Folia Psychiatrica et Neurologica Japonica, Vol. 25, No. 1, 1971 “Sleep Apnoea” and Sleep Regulating Mechanism -A case effectively treated with monochlorimipramine- Hisashi KUMASHIRO, M.D. Department of Neuro-Psychiatry, Fukushima Medical College, Fukushima Mitsumoto SATO, M.D., Junichiro HIRATA, M.D., Osamu BABA, M.D. and Saburo OTSUKI, M.D. Department of Neuro-Psychiatry, Okayama University Medical School, Okayama INTRODUCTION Of hypersomnia with periodic apnoea Lugaresi et al.I5) consider the mechanism of the periodic apnoea that sets in when the patient becomes drowsy as a central type and state hypothetically that the periodic apnoea (sleep apnoea) of this central type is the ex- pression of a primitive depression of the re- ticular activating system. Namely, hyper- somnia with sleep apnoea may in fact be explained by hypoexcitability of the reticu- lar activating system. We have investigated a case of sleep apnoea caused by tabes dor- salis and cerebral arteriosclersois, and have found that this sleep apnoea is closely asso- ciated with disturbance of the sleep regulat- ing mechanism. Hence we consider that even in this case hypoexcitability of the re ticular activating system is responsible. On such an assumption we administered to the patient methyl phenidatesJJ2) ( a stimulant of the reticular activating system) and im- pramine, monochlorimipramine which is an- tidepressant as well as effective drug to narcolepsy, and obtained markedly satis- factory results. This paper describes the results of our study as well as gives our view regarding the relationship between sleep apnoea and sleep regulating mecha- nism. ~~ Received for publication Apr. 6, 1971. REPORT OF THE CASE The case Y.D. is a 69-year old male who had no remarkable familial history to be mentioned. At the age of 3 years the pa- tient suffered tabes dorsalis for which he received antisyphilitic therapy including fever treatment, and pain in the legs dis- appeared but ataxic gait remained. Sub- sequently at the age of 54 years (1953) he began to have periodic aponea (respiratory arrest) in his sleep at night when he was tired or had taken alcoholic drinks. Then this periodic apnoea during sleep was divid- ed into “apnoea-tonic convulsion” type and “respiration arrest” type by the degree of apnoea. In other words, the former type appears with a gradual shallow breathing which progresses to a complete apnoea in his sleep, accompanied by cyanosis of the entire body. Then his breathing becomes only inhalation which is accompanied by vocalization of hissing sounds repeated 1 to 3 times which then turns to general tonic convulsion. His family member will then compress his chest to give artificial respira- tion, and he recovers his respiration and con- sciousness starting with exhalation and mic- turition. The seizure after this vocalization lasts 10 to 60 seconds. The latter, “re- spiration arrest” type, is moderate one in which the respiration arrest and cyanosis last for about one minute, and the respira-
Transcript
Folia Psychiatrica et Neurologica Japonica, Vol. 25, No. 1, 1971
“Sleep Apnoea” and Sleep Regulating Mechanism -A case effectively treated with monochlorimipramine-
Hisashi KUMASHIRO, M.D. Department of Neuro-Psychiatry, Fukushima Medical College, Fukushima
Department of Neuro-Psychiatry, Okayama University Medical School, Okayama
INTRODUCTION Of hypersomnia with periodic apnoea
Lugaresi et al.I5) consider the mechanism of the periodic apnoea that sets in when the patient becomes drowsy as a central type and state hypothetically that the periodic apnoea (sleep apnoea) of this central type is the ex- pression of a primitive depression of the re- ticular activating system. Namely, hyper- somnia with sleep apnoea may in fact be explained by hypoexcitability of the reticu- lar activating system. We have investigated a case of sleep apnoea caused by tabes dor- salis and cerebral arteriosclersois, and have found that this sleep apnoea is closely asso- ciated with disturbance of the sleep regulat- ing mechanism. Hence we consider that even in this case hypoexcitability of the r e ticular activating system is responsible. On such an assumption we administered to the patient methyl phenidatesJJ2) (a stimulant of the reticular activating system) and im- pramine, monochlorimipramine which is an- tidepressant as well as effective drug to narcolepsy, and obtained markedly satis- factory results. This paper describes the results of our study as well as gives our view regarding the relationship between sleep apnoea and sleep regulating mecha- nism. ~~
Received for publication Apr. 6, 1971.
REPORT OF THE CASE The case Y.D. is a 69-year old male who
had no remarkable familial history to be mentioned. At the age of 3 years the pa- tient suffered tabes dorsalis for which he received antisyphilitic therapy including fever treatment, and pain in the legs dis- appeared but ataxic gait remained. Sub- sequently at the age of 54 years (1953) he began to have periodic aponea (respiratory arrest) in his sleep at night when he was tired or had taken alcoholic drinks. Then this periodic apnoea during sleep was divid- ed into “apnoea-tonic convulsion” type and “respiration arrest” type by the degree of apnoea. In other words, the former type appears with a gradual shallow breathing which progresses to a complete apnoea in his sleep, accompanied by cyanosis of the entire body. Then his breathing becomes only inhalation which is accompanied by vocalization of hissing sounds repeated 1 to 3 times which then turns to general tonic convulsion. His family member will then compress his chest to give artificial respira- tion, and he recovers his respiration and con- sciousness starting with exhalation and mic- turition. The seizure after this vocalization lasts 10 to 60 seconds. The latter, “re- spiration arrest” type, is moderate one in which the respiration arrest and cyanosis last for about one minute, and the respira-
42 H. Kumashiro, M. Sato, J. Hirata, 0. Baba and S. Otsuki
Meelofenoxate hydrochloride -
Me*y’ ’henidate 20mgNethyl Phenidate IOmg. - = I Imipramine 50mg.
Amitriptyline 50m~.
Mono C hl ori mi prami ne 5 h g . tracheostomg - -1
Unconsci =-,, uusness , , Apnoeat,oni convulsion c diacliarqe -
respiration arres t
1969 1970 - _ _ _ Aug. Sep. Oct. Nou. Dec. Jan.
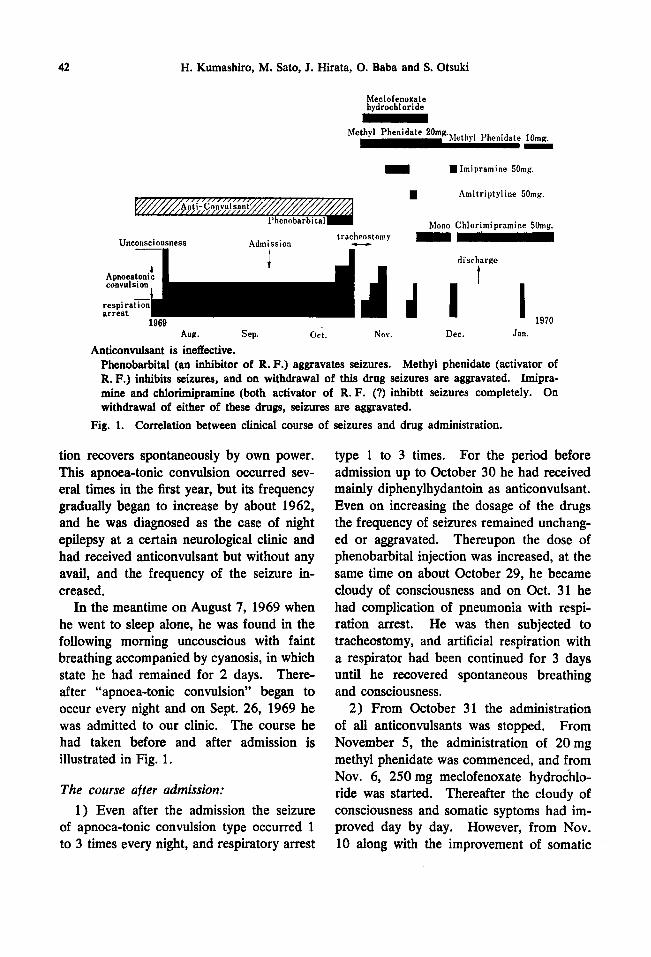
Anticonvulsant is ineffective. Phenobarbital (an inhibitor of R. F.) aggravates seizures. Methyl phenidate (activator of R. F.) inhibits seizures, and on withdrawal of this drug seizures are aggravated. Imipra- mine and chlorimipramine (both activator of R. F. (?) inhibtt seizures completely. On withdrawal of either of these drugs, seizures are aggravated.
Fig. 1. Correlation between clinical course of seizures and drug administration.
tion recovers spontaneously by own power. This apnoea-tonic convulsion occurred sev- eral times in the first year, but its frequency gradually began to increase by about 1962, and he was diagnosed as the case of night epilepsy at a certain neurological clinic and had received anticonvulsant but without any avail, and the frequency of the seizure in- creased.
In the meantime on August 7, 1969 when he went to sleep alone, he was found in the following morning uncouscious with faint breathing accompanied by cyanosis, in which state he had remained for 2 days. There- after “apnoea-tonic convulsion” began to occur every night and on Sept. 26, 1969 he was admitted to our clinic. The course he had taken before and after admission is illustrated in Fig. 1 .
The course after admission: 1) Even after the admission the seizure
of apnoea-tonic convulsion type occurred 1 to 3 times every night, and respiratory arrest
type 1 to 3 times. For the period before admission up to October 30 he had received mainly diphenylhydantoin as anticonvulsant. Even on increasing the dosage of the drugs the frequency of seizures remained unchang- ed or aggravated. Thereupon the dose of phenobarbital injection was increased, at the same time on about October 29, he became cloudy of consciousness and on Oct. 31 he had complication of pneumonia with respi- ration arrest. He was then subjected to tracheostomy, and artificial respiration with a respirator had been continued for 3 days until he recovered spontaneous breathing and consciousness.
2) From October 31 the administration of all anticonvulsants was stopped. From November 5, the administration of 20 mg methyl phenidate was commenced, and from Nov. 6, 250 mg meclofenoxate hydrochlo- ride was started. Thereafter the cloudy of consciousness and somatic syptoms had im- proved day by day. However, from Nov. 10 along with the improvement of somatic
“Sleep Apnoea” and Sleep Regulating Mechanism 43
conditions respiration arrest and apnoea- tonic convulsion again began to appear every night.
3 ) From Nov. 16, the day when this sleep apnoea had appeared frequently, 50 mg imi- prarnine was administered before going to sleep. As a result the sleep apnoea that had occurred so frequently never appeared for 9 subsequent days. However, as there oc- curred respiration arrest several times on the tenth day, the drug was changed to amit- riptyline (50 mg) but to no avail. From Nov. 28 the drug was switched to mono- chlorimipramine (50 mg) . Thereafter the seizure of sleep apnoea was almost com- pletely inhibited. During this time we tried again imipramine on December 13, but as apnoea-tonic convulsion occurred more than twice every day, the drug was again shifted back to monochlorimipramine. As a result all seizures had completely disappeared. Therefore, on Dec. 27 the patient was dis- charged from the clinic, who left us in high spirit on his own feet. As we had noticed no seizure in the beginning of December when we reduced dose of methyl phenidate from 20 mg to 10 mg, we stopped giving methyl phenidate for a time being after the discharge from the clinic (Jan., 1970), but seeing recurrence of apnoea-tonic convul- sion, we have again instituted this drug.
4) As described in the foregoing, we are continuing the oral administration of 10 mg methyl phenidate after breakfast and 50 mg monochlorimipramine before going to bed, and we find all the seizures to have been suppressed for about 15 months up to date. Only when the patient breaks the rule and takes alcoholic drinks or when he is over- tired from work, seizures appear several times. Otherwise he enjoys family life, goes out occasionally, and assumes his post of a company president apparently in good health, taking a nap every day at noon time.
CLINICAL EXAMINATION RESULTS Peripheral blood picture and urinary find-
ings are normal. The test results are serum synphilitic test (+) ; serum total protein, 7.6 mg/dl; as to the protein fraction tests: albumin 54; TGlobulin 46; a1-G, 3; ae-G, 9; P-G, 10.5; yl-G, 23.5(%); and A/G ratio, 1.17. Serochemical tests gave 104 pg/ dl Fe, 115 pg/dl Cu, 143.5 mgEq./l Na, 3.0 mEq./l K, 10.6 mg/d serum-urea-N, 204 mg/dl cholesterol, 2.7 B.L.U. Alkali- Pase, 15 units of GOT, 17 units of GPT, 3 units of TTT, 10 units of ZTT, and CCLF (+ 4- ) . The spinal tap gives: normal pres- sure, xanthochromia ( f ) , Nonne (+ ) , Pandy ( + +), Queckensteadt normal, cell count, 12/3, glucose 50 mg/dl, 444.1 mg/dl C1, 112 mg/dl protein content, and the pro- tein fractions prove to be: 4.5 prealbumin, 49.1 albumin, 3.6 aL, 4.0 al 12.0 FQ, 12.0 Tr, 4.4 b, 24.4 r ( % ), CSF syphilitic test (+), as for the findings of fundus of eye: S,,-,,, degree of arteriosclerosis, and angiography gave arteriosclerotic signs such as stenosis and tortuous cerebral blood ves- sels. Craniogram gave normal picture, ECG showed a slight enlargement of the right ventricle, and the vital capacity to be 3,400~~. In addition, WAIS test before discharge proved to be IQ 93.
EEG Findings: A) EEG before the administration of mono-
(1 ) Four days after admission when the patient had frequent sleep apnoea.
As can be seen in Fig. 2 (Sept. 29), EEG in the daytime when the patient was at rest and awake, showed only slow alpha waves of 8 c/s 30-7Opv mixed with some sporadic 6 waves, but there could be observed not any paroxysm nor focal sign even in at- tempts at various activation.
(2) The all night sleep polygraph (EEG
chlorimipramine:
44 H. Kumashiro, M. Sato, J. Hirata, 0. Baba and S. Otsuki
RFp-RE
- 1 . D . 6 9 r . I . st,.mm, )rr- .-
There can be observed 8c/s slow alpha waves mixed with slight sporadic 0 waves. Fig. 2. EEG before the administration of monoclorimipramine on Sept. 29, 1%9 during
the daytime when the patient was at rest and awake with frequent seizures of sleep apnoea.
L Fp-RFp
LO-R6
RFp-RO
LFp-LO
ECG
Respiration
Eyemovement -1 f h K * r
suu ( cnml*~~* l* ) 1. D. yh. II, ko *LV im 1.m 4.n.
There can be observed not any deep sleep pattern or activating sleep pattern, but the stage of suppressed waves can be seen.
Fig. 3. EEG (all night sleep polygraph) before administration of monochlorimipramine on Oct. 11, 1%9 when the patient was thought to be in deep sleep with frequent seizures of sleep apnoea.
(note abnormal sleep pattern)
"Sleep Apnoea" and Sleep Regulating Mechanism 45
O. D. m .. I(. br. is. iw 2.m 1.11.) VlUylUllO '4 . ) r u t &U bKu
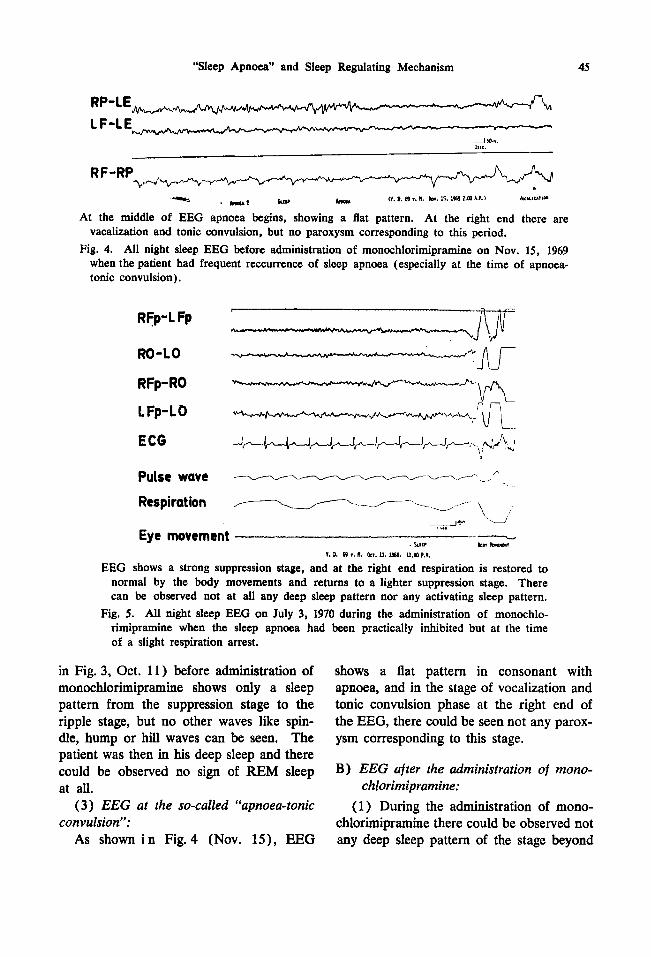
At the middle of EEG apnoea begins, showing a flat pattern. At the right end there are vacalization and tonic convulsion, but no paroxysm corresponding to this period.
Fig. 4. All night sleep EEG before administration of monochlorimipramine on Nov. 15, 1969 when the patient had frequent reccurrence of sleep apnoea (especially at the time of apnoea- tonic convulsion).
t
RFp-L Fp
---------.-------"w Ro-LO
RFp-RO
L Fp-LO
ECG Jf--JvJ-J++J44#4Y . ,j""" ' 6 4
Pulse wave :.---.A/
Respiration
Eye movement
-L---- -. u ,-- \ 19.. \J I ,.I - . suu ba? Ib*lur
.I- D. (0 I, R. on. u. iw. u.m P.M.
EEG shows a strong suppression stage, and at the right end respiration is restored to normal by the body movements and returns to a lighter suppression stage. There can be observed not at all any deep sleep pattern nor any activating sleep pattern.
Fig. 5. All night sleep EEG on July 3, 1970 during the administration of monochlo- rimipramine when the sleep apnoea had been practically inhibited but at the time of a slight respiration arrest.
in Fig. 3, Oct. 11) before administration of monochlorimipramine shows only a sleep pattern from the suppression stage to the ripple stage, but no other waves like spin- dle, hump or hill waves can be seen. The patient was then in his deep sleep and there could be observed no sign of REM sleep at all.
( 3 ) EEG at the so-called "apnoea-tonic convulsion":
As shown i n Fig.4 (Nov. 15), EEG
shows a flat pattern in consonant with apnoea, and in the stage of vocalization and tonic convulsion phase at the right end of the EEG, there could be seen not any parox- ysm corresponding to this stage.
B) EEG after the administration of mono-
(1) During the administration of mono- chlorimipramine there could be observed not any deep sleep pattern of the stage beyond
chlorimipramine:
46 H. Kumashiro, M. Sato, J. Hirata, 0. Baba and S. Otsuki
that of suppression stage. In the course of observations, at the stage when the patient was thought to be in his deepest sleep, there was slight respiration arrest, but his EEG at this instance (on July 3) as shown in Fig. 5 , shows only the advanced stage of suppression, so that the respiration was re- stored immediately by the body movements, which reverted back to more moderate sup- pression stage, and this process had occur- red repeatedly. When compared to the state prior to the monochlorimipramine ad- ministration, the sleep during the entire night appeared to be somewhat lighter with more frequent body movements after its ad- ministration.
DISCUSSION First of all we observed positive results
to such tests as of Westphal syndrome, Romberg sign, serum and cerebrospinal fluid syphilitic tests, and a decline in the ligiht reflex of the pupil and a decrease in the vibration sense of the lower limbs. From these findings this case seems to correspond to ataxia in stage I1 of tabes dorsalis by the classification of Leyden’). And as one of the visceral crisis respiration crisis seems to be closely associated with sleep apnoea of this case. In addition, the involvement of cerebral ateriosclerosis cannot be denied. As to differential diagnosis we can think of epileptic origin and that of Pickwickian syndrome. As for the epileptic one respira- tory arrest (Jackson*)) is pointed out as one of uncinate fit, and apnoea that appears be- fore the commencement of generalized sei- zure, at the time of centrencephalic serizure discharge, and the seizure discharge cor- related to the absence (UmbashlD), John- sonf”, MirskylBJ7)). However, all of them have observed periodic spike discharges in EEG. In the present case inspite of various attempts at activation since paroxysm could never be observed in his EEG and flat EEG
was observable at the onset of apnoea-tonic convulsion, and further various anticonvul- sants proved to be of no avail, epileptic origin was ruled out. As to Pickwichian s y n d r ~ m e ~ ~ J ~ s ~ ~ ) , according to the report first presented by Burwell et a12), the essential symptome of this syndrome are obesity, hypersomnia, and periodic apnea, and as the symptoms secondary to them are fibrillation of the muscles, cyanosis, secondary erythro- cytemia, right ventricular hypertrophy, and right ventricular insufficiency.
In our case, since we can only recognize periodic apnea and cyanosis, and the other symptoms are lacking, we cannot classify them to Pickwickian syndrome. However, as Kuhlol*) allocates 5 cases with hyper- somnia as the principal symptome accom- panied by periodic apnea and cyanosis to Pickwickian syndrome, it may be said that our case is closely related to this syndrome. Now that discussion is being carried out on the problem whether the onset mechanism of apnea is of the peripheral or the central nature3J4), it would be significant to con- sider these cases with focus on the onset mechanism of apnea. In view of this, the present discussion has been conducted cen- tering around the onset mechanism of apnea. First looking at the case from the aspect of EEG, his sleep EEG clearly shows abnormal sleep pattern. Namely, even at the stage thought to be in his deepest sleep, electro- encephalographically there appears the stage of suppressed waves or the stage of ripple waves, but no pattern suggestive of still deeper sleep. Of course, no E M sleep pattern can be recognized but EEG shows abnormal sleep pattern. Following the idea of KanekolO) et al.12), this seems to be due to the abnormality of sleep regulating mech- anism induced by the functional decline of the reticular formation (R.F.) , It is known that as the sleep becomes deeper and falls into activated sleep, the involvement of
“Sleep Apnoea” and Sleep Regulating Mechanism 47
medulla oblongata in the respiratory func- tion is increased, and even in normal person there can occur respiration arrest or change in Cheyne-Stokes pattern after exhalation at the stage of REM sleep1s). From the fact that apnoea-tonic convulsion of this case ap- pears only when the depth of sleep has ex- ceeded a certain fixed limit, sleep apnoea of this sort can be said to be periodic apnoea of central type similar to the concept of Lugaresi15), and it is possible to consider of hypoexcitability of reticular activating sys- tem of the medulla oblongata and the brain stem. It seems that in this manner respira- tory arrest appears first after exhalation, and the brain stem is activated compensatorily as the oxygen concentration in the circulat- ing blood of the brain decreases, resulting in anoxic convulsion4), which finally leads to the restoration of respiration.
What has so far been described may be supported by the following points: Namely, sleep apnoea of the present case is markedly aggravated by phenobarbital1*) which is known to inhibit selectively the brain stem reticular activating system (R. F.), while on the contrary, it is improved by methyl pheni- date6JJ2) which is known to activate R.F., and it has been demonstrated by the clinico- pharmacological effects that the aggraviation of sleep apnoea occurs due to such an in- terruption.
Now, turning to the marked effects of imipramine and monochlorimipramine on sleep apnoea, at first we may look at nar- colepsy which resembles the present case. It is reported that in this instance atonia and sleep paralysis occur also in association with the depth of sleep, especially with the activated sleep stage, and to these symptoms imipraminesJ2) is effective, and such an im- provement is thought12) to be due to the in- hibotory effect of imipramine on activated sleep. The fact that atonia and paralysis that occur in the sleep of narcolepsy and
that sleep apnoea in the present case in study suggests both cases to have a common disturbance of sleep regulating mechanism. Namely, symptoms in either case appear at a certain sleep level, and methyl phenidate, an R.F. stimulant, is effective, on the con- trary, phenobarbital, R.F. inhibitor, is ag- gravative, and also imipramine is markedly effective. But imipramine is said to have hardly any effect on sleep itself in narco- lepsy, and also in our case all night sleep polygraph (sleep EEG) shows no appre- ciable changes in sleep pattern before and after the administration of this drug.
Now there arises a question what is speci- fic action mechanism of imipramine, mono- chlorimpramine. EEG findings suggest that imipramine and monochlorimipramine act inhibitorily at a certain sleep level when the patient begins to enter sleep paralysis or sleep apnoea. On observations of sleeping conditions of our case at the time when sleep apnoea is inhibited by monochlorimipra- mine, we find that the patient makes a good deal of body movements, turning body dur- ing sleep, and has somewhat insacient sleep so he takes a nap on the following day to compensate it. In other words, chlor- imipromine seems to have maintained a cer-
~ H ~ - - c H ~ - - c H ~ - N * HC1
Imipramine
CH-CH~-CH~-S< - HCI C H3
Monochlorirnipramine (Anafranil) Fig. 6. Chemical formula.
48 H. Kumashiro, M. Sato, J. Hirata, 0. Baba and S. Otsuki
tain shallow sleep by the body turning. Finally as to the difference in the action
mechanism between imipramine and mono- chlorimipramine, both have very similar chemical structure as shown in Fig. 6, and according to Kimura et aL5J1) these two drugs have no fundamental difference in their pharmacological effect, but monochlor- imipramine a slightly weaker effect yet more rapid action, and is useful in the patient who has become tolerant to imipramine. With our case likewise monochlorimipramine shows a marked effect when the patient has become tolerant to imipramine, and for 15 months since there can be seen no tolerancy and a steady effect on sleep apnoea is being maintained.
ABSTRACT The patient was a 69-year old male, with
apnoea-tonic convulsion in sleep as the chief complaint. Over the period of 17 years prior to his admission to our clinic he had been treated as a case of night epilepsy, without improvement but aggravation. Satis- factory results of our treatment are briefly summarized as follows.
1 ) Anticonvulsants including diphenyl- hydantoin proved ineffective, and phenobar- bital aggravated seizures markedly.
2) Methyl phenidate and imipramine or monochlorimipramine proved to be effective, and the last drug was completely suppressed the sleep apnoea. During 15 months after discharge the continuous use of this drug has effectively inhibited the seizures up to date.
3 ) EEG of our case shows abnormal sleep pattern which has no deep sleep pat- tern. And no remarkable EEG changes were observed before and after administra- tion of monochlorimipramine, but body movements during sleep were more frequent after the administration.
4) By recording EEG at the onset of th is seizure there was recognized flat EEG sug-
gesting that the tonic convulsion occurring after apnoea is an anoxic convulsion.
5) As for the action mechanism of mono- chlorimipramine, on the basis of our find- ings that this sleep apnoea is closely asso- ciated with a certain depth of sleep, which resembles sleep paralysis of narcolepsy, and it has been concluded that the action mech- anism of imipramine and monochlorimipra- mine is directed to the disturbance of sleep regulating mechanism.
6) It is assumed that the mechanism of the present case consists of visceral crisis of tabes dorsalis, resultant hypoexcitability of the brain stem reticular activating system and disturbance of sleep regulating mecha- nism.
REFERENCES Arata, J.: Neurosyphilis, in Tsubaki, T. ed Clinical Neurology, Igakushoin, Tokyo, 455, 1966, (in Jap). Burwell, C. S., Robin, E. D., Whaley, R. D. and Bickelmann, A. G.: Extreme obesity as- sociated with alveolar hypoventilation, A Pickwickian syndrome, Amer J Med, 21:
Furuya, E., Wakamatsu, H., and Hishikawa, Y.: Pickwickian syndrome, Clin Neurol, 12: 670-675, 1970. Gastaut, H. and Fischer-Williams, M.: The physiopathology of epileptic seizures, in Handbook of Physiology, Neurophysiology, Vol 1, Amer Physiol Soc Washington, D.C., 1957. Honda, H. and Takahashi, Y.: Pharmaco- therapy of narcolepsy, Proceeding of 1st meeting of neuro-psychotropic drug therapy, 11 , 1969, (in Jap). Ikeda, T., Katsurada, K. and Ogawa, M.: A method of prognostic assessment of pa- tients with clouding of consciousness, clinical Electroencephalography, 11: 138, 1969, (in
Ikeda, T., Katsurada, K. and Yamada, R.: The prognostic assessment of patients with severe disturbance of consciousness (111, clinical Electroencephalography, 12: 144, 1970, (in Jap). Jackson, J. H.: On asphyxia in slight epilep- tic paroxysms, Lancet, 79-80, 1899.
811-818, 1956.
Jap).
“Sleep Apnoea” and Sleep Regulating Mechanism 49
Johnson, L. C. and Davidoff, R. A.: Auto- nomic changes during paroxysmal EEG acti- vity, Electroenceph clin Neurophysiol, 17:
Kaneko, Z. and Hishikawa, Y.: Electro- encephalographic study on narcolepsy-with special reference to paradoxical sleep-, Ad- vances in Neurological Sciences, 10 : 132- 140, 1966, (in Jap). Kimura, B.: Erfahrungen mit einem neuen Thimoleptikum Cloripramin (Anafranil) , Medical Consultation & New Remedies, 7: 377-385, 1970, (in Jap). Kirikae, T.: Therapy of hypersomnia and disturbance of sleep rhythm, Sag6 Rinsho, 17: 2491-2495, 1968, (in Jap). Koseki, E.: in Tokizane, T. ed. Japanese Handbook of Physiology, Vol V Physiology of Brain and Nerve, Igaku Shoin, Tokyo, 1967, (in Jap). Kuhlo, W.: Sleep attack with apone. In The Abnormalities of Sleep in Man, ed by Gastaut, H. et al, Aulo Gaggi Editore,
25-35, 1964.
Bologna, 205, 1968. Lugaresi, E., Coccagna, G., Ceroni, G. B., Mantovani, M. and Pazzaglia, P.: Hyper- somnia with periodic apnoea: Problems of classification, Electroenceph clin Neurophy- siol, 27: 99, 1969. Mirsky, A.F. and Van Buren, J.M.: On the nature of the “absence” in centrencepha- lic epilepsy, Electroenceph clin Neurophysiol,
Nelson, D. A. and Pay, C. D.: Respiratory arrest from seizure discharges in limbic sys- tem, Arch Neurol, 19: 199-207, 1968. Takaori, S. and Nakai, Y.: Pharmacology of hypnotics, S6gB Ripsho, 17: 2452-2457, 1968, (in Jap). Umbach, W.: Electrophysiologosche und Regulative Phaenomene bei Stereotaktischen Hirnoperationen, Springer Verlag, Berlin, 1966. Ward, W. A. and Kelsey, W. M.: The pick- wickian syndrome, J Pediatrics, 61: 745- 750, 1962.