phone
1. Try to discuss the issue directly with the legislator. If you can’t speak with the Legislator, ask to speak with a Legislative Assistant.
2. Identify yourself, where you are from, what bill and issue you are calling in reference to,
and the time frame on the bill. It is important that you know the bill number and reference in your conversation. You should also reference the bill by the issue it deals with. Many thousands of bills are introduced in any session – the bill number, without any subject reference, may not “ring a bell”.
3. Often you will not be able to speak directly with the member. This does not mean your
phone call is unimportant. Sharing your comments and opinions with the aides is equally significant. Most offices keep track of how many constituents call on an issue and share this information with the member before they vote.
4. Never call the State House without leaving a message with your name, number, where
you are from, and your position! Don’t just leave your name and number: state your position – in favor or opposed to a measure. These get counted too! Nine out of ten times you will get a call back.
5. Keep the phone call short and friendly. You should make five points:
a. Tell them your position on the bill (in favor, or opposed).
b. Tell them why you, as a dietitian, oppose or support the bill in terms of your practice or experience. This should not be a long story, but, as a dietitian who practices, or lives, in their district, simply explain why you know this proposal
233
will help/hurt your profession. Remember: one of the most important factors is how a bill will affect a legislator’s constituents.
c. Request that the legislator take a specific action. For example, ask the member to
vote in favor of a measure, help move the bill out of committee, etc.
d. Ask the legislator’s opinion.
i. If the legislators position is the same, express your support and thank them.
ii. If the legislator disagrees, politely express your disappointment. If there is time, offer to send them factual information supporting your views.
iii. If the legislator does not have an opinion, explore his/her concerns (depending on the time available), and offer to send additional factual information.
e. Never press the legislator or aide who has not taken an opinion and never, never
argue with a member or aide! Ask the legislator’s opinion.
f. Thank the legislator or aide for his/her time in considering your views. Tips On Meeting With A Legislator
1. A personal visit with a legislator is an effective way to emphasize your interest in an issue or bill. Some tips for meeting a legislator in order to urge support or opposition to legislation are as follows:
2. When making an appointment, state the subject to be discussed, the time required, and identify all persons who will attend.
3. Select a spokesperson if there is a group. Discuss and agree on your presentation ahead of time.
4. Know the facts, both legislatively and how it relates to your profession. If you are discussing a bill, know the current number and title.
5. Present the facts in an orderly, concise, positive manner.
6. Relate the positive impact of legislation you support and identify problems it will correct.
7. Relate the negative impact of legislation you oppose and suggest, where appropriate, a different approach.
8. Leave concise fact sheets, if possible.
9. Encourage questions and objective discussion.
234
10. Politely request favorable consideration of your issue, thank the legislator for his/her time and courtesy, then leave promptly.
235
Community Health Center Rotation
Demographic & Data Collection Assessment
Complete the following worksheet using information about the community you are located in for your community health center rotation. It would be to your benefit to complete this assessment prior to your rotation so that you are familiar with the population you will be working with and the resources available to this population. Resources you may use include the Boston Redevelopment Authority, Boston Public Library, Government Publication Room at the State House, and Census data. Additionally, each health center often has a summary of their community demographics which will be helpful. You can even take a walk around the community to get a better feel for the population and resources available. 1. What is the name and location of the community health center? 2. What is the population of the community? Total__________ Men__________ Women__________ 3. What is the age breakdown of the population? 4. What is the racial and ethnic breakdown of the population? White, Non-Hispanic__________ Black, Non-Hispanic__________ Hispanic__________ Asian__________ Other__________ 5. What are the main languages, other than English, that are spoken in this community?
236
6. Do the food preferences of this community differ from that of the average American?
If so, what are the major differences (i.e. food preparation, types of foods consumed, timing and frequency of meals, etc.).
7. What are the major health concerns common to this community (i.e. diabetes, cancer,
heart disease, etc.)? Which can be addressed via nutrition counseling? 8. What is the average family size?_______________ 9. What is the average income level?_______________ 10. What percent of the population is at or below 100% of the poverty
level_______________ 11. What type of housing do you see? What is the general condition of the housing
available?
237
12. How many individuals does your health center serve? Is this where most people in the
community receive their health care? If not, where else is health care provided in the community?
13. Is there a WIC program in the community? Give the location. How many women,
infants and children are served by the program in this community? 14. Is there a welfare (transitional assistance) office in the community? Give the location
and telephone number for the food stamp program. 15. Are there local soup kitchens and food pantries? Give their location. 16. Name the supermarkets in the community. Do they carry WIC approved foods and do
they accept WIC checks?

238
17. Does the community offer the Massachusetts farmers’ market coupon program? If so,
what are the locations of the farmers’ markets?
18. Is public transportation available to the health center, WIC program, welfare office, grocery store, etc.? What type?
19. Given the information you have collected, briefly describe some of the nutrition and
health problems you would expect to encounter in this community. What resources are available to deal with these problems, and what resources are lacking or inaccessible? Identify one or two strategies that could be used to alleviate some of the nutrition- or health-related problems in this community.
239
Community Health Center Rotation
Nutrition Programs & Services Worksheet
1. Describe the difference between a nutritional survey and nutritional surveillance. 2. Describe the following nutritional surveys (i.e. goals for data collection, past survey
results, significance of the results to the field of dietetics). Ten State Survey (1970) National Health and Nutrition Examination Survey (NHANES-Ongoing) USDA Household Food Consumption Surveys (Ongoing)
240
3. Describe the following federal programs and answer the basic questions outlined below
for each program: What federal organization supports the program? What is the programs target population? What are the programs eligibility guidelines? What nutritional services does the program provide? If supplemental foods are distributed, where are they obtained from and what types of
foods are generally provided?
A) School Breakfast and Lunch Programs (Child Nutrition Act)
B) Special Milk Program
C) Child Care Food Program

241
D) Headstart
E) Older Americans Act - Title IIIC
F) Medicare
G) Medicaid

242
4. Describe home delivered meals. Who is eligible for these meals?
5. What are congregate meals? Who is eligible? 6. Describe a food pantry and soup kitchen. How do they fit into the emergency food
network? Who is eligible?
243
Community Health Center Rotation
Supplemental Nutrition Assistance Program Worksheet 1. After applying for SNAP and providing all the required documentation, how long
should it take for an eligible applicant to receive the stamps? 2. What are the income requirements for SNAP eligibility? What are the exceptions to this
income requirement? 3. While receiving SNAP, if you are unemployed or working less than 20 hours a week you
must “register” to work. Who are the exceptions to this case?
A. B.
4. Do you need a permanent address to receive SNAP?

244
5. Can homeless people receive SNAP?
6. Which members of the family applying for SNAP require social security cards? If you
do not have proof of citizenship, can you receive SNAP? 7. Once you become eligible to receive SNAP, how long do you remain certified? 8. List the items you can and cannot purchase with SNAP.

245
Community Health Center Rotation
Case Study
A pregnant Haitian women, age 23, has just arrived in this country with her children ages 2, 5 and 7. Mrs. Jean-Pierre is staying with her cousin in an uncomfortable living situation. The only provision is shelter because Mrs. Jean-Pierre’s cousin can barely feed her family let alone worry about feeding four other mouths.
What federal programs is Mrs. Jean Pierre eligible for? List the potential sources of food
and income that Mrs. Jean-Pierre and her children can receive. Utilize these foods and resources to develop a meal plan. Can the food and income resources available to this family ensure proper nutritional status? Will the food or income resources change when the infant is born?

246
SIMMONS COLLEGE DIETETIC INTERNSHIP PROGRAM
Foodservice Worksheets Food Service & Management Rotation
Types of Foodservice Systems 1. Describe the advantages and disadvantages of the following types of foodservice
systems: Conventional
Commissary
Ready-Prepared (Cook-Chill)
Assembly Serve

247
Food Service & Management Rotation
The Menu 1. Why is the menu considered the primary control of the foodservice operation?
2. Describe the following types of menus: Static
Cycle
Single-use
Degree of Choice 3. Describe how the following factors influence menu planning: clientele, nutritional
influence, physical facility, personnel, budget, aesthetics, external factors (climate, seasons, etc.).

248
4. Describe the following three methods for pricing menus:
Factor Method
Prime Cost Method
Actual Cost Method

249
Food Service & Management Rotation
Purchasing 1. Describe the following types of middlemen involved in the purchasing process:
Wholesalers
Brokers
Commissioners
Manufacturers’ Representatives
Retailers

250
2. Define forecasting and its importance in the purchasing process. 3. Describe how the following factors can affect the accuracy of forecasts: availability of
resources (money, personnel, raw materials); technological, societal and governmental changes; economic outlook; and population trends.
4. Describe value analysis and make-or-buy decisions. How are these techniques used by a
purchaser to procure required products for minimum cost? 5. What’s the difference between informal and formal purchasing? 6. What is bid buying? 7. What’s the difference between a purchase requisition, purchase order and invoice?

251
Food Service & Management Rotation
Receiving, Storage & Inventory Control 1. Describe the significance of the following steps in the receiving process:
Inspection against the purchase order Inspection against the invoice Acceptance or rejection of orders Completion of receiving orders Removal to storage
2. What’s the difference between invoice receiving, blind check receiving and partial blind
receiving?

252
3. Describe the following types of storage facilities and equipment:
Storage Facility/Equipment
Description/Ideal Features Foods Commonly Stored Here
Proper Temperatures
Dry Storage Facility Coolers
Thawers or Tempering Boxes Storage Freezers
Processing Freezers
4. Define inventory. Why is the development and maintenance of an inventory system
important? What’s the difference between physical inventory and perpetual inventory?
253
5. Define issuing. What’s the difference between direct issues and storeroom issues? 6. Describe the following tools available to assist managers in determining quantities for
purchase, inventory levels, and cost of maintaining inventories: ABC Method
Mini-Maximum Method
Economic Order Quantity Method 7. Describe the significance of the following methods for inventory valuation:
Purchase Price

254
Weighted Average Purchase Price FIFO
LIFO

255
Food Service & Management Rotation
Production Planning & Control 1. Define production. 2. Define production demand forecasting. How does this help with cost control in a food
service organization? 3. What are production meetings? What topics are discussed at these meetings? 4. Describe why employee scheduling, standardized recipes, and quality and quantity
control are so important to production control?

256
5. What are the cup and ounce measurements for the following scoop sizes?
Scoop Size Measure (cup, tsp, tbsp) Ounces
# 6
# 8
# 10
# 12
# 16
# 20
# 24
# 30
# 40
# 60
257
Food Service & Management Rotation
Methods of Production 1. Describe the following pieces of equipment common to food service establishments. Put
a check in the last column if your food service facility possesses the particular piece of equipment.
Equipment Function/Description
Bainmarie
Blender
Broiler, Char or Open Hearth
Convection Oven
Deck Oven
Dolly
Dough Mixer
258
Griddle
Hot Plate
Kettle, Steam Jacketed
Kettle, Tabletop
Microwave Oven
Oven-top Fryer
Pre-rinse or Pre-wash Sink
Pressure Cooker
Range Oven
Roll-in Rack Oven

259
2. Describe the following cooking methods. Cooking Method Description Appropriate Foods
For This Method Inappropriate Foods
For This Method
Moist Heat Methods
Blanching
Boiling
Braising
Poaching
Simmering
Steaming
Stewing
Dry Heat Methods
Baking

260
Barbecuing
Dry Heat Methods
Broiling
Charbroiling
Deep Frying
Grilling
Oven Frying
Pan Frying
Roasting
Sauteing
261
Food Service & Management Rotation
Foodborne Pathogens 1. Describe the difference between the four major types of food spoilage:
Microbiological
Biochemical
Physical Chemical
2. What’s the difference between foodborne poisoning/intoxication and foodborne
infections?

262
3. Fill in the following chart identifying major foodborne illnesses.
Foodborne Pathogen
Foods Usually Involved & Time
Frame for Onset of Symptoms
How Introduced Into Food
Preventative or Corrective Procedures
Food Poisoning/Intoxication
Staphylococcus Aureus
Clostridium Botulinum
Clostridium Perfringens
Foodborne Infections
Salmonella
Streptococcus
Listeria Monocytogenes
Campylobacter Jejuni

263
Food Service & Management Rotation
1. Describe the following laws and regulations involved in the employment process.
Unemployement Compensation
Workman’s Compensation
National Labor Relations Act (Wagner Act-1935)
Taft Hartley Relations Act (Labor Management Relations Act-1947)
Labor Management Reporting and Disclosure Act (1959)

264
Fair Labor Standards Act (1938)
Civil Rights Act (1964)
Age Discrimination Act (1967)
Equal Employment Opportunity Act (1972) 2. Define the following concepts involved in job design.
Job Description

265
Job Analysis
Job Specification
Work Schedule
Job Breakdown 3. Describe the following types of personnel actions.
Promotion

266
Transfer
Separation
Compensation (salary vs. wage)
Benefits (statutory vs. compensatory vs. supplementary) 4. Describe the following motivational theories, strategies and studies commonly used as
leadership tools. Maslow’s Hierarchy of Needs
267
Herzberg’s Theory
Macgregor (Theory X and Y)
Hawthorne Studies (Western Electric) 5. Describe the difference between the following leadership styles.
Autocratic
Bureaucratic
268
Diplomatic
Participative
Free Reign 6. Describe the five primary management functions: Planning, Organizing, Staffing,
Leading/Directing and Controlling.
269
7. What’s the difference between the following types of work schedules?
Master Schedule
Shift / Staggered Schedule
Production Schedule
8. What are the three major costs in a food service operation? Which is the least controllable? The most manageable?

















