© Copyright 2007 – Eastern Association for the Surgery of Trauma 1
PRACTICE MANAGEMENT GUIDELINES
FOR SMALL BOWEL OBSTRUCTION
EAST Practice Parameter Workgroup for Management of Small Bowel Obstruction
© Copyright 2007 – Eastern Association for the Surgery of Trauma 2
Jose J. Diaz, Jr. MD; Co-Chair
Vanderbilt University Medical Center
Nashville, TN
E-mail: [email protected]
Faran Bokhari, MD; Vice-Chair
Stroger Hospital of Cook County
Chicago, IL
[email protected]
Nathan T. Mowery, MD
Vanderbilt University Medical Center
Nashville, TN
[email protected]
Jose A. Acosta, MD
San Diego, CA
[email protected]
Ernest F.J, Block, MD
Orlando Regional Healthcare System
Orlando, FL
[email protected]
William J. Bromberg, MD
Memorial Health University Medical Center
Savannah, GA
[email protected]
© Copyright 2007 – Eastern Association for the Surgery of Trauma 3
Bryan R. Collier, DO
Vanderbilt University Medical Center
Nashville, TN
[email protected]
Daniel C. Cullinane, MD
Mayo Clinic
Rochester, MN
[email protected]
Kevin M. Dwyer, MD
Inova Fairfax Hospital
Falls Church, VA
[email protected]
Margaret M. Griffen, MD
SHANDS – Jacksonville
Jacksonville, FL
[email protected]
John C. Mayberry, MD
Oregon Health & Science University
Portland, OR
[email protected]
Rebecca Jerome
Vanderbilt University Medical Center
Nashville, TN
[email protected]
© Copyright 2007 – Eastern Association for the Surgery of Trauma 4
Practice Management Guidelines for Small Bowel Obstruction
I. Statement of the Problem
The description of patients presenting with small bowel obstruction dates back to the
third or fourth century, when early surgeons created enterocutaneous fistulas to relieve a
bowel obstruction. Despite this success with operative therapy, the nonoperative
management of these patients with attempted reduction of hernias, laxatives, ingestion of
heavy metals (e.g., lead or mercury), and leeches to remove toxic agents from the blood
was the rule until the late 1800s, when antisepsis and aseptic surgical techniques made
operative intervention safer and more acceptable. A better understanding of the
pathophysiology of bowel obstruction and the use of isotonic fluid resuscitation,
intestinal tube decompression, and antibiotics have greatly reduced the mortality rate for
patients with mechanical bowel obstruction.1, 2 However, the means for determining when
a period of observation is warranted versus early surgical intervention continues to be an
area of debate. With the advances in imaging techniques additional information can be
supplied to the clinical information obtained from the history and physical. The question
of whether these technological advancements have allowed a more sophisticated
evaluation of these patients is yet to be determined. In addition which tests supply the
most information has yet to be clearly described.
Additionally the optimal length of observation continues to be debated. In the era
of a push toward shorter hospital stays correctly identifying patients who are to fail
observation is even more important. It is important to determine if clinical or
radiographic clues can increase our sensitivity in determining such patients.
Finally, as minimally invasive surgery grows and finds new applications are there
reproducible benefits to the patients in pursuing these intervention as both a diagnostic
and therapeutic intervention.
II. Process
A computerized search of the National Library of Medicine MEDLINE database was
undertaken using the PubMed Entrez interface. English language citations during the
period of 1991 through 2006 using the primary search strategy:
© Copyright 2007 – Eastern Association for the Surgery of Trauma 5
intestinal obstruction[mh] AND intestine, small[mh] AND humans[mh] NOT
(case reports[pt] OR letter[pt] OR comment[pt] OR news[pt])
Review articles were also excluded. The PubMed Related Articles algorithm was also
employed to identify additional articles similar to the items retrieved by the primary
strategy. Of approximately 550 articles identified by these two techniques, those dealing
with either prospective or retrospective studies examining small bowel obstruction were
selected, comprising 131 institutional studies evaluating diagnosis and management of
adult patients with suspected or proven small bowel obstruction. The articles were
reviewed by a group of eleven trauma / critical care surgeons who collaborated to
produce this practice management guideline. (Table 1)
The correlation between the evidence and the level of recommendations is as follows:
Level 1: This recommendation is convincingly justifiable based on the available scientific
information alone. It is usually based on Class I data, however, strong Class II evidence
may form the basis for a level 1 recommendation, especially if the issue does not lend
itself to testing in a randomized format. Conversely, weak or contradictory Class I data
may not be able to support a level 1 recommendation.
Level 2: This recommendation is reasonably justifiable by available scientific evidence
and strongly supported by expert critical care opinion. It is usually supported by Class II
data or a preponderance of Class III evidence.
Level 3: This recommendation is supported by available data but adequate scientific
evidence is lacking. It is generally supported by Class III data. This type of
recommendation is useful for educational purposes and in guiding future studies.3
III. Recommendations (Figure 1 – Flow diagram)
Diagnosis:
© Copyright 2007 – Eastern Association for the Surgery of Trauma 6
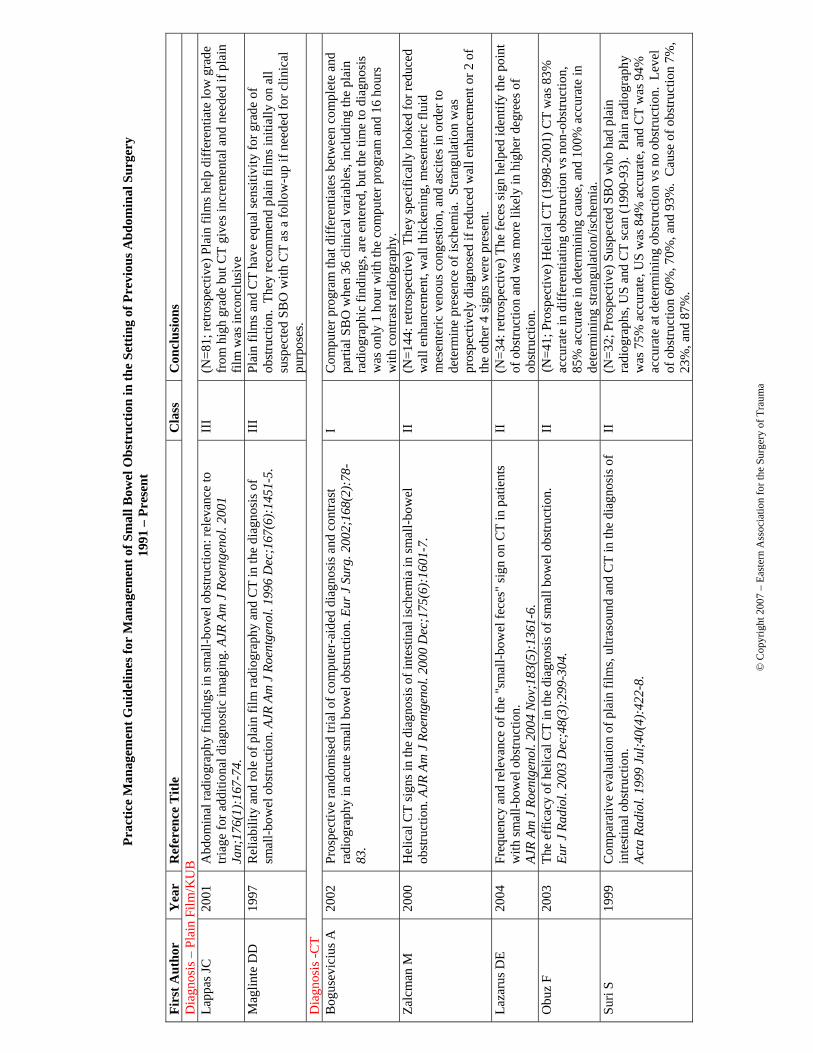
1. All patients being evaluated for small bowel obstruction should have plain films
due to the fact that plain films are as sensitive as CT to differentiate obstruction
vs. non-obstruction. LEVEL III
2. All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management. LEVEL I
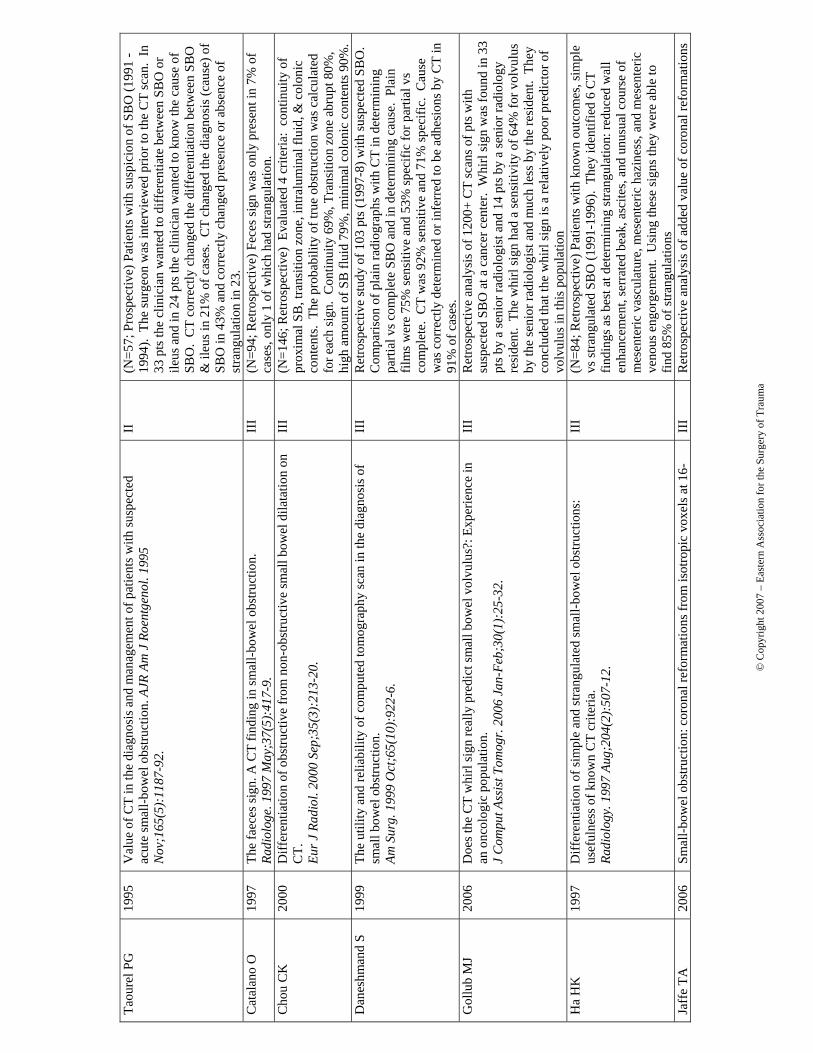
3. Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention (Table 2). LEVEL II
4. MRI and ultrasound are an alternative to CT with similar sensitivity and
identification of etiology, but have several logistical limitations. LEVEL III
5. There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction. LEVEL II
6. Nonionic low osmolar weight contrast is an alternative to barium for contrast
studies to evaluate for SBO for diagnostic purposes. LEVEL I
Management:
1. Patients with plain film finding of small bowel obstruction and Clinical markers
(fever, leukocytosis, tachycardia, metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration. LEVEL I
2. Patients without the above mentioned clinical picture, and a partial SBO or a
complete SBO can undergo non-operative management safely; although, complete
obstruction has a higher level of failure. LEVEL I
3. Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery. LEVEL III
4. There is no significant difference with regard to the decompression achieved, the
success of nonoperative treatment, or the morbidity rate after surgical intervention
comparing long tube decompression with the use of nasogastric tubes. LEVEL I
© Copyright 2007 – Eastern Association for the Surgery of Trauma 7
5. Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM), decrease length of stay, and is both therapeutic
and diagnostic. LEVEL II
6. In a highly selected group of patients the laparoscopic treatment of small bowel
obstruction should be considered and leads to a shorter hospital length of stay.
LEVEL II
Scientific Foundation
A. Historical Background
Mechanical small-bowel obstruction is the most frequently encountered surgical disorder
of the small intestine. Although a wide range of etiologies for this condition exist, intra-
abdominal adhesions related to prior abdominal surgery is the etiologic factor in up to
75% of cases of small-bowel obstruction. More than 300,000 patients are estimated to
undergo surgery to treat adhesion-induced small-bowel obstruction in the United States
annually.4
B. Diagnostic Evaluation of Small Bowel Obstruction
The diagnostic evaluation should focus on the following goals: distinguishing mechanical
obstruction from ileus; determining the etiology of the obstruction; discriminating partial
(low grade) from complete (high grade) obstruction; and discriminating simple from
strangulating obstruction.
Important elements to obtain on history include prior abdominal operations (suggesting
the presence of adhesions) and the presence of abdominal disorders (e.g., intra-abdominal
cancer or inflammatory bowel disease) that may provide insights into the etiology of
obstruction. Upon examination, a meticulous search for hernias (particularly in the
inguinal and femoral regions) should be conducted. The stool should be checked for
gross or occult blood, the presence of which is suggestive of intestinal strangulation.
Plain Films
The diagnosis of small-bowel obstruction is usually confirmed with radiographic
examination. The abdominal series consists of a radiograph of the abdomen with the
© Copyright 2007 – Eastern Association for the Surgery of Trauma 8
patient in a supine position, a radiograph of the abdomen with the patient in an upright
position, and a radiograph of the chest with the patient in an upright position. There is
class III evidence to suggest that plain films are as sensitive as CT for the detection of a
high grade bowel obstruction (86% vs. 82%).5 Data also suggests that plain films are less
sensitive in the setting of low grade or partial bowel obstruction. The sensitivity of
abdominal radiographs in the detection of small-bowel obstruction ranges from 70 to
86%.6, 7 Despite these limitations, abdominal radiographs remain an important study in
patients with suspected small-bowel obstruction because of their widespread availability
and low cost.
Computed tomographic (CT)
There is numerous Class II data to suggest that CT provides incremental information over
other imaging forms to the level, etiology and accuracy at differentiating low grade from
high grade bowel obstruction leading to changes in planned management.8-10 Computed
tomographic (CT) scanning is 80 to 90% sensitive and 70 to 90% specific in the detection
of small-bowel obstruction.11 The findings of small-bowel obstruction include a discrete
transition zone with dilation of bowel proximally, decompression of bowel distally,
intraluminal contrast that does not pass beyond the transition zone, and a colon
containing little gas or fluid.
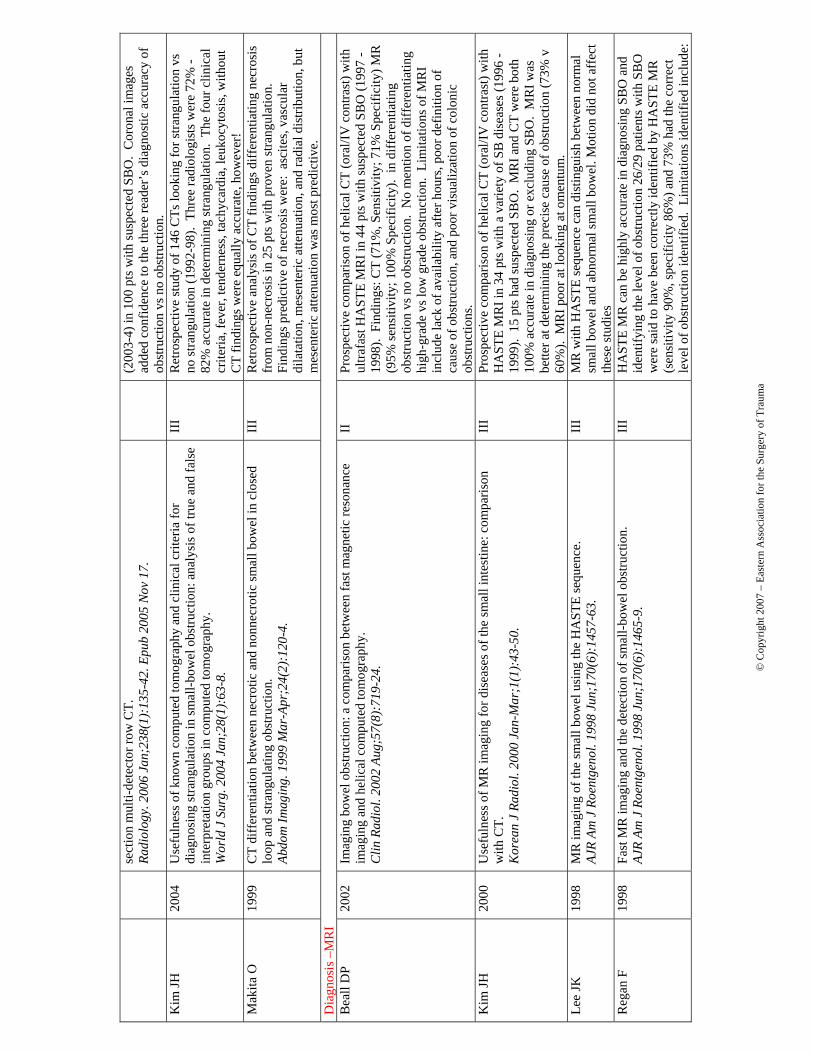
There is class II data to suggest that CT is 85 -100% sensitive for ischemia and
strangulation later confirmed by surgery.12-15 Ischemia was suggested on CT with:
serrated beak, unusual course of mesenteric vasculature, mesenteric haziness, reduced
wall enhancement, wall thickening, mesenteric fluid, mesenteric venous congestion, and
ascites.16-18 CT scanning also offers a global evaluation of the abdomen and may
therefore reveal the etiology of obstruction.19-21 The global picture afforded is especially
relevant when evaluating the acute abdomen when multiple etiologies are on the
differential diagnosis.
© Copyright 2007 – Eastern Association for the Surgery of Trauma 9
Enteroclysis
A limitation of CT scanning is its low sensitivity (<50%) in the detection of low-grade or
partial small-bowel obstruction. A subtle transition zone or unsuspected closed loop
obstruction may be difficult to identify in the axial images obtained during CT scanning.
In such cases, contrast examinations of the small bowel, either small-bowel series (small-
bowel follow-through) or enteroclysis, can be helpful.22 Nonionic low osmolar weight
contrast is an alternative to barium for contrast studies to evaluate for SBO.23 These
examinations are more labor intensive and less-rapidly performed than CT scanning, but
may offer greater sensitivity in the detection of luminal and mural etiologies of
obstruction, such as primary intestinal tumors, with sensitivity and specificity
approaching 100% when coupled with CT.24 Enteroclysis is rarely performed in the acute
setting, but offers greater sensitivity than small-bowel series in the detection of lesions
that may be causing partial small-bowel obstruction.25
Ultrasound
Class II data suggests ultrasound is comparable to plain film for the diagnosis, etiology
and strangulation in small bowel obstruction and can better identify free fluid which may
signal the need for operative intervention.26-30
MRI
Class II data reports the accuracy MRI at least approaches that of CT with both
differentiating obstruction vs no obstruction at an almost 100% sensativity.31 MRI has
also been shown to be effective in defining location and etiology of obstruction with at
least equivalent accuracy of CT.32-34 Limitations of MRI include: lack of availability
after hours, poor definition of mass lesions, and poor visualization of colonic obstructions
did not show inflammation as well as CT, and does not show viability.35, 36
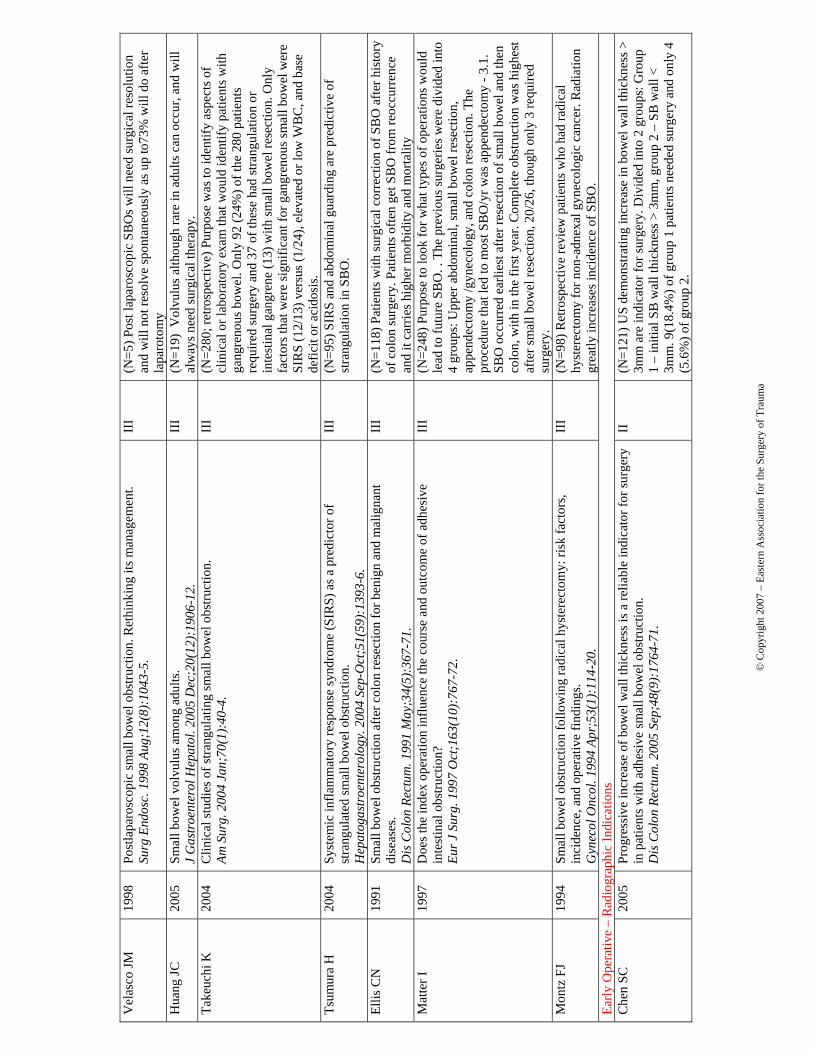
C. Evaluation of the Evidence Supporting Early Operative Management
The standard therapy for small-bowel obstruction is expeditious surgery. The rationale
for this approach is to minimize the risk for bowel strangulation, which is associated with
© Copyright 2007 – Eastern Association for the Surgery of Trauma 10
an increased risk for morbidity and mortality. The literature would suggest that clinical
signs supported by simple imaging studies can identify the vast majority of patients
presenting with surgical small bowel obstruction.37, 38 Early operative intervention in
patients with fever, leukocytosis, peritonitis, tachycardia, metabolic acidosis, and
continuous pain will identify strangulation 45% of the time39-41 Complete SBO should be
operated on early as the primary mode of therapy. Studies would suggest that 31-43% of
patients with complete SBO or peritonitis will resolve without requiring some form of
bowel resection. 42, 43
Other reported benefits of the operative management of SBO is the description by class II
data that reports lower reoccurrence rate and longer disease free intervals with operative
intervention when compared to conservative management. 44-47
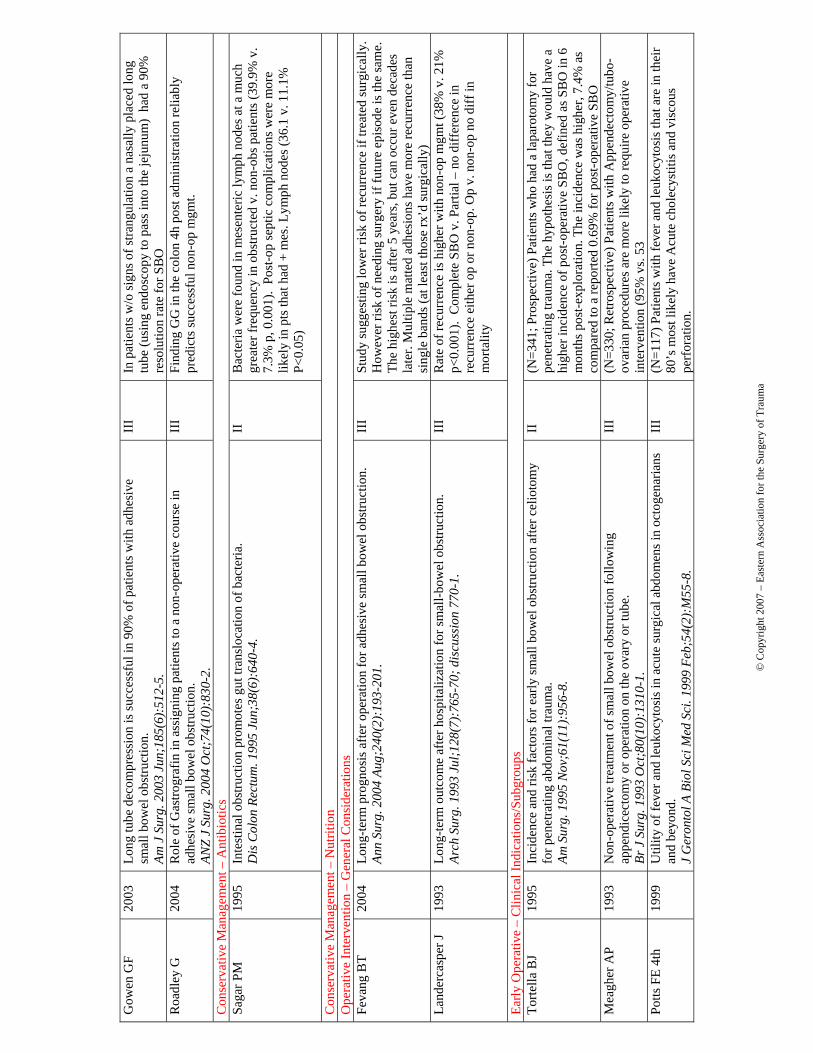
D. Evaluation of the Evidence Supporting Conservative Management
Exceptions to the recommendation for expeditious surgery for intestinal obstruction
include partial small-bowel obstruction, obstruction occurring in the early postoperative
period, intestinal obstruction as a consequence of Crohn's disease, and carcinomatosis.
Progression to strangulation (3-6% with conservative management) is unlikely to occur
with partial small-bowel obstruction, and an attempt at nonoperative resolution is
warranted.48 Level II data suggests that nonoperative management has been documented
to be successful in 65 to 81% of patients with partial small-bowel obstruction or in
patients without peritonitis.1 Of those successfully treated non-operatively, only 5 to 15%
have been reported to have symptoms that were not substantially improved within 48
hours after initiation of therapy.49-52 Therefore, most patients with partial small
obstruction whose symptoms do not improve within 48 hours after initiation of
nonoperative therapy should undergo surgery. There has been some level III data to
suggest that this time period can be safely lengthened to 5 days without increase the
likelihood of strangulation necessitating bowel resection although definite data to support
these claims is not available.2 Patients undergoing non-operative therapy should be
© Copyright 2007 – Eastern Association for the Surgery of Trauma 11
followed with serial abdominal exams for signs of peritonitis which would necessitate
immediate operative intervention.
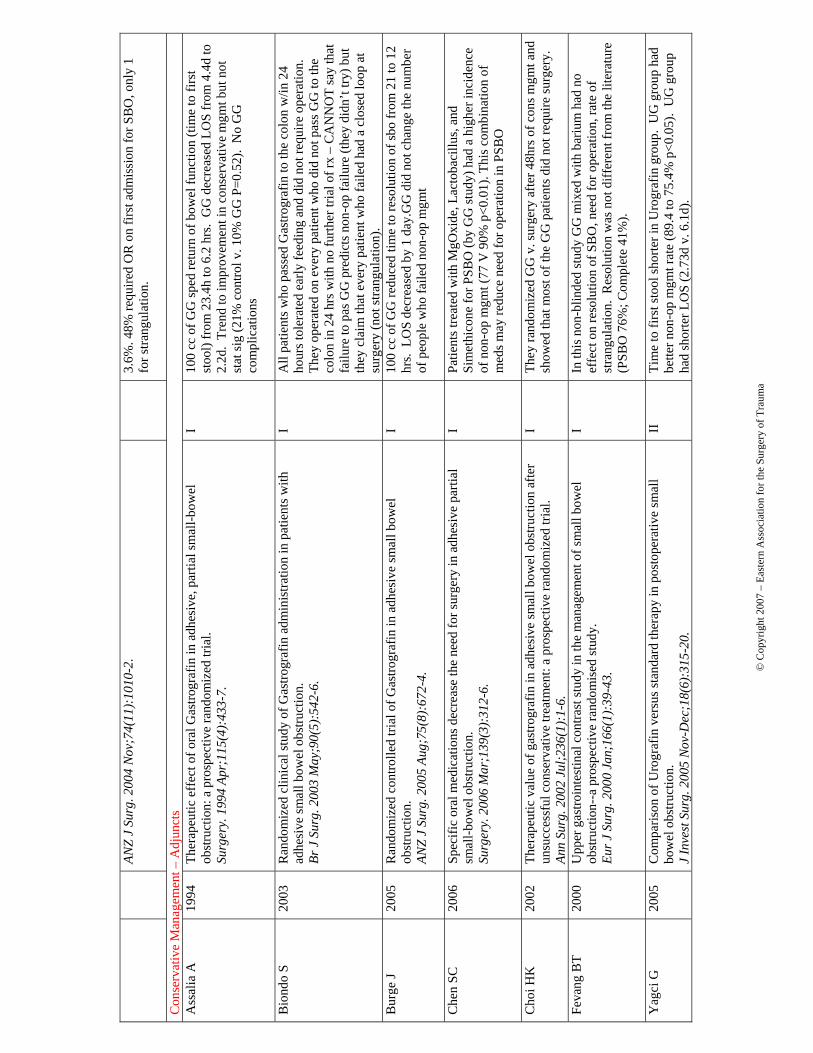
Adjuncts to Conservative Management
Hypertonic contrast in PSBO
The administration of hypertonic water-soluble contrast agents, such as Gastrografin used
in upper GI and small-bowel follow-through examinations, causes a shift of fluid into the
intestinal lumen, thereby increasing the pressure gradient across the site of obstruction.
Level II data suggests that this effect may speed the return of bowel function (time to
bowel movement) and decrease the length of stay of patients undergoing non-operative
management of partial small bowel obstruction.53-58
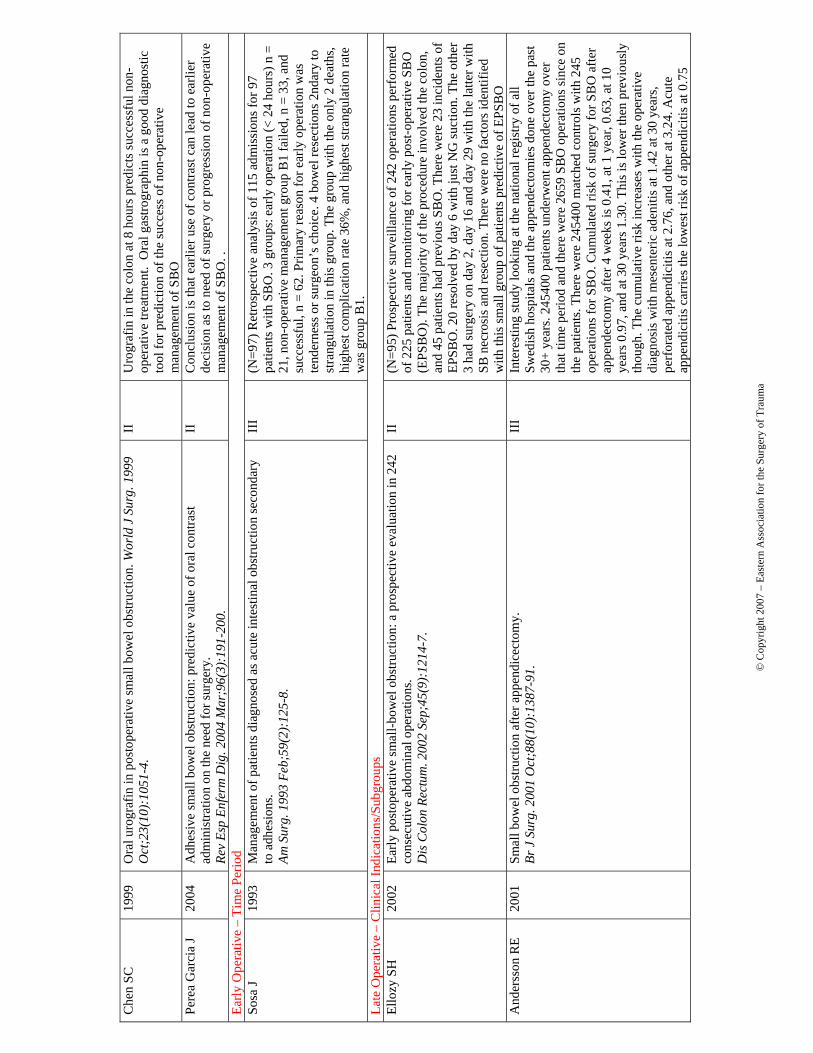
E. Operative Approach
Successful laparoscopic surgery for bowel obstruction is being reported with greater
frequency. Reported data suggest that up to 60% of small-bowel obstruction cases caused
by adhesions may be amenable to laparoscopic therapy.59 The reported conversion rate is
20-51.9%60-67 and the complication rate (bowel injury) is 6.5-18.0%.60, 68 Conversion to
open procedure have been reported secondary to density of adhesions, inability to fix the
obstruction, cause of obstruction not amenable to laparoscopic therapy, intestinal
necrosis, and intestinal perforation. Factors that favor laparoscopic success are SBO post
appendectomy, with bands as cause, with less then two previous surgeries, and shorter
time of symptoms.69 It has been reported that conversion rate can be decreased to as low
as 6.9% when the surgery is guided by preoperative enteroclysis.70 The laparoscopic
treatment of small bowel obstruction appears to be effective and leads to a shorter
hospital stay in a highly selected group of patients.71, 72 There has also been literature to
support that patients treated with laparoscopic intervention have lower hernia rate and
SBO but require the same amount of operative intervention.73 Patients fitting the criteria
for consideration of laparoscopic management include those with (1) mild abdominal
distention allowing adequate visualization, (2) a proximal obstruction, (3) a partial
obstruction, and (4) an anticipated single-band obstruction. Currently, patients who have
advanced, complete, or distal small bowel obstructions are not candidates for
laparoscopic treatment. Unfortunately, the majority of patients with obstruction are in this
© Copyright 2007 – Eastern Association for the Surgery of Trauma 12
group. Similarly, patients with matted adhesions or those who remain distended after
nasogastric intubation should be managed with conventional laparotomy. Therefore, the
future role of laparoscopic procedures in the treatment of these patients remains to be
defined.
F. Adjuncts to Surgery
Antibiotics
Broad-spectrum antibiotics are commonly administered because of concerns that
bacterial translocation may occur in the setting of small-bowel obstruction; however,
there are no controlled data to support or refute this approach.74
Long Tube
Prospective randomized trials demonstrated no significant differences with regard to the
decompression achieved, the success of nonoperative treatment, or the morbidity rate
after surgical intervention compared with the use of nasogastric tubes. Furthermore, the
use of these long tubes has been associated with a significantly longer hospital stay,
duration of postoperative ileus, and postoperative complications in some series.
Therefore, it appears that long intestinal tubes offer no benefit in the preoperative setting
over nasogastric tubes.75, 76
Hyaluronic acid-carboxycellulose membrane (Seprafilm)
The overall rate of post-operative SBO showed no difference with or without Seprafilm.
However, Seprafilm did have lower (1.8 vs 3.4%) of SBO requiring reoperation.77-80
V. Summary
To summarize, plain abdominal radiographs are usually diagnostic of bowel obstruction
in more than 60% of the cases, but further evaluation (possibly by CT or barium
radiography) may be necessary in 20% to 30% of cases. CT examination is particularly
useful in patients with a history of abdominal malignancy, in postsurgical patients, and in
patients who have no history of abdominal surgery and present with symptoms of bowel
© Copyright 2007 – Eastern Association for the Surgery of Trauma 13
obstruction. Barium studies are recommended in patients with a history of recurring
obstruction or low-grade mechanical obstruction to precisely define the obstructed
segment and degree of obstruction.
VI. Future Investigations
Future studies should be conducted in a prospective, randomized fashion concentrating
on the timing of operative intervention for small bowel obstruction.
© Copyright 2007 – Eastern Association for the Surgery of Trauma 14
REFERENCES
1. Hartwell JA and Hoguet JP. Experimental intestinal obstruction in dogs with special
reference to the cause of death and the treatment by large amounts of normal saline
solution. JAMA 59, 82-87. 1912.
Ref Type: Abstract
2. Wangensteen OH. Historical aspects of the management of acute intestinal
obstruction. Surgery. 1969;65:363-383.
3. PRACTICE MANAGEMENT GUIDELINES FOR TRAUMA EAST AD
HOC COMMITTEE ON
GUIDELINE DEVELOPMENT. 1-23-0098.
Ref Type: Conference Proceeding
4. Ray NF, Denton WG, Thamer M, Henderson SC, Perry S. Abdominal adhesiolysis:
inpatient care and expenditures in the United States in 1994. J Am Coll Surg.
1998;186:1-9.
5. Maglinte DD, Reyes BL, Harmon BH et al. Reliability and role of plain film
radiography and CT in the diagnosis of small-bowel obstruction. AJR Am J
Roentgenol %1996 Dec ;167 (6 ):1451 -5.
6. Maglinte DD, Heitkamp DE, Howard TJ, Kelvin FM, Lappas JC. Current concepts
in imaging of small bowel obstruction. Radiol Clin North Am. 2003;41:263-83, vi.
© Copyright 2007 – Eastern Association for the Surgery of Trauma 15
7. Suri S, Gupta S, Sudhakar PJ, Venkataramu NK, Sood B, Wig JD. Comparative
evaluation of plain films, ultrasound and CT in the diagnosis of intestinal
obstruction. Acta Radiol %1999 Jul ;40 (4):422 -8.
8. Daneshmand S, Hedley CG, Stain SC. The utility and reliability of computed
tomography scan in the diagnosis of small bowel obstruction. Am Surg %1999 Oct
;65 (10):922 -6.
9. Suri S, Gupta S, Sudhakar PJ, Venkataramu NK, Sood B, Wig JD. Comparative
evaluation of plain films, ultrasound and CT in the diagnosis of intestinal
obstruction. Acta Radiol %1999 Jul ;40 (4):422 -8.
10. Taourel PG, Fabre JM, Pradel JA, Seneterre EJ, Megibow AJ, Bruel JM. Value of
CT in the diagnosis and management of patients with suspected acute small-bowel
obstruction. AJR Am J Roentgenol %1995 Nov ;165 (5):1187 -92.
11. Maglinte DD, Heitkamp DE, Howard TJ, Kelvin FM, Lappas JC. Current concepts
in imaging of small bowel obstruction. Radiol Clin North Am. 2003;41:263-83, vi.
12. Daneshmand S, Hedley CG, Stain SC. The utility and reliability of computed
tomography scan in the diagnosis of small bowel obstruction. Am Surg %1999 Oct
;65 (10):922 -6.
© Copyright 2007 – Eastern Association for the Surgery of Trauma 16
13. Makita O, Ikushima I, Matsumoto N, Arikawa K, Yamashita Y, Takahashi M. CT
differentiation between necrotic and nonnecrotic small bowel in closed loop and
strangulating obstruction. Abdom Imaging %1999 Mar -Apr;24 (2):120 -4.
14. Obuz F, Terzi C, Sokmen S, Yilmaz E, Yildiz D, Fuzun M. The efficacy of helical
CT in the diagnosis of small bowel obstruction. Eur J Radiol %2003 Dec ;48
(3):299 -304.
15. Zalcman M, Sy M, Donckier V, Closset J, Gansbeke DV. Helical CT signs in the
diagnosis of intestinal ischemia in small-bowel obstruction. AJR Am J Roentgenol
%2000 Dec ;175 (6 ):1601 -7.
16. Obuz F, Terzi C, Sokmen S, Yilmaz E, Yildiz D, Fuzun M. The efficacy of helical
CT in the diagnosis of small bowel obstruction. Eur J Radiol %2003 Dec ;48
(3):299 -304.
17. Zalcman M, Sy M, Donckier V, Closset J, Gansbeke DV. Helical CT signs in the
diagnosis of intestinal ischemia in small-bowel obstruction. AJR Am J Roentgenol
%2000 Dec ;175 (6 ):1601 -7.
18. Ha HK, Kim JS, Lee MS et al. Differentiation of simple and strangulated small-
bowel obstructions: usefulness of known CT criteria. Radiology %1997 Aug ;204
(2):507 -12.
© Copyright 2007 – Eastern Association for the Surgery of Trauma 17
19. Lappas JC, Reyes BL, Maglinte DD. Abdominal radiography findings in small-
bowel obstruction: relevance to triage for additional diagnostic imaging. AJR Am J
Roentgenol %2001 Jan ;176 (1):167 -74.
20. Maglinte DD, Heitkamp DE, Howard TJ, Kelvin FM, Lappas JC. Current concepts
in imaging of small bowel obstruction. Radiol Clin North Am. 2003;41:263-83, vi.
21. Suri S, Gupta S, Sudhakar PJ, Venkataramu NK, Sood B, Wig JD. Comparative
evaluation of plain films, ultrasound and CT in the diagnosis of intestinal
obstruction. Acta Radiol %1999 Jul ;40 (4):422 -8.
22. Maglinte DD, Nolan DJ, Herlinger H. Preoperative diagnosis by enteroclysis of
unsuspected closed loop obstruction in medically managed patients. J Clin
Gastroenterol %1991 Jun ;13(3):308 -12.
23. Sandikcioglu TG, Torp-Madsen S, Pedersen IK, Raaschou K, Mygind T, Thomsen
HS. Contrast radiography in small bowel obstruction. A randomized trial of barium
sulfate and a nonionic low-osmolar contrast medium. Acta Radiol %1994 Jan ;35
(1):62 -4.
24. Boudiaf M, Jaff A, Soyer P, Bouhnik Y, Hamzi L, Rymer R. Small-bowel diseases:
prospective evaluation of multi-detector row helical CT enteroclysis in 107
consecutive patients. Radiology %2004 Nov ;233 (2):338 -44 Epub 2004 Sep
30.Epub.
© Copyright 2007 – Eastern Association for the Surgery of Trauma 18
25. Boudiaf M, Jaff A, Soyer P, Bouhnik Y, Hamzi L, Rymer R. Small-bowel diseases:
prospective evaluation of multi-detector row helical CT enteroclysis in 107
consecutive patients. Radiology %2004 Nov ;233 (2):338 -44 Epub 2004 Sep
30.Epub.
26. Czechowski J. Conventional radiography and ultrasonography in the diagnosis of
small bowel obstruction and strangulation. Acta Radiol %1996 Mar ;37 (2):186 -9.
27. Grassi R, Romano S, D'Amario F et al. The relevance of free fluid between
intestinal loops detected by sonography in the clinical assessment of small bowel
obstruction in adults. Eur J Radiol %2004 Apr;50 (1):5-14.
28. Ko YT, Lim JH, Lee DH, Lee HW, Lim JW. Small bowel obstruction: sonographic
evaluation. Radiology %1993 Sep ;188 (3):649 -53.
29. Schmutz GR, Benko A, Fournier L, Peron JM, Morel E, Chiche L. Small bowel
obstruction: role and contribution of sonography. Eur Radiol %1997 ;7 (7 ):1054 -
8.
30. Suri S, Gupta S, Sudhakar PJ, Venkataramu NK, Sood B, Wig JD. Comparative
evaluation of plain films, ultrasound and CT in the diagnosis of intestinal
obstruction. Acta Radiol %1999 Jul ;40 (4):422 -8.
© Copyright 2007 – Eastern Association for the Surgery of Trauma 19
31. Kim JH, Ha HK, Sohn MJ et al. Usefulness of MR imaging for diseases of the small
intestine: comparison with CT. Korean J Radiol %2000 Jan -Mar ;1(1):43 -50.
32. Beall DP, Fortman BJ, Lawler BC, Regan F. Imaging bowel obstruction: a
comparison between fast magnetic resonance imaging and helical computed
tomography. Clin Radiol %2002 Aug ;57 (8 ):719 -24.
33. Kim JH, Ha HK, Sohn MJ et al. Usefulness of MR imaging for diseases of the small
intestine: comparison with CT. Korean J Radiol %2000 Jan -Mar ;1(1):43 -50.
34. Regan F, Beall DP, Bohlman ME, Khazan R, Sufi A, Schaefer DC. Fast MR
imaging and the detection of small-bowel obstruction. AJR Am J Roentgenol %1998
Jun ;170 (6 ):1465 -9.
35. Regan F, Beall DP, Bohlman ME, Khazan R, Sufi A, Schaefer DC. Fast MR
imaging and the detection of small-bowel obstruction. AJR Am J Roentgenol %1998
Jun ;170 (6 ):1465 -9.
36. Beall DP, Fortman BJ, Lawler BC, Regan F. Imaging bowel obstruction: a
comparison between fast magnetic resonance imaging and helical computed
tomography. Clin Radiol %2002 Aug ;57 (8 ):719 -24.
© Copyright 2007 – Eastern Association for the Surgery of Trauma 20
37. Bogusevicius A, Maleckas A, Pundzius J, Skaudickas D. Prospective randomised
trial of computer-aided diagnosis and contrast radiography in acute small bowel
obstruction. Eur J Surg %2002 ;168 (2):78 -83.
38. Kim JH, Ha HK, Kim JK et al. Usefulness of known computed tomography and
clinical criteria for diagnosing strangulation in small-bowel obstruction: analysis of
true and false interpretation groups in computed tomography. World J Surg %2004
Jan ;28 (1):63 -8 Epub 2003 Dec 4.Epub.
39. Fevang BT, Jensen D, Svanes K, Viste A. Early operation or conservative
management of patients with small bowel obstruction? Eur J Surg %2002 ;168 (8 -
9 ):475 -81.
40. Takeuchi K, Tsuzuki Y, Ando T et al. Clinical studies of strangulating small bowel
obstruction. Am Surg %2004 Jan ;70 (1):40 -4.
41. Tsumura H, Ichikawa T, Hiyama E, Murakami Y, Sueda T. Systemic inflammatory
response syndrome (SIRS) as a predictor of strangulated small bowel obstruction.
Hepatogastroenterology %2004 Sep -Oct ;51 (59 ):1393 -6.
42. Fevang BT, Jensen D, Svanes K, Viste A. Early operation or conservative
management of patients with small bowel obstruction? Eur J Surg %2002 ;168 (8 -
9 ):475 -81.
© Copyright 2007 – Eastern Association for the Surgery of Trauma 21
43. Nauta RJ. Advanced abdominal imaging is not required to exclude strangulation if
complete small bowel obstructions undergo prompt laparotomy. J Am Coll Surg
%2005 Jun ;200 (6 ):904 -11.
44. Fevang BT, Fevang J, Lie SA, Soreide O, Svanes K, Viste A. Long-term prognosis
after operation for adhesive small bowel obstruction. Ann Surg %2004 Aug ;240
(2):193 -201.
45. Landercasper J, Cogbill TH, Merry WH, Stolee RT, Strutt PJ. Long-term outcome
after hospitalization for small-bowel obstruction. Arch Surg %1993 Jul ;128 (7
):765 -70.discussion.
46. Miller G, Boman J, Shrier I, Gordon PH. Natural history of patients with adhesive
small bowel obstruction. Br J Surg %2000 Sep ;87 (9 ):1240 -7.
47. Williams SB, Greenspon J, Young HA, Orkin BA. Small bowel obstruction:
conservative vs. surgical management. Dis Colon Rectum %2005 Jun ;48 (6 ):1140
-6.
48. Fevang BT, Jensen D, Svanes K, Viste A. Early operation or conservative
management of patients with small bowel obstruction? Eur J Surg %2002 ;168 (8 -
9 ):475 -81.
© Copyright 2007 – Eastern Association for the Surgery of Trauma 22
49. Brolin RE, Krasna MJ, Mast BA. Use of tubes and radiographs in the management
of small bowel obstruction. Ann Surg. 1987;206:126-133.
50. Peetz DJ, Jr., Gamelli RL, Pilcher DB. Intestinal intubation in acute, mechanical
small-bowel obstruction. Arch Surg. 1982;117:334-336.
51. Cox MR, Gunn IF, Eastman MC, Hunt RF, Heinz AW. The safety and duration of
non-operative treatment for adhesive small bowel obstruction. Aust N Z J Surg
%1993 May ;63 (5):367 -71.
52. Fevang BT, Jensen D, Svanes K, Viste A. Early operation or conservative
management of patients with small bowel obstruction? Eur J Surg %2002 ;168 (8 -
9 ):475 -81.
53. Assalia A, Schein M, Kopelman D, Hirshberg A, Hashmonai M. Therapeutic effect
of oral Gastrografin in adhesive, partial small-bowel obstruction: a prospective
randomized trial. Surgery %1994 Apr;115 (4):433 -7.
54. Burge J, Abbas SM, Roadley G et al. Randomized controlled trial of Gastrografin in
adhesive small bowel obstruction. Anz J Surg %2005 Aug ;75 (8 ):672 -4.
55. Choi HK, Chu KW, Law WL. Therapeutic value of gastrografin in adhesive small
bowel obstruction after unsuccessful conservative treatment: a prospective
randomized trial. Ann Surg %2002 Jul ;236 (1):1-6.
© Copyright 2007 – Eastern Association for the Surgery of Trauma 23
56. Choi HK, Law WL, Ho JW, Chu KW. Value of gastrografin in adhesive small
bowel obstruction after unsuccessful conservative treatment: a prospective
evaluation. World J Gastroenterol %2005 Jun 28 ;11(24 ):3742 -5.
57. Fevang BT, Jensen D, Fevang J et al. Upper gastrointestinal contrast study in the
management of small bowel obstruction--a prospective randomised study. Eur J
Surg %2000 Jan ;166 (1):39 -43.
58. Yagci G, Kaymakcioglu N, Can MF, Peker Y, Cetiner S, Tufan T. Comparison of
Urografin versus standard therapy in postoperative small bowel obstruction. J Invest
Surg %2005 Nov -Dec ;18 (6 ):315 -20.
59. Fischer CP, Doherty D. Laparoscopic approach to small bowel obstruction. Semin
Laparosc Surg. 2002;9:40-45.
60. Borzellino G, Tasselli S, Zerman G, Pedrazzani C, Manzoni G. Laparoscopic
approach to postoperative adhesive obstruction. Surg Endosc %2004 Apr;18
(4):686 -90 Epub 2004 Mar %19. 1919.
61. Chopra R, Mcvay C, Phillips E, Khalili TM. Laparoscopic lysis of adhesions. Am
Surg %2003 Nov ;69 (11):966 -8.
© Copyright 2007 – Eastern Association for the Surgery of Trauma 24
62. Leon EL, Metzger A, Tsiotos GG, Schlinkert RT, Sarr MG. Laparoscopic
management of small bowel obstruction: indications and outcome. J Gastrointest
Surg %1998 Mar -Apr;2(2):132 -40.
63. Levard H, Boudet MJ, Msika S et al. Laparoscopic treatment of acute small bowel
obstruction: a multicentre retrospective study. Anz J Surg %2001 Nov ;71 (11):641
-6.
64. Wullstein C, Gross E. Laparoscopic compared with conventional treatment of acute
adhesive small bowel obstruction. Br J Surg %2003 Sep ;90 (9 ):1147 -51.
65. Liauw JJ, Cheah WK. Laparoscopic management of acute small bowel obstruction.
Asian J Surg %2005 Jul ;28 (3):185 -8.
66. Suzuki K, Umehara Y, Kimura T. Elective laparoscopy for small bowel obstruction.
Surg Laparosc Endosc Percutan Tech %2003 Aug ;13(4):254 -6.
67. Tsumura H, Ichikawa T, Murakami Y, Sueda T. Laparoscopic adhesiolysis for
recurrent postoperative small bowel obstruction. Hepatogastroenterology %2004
Jul -Aug ;51 (58 ):1058 -61.
68. Chopra R, Mcvay C, Phillips E, Khalili TM. Laparoscopic lysis of adhesions. Am
Surg %2003 Nov ;69 (11):966 -8.
© Copyright 2007 – Eastern Association for the Surgery of Trauma 25
69. Levard H, Boudet MJ, Msika S et al. Laparoscopic treatment of acute small bowel
obstruction: a multicentre retrospective study. Anz J Surg %2001 Nov ;71 (11):641
-6.
70. Suter M, Zermatten P, Halkic N, Martinet O, Bettschart V. Laparoscopic
management of mechanical small bowel obstruction: are there predictors of success
or failure? Surg Endosc %2000 May ;14(5):478 -83.
71. Leon EL, Metzger A, Tsiotos GG, Schlinkert RT, Sarr MG. Laparoscopic
management of small bowel obstruction: indications and outcome. J Gastrointest
Surg %1998 Mar -Apr;2(2):132 -40.
72. Strickland P, Lourie DJ, Suddleson EA, Blitz JB, Stain SC. Is laparoscopy safe and
effective for treatment of acute small-bowel obstruction? Surg Endosc %1999 Jul
;13(7 ):695 -8.
73. Duepree HJ, Senagore AJ, Delaney CP, Fazio VW. Does means of access affect the
incidence of small bowel obstruction and ventral hernia after bowel resection?
Laparoscopy versus laparotomy. J Am Coll Surg %2003 Aug ;197 (2):177 -81.
74. Sagar PM, MacFie J, Sedman P, May J, Mancey-Jones B, Johnstone D. Intestinal
obstruction promotes gut translocation of bacteria. Dis Colon Rectum %1995 Jun
;38 (6 ):640 -4.
© Copyright 2007 – Eastern Association for the Surgery of Trauma 26
75. Meissner K. Effectiveness of intestinal tube splinting: a prospective observational
study. Dig Surg %2000 ;17(1):49 -56.
76. Meissner K. Small bowel obstruction following extended right hemicolectomy and
subtotal colectomy: assessing the benefit of prophylactic tube splinting. Dig Surg
%2001 ;18 (5):388 -92.
77. Fazio VW, Cohen Z, Fleshman JW et al. Reduction in adhesive small-bowel
obstruction by Seprafilm adhesion barrier after intestinal resection. Dis Colon
Rectum %2006 Jan ;49 (1):1-11.
78. Kudo FA, Nishibe T, Miyazaki K, Murashita T, Nishibe M, Yasuda K. Use of
bioresorbable membrane to prevent postoperative small bowel obstruction in
transabdominal aortic aneurysm surgery. Surg Today %2004;34 (8 ):648 -51.
79. Kudo FA, Nishibe T, Miyazaki K, Murashita T, Nishibe M, Yasuda K. Use of
bioresorbable membrane to prevent postoperative small bowel obstruction in
transabdominal aortic aneurysm surgery. Surg Today %2004;34 (8 ):648 -51.
80. Mohri Y, Uchida K, Araki T et al. Hyaluronic acid-carboxycellulose membrane
(Seprafilm) reduces early postoperative small bowel obstruction in gastrointestinal
surgery. Am Surg %2005 Oct ;71 (10):861 -3.
© Copyright 2007 – Eastern Association for the Surgery of Trauma 27
1 Nauta RJ 2 Seror D
Pr
actic
e M
anag
emen
t Gui
delin
es fo
r M
anag
emen
t of S
mal
l Bow
el O
bstr
uctio
n in
the
Sett
ing
of P
revi
ous A
bdom
inal
Sur
gery
19
91 –
Pre
sent
Firs
t Aut
hor
Yea
r R
efer
ence
Titl
e C
lass
C
oncl
usio
ns
Dia
gnos
is –
Pla
in F
ilm/K
UB
Lapp
as JC
20
01
Abd
omin
al ra
diog
raph
y fin
ding
s in
smal
l-bow
el o
bstru
ctio
n: re
leva
nce
to
triag
e fo
r add
ition
al d
iagn
ostic
imag
ing.
AJR
Am
J R
oent
geno
l. 20
01
Jan;
176(
1):1
67-7
4.
III
(N=8
1; re
trosp
ectiv
e) P
lain
film
s hel
p di
ffer
entia
te lo
w g
rade
fr
om h
igh
grad
e bu
t CT
give
s inc
rem
enta
l and
nee
ded
if pl
ain
film
was
inco
nclu
sive
M
aglin
te D
D
1997
R
elia
bilit
y an
d ro
le o
f pla
in fi
lm ra
diog
raph
y an
d C
T in
the
diag
nosi
s of
smal
l-bow
el o
bstru
ctio
n. A
JR A
m J
Roe
ntge
nol.
1996
Dec
;167
(6):
1451
-5.
II
I Pl
ain
film
s and
CT
have
equ
al se
nsiti
vity
for g
rade
of
obst
ruct
ion.
The
y re
com
men
d pl
ain
film
s ini
tially
on
all
susp
ecte
d SB
O w
ith C
T as
a fo
llow
-up
if ne
eded
for c
linic
al
purp
oses
. D
iagn
osis
-CT
Bog
usev
iciu
s A
2002
Pr
ospe
ctiv
e ra
ndom
ised
tria
l of c
ompu
ter-
aide
d di
agno
sis a
nd c
ontra
st
radi
ogra
phy
in a
cute
smal
l bow
el o
bstru
ctio
n. E
ur J
Sur
g. 2
002;
168(
2):7
8-83
.
I C
ompu
ter p
rogr
am th
at d
iffer
entia
tes b
etw
een
com
plet
e an
d pa
rtial
SB
O w
hen
36 c
linic
al v
aria
bles
, inc
ludi
ng th
e pl
ain
radi
ogra
phic
find
ings
, are
ent
ered
, but
the
time
to d
iagn
osis
w
as o
nly
1 ho
ur w
ith th
e co
mpu
ter p
rogr
am a
nd 1
6 ho
urs
with
con
trast
radi
ogra
phy.
Za
lcm
an M
20
00
Hel
ical
CT
sign
s in
the
diag
nosi
s of i
ntes
tinal
isch
emia
in sm
all-b
owel
ob
stru
ctio
n. A
JR A
m J
Roe
ntge
nol.
2000
Dec
;175
(6):
1601
-7.
II
(N
=144
: ret
rosp
ectiv
e) T
hey
spec
ifica
lly lo
oked
for r
educ
ed
wal
l enh
ance
men
t, w
all t
hick
enin
g, m
esen
teric
flui
d m
esen
teric
ven
ous c
onge
stio
n, a
nd a
scite
s in
orde
r to
dete
rmin
e pr
esen
ce o
f isc
hem
ia.
Stra
ngul
atio
n w
as
pros
pect
ivel
y di
agno
sed
if re
duce
d w
all e
nhan
cem
ent o
r 2 o
f th
e ot
her 4
sign
s wer
e pr
esen
t.
Laza
rus D
E 20
04
Freq
uenc
y an
d re
leva
nce
of th
e "s
mal
l-bow
el fe
ces"
sign
on
CT
in p
atie
nts
with
smal
l-bow
el o
bstru
ctio
n.
AJR
Am J
Roe
ntge
nol.
2004
Nov
;183
(5):
1361
-6.
II
(N=3
4: re
trosp
ectiv
e) T
he fe
ces s
ign
help
ed id
entif
y th
e po
int
of o
bstru
ctio
n an
d w
as m
ore
likel
y in
hig
her d
egre
es o
f ob
stru
ctio
n.
Obu
z F
2003
Th
e ef
ficac
y of
hel
ical
CT
in th
e di
agno
sis o
f sm
all b
owel
obs
truct
ion.
Eu
r J R
adio
l. 20
03 D
ec;4
8(3)
:299
-304
. II
(
N=4
1; P
rosp
ectiv
e) H
elic
al C
T (1
998-
2001
) CT
was
83%
ac
cura
te in
diff
eren
tiatin
g ob
stru
ctio
n vs
non
-obs
truct
ion,
85
% a
ccur
ate
in d
eter
min
ing
caus
e, a
nd 1
00%
acc
urat
e in
de
term
inin
g st
rang
ulat
ion/
isch
emia
. Su
ri S
1999
C
ompa
rativ
e ev
alua
tion
of p
lain
film
s, ul
traso
und
and
CT
in th
e di
agno
sis o
f in
test
inal
obs
truct
ion.
Ac
ta R
adio
l. 19
99 J
ul;4
0(4)
:422
-8.
II
(N=3
2; P
rosp
ectiv
e) S
uspe
cted
SB
O w
ho h
ad p
lain
ra
diog
raph
s, U
S an
d C
T sc
an (1
990-
93).
Pla
in ra
diog
raph
y w
as 7
5% a
ccur
ate,
US
was
84%
acc
urat
e, a
nd C
T w
as 9
4%
accu
rate
at d
eter
min
ing
obst
ruct
ion
vs n
o ob
stru
ctio
n. L
evel
of
obs
truct
ion
60%
, 70%
, and
93%
. C
ause
of o
bstru
ctio
n 7%
, 23
%, a
nd 8
7%.
© C
opyr
ight
200
7 –
East
ern
Ass
ocia
tion
for t
he S
urge
ry o
f Tra
uma
Taou
rel P
G
1995
V
alue
of C
T in
the
diag
nosi
s and
man
agem
ent o
f pat
ient
s with
susp
ecte
d ac
ute
smal
l-bow
el o
bstru
ctio
n. A
JR A
m J
Roe
ntge
nol.
1995
N
ov;1
65(5
):11
87-9
2.
II
(N=5
7; P
rosp
ectiv
e) P
atie
nts w
ith su
spic
ion
of S
BO
(199
1 -
1994
). T
he su
rgeo
n w
as in
terv
iew
ed p
rior t
o th
e C
T sc
an.
In
33 p
ts th
e cl
inic
ian
wan
ted
to d
iffer
entia
te b
etw
een
SBO
or
ileus
and
in 2
4 pt
s the
clin
icia
n w
ante
d to
kno
w th
e ca
use
of
SBO
. C
T co
rrec
tly c
hang
ed th
e di
ffer
entia
tion
betw
een
SBO
&
ileu
s in
21%
of c
ases
. C
T ch
ange
d th
e di
agno
sis (
caus
e) o
f SB
O in
43%
and
cor
rect
ly c
hang
ed p
rese
nce
or a
bsen
ce o
f st
rang
ulat
ion
in 2
3.
Cat
alan
o O
19
97
The
faec
es si
gn. A
CT
findi
ng in
smal
l-bow
el o
bstru
ctio
n.
Radi
olog
e. 1
997
May
;37(
5):4
17-9
.
III
(N=9
4; R
etro
spec
tive)
Fec
es si
gn w
as o
nly
pres
ent i
n 7%
of
case
s, on
ly 1
of w
hich
had
stra
ngul
atio
n.
Cho
u C
K
2000
D
iffer
entia
tion
of o
bstru
ctiv
e fr
om n
on-o
bstru
ctiv
e sm
all b
owel
dila
tatio
n on
C
T.
Eur J
Rad
iol.
2000
Sep
;35(
3):2
13-2
0.
III
(N=1
46; R
etro
spec
tive)
Eva
luat
ed 4
crit
eria
: co
ntin
uity
of
prox
imal
SB
, tra
nsiti
on z
one,
intra
lum
inal
flui
d, &
col
onic
co
nten
ts.
The
prob
abili
ty o
f tru
e ob
stru
ctio
n w
as c
alcu
late
d fo
r eac
h si
gn.
Con
tinui
ty 6
9%, T
rans
ition
zon
e ab
rupt
80%
, hi
gh a
mou
nt o
f SB
flui
d 79
%, m
inim
al c
olon
ic c
onte
nts 9
0%.
D
anes
hman
d S
1999
Th
e ut
ility
and
relia
bilit
y of
com
pute
d to
mog
raph
y sc
an in
the
diag
nosi
s of
smal
l bow
el o
bstru
ctio
n.
Am S
urg.
199
9 O
ct;6
5(10
):92
2-6.
III
Ret
rosp
ectiv
e st
udy
of 1
03 p
ts (1
997-
8) w
ith su
spec
ted
SBO
. C
ompa
rison
of p
lain
radi
ogra
phs w
ith C
T in
det
erm
inin
g pa
rtial
vs c
ompl
ete
SBO
and
in d
eter
min
ing
caus
e. P
lain
fil
ms w
ere
75%
sens
itive
and
53%
spec
ific
for p
artia
l vs
com
plet
e. C
T w
as 9
2% se
nsiti
ve a
nd 7
1% sp
ecifi
c. C
ause
w
as c
orre
ctly
det
erm
ined
or i
nfer
red
to b
e ad
hesi
ons b
y C
T in
91
% o
f cas
es.
Gol
lub
MJ
2006
D
oes t
he C
T w
hirl
sign
real
ly p
redi
ct sm
all b
owel
vol
vulu
s?: E
xper
ienc
e in
an
onc
olog
ic p
opul
atio
n.
J C
ompu
t Ass
ist T
omog
r. 20
06 J
an-F
eb;3
0(1)
:25-
32.
III
Ret
rosp
ectiv
e an
alys
is o
f 120
0+ C
T sc
ans o
f pts
with
su
spec
ted
SBO
at a
can
cer c
ente
r. W
hirl
sign
was
foun
d in
33
pts b
y a
seni
or ra
diol
ogis
t and
14
pts b
y a
seni
or ra
diol
ogy
resi
dent
. Th
e w
hirl
sign
had
a se
nsiti
vity
of 6
4% fo
r vol
vulu
s by
the
seni
or ra
diol
ogis
t and
muc
h le
ss b
y th
e re
side
nt.
They
co
nclu
ded
that
the
whi
rl si
gn is
a re
lativ
ely
poor
pre
dict
or o
f vo
lvul
us in
this
pop
ulat
ion
Ha
HK
19
97
Diff
eren
tiatio
n of
sim
ple
and
stra
ngul
ated
smal
l-bow
el o
bstru
ctio
ns:
usef
ulne
ss o
f kno
wn
CT
crite
ria.
Radi
olog
y. 1
997
Aug;
204(
2):5
07-1
2.
III
(N=8
4; R
etro
spec
tive)
Pat
ient
s with
kno
wn
outc
omes
, sim
ple
vs st
rang
ulat
ed S
BO
(199
1-19
96).
The
y id
entif
ied
6 C
T fin
ding
s as b
est a
t det
erm
inin
g st
rang
ulat
ion:
redu
ced
wal
l en
hanc
emen
t, se
rrat
ed b
eak,
asc
ites,
and
unus
ual c
ours
e of
m
esen
teric
vas
cula
ture
, mes
ente
ric h
azin
ess,
and
mes
ente
ric
veno
us e
ngor
gem
ent.
Usi
ng th
ese
sign
s the
y w
ere
able
to
find
85%
of s
trang
ulat
ions
Ja
ffe
TA
2006
Sm
all-b
owel
obs
truct
ion:
cor
onal
refo
rmat
ions
from
isot
ropi
c vo
xels
at 1
6-II
I R
etro
spec
tive
anal
ysis
of a
dded
val
ue o
f cor
onal
refo
rmat
ions
© C
opyr
ight
200
7 –
East
ern
Ass
ocia
tion
for t
he S
urge
ry o
f Tra
uma
sect
ion
mul
ti-de
tect
or ro
w C
T.
Radi
olog
y. 2
006
Jan;
238(
1):1
35-4
2. E
pub
2005
Nov
17.
(200
3-4)
in 1
00 p
ts w
ith su
spec
ted
SBO
. C
oron
al im
ages
ad
ded
conf
iden
ce to
the
thre
e re
ader
’s d
iagn
ostic
acc
urac
y of
ob
stru
ctio
n vs
no
obst
ruct
ion.
K
im JH
20
04
Use
fuln
ess o
f kno
wn
com
pute
d to
mog
raph
y an
d cl
inic
al c
riter
ia fo
r di
agno
sing
stra
ngul
atio
n in
smal
l-bow
el o
bstru
ctio
n: a
naly
sis o
f tru
e an
d fa
lse
inte
rpre
tatio
n gr
oups
in c
ompu
ted
tom
ogra
phy.
W
orld
J S
urg.
200
4 Ja
n;28
(1):
63-8
.
III
Ret
rosp
ectiv
e st
udy
of 1
46 C
Ts lo
okin
g fo
r stra
ngul
atio
n vs
no
stra
ngul
atio
n (1
992-
98).
Thr
ee ra
diol
ogis
ts w
ere
72%
- 82
% a
ccur
ate
in d
eter
min
ing
stra
ngul
atio
n. T
he fo
ur c
linic
al
crite
ria, f
ever
, ten
dern
ess,
tach
ycar
dia,
leuk
ocyt
osis
, with
out
CT
findi
ngs w
ere
equa
lly a
ccur
ate,
how
ever
!
Mak
ita O
19
99
CT
diff
eren
tiatio
n be
twee
n ne
crot
ic a
nd n
onne
crot
ic sm
all b
owel
in c
lose
d lo
op a
nd st
rang
ulat
ing
obst
ruct
ion.
Ab
dom
Imag
ing.
199
9 M
ar-A
pr;2
4(2)
:120
-4.
III
Ret
rosp
ectiv
e an
alys
is o
f CT
findi
ngs d
iffer
entia
ting
necr
osis
fr
om n
on-n
ecro
sis i
n 25
pts
with
pro
ven
stra
ngul
atio
n.
Find
ings
pre
dict
ive
of n
ecro
sis w
ere:
asc
ites,
vasc
ular
di
lata
tion,
mes
ente
ric a
ttenu
atio
n, a
nd ra
dial
dis
tribu
tion,
but
m
esen
teric
atte
nuat
ion
was
mos
t pre
dict
ive.
D
iagn
osis
–M
RI
Bea
ll D
P 20
02
Imag
ing
bow
el o
bstru
ctio
n: a
com
paris
on b
etw
een
fast
mag
netic
reso
nanc
e im
agin
g an
d he
lical
com
pute
d to
mog
raph
y.
Clin
Rad
iol.
2002
Aug
;57(
8):7
19-2
4.
II
Pros
pect
ive
com
paris
on o
f hel
ical
CT
(ora
l/IV
con
trast
) with
ul
trafa
st H
AST
E M
RI i
n 44
pts
with
susp
ecte
d SB
O (1
997
-19
98).
Fin
ding
s: C
T (7
1%, S
ensi
tivity
; 71%
Spe
cific
ity) M
R
(95%
sens
itivi
ty; 1
00%
Spe
cific
ity).
in d
iffer
entia
ting
obst
ruct
ion
vs n
o ob
stru
ctio
n. N
o m
entio
n of
diff
eren
tiatin
g hi
gh-g
rade
vs l
ow g
rade
obs
truct
ion.
Lim
itatio
ns o
f MR
I in
clud
e la
ck o
f ava
ilabi
lity
afte
r hou
rs, p
oor d
efin
ition
of
caus
e of
obs
truct
ion,
and
poo
r vis
ualiz
atio
n of
col
onic
ob
stru
ctio
ns.
K
im JH
20
00
Use
fuln
ess o
f MR
imag
ing
for d
isea
ses o
f the
smal
l int
estin
e: c
ompa
rison
w
ith C
T.
Kor
ean
J Ra
diol
. 200
0 Ja
n-M
ar;1
(1):
43-5
0.
III
Pros
pect
ive
com
paris
on o
f hel
ical
CT
(ora
l/IV
con
trast
) with
H
AST
E M
RI i
n 34
pts
with
a v
arie
ty o
f SB
dis
ease
s (19
96 -
1999
). 1
5 pt
s had
susp
ecte
d SB
O.
MR
I and
CT
wer
e bo
th
100%
acc
urat
e in
dia
gnos
ing
or e
xclu
ding
SB
O.
MR
I was
be
tter a
t det
erm
inin
g th
e pr
ecis
e ca
use
of o
bstru
ctio
n (7
3% v
60
%).
MR
I poo
r at l
ooki
ng a
t om
entu
m.
Le
e JK
19
98
MR
imag
ing
of th
e sm
all b
owel
usi
ng th
e H
AST
E se
quen
ce.
AJR
Am J
Roe
ntge
nol.
1998
Jun
;170
(6):
1457
-63.
II
I M
R w
ith H
AST
E se
quen
ce c
an d
istin
guis
h be
twee
n no
rmal
sm
all b
owel
and
abn
orm
al sm
all b
owel
. Mot
ion
did
not a
ffec
t th
ese
stud
ies
Reg
an F
19
98
Fast
MR
imag
ing
and
the
dete
ctio
n of
smal
l-bow
el o
bstru
ctio
n.
AJR
Am J
Roe
ntge
nol.
1998
Jun
;170
(6):
1465
-9.
II
I H
AST
E M
R c
an b
e hi
ghly
acc
urat
e in
dia
gnos
ing
SBO
and
id
entif
ying
the
leve
l of o
bstru
ctio
n 26
/29
patie
nts w
ith S
BO
w
ere
said
to h
ave
been
cor
rect
ly id
entif
ied
by H
AST
E M
R
(sen
sitiv
ity 9
0%, s
peci
ficity
86%
) and
73%
had
the
corr
ect
leve
l of o
bstru
ctio
n id
entif
ied.
Lim
itatio
ns id
entif
ied
incl
ude:
© C
opyr
ight
200
7 –
East
ern
Ass
ocia
tion
for t
he S
urge
ry o
f Tra
uma
abse
nce
of d
ilatio
n in
situ
atio
ns w
here
pro
long
ed N
G su
ctio
n ha
s bee
n em
ploy
ed, M
RI i
s not
goo
d at
iden
tifyi
ng m
asse
s in
clud
ing
mal
igna
ncie
s, di
d no
t sho
w in
flam
mat
ion
as g
ood
as C
T, a
nd d
oes n
ot sh
ow v
iabi
lity.
Dia
gnos
is –
Ultr
asou
nd
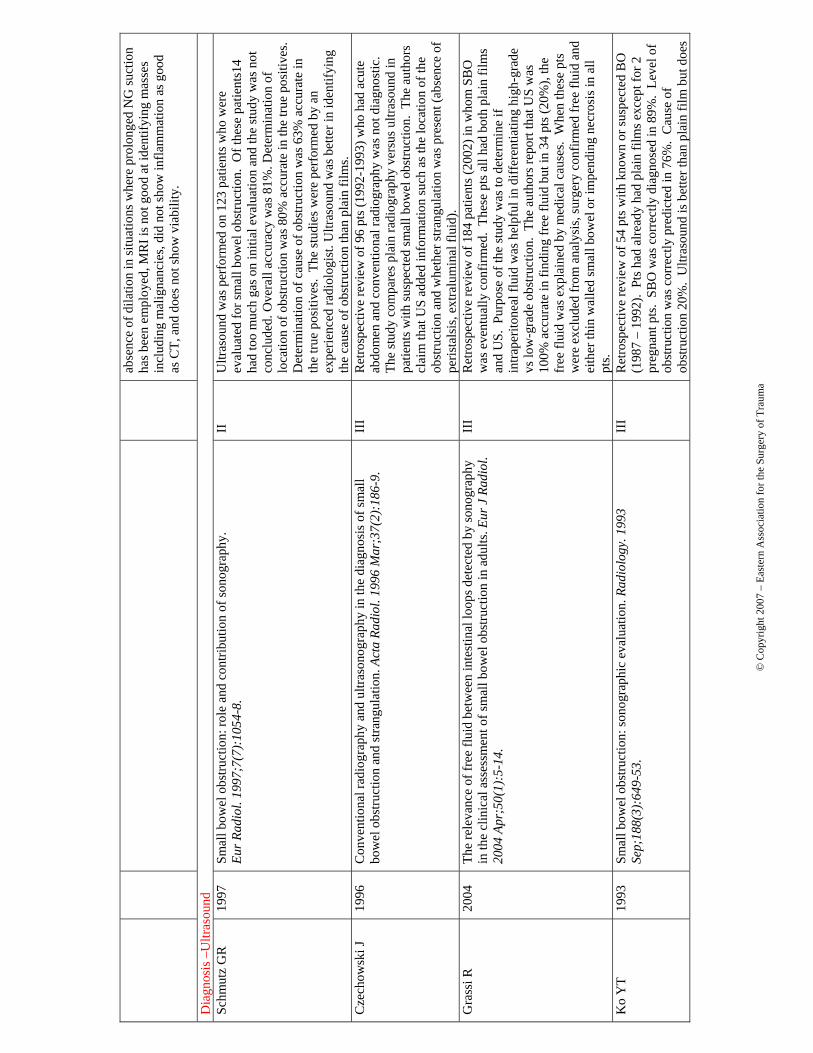
Schm
utz
GR
19
97
Smal
l bow
el o
bstru
ctio
n: ro
le a
nd c
ontri
butio
n of
sono
grap
hy.
Eur R
adio
l. 19
97;7
(7):
1054
-8.
II
U
ltras
ound
was
per
form
ed o
n 12
3 pa
tient
s who
wer
e ev
alua
ted
for s
mal
l bow
el o
bstru
ctio
n. O
f the
se p
atie
nts1
4 ha
d to
o m
uch
gas o
n in
itial
eva
luat
ion
and
the
stud
y w
as n
ot
conc
lude
d. O
vera
ll ac
cura
cy w
as 8
1%. D
eter
min
atio
n of
lo
catio
n of
obs
truct
ion
was
80%
acc
urat
e in
the
true
posi
tives
. D
eter
min
atio
n of
cau
se o
f obs
truct
ion
was
63%
acc
urat
e in
th
e tru
e po
sitiv
es.
The
stud
ies w
ere
perf
orm
ed b
y an
ex
perie
nced
radi
olog
ist.
Ultr
asou
nd w
as b
ette
r in
iden
tifyi
ng
the
caus
e of
obs
truct
ion
than
pla
in fi
lms.
Cze
chow
ski J
1996
C
onve
ntio
nal r
adio
grap
hy a
nd u
ltras
onog
raph
y in
the
diag
nosi
s of s
mal
l bo
wel
obs
truct
ion
and
stra
ngul
atio
n. A
cta
Radi
ol. 1
996
Mar
;37(
2):1
86-9
. II
I R
etro
spec
tive
revi
ew o
f 96
pts (
1992
-199
3) w
ho h
ad a
cute
ab
dom
en a
nd c
onve
ntio
nal r
adio
grap
hy w
as n
ot d
iagn
ostic
. Th
e st
udy
com
pare
s pla
in ra
diog
raph
y ve
rsus
ultr
asou
nd in
pa
tient
s with
susp
ecte
d sm
all b
owel
obs
truct
ion.
The
aut
hors
cl
aim
that
US
adde
d in
form
atio
n su
ch a
s the
loca
tion
of th
e ob
stru
ctio
n an
d w
heth
er st
rang
ulat
ion
was
pre
sent
(abs
ence
of
peris
tals
is, e
xtra
lum
inal
flui
d).
Gra
ssi R
20
04
The
rele
vanc
e of
free
flui
d be
twee
n in
test
inal
loop
s det
ecte
d by
sono
grap
hy
in th
e cl
inic
al a
sses
smen
t of s
mal
l bow
el o
bstru
ctio
n in
adu
lts. E
ur J
Rad
iol.
2004
Apr
;50(
1):5
-14.
III
Ret
rosp
ectiv
e re
view
of 1
84 p
atie
nts (
2002
) in
who
m S
BO
w
as e
vent
ually
con
firm
ed.
Thes
e pt
s all
had
both
pla
in fi
lms
and
US.
Pur
pose
of t
he st
udy
was
to d
eter
min
e if
intra
perit
onea
l flu
id w
as h
elpf
ul in
diff
eren
tiatin
g hi
gh-g
rade
vs
low
-gra
de o
bstru
ctio
n. T
he a
utho
rs re
port
that
US
was
10
0% a
ccur
ate
in fi
ndin
g fr
ee fl
uid
but i
n 34
pts
(20%
), th
e fr
ee fl
uid
was
exp
lain
ed b
y m
edic
al c
ause
s. W
hen
thes
e pt
s w
ere
excl
uded
from
ana
lysi
s, su
rger
y co
nfirm
ed fr
ee fl
uid
and
eith
er th
in w
alle
d sm
all b
owel
or i
mpe
ndin
g ne
cros
is in
all
pts.
K
o Y
T 19
93
Smal
l bow
el o
bstru
ctio
n: so
nogr
aphi
c ev
alua
tion.
Rad
iolo
gy. 1
993
Sep;
188(
3):6
49-5
3.
II
I R
etro
spec
tive
revi
ew o
f 54
pts w
ith k
now
n or
susp
ecte
d B
O
(198
7 –
1992
). P
ts h
ad a
lread
y ha
d pl
ain
film
s exc
ept f
or 2
pr
egna
nt p
ts.
SBO
was
cor
rect
ly d
iagn
osed
in 8
9%.
Leve
l of
obst
ruct
ion
was
cor
rect
ly p
redi
cted
in 7
6%.
Cau
se o
f ob
stru
ctio
n 20
%.
Ultr
asou
nd is
bet
ter t
han
plai
n fil
m b
ut d
oes
© C
opyr
ight
200
7 –
East
ern
Ass
ocia
tion
for t
he S
urge
ry o
f Tra
uma
not s
how
stra
ngul
atio
n w
ell.
Dia
gnos
is –
Ente
rocl
ysis
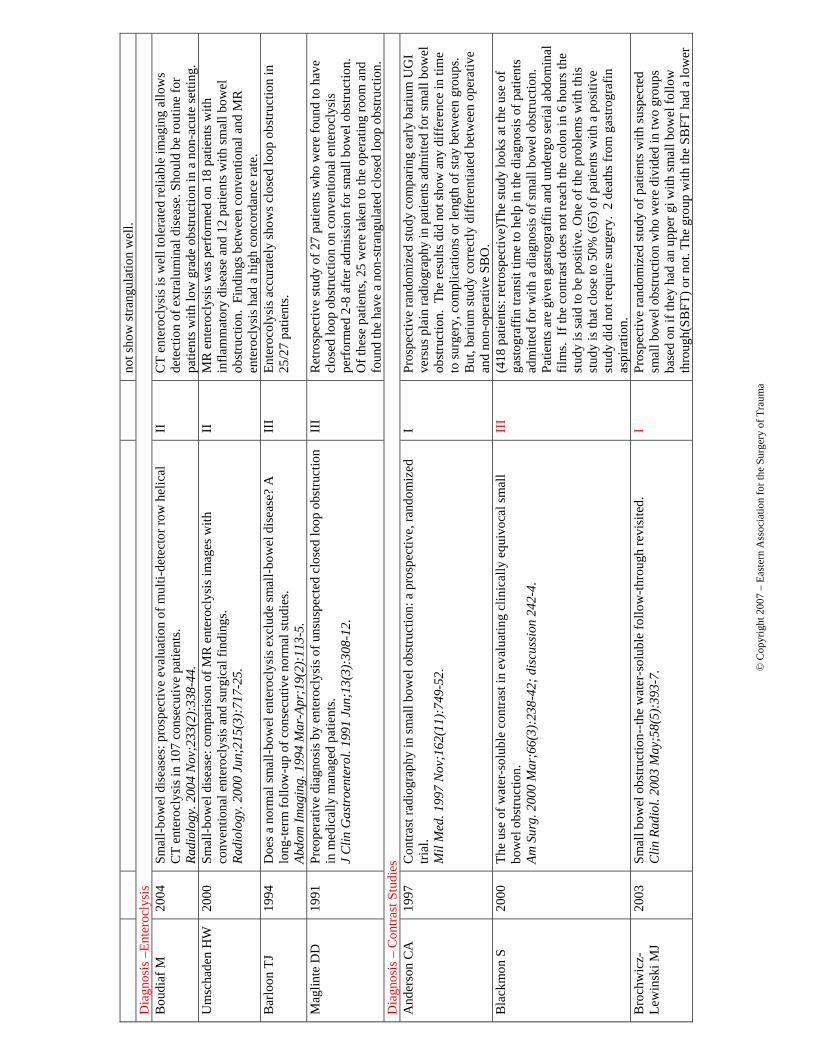
B
oudi
af M
20
04
Smal
l-bow
el d
isea
ses:
pro
spec
tive
eval
uatio
n of
mul
ti-de
tect
or ro
w h
elic
al
CT
ente
rocl
ysis
in 1
07 c
onse
cutiv
e pa
tient
s. Ra
diol
ogy.
200
4 N
ov;2
33(2
):33
8-44
.
II
CT
ente
rocl
ysis
is w
ell t
oler
ated
relia
ble
imag
ing
allo
ws
dete
ctio
n of
ext
ralu
min
al d
isea
se. S
houl
d be
rout
ine
for
patie
nts w
ith lo
w g
rade
obs
truct
ion
in a
non
-acu
te se
tting
. U
msc
hade
n H
W
2000
Sm
all-b
owel
dis
ease
: com
paris
on o
f MR
ent
eroc
lysi
s im
ages
with
co
nven
tiona
l ent
eroc
lysi
s and
surg
ical
find
ings
. Ra
diol
ogy.
200
0 Ju
n;21
5(3)
:717
-25.
II
MR
ent
eroc
lysi
s was
per
form
ed o
n 18
pat
ient
s with
in
flam
mat
ory
dise
ase
and
12 p
atie
nts w
ith sm
all b
owel
ob
stru
ctio
n. F
indi
ngs b
etw
een
conv
entio
nal a
nd M
R
ente
rocl
ysis
had
a h
igh
conc
orda
nce
rate
. B
arlo
on T
J
1994
D
oes a
nor
mal
smal
l-bow
el e
nter
ocly
sis e
xclu
de sm
all-b
owel
dis
ease
? A
lo
ng-te
rm fo
llow
-up
of c
onse
cutiv
e no
rmal
stud
ies.
Abdo
m Im
agin
g. 1
994
Mar
-Apr
;19(
2):1
13-5
.
III
Ente
roco
lysi
s acc
urat
ely
show
s clo
sed
loop
obs
truct
ion
in
25/2
7 pa
tient
s.
Mag
linte
DD
1991
Pr
eope
rativ
e di
agno
sis b
y en
tero
clys
is o
f uns
uspe
cted
clo
sed
loop
obs
truct
ion
in m
edic
ally
man
aged
pat
ient
s. J
Clin
Gas
troe
nter
ol. 1
991
Jun;
13(3
):30
8-12
.
III
Ret
rosp
ectiv
e st
udy
of 2
7 pa
tient
s who
wer
e fo
und
to h
ave
clos
ed lo
op o
bstru
ctio
n on
con
vent
iona
l ent
eroc
lysi
s pe
rfor
med
2-8
afte
r adm
issi
on fo
r sm
all b
owel
obs
truct
ion.
O
f the
se p
atie
nts,
25 w
ere
take
n to
the
oper
atin
g ro
om a
nd
foun
d th
e ha
ve a
non
-stra
ngul
ated
clo
sed
loop
obs
truct
ion.
D
iagn
osis
– C
ontra
st S
tudi
es
And
erso
n C
A
1997
C
ontra
st ra
diog
raph
y in
smal
l bow
el o
bstru
ctio
n: a
pro
spec
tive,
rand
omiz
ed
trial
. M
il M
ed. 1
997
Nov
;162
(11)
:749
-52.
I Pr
ospe
ctiv
e ra
ndom
ized
stud
y co
mpa
ring
early
bar
ium
UG
I ve
rsus
pla
in ra
diog
raph
y in
pat
ient
s adm
itted
for s
mal
l bow
el
obst
ruct
ion.
The
resu
lts d
id n
ot sh
ow a
ny d
iffer
ence
in ti
me
to su
rger
y, c
ompl
icat
ions
or l
engt
h of
stay
bet
wee
n gr
oups
. B
ut, b
ariu
m st
udy
corr
ectly
diff
eren
tiate
d be
twee
n op
erat
ive
and
non-
oper
ativ
e SB
O.
Bla
ckm
on S
20
00
The
use
of w
ater
-sol
uble
con
trast
in e
valu
atin
g cl
inic
ally
equ
ivoc
al sm
all
bow
el o
bstru
ctio
n.
Am S
urg.
200
0 M
ar;6
6(3)
:238
-42;
dis
cuss
ion
242-
4.
III
(418
pat
ient
s: re
trosp
ectiv
e)Th
e st
udy
look
s at t
he u
se o
f ga
stog
raff
in tr
ansi
t tim
e to
hel
p in
the
diag
nosi
s of p
atie
nts
adm
itted
for w
ith a
dia
gnos
is o
f sm
all b
owel
obs
truct
ion.
Pa
tient
s are
giv
en g
astro
graf
fin a
nd u
nder
go se
rial a
bdom
inal
fil
ms.
If th
e co
ntra
st d
oes n
ot re
ach
the
colo
n in
6 h
ours
the
stud
y is
said
to b
e po
sitiv
e. O
ne o
f the
pro
blem
s with
this
st
udy
is th
at c
lose
to 5
0% (6
5) o
f pat
ient
s with
a p
ositi
ve
stud
y di
d no
t req
uire
surg
ery.
2 d
eath
s fro
m g
astro
graf
in
aspi
ratio
n.
Bro
chw
icz-
Lew
insk
i MJ
2003
Sm
all b
owel
obs
truct
ion-
-the
wat
er-s
olub
le fo
llow
-thro
ugh
revi
site
d.
Clin
Rad
iol.
2003
May
;58(
5):3
93-7
. I
Pros
pect
ive
rand
omiz
ed st
udy
of p
atie
nts w
ith su
spec
ted
smal
l bow
el o
bstru
ctio
n w
ho w
ere
divi
ded
in tw
o gr
oups
ba
sed
on if
they
had
an
uppe
r gi w
ith sm
all b
owel
follo
w
thro
ugh(
SBFT
) or n
ot. T
he g
roup
with
the
SBFT
had
a lo
wer
© C
opyr
ight
200
7 –
East
ern
Ass
ocia
tion
for t
he S
urge
ry o
f Tra
uma
inci
denc
e of
ope
ratio
n bu
t thi
s diff
eren
ce d
id n
ot a
chie
ve
stat
istic
al d
iffer
ence
. The
leng
th o
f sta
y w
as n
ot a
ffec
ted
by
the
SBFT
. The
pat
ient
s wer
e ra
ndom
ized
and
the
surg
eons
ch
ange
d th
eir c
linic
al m
anag
emen
t pla
n ba
sed
on th
e re
sults
.
M
akan
juol
a D
. 19
98
Com
pute
d to
mog
raph
y co
mpa
red
with
smal
l bow
el e
nem
a in
clin
ical
ly
equi
voca
l int
estin
al o
bstru
ctio
n.
Clin
Rad
iol.
1998
Mar
;53(
3):2
03-8
.
III
49 p
ts h
ad b
oth
CT
and
‘sm
all b
owel
ene
ma’
. 43/
49 p
ts h
ad
defin
ite in
test
inal
obs
truct
ion
(42
per s
urge
ry).
SBE
was
mor
e se
nsiti
ve in
det
ectin
g B
owel
obs
truct
ion
than
CT
(100
% v
s 83
%).
The
7 m
isse
d by
CT
had
shor
t seg
men
t ste
nosi
s. C
oncl
usio
n: In
clin
ical
ly su
spic
ious
cas
es o
f obs
truct
ion
whe
re C
T is
neg
, use
SB
E Sa
ndik
ciog
lu
TG
1994
C
ontra
st ra
diog
raph
y in
smal
l bow
el o
bstru
ctio
n. A
rand
omiz
ed tr
ial o
f ba
rium
sulfa
te a
nd a
non
ioni
c lo
w-o
smol
ar c
ontra
st m
ediu
m.
Acta
Rad
iol.
1994
Jan
;35(
1):6
2-4.
I N
onio
nic
low
osm
olar
wei
ght c
ontra
st is
an
alte
rnat
ive
to
bariu
m fo
r con
trast
stud
ies t
o ev
alua
te fo
r SB
O.
C
hung
CC
19
96
A p
rosp
ectiv
e st
udy
on th
e us
e of
wat
er-s
olub
le c
ontra
st fo
llow
-thro
ugh
radi
olog
y in
the
man
agem
ent o
f sm
all b
owel
obs
truct
ion.
Au
st N
Z J
Sur
g. 1
996
Sep;
66(9
):59
8-60
1.
II
Safe
pro
cedu
re, e
arly
surg
ery
shou
ld o
ccur
if p
atie
nts h
ave
“sig
nific
ant o
bstru
ctio
n” (c
ontra
st d
oesn
’t re
ach
cecu
m in
4
hour
s) a
nd a
4 h
our c
utof
f for
con
trast
reac
hing
the
cecu
m in
pr
edic
tive
of o
utco
me
for S
BO
in th
ose
with
his
tory
of
surg
ery.
Jo
yce
WP
19
92
The
valu
e of
wat
er-s
olub
le c
ontra
st ra
diol
ogy
in th
e m
anag
emen
t of a
cute
sm
all b
owel
obs
truct
ion.
An
n R
Col
l Sur
g En
gl. 1
992
Nov
;74(
6):4
22-5
.
II
Wat
er-s
olub
le c
ontra
st st
udy
is sa
fe a
nd e
asy
to u
se a
nd
diag
nost
ic st
udy
of c
hoic
e fo
r sus
pect
ed S
BO
. Nor
mal
co
ntra
st st
udy
can
rule
out
ope
rativ
e SB
O.
Peck
JJ
1999
Th
e ro
le o
f com
pute
d to
mog
raph
y w
ith c
ontra
st a
nd sm
all b
owel
follo
w-
thro
ugh
in m
anag
emen
t of s
mal
l bow
el o
bstru
ctio
n.
Am J
Sur
g. 1
999
May
;177
(5):
375-
8.
III
With
equ
ivoc
al fi
ndin
gs o
f SB
O fi
rst C
T an
d th
en S
BFT
sh
ould
be
used
. The
com
bine
d se
nsiti
vity
and
spec
ifici
ty a
re
95%
and
86%
resp
ectiv
ely,
hig
her t
han
thos
e of
eac
h al
one.
Enoc
hsso
n L
2001
C
ontra
st ra
diog
raph
y in
smal
l int
estin
al o
bstru
ctio
n, a
val
uabl
e di
agno
stic
to
ol?
Eur J
Sur
g. 2
001
Feb;
167(
2):1
20-4
.
III
The
outc
ome
of o
ral c
ontra
st st
udie
s can
be
pred
icte
d by
pla
in
radi
ogra
phs.
Con
trast
stud
ies a
re sa
fe a
nd m
ay b
e th
erap
eutic
.
Dix
on P
M
19
93
The
smal
l bow
el e
nem
a: a
ten
year
revi
ew.
Clin
Rad
iol.
1993
Jan
;47(
1):4
6-8.
II
I R
outin
e us
e of
smal
l bow
el e
nem
a in
eva
luat
ion
of p
atie
nts
with
susp
ecte
d sm
all b
owel
pat
holo
gy d
emon
stra
tes a
ver
y hi
gh se
nsiti
vity
(93.
1%) a
nd sp
ecifi
city
(96.
9%) a
nd
obst
ruct
ion
had
a se
nsiti
vity
of 9
8%.
Con
serv
ativ
e M
anag
emen
t – G
ener
al C
onsi
dera
tions
C
onse
rvat
ive
Man
agem
ent –
Clin
ical
Indi
cato
rs/T
ime
Perio
d M
iller
G
2000
N
atur
al h
isto
ry o
f pat
ient
s with
adh
esiv
e sm
all b
owel
obs
truct
ion.
Br
J S
urg.
200
0 Se
p;87
(9):
1240
-7.
II
I Pa
tient
s are
nev
er fr
ee o
f ris
k fo
r pos
t-op
obs 2
nd to
adh
esio
ns
(14%
pre
sent
>20
yrs
pos
t-op)
. R
ate
of re
curr
ence
was
33%
© C
opyr
ight
200
7 –
East
ern
Ass
ocia
tion
for t
he S
urge
ry o
f Tra
uma
over
all (
32%
for o
pera
tion,
34%
(NS)
for c
ons.
Mgm
t), e
ach
recu
rren
ce ra
ised
risk
of f
utur
e re
curr
ence
. C
olor
ecta
l pr
oced
ures
wer
e m
ore
likel
y to
resu
lt in
mat
ted
adhe
sion
s v.
sing
le b
ands
and
resu
lt in
mor
e re
adm
its.
Rec
urre
nce
rate
s b/
w o
p an
d no
n-op
wer
e si
mila
r.
Nau
ta R
J 20
05
Adv
ance
d ab
dom
inal
imag
ing
is n
ot re
quire
d to
exc
lude
stra
ngul
atio
n if
com
plet
e sm
all b
owel
obs
truct
ions
und
ergo
pro
mpt
lapa
roto
my.
J
Am C
oll S
urg.
200
5 Ju
n;20
0(6)
:904
-11.
III
Pape
r val
idat
es th
at c
ompl
ete
SBO
war
rant
s no
addi
tiona
l im
agin
g ot
her t
han
plai
n fil
ms.
71%
of P
SBO
by
plai
n fil
m
with
out p
erito
nitis
reso
lved
with
con
serv
ativ
e m
anag
emen
t.
In p
atie
nts w
ith c
ompl
ete
SBO
, the
re w
as a
ver
y hi
gh ra
te o
f bo
wel
rese
ctio
n (3
1%).
This
sugg
ests
that
a c
ompl
ete
SBO
is
a su
rgic
al d
isea
se.
Sero
r D
19
93
How
con
serv
ativ
ely
can
post
oper
ativ
e sm
all b
owel
obs
truct
ion
be tr
eate
d?
Am J
Sur
g. 1
993
Jan;
165(
1):1
21-5
; dis
cuss
ion
125-
6.
III
73%
resp
onse
to c
onse
rvat
ive
tx in
all
SBO
(Com
plet
e an
d Pa
rtial
). N
o di
ffer
ence
in W
BC
, fev
er, p
ulse
in th
ose
who
re
quire
d su
rger
y. N
o w
orse
out
com
e in
thos
e w
atch
ed o
ver 5
da
ys B
UT
no o
ne th
at h
adn’
t got
ten
bette
r by
5 da
ys g
ot b
ette
r w
/o su
rger
y. W
eak
supp
ort o
f con
clus
ions
.
Will
iam
s SB
20
05
Smal
l bow
el o
bstru
ctio
n: c
onse
rvat
ive
vs. s
urgi
cal m
anag
emen
t. D
is C
olon
Rec
tum
. 200
5 Ju
n;48
(6):
1140
-6.
III
Inci
denc
e of
recu
rren
t SB
O is
hig
her i
n co
nser
vativ
ely
man
aged
pts
than
in o
pera
tivel
y m
anag
ed p
ts (4
0.5%
v.
26.8
%).
Tim
e to
recu
rren
ce in
con
serv
ativ
e m
anag
ed p
atie
nts
was
shor
ter (
153
v. 4
11 d
ays)
Mill
er G
20
02
Rea
dmis
sion
for s
mal
l-bow
el o
bstru
ctio
n in
the
early
pos
tope
rativ
e pe
riod:
et
iolo
gy a
nd o
utco
me.
C
an J
Sur
g. 2
002
Aug;
45(4
):25
5-8.
III
Def
ined
ear
ly p
ost-o
p bo
wel
obs
truct
ion
as w
ithin
50
days
be
caus
e ha
d bi
g gr
oup
who
pre
sent
ed b
/w 3
5-50
day
s. M
ost
freq
uent
pro
cedu
re w
as a
smal
l bow
el o
pera
tion
for S
BO
. 23
% re
quire
d op
erat
ion.
3.3
% st
rang
ulat
ion.
Sug
gest
s non
-op
erat
ive
man
agem
ent o
f pos
t-op
obst
ruct
ion.
Sh
ih S
C
2003
A
dhes
ive
smal
l bow
el o
bstru
ctio
n: h
ow lo
ng c
an p
atie
nts t
oler
ate
cons
erva
tive
treat
men
t?
Wor
ld J
Gas
troe
nter
ol. 2
003
Mar
;9(3
):60
3-5.
III
Pape
r rea
lly su
gges
ts if
you
wai
t too
long
, you
will
hav
e co
mpl
icat
ions
.
Feva
ng B
T 20
02
Early
ope
ratio
n or
con
serv
ativ
e m
anag
emen
t of p
atie
nts w
ith sm
all b
owel
ob
stru
ctio
n?
Eur J
Sur
g. 2
002;
168(
8-9)
:475
-81.
II
Sign
ifica
nt d
iffer
ence
in st
rang
ulat
ion
betw
een
early
and
late
op
erat
ion;
sugg
ests
surg
eons
can
cho
ose
whi
ch p
atie
nts n
eed
imm
edia
te su
rger
y ba
sed
on c
linic
al e
valu
atio
n. O
pera
te fo
r co
ntin
uous
pai
n, fe
ver,
tach
ycar
dia,
per
itoni
tis, l
euko
cyto
sis,
met
aci
dosi
s
Rya
n M
D
2004
A
dhes
iona
l sm
all b
owel
obs
truct
ion
afte
r col
orec
tal s
urge
ry.
III
The
3 ye
ar ra
te fo
r SB
O fo
llow
ing
a co
lore
ctal
pro
cedu
re is
© C
opyr
ight
200
7 –
East
ern
Ass
ocia
tion
for t
he S
urge
ry o
f Tra
uma
ANZ
J Su
rg. 2
004
Nov
;74(
11):
1010
-2.
3.
6%. 4
8% re
quire
d O
R o
n fir
st a
dmis
sion
for S
BO
, onl
y 1
for s
trang
ulat
ion.
Con
serv
ativ
e M
anag
emen
t – A
djun
cts
Ass
alia
A
19
94
Ther
apeu
tic e
ffec
t of o
ral G
astro
graf
in in
adh
esiv
e, p
artia
l sm
all-b
owel
ob
stru
ctio
n: a
pro
spec
tive
rand
omiz
ed tr
ial.
Surg
ery.
199
4 Ap
r;11
5(4)
:433
-7.
I 10
0 cc
of G
G sp
ed re
turn
of b
owel
func
tion
(tim
e to
firs
t st
ool)
from
23.
4h to
6.2
hrs
. G
G d
ecre
ased
LO
S fr
om 4
.4d
to
2.2d
. Tr
end
to im
prov
emen
t in
cons
erva
tive
mgm
t but
not
st
at si
g (2
1% c
ontro
l v. 1
0% G
G P
=0.5
2).
No
GG
co
mpl
icat
ions
Bio
ndo
S 20
03
Ran
dom
ized
clin
ical
stud
y of
Gas
trogr
afin
adm
inis
tratio
n in
pat
ient
s with
ad
hesi
ve sm
all b
owel
obs
truct
ion.
Br
J S
urg.
200
3 M
ay;9
0(5)
:542
-6.
I A
ll pa
tient
s who
pas
sed
Gas
trogr
afin
to th
e co
lon
w/in
24
hour
s tol
erat
ed e
arly
feed
ing
and
did
not r
equi
re o
pera
tion.
Th
ey o
pera
ted
on e
very
pat
ient
who
did
not
pas
s GG
to th
e co
lon
in 2
4 hr
s with
no
furth
er tr
ial o
f rx
– C
AN
NO
T sa
y th
at
failu
re to
pas
GG
pre
dict
s non
-op
failu
re (t
hey
didn
’t try
) but
th
ey c
laim
that
eve
ry p
atie
nt w
ho fa
iled
had
a cl
osed
loop
at
surg
ery
(not
stra
ngul
atio
n).
Bur
ge J
2005
R
ando
miz
ed c
ontro
lled
trial
of G
astro
graf
in in
adh
esiv
e sm
all b
owel
ob
stru
ctio
n.
ANZ
J Su
rg. 2
005
Aug;
75(8
):67
2-4.
I 10
0 cc
of G
G re
duce
d tim
e to
reso
lutio
n of
sbo
from
21
to 1
2 hr
s. L
OS
decr
ease
d by
1 d
ay.G
G d
id n
ot c
hang
e th
e nu
mbe
r of
peo
ple
who
faile
d no
n-op
mgm
t
Che
n SC
20
06
Spec
ific
oral
med
icat
ions
dec
reas
e th
e ne
ed fo
r sur
gery
in a
dhes
ive
parti
al
smal
l-bow
el o
bstru
ctio
n.
Surg
ery.
200
6 M
ar;1
39(3
):31
2-6.
I Pa
tient
s tre
ated
with
MgO
xide
, Lac
toba
cillu
s, an
d Si
met
hico
ne fo
r PSB
O (b
y G
G st
udy)
had
a h
ighe
r inc
iden
ce
of n
on-o
p m
gmt (
77 V
90%
p<0
.01)
. Thi
s com
bina
tion
of
med
s may
redu
ce n
eed
for o
pera
tion
in P
SBO
Cho
i HK
20
02
Ther
apeu
tic v
alue
of g
astro
graf
in in
adh
esiv
e sm
all b
owel
obs
truct
ion
afte
r un
succ
essf
ul c
onse
rvat
ive
treat
men
t: a
pros
pect
ive
rand
omiz
ed tr
ial.
Ann
Surg
. 200
2 Ju
l;236
(1):
1-6.
I Th
ey ra
ndom
ized
GG
v. s
urge
ry a
fter 4
8hrs
of c
ons m
gmt a
nd
show
ed th
at m
ost o
f the
GG
pat
ient
s did
not
requ
ire su
rger
y.
Feva
ng B
T 20
00
Upp
er g
astro
inte
stin
al c
ontra
st st
udy
in th
e m
anag
emen
t of s
mal
l bow
el
obst
ruct
ion-
-a p
rosp
ectiv
e ra
ndom
ised
stud
y.
Eur J
Sur
g. 2
000
Jan;
166(
1):3
9-43
.
I In
this
non
-blin
ded
stud
y G
G m
ixed
with
bar
ium
had
no
effe
ct o
n re
solu
tion
of S
BO
, nee
d fo
r ope
ratio
n, ra
te o
f st
rang
ulat
ion.
Res
olut
ion
was
not
diff
eren
t fro
m th
e lit
erat
ure
(PSB
O 7
6%; C
ompl
ete
41%
).
Yag
ci G
20
05
Com
paris
on o
f Uro
graf
in v
ersu
s sta
ndar
d th
erap
y in
pos
tope
rativ
e sm
all
bow
el o
bstru
ctio
n.
J In
vest
Sur
g. 2
005
Nov
-Dec
;18(
6):3
15-2
0.
II
Tim
e to
firs
t sto
ol sh
orte
r in
Uro
graf
in g
roup
. U
G g
roup
had
be
tter n
on-o
p m
gmt r
ate
(89.
4 to
75.
4% p
<0.0
5).
UG
gro
up
had
shor
ter L
OS
(2.7
3d v
. 6.1
d).
© C
opyr
ight
200
7 –
East
ern
Ass
ocia
tion
for t
he S
urge
ry o
f Tra
uma
Gow
en G
F 20
03
Long
tube
dec
ompr
essi
on is
succ
essf
ul in
90%
of p
atie
nts w
ith a
dhes
ive
smal
l bow
el o
bstru
ctio
n.
Am J
Sur
g. 2
003
Jun;
185(
6):5
12-5
.
III
In p
atie
nts w
/o si
gns o
f stra
ngul
atio
n a
nasa
lly p
lace
d lo
ng
tube
(usi
ng e
ndos
copy
to p
ass i
nto
the
jeju
num
) ha
d a
90%
re
solu
tion
rate
for S
BO
R
oadl
ey G
20
04
Rol
e of
Gas
trogr
afin
in a
ssig
ning
pat
ient
s to
a no
n-op
erat
ive
cour
se in
ad
hesi
ve sm
all b
owel
obs
truct
ion.
AN
Z J
Surg
. 200
4 O
ct;7
4(10
):83
0-2.
III
Find
ing
GG
in th
e co
lon
4h p
ost a
dmin
istra
tion
relia
bly
pred
icts
succ
essf
ul n
on-o
p m
gmt.
Con
serv
ativ
e M
anag
emen
t – A
ntib
iotic
s Sa
gar P
M
19
95
Inte
stin
al o
bstru
ctio
n pr
omot
es g
ut tr
ansl
ocat
ion
of b
acte
ria.
Dis
Col
on R
ectu
m. 1
995
Jun;
38(6
):64
0-4.
II
B
acte
ria w
ere
foun
d in
mes
ente
ric ly
mph
nod
es a
t a m
uch
grea
ter f
requ
ency
in o
bstru
cted
v. n
on-o
bs p
atie
nts (
39.9
% v
. 7.
3% p
, 0.0
01).
Pos
t-op
sept
ic c
ompl
icat
ions
wer
e m
ore
likel
y in
pts
that
had
+ m
es. L
ymph
nod
es (3
6.1
v. 1
1.1%
P<
0.05
)
Con
serv
ativ
e M
anag
emen
t – N
utrit
ion
Ope
rativ
e In
terv
entio
n –
Gen
eral
Con
side
ratio
ns
Feva
ng B
T 20
04
Long
-term
pro
gnos
is a
fter o
pera
tion
for a
dhes
ive
smal
l bow
el o
bstru
ctio
n.
Ann
Surg
. 200
4 Au
g;24
0(2)
:193
-201
. II
I St
udy
sugg
estin
g lo
wer
risk
of r
ecur
renc
e if
treat
ed su
rgic
ally
. H
owev
er ri
sk o
f nee
ding
surg
ery
if fu
ture
epi
sode
is th
e sa
me.
Th
e hi
ghes
t ris
k is
afte
r 5 y
ears
, but
can
occ
ur e
ven
deca
des
late
r. M
ultip
le m
atte
d ad
hesi
ons h
ave
mor
e re
curr
ence
than
si
ngle
ban
ds (a
t lea
st th
ose
rx’d
surg
ical
ly)
Land
erca
sper
J
1993
Lo
ng-te
rm o
utco
me
afte
r hos
pita
lizat
ion
for s
mal
l-bow
el o
bstru
ctio
n.
Arch
Sur
g. 1
993
Jul;1
28(7
):76
5-70
; dis
cuss
ion
770-
1.
III
Rat
e of
recu
rren
ce is
hig
her w
ith n
on-o
p m
gmt (
38%
v. 2
1%
p<0.
001)
. C
ompl
ete
SBO
v. P
artia
l – n
o di
ffer
ence
in
recu
rren
ce e
ither
op
or n
on-o
p. O
p v.
non
-op
no d
iff in
m
orta
lity
Ea
rly O
pera
tive
– C
linic
al In
dica
tions
/Sub
grou
ps
Torte
lla B
J
1995
In
cide
nce
and
risk
fact
ors f
or e
arly
smal
l bow
el o
bstru
ctio
n af
ter c
elio
tom
y fo
r pen
etra
ting
abdo
min
al tr
aum
a.
Am S
urg.
199
5 N
ov;6
1(11
):95
6-8.
II
(N=3
41; P
rosp
ectiv
e) P
atie
nts w
ho h
ad a
lapa
roto
my
for
pene
tratin
g tra
uma.
The
hyp
othe
sis i
s tha
t the
y w
ould
hav
e a
high
er in
cide
nce
of p
ost-o
pera
tive
SBO
, def
ined
as S
BO
in 6
m
onth
s pos
t-exp
lora
tion.
The
inci
denc
e w
as h
ighe
r, 7.
4% a
s co
mpa
red
to a
repo
rted
0.69
% fo
r pos
t-ope
rativ
e SB
O
Mea
gher
AP
19
93
Non
-ope
rativ
e tre
atm
ent o
f sm
all b
owel
obs
truct
ion
follo
win
g ap
pend
icec
tom
y or
ope
ratio
n on
the
ovar
y or
tube
. Br
J S
urg.
199
3 O
ct;8
0(10
):13
10-1
.
III
(N=3
30; R
etro
spec
tive)
Pat
ient
s with
App
ende
ctom
y/tu
bo-
ovar
ian
proc
edur
es a
re m
ore
likel
y to
requ
ire o
pera
tive
inte
rven
tion
(95%
vs.
53
Potts
FE
4th
1999
U
tility
of f
ever
and
leuk
ocyt
osis
in a
cute
surg
ical
abd
omen
s in
octo
gena
rians
an
d be
yond
. J
Ger
onto
l A B
iol S
ci M
ed S
ci. 1
999
Feb;
54(2
):M
55-8
.
III
(N=1
17) P
atie
nts w
ith fe
ver a
nd le
ukoc
ytos
is th
at a
re in
thei
r 80
’s m
ost l
ikel
y ha
ve A
cute
cho
lecy
stiti
s and
vis
cous
pe
rfor
atio
n.
© C
opyr
ight
200
7 –
East
ern
Ass
ocia
tion
for t
he S
urge
ry o
f Tra
uma
Vel
asco
JM
1998
Po
stla
paro
scop
ic sm
all b
owel
obs
truct
ion.
Ret
hink
ing
its m
anag
emen
t. Su
rg E
ndos
c. 1
998
Aug;
12(8
):10
43-5
.
III
(N=5
) Pos
t lap
aros
copi
c SB
Os w
ill n
eed
surg
ical
reso
lutio
n an
d w
ill n
ot re
solv
e sp
onta
neou
sly
as u
p to
73%
will
do
afte
r la
paro
tom
y H
uang
JC
2005
Sm
all b
owel
vol
vulu
s am
ong
adul
ts.
J G
astr
oent
erol
Hep
atol
. 200
5 D
ec;2
0(12
):19
06-1
2.
II
I (N
=19)
Vol
vulu
s alth
ough
rare
in a
dults
can
occ
ur, a
nd w
ill
alw
ays n
eed
surg
ical
ther
apy.
Ta
keuc
hi K
20
04
Clin
ical
stud
ies o
f stra
ngul
atin
g sm
all b
owel
obs
truct
ion.
Am
Sur
g. 2
004
Jan;
70(1
):40
-4.
III
(N=2
80; r
etro
spec
tive)
Pur
pose
was
to id
entif
y as
pect
s of
clin
ical
or l
abor
ator
y ex
am th
at w
ould
iden
tify
patie
nts w
ith
gang
reno
us b
owel
. Onl
y 92
(24%
) of t
he 2
80 p
atie
nts
requ
ired
surg
ery
and
37 o
f the
se h
ad st
rang
ulat
ion
or
inte
stin
al g
angr
ene
(13)
with
smal
l bow
el re
sect
ion.
Onl
y fa
ctor
s tha
t wer
e si
gnifi
cant
for g
angr
enou
s sm
all b
owel
wer
e SI
RS
(12/
13) v
ersu
s (1/
24),
elev
ated
or l
ow W
BC
, and
bas
e de
ficit
or a
cido
sis.
Ts
umur
a H
20
04
Syst
emic
infla
mm
ator
y re
spon
se sy
ndro
me
(SIR
S) a
s a p
redi
ctor
of
stra
ngul
ated
smal
l bow
el o
bstru
ctio
n.
Hep
atog
astr
oent
erol
ogy.
200
4 Se
p-O
ct;5
1(59
):13
93-6
.
III
(N=9
5) S
IRS
and
abdo
min
al g
uard
ing
are
pred
ictiv
e of
st
rang
ulat
ion
in S
BO
.
Ellis
CN
1991
Sm
all b
owel
obs
truct
ion
afte
r col
on re
sect
ion
for b
enig
n an
d m
alig
nant
di
seas
es.
Dis
Col
on R
ectu
m. 1
991
May
;34(
5):3
67-7
1.
III
(N=1
18) P
atie
nts w
ith su
rgic
al c
orre
ctio
n of
SB
O a
fter h
isto
ry
of c
olon
surg
ery.
Pat
ient
s ofte
n ge
t SB
O fr
om re
occu
rren
ce
and
it ca
rrie
s hig
her m
orbi
dity
and
mor
talit
y M
atte
r I
1997
D
oes t
he in
dex
oper
atio
n in
fluen
ce th
e co
urse
and
out
com
e of
adh
esiv
e in
test
inal
obs
truct
ion?
Eu
r J S
urg.
199
7 O
ct;1
63(1
0):7
67-7
2.
III
(N=2
48) P
urpo
se to
look
for w
hat t
ypes
of o
pera
tions
wou
ld
lead
to fu
ture
SB
O. .
The
pre
viou
s sur
gerie
s wer
e di
vide
d in
to
4 gr
oups
: Upp
er a
bdom
inal
, sm
all b
owel
rese
ctio
n,
appe
ndec
tom
y /g
ynec
olog
y, a
nd c
olon
rese
ctio
n. T
he
proc
edur
e th
at le
d to
mos
t SB
O/y
r was
app
ende
ctom
y - 3
.1.
SBO
occ
urre
d ea
rlies
t afte
r res
ectio
n of
smal
l bow
el a
nd th
en
colo
n, w
ith in
the
first
yea
r. C
ompl
ete
obst
ruct
ion
was
hig
hest
af
ter s
mal
l bow
el re
sect
ion,
20/
26, t
houg
h on
ly 3
requ
ired
surg
ery.
M
ontz
FJ
1994
Sm
all b
owel
obs
truct
ion
follo
win
g ra
dica
l hys
tere
ctom
y: ri
sk fa
ctor
s, in
cide
nce,
and
ope
rativ
e fin
ding
s. G
ynec
ol O
ncol
. 199
4 Ap
r;53
(1):
114-
20.
III
(N=9
8) R
etro
spec
tive
revi
ew p
atie
nts w
ho h
ad ra
dica
l hy
ster
ecto
my
for n
on-a
dnex
al g
ynec
olog
ic c
ance
r. R
adia
tion
grea
tly in
crea
ses i
ncid
ence
of S
BO
. Ea
rly O
pera
tive
– R
adio
grap
hic
Indi
catio
ns
Che
n SC
20
05
Prog
ress
ive
incr
ease
of b
owel
wal
l thi
ckne
ss is
a re
liabl
e in
dica
tor f
or su
rger
y in
pat
ient
s with
adh
esiv
e sm
all b
owel
obs
truct
ion.
D
is C
olon
Rec
tum
. 200
5 Se
p;48
(9):
1764
-71.
II
(N=1
21) U
S de
mon
stra
ting
incr
ease
in b
owel
wal
l thi
ckne
ss >
3m
m a
re in
dica
tor f
or su
rger
y. D
ivid
ed in
to 2
gro
ups:
Gro
up
1 –
initi
al S
B w
all t
hick
ness
> 3
mm
, gro
up 2
– S
B w
all <
3m
m. 9
(18.
4%) o
f gro
up 1
pat
ient
s nee
ded
surg
ery
and
only
4
(5.6
%) o
f gro
up 2
.
© C
opyr
ight
200
7 –
East
ern
Ass
ocia
tion
for t
he S
urge
ry o
f Tra
uma
Che
n SC
19
99
Ora
l uro
graf
in in
pos
tope
rativ
e sm
all b
owel
obs
truct
ion.
Wor
ld J
Sur
g. 1
999
Oct
;23(
10):
1051
-4.
II
U
rogr
afin
in th
e co
lon
at 8
hou
rs p
redi
cts s
ucce
ssfu
l non
-op
erat
ive
treat
men
t. O
ral g
astro
grap
hin
is a
goo
d di
agno
stic
to
ol fo
r pre
dict
ion
of th
e su
cces
s of n
on-o
pera
tive
man
agem
ent o
f SB
O
Pere
a G
arci
a J
2004
A
dhes
ive
smal
l bow
el o
bstru
ctio
n: p
redi
ctiv
e va
lue
of o
ral c
ontra
st
adm
inis
tratio
n on
the
need
for s
urge
ry.
Rev
Esp
Enfe
rm D
ig. 2
004
Mar
;96(
3):1
91-2
00.
II
Con
clus
ion
is th
at e
arlie
r use
of c
ontra
st c
an le
ad to
ear
lier
deci
sion
as t
o ne
ed o
f sur
gery
or p
rogr
essi
on o
f non
-ope
rativ
e m
anag
emen
t of S
BO
. .
Early
Ope
rativ
e –
Tim
e Pe
riod
Sosa
J
1993
M
anag
emen
t of p
atie
nts d
iagn
osed
as a
cute
inte
stin
al o
bstru
ctio
n se
cond
ary
to a
dhes
ions
. Am
Sur
g. 1
993
Feb;
59(2
):12
5-8.
III
(N=9
7) R
etro
spec
tive
anal
ysis
of 1
15 a
dmis
sion
s for
97
patie
nts w
ith S
BO
. 3 g
roup
s: e
arly
ope
ratio
n (<
24
hour
s) n
=
21, n
on-o
pera
tive
man
agem
ent g
roup
B1
faile
d, n
= 3
3, a
nd
succ
essf
ul, n
= 6
2. P
rimar
y re
ason
for e
arly
ope
ratio
n w
as
tend
erne
ss o
r sur
geon
’s c
hoic
e. 4
bow
el re
sect
ions
2nd
ary
to
stra
ngul
atio
n in
this
gro
up. T
he g
roup
with
the
only
2 d
eath
s, hi
ghes
t com
plic
atio
n ra
te 3
6%, a
nd h
ighe
st st
rang
ulat
ion
rate
w
as g
roup
B1.
La
te O
pera
tive
– C
linic
al In
dica
tions
/Sub
grou
ps
Ello
zy S
H
2002
Ea
rly p
osto
pera
tive
smal
l-bow
el o
bstru
ctio
n: a
pro
spec
tive
eval
uatio
n in
242
co
nsec
utiv
e ab
dom
inal
ope
ratio
ns.
Dis
Col
on R
ectu
m. 2
002
Sep;
45(9
):12
14-7
.
II
(N=9
5) P
rosp
ectiv
e su
rvei
llanc
e of
242
ope
ratio
ns p
erfo
rmed
of
225
pat
ient
s and
mon
itorin
g fo
r ear
ly p
ost-o
pera
tive
SBO
(E
PSB
O).
The
maj
ority
of t
he p
roce
dure
invo
lved
the
colo
n,
and
45 p
atie
nts h
ad p
revi
ous S
BO
. The
re w
ere
23 in
cide
nts o
f EP
SBO
. 20
reso
lved
by
day
6 w
ith ju
st N
G su
ctio
n. T
he o
ther
3
had
surg
ery
on d
ay 2
, day
16
and
day
29 w
ith th
e la
tter w
ith
SB n
ecro
sis a
nd re
sect
ion.
The
re w
ere
no fa
ctor
s ide
ntifi
ed
with
this
smal
l gro
up o
f pat
ient
s pre
dict
ive
of E
PSB
O
And
erss
on R
E 20
01
Smal
l bow
el o
bstru
ctio
n af
ter a
ppen
dice
ctom
y.
Br J
Sur
g. 2
001
Oct
;88(
10):
1387
-91.
III
Inte
rest
ing
stud
y lo
okin
g at
the
natio
nal r
egis
try o
f all
Swed
ish
hosp
itals
and
the
appe
ndec
tom
ies d
one
over
the
past
30
+ ye
ars.
2454
00 p
atie
nts u
nder
wen
t app
ende
ctom
y ov
er
that
tim
e pe
riod
and
ther
e w
ere
2659
SB
O o
pera
tions
sinc
e on
th
e pa
tient
s. Th
ere
wer
e 24
5400
mat
ched
con
trols
with
245
op
erat
ions
for S
BO
. Cum
ulat
ed ri
sk o
f sur
gery
for S
BO
afte
r ap
pend
ecto
my
afte
r 4 w
eeks
is 0
.41,
at 1
yea
r, 0.
63, a
t 10
year
s 0.9
7, a
nd a
t 30
year
s 1.3
0. T
his i
s low
er th
en p
revi
ousl
y th
ough
. The
cum
ulat
ive
risk
incr
ease
s with
the
oper
ativ
e di
agno
sis w
ith m
esen
teric
ade
nitis
at 1
.42
at 3
0 ye
ars,
perf
orat
ed a
ppen
dici
tis a
t 2.7
6, a
nd o
ther
at 3
.24.
Acu
te
appe
ndic
itis c
arrie
s the
low
est r
isk
of a
ppen
dici
tis a
t 0.7
5
© C
opyr
ight
200
7 –
East
ern
Ass
ocia
tion
for t
he S
urge
ry o
f Tra
uma
Edna
TH
19
98
Smal
l bow
el o
bstru
ctio
n in
pat
ient
s pre
viou
sly
oper
ated
on
for c
olor
ecta
l ca
ncer
. Eu
r J S
urg.
199
8 Au
g;16
4(8)
:587
-92.
III
(N=4
72) S
tudy
of 4
72 p
atie
nts w
ith o
pera
tion
for c
olor
ecta
l C
A fo
llow
ed fo
r 5.5
yea
rs to
est
ablis
h th
e in
cide
nce
of S
BO
. 35
1 ha
d a
cura
tive
proc
edur
e, th
e ot
her 1
21 p
allia
tive.
36/
351
of th
e cu
rativ
e de
velo
ped
an S
BO
that
nee
ded
surg
ery,
whi
le
5/12
1 of
the
palli
ativ
e pr
oced
ures
dev
elop
ed S
BO
pos
t op
erat
ion.
Etio
logy
of S
BO
can
cer i
n ha
lf an
d th
ese
patie
nts'
post
-op
mor
talit
y w
as m
uch
high
er. >
100
0 cc
blo
od lo
ss a
t in
itial
surg
ery
lead
s to
a hi
gher
rate
of S
BO
, as d
oes t
he
grea
ter d
isse
ctio
n of
a c
urat
ive
proc
edur
e Fr
aser
SA
20
02
Imm
edia
te p
ostla
paro
tom
y sm
all b
owel
obs
truct
ion:
a 1
6-ye
ar re
trosp
ectiv
e an
alys
is.
Am S
urg.
200
2 Se
p;68
(9):
780-
2.
III
(N=5
2) R
etro
spec
tive
revi
ew o
f 15
year
s of e
xper
ienc
e to
find
52
pat
ient
s with
imm
edia
te p
ost-o
pera
tive
SBO
. 22
of th
ese
patie
nts n
eede
d su
rgic
al c
orre
ctio
n. T
imin
g of
SB
O w
as a
bout
8
days
pos
t-op.
tim
ing
to b
egin
ning
of s
ympt
oms t
o su
rger
y w
as 5
day
s. R
ate
of n
on-o
pera
tive
treat
men
t was
60%
, and
th
ese
patie
nts h
ad le
ss c
ompl
icat
ions
and
less
LO
S Si
porin
K
19
93
Smal
l bow
el o
bstru
ctio
n af
ter a
bdom
inal
aor
tic su
rger
y.
Am S
urg.
199
3 D
ec;5
9(12
):84
6-9.
II
I (N
=44)
Ret
rosp
ectiv
e re
view
of 1
475
patie
nts w
ith e
ither
A
AA
repa
ir or
Gra
ft re
plac
emen
t of t
he A
orta
for o
cclu
sive
di
seas
e to
iden
tify
the
inci
denc
e of
SB
O in
this
pop
ulat
ion.
44
patie
nts w
ith S
BO
in th
e im
med
iate
pos
t-ope
rativ
e pe
riod
(to
30 d
ays)
foun
d. 1
8 re
quire
d op
erat
ion,
lysi
s of a
dhes
ions
and
2
rese
ctio
ns.
But
ler J
A
19
91
Smal
l bow
el o
bstru
ctio
n in
pat
ient
s with
a p
rior h
isto
ry o
f can
cer.
Am J
Sur
g. 1
991
Dec
;162
(6):
624-
8.
III
(N=5
4; R
etro
spec
tive)
Pat
ient
s with
com
plet
e or
par
tial S
BO
af
ter s
urge
ry a
t som
e tim
e fo
r can
cer.
37 (6
9%) o
f the
se
patie
nts h
ad o
pera
tive
ther
apy.
67%
of t
he g
roup
had
ch
emo/
radi
atio
n th
erap
y. 5
0% h
ad k
now
n re
curr
ence
. 25/
37
with
surg
ery
had
recu
rren
t can
cer a
s the
cau
se o
f the
CA
. O
nly
11 p
atie
nts c
lear
ed n
on-o
pera
tivel
y. 4
9% o
f the
op
erat
ive
patie
nts h
ad m
ajor
com
plic
atio
ns, a
nd th
e op
erat
ive
mor
talit
y w
as 1
6%, i
n ho
spita
l mor
talit
y of
22%
. La
te O
pera
tive
– R
adio
grap
hic
Indi
catio
ns
Cho
i HK
20
05
Val
ue o
f gas
trogr
afin
in a
dhes
ive
smal
l bow
el o
bstru
ctio
n af
ter u
nsuc
cess
ful
cons
erva
tive
treat
men
t: a
pros
pect
ive
eval
uatio
n.
Wor
ld J
Gas
troe
nter
ol. 2
005
Jun
28;1
1(24
):37
42-5
.
II
(N=2
12) 1
00cc
of G
astro
graf
in u
sed
48h
post
SB
O w
ithou
t im
prov
emen
t del
inea
ted
thos
e w
ho n
eede
d su
rger
y (c
ontra
st
not i
n co
lon
at 2
4h) a
nd th
ose
who
did
not
(con
trast
in c
olon
at
24h
). Th
e ne
ed fo
r OR
redu
ced
by 7
4% w
ith a
stra
ngul
atio
n ra
te o
f 0.8
%.
Ono
ue S
20
02
The
valu
e of
con
trast
radi
olog
y fo
r pos
tope
rativ
e ad
hesi
ve sm
all b
owel
ob
stru
ctio
n.
II
(N=1
07) 4
0 cc
Gas
trogr
afin
+ 4
0cc
wat
er p
rovi
ded
with
in 2
4h
of S
BO
adm
issi
on a
fter N
GT
deco
mpr
essi
on a
nd IV
F.
© C
opyr
ight
200
7 –
East
ern
Ass
ocia
tion
for t
he S
urge
ry o
f Tra
uma
Hep
atog
astr
oent
erol
ogy.
200
2 N
ov-D
ec;4
9(48
):15
76-8
. Rel
ated
Art
icle
s, Li
nks
Gas
trogr
affin
is u
sefu
l in
iden
tifyi
ng a
nd tr
eatin
g SB
O n
on-
oper
ativ
ely,
thou
gh th
e in
cide
nce
of st
rang
ulat
ion
is n
ot
affe
cted
. La
te O
pera
tive
– Ti
me
Perio
d C
ox M
R
19
93
The
safe
ty a
nd d
urat
ion
of n
on-o
pera
tive
treat
men
t for
adh
esiv
e sm
all b
owel
ob
stru
ctio
n.
Aust
N Z
J S
urg.
199
3 M
ay;6
3(5)
:367
-71.
III
(N=1
23) 2
or m
ore
indi
cato
rs (f
ever
, tac
hyca
rdia
, con
stan
t pa
in, W
BC
>16)
of S
B st
rang
ulat
ion
on a
dmis
sion
de
mon
stra
tes b
y O
R 7
6% n
on-v
iabl
e SB
. With
out i
ndic
ator
s, 69
% m
anag
ed n
on-o
p w
ith re
solu
tion
of S
B. E
vide
nce
does
no
t sup
port
auth
or’s
stat
emen
t to
aban
don
non-
op a
t 48h
. O
pera
tive
App
roac
h –
Lapr
osco
pic
vs. O
pen
Bor
zelli
no G
20
04
Lapa
rosc
opic
app
roac
h to
pos
tope
rativ
e ad
hesi
ve o
bstru
ctio
n.
Surg
End
osc.
200
4 Ap
r;18
(4):
686-
90.
III
(N=6
5) U
sing
lapa
rosc
opy,
6.5
% in
traop
com
plic
atio
n, 2
0%
conv
ersi
on ra
te a
nd 1
5.4%
recu
rren
ce. U
S gu
ide
to e
nter
ab
dom
en w
ithou
t any
inju
ry o
n en
tranc
e. R
elat
ive
cont
rain
dica
tions
such
as m
assi
ve d
iste
ntio
n, n
o fr
ee
quad
rant
, and
susp
ecte
d st
rang
ulat
ion
disc
usse
d. A
utho
r em
phas
izes
succ
ess w
ith n
umbe
rs a
bove
. C
hopr
a R
20
03
Lapa
rosc
opic
lysi
s of a
dhes
ions
. Am
Sur
g. 2
003
Nov
;69(
11):
966-
8.
III
(N=7
5) U
sing
lapa
rosc
opy,
4.3
% S
B re
sect
ion,
32%
co
nver
sion
rate
, and
ove
rall
low
er O
R ti
me,
infe
ctio
us
com
plic
atio
ns, p
ost-o
p ile
us, a
nd L
OS.
Aut
hor s
tate
s “vi
able
op
tion.
” D
uepr
ee H
J 20
03
Doe
s mea
ns o
f acc
ess a
ffec
t the
inci
denc
e of
smal
l bow
el o
bstru
ctio
n an
d ve
ntra
l her
nia
afte
r bow
el re
sect
ion?
Lap
aros
copy
ver
sus l
apar
otom
y.
J Am
Col
l Sur
g. 2
003
Aug;
197(
2):1
77-8
1.
III
(N=7
16) U
se o
f lap
aros
copy
for b
owel
rese
ctio
n de
crea
ses
vent
ral h
erni
a an
d SB
O re
quiri
ng h
ospi
tal r
eadm
issi
on. S
B
requ
iring
ope
rativ
e in
terv
entio
n w
as si
mila
r bet
wee
n la
paro
scop
y an
d op
en.
Wul
lste
in C
20
03
Lapa
rosc
opic
com
pare
d w
ith c
onve
ntio
nal t
reat
men
t of a
cute
adh
esiv
e sm
all
bow
el o
bstru
ctio
n.
Br J
Sur
g. 2
003
Sep;
90(9
):11
47-5
1.
III
(N=1
04) U
sing
lapa
rosc
opy,
17.
3% p
erfo
ratio
n, 5
1.9%
co
nver
sion
, and
long
er o
pera
tive
times
. Po
st-o
pera
tive
com
plic
atio
ns, r
etur
n of
bow
el fu
nctio
n, a
nd L
OS
less
for
lapa
rosc
opy.
Le
on E
L 19
99
Lapa
rosc
opic
man
agem
ent o
f sm
all b
owel
obs
truct
ion:
indi
catio
ns a
nd
outc
ome.
J
Gas
troi
ntes
t Sur
g. 1
998
Mar
-Apr
;2(2
):13
2-40
.
III
(N=4
0) L
apar
osco
py su
cces
sful
35%
ass
iste
d 30
%, a
nd 3
5%
conv
ersi
on. .
Rea
sons
for c
onve
rsio
n in
clud
ed d
ense
ad
hesi
ons,
need
for b
owel
rese
ctio
n, C
rohn
s, 2
canc
ers a
nd
larg
e ly
mph
nod
es. T
hose
con
verte
d lo
nger
LO
S.
Leva
rd H
20
01
Lapa
rosc
opic
trea
tmen
t of a
cute
smal
l bow
el o
bstru
ctio
n: a
mul
ticen
tre
retro
spec
tive
stud
y.
ANZ
J Su
rg. 2
001
Nov
;71(
11):
641-
6.
III
(N=3
08) L
apar
osco
py c
onve
rsio
n ra
te 4
5.4%
. Fac
tors
that
fa
vor l
apar
osco
pic
succ
ess a
re S
BO
pos
t app
ende
ctom
y, w
ith
band
s as c
ause
, with
less
then
2 p
revi
ous s
urge
ries,
and
shor
ter t
ime
of sy
mpt
oms.
Thos
e no
t con
verte
d ha
d sh
orte
r LO
S, fe
wer
com
plic
atio
ns, a
nd e
arlie
r bow
el fu
nctio
n.
© C
opyr
ight
200
7 –
East
ern
Ass
ocia
tion
for t
he S
urge
ry o
f Tra
uma
Liau
w JJ
20
05
Lapa
rosc
opic
man
agem
ent o
f acu
te sm
all b
owel
obs
truct
ion.
As
ian
J Su
rg. 2
005
Jul;2
8(3)
:185
-8.
III
(N=9
) Con
vers
ion
rate
of 2
2%.
Sute
r M
2000
La
paro
scop
ic m
anag
emen
t of m
echa
nica
l sm
all b
owel
obs
truct
ion:
are
ther
e pr
edic
tors
of s
ucce
ss o
r fai
lure
? Su
rg E
ndos
c. 2
000
May
;14(
5):4
78-8
3.
III
(N=1
5) E
nter
ocly
sis g
uide
d la
paro
scop
y co
nver
sion
rate
of
6.7%
.
Suzu
ki K
20
03
Elec
tive
lapa
rosc
opy
for s
mal
l bow
el o
bstru
ctio
n.
Surg
Lap
aros
c En
dosc
Per
cuta
n Te
ch. 2
003
Aug;
13(4
):25
4-6.
II
I (N
=40)
Lap
aros
copy
con
vers
ion
rate
of 4
0%. I
ntra
op
ente
roto
mie
s 10%
. Lat
e re
curr
ence
2.5
%
Tsum
ura
H
2004
La
paro
scop
ic a
dhes
ioly
sis f
or re
curr
ent p
osto
pera
tive
smal
l bow
el
obst
ruct
ion.
H
epat
ogas
troe
nter
olog
y. 2
004
Jul-A
ug;5
1(58
):10
58-6
1.
III
(N=8
3) 5
7% in
itial
succ
ess r
ate
with
dur
atio
n of
surg
ery
(>12
0min
) and
bow
el d
iam
eter
(>4c
m) p
redi
ctiv
e of
co
nver
sion
. Reo
pera
tion
rate
of 9
%. B
owel
per
fora
tion
and
need
for c
onve
rsio
n in
crea
sed
post
-op
com
plic
atio
ns.
Pekm
ezci
S
2002
En
tero
clys
is-g
uide
d la
paro
scop
ic a
dhes
ioly
sis i
n re
curr
ent a
dhes
ive
smal
l bo
wel
obs
truct
ions
. Su
rg L
apar
osc
Endo
sc P
ercu
tan
Tech
. 200
2 Ju
n;12
(3):
165-
70.
III
(N=2
1) 5
7% la
paro
scop
y on
ly, 2
4% a
ssis
ted,
19%
con
vers
ion
rate
. Util
izin
g la
paro
scop
y (+
/- as
sist
ed) d
imin
ishe
d tim
e fo
r bo
wel
func
tion
and
LOS.
St
rickl
and
P 19
99
Is la
paro
scop
y sa
fe a
nd e
ffec
tive
for t
reat
men
t of a
cute
smal
l-bow
el
obst
ruct
ion?
Su
rg E
ndos
c. 1
999
Jul;1
3(7)
:695
-8.
III
(N=2
5) C
ompl
ete
adhe
siol
ysis
72%
. Lap
ass
iste
d 24
%. O
pen
4%. U
tiliz
ing
lapa
rosc
opy
(+/-
assi
sted
) dim
inis
hed
time
for
bow
el fu
nctio
n an
d LO
S.
Ope
rativ
e A
ppro
ach
– A
djun
cts
Fazi
o V
W
2006
R
educ
tion
in a
dhes
ive
smal
l-bow
el o
bstru
ctio
n by
Sep
rafil
m a
dhes
ion
barr
ier
afte
r int
estin
al re
sect
ion.
D
is C
olon
Rec
tum
. 200
6 Ja
n;49
(1):
1-11
.
I (N
=179
1) P
t blin
ded
rand
omiz
ed m
ultic
ente
r tria
l to
eval
Se
praf
ilm. T
he o
vera
ll ra
te o
f pos
t-ope
rativ
e SB
O sh
owed
no
diff
eren
ce w
ith o
r with
out S
epra
film
. How
ever
, Sep
rafil
m d
id
have
low
er (1
.8 v
s 3.4
%) o
f SB
O re
quiri
ng re
oper
atio
n (N
=90)
. K
ieff
er R
W
19
93
Indi
catio
ns fo
r int
erna
l ste
ntin
g in
inte
stin
al o
bstru
ctio
n.
Mil
Med
. 199
3 Ju
l;158
(7):
478-
9.
III
(N=1
6) U
sing
inte
rnal
sten
ting
with
Bak
er je
juna
l tub
e,
recu
rren
t rat
e of
obs
truct
ion
was
25%
. Non
-obs
truct
ive
intra
-ab
dom
inal
com
plic
atio
n ra
te 1
8.7%
. M
eiss
ner K
20
00
Effe
ctiv
enes
s of i
ntes
tinal
tube
splin
ting:
a p
rosp
ectiv
e ob
serv
atio
nal s
tudy
. D
ig S
urg.
200
0;17
(1):
49-5
6.
II
(N=1
86) W
ith in
tern
al sp
lintin
g, 9
% c
ompl
icat
ions
, 2%
pr
oced
ural
com
plic
atio
ns, 3
% re
oper
atio
n. N
o ea
rly S
BO
. Lo
wer
late
SB
O c
ompa
red
to h
isto
rical
out
com
e da
ta.
Kud
o FA
20
04
Use
of b
iore
sorb
able
mem
bran
e to
pre
vent
pos
tope
rativ
e sm
all b
owel
ob
stru
ctio
n in
tran
sabd
omin
al a
ortic
ane
urys
m su
rger
y.
Surg
Tod
ay. 2
004;
34(8
):64
8-51
.
III
(N=5
1) E
arly
SB
O w
as lo
wer
with
Sep
rafil
m e
vide
nt b
y ea
rlier
die
t int
ake
and
less
abd
omin
al c
ompl
aint
s. N
o re
oper
atio
ns w
ere
requ
ired
in e
ither
gro
up.
Mei
ssne
r K
2001
Sm
all b
owel
obs
truct
ion
follo
win
g ex
tend
ed ri
ght h
emic
olec
tom
y an
d su
btot
al c
olec
tom
y: a
sses
sing
the
bene
fit o
f pro
phyl
actic
tube
splin
ting.
D
ig S
urg.
200
1;18
(5):
388-
92.
III
(N=3
4) In
test
inal
tube
splin
ting
show
ed n
on-s
tatis
tical
few
er
early
and
late
SB
O
Moh
ri Y
20
05
Hya
luro
nic
acid
-car
boxy
cellu
lose
mem
bran
e (S
epra
film
) red
uces
ear
ly
III
(N=1
84) I
ncid
ence
of e
arly
SB
O lo
wer
with
Sep
rfilm
. No
© C
opyr
ight
200
7 –
East
ern
Ass
ocia
tion
for t
he S
urge
ry o
f Tra
uma
post
oper
ativ
e sm
all b
owel
obs
truct
ion
in g
astro
inte
stin
al su
rger
y.
Am S
urg.
200
5 O
ct;7
1(10
):86
1-3.
diff
eren
ce in
surg
ical
site
infe
ctio
n.
Spro
use
LR 2
nd
2001
Tw
elve
-yea
r exp
erie
nce
with
the
Thow
long
inte
stin
al tu
be: a
mea
ns o
f pr
even
ting
post
oper
ativ
e bo
wel
obs
truct
ion.
Am
Sur
g. 2
001
Apr;
67(4
):35
7-60
.
III
(N=3
4) T
rans
gast
ric T
how
tube
had
no
long
term
(>4y
) with
pt
s who
had
ope
rativ
e in
terv
entio
n fo
r adh
esio
n SB
O.
Follo
w-u
p re
cord
ed v
ia p
hone
cal
ls to
pat
ient
s (25
of 3
4).
Com
plic
atio
ns a
ll re
late
d to
gas
trost
omy
(25%
) R
odrig
uez-
Rue
sga
R
1995
Tw
elve
-yea
r exp
erie
nce
with
the
long
inte
stin
al tu
be.
Wor
ld J
Sur
g. 1
995
Jul-A
ug;1
9(4)
:627
-30;
dis
cuss
ion
630-
1.
III
(N=4
7) C
ompl
ex su
rgic
al p
atie
nt w
ith m
edia
n 4
prev
ious
la
paro
tom
ies.
23.4
% re
curr
ent S
BO
, onl
y 2
requ
ired
reop
erat
ion.
K
oren
aga
D
2001
Fa
ctor
s inf
luen
cing
the
deve
lopm
ent o
f sm
all i
ntes
tinal
obs
truct
ion
follo
win
g to
tal g
astre
ctom
y fo
r gas
tric
canc
er: t
he im
pact
of r
econ
stru
ctiv
e ro
ute
in th
e R
oux-
en-Y
pro
cedu
re.
Hep
atog
astr
oent
erol
ogy.
200
1 Se
p-O
ct;4
8(41
):13
89-9
2.
III
(N=4
8) 2
2.9%
pre
sent
ed w
ith m
echa
nica
l obs
truct
ion
and
an
teco
lic a
nast
omos
is fo
und
to b
e pr
edic
tive
fact
or. 4
5%
requ
ired
reop
erat
ion.
Poon
JT
2004
Sm
all b
owel
obs
truct
ion
follo
win
g lo
w a
nter
ior r
esec
tion:
the
impa
ct o
f di
vers
ion
ileos
tom
y.
Lang
enbe
cks A
rch
Surg
. 200
4 Au
g;38
9(4)
:250
-5.
II
(N=2
14) S
BO
follo
win
g LA
R is
10.
3%, t
he m
ajor
ity b
enig
n an
d no
t mal
igna
nt re
curr
ence
. D
iver
ting
ileos
tom
y in
crea
ses
inci
denc
e of
ear
ly S
BO
. H
olm
dahl
L
1997
A
dhes
ions
: pre
vent
ion
and
com
plic
atio
ns in
gen
eral
surg
ery.
Eu
r J S
urg.
199
7 M
ar;1
63(3
):16
9-74
. II
I Su
rvey
sent
out
to su
rgic
al d
epar
tmen
t hea
ds in
Sw
eden
. 84%
(8
7uni
ts) r
espo
nse
rate
. >4
700
adm
issi
ons f
or a
dhes
ion
SBO
, 47
% o
pera
tive
rate
. O
ver 1
500
oper
atio
ns/y
com
plic
ated
by
prev
ious
ly fo
rmed
adh
esio
ns. A
utho
r sug
gest
s was
hing
glo
ves
and
sutu
ring
perit
oneu
m c
ould
hel
p bu
t no
evid
ence
pro
vide
d.
SBO
in P
regn
ancy
M
eyer
son
S
19
95
Smal
l bow
el o
bstru
ctio
n in
pre
gnan
cy.
Am J
Gas
troe
nter
ol. 1
995
Feb;
90(2
):29
9-30
2.
III
9 ca
ses o
ver 1
5 ye
ars a
nd 1
50,3
86 d
eliv
erie
s. Pr
evio
us
surg
ery
8 of
9 c
ases
. Ope
ratio
n re
quire
d in
8 o
f 9 p
atie
nts.
No
mat
erna
l dea
ths.
3 of
9 fe
tal d
eath
s (22
-30
wks
)
© C
opyr
ight
200
7 –
East
ern
Ass
ocia
tion
for t
he S
urge
ry o
f Tra
uma