Page 1
Effective Date: 01/01/16 Author: Heisey, Shirley S Review History: None Owner: Oxler, Karen F Revision History: 7/30/2015 Page 1 of 23
POLICY PURPOSE
To provide an interdisciplinary, standardized approach to the assessment of skin, prevention of
breakdown, and management of wounds.
GOALS
1. Identify at risk patients and initiate early interventions for prevention of skin breakdown.
2. Protect against the adverse effects of pressure, shear, friction, and moisture.
3. Reduce the incidence of hospital-acquired pressure ulcers.
SCOPE
Any licensed or unlicensed professional that has the ability to assess and/or intervene to the patient’s
Braden risk including personnel from the following areas:
- Nursing
- Physical Therapy
- Occupational Therapy
- Nutritional Services
- Respiratory
- Non licensed staff who will care for patients and document within their scope
- All patients at Lancaster General Hospital (Duke Street, WBH)
POLICY DETAILS
Supportive Data: The skin is the largest organ of the body and therefore is easily affected by all other
organ systems. A structured approach to pressure ulcer reduction can be achieved through the use of a
risk assessment scale in combination with a comprehensive skin assessment and clinical judgment.
Lyder et al (Journal of American Geriatric Society, 2012) found that individuals who developed pressure
ulcers were more likely to die during the hospital stay, have generally longer hospital stays, and were
more likely to be readmitted than those who did not acquire pressure ulcers.
POLICY TITLE: SKIN CARE – ASSESSMENT PREVENTION AND
INTERVENTION POLICY Former Policy Title:
Page 2
POLICY TITLE: SKIN CARE ASSESSMENT PREVENTION AND INTERVENTION
Effective Date: 01/01/16 Author: Heisey, Shirley S Review History: None Owner: Oxler, Karen F Revision History: 7/30/2015 Page 2 of 23
DEFINITION(S)
Pressure Ulcer
(PU)
A pressure ulcer is localized injury to the skin and/or underlying tissue usually over a
bony prominence, as a result of pressure, or pressure in combination with shear.
Pressure – Pressure is the force that is applied vertically or perpendicular to the
surface of the skin. Pressure compresses underlying tissue and small blood vessels
hindering blood flow and nutrient supply. Tissues become ischemic and are
damaged or die.
Shear – Shear occurs when one layer of tissue slides horizontally over another,
deforming adipose and muscle tissue, and disrupting blood flow (e.g., when the
head of the bed is raised >30 degrees). Both require pressure exerted by body
against bed/chair surface to create the tissue injury.
Other location – Pressure ulcers can develop on any skin surface subject to
excess pressure such as under oxygen tubing, drainage tubing, casts, cervical
collars or other medical devices. (NDNQI, 2013)
Community
Acquired
Pressure Ulcer
(CAPU)
Pressure ulcers that developed prior to hospital admission. The existence of the pressure
ulcer(s) was documented on the admission skin assessment or the survey was done on day
1 of the patient’s hospital stay and the pressure ulcer was already present. Pressure ulcers
that are present on admission (POA) and worsen during the patient’s length of stay are
still considered community acquired.
Must be assessed and documented within 24 hours of admission or PU is
considered Hospital Acquired per NDNQI (2013).
Hospital
Acquired
Pressure Ulcer
(HAPU)
Hospital acquired refers to new pressure ulcer(s) that developed after admission to your
facility. Also termed nosocomial or facility-acquired. The patient’s admission record
should be reviewed for the documentation of a pressure ulcer. If there is no documentation
that the pressure ulcer was present on admission, then the pressure ulcer is counted as
hospital acquired. (NDNQI)
Stage I
Intact skin with non-blanchable redness of a localized area usually over a bony
prominence. Darkly pigmented skin may not have visible blanching; its color may
differ from the surrounding area. The area may be painful, firm, soft, warmer or
cooler as compared to adjacent tissue. May be difficult to detect in individuals
with dark skin tones.
Stage II Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink
wound bed, without slough. May also present as an intact or open/ruptured serum-
filled blister.
Note: This stage should not be used to describe skin tears, tape burns,
perineal dermatitis, maceration or excoriation.
Stage III Full thickness tissue loss. Subcutaneous fat may be visible but bone, tendon, or
muscle are not exposed. Slough may be present but does not obscure the depth of
tissue loss. May include undermining and tunneling.
Note: The bridge of the nose, ear, occiput and malleolus do not have
(adipose) subcutaneous tissue. Thus these areas with underlying cartilage
structure rarely have pressure ulcers Staged as stage III. In contrast, areas of
Page 3
POLICY TITLE: SKIN CARE ASSESSMENT PREVENTION AND INTERVENTION
Effective Date: 01/01/16 Author: Heisey, Shirley S Review History: None Owner: Oxler, Karen F Revision History: 7/30/2015 Page 3 of 23
significant adiposity can develop extremely deep Stage III pressure ulcers.
Bone/tendon is not visible or directly palpable.
Stage IV Full thickness tissue loss with exposed bone, cartilage, tendon or muscle. Slough
or eschar may be present on some parts of the wound bed. Often include
undermining and tunneling
Note: Stage IV pressure ulcers can extend into muscle and /or supporting
structures (e.g,. fascia, tendon or joint capsule) making osteomyelitis possible.
Exposed bone/tendon is visible or directly palpable.
It is the opinion of NPUAP that cartilage serves the same anatomical function as bone.
Therefore, pressure ulcers that have exposed cartilage should be classified as a Stage IV
http://www.npuap.org/wp-content/uploads/2012/01/Cartilage-Position-
Statement1.pdf
Mucosal
Pressure Ulcer/
Indeterminable
Pressure ulcers found on mucous membranes with a history of a medical device in
use at the location of the ulcer.
The position of the National Pressure Ulcer Advisory Panel (NPUAP) is that
pressure ulcers on mucosal surfaces are not to be staged using the pressure ulcer
staging system. It is understood that these ulcers may indeed be due to pressure,
however anatomically analogous tissue comparisons cannot be made. Further, it is
NPUAP’s position that mucosal pressure ulcers not be classified as partial or full
thickness, because the clinical assessment of the tissue does not allow the
distinction. Therefore, the position of NPUAP is that pressure ulcers on mucous
membranes be labeled as mucosal pressure ulcers without a stage identified.
(NPUAP, 2012) http://www.npuap.org/wp-
content/uploads/2012/03/Mucosal_Pressure_Ulcer_Position_Statement_final.pdf
Suspected Deep
Tissue Injury
(sDTI)
Purple or maroon localized area of discolored intact skin or blood-filled blister due
to Damage of underlying soft tissue from pressure and/or shear. The area may be
preceded by tissue that is painful, firm, mushy, boggy, warmer or cooler as
compared to adjacent tissue.
Note: sDTI may be difficult to detect in individuals with dark skin tones, Pain
may be the only symptom Evolution may include a thin blister over a dark
wound bed. The wound may further evolve and become covered by thin eschar.
Evolution may be rapid exposing additional layers of tissue even with optimal
treatment.
Unstageable Full thickness tissue loss in which the base of the ulcer is covered by slough
(yellow, tan, gray, green or brown) and/or eschar (tan, brown or black) in the
wound bed.
Eschar Black or brown necrotic devitalized tissue; tissue can be loose or firmly adherent,
hard, soft, or soggy. (WOCN, 2010)
Incontinence
Associated
Dermatitis
(IAD)
An inflammation of the skin that occurs when urine or stool comes into contact
with perineal or perigenital skin. (WOCN, 2010).
Page 4
POLICY TITLE: SKIN CARE ASSESSMENT PREVENTION AND INTERVENTION
Effective Date: 01/01/16 Author: Heisey, Shirley S Review History: None Owner: Oxler, Karen F Revision History: 7/30/2015 Page 4 of 23
Fungal
Infection
Inflammation with satellite red or white vesicles (Bryant & Nix, 2012)
Intertrigo Mild inflammatory process that occurs on opposing skin surfaces caused by
friction and moisture such as groin or axilla (Bryant & Nix, 2012)
Definitions obtained from American Nurses Association, NDNQI Data Collection Guidelines (2013)
unless otherwise noted.
http://www.npuap.org/resources/educational-and-clinical-resources/npuap-pressure-ulcer-
stagescategories/
ROLE(S)/REPONSIBILITIES
Direct Patient Care
Providers Responsible to visually inspect skin integrity during the provision of care and
report and document any significant findings to the RN or physician.
Registered Nurse
Complete and document Braden Risk Assessment Score and head to toe skin
assessment within 8 hours of admission, daily, and with any change in condition
or transfer of care
Activate appropriate clinical practice guidelines based on patient condition and
level of Braden risk and additional risk factors
Consult Wound Care RN if any (POA) pressure ulcer worsens or progresses to
next stage and upon assessment of any newly identified unit acquired pressure
ulcer
2 RNs to validate new or changes in pressure ulcers on the off shift and weekends
when WOCN not available
Collaborate with interdisciplinary team to address early intervention based on
Braden subscores and initiate interdisciplinary plan of care
Inpatient
Wound/Ostomy
Certified RN
Validate nurse findings for POA pressure ulcers stage III, IV, suspected DTI, and
unstageable, indeterminable
Validate nurse findings for hospital/unit acquired pressure ulcers. See when to
consult the inpatient wound/ostomy nurse appendix
Registered
Dietician Collaborate with Registered Nurse and Physician to obtain appropriate nutrition
orders for at risk patients
Provide nutrition education to at risk patients and their families
Occupational
Therapy/Physical
Therapy
Collaborate with Registered Nurse to educate patient and family on positioning
techniques in bed and in chair for at risk patients
Collaborate with Physician and Registered Nurse to determine the need for a seat
cushion
Respiratory
Therapy Assess areas of skin that are in contact with respiratory equipment during routine
treatments.
Initial Risk Assessment & Reassessment Provider Any licensed professional that has the ability to assess and intervene to the
Page 5
POLICY TITLE: SKIN CARE ASSESSMENT PREVENTION AND INTERVENTION
Effective Date: 01/01/16 Author: Heisey, Shirley S Review History: None Owner: Oxler, Karen F Revision History: 7/30/2015 Page 5 of 23
patient’s Braden risk
Initial Braden
Risk Screen
Initial Braden risk screening will be documented within 8 hours of admission.
Braden Risk
Reassessment
Braden risk reassessment will be completed daily, with any significant change
in condition, or transition in care.
PROCEDURE:
Assessment Standards
Risk Assessment: All patients will be assessed for risk of pressure ulcers and skin breakdown
using the Braden Scale, within eight hours of admission, daily, with any significant change in
condition, or transfer of department. If the patient has a Braden Score of < 18 launch Pressure
Ulcer Risk (Using Braden Scale) (Adult)
Note: The Braden Scale for Predicting Risk is a standardized tool used for determining the level
of risk for pressure ulcers in adult patients.
15-18 = mild risk
13-14 = moderate risk
10-12 = high risk
</= 9 = very high risk
Appendix A: Braden Scale for Predicting Pressure Sore Risk
Skin Assessment: Perform head to toe assessment of skin within 8 hours of admission, daily, with any
significant change in condition. On transfer of department the assessment must be documented within 4
hours of transfer. If outside the 4 hours this would be unit acquired and document in Patient Care
Summary appropriate skin LDA in Doc Flow sheets.
Major Risk Factors for the Development of Pressure Ulcers
- General state of health (poor, debilitated, moribund, elderly)
- Chronic illness (e.g., diabetes, COPD, immunosuppression)
- Poor nutritional state
- Immobility due to diagnosis of fractured hip, fractured femur, sepsis, diabetic patient
on bed rest, restraints, etc.
- Incontinence
- Oxygenation/Circulation (peripheral vascular disease, respiratory or circulatory
impairment, smoking)
- Medications (e.g., corticosteroids, chemotherapy, anticoagulants, sedatives,
analgesics)
- Altered levels of consciousness (e.g., lethargic, comatose)
- Spasticity, contractures
- Edema
- Peripheral neuropathy
- Acute care length of stay greater than or equal to 5 days
- Infection/Fever
Page 6
POLICY TITLE: SKIN CARE ASSESSMENT PREVENTION AND INTERVENTION
Effective Date: 01/01/16 Author: Heisey, Shirley S Review History: None Owner: Oxler, Karen F Revision History: 7/30/2015 Page 6 of 23
- Diastolic BP less than 60mm Hg
- Hemodynamic instability
Assess for other extrinsic risk factors:
- Review resolved/unresolved pressure ulcer LDA’s (Lines/Drains/Airway) for current
risk of breakdown
- Use of supportive medical devices: nasal cannulas, tubes (ie: nasogastric tubes, foley
catheters, fecal management systems, etc), glasses, hearing aids, casts, respiratory
mask, immobilizers, ace wraps
- Poor hygiene
- Undergoing surgery with long operative procedures
- Prolonged time on litters
- History of skin breakdown/pressure ulcers
- Poor dentition
- Dysphagia
See Appendix D: Device-Related Skin Protection Guide
Measuring:
What: Bruises, rashes, lesions, ulcers, wounds, reddened areas, skin tears, incision lines
How: Length (L) is 12(toward patient’s head) to 6 o’clock (toward the patient’s feet)
Width (W) is 3 to 9 o’clock
Depth (D) is straight 90 degrees down into deepest wound area. To measure the depth of
a wound, use a sterile, cotton-tipped applicator
Tunneling/Sinus tract- measure longest tract using sterile cotton-tipped applicator,
Document tract length and use a clock face to indicate direction of tunneling
Undermining – measure underlying tissue void at wound edge from ** o’clock to **
o’clock using sterile cotton-tipped applicator.
Document length and use a clock face to indicate direction of tissue void
When: On admission, Weekly (Mondays), with any significant changes i.e. debridement,
growth, and with initial Negative Pressure wound dressing changes.
Documentation for prevention and treatment Pressure Ulcers:
Assessments and interventions should be documented in EMR as follows:
Prior to initial assessment review Epic documentation under discharge tab, LDA removal for
previous documented skin LDA’s
- Re- launch active LDA’s/resolve old LDA’s after skin assessment to align with current
assessment findings.
- If no LDA exists for assessed pressure ulcer then launch a new one.
- Documentation on all rows under current LDA’s
- If Pressure Ulcer Found Launch and initiate Pressure Ulcer CPG and Pressure Risk CPG
- Utilize EMR Patient Story to communicate presence of Pressure Ulcers/Wounds on
admission, discharge and intradepartmental transfer during Hand-off report.
Page 7
POLICY TITLE: SKIN CARE ASSESSMENT PREVENTION AND INTERVENTION
Effective Date: 01/01/16 Author: Heisey, Shirley S Review History: None Owner: Oxler, Karen F Revision History: 7/30/2015 Page 7 of 23
- As part of 24 Hour Chart Check remove any Pressure Ulcer/Wound/Incision LDA that is
no longer present on patient in current admission. This can be done by clicking on
Discharge tab LDA Removal Remove Now
Education:
- Using the teach-back method, educate patients, caregivers, and healthcare providers
involved in the continuum of care about prevention, treatment and factors contributing to
recurrence of pressure ulcers. Evaluate patient/caregiver learning as evidenced by their
ability to describe the disease process and prevention/treatment plans, correct
demonstration of care, and active participation in the treatment plan.
- Document any and all teaching re: wound/pressure ulcer under appropriate education title
automatically launched when CPG launched. Additional titles can be added individually
as is appropriate.
- Utilize Clinical reference tab in EMR to provide “Your Care Instruction” education
sheets to patients and family.
Special Populations: The modified Braden Q for Neonates will be the tool used in the NICU. The
Braden Q will be used for the risk assessment of infants and pediatric patients up to the age of 8. For
patients greater than 8 years old use the Braden Scale for Adults, understanding that in the pediatric
population, most pressure injuries are caused by medical devices that the Braden Scale cannot predict.
Prevention
Interventions for all patients -
- Ambulate patient if possible
- Make sure knee is supported when elevating lower extremities
- Do not use vigorous massage over reddened areas and bony prominences
- Limit to one incontinence pad under patient
- Cleanse skin after each incontinence episode with non-irritating soaps
Note: normal pH of skin is 4.5-5.5 (acidic), choose cleansers lower on the
alkaline side, pH balanced, and lipid-based.
- Apply clean linen and incontinence pad daily and as needed
- Offer to moisturize skin with lotion daily and as needed
- Apply skin protectant cream (barrier cream) to skin that is exposed to feces,
urine, or moisture; reapply after cleansing
- Avoid positioning patient directly on bony prominences
- Utilize pressure redistribution surfaces
- Consider use of Foam Dressing per criteria listed in Appendix G
- Encourage eating and drinking if not contraindicated by Plan of Care
- Encourage patient to reposition or assist patient if they are unable to position
self. While in bed, repositioning should occur at least every 2 hours. While in
chair, repositioning should occur every hour.
- Offloading devices for the chair and heels include:
Air filled seat cushion/ SAPS
Air filled heel protector boots and padded fabric heel protector
boots. -
Page 8
POLICY TITLE: SKIN CARE ASSESSMENT PREVENTION AND INTERVENTION
Effective Date: 01/01/16 Author: Heisey, Shirley S Review History: None Owner: Oxler, Karen F Revision History: 7/30/2015 Page 8 of 23
- Avoid positioning directly on the trochanter when using the side-lying lateral
position
- Educate patient, family members, and caregivers on pressure ulcer prevention
strategies
Interventions based on Braden Subscores
1. Sensory Perception (Score </= 3 implement following interventions)
- Teach patient and family importance of turning and positioning
- Encourage small frequent changes in position
- Use pillows to separate bony prominences
- Elevate heels off bed by placing pillow under calf muscle
- Instruct/assist patient to change position while in chair or wheelchair
- Consider limiting time in chair to one hour or less
- Use, positioning pad or mechanical lift to lift/move patient while in bed
2. Moisture (Score </= 3 implement following interventions)
- Assess and address cause of moisture
- Evaluate type of incontinence, if any (urinary, fecal, or both) and implement
toileting schedule or bowel/bladder program when appropriate
- Contain any wound drainage using sterile gauze dressing and changing upon
moderate saturation (unless specific dressing type and frequency ordered by
physician)
- Keep skin folds dry
- Use incontinence skin barrier cream and absorbent pads as needed to protect
and maintain intact skin
- Consider fecal management system if skin breakdown is already present and
patient is incontinent of stool
- Do not use incontinence briefs unless patient is out of bed, going for a test, or
going to /participating with physical therapy
3. Activity (Score </= 3 implement following interventions)
- Encourage activity as tolerated (Walk patient 3 times/day)
- Teach patient and family importance of turning and positioning to prevent
pressure ulcers
- Elevate heels off bed by placing pillow under calf muscle
- Keep head of bed (HOB) at or below 30 degrees unless medically
contraindicated to prevent shearing
- Instruct/assist patient to change position while in chair or wheelchair
- Consider limiting time in chair to one hour or less
- Use Under pad or Turning System to lift/move patient while in bed
- Consider consult to Physical Therapy/Occupational Therapy
- If patient chair-bound consult OT for seating evaluation
- Apply Sacral Foam Dressing unless contraindicated per criteria listed in
Appendix G
4. Mobility (Score </= 3 implement following interventions)
- See Activity interventions
Page 9
POLICY TITLE: SKIN CARE ASSESSMENT PREVENTION AND INTERVENTION
Effective Date: 01/01/16 Author: Heisey, Shirley S Review History: None Owner: Oxler, Karen F Revision History: 7/30/2015 Page 9 of 23
5. Nutrition (Score </= 3 implement following interventions)-
See Appendix C: Nutrition
- Provide tray set up and assistance when required
- Offer supplements high in protein in addition to usual diet
- Consult nutrition for Braden subscore </= 2 and total Braden score of </= 18
- Record % oral intake (doc flow sheet under Nutrition)
- Record oral fluid intake (I&O documentation)
6. Friction & Shear (Score </= 2 implement following interventions)
- Use absorbent pads if needed to mechanically lift/move patient in bed
- Keep HOB at or below 30 degrees unless medically contraindicated to prevent
shearing
- Consider use of heel/elbow protectors
- Reduce pressure created by medical devices, use of foam (See Device
Appendix)
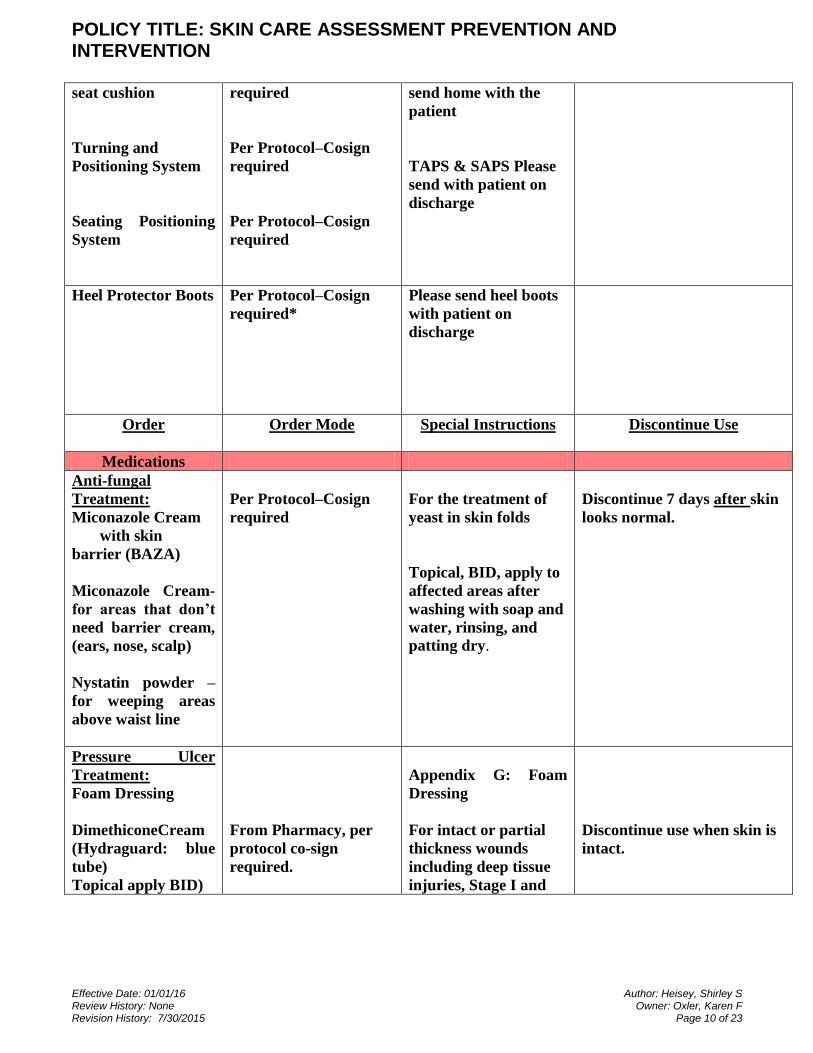
Skin Care Orders for Nursing
**When entering a Per Protocol – Cosign required order an SBAR will be completed explaining
the need for and reasoning behind the order.
Order Order Mode Special Instructions Discontinue Use
Equipment
Specialty Beds
Low Air Low
Mattress
replacement (First
Step/ ETS )
Low Airloss Bed (
Kinair)
Bariatric Bed
Air Filled seat
cushion
Air Filled Bariatric
Nursing Referral
Nursing Referral
Nursing Referral
Nursing Referral
Per Protocol–Cosign
For use treatment of
severe moisture related
skin breakdown
Recent onset paralysis,
stage 4 on trunk, post
flap graft on trunk,
Over 500lbs, or needed
for improved bed
mobility with large
abdominal girth.
Up to 350lbs- please
send home with the
patient
Over 350lbs- please
May discontinue low airloss
replacement when moisture
related skin damage resolves.
Page 10
POLICY TITLE: SKIN CARE ASSESSMENT PREVENTION AND INTERVENTION
Effective Date: 01/01/16 Author: Heisey, Shirley S Review History: None Owner: Oxler, Karen F Revision History: 7/30/2015 Page 10 of 23
seat cushion
Turning and
Positioning System
Seating Positioning
System
required
Per Protocol–Cosign
required
Per Protocol–Cosign
required
send home with the
patient
TAPS & SAPS Please
send with patient on
discharge
Heel Protector Boots Per Protocol–Cosign
required*
Please send heel boots
with patient on
discharge
Order Order Mode Special Instructions Discontinue Use
Medications
Anti-fungal
Treatment:
Miconazole Cream
with skin
barrier (BAZA)
Miconazole Cream-
for areas that don’t
need barrier cream,
(ears, nose, scalp)
Nystatin powder –
for weeping areas
above waist line
Per Protocol–Cosign
required
For the treatment of
yeast in skin folds
Topical, BID, apply to
affected areas after
washing with soap and
water, rinsing, and
patting dry.
Discontinue 7 days after skin
looks normal.
Pressure Ulcer
Treatment:
Foam Dressing
DimethiconeCream
(Hydraguard: blue
tube)
Topical apply BID)
From Pharmacy, per
protocol co-sign
required.
Appendix G: Foam
Dressing
For intact or partial
thickness wounds
including deep tissue
injuries, Stage I and
Discontinue use when skin is
intact.
Page 11
POLICY TITLE: SKIN CARE ASSESSMENT PREVENTION AND INTERVENTION
Effective Date: 01/01/16 Author: Heisey, Shirley S Review History: None Owner: Oxler, Karen F Revision History: 7/30/2015 Page 11 of 23
Hydrogel: NSS
(Intrasite Gel)
Topical, apply BID
to affected areas and
cover with
secondary dressing.
From Pharmacy, per
protocol, co-sign
required
Stage II Pressure
ulcers. May also be
used on arms and legs
for very dry skin.
For application on full
thickness wounds
including Stage III and
Stage IV pressure
ulcers.
Discontinue use when skin is
intact.
PMR/Diet/Nursing
PT/OT Seating
Consult
Per Protocol–Cosign
required
New stage IV Pressure
Ulcer, Quadriplegic or
Paraplegic
Nutrition Consult Nursing Referral See Appendix C:
Nutrition
Fecal Management
System
Per Protocol–Cosign
required
For frequent
incontinence of stool
creating risk of skin
breakdown
See Fecal Management
System Procedure
Strategies for Safe Patient Hand-off Across the Continuum of Care
- All surgical/invasive procedural patients are considered at risk for pressure
ulcer development and standard pressure ulcer prevention is initiated
- Upon intradepartmental transfer (i.e., ED to unit, unit to pre-procedure, pre-
procedure to post-procedure, post-procedure to unit, etc) the sending RN will
communicate to the receiving RN:
- Most recent Braden Assessment Score
- Any history of previous pressure ulcer
- Any current pressure ulcers
- Following a surgery/procedure, sending RN will also include in report to
receiving RN:
- Length of time on the table
- Patient positioning during procedure
Position Areas at risk for pressure ulcer
- Supine - Scapula, occiput, elbows, sacrum, coccyx,
heels
- Lateral - Ear, acromion process, trochanter, medial
Page 12
POLICY TITLE: SKIN CARE ASSESSMENT PREVENTION AND INTERVENTION
Effective Date: 01/01/16 Author: Heisey, Shirley S Review History: None Owner: Oxler, Karen F Revision History: 7/30/2015 Page 12 of 23
and lateral condyles of the knee, malleolus, foot
edge on involved side
- Prone/Jackknife Nose, forehead, chest, acromion process, genitalia,
breasts, iliac crests, patella, foot edge and toes
(Bryant & Nix, 2012)
RELATED DOCUMENTS
NPUAP Quick Reference Guide for Prevention
NPUAP Quick Reference Guide for Treatment
AACN Manual
APPENDICE(S): Reference Guide
Appendix A: Braden Scale for Predicting Pressure Sore Risk
Appendix B: Skin Care Orders Chart
Appendix C: Nutrition
Appendix D: Device-Related Skin Protection Guide
Appendix E: When to Consult Inpatient Wound Care Nurse
Appendix F: Molnlycke Product Guide
Appendix G: Foam Dressing
REFERENCES
American Nurses Association (2013). NDNQI Data Collection Guidelines.
Bryant, R. & Nix, D. (2012). Acute & Chronic Wounds (4th). Current management concepts.
Clinical Practice Guideline: SKIN INTEGRITY IMPAIRMENT, RISK/ACTUAL from CPM Resource
Center, Elsevier, v-Fall 2011
Clinical Practice Guideline: PRESSURE ULCER RISK (USING BRADEN SCALE) from CPM
Resource Center, Elsevier, v-Fall 2011
Clinical Practice Guideline: PRESSURE ULCER from CPM Resource Center, Elsevier, v-Fall 2011
European Pressure Ulcer Advisory Panel and National Pressure Ulcer Advisory Panel. (2009).
Prevention and treatment of pressure ulcers: quick reference guide. Washington D.C.: National Advisory
Panel. http://www.npuap.org/wp-content/uploads/2012/03/Final_Quick_Prevention_for_web_2010.pdf
Lyder, C. H., Wang, Y., Metersky, M., Curry, M., Kliman, R., Verzier, N. R., & Hunt, D. R. (2012).
Hospital-Acquired Pressure Ulcers: Results from the National Medicare Patient Safety Monitoring
System Study. Journal Of The American Geriatrics Society, 60(9), 1603-1608.
doi:http://dx.doi.org/10.1111/j.1532- 5415.2012.04106.x
Page 13
POLICY TITLE: SKIN CARE ASSESSMENT PREVENTION AND INTERVENTION
Effective Date: 01/01/16 Author: Heisey, Shirley S Review History: None Owner: Oxler, Karen F Revision History: 7/30/2015 Page 13 of 23
National Pressure Ulcer Advisory Panel. Pressure Ulcers with Exposed Cartilage are Stage IV Pressure
Ulcers: An NPUAP Position Statement. 2012. Available from: http://www.npuap.org/
Parslow, N., Barton, P., Harris, C., Harrison, M., Labreche, D., MacLeod, F., et al. (2005). Risk
assessment and prevention of pressure ulcers. Registered Nurses' Association of Ontario (RNAO).
Retrieved April 10, 2013, from http://www.rnao.org/Page.asp?PageID=924&ContentID=816
Wound Ostomy and Continence Nurses Society. (2010). Guideline for prevention and management of
pressure ulcers. Mount Laurel, NJ: WOCN.
Appendix A: Braden Scale for Predicting Pressure Sore Risk
Page 14
POLICY TITLE: SKIN CARE ASSESSMENT PREVENTION AND INTERVENTION
Effective Date: 01/01/16 Author: Heisey, Shirley S Review History: None Owner: Oxler, Karen F Revision History: 7/30/2015 Page 14 of 23
Appendix B: Skin Care Order Chart
Page 15
POLICY TITLE: SKIN CARE ASSESSMENT PREVENTION AND INTERVENTION
Effective Date: 01/01/16 Author: Heisey, Shirley S Review History: None Owner: Oxler, Karen F Revision History: 7/30/2015 Page 15 of 23
Skin Care Orders for Nursing
**When entering a Per Protocol – Cosign required order an SBAR will be completed explaining
the need for and reasoning behind the order.
Order Order Mode Special Instructions Discontinue Use
Equipment
Specialty Beds
Low Air Low Mattress
replacement (First Step/
ETS)
Low Air loss Bed ( Kinair)
Bariatric Bed
Air Filled seat cushion
Air Filled Bariatric seat
cushion
Turning and Positioning
System
Seating Positioning System
Nursing Referral
Nursing Referral
Nursing Referral
Nursing Referral
Per Protocol–Cosign
required
Per Protocol–Cosign
required
Per Protocol–Cosign
required
For use treatment of
severe moisture related
skin breakdown
Recent onset paralysis,
stage IV on anatomical
trunk, post flap graft on
anatomical trunk,
Over 500lbs, or needed for
improved bed mobility
with large abdominal
girth.
Up to 350lbs- please send
home with the patient
Over 350lbs- please send
home with the patient
TAPS & SAPS Please send
with patient on discharge
May discontinue
low air loss
replacement when
moisture related
skin damage
resolves.
Heel Protector Boots Per Protocol–Cosign
required*
Please send heel boots
with patient on discharge
Page 16
POLICY TITLE: SKIN CARE ASSESSMENT PREVENTION AND INTERVENTION
Effective Date: 01/01/16 Author: Heisey, Shirley S Review History: None Owner: Oxler, Karen F Revision History: 7/30/2015 Page 16 of 23
Order Order Mode Special Instructions Discontinue Use
Medications
Anti-fungal Treatment:
Miconazole Cream
with skin barrier
(BAZA)
Miconazole Cream- for
areas that don’t need
barrier cream, (ears, nose,
scalp)
Nystatin powder – for
weeping areas above waist
line
Per Protocol–Cosign
required
For the treatment of yeast
in skin folds
Topical, BID, apply to
affected areas after
washing with soap and
water, rinsing, and patting
dry.
Discontinue 7 days
after skin looks
normal.
Pressure Ulcer Treatment:
Foam Dressing
Dimethicone Cream
(Hydraguard: blue tube)
Topical apply BID)
Hydrogel: NSS (Intrasite
Gel)
Topical, apply BID to
affected areas and cover
with secondary dressing.
From Pharmacy, per
protocol co-sign
required.
From Pharmacy, per
protocol, co-sign
required
Appendix G: Foam
Dressing
For intact or partial
thickness wounds
including deep tissue
injuries, Stage I and Stage
II Pressure ulcers. May
also be used on arms and
legs for very dry skin.
For application on full
thickness wounds
including Stage III and
Stage IV pressure ulcers.
Discontinue use
when skin is intact.
Discontinue use
when skin is intact.
PMR/Diet/Nursing
PT/OT Seating Consult Per Protocol–Cosign
required
New stage IV Pressure
Ulcer, Quadriplegic or
Paraplegic
Nutrition Consult Nursing Referral Appendix C: Nutrition
Fecal Management System Per Protocol–Cosign
required
For frequent incontinence
of stool creating risk of
skin breakdown
Page 17
POLICY TITLE: SKIN CARE ASSESSMENT PREVENTION AND INTERVENTION
Effective Date: 01/01/16 Author: Heisey, Shirley S Review History: None Owner: Oxler, Karen F Revision History: 7/30/2015 Page 17 of 23
See Fecal Management
System Procedure
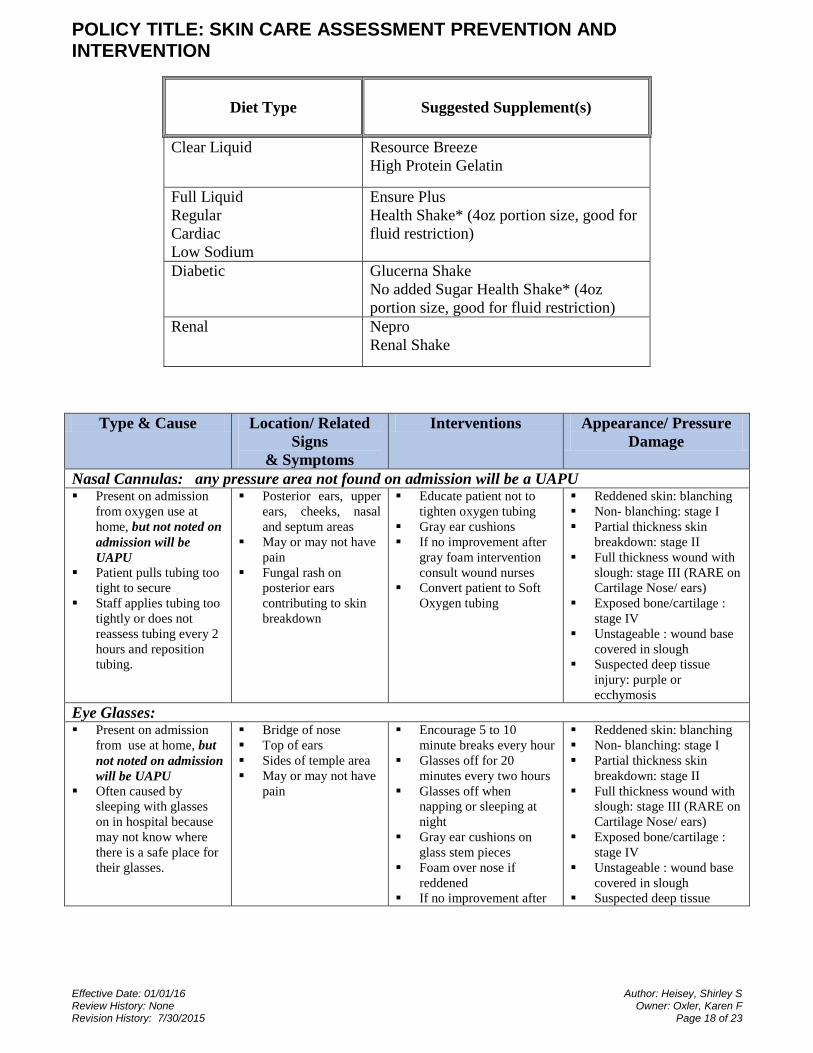
Appendix C: Nutrition
Appendix D: Device-Related Skin Protection Guide
Page 18
POLICY TITLE: SKIN CARE ASSESSMENT PREVENTION AND INTERVENTION
Effective Date: 01/01/16 Author: Heisey, Shirley S Review History: None Owner: Oxler, Karen F Revision History: 7/30/2015 Page 18 of 23
Type & Cause Location/ Related
Signs
& Symptoms
Interventions Appearance/ Pressure
Damage
Nasal Cannulas: any pressure area not found on admission will be a UAPU Present on admission
from oxygen use at
home, but not noted on
admission will be
UAPU
Patient pulls tubing too
tight to secure
Staff applies tubing too
tightly or does not
reassess tubing every 2
hours and reposition
tubing.
Posterior ears, upper
ears, cheeks, nasal
and septum areas
May or may not have
pain
Fungal rash on
posterior ears
contributing to skin
breakdown
Educate patient not to
tighten oxygen tubing
Gray ear cushions
If no improvement after
gray foam intervention
consult wound nurses
Convert patient to Soft
Oxygen tubing
Reddened skin: blanching
Non- blanching: stage I
Partial thickness skin
breakdown: stage II
Full thickness wound with
slough: stage III (RARE on
Cartilage Nose/ ears)
Exposed bone/cartilage :
stage IV
Unstageable : wound base
covered in slough
Suspected deep tissue
injury: purple or
ecchymosis
Eye Glasses: Present on admission
from use at home, but
not noted on admission
will be UAPU
Often caused by
sleeping with glasses
on in hospital because
may not know where
there is a safe place for
their glasses.
Bridge of nose
Top of ears
Sides of temple area
May or may not have
pain
Encourage 5 to 10
minute breaks every hour
Glasses off for 20
minutes every two hours
Glasses off when
napping or sleeping at
night
Gray ear cushions on
glass stem pieces
Foam over nose if
reddened
If no improvement after
Reddened skin: blanching
Non- blanching: stage I
Partial thickness skin
breakdown: stage II
Full thickness wound with
slough: stage III (RARE on
Cartilage Nose/ ears)
Exposed bone/cartilage :
stage IV
Unstageable : wound base
covered in slough
Suspected deep tissue
Diet Type
Suggested Supplement(s)
Clear Liquid Resource Breeze
High Protein Gelatin
Full Liquid
Regular
Cardiac
Low Sodium
Ensure Plus
Health Shake* (4oz portion size, good for
fluid restriction)
Diabetic Glucerna Shake
No added Sugar Health Shake* (4oz
portion size, good for fluid restriction)
Renal Nepro
Renal Shake
Page 19
POLICY TITLE: SKIN CARE ASSESSMENT PREVENTION AND INTERVENTION
Effective Date: 01/01/16 Author: Heisey, Shirley S Review History: None Owner: Oxler, Karen F Revision History: 7/30/2015 Page 19 of 23
Type & Cause Location/ Related
Signs
& Symptoms
Interventions Appearance/ Pressure
Damage
gray foam intervention
consult wound nurses
injury: purple or
ecchymosis color
C-Pap Masks/ Oxygen Masks, ET Tubes:
Present on admission
from use at home, but
not noted on admission
will be UAPU
Patient may be pulling
at mask to increase
friction damage
Be careful when patient
is on side that mask is
not being crushed by
bed or pillow.
Posterior ears, upper
ears, cheeks, nasal
and septum areas
May or may not have
pain
Sweating increases
risk of skin
breakdown because
of increase
maceration of skin
Foam over nose and
cheek areas
Recommend foam Trach
ties with Velcro
securement for ears with
noted injury or patient
pulling on mask
May need gray ear foam
cushions over elastic
support ties on some
types of masks
If no improvement after
interventions consult
wound nurses
Reddened skin: blanching
Non- blanching: stage I
Partial thickness skin
breakdown: stage II
Full thickness wound with
slough: stage III (RARE on
Cartilage Nose/ ears)
Exposed bone: stage IV
Unstageable : wound base
covered in slough
Suspected deep tissue
injury: purple or
ecchymosis color
Indeterminable: On
mucous Membranes
Fecal Management System, catheters, condom catheters:
Skin weakened from
chronic moisture and
enzymatic content of
fecal leakage on peri-
rectal skin is more
likely to develop skin
breakdown
Fecal management
tubing should be
repositioned with each
patient repositioning in
bed or prevent patient
from laying on tube
Please also refer to the
Fecal Management Rectal
Tube CPP.
Peri-rectal skin
Posterior thighs if
patient was laying on
tubing
Patient may develop
yeast rash from
increased moisture in
area
Skin barrier buttocks
paste at each
repositioning and PRN
for leakage events
Miconazole with barrier
for yeast rash BID for
redness, no improvement
in 24 hours consult
wound nurse
Reddened skin: blanching
Non- blanching: stage I
Partial thickness skin
breakdown: stage II
Full thickness wound with
slough: stage III
Exposed bone: stage IV
Unstageable : wound base
covered in slough
Suspected deep tissue
injury: purple or
ecchymosis color
Linens and Lines:
Page 20
POLICY TITLE: SKIN CARE ASSESSMENT PREVENTION AND INTERVENTION
Effective Date: 01/01/16 Author: Heisey, Shirley S Review History: None Owner: Oxler, Karen F Revision History: 7/30/2015 Page 20 of 23
Type & Cause Location/ Related
Signs
& Symptoms
Interventions Appearance/ Pressure
Damage
Extra linens under
patient increase warmth
of skin and risk of skin
breakdown
No bottom sheets are
needed for Low Air
loss ; negate therapy of
air flow bed.
Patient laying on
tubing: SCD tubing, IV
lines, call bells, heart
monitors, foley tubing,
NG tubing, bath
blankets, wrinkled
linens, lift pad will
create focal pressure
areas on the skin.
Anywhere under the
patient
Tubing taped too
tightly to skin
Assess carefully with
each repositioning of
patient that there are no
wrinkled, extra linens
under patient.
Assess carefully that
devices are properly
positioned.
Reddened skin: blanching
Non- blanching: stage I
Partial thickness skin
breakdown: stage II
Full thickness wound with
slough: stage III
Exposed bone: stage IV
Unstageable : wound base
covered in slough
Suspected deep tissue
injury: purple or
ecchymosis color
Casts, braces, ACE wraps, SCDs and TED stockings: When applying the cast
or brace over boney
prominences pressure
areas may develop.
Any surface that can
have pressure from
the brace, ace or cast.
May appear as red,
purple or a wound
when the device is
removed.
Unexplained pain
under the device
Patients with diabetic
neuropathy , spinal
injury or stroke may
not have any pain so
skin observation is
essential for skin
protection
If brace is secured with
Velcro assess under
brace every 4 hours and
prn with pain or swelling
TED stockings reassess
every 8 hours and prn
with pain or swelling
Reassess skin under
SCD’s with each
repositioning
Access skin every 4
hours under edges of ace
wrap and loosen ACE if
limb becomes swollen
Apply padding with
foam dressing at the time
of application to known
problem areas.
Reddened skin: blanching
Non- blanching: stage I
Partial thickness skin
breakdown: stage II
Full thickness wound with
slough: stage III (RARE on
Cartilage Nose/ ears)
Exposed bone: stage IV
Unstageable : wound base
covered in slough
Suspected deep tissue
injury: purple or
ecchymosis color
Indeterminable: Known
pressure ulcer unable to
assess under non-removal
brace/cast.
Nasal Gastric Tube: When placing NG tube
if able place as OG
while patient has ET
tube and secure to ET
tube
When placing on nose
please do not secure
that tube is tight to
inner nares
Reassess peri tube skin
every 2 hours and more
Inner or upper nares
where tube may be
resting
Assess for moisture in
area and patient may
need topical like
bacitracin ointment to
protect skin
Secure to ET tube when
unable with Hollister
device
Reposition NG tube
every 8 hours and PRN if
any redness
Utilize the Hollister NG
tube securement device
when able.
Reddened skin: blanching
Non- blanching: stage I
Partial thickness skin
breakdown: stage II
Full thickness wound with
slough: stage III (RARE on
Cartilage Nose/ ears)
Exposed bone: stage IV
Unstageable : wound base
covered in slough
Suspected deep tissue
injury: purple or
Page 21
POLICY TITLE: SKIN CARE ASSESSMENT PREVENTION AND INTERVENTION
Effective Date: 01/01/16 Author: Heisey, Shirley S Review History: None Owner: Oxler, Karen F Revision History: 7/30/2015 Page 21 of 23
Type & Cause Location/ Related
Signs
& Symptoms
Interventions Appearance/ Pressure
Damage
frequently if any
redness or excessive
moisture
Please also refer to the GI
Tube Management CPP.
ecchymosis color
Indeterminable: On
mucous Membranes
Appendix E: When to consult the Inpatient Wound- Ostomy Nurse
(After your Nursing Wound Care Assessment and Documentation)
CONSULT INPATIENT WOUND OSTOMY NURSE
Place Consult in Epic “Wound Ostomy Inpatient Nurse Consult”
All Hospital Acquired Pressure Ulcers (ALL Pressure Ulcer with Event reports placed)
All patients with an Ostomy
All Wound V.A.C.S. or other NPWT Device
Any patients on/Ordered a Low Air Loss Bed
All Pressure Ulcers Stages III and IV, suspected Deep Tissue Injuries, Unstageable
Questionable or Advancing Pressure Ulcers
CONSULT CLINICAL NURSE EDUCATORS FOR SUPPORT
(Does not require a consult to the inpatient Wound Nurses)
Questions on Initiating Nursing Interventions from Skin Care Protocol
o Yeast
o Present on Admission / Healing Pressure Ulcers Stages I and II
Patients with wound care orders and Current Physician Management
How to apply ostomy wafer
Stand by assistance for VAC dressing changes if need support
Appendix F: Molnlycke Product Guide
Page 22
POLICY TITLE: SKIN CARE ASSESSMENT PREVENTION AND INTERVENTION
Effective Date: 01/01/16 Author: Heisey, Shirley S Review History: None Owner: Oxler, Karen F Revision History: 7/30/2015 Page 22 of 23
Page 23
POLICY TITLE: SKIN CARE ASSESSMENT PREVENTION AND INTERVENTION
Effective Date: 01/01/16 Author: Heisey, Shirley S Review History: None Owner: Oxler, Karen F Revision History: 7/30/2015 Page 23 of 23