Sinus valsalva aneurysm on cardiac CT angiography:Assessment and detectionJohn M Troupis,1 Arthur Nasis,2 Sundeep Pasricha,1 Mihir Patel,1 Andris Harald Ellims4 andSujith Seneviratne3
1Diagnostic Imaging, Monash Medical Centre, Southern Health, 2Monash Cardiovascular Research Centre, Monash Heart, Southern Health, 3Monash
Heart, Southern Health, Melbourne, and 4Department of Cardiovascular Medicine, Alfred Hospital, Prahran, Victoria, Australia
After the advent of ECG gated cardiac CT angiography (CCTA) there has beensignificant improvement in image quality of the ascending aorta. As a resultthe sinuses of valsalva are readily assessable. Sinuses of valsalva aneurysmcan cause significant dysfunction of the aortic root and annulus and can becongenital or acquired. The aneurysm most commonly originates from theright coronary sinus. Complications related to sinuses of valsalva aneurysmcan cause chest pain and can be life threatening. The cardiac imager shouldactively assess the sinuses of valsalva in every CCTA study.
Key words: aortic root; cardiac CT angiography; sinuses of valsalva aneurysm;sinuses of valsalva.
As cardiac CT angiography (CCTA) has developed intoa readily accessible and useful tool for the exclusionof obstructive coronary artery disease in the acutelyunwell patient with chest pain,1 cardiac imagers arebeing exposed to images with significant improvementin visibility of the ascending aorta.2
The aortic root, which is seen on CCTA, includesthe aortic annulus, sinus of valsalva and the sinotu-bular junction. Sinuses of valsalva aneurysm (SVA) canlead to significant dysfunction of the aortic root andannulus and may be life threatening.3 As such, theyshould be carefully assessed in anyone with eitherischaemic-type chest pain, or alternatively, dissection-type symptoms.
Definition
The sinuses of valsalva are three focal expansions thatform the walls of the aortic root. The right coronaryartery arises from the right sinus and the left coronaryartery arises from the left sinus, with the left sinus lyingslightly more superiorly than the right sinus4
SVA is defined as dilatation or enlargement of one ormore of the aortic sinuses between the aortic valveannulus and the sinotubular junction4
Prevalence
The incidence ranges from 0.1 to 3.5% of all congenitalheart defects5 with proposed prevalence of 0.09% in thegeneral population.6
Causes
The acquired SVA is more common than the congenitaland most often is caused by weakness at the junction ofthe aortic media and the annulus fibrosis, due to con-genital deficiency of elastic lamellae with separation ofthe media in the sinus from the media adjacent to theaortic valve annulus.
Acquired SVA are associated with infections(syphilis, TB), atherosclerosis, connective tissue disor-ders or trauma.7–9 There is usually elastic connectivetissue degeneration as the associated underlying weak-ness of the wall of the sinus.
bs_bs_banner
Journal of Medical Imaging and Radiation Oncology 57 (2013) 444–447
Aortic root dissection can be differentiated due to thepresence of a dissection flap, which may be in closeapposition to the sinus and in particular at the sinotu-bular junction.
Measurement
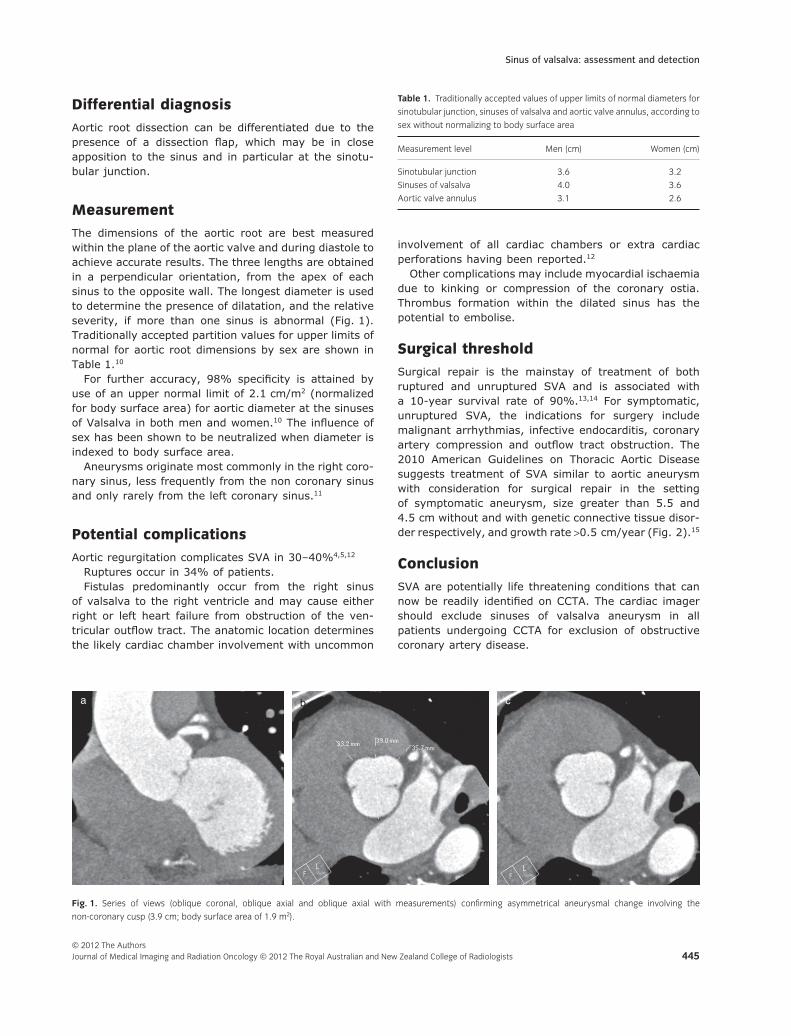
The dimensions of the aortic root are best measuredwithin the plane of the aortic valve and during diastole toachieve accurate results. The three lengths are obtainedin a perpendicular orientation, from the apex of eachsinus to the opposite wall. The longest diameter is usedto determine the presence of dilatation, and the relativeseverity, if more than one sinus is abnormal (Fig. 1).Traditionally accepted partition values for upper limits ofnormal for aortic root dimensions by sex are shown inTable 1.10
For further accuracy, 98% specificity is attained byuse of an upper normal limit of 2.1 cm/m2 (normalizedfor body surface area) for aortic diameter at the sinusesof Valsalva in both men and women.10 The influence ofsex has been shown to be neutralized when diameter isindexed to body surface area.
Aneurysms originate most commonly in the right coro-nary sinus, less frequently from the non coronary sinusand only rarely from the left coronary sinus.11
Potential complications
Aortic regurgitation complicates SVA in 30–40%4,5,12
Ruptures occur in 34% of patients.Fistulas predominantly occur from the right sinus
of valsalva to the right ventricle and may cause eitherright or left heart failure from obstruction of the ven-tricular outflow tract. The anatomic location determinesthe likely cardiac chamber involvement with uncommon
involvement of all cardiac chambers or extra cardiacperforations having been reported.12
Other complications may include myocardial ischaemiadue to kinking or compression of the coronary ostia.Thrombus formation within the dilated sinus has thepotential to embolise.
Surgical threshold
Surgical repair is the mainstay of treatment of bothruptured and unruptured SVA and is associated witha 10-year survival rate of 90%.13,14 For symptomatic,unruptured SVA, the indications for surgery includemalignant arrhythmias, infective endocarditis, coronaryartery compression and outflow tract obstruction. The2010 American Guidelines on Thoracic Aortic Diseasesuggests treatment of SVA similar to aortic aneurysmwith consideration for surgical repair in the settingof symptomatic aneurysm, size greater than 5.5 and4.5 cm without and with genetic connective tissue disor-der respectively, and growth rate >0.5 cm/year (Fig. 2).15
Conclusion
SVA are potentially life threatening conditions that cannow be readily identified on CCTA. The cardiac imagershould exclude sinuses of valsalva aneurysm in allpatients undergoing CCTA for exclusion of obstructivecoronary artery disease.
a cb
Fig. 1. Series of views (oblique coronal, oblique axial and oblique axial with measurements) confirming asymmetrical aneurysmal change involving the
non-coronary cusp (3.9 cm; body surface area of 1.9 m2).
Table 1. Traditionally accepted values of upper limits of normal diameters for
sinotubular junction, sinuses of valsalva and aortic valve annulus, according to
1. Becker HC, Johnson T. Cardiac CT for the assessmentof chest pain: imaging techniques and clinicalresults. Eur J Radiol 2011; (Epub ahead of print)doi: 10.1016/j.ejrad.2011.05.038.
2. Roos JE, Willman JK, Weishaupt D et al. Thoracicaorta: motion artifact reduction with retrospectiveand prospective electrocardiography-assistedmulti-detector row CT. Radiology 2002; 222: 271–7.
3. Schullerer D, Emmert MY, Jacobs S et al. Aneurysmof coronary sinus of valsalva can rupture anytime!Heart Surg Forum 2011; 14: E210–1.
4. Ring WS. Congenital heart surgery nomenclature anddatabase project: aortic aneurysm, sinus of valsalvaaneurysm, and aortic dissection. Ann Thorac Surg2000; 69 (Suppl 4): S147–63.
5. Takach TJ, Reul GJ, Duncan JM et al. Sinus ofValsalva aneurysm or fistula: management andoutcome. Ann Thorac Surg 1999; 68: 1573–7.
6. Smith WA. Aneurysm of the sinus of Valsalva, withreport of 2 cases. JAMA 1914; 62: 1878–80.
7. Batiste C, Bansal RC, Razzouk AJ. Echocardiographicfeatures of an unruptured mycotic aneurysm of the
right aortic sinus of Valsalva. J Am Soc Echocardiogr2004; 17: 474–7.
8. Medeiros Sobrinho JH, Silva MA, Fontes WF et al.Syphilitic aneurysm communicating with an aorticsinus of Valsalva. A case report. Arq Bras Cardiol1989; 52: 341–4.
9. Greiss I, Ugolini P, Joyal M, Bouchard D, Mercier LA.Ruptured aneurysm of the left sinus of Valsalvadiscovered 41 years after a decelerational injury.J Am Soc Echocardiogr 2004; 17: 906–9.
10. Roman MJ, Devereux RB, Kramer-Fox R, O’LoughlinJ. Two-dimensional echocardiographic aortic rootdimensions in normal children and adults. Am JCardiol 1989; 64: 507–12.
11. Fishbein MC, Obma R, Roberts WC. Unruptured sinusof Valsalva aneurysm. Am J Cardiol 1975; 35:918–22.
12. Moustafa S, Mookadam F, Cooper L et al. Sinusof valsalva aneurysms – 47 years of a single centreexperience and systemic overview of publishedreports. Am J Cardiol 2007; 99: 1159–64.
13. Taguchi K, Sasaki N, Matsuura Y, Uemura R. Surgicalcorrection of aneurysm of the sinus of Valsalva. Areport of forty-five consecutive patients including
a b
c
d
e
Fig. 2. A 44-year-old man requiring a CCTA
for the exclusion of obstructive coronary artery
disease, prior to surgery for a dilated aortic root.
eight with total replacement of the aortic valve.Am J Cardiol 1969; 23: 180–91.
14. Wang ZJ, Zou CW, Li DC et al. Surgical repair ofsinus of valsalva aneurysm in Asian patients. AnnThorac Surg 2007; 83: 2066–72.
15. Hiratzka LF, Bakris GL, Beckman JA et al. 2010ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVMGuidelines for the diagnosis and management ofpatients with thoracic aortic disease. A Report of the
American College of Cardiology Foundation/AmericanHeart Association Task Force on Practice Guidelines,American Association for Thoracic Surgery, AmericanCollege of Radiology, American Stroke Association,Society of Cardiovascular Anesthesiologists, Societyfor Cardiovascular Angiography and Interventions,Society of Interventional Radiology, Society ofThoracic Surgeons, and Society for VascularMedicine. J Am Coll Cardiol 2010; 55: e27–e129.