Page 1
1
Small (and large) Blue CellTumors of the Skull Base
Jennifer L. Hunt, MD, MEdAubrey J. Hough Jr, MD, Endowed Professor of Pathology
Chair of Pathology and Laboratory MedicineUniversity of Arkansas for Medical Sciences
[email protected]
Page 2
2
Sino-Nasal Lesions
• High Grade Epithelial Tumors• Tumors with neuroendocrine differentiation• Other lesions in the differential diagnosis
Page 3
3
Sinonasal Undifferentiated Carcinoma
• Incidence: Rare• Clinical
• Present with large invasive tumors• Metastases are frequent• Symptoms include nasal obstruction, epistaxis,
visual and headache• Prognosis is poor
• ~20-25% overall survival at 5 years
Page 4
4
Sinonasal Undifferentiated Carcinoma
• Histopathology• Undifferentiated tumor cells• Mitoses and necrosis• Vascular invasion and adjacent structures
• Immunohistochemistry• Positive for Cytokeratin• Controversy: Neuroendocrine marker positivity
Page 9
9
Differential Diagnosis
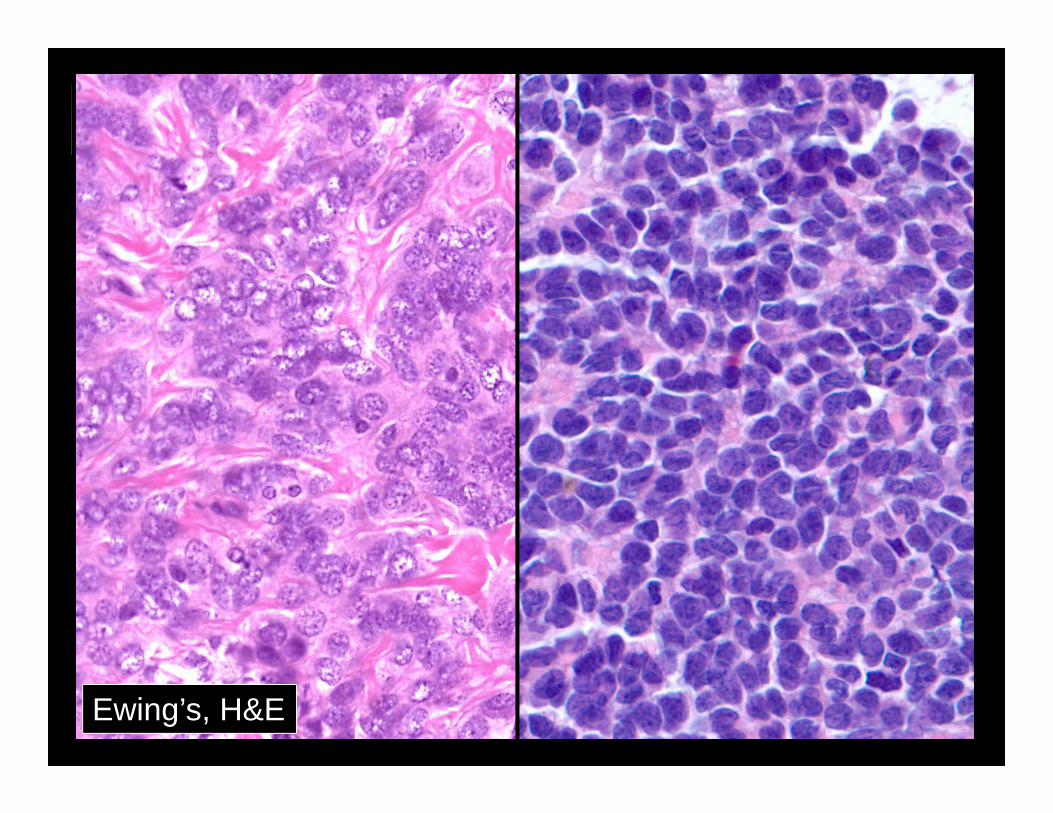
• Melanoma• Ewings/PNET• Rhabdomyosarcoma• NUT midline carcinoma• Lymphoepithelial carcinoma• Lymphoma• Neuroendocrine carcinoma
Page 10
10Mucosal Melanoma, H&E
Page 12
Rhabdomyosarcoma, H&E
Page 13
13
Work-Up of High Grade Tumor• Cytokeratin stains• Neuroendocrine stains• S100• HMB45• CD99• Myogenin• Desmin• Lymphoma markers
Page 14
14
NUT Midline Carcinoma
• Nut midline carcinomas• More common in young people
• Average age 17 years • Very aggressive (lethal) tumors
• Histology • Undifferentiated morphology• Abrupt keratinization in 82%• NUT-BRD4 translocation
French CA, JCO, 22(20):4135, 2004
Page 15
NUT midline carcinoma, H&E
Page 16
16
SNUC and NUT Translocation
• Stelow, et al• Undifferentiated carcinomas of UADT
• NUT rearrangement in 5/28 cases• NUT IHC positive in 3/5 cases
• Bishop, et al• NUT IHC in 151 primary sinonasal carcinomas
• 2 of 13 SNUCs positive • 1/87 squamous cell carcinomas positive
Stelow E, et al. AJSP, 32(6), 2008Bishop J, et al. AJSP, 36(8), 2012
Page 17
17
Sino-Nasal Lesions
• High Grade Epithelial Tumors• Tumors with neuroendocrine differentiation• Other lesions in the differential diagnosis
Page 18
18
Olfactory Neuroblastoma
• Incidence• Relatively rare (2% of sinonasal tumors)• Broad age range
• Peaks in 2nd and 6th decades
• Clinical• Sinonasal symptoms: nasal obstruction,
epistaxis, non-specific symptoms• Usually arises in the upper nasal cavity
(superior nasal concha, upper septum, roof of nose, cribriform plate)
Page 19
19
Olfactory Neuroblastoma
• Histopathology• Small to medium sized cells in nests• Usually minimal pleomorphism• Rosettes
• Homer Wright: Central fibrillary material • Up 30-50%
• Flexner-Wintersteiner: True lumen• Rare (~5%)
• Neuropil
Page 20
20Olfactory neuroblastoma
Page 21
21Involvement of the specialized olfactory epithelium
Page 22
22Olfactory neuroblastoma, Homer Wright
Page 23
23Olfactory neuroblastoma: Flexner-Wintersteiner
Page 24
24
Olfactory Neuroblastoma
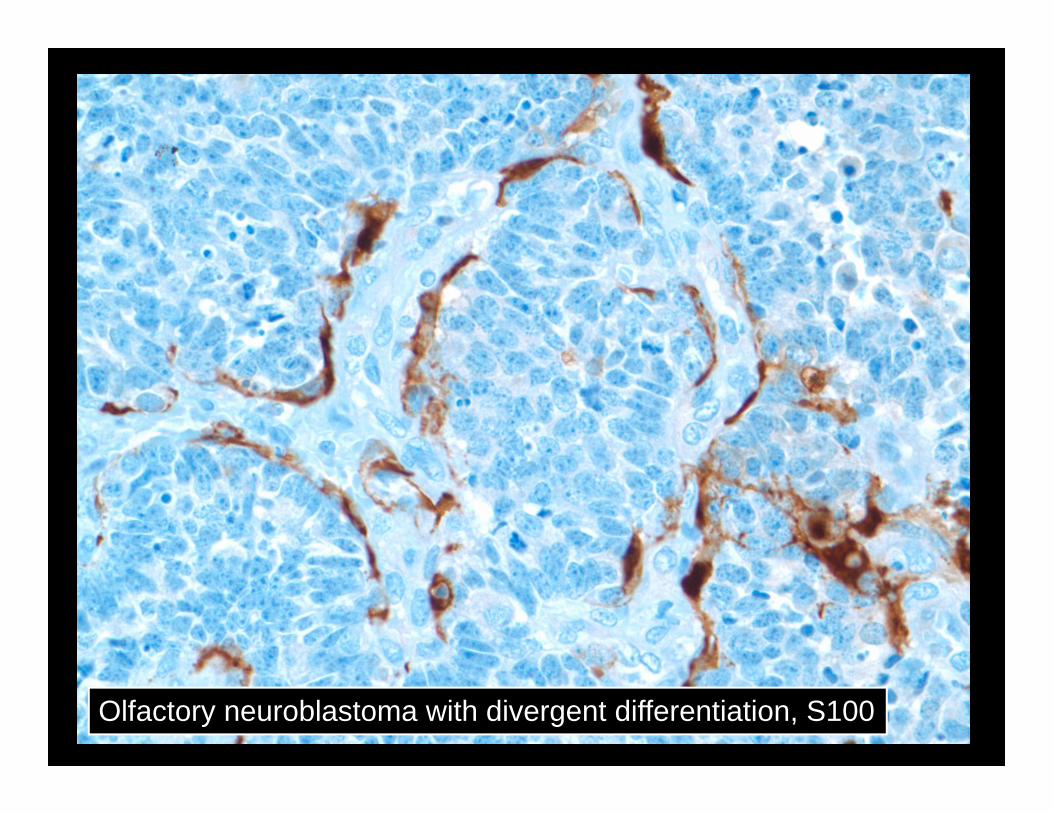
• Immunohistochemistry• Synpatophysin, chromogranin positive• S100 can have sustentacular pattern• CAM5.2 occasionally focally positive
Page 25
25Olfactory neuroblastoma, S100 stain
Page 26
26Olfactory neuroblastoma, Synaptophysin
Page 27
27
Olfactory Neuroblastoma
• Hyams grading (histologic grade)• Kadish stage (clinical staging)
• Vs. AJCC staging system
Page 28
28
Olfactory Neuroblastoma
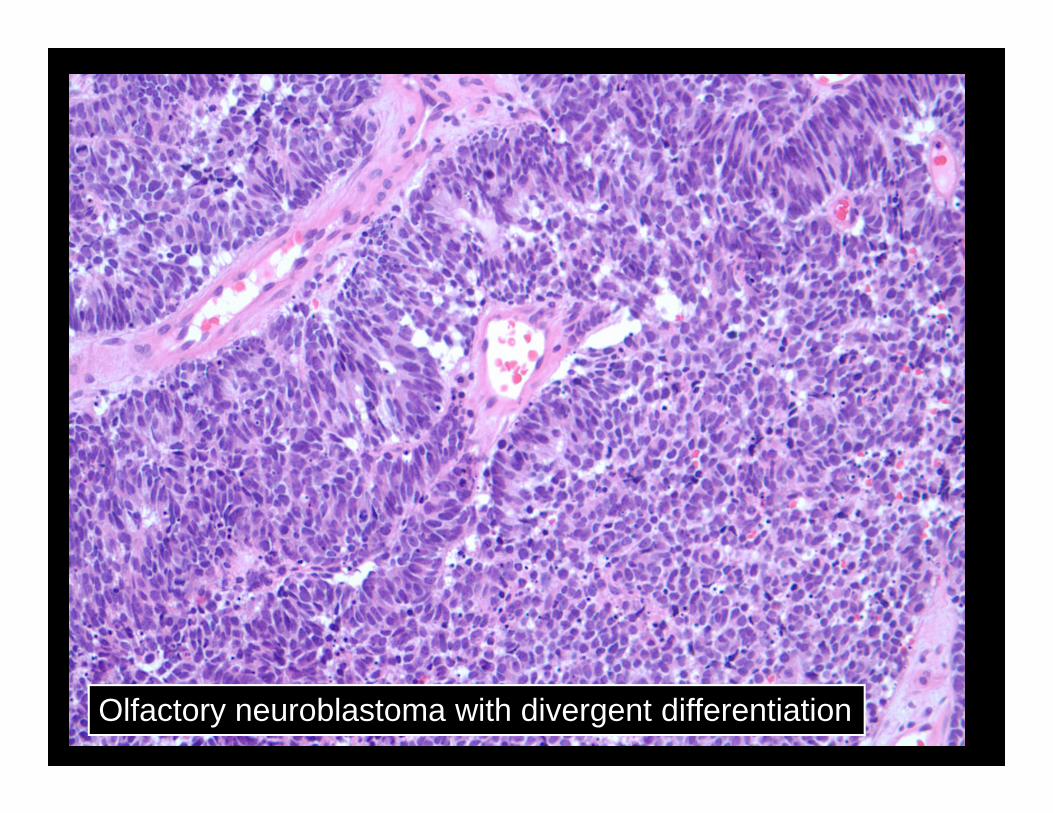
• Divergent Differentiation• Often high grade tumors• Other components present
• Rhabdomyosarcoma• Epithelial (Carcinoma)• Glandular (Adenocarcinoma)• Ganglion cells
Page 29
Olfactory neuroblastoma with divergent differentiation
Page 30
Olfactory neuroblastoma with divergent differentiation, S100
Page 31
Olfactory neuroblastoma with divergent differentiation
Synaptophysin Cytokeratin
Page 32
32
Differential Diagnosis
• Sinonasal neuroendocrine carcinoma• Paraganglioma• Ectopic pituitary adenoma
Page 33
33
Sinonasal Neuroendocrine Carcinoma
• Incidence• Rare tumor• Sinonasal neuroendocrine carcinoma (SNEC)
• Etiology• Possibly from olfactory epithelium
• Treatment and Prognosis• Combination therapy
Page 34
34
Sinonasal Neuroendocrine Carcinoma
• Histology• Solid sheets, ribbons, or trabeculae• Large cells with coarse chromatin and nucleoli• Necrosis and mitoses
• IHC• Chromogranin, syaptophysin, NSE• Cytokeratin
Page 35
35Neuroendocrine carcinoma
Page 36
36Neuroendocrine carcinoma
Page 37
Neuroendocrine carcinoma, synaptophysin
Page 38
38
Ectopic Pituitary
• Clinical• Occur along the embryological migration and
invagination pathway of Rathke’s Pouch• Distinguish radiologically, clinically and
surgically from invasive pituitary adenoma• Broad age range; most common in 6th decade• Frequently mis-diagnosed
Page 39
39
Ectopic Pituitary
• Pathology• Bland appearing neuroendocrine lesion• Hormones: FSH, LH, GH, TSH, ACTH, PRL,
Calcitonin
Page 40
Ectopic pituitary adenoma
Page 41
Ectopic pituitary adenoma, ACTH
Page 42
42
Summary
• High Grade Tumors• Sinonasal undifferentiated carcinoma• Differential Diagnosis: Ewings/PNET,
melanoma, Rhabdomyosarcoma• Tumors with neuroendocrine differentiation
• Sinonasal neuroendocrine carcinoma• Olfactory neuroblastoma• Ectopic pituitary adenoma