16
A COMPLEX ENDOLEAK REPAIR Resident(s): Ihab Akladious, MD Attending(s): Raj Pyne, MD Program/Dept(s): Rochester General Hospital, Rochester , NY Originally Posted: December 01, 2014

8/11/2019 SIR RFS Case Series: A Complex Endoleak Repair
http://slidepdf.com/reader/full/sir-rfs-case-series-a-complex-endoleak-repair 1/17
A COMPLEX ENDOLEAK RE
Resident(s): Ihab Akladious, MDAttending(s): Raj Pyne, MD
Program/Dept(s): Rochester General Hospital, Rochester, NY
Originally Posted:
8/11/2019 SIR RFS Case Series: A Complex Endoleak Repair
http://slidepdf.com/reader/full/sir-rfs-case-series-a-complex-endoleak-repair 2/17
CHIEF COMPLAINT & HPI
History of Present Illness
71 y/o female with history of thoracic and abdominal aortic aneurysms s/p combinedand EVAR with debranching procedure to reconstitute flow to the mesenteric arterikidneys (common graft from aortic bifurcation to right renal artery, proper hepatic aSMA, and second graft from right common iliac artery to left renal artery), presentspost-operatively for surveillance CT examination

8/11/2019 SIR RFS Case Series: A Complex Endoleak Repair
http://slidepdf.com/reader/full/sir-rfs-case-series-a-complex-endoleak-repair 3/17
RELEVANT HISTORY
Past Medical History Hypertension
Aortic valve stenosis
Thoracic aortic aneurysm
Abdominal aortic aneurysm
Past Surgical History Aortic valve replacement
TEVAR, EVAR and debranching procedure
Medications Aspirin, simvastatin, losartan-HCTZ, ipratropium nasal spray
Allergies NKDA

8/11/2019 SIR RFS Case Series: A Complex Endoleak Repair
http://slidepdf.com/reader/full/sir-rfs-case-series-a-complex-endoleak-repair 4/17
DIAGNOSTIC WORKUP – CTA 5 MONTHS AFTER
A: Coronal image from CT angiogram shows aType II endoleak (arrow) within the nativeaneurysm sac adjacent to both thoracic andabdominal endografts
B and C: Sagittal and axial images from CT angiogram shendoleak with retrograde filling from the celiac trunk (arr
A B
C
8/11/2019 SIR RFS Case Series: A Complex Endoleak Repair
http://slidepdf.com/reader/full/sir-rfs-case-series-a-complex-endoleak-repair 5/17
DIAGNOSTIC WORKUP – CTA 5 MONTHS AFTER
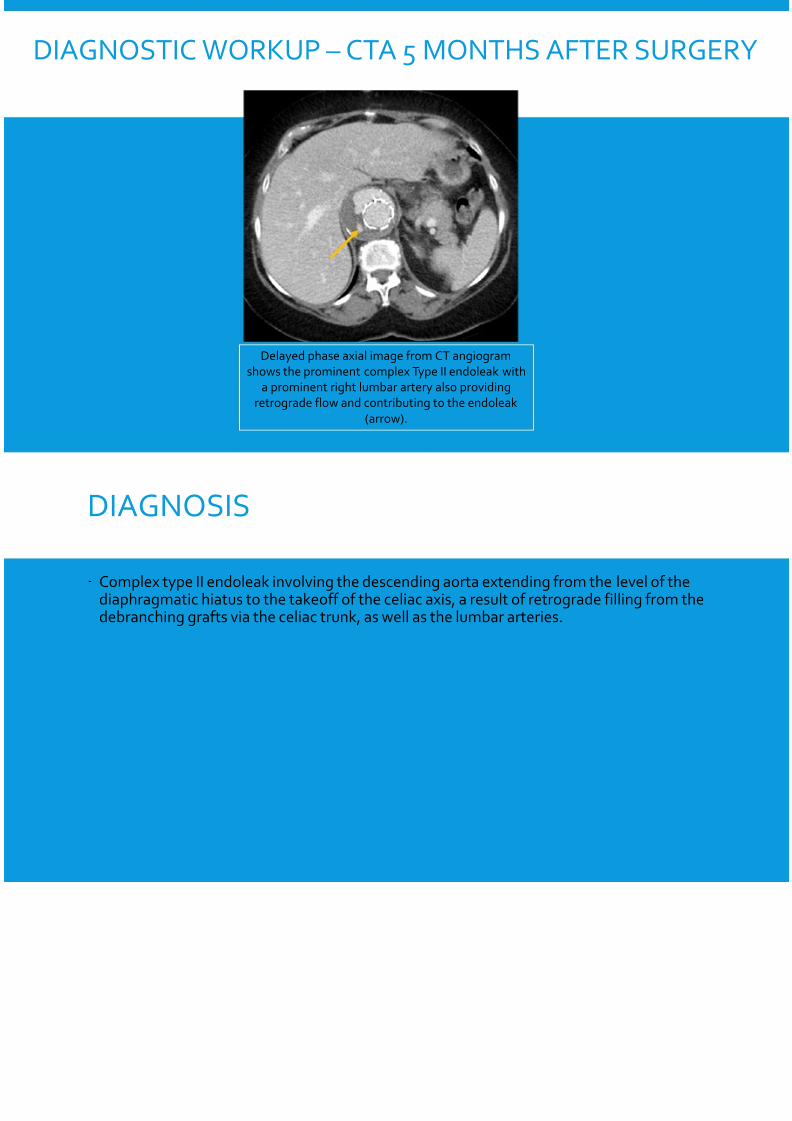
Delayed phase axial image from CT angiogram
shows the prominent complex Type II endoleak with
a prominent right lumbar artery also providing
retrograde flow and contributing to the endoleak
(arrow).

8/11/2019 SIR RFS Case Series: A Complex Endoleak Repair
http://slidepdf.com/reader/full/sir-rfs-case-series-a-complex-endoleak-repair 6/17
DIAGNOSIS
Complex type II endoleak involving the descending aorta extending from the levdiaphragmatic hiatus to the takeoff of the celiac axis, a result of retrograde fillindebranching grafts via the celiac trunk, as well as the lumbar arteries.

8/11/2019 SIR RFS Case Series: A Complex Endoleak Repair
http://slidepdf.com/reader/full/sir-rfs-case-series-a-complex-endoleak-repair 7/17
QUESTION
Which type of endoleak is related to an inadequate seal at the ends of a stent graon one of the following answers)
A. Type I
B. Type II
C. Type III
D. Type IV E. Type V

8/11/2019 SIR RFS Case Series: A Complex Endoleak Repair
http://slidepdf.com/reader/full/sir-rfs-case-series-a-complex-endoleak-repair 8/17
CORRECT!
Which type of endoleak is related to an inadequate seal at the ends of a stent graon one of the following answers)
A. Type I. This is a leak at the graft ends from an inadequate seal.
B. Type II. This is an endoleak that occurs when the aneurysm sac is filled by a branch ve
C. Type III. This type of endoleak is caused by graft failure.
D. Type IV. This type of endoleak is caused by graft porosity.E. Type V. No discernable endoleak is present but the aneurysm size continues to incre
(endotension).
CONTINUE WITH CASE
8/11/2019 SIR RFS Case Series: A Complex Endoleak Repair
http://slidepdf.com/reader/full/sir-rfs-case-series-a-complex-endoleak-repair 9/17
SORRY, THAT’S INCORRECT.
Which type of endoleak is related to an inadequate seal at the ends of a stent graon one of the following answers)
A. Type I. This is a leak at the graft ends from an inadequate seal.
B. Type II. This is an endoleak that occurs when the aneurysm sac is filled by a branch ve
C. Type III. This type of endoleak is caused by graft failure.
D. Type IV. This type of endoleak is caused by graft porosity.E. Type V. No discernable endoleak is present but the aneurysm size continues to incre
(endotension).
CONTINUE WITH CASE
8/11/2019 SIR RFS Case Series: A Complex Endoleak Repair
http://slidepdf.com/reader/full/sir-rfs-case-series-a-complex-endoleak-repair 10/17
INTERVENTION
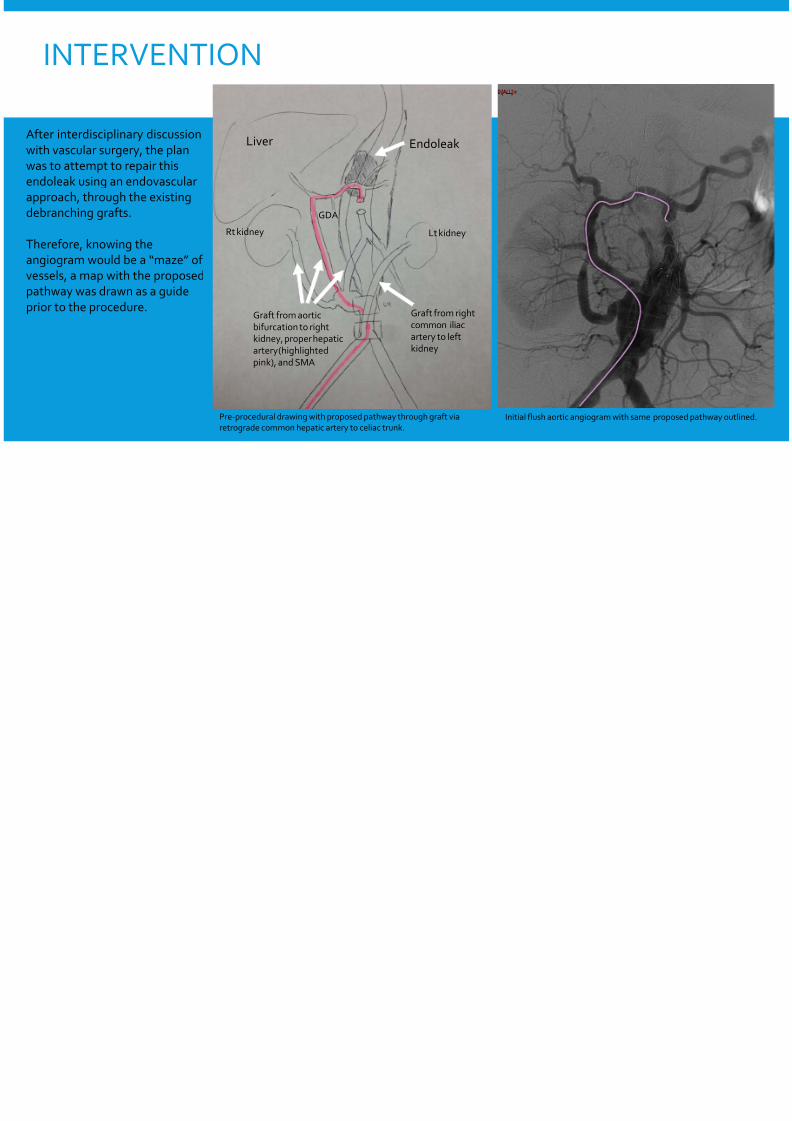
After interdisciplinary discussionwith vascular surgery, the plan
was to attempt to repair this
endoleak using an endovascular
approach, through the existing
debranching grafts.
Therefore, knowing the
angiogram would be a “maze” of
vessels, a map with the proposedpathway was drawn as a guide
prior to the procedure.
Endoleak
Pre-procedural drawing with proposed pathway through graft viaretrograde common hepatic artery to celiac trunk.
Initial flush aortic angiogram with
Graft from aorticbifurcation to rightkidney, proper hepaticartery (highlightedpink), and SMA
Graft from rightcommon iliacartery to leftkidney
Liver
Rt kidney Lt kidney
GDA
Endoleak
8/11/2019 SIR RFS Case Series: A Complex Endoleak Repair
http://slidepdf.com/reader/full/sir-rfs-case-series-a-complex-endoleak-repair 11/17
INTERVENTION – PRE-EMBOLIZATIONANGIOGRAPHY
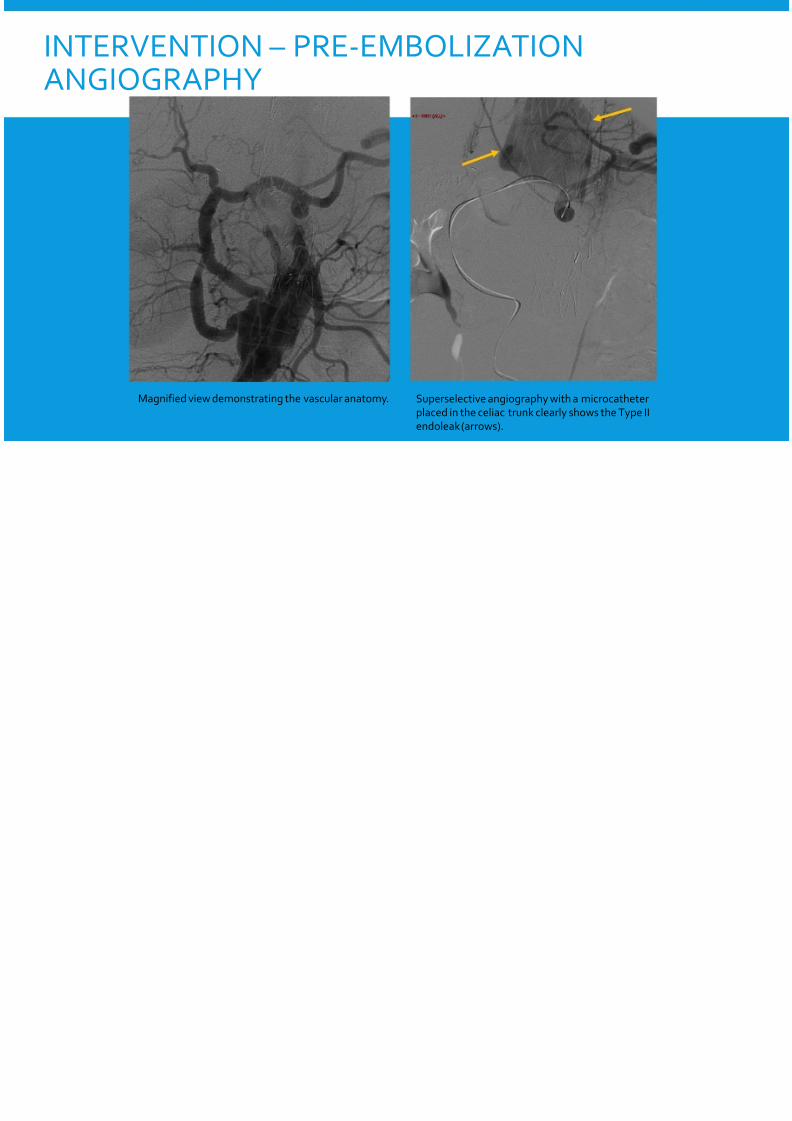
Magnified view demonstrating the vascular anatomy. Superselective angiography with a microcathe
placed in the celiac trunk clearly shows the Tyendoleak (arrows).

8/11/2019 SIR RFS Case Series: A Complex Endoleak Repair
http://slidepdf.com/reader/full/sir-rfs-case-series-a-complex-endoleak-repair 12/17
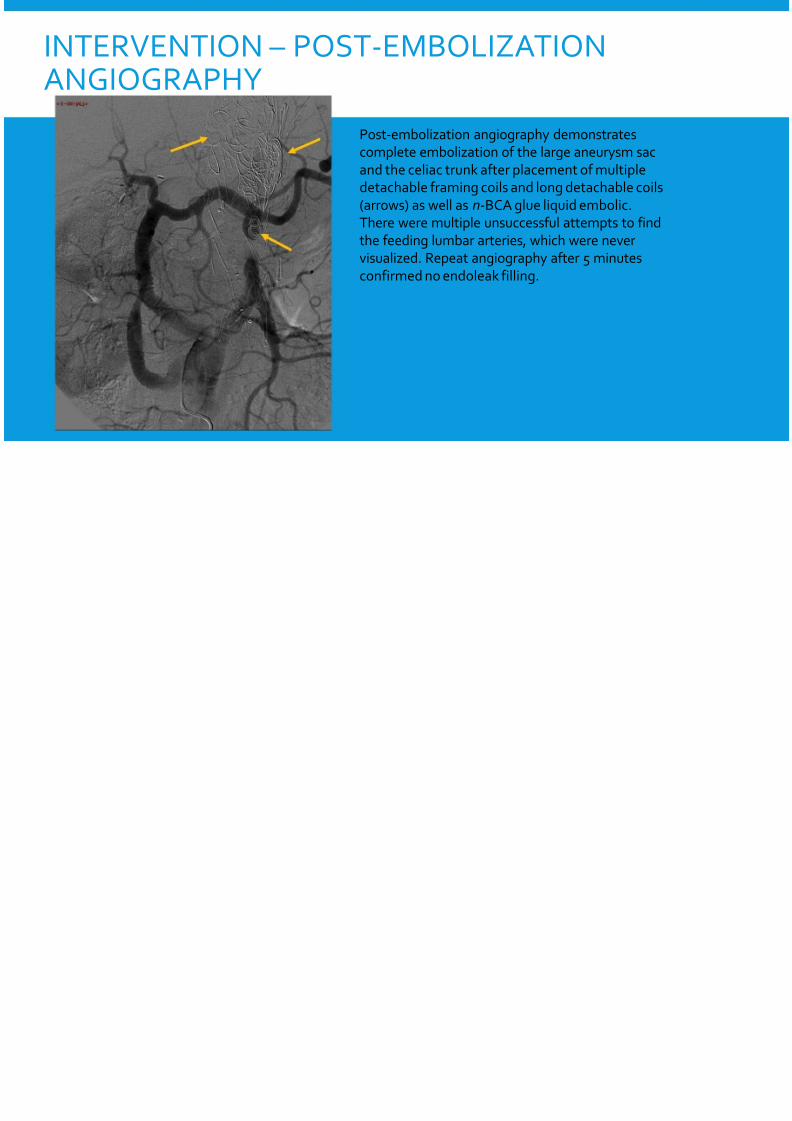
INTERVENTION – POST-EMBOLIZATIONANGIOGRAPHY
Post-embolization angiography demonstratecomplete embolization of the large aneurysmand the celiac trunk after placement of multipdetachable framing coils and long detachable(arrows) as well as n-BCA glue liquid embolicThere were multiple unsuccessful attempts tothe feeding lumbar arteries, which were nevevisualized. Repeat angiography after 5 minut
confirmed no endoleak filling.

8/11/2019 SIR RFS Case Series: A Complex Endoleak Repair
http://slidepdf.com/reader/full/sir-rfs-case-series-a-complex-endoleak-repair 13/17
SUMMARY & TEACHING POINTS
•Large complex Type II endoleak in a patient status post TEVAR and EVAR witprocedure to reperfuse her mesenteric vessels
• Two sources were identified for the endoleak, including the celiac artery as wlumbar arteries
• Proper planning was essential given the complicated anatomy following theand a map drawn based off of the CTA was invaluable in navigating to the or
endoleak at the celiac trunk• Technically successful endovascular endoleak repair through the debranchin
retrograde approach from the proper hepatic artery with successful coil andembolization of the endoleak as well as the celiac trunk feeding vessel

8/11/2019 SIR RFS Case Series: A Complex Endoleak Repair
http://slidepdf.com/reader/full/sir-rfs-case-series-a-complex-endoleak-repair 14/17
QUESTION
How are type II endoleaks typically repaired?
A. Placement of extension endograft modules adjacent to the endoleak
B. Placement of transmural fixation devices to anchor the endograft to th
C. Trans-arterial/trans-lumbar embolization of the endoleak cavity and fe
D. Open surgical repair
8/11/2019 SIR RFS Case Series: A Complex Endoleak Repair
http://slidepdf.com/reader/full/sir-rfs-case-series-a-complex-endoleak-repair 15/17
CORRECT!
How are type II endoleaks typically repaired?
A. Placement of extension endograft modules adjacent to the endoleak
B. Placement of transmural fixation devices to anchor the endograft to th
C. Trans-arterial/trans-lumbar embolization of the endoleak cavity and fe
D. Open surgical repair
CONTINUE WITH CASE

8/11/2019 SIR RFS Case Series: A Complex Endoleak Repair
http://slidepdf.com/reader/full/sir-rfs-case-series-a-complex-endoleak-repair 16/17
SORRY, THAT’S INCORRECT.
How are type II endoleaks typically repaired?
A. Placement of extension endograft modules adjacent to the endoleak
B. Placement of transmural fixation devices to anchor the endograft to th
C. Trans-arterial/trans-lumbar embolization of the endoleak cavity and fe
D. Open surgical repair
CONTINUE WITH CASE

8/11/2019 SIR RFS Case Series: A Complex Endoleak Repair
http://slidepdf.com/reader/full/sir-rfs-case-series-a-complex-endoleak-repair 17/17
REFERENCES
Rosen R.J., Green R.M. Endoleak Management following Endovascular Aneurysm Repair. J Vasc Inte2008; 19(6):S37-S43
Stavropoulos S.W., Charagundla S.R. Imaging techniques for detection and management of endoleendovascular aortic aneurysm repair. Radiology. 2007;243 (3): 641-55
Bashir M.R., Ferral H. et-al. Endoleaks after endovascular abdominal aortic aneurysm repair: managstrategies according to CT findings. AJR Am J Roentgenol. 2009;192 (4): W178-86
Hong C., Heiken J.P. et-al. Clinical significance of endoleak detected on follow-up CT after endovascabdominal aortic aneurysm. AJR Am J Roentgenol. 2008;191 (3): 808-13

















