58
Simulation Based Medical Education Trevor Langhan PGY-4 Masters of Medical Education Candidate University of Calgary
| Date post: | 24-Dec-2015 |
| Category: |
Documents |
| Upload: | carol-price |
| View: | 215 times |
| Download: | 0 times |

Simulation Based Medical Education
Trevor Langhan PGY-4Masters of Medical Education Candidate
University of Calgary

Rounds Outline
• Ethics of Simulation Based Medical Education• Uses of Simulation Based Medical Education• Procedural skill acquisition with simulation techniques• Local initiatives in Simulation Based Medical Education
research

Medical Education
“medical teaching must at some point use live patients to hone the skills of health professionals.”
• Balanced with the obligation to provide optimal treatment and to ensure patient safety
• Traditional apprenticeship model has learners receiving guided instruction during skill acquisition
“see one, do one, teach one.”

Why Simulation?
• 1999 Institute of Medicine report – – ‘to err is human’– Highlighted the cognitive and technical errors in
medical education
• Patient safety became an important agenda item– Licensing and governing bodies challenged to
improve physician confidence and patient safety

Ethical Themes of Simulation
1. Best standards of care and training
2. Error management and patient safety
3. Patient autonomy
4. Social justice – resource allocation
“patients are to be protected whenever possible and they are not commodities to be used as
conveniences of training.”

1. Best Standards
• Best standard for patient care– First do no harm to patients
• Using patients as learning instruments is only justified when all approaches to minimize risks have been taken
– Simulation allows trainees’ first encounters with real patients to be at higher technical and clinical proficiencies

1. Best Standards
• Best standard for education– Responsibility of educators to provide clinicians with
best training• Best standard for evaluation
– Traditional evaluation focused on cognitive domain– With simulation can assess attitudinal and
psychomotor as well

2. Error management
• Even with supervision it is inevitable that trainees cause preventable injuries
• In clinical setting errors must be stopped promptly• In simulation errors may be allowed to progress• Errors can occur at any level in medical education
– SBME has uses in UME, PGME, CME
3. Patient Autonomy
• Patients have the right to direct their own care• Historical reports of procedures or physical exam skills
being practiced on:– Deceased– Drugged– Anesthetized

4. Social Justice
• Basic principle of distributive justice states:– Citizens equally share the risks of medical innovation,
research and practice training• Most teaching institutions are urban and provide
disproportionate care to the poor and under privileged• SBME may help equilibrate this imbalance

Simulation Based Medical Education
• Simulation is a complimentary teaching method in the medical profession:
“any educational activity that uses simultative aids to enhance medical educational message”
“not to replace traditional methods, but to add to”

Anesthesia Sim1986
1990 and now
Interactive2000s
Resus Annie1960
Mannikins cadaver
Task trainer Virtual Reality
SBME - uses
• As described by Ziv:– ‘hands on’ uses to teach clinical skills– CME tool for practicing MDs– Teamwork training to enhance patient safety– Introduction of new technologies in safe manner– Ultimately may be used for assessment for licensing
and certification– In broad range of situations
• Traditional classrooms, home PC, simulation suites

What is Simulation?
• Simulation is a technique – not a technology• Use in Medical Education is to:
“replace or amplify real experiences with guided experiences that evoke or replicate aspects of the real
world.”

What is Simulation?
• Simulation is defined as:
“the representation of the operation or features of one process or system through the use of another.”
“the artificial replication of sufficient components of a real-world situation to achieve certain goals.”
What is Simulation?
• Simulation is a representation of reality• How well does it represent actual clinical reality?
• A question of fidelity
What is fidelity?
“is the extent to which the appearance and behavior of the simulation match the appearance and behavior of the simulated system”
“precision of reproduction, the extent to which an electronic device, for example, a stereo system or television,
accurately reproduces sound or images”

A. Ziv’s definition of High Fidelity
1. Screen based simulator• May or may not interact
2. Procedural simulators (task trainers)• Static models with tactile cues
3. Realistic Patient Simulators4. Virtual reality
• Evolving technology• Combine virtual world with simulation +/-
standardized patients to form microsystems

A. Ziv’s definition of Low Fidelity
1. Simple 3-D models
2. Animal models
3. Human cadavers• Realistic but lack physiologic response
4. Basic Plastic Manikin• Simple skills trainers• Physical exam teachers • Clinical skills teachers
5. Simulated or standardized patients• Best for clinical skills teaching
Low Fidelity
• If simulation is a manifestation of reality• And some models have “low fidelity”
– Or poorly mimic reality
Can they make any difference?
i.e. Do they change behavior?

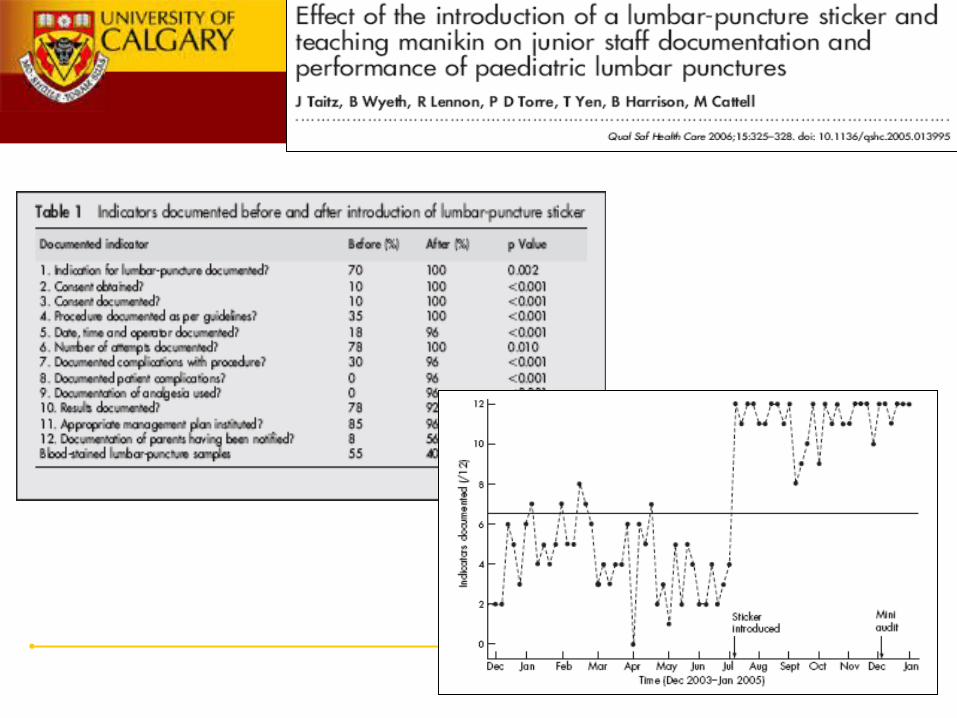
• Reviewed 40 consecutive charts in preceding 6 months• Intervention was a instruction of LP on manikin and proforma• Prospectively reviewed 25 next consecutive patient charts
• Findings:– 4/12 clinical markers improved to 12/12 (p<0.01)– Improved charting– Change in behavior of junior staff
• Limitations:– Hawthorne effect– No change in % of traumatic taps
• What can be the effect of Low Fidelity training?• Are skills learned on ‘non-realistic’ or ‘non-interactive’
models not transferable to real clinical life?
“Learning transfer is the application of skills and knowledge learned in one context to another context.”

• The authors have published a number of small studies touting the benefit of Low-fidelity simulation
• Stating:
“to ensure success with skill transfer need to identify the essential construct inherent to the relevant procedure”
“low fidelity models can then be developed to fit the procedure”
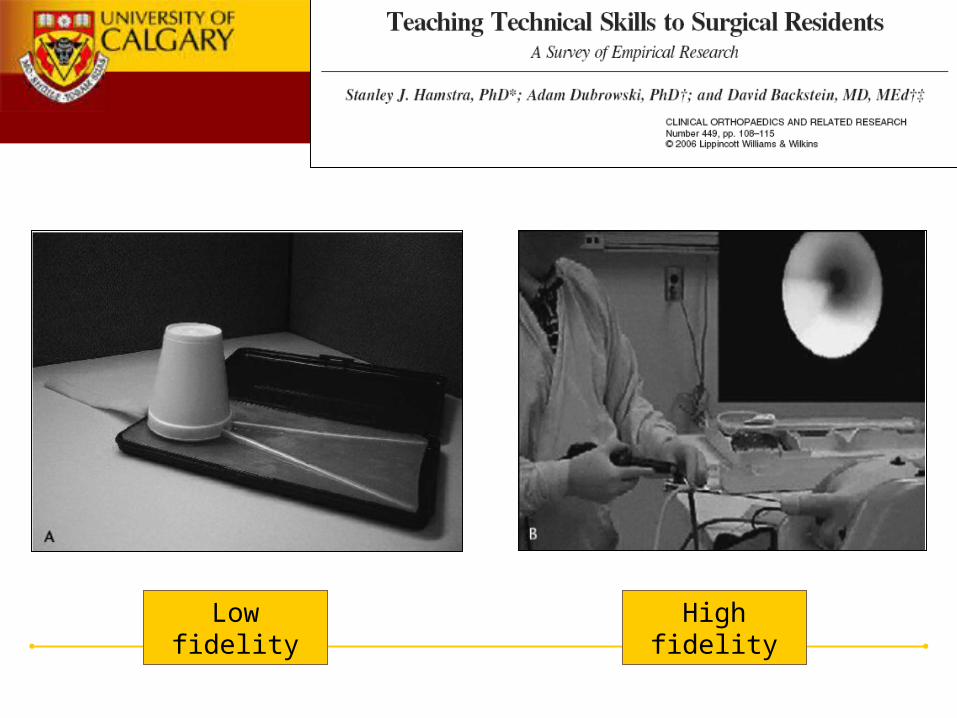
• 40 final year medical students– Assigned to low-fidelity, high-fidelity, didactic group
• Trained to remove stone from mid-ureter• Performance measured on expert rating scale and time
to completion• Hands-on far superior to didactic
– No difference between low and high fidelity
Low Fidelity
• If there has been some gain in procedural skill with low fidelity simulation
• Is that skill retained?• Does the retention last as long as with Higher Fidelity
training?

• 18 surgical residents re-evaluated on high fidelity model 4 months after randomization to didactic vs. low vs. high fidelity training

Theory
“to ensure success with skill transfer need to identify the essential construct inherent to the relevant procedure”
• Has some cross over to Experiential Learning Theory• Not as clear in regards to generalizability and application
“focus training on the process and ask trainees to suspend disbelief about the physical substrate”
Theory

• The developers of simulators are not driven by the same agenda as those who are using them
• Ravert et al. (2002) literature search:– Quantitative studies on simulation – 513 references– 9 studies since 1980 met criteria– Of those 75% had positive effect of skill acquisition
“we must not allow technology to drive the educational agenda but rather pursue the development of technology
which will assist developing areas of identified training need”

• STEPS:
1. Develop a curriculum
2. Learners prepared with cognitive knowledge of procedure
3. Techniques then demonstrated with clarifying commentary
4. Learners then directly observed performing the skill
5. Repetition encouraged
6. Encourage learner self-assessment (reflection)
7. Formative feedback imperative
Local Research and Work in SBME
• Hemodynamic instability is a common clinical encounter in Emergency Medicine
• Procedures and interventions require a confident skilled hand
• Can’t delay a needed procedure in an unstable patient• By definition, resuscitation skills are not indicated in
stable patients• ? How do junior learners (or CME docs) gain these
skills?

Local Research and Work in SBME
• Hemodynamic Instability Course (HIC)– Dr. Lord– Dr. Rigby– Dr. Walker– Dr. Dan Howes
• Many local guest lecturers/facilitators

Methods
• We undertook a prospective trial to assess the impact of a hemodynamic instability course.
• Research Question: – Does Moderate Fidelity Simulation Training in
Resuscitation Procedures Improve Residents’ Self-Assessed Competence?
• Prospective convenience sample of 37 University of Calgary residents
• Intervention: – 8 hour intensive simulation based training course on the
management of hemodynamically unstable patients

Methods
• Survey questionnaire applied to each resident:– Scored a variety of self-assessment questions on a 5
point Likert scale• Pre-intervention• Post-intervention
– Expert assessment during study on IJ placement station on manikin (OSCE format)
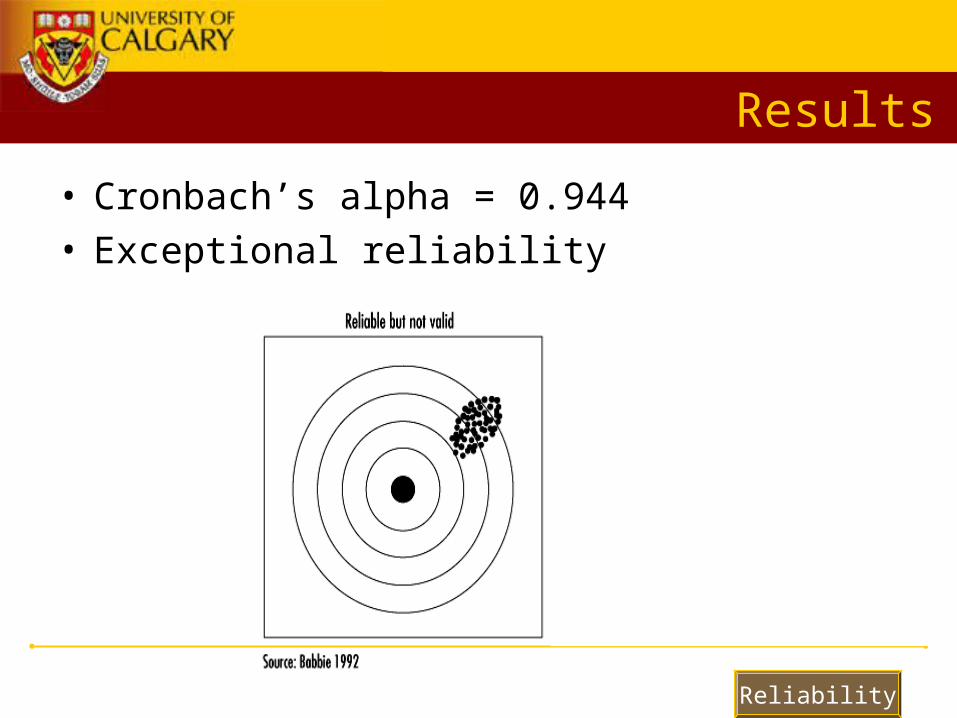
• Statistical tests used:– Pearson’s correlation coefficient– Descriptive statistics (mean, range, SD)– Cronbach’s alpha (Reliability)– Paired sample T tests (compare pre and post)

Results
Male Female Total Excluded Analysis
FRCPC 6 3 9 - 9
CCFP-EM 3 1 4 - 4
CCFP 8 10 18 1 17
GIM 2 4 6 1 5
37 35
• 2 Residents excluded from analysis– 1 GIM : did not have expert assessment station– 1 CCFP : did not complete the post-intervention assessment

Results
• Participant demographics:– Age: mean 30.65 (range 25-44 years)– 72% were PGY 1 or 2 (27/37)
• CCFP-EM and FRCPC residents– 3rd year or above residents (n=10)

Correlation Matrix
Expert Overall
ImpressionSum general confidence CVC confidence
Sum of Expert assessment
scores
Expert Overall Impression
Pearson Correlation 1
Self-assessed General confidence
Pearson Correlation .558(**) 1
Sig. (2-tailed) .000
Self-assessed CVC confidence
Pearson Correlation .689(**) .813(**) 1
Sig. (2-tailed) .000 .000
Expert assessment scores
Pearson Correlation .787(**) .478(**) .485(**) 1
Sig. (2-tailed) .000 .004 .003 .000
Results
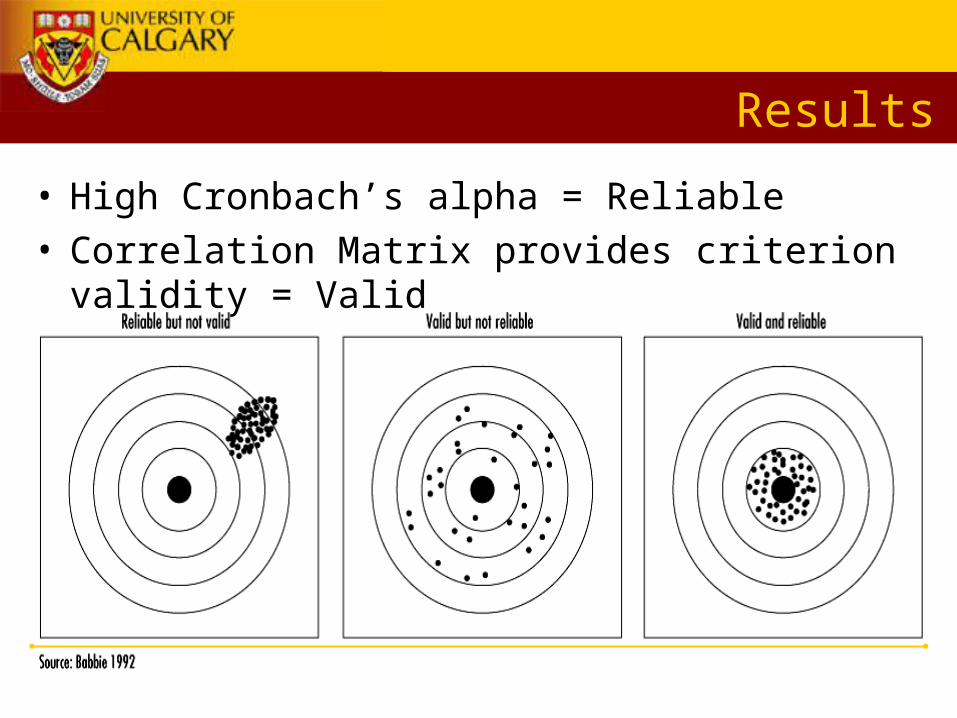
• High Cronbach’s alpha = Reliable• Correlation Matrix provides criterion validity = Valid

Self-assessment Pre & Post HIC
Paired Sample T tests
Mean
Std. Deviation
95% Confidence Interval of the Difference
Sig. (p<0.05)
General Confidence Pre & Post
2.54 3.03 3.59 1.50 .000
CVC Confidence Pre & Post
6.77 4.49 8.32 5.23 .000
Transfusion Medicine Confidence Pre & Post
2.06 1.23 2.48 1.63 .000
Vasopressor ConfidencePre & Post 2.31 1.65 2.88 1.75 .000
Intraosseous Line Confidence Pre & Post 3.23 2.26 4.01 2.45 .000

Conclusions
• Our data suggests that:
• Simulation based procedural skill training can improve self-assessed procedural skill competence
• In our sample, self-assessed competence was highly correlated to assessment by an ‘expert’ observer providing criterion validity to self-assessed skill
• Simulation training allows repetition and practice in a safe environment without compromising patient safety
Limitations
• Local study – may not be externally valid• Intensive 8 hour session may be the difference, not the
act of simulating the procedure• Known biases in Likert scales:
– ‘central tendency bias’ – ‘acquiescnce response bias’– ‘social desirability bias’
• Unsure of ‘Knowledge Transferability’

Future Directions
• Will apply the self-assessment instrument to residents again in April 2007 for assessment of ‘retention of knowledge’
• Presentation at CAEP• Manuscript preparation
• HIC will be touring to Western Canadian sites to promote rural MD training and CME

SUMMARY - Pitfalls of SBME
1. Culture in medicine is resistant to change
2. Match educational goal & learner with appropriate model
3. Need to train the trainers
4. Quantitative testing and assessment to prove validity
5. Sustainable business model
6. Prove cost reduction to health care with minimizing medical error

Summary
• Reviewed Ethical reasons to pursue SBME• Defined simulation and fidelity• Examined current research and learning theory of
procedural skills simulation education• Listed advantages to SBME• Briefly listed potential pitfalls

Experience
Something happens! Reflection
What happened?
Generalization
Why did it happen?
Application
Now do it!
(Kolb: Experiential Learning -Experience as the Source of Learning and Development (1984))
Experiential Learning Cycle
Theory

• Learning in medical education is opportunistic• Clinical expertise is a complex phenomenon• No single theory can account for it’s acquisition• Argues for a closer relationship between task based
practice and clinical reality
Theory
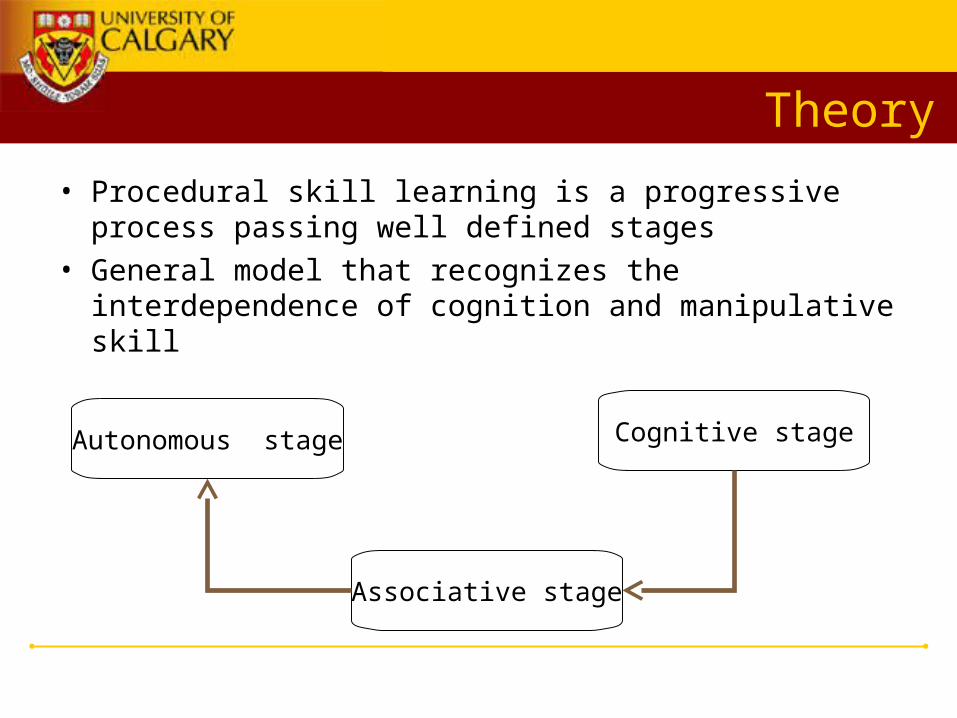
• Procedural skill learning is a progressive process passing well defined stages
• General model that recognizes the interdependence of cognition and manipulative skill
Cognitive stageAutonomous stage
Associative stage

Theory
• Lev Vygotsky 1896-1934– Russian psychologist– Most of his work with children and adolescent– Has some applicability to adult learning– Zone of Proximal Development:
“place where guided learning takes place and where intervention by a teacher will have the greatest
potential”
Theory
• ZPD model would have instruction preceding development
• Would then awaken and rouse set of functions in stage of maturing
• Modern educators use term “scaffolding”– Teacher provides help when needed, but fades into
background when learner becomes independent– Apprenticeship model at heart of medicine
• Legitimate peripheral participation– Newcomers to practice undergo absorption into a
‘community of practice’– Learn from peers as well as tutors
• Royal Naval (Godden & Baddeley) Divers– Divers who learned new material underwater recalled
it better in that context– Reverse true for out of water diver memory– ? Importance of context

• Kneebone argues for breakdown of artificial divide between simulation and patient care
• Envisions distributed learning along clinical workplace• Explicit contextualization of learning
Theory