46
Sleeve is Only the Beginning…”Plus” Options Peng (Charles) Zhang, MD PhD Professor and Vice Chair of Surgery Fudan University Pudong Medical Center

Sleeve is Only the Beginning…”Plus” Options
Peng (Charles) Zhang, MD PhD
Professor and Vice Chair of Surgery
Fudan University Pudong Medical Center

Disclosures
• None

Category of Bariatric Surgery
• Intake restriction: LAGB, LSG, Gastric balloon, etc.
• Malabsorption: BPD-DS, etc.
• Combinational: Gastric bypass, etc.

Classification of Bariatric Surgery Procedures
Gastric Volume ReductionWithout Intestinal
ManipulationCombinational
Intestinal Length ReductionWithout
Gastric Manipulation
LAGB RYGBJejunocolic
Bypass
SleeveGastrectomy
BPD-DSJejunoileal
Bypass
GastricPlication
Mini-GastricBypass
DuodenojejunalBypass
GastricBalloon
SingleAnastomosis DS
And so on … …

Current Viable Procedure all Involve Gastric Volume Reduction
Gastric Volume ReductionWithout Intestinal
ManipulationCombinational
Intestinal Length ReductionWithout
Gastric Manipulation
LAGB RYGBJejunocolic
Bypass
SleeveGastrectomy
BPD-DSJejunoileal
Bypass
GastricPlication
Mini-GastricBypass
DuodenojejunalBypass
GastricBalloon
SingleAnastomosis DS
And so on … …

Combinational Procedures should Represent the Future
Gastric Volume ReductionWithout Intestinal
ManipulationCombinational
Intestinal Length ReductionWithout
Gastric Manipulation
LAGB RYGBJejunocolic
Bypass
SleeveGastrectomy
BPD-DSJejunoileal
Bypass
GastricPlication
Mini-GastricBypass
DuodenojejunalBypass
GastricBalloon
SingleAnastomosis DS
And so on … …

Why RYGB is the “Gold Standard”?
LAGB LSG RYGB BPD-DS
Excessive
Weight
Loss
47% 68% 62% 70%
Buchwald et al. JAMA. 2004;292:17241737
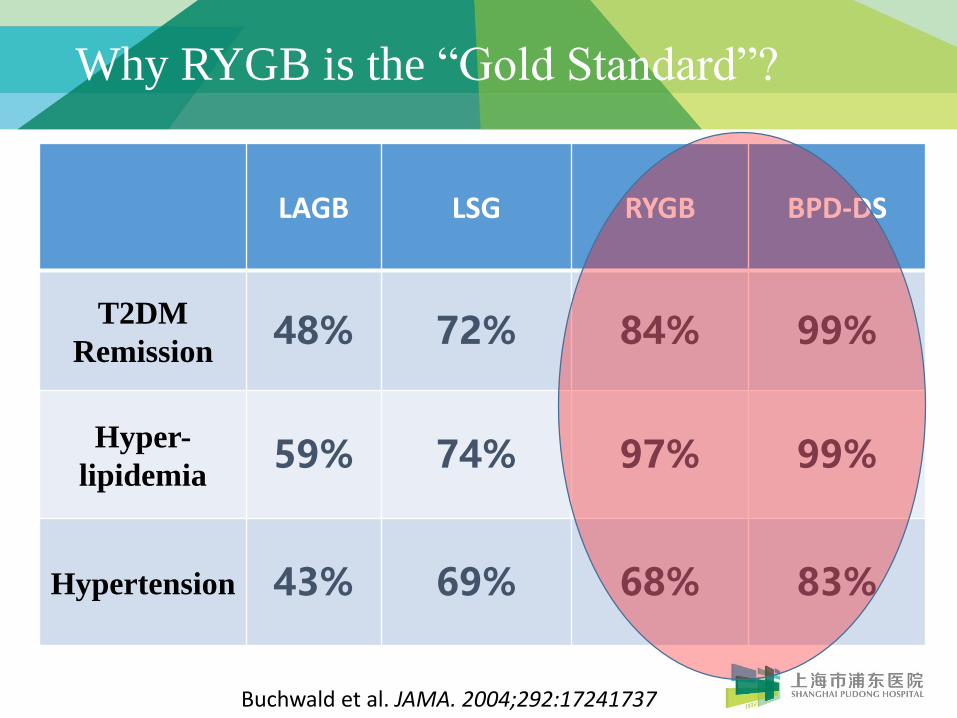
Why RYGB is the “Gold Standard”?
LAGB LSG RYGB BPD-DS
T2DM
Remission48% 72% 84% 99%
Hyper-
lipidemia59% 74% 97% 99%
Hypertension 43% 69% 68% 83%
Buchwald et al. JAMA. 2004;292:17241737
What’s “Wrong” with Gastric Bypass?
• No pylorus: dumping syndrome
• Gastro-Jejunal anastomosis: marginal ulceration
• Two transections on GI tract: internal hernia
• Gastric remnant: carcinoma

Why we concern about RYGB?
Rank CountryAge-Standardized Rate
per 100,000 (World)
1 Korea, Republic of 41.8
2 Mongolia 32.5
3 Japan 29.9
4 Guatemala 23.7
5 China 22.7
6 Tajikistan 21.7
7 Kazakhstan 21.6
8 Kyrgyzstan 21.4
9 Albania 20.1
10 Belarus 18.8
11 Turkmenistan 18.2
12 Costa Rica 17.3
13 Bhutan 17.2
14 Honduras 17.0
15 Ecuador 16.9
16 FYR Macedonia 16.5
17 El Salvador 16.4
18 Viet Nam 16.3
19 Russian Federation 16.0
20 Peru 15.8
Top 20 countries with the
highest gastric cancer
prevalence
World Cancer Research
Fund International

Why we concern about RYGB?
Smoking Prevalence in Adults
Graph adopted from World Bank
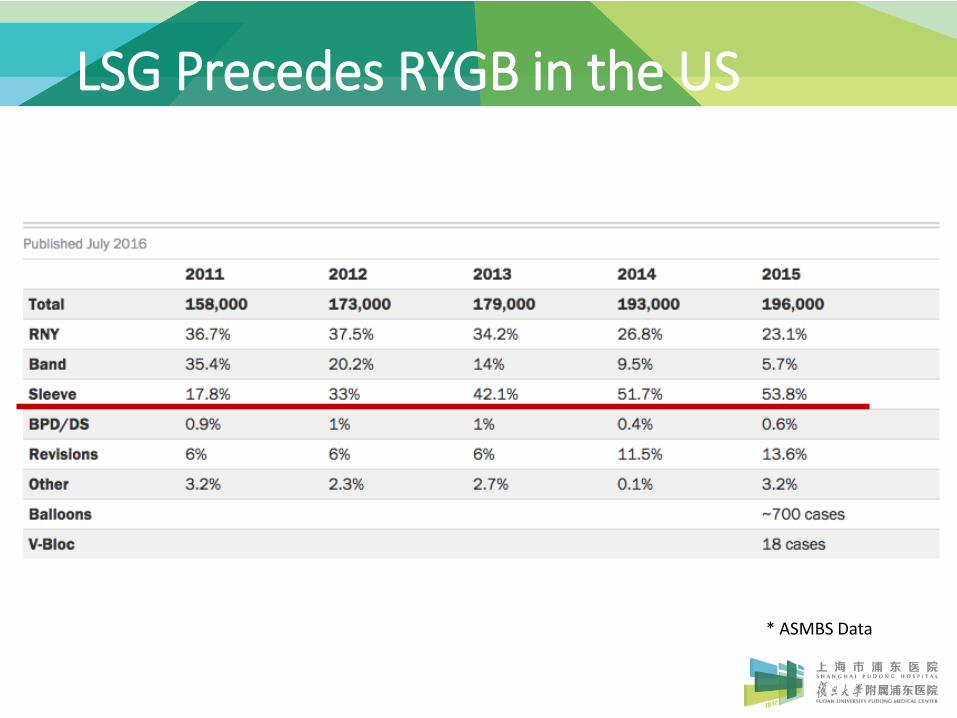
LSG Precedes RYGB in the US
* ASMBS Data

LSG Precedes RYGB Globally
Angrisani L, et al. Obesity Surgery, 2017

What’s “Good” with Sleeve Gastrectomy?
• Pylorus preservation: prevent dumping syndrome
• No GI rerouting: reduce marginal ulceration
• No transection on GI tract: prevent internal hernia
• No Gastric remnant: no worry about remnantcarcinoma
• How about GERD?
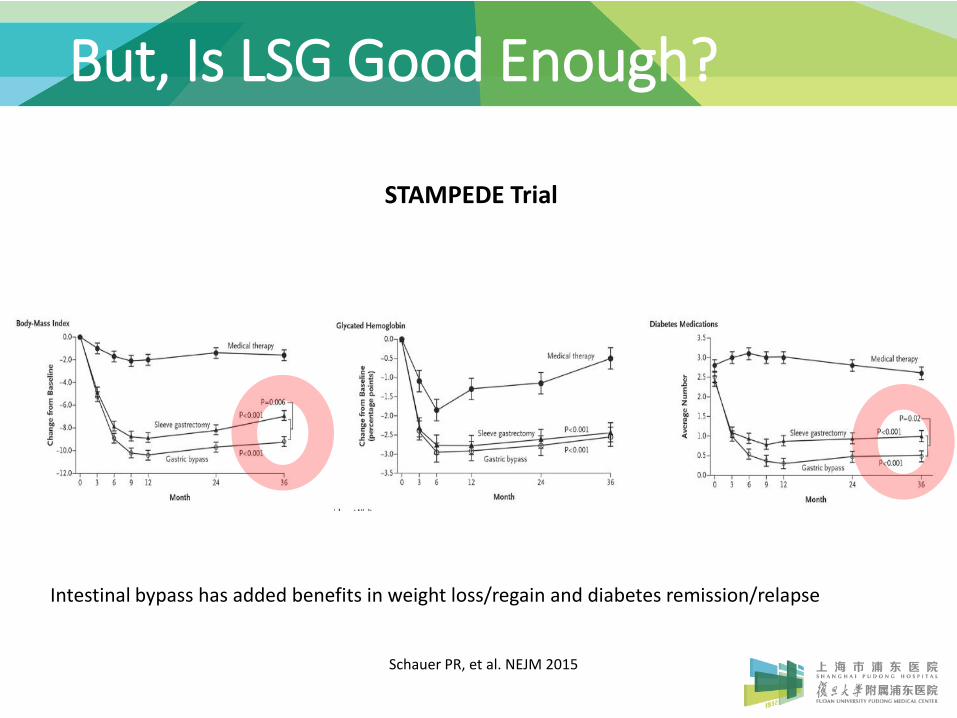
Schauer PR, et al. NEJM 2015
STAMPEDE Trial
But, Is LSG Good Enough?
Intestinal bypass has added benefits in weight loss/regain and diabetes remission/relapse
Organ Metabolic Regulation Function
Stomach ?
Duodenum ?
Jejunum ?
Ileum ?
Re-defining Gastrointestinal Function

The Role of Gastric Volume Reduction
With Gastric Volume Reduction W/O Gastric Volume Reduction
With Intestinal Length Reduction
Roux-en-YGastric Bypass
Duodenal-JejunalBypass
Without Intestinal Length Reduction
SleeveGastrectomy
Non-surgicalWeight Loss

FIBCMUMBAI
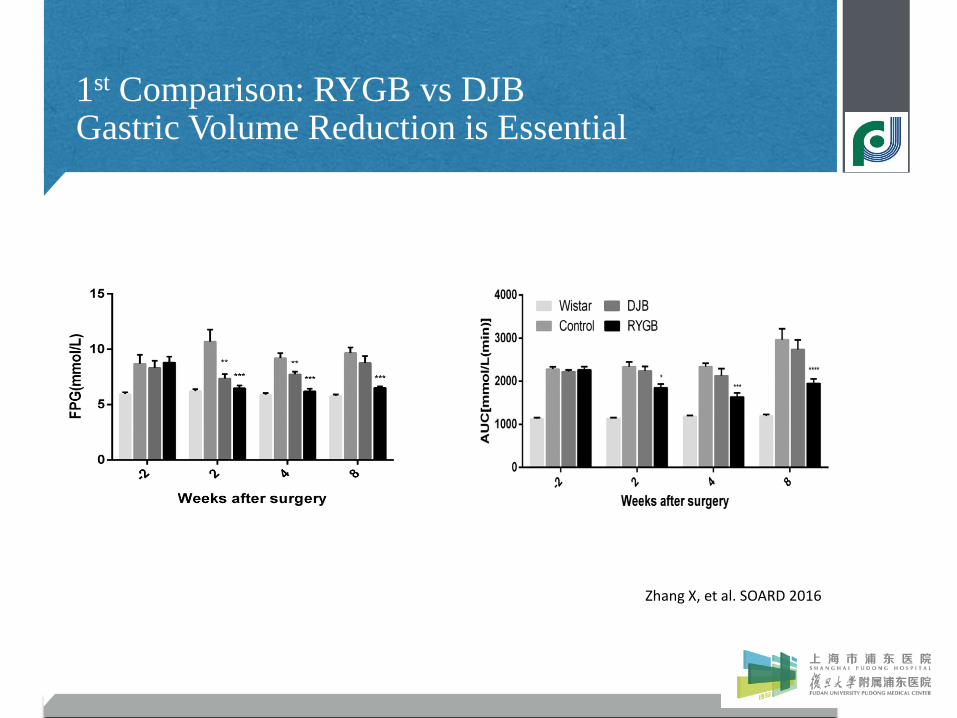
1st Comparison: RYGB vs DJBGastric Volume Reduction is Essential
FIBCMUMBAI
1st Comparison: RYGB vs DJBGastric Volume Reduction is Essential
Zhang X, et al. SOARD 2016

FIBCMUMBAI
2nd Comparison (STAMPEDE Trial):Gastric Volume Reduction Beats Intensive Medical Treatment
1. Sleeve gastrectomy gains significant better outcome than intensive medical treatment
2. By adding intestinal manipulation, there may be additional benefits
Schauer PR, et al. NEJM, 2015
FIBCMUMBAI
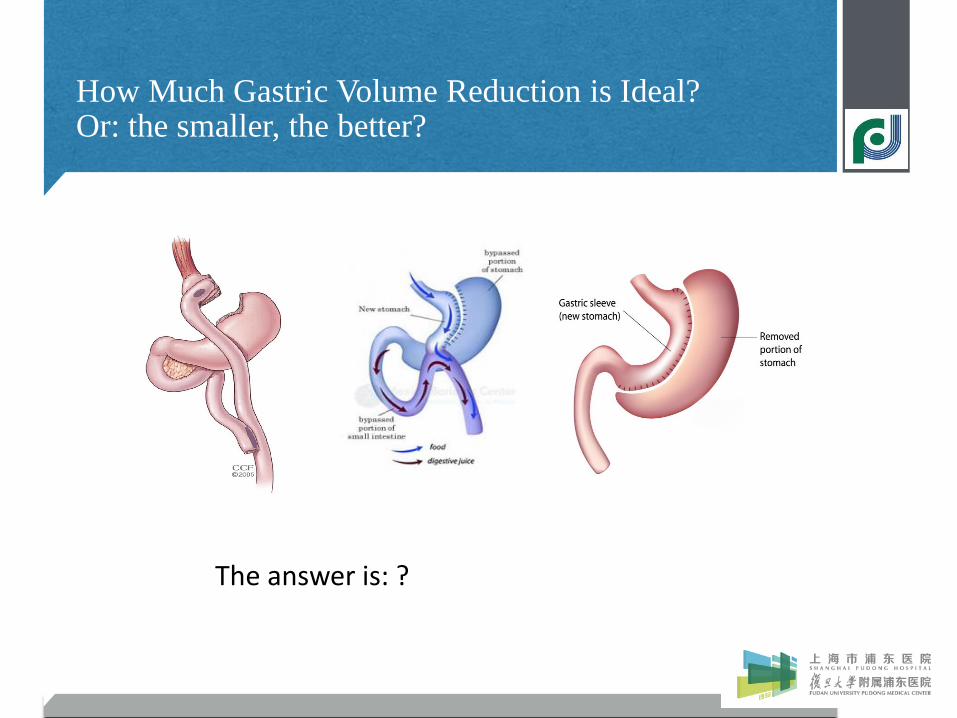
How Much Gastric Volume Reduction is Ideal?Or: the smaller, the better?
The answer is: ?

FIBCMUMBAI
Smaller bougie size does not always translate into a better outcome in LSG
Yuval JB, et al. Obes Surg (2013) 23:1685–1691

FIBCMUMBAI
Size of pyloric antrum does not lead todifference in weight loss
2.5 cm vs 6 cm:No difference in wt loss at 1 yr
Michalsky D, et al. Obes Surg, 2013, 23: 567-573

FIBCMUMBAI
Gastric sleeve volume increases has no correlation with BMI Regain
Ferrer-Marquez M, et al. Obes Surg DOI 10.1007/s11695-016-2274-1

FIBCMUMBAI
Gastric hormone (ghrelin) may be the driverfor weight and metabolic outcome

FIBCMUMBAI
Physiological functions mediated by ghrelin

FIBCMUMBAI
Where is the “Sweet Spot” on the stomach?
Hormones
Gastric Empty
1. Remove Gastric Fundus: As long Ghrelin secretion is decreased “enough”
2. Preserve Pylorus: Gastric empty
3. Gastric Body Reduction: Decrease gastric volume

FIBCMUMBAI
Role of Duodenum in Glucose Metabolism(Gene Analysis)
Liang Y, et al. SOARD, 2017 (epub ahead of print)

FIBCMUMBAI
Duodenum Regulates Glucose Metabolism(Gene Analysis)
Liang Y, et al. SOARD, 2017 (epub ahead of print)
Transcriptional factor Network
FIBCMUMBAI
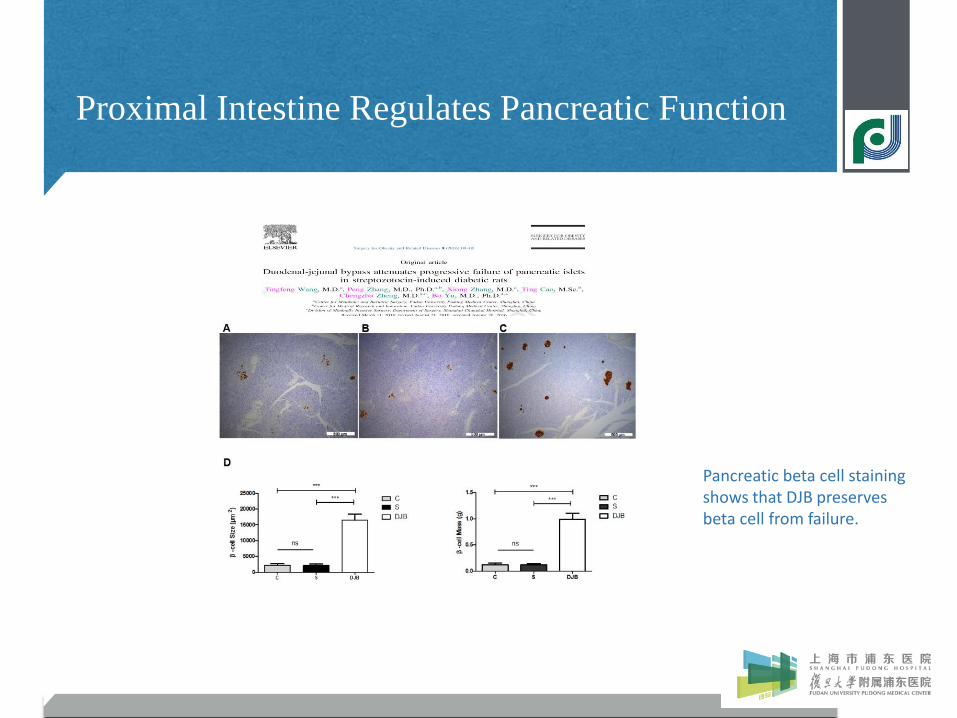
Proximal Intestine Regulates Pancreatic Function
Pancreatic beta cell staining shows that DJB preserves beta cell from failure.
FIBCMUMBAI
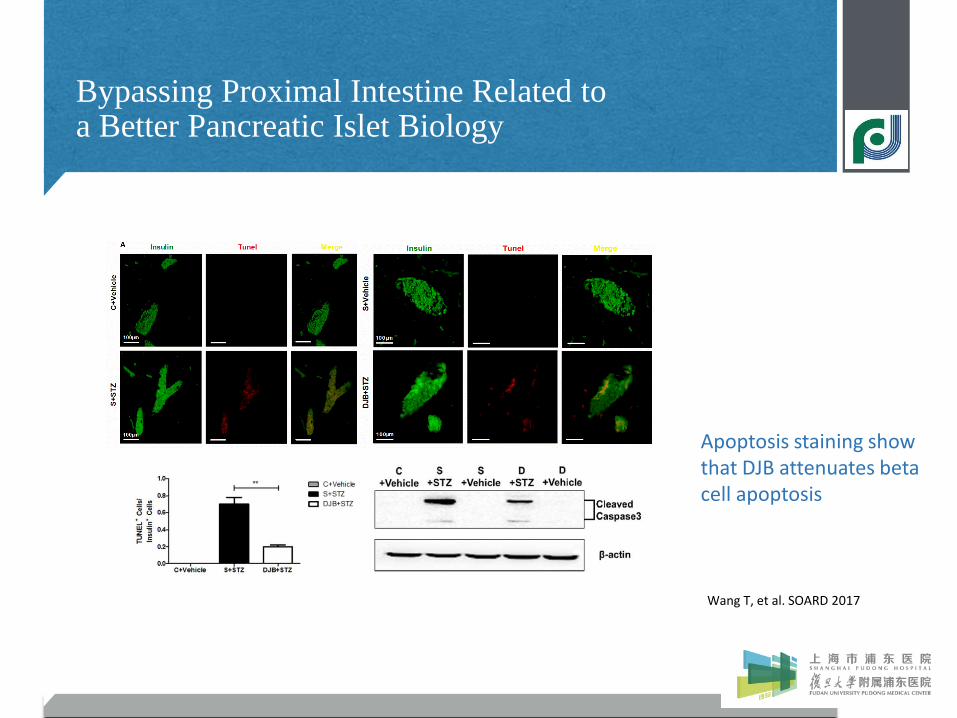
Bypassing Proximal Intestine Related to a Better Pancreatic Islet Biology
Wang T, et al. SOARD 2017
Apoptosis staining show that DJB attenuates beta cell apoptosis

FIBCMUMBAI
Role of Jejunum in Glucose Metabolism(Gene Analysis) --- Unpublished data
Unpublished Data
FIBCMUMBAI
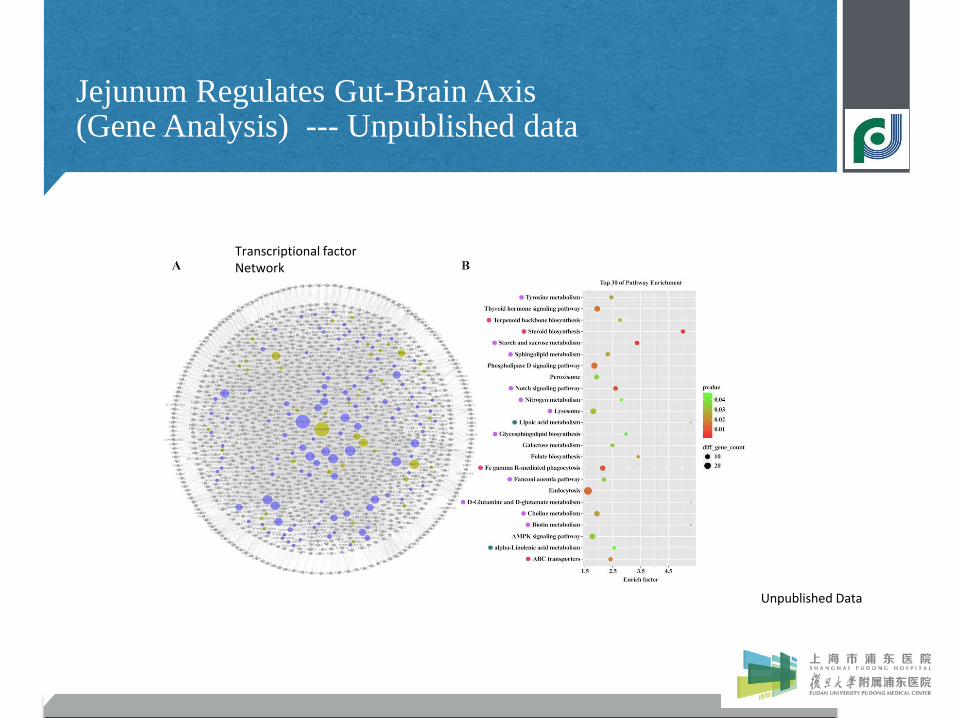
Jejunum Regulates Gut-Brain Axis(Gene Analysis) --- Unpublished data
Transcriptional factorNetwork
Unpublished Data
FIBCMUMBAI
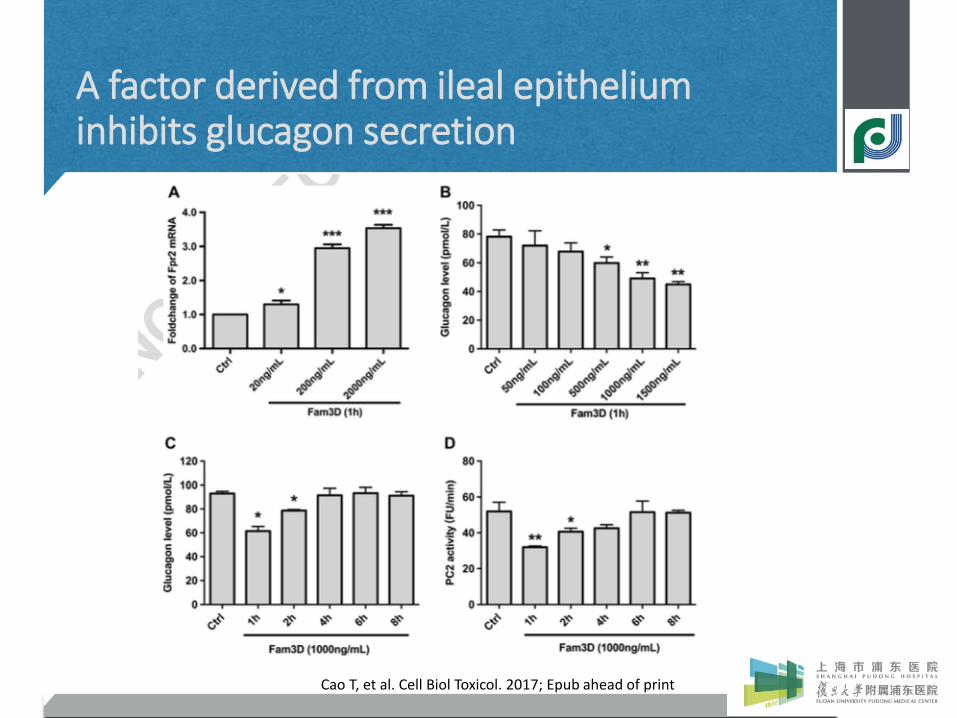
A factor derived from ileal epitheliuminhibits glucagon secretion
Cao T, et al. Cell Biol Toxicol. 2017; Epub ahead of print

Organ Function
StomachEnergy Set-point(Gastric cardia: sense fullness; Body:food reservoir; Pylorus: emptying)
Duodenum Pancreatic islet function regulation
Jejunum “Gut-Brain axis” initiator
Ileum “Gut-Endocrine Axis” Initiator ?
Re-defining Gastrointestinal Function
1. Zhang X, et al. Surg Obes Relat Dis. 2016;12(8):1569-15762. Wang T, et al. Surg Obes Relat Dis. 2017;13(2):250-2603. Liang Y, et al. Surg Obes Relat Dis. 2017; Epub ahead of print4. Cao T, et al. Cell Biol Toxicol. 2017; Epub ahead of print
“Ideal” Bariatric/Metabolic Surgery
• Gastric volume reduction
---> Inhibit ghrelin secretion
• Pylorus preservation
---> Programed gastric emptying, Anti-bile reflux
• Duodenal bypass
---> Further pancreatic islet function improvement
• Jejunal bypass
---> “gut-brain axis” leverage

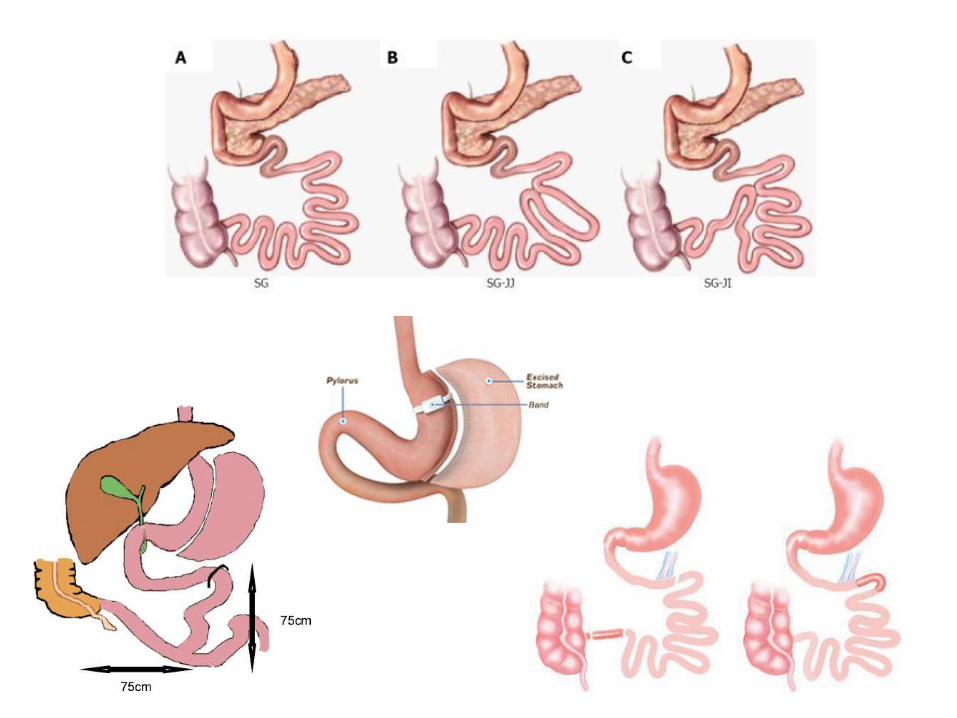
“Sleeve + X”: Next Generation Bariatric Surgery
(Pylorus preservation)
Sleeve
+
DJB
Sleeve
+
Single Anastomosis
1. Physiological pylorus: less dumping2. G-J anastomosis with bile afferent: less
marginal ulcer3. No gastric remnant: no worry remnant
carcinoma
1. Physiological pylorus: less dumping2. G-J anastomosis with bile afferent: less
marginal ulcer3. No gastric remnant: no worry remnant
carcinoma4. One GI transection: less internal hernia

Sleeve + Single Anastomosis
Sleeve + Loop DJB(Duodenal-Jejunal Bypass)
SADI-S(Duodenal-Ileal Bypass)
SIPS(Duodenal Switch)
Gastric Bougie 32-36 Fr > 54 Fr 40-42 Fr
Length ofbypassed intestine
150-300 cm Depends Depends
Length ofcommon channel
Depends 200-250 cm 300 cm
Category Combinational Malabsorption Combinational
Clinical outcome Similar to RYGB Similar to BPD-DSSuperior to RYGB、Similar to BPD-DS
Complications Lipid elevation?Malnutrition,
DiarrheaDiarrhea?

Why we do SIPS?
• Outcome similar to BPD-DS,Superior to gastric bypass and
sleeve gastrectomy
• 1 yr EBMIL 84%
• v.s. gastric bypass:
• Less dumping, less internal hernia, less marginal
• No worry about gastric remnant carcinoma
• v.s. sleeve gastrectomy:
• Add intestinal effect, lead to a better antidiabetic outcome
• v.s. BPD-DS:
• Less early complications(1.6% vs 20.9%)*
• Less OR time(69.9 vs 136.9 min)*
• GERD:
• Superior to LSG (slight larger gastric tube), but still a concern* Topart P, et al. Surg Obes Relat Dis. 2017

“Ideal” Bariatric/Metabolic Surgery
• Single-anastomosis duodenal switch procedures are considered investigational at present. The procedure should be performed under a study protocol with third-party oversight (local or regional ethics committee, institutional review board, data monitoring and safety board, clinicaltrials.gov, or equivalent authority) to ensure continuous evaluation of patient safety and to review adverse events and outcomes.
• Publication of short- and long-term safety and efficacy outcomes is strongly encouraged.
• Data for these procedures from accredited centers should be reported to the Metabolic and Bariatric Surgery Accreditation and Quality Improvement Program database and separately recorded as single-anastomosis DS procedures to allow accurate data collection.

“Future” Choice of Surgery?
Simple Obesity
or
Obesity with T2DM (<10yrs)
SuperObesity(BMI>50)
or
Obesity with T2DM (>12 yrs)
Obesity with T2DM (>12 years)
And
Symptomatic GERD
uncontrollable with PPI

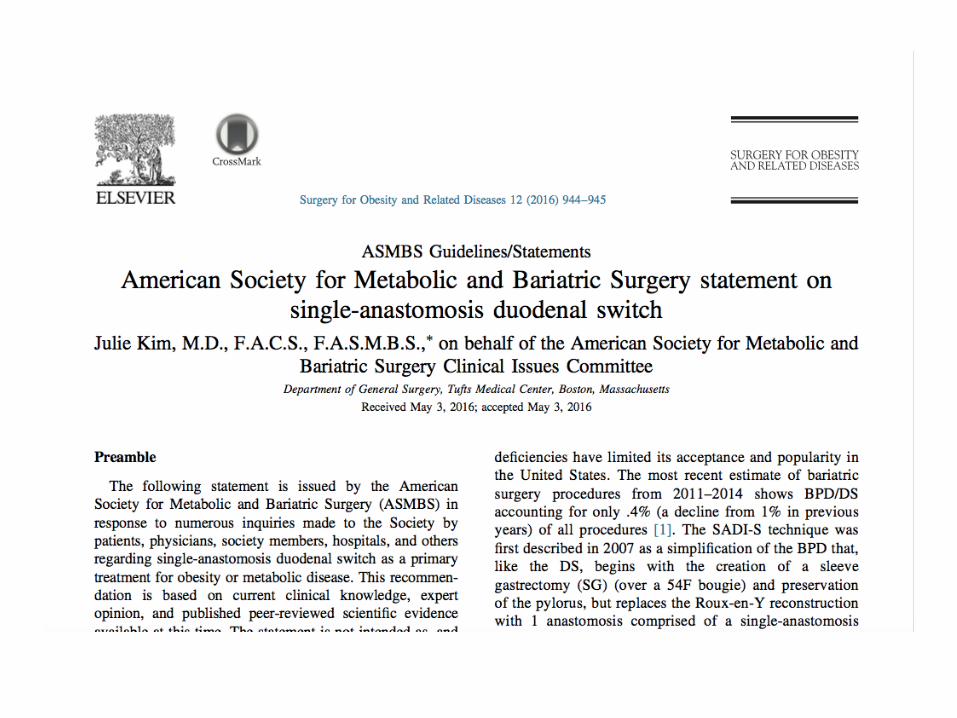
Other “Sleeve + X” Procedures
• Sleeve + JJB
• Sleeve + J-I anastomosis
• Sleeve + Band
• Sleeve + Ileal transposition

Summary
• Each GI segment has a role in metabolic regulation
• Gastric volume reduction is essential
• Pylorus should be preserved
• Intestinal exclusion gives added metabolic effect
• SIPS may become the next generation “goldstandard” in bariatric/metabolic surgery

46

















