Simultaneous Expression of Activated Lymphoid CellAssociated and Granulocytic Cell-Associated Antigens onHodgkin's and Reed-Sternberg Cells in Hodgkin's Disease
Masafumi Abe, Eiko Wachi and Haruki WakasaDepartment of Pathology, Fukushima Medical College, Japan
SUMMARY
The surface antigens ofHodgkin cells and Reed-Sternberg cells (H- and R-S cells), including lacunar cells, were analyzed with a large panel ofmonoclonal and polyclonal antibodies by an immunohistochemical method and an immunoelectron microscopic technique.H- and R-S cells in each histologic subtype of nodular sclerosis, mixed cellularity andlymphocyte depletion were stained similarly with anti-Leu-M 1, anti-Leu-11 b, TG 8, antiHLA-DR, anti lL-2 R, RSC-1 (Ki-1) and anti-alpha-l-antitrypsin, but not with otherantibodies examined. These findings suggest the following: (1) H- and R-S cells ofnodularsclerosis, mixed cellularity and lymphocyte depletion are not heterogenous, at least interms ofsurface antigen expression, and (2) H- and R-S cells may be lymphoid cells whichsimultaneously express activated lymphoid cell-associated antigens (e.g., HLA-DR, RSC1 and lL-2 R) and granulocytic cell-associated antigens (e.g., Leu-M 1 and TG 8).
Introduction Material and Methods
With regard to the origin and nature of Hodgkin cells(H cells) and Reed-Sternberg cells (R-S cells) in Hodgkin'sdisease, many studies have su~gested a T-Iymphocyte origin,13 B-Ijm8hocyte origin,3, , 33 monocyte-macrophageorigin,9, 1, ,27 activated lymphoid cell origin30 and aninterdigitating reticulum (ID) cell origin,u In addition,several investigations of immunoglobin and T cell receptorgene analyses of Hodgkin's disease have provided a lead toa possible T 6 or B cell origin2, 34 of H- and R-S cells.However, considerable controversy still remains.
In an attempt to further clarify the origin and nature ofH- and R-S cells, we analyzed twenty-five cases of Hodgkin's disease of several histologic subtypes with a largepanel of monoclonal and polyclonal antibodies by usingan immunoeleetron microscopic technique as well as animmunohistochemical method. In addition, phenotypicdifferences between H- and R-S cells and interdigitatingreticulum cells (ID cells) were also studied.
; 12 cases of Hodgkin's disease were used forimmunohistochemical and immunoelectron microscopic studies.The histologic subtypes were nodular sclerosis (4 cases), mixedcellularity (7 cases) and lymphocyte depletion (1 case). Parallelfrozen sections were stained with hematoxylin and eosin for theidentification of Hodgkin and Reed-Sternberg cells (H- and R-Scells) and other non-neoplastic cells. In addition, 3 cases of dermatopathic lymphadenitis were used for studying of the reactivityof ID cells.
(b) Paraffin blocks of formalin-fixed tissues: 25 cases of Hodgkin's disease and 2 cases of dermatophatic lymphadenitis wereused in the immunohistochemical study. The cases of Hodgkin'sdisease included the following types: lymphocyte predominance(1 case), nodular sclerosis (6 cases), mixed cellularity (14 cases)and lymphocyte depletion (4 cases).
2) Reagents: The monoclonal and polyclonal antibodies usedin this study are listed in Table 1. Normal swine serum, swineanti-rabbit immunoglobulin and peroxidase-antiperoxidase complex (PAP) were purchased from DAKOPATTS (Denmark). Rab-
bit anti-mouse IgG and rabbit anti-mouse IgM were obtainedfrom Cappel Laboratories Inc. (Cochranville, PA, USA). Avidinbiotin-peroxidase complex (ABC kit) was purchased from VectorLaboratories Inc. (Burlingame, CA, USA). 3) Staining procedures: Immunohistochemical staining was performed by the PAPmethod of Sternberger et apt with some modifications, or by theABC method as described by Hsu et al. tO Immunoelectron microscopy was carried out according to the pre-embeddingmethod, with some modifications. Briefly, PLP-fixed frozen sections were stained by an indirect immunostaining procedure. Thesections were then fixed with 2.5% glutaraldehyde and incubatedin 3, 3'-diamino-benzidine-tetrahydrochloride (DAB) substratesolution with 0.01% hydrogen peroxidase. Sections were postfixed with 1% osmium tetroxide, dehydrated, embedded andthen obsereved electron microscopically without counterstaining.
Controls to specify the method were performed by omitting theprimary antibody or by replacing the primary antibody withBALB/C mouse serum.
4) Semi-quantitative evaluation of immunostaining: The percentage of H- and R-S cells in each case showing positivity foreach monoclonal antibody was determined using the followingformula:
the number of positive H- and R-S cells-,-----:---:-::-:--"---::-::--:----:-:-....,-:::-;--,....--,,- x 100 (%)the number of H- and R-S cells (fifty in total)
The grading system was as follows: -: no positive cells; +/-:up to 9%; +: up to 49%; ++: up to 79%; and +++: up to100%.
Table 1. Monoclonal and Polyclonal Antibodies Used
Immunohistochemical Study of Hodgkin'S Disease' 419
Results
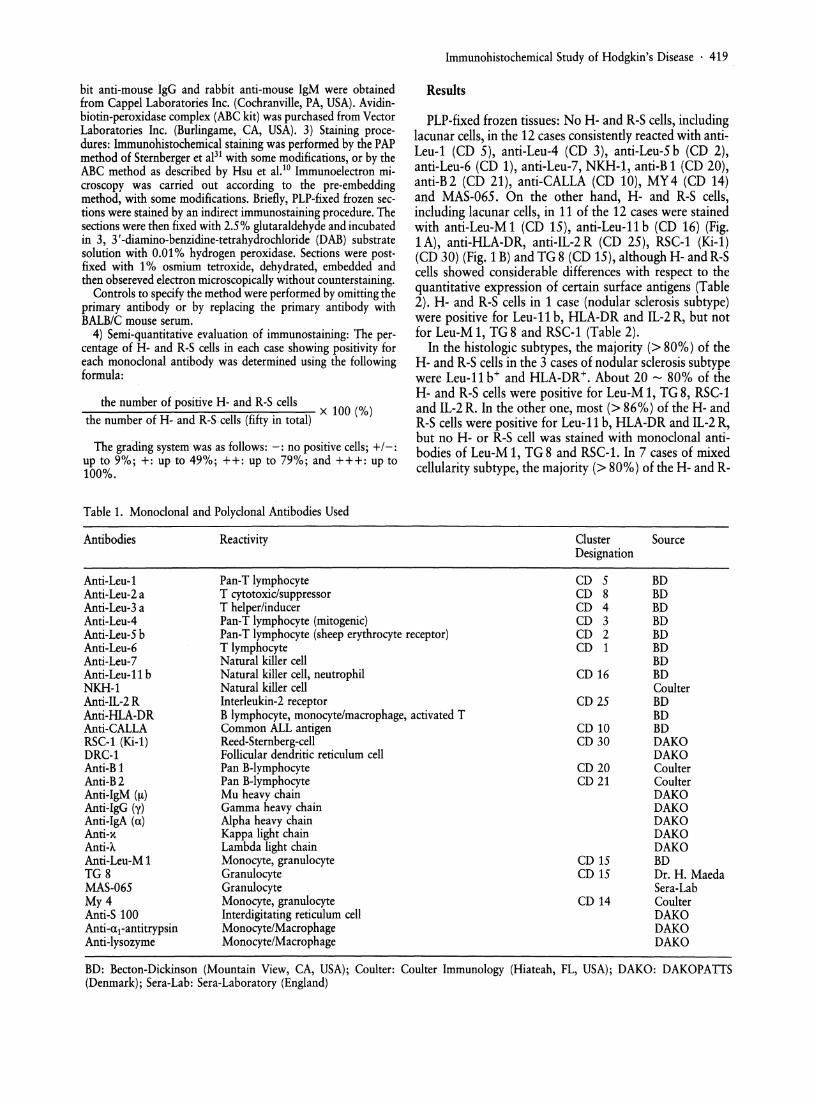
PLP-fixed frozen tissues: No H- and R-S cells, includinglacunar cells, in the 12 cases consistently reacted with antiLeu-l (CD 5), anti-Leu-4 (CD 3), anti-Leu-5 b (CD 2),anti-Leu-6 (CD 1), anti-Leu-7, NKH-l, anti-B 1 (CD 20),anti-B2 (CD 21), anti-CALLA (CD 10), MY 4 (CD 14)and MAS-065. On the other hand, H- and R-S cells,including lacunar cells, in 11 of the 12 cases were stainedwith anti-Leu-M 1 (CD 15), anti-Leu-ll b (CD 16) (Fig.1A), anti-HLA-DR, anti-IL-2 R (CD 25), RSC-l (Ki-l)(CD 30) (Fig. 1B) and TG 8 (CD 15), although H- and R-Scells showed considerable differences with respect to thequantitative expression of certain surface antigens (Table2). H- and R-S cells in 1 case (nodular sclerosis subtype)were positive for Leu-ll b, HLA-DR and IL-2 R, but notfor Leu-M 1, TG8 and RSC-l (Table 2).
In the histologic subtypes, the majority (> 80%) of theH- and R-S cells in the 3 cases of nodular sclerosis subtypewere Leu-ll b+ and HLA-DR+. About 20 - 80% of theH- and R-S cells were positive for Leu-M 1, TG 8, RSC-land IL-2 R. In the other one, most (> 86%) of the H- andR-S cells were positive for Leu-ll b, HLA-DR and IL-2R,but no H- or R-S cell was stained with monoclonal antibodies of Leu-M 1, TG 8 and RSC-l. In 7 cases of mixedcellularity subtype, the majority (> 80%) of the H- and R-
"NS, Nodular sclerosis; MC, Mixed cellularity; LD, Lymphocyte depletion; -: no positive cells, +/-: up to 9% positive cells, +: up to49% positive cells, ++: up to 79% positive cells, +++: up to 100% cells
Supported by Grant No. 61010101 from the Ministry of Education, Science and Culture of Japan.
Table 3. Comparison between the Reactivities of Anti-Leu-M 1,-Leu-11 b, -HLA-DR, -IL-2 R, -lysozyme, -S-100, TG8 and RSC1 with H- and R-S Cells and ID Cells
S cells were Leu-M 1+, Leu-ll b+ and TG8+. About 30100% of the H- and R-S cells showed a positive reactionwith anti-IL-2 R, anti-HLA-DR and RSC-1. In one lymphocyte depletion subtype case, the majority (> 96%) ofthe H- and R-S cells were Leu-M1\ Leu-llb+, TG8+and HLA-DR+, and a large minority (>30%) of the Hand R-S cells were RSC-1 + and IL-2 R+.
ID cells associated with dermatopathic lymphadenitiswere Leu-r, Leu-2a- (CD 8), Leu-3a- (CD 4), Leu-4-,Leu-S b-, Leu-6-, Leu-T, MAS-06S-, Br, B2- andDRC-r. In addition, ID cells were not stained with antiLeu-M 1, anti-Leu-11 b, anti-HLA-DR, anti-IL-2 R, RSC1 and TG 8 all of which were positive for H- and R-S cells(Table 3).
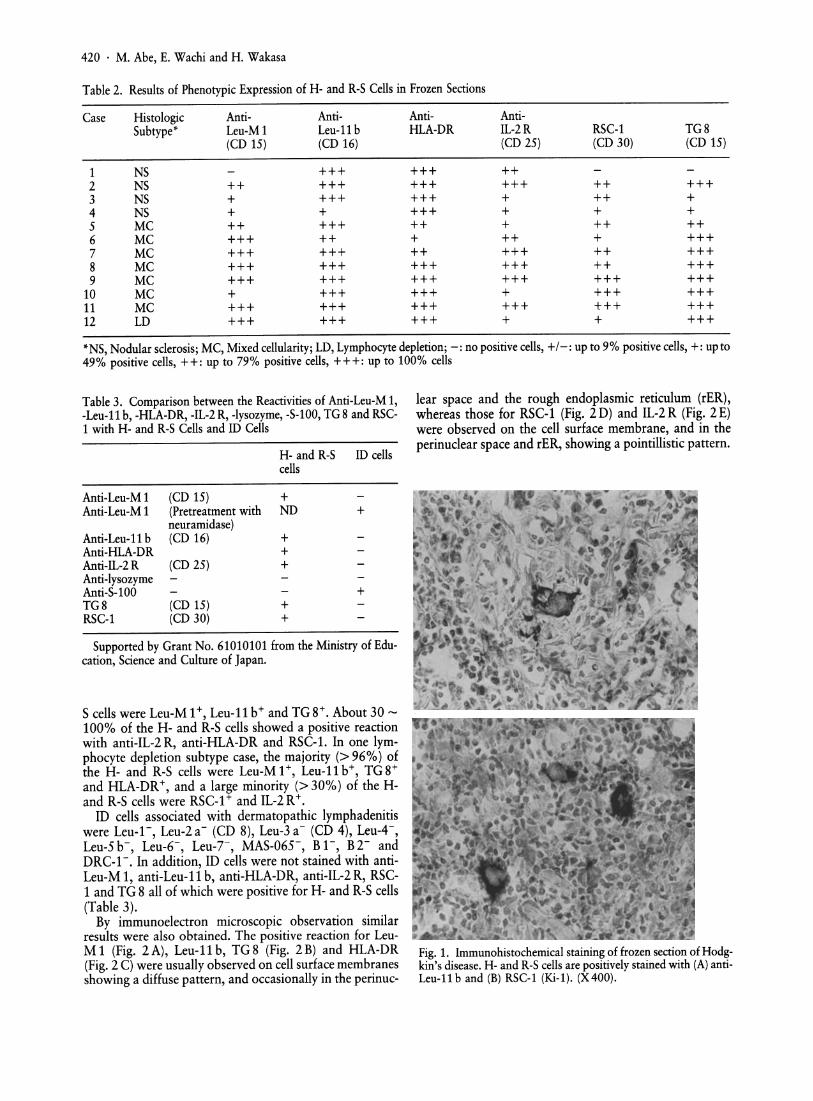
By immunoelectron microscopic observation similarresults were also obtained. The positive reaction for LeuM1 (Fig. 2A), Leu-llb, TG8 (Fig. 2B) and HLA-DR(Fig. 2 C) were usually observed on cell surface membranesshowing a diffuse pattern, and occasionally in the perinuc-
Fig. 1. Immunohistochemical staining of frozen section of Hodgkin's disease. H- and R-S cells are positively stained with (A) antiLeu-11 b and (B) RSC-l (Ki-l). (X400).
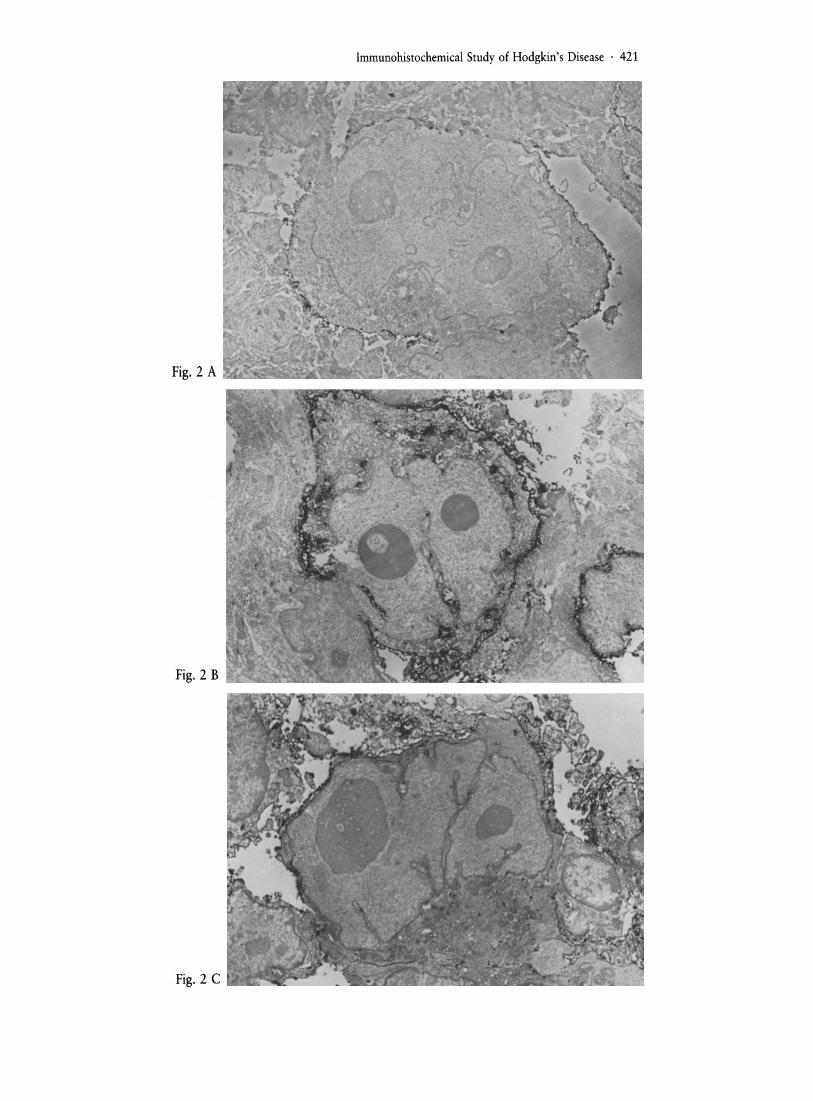
lear space and the rough endoplasmic reticulum (rER),whereas those for RSC-1 (Fig. 2D) and IL-2R (Fig. 2E)were observed on the cell surface membrane, and in theperinuclear space and rER, showing a pointillistic pattern.
+
+
ID cellsH- and R-Scells
Anti-Leu-M 1 (CD 15) +Anti-Leu-M 1 (Pretreatment with NO
Immunohistochemical Study of Hodgkin's Disease . 421
422 . M. Abe, E. Wachi and H. Wakasa
Fig. 2 D
Fig. 2 E
Fig. 2. Immunoelectron microscopic staining of Hodgkin's disease. Hand R-S cellsstained with (A) anti-Leu-M 1, (B) TG 8, (C)anti-HLA-DR, (D) RSC-1 (Ki-1) and (E) anti-IL-2 R show positive reactions in the surface membrane, perinuclear space and rERwith a diffuse or dotted pattern. Anti-HLADR and anti-Leu-ll b show staining patterns similar to that of anti-Leu-M 1.(A) anti-Leu-M 1 (X 7,200)(B) TG 8 (X 7,200)(C) anti-HLA-DR (X 5,200)(D) RSC-1 (X 5,000)(E) anti-IL-2R (X6,100)
Paraffin blocks of formalin-fixed tissues: In 7 of 25cases of Hodgkin's disease, H- and R-S cells were stainedwith anti-immunoglobulin antibodies (anti-IgG, anti-xand anti-A), but this staining was interpreted as nonspecificuptake because of the polyclonal nature of the intracytoplasmic immunoglobulins. No H- or R-S cells in any ofthecases reacted with anti-lysozyme or anti-S-l00 antibodies.About 18 - 76% of the H- and R-S cells in 6 cases, (1 caseof nodular sclerosis, 2 of mixed cellularity and 3 of lymphocyte depletion) showed positive reactions with antialpha-I-antitrypsin. Out of 22 cases, in all but 3 cases, themajority of H- and R-S cells (>50%) were strongly positive for Leu-M 1. However, the number of positive H- andR-S cells varied from case to case.
ID cells in 2 cases with dermatophatic lymphadenitisreacted weakly with anti-S 100 antibody. No ID cells werepositive for Leu-M 1 in these cases, however, ID cells in 2cases were positive for Leu-M 1 with neuramidase pretreatment.
Discussion
It has long been doubted whether Hodgkin's diseasecomprising 4 histologic subtypes is a homogeneous entity,since clinical, epidemiologic and immunohistochemicaldifferences between nodular sclerosis and other histologicsubtypes or between nodular lymphocyte predominanceand other histologic subtypes suggest that these may bedifferent diseases.n, 25, 26, 1.7, 32 Hsu et alY reported thatHodgkin's disease was a homogeneous entity and that Hand R-S cells originated from ID cells since a great majority of the H- and R-S cells reacted with T 200, anti-HLADR, anti-Leu-l0, AIG3, anti-Tac, OKT 9 and anti-LeuM 1 in a similar or identical manner in each histologicsubtype of Hodgkin's disease. On the other hand, Stein etal.30 proposed that Hodgkin's disease was a heterogeneousentity since the possibility that the H- and R-S cells werederived from activated T cell or activated B cells wasevaluated. In addition, Pinkus et aI,23 and Timens et al.35
recently reported that the nodular lymphocyte predominance subtype of Hodgkin's disease could be distinguishedfrom other subtypes.
In the present study, H- and R-S cells (including lacunarcells) in each histologic subtype of Hodgkin's disease,except for lymphocyte predominance, reacted in a similarmanner with anti-Leu-M 1, anti-Leu-ll b, TG 8, antiHLA-DR, anti-IL-2 Rand RSC-1, and showed an identicalphenotype. Immunoelectron microscopy confirmed thatthe H- and R-S cells were reactive with these monoclonalantibodies. These findings seem to suggest that H- and R-Scells in Hodgkin's disease comprising nodular sclerosis,mixed cellularity and lymphocyte depletion arehomogeneous, at least in terms of surface antigen expression. It is necessary to determine more accurately whetherthis is also true in PLP-fixed frozen tissues from lymphocyte predominance cases.
The expression of HLA-DR, RSC-1 and IL-2R on theH- and R-S cells seems to imply that H- and R-S cellsundergo activation since these antigens, especially the latter two, are considered to be activation-associated markersbecause: (1) the RSC-1 antigen is expressed on activated Tcells and B cells, especially on activated large lymphoidcells.30 (2) the IL-2 R antigen is also expressed on activatedBcells,19 as well as activated T cells.36 (3) HLA-DR can bedetected on the surface of activated T cells.4 In addition,the IL-2 Rand RSC-1 antigens is not usually detected ongranulocytes or monocytes/macrophages. This, therefore,suggests that H- and R-S cells have some properties ofactivated lymphoid cells, as already noted by Stein et a1.30
The reactivity of H- and R-S cells with monoclonal antibodies Leu-M 1 and TG 8 has raised the problem thatthese cells may possess granulocytic cell-associated antigens as already reported by several investigators2o, 24, 28, 29who found the presence of the granulocytic cell-associatedantigen (CD 15) in H- and R-S cells, since (1) anti-Leu-M 1reacts with granulocytes and monocytes,6 and (2) TG 8 is amonoclonal antibody recognizing a differentiation antigenwhich appears between the myeloblast and myelocytestages.21 However, monoclonal antibody Leu-M 1 is alsocapable of reacting with mitogen-activated T-cells (helper/inducer T cells),8 some T-celllines8and occasionally withT-cell neoplasms.37 In addition, the presence of CD 15 ontumor cells where sialylation may be abnormal may beunreliable to a guide to the tumor cell lineage12
• Thesereagents, therefore, do not specially define a granulocyticlineage for H- and R-S cells.
With regard to the origin of H- and R-S cells, Hsu etal. ll recently proposed that H- and R-S cells in Hodgkin'sdisease might originate from ID cells. However, we couldnot find any evidence that H- and R-S cells came from IDcells because Leu-M 1, Leu-11 b, TG 8, HLA-DR, RSC-1and IL-2 R antigens, which were expressed on the H- andR-S cells, were not detected on the ID cells, whereas S-100protein antigens on the ID cells were not expressed on theH- and R-S cells. In addition, it is unseemingly consideredthat the origin of H- and R-S cells is monocytes/macrophages based on the following reasons: (1) TG 8, RSC-1and IL-2 R antigens are not detected on the surface ofmonocytes or macrophages, (2) anti-lysozyme and MY 47
Immunohistochemical Study of Hodgkin's Disease· 423
do not react with H- and R-S cells, and (3) the expressionof alpha-1-antitrypsin antigen is not restricted to monocytes and macro~hages, and is also recognized on certainlymphoid cells. °
H- and R-S cells reacted with monoclonal antibody Leu11 b recognizing Fe receptor on neutrophils as well asnatural killer (NK) cells, however, this positive reactioncould not be well evaluated.
Finally, in the present study we found that H- and R-Scells had coexpression of activated lymphoid cell-associated markers (e.g. HLA-DR, RSC-1 and IL-2R) andgranulocytic cell-associated markers (e. g. Leu-M 1 andTG 8). This finding raises the possibility that the origin ofH- and R-S cells is a lymphoid cell showing properties ofactivated lymphoid cells and granulocytic cells in terms ofmarker expression. It is not unusual in acute leukemiasthat individual leukemic cells simultaneously express lymphoid and myeloid features. I, 16 Such acute leukemias aretermed acute mixed lineage leukemia, biphenotypicleukemia or hybrid acute leukemia. The generation isexplained on the basis of (a) malignant transformation ofa progenitor cell capable of development along eithermyeloid or lymphoid lineages, or (b) aberrant gene expression resulting from the leukemogenic event. H- and R-Scells (including lacunar cells) in Hodgkin's disease appearto be biphenotypic cells which simultaneously expressactivated lymphoid- and granulocytic cell-associated antigens. The reason may be attributed to aberrant geneexpression resulting in the addition of granulocytic cellassociated antigens to activated lymphoid cells since nopluripotent stem cell exists in the peripheral lymphoid tissue and no normal counterpart of H- and R-S cells expressing biphenotypes has been found. In addition, this aberrant gene expression might cause the lack of T or B celldifferentiation antigens on H- and R-S cells.
References
1 Ben-Basst I, Gale RP (1984) Hybrid acute leukemia.Leukemia Research 8: 929-936
3 Dorreen MS, Habeshaw JAL, Stansfeld AG, Wrigley PFM,Lister TA (1984) Characteristics of Sternberg-Reed and relatedcells in Hodgkin's disease: An immunohistological study. Br JCancer 49: 465-476
4 Engleman EG, Warnke R, Fox RI, Levy R (1981) Studies of ahuman T lymphocyte antigen recognized by a monoclonal antibody. Proc Nat! Acad Sci USA 78: 1971-1975
5 Gladkowska-Dura MJ, Bura WI, Johnson WW (1981) Lightand immunoelectron-microscopic study of Hodgkin's disease:Evidence of immunoglobulin synthesis by tumor cells. VirchowArch (Cell Pathol) 37: 109-124
6 Griesser H, Feller A, Lennert K, Minden M, Mak TW (1986)Rearrangement of the ~ chain of the T cell antigen receptor andimmunoglobulin genes in lymphoproliferative disease. J. ClinInvest 78: 1179-1184
7 Griffin JD, Mayer RJ, Weinstein HJ, Rosenthal DS, CoralFS, Beveridge RP (1983) Surface marker analysis of acutemyeloblastic leukemia: Identification of differentiation - associated phenotypes. Blood 62: 557-563
424 . M. Abe, E. Wachi and H. Wakasa
8 Hanjan SNS, Kearney JK, Cooper MD (1982) A monoclonalantibody (MMA) that identifies a differentiation antigen onhuman myelomonocytic cells. Clin Immunol Immunopathol 23:172-188
9 Hansen NE, Clausen PP, Karie H, Christoffersen P (1981)Tissue and plasma lysozyme in Hodgkin's disease. Scand JHaematol; 27: 186-192
10 Hsu SM, Raine L, Franger H (1981) The use of avidinbiotin-peroxidase complex (ABC) in immunoperoxidase techniques: A comparison between ABC and unlabeled antibody(PAP) procedures. J Histochem Cytochem 29: 577-580
11 Hsu SM, Yang K, Jaffe ES (1985) Pheotypic expression ofHodgkin's and Reed-Sternberg cells in Hodgkin's disease. Am JPatho1209-217
12 Jones DB (1987) The histogenesis of the Reed-Sternberg celland its mononuclear counterparts. J Pathol151: 191-195
14 Lukes RJ, Butler 11, Hicks EB (1966) Natural history ofHodgkin's disease as related to its pathologic picture. Cancer 19:317-344
15 McLean IW, Nakane PK (1974) Periodate-Iysine-paraformaldehyde fixative: a new fixative for immunoelectron microsCOpt J Histochem Cytochem 22: 1077-1083
Mirro J, Zipf TF, Pui C-H, Kitchingman G, Williams D,Melnin S, Murphy SB, Staso S (1985) Acute mixed lineageleukemia: c1inico-pathologic correlations and prognostic significance. Blood 66: 1115-1123
17 Mir R, Kah LB (1983) Immunohistochemistry of Hodgkin'sdisease. A study of 20 cases. Cancer 6: 515~523
18 Mori N, Oka K, Sakuma H, Tsunoda R, Kojima M (1985)Immunoeleetron microscopic study of Hodgkin's disease. Cancer56: 2605-2611
19 Muraguchi A, Kehrl JH, Longo DL, Volkman DJ, Smith Ka,Fauci AS (1985) Interleukin 2 in human B cell function. J Exp.Med 161: 181-197
20 Norton AJ, Isaacson PG (1985) Granulocyte and HLA-DRregion specific monoclonal antibodies in the diagnosis of Hodgkin's disease. J Clin Pathol38: 1241-1246
21 Ozaki Y, Ohashi T, Ohto H, Maeda H (1985) A monoclonal antibody against human neutrophil: Evaluation of itseffects on neutrophil function and partial characterization of theantigen. Acta Haematol Jpn 48: 980-991
22 Perussia B, Triuchieri G, Jackson A, Warner NL, Faust ],Rumpold H, Kraft D, Lanier L (1984) The Fe receptor for IgG onhuman natural killer cells: Phenotypic, functional, and comparative studies using monoclonal antibodies. J Immunol 133:180-189
23 Pinkus GS, Said JW (1985) Hodgkin's disease, lymphocytepredominance type nodular - A distinct entity? Am J Pathol118:1-6
24 Pinkus GS, Thomas P, Said JW (1985) Leu-M 1 - a markerfor Reed-Sternberg cells in Hodgkin's Disease. An immunoperox-
idase study of paraffin-embedded tissue. Am J Pathol 119:244-252
25 Poppema S (1980) The diversity of the immunohistologicalstaining pattern of Sternberg-Reed cells. J Histochem Cytochem'28: 788-791
26 Poppema S, Kaiserling E, Lennert K (1979) Hodgkin's disease with lymphocyte predominance, nodular type (nodular paragranuloma) and progressively transformed germinal centers - acytohistological study. Histopathology 3: 295-308
28 Stein H, Vchanska-Ziegler B, Gerdes J, Ziegler A, Wernet P(1982) Hodgkin and Sternberg-Reed cells contain antigensspecific to the cells of granulopoiesis. Int J Cancer 29: 283-290
29 Stein H, Gerdes J, Schwab U, Leinke H, Diehl V, Mason Y,Bartels H, Ziegler A (1983) Evidence for the detection of thenormal counterpart of Hodgkin and Sternberg-Reed cells.Hematol Oncol1: 21-29
30 Stein H, Mason DY, Gerdes J, O'Connor W, Wainscoat J,Pallesen G, Gatter K, Falini B, Delsol G, Lemke H, Schwarting R,Lennert K (1985) The expression of the Hodgkin's disease associated antigen Ki-1 in reactive and neoplastic lymphoid tissue: Evidence that Reed-Sternberg cells and histiocytic malignancies arederived from activated lymphoid cells. Blood 66: 848-858
31 Sterberger LA, Hardy PH Jr, Cuculis 11, Meyer HG (1970)The unlabeled antibody-enzyme method of immunohistochemistry. Preparation and properties of soluble antigen-antibody complex (horseraddish peroxidase-antihorseraddish peroxidase) andits use in identification of spirochetes. J Histochem Cytochem 18:315-333
32 Strum SB, Rappaport H (1971) Interrelation of the histologic types of Hodgkin's disease. Arch Pathol 91: 127-134
33 Stuart AE, Volsen SG, Zola H (1983) The reactivity ofReed-Sternberg cells with monoclonal antisera at thin section andultrastruetuallevels. J Pathol 141: 71-82
34 Sundeen J, Lipford E, Uppenhamp M, Sussman E, Wahl L,Raffeld M, Cossman J (1987) Rearranged antigen receptor genesin Hodgkin's disease 70: 186-191
35 Timens W, Visser L, Poppema S (1986) Nodular lymphocyte predominance type of Hodgkin's disease is a germinal centerIymfhoma. Lab Invest 54: 457-461
3 Uchiyama T, Broder S, Waldman TA (1981) A monoclonalantibody (anti-Tac) reactive with activated and functionallymature T-cells: I. Production of anti-Tac monoclonal antibodyand distribution of Tac+ cells. J Immunol126: 1393-1397
37 Wieczorek R, Burke JS, Knowles DM 2d (1985) Leu-M 1antigen expression in T-cell neoplasia. Am J Pathol 121:374-380
38 Zola H, Mcmanara P, Thomas M, Smart 1], Brdely J (1981)The preparation and properties of monoclonal antibodies againsthuman granulocyte membrane antigens. Br J Haematol 48:481-490.
Received August 21, 1987 . Accepted in revised form January 26, 1988