80
SMALL HOSPITAL, BIG SERVICE WORKING PROPOSAL FOR THE FUTURE OF NENAGH HOSPITAL The Way Forward for Smaller Acute General Hospitals in Ireland March 2006
| Date post: | 18-Mar-2016 |
| Category: |
Documents |
| Upload: | testing-tester |
| View: | 219 times |
| Download: | 0 times |

SMALL HOSPITAL,BIG SERVICE
WORKING PROPOSAL FOR THE FUTURE OF NENAGH HOSPITAL
The Way Forward for Smaller Acute General Hospitals in Ireland
March 2006

610141617192022
262627283132
373739
4142434445464647
SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital
CONTENTS
EXECUTIVE SUMMARY
INTRODUCTION
THE PROJECT & METHODOLOGY
NENAGH HOSPITAL NOW AND TOMORROW3.1 Making the Mid West Region Acute Hospitals
Network Work for Patients3.1.1 A Functioning, Patient-Centred Acute Hospitals Network3.1.2 Connections between Primary, Secondary and Tertiary Care3.1.3 Transport – How the Patient Gets to Hospital
3.2 Profile of Nenagh Hospital3.2.1 Volume of Work3.2.2 Services Provided3.2.3 Admissions & Discharges – Practices & Procedures3.2.4 Management & Administration3.2.5 Facilities and Use of Space
3.3 Emergency Services3.3.1 Treatment of Emergencies - A Primary Concern3.3.2 The Future of Accident & Emergency Services
3.4 Medical Services3.4.1 Quantifying Demand3.4.2 Contribution to Mid West Regional Acute Medical Service3.4.3 Issues facing Medical Service at Nenagh Hospital3.4.4 Geriatrics3.4.5 Cardiology3.4.6 Gastro-Enterology3.4.7 Clinical Nurse Specialist
1
2
3
>>
>>
>>
>>

48515253
585859
5959
SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital
3.5 Surgical Services3.5.1 General Surgical Beds in Limerick Regional Hospital3.5.2 Day Surgery3.5.3 Future of Surgery at Nenagh Hospital
3.6 Diagnostic Services3.6.1 Radiology Services3.6.2 Laboratory Services
3.7 Other Services3.7.1 Acute Psychiatry
THE NATIONAL ISSUES AND HOW THEYAFFECT SMALL RURAL HOSPITALS
4.1 Patient Safety3.1.1 Volumes and Outcomes3.1.2 Inter Hospitals Transfers
4.2 Cost Versus Contribution
4.3 Medical Staffing4.3.1 Medical Education and On Call Rotas4.3.2 Medical Training Posts & Attractiveness of Positions
in Smaller Acute Units
4.3 Critical Mass of Services - What services are needed for a safe, viable acute hospital?
CONCLUSIONS AND RECOMENDATIONSPRIORITIES FOR ACTION
List of Tables and FiguresAcknowledgementsBibliography
4
5
62636365
6872 7272
73
76>>
>>

EXECUTIVE SUMMARY
Nenagh Hospital is a 75-bed hospital serving a population of approximately 70,000 people, provid-
ing 24/7 emergency care to its patients. In 2004, Nenagh Hospital treated 4,359 in-patients and
2,869 day cases. There were 12,972 attendances at A&E and 11,067 at Out Patient Clinics.
Nenagh Hospital is part of a network of acute general hospitals with Limerick Regional hospital as
its regional centre. For the community, Nenagh Hospital represents a safety net, a first port of
call in emergencies or when they become acutely ill. It represents the opportunity to be treat-
ed or have a member of the family treated in the community, nursed by people you know and
who know you. It represents easily accessible and quality care. General Practitioners value
the direct referral system which ensures that patients diagnosed as needing acute in-patient
care are not waiting for hours on trolleys in an A&E department to be re-assessed by a junior
doctor.
There are two blueprints that have been presented for the future of the Health Service – the
National Health Strategy and the Hanly Report. In the years since their publication, little clear
progress has been made towards implementing the recommendations of these documents.
Neither gives clear direction for the future of this hospital that is in line with the current reality for
patients and their families. The future remains unclear, therefore any recommendations made
must make sense under all futures.
The Hanly Report proposes changing Nenagh Hospital to a local hospital. This would funda-
mentally alter the service offered making Nenagh Hospital, in essence, a location for elective day
surgery and elective medicine, with a nurse-led minor injuries unit. There would be no on-site
medical presence overnight or at the weekends. Nenagh Hospital would not accept emergencies
or be equipped or staffed to deal with them. But 90% of current in-patient admissions to Nenagh
Hospital are emergencies.
Under the Hanly proposals, all Nenagh Hospital in-patients would go to Limerick Regional
Hospital. Limerick Regional Hospital is one of Ireland’s busiest hospital’s with more 23,000 in-
patient admissions and 50,000 attendances at A&E and a short length of stay. Limerick Regional
Hospital is currently short over 5,000 surgical bed days and 12,700 medical bed days to deal
with its own workload. Nenagh Hospital patients use over 7,200 surgical and 18,000 medical bed
days annually. There are currently no plans to add bed capacity at Limerick Regional Hospital
and the Hanly Report did not look at capital costs for this.
Hanly says “Patients in local hospitals would be treated under agreed protocols.” 1 This is put-
ting excessive faith in protocols. There is a protocol already in place for major traumas, (eg seri-
ous car accidents), which states that these patients should bypass Nenagh Hospital and go
directly to Limerick Regional Hospital. However, major traumas still regularly arrive by ambulance
to Nenagh Hospital for stabilisation before transfer. Paediatric and obstetric emergencies also
arrive at Nenagh Hospital in breach of long-standing regional protocols which state that they
should go to Limerick.
1 Report of the National Taskforce on Medical Staffing, 2003, p68.
SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital 6

There appears to be a significant gap between what is proposed for acute health services for
North Tipperary and the need that is experienced on the ground. Taking an attitude of “What
we have, we hold” is not the answer. However, if one looks at it from the perspective of “What
we need, we hold and develop” we are closer to a solution. There is an important question
which must be asked: Would this report be necessary if Limerick Regional Hospital was a
large, well-equipped major hospital with low bed occupancy and room in the Intensive Care
Unit? If there were beds and service guaranteed for the patients of North Tipperary? If there
was an ambulance service at every cross-roads adequately resourced and fully trained? If
inter-hospital transfer was a matter of one phone call? If the roads were better? The answer is
probably not. However, these conditions do not yet exist. Any change to services at Nenagh
Hospital and within the region has to recognise this fact.
Maintaining the status quo is not enough. Nenagh Hospital, like all hospitals, is changing con-
stantly, because medicine is changing constantly. More can be done, and should be done, for
patients. A hospital needs to develop and change, but that change has to improve patient care
and patient safety in a real way. If the Hanly Report were to be the blueprint for future hospital
services, there would have to be a recognition that a significant period of overlap between the
current situation and any future situation is required. Services cannot be withdrawn or diminished
when replacement services are not in place. It is not reasonable and it is not safe.
There are a number of foundation stones that will make change possible and which are valid
under all futures:
• Links and cooperation between the local acute services at Nenagh Hospital and the
regional acute services in Limerick Regional Hospital must be strengthened and devel-
oped at planning, management and operational levels. This represents major organisation-
al and cultural change and will not happen overnight. Until the network is operating and
cooperating smoothly and seamlessly, it is unrealistic to expect staff or patients to trust that
changes to the system will improve patient care.
• Instead of North Tipperary patients joining the waiting list queue in Limerick Regional
Hospital, there is the opportunity to reverse the flow and to use the facilities in
Nenagh Hospital to allow many patients to be treated quicker and just as well. This
will be done by making theatre time available to surgeons from Limerick Regional
Hospital.
• Increasing the number of specialist consultation clinics and access to Nenagh’s operating
theatres for Limerick Regional Hospital surgeons, will permit the use of Nenagh Hospital’s
potential for increased amounts of day case and 5-day surgery, not only for North
Tipperary patients, but for patients across the region.
• One of the biggest problems for Nenagh Hospital is physical space. There is insufficient
space for current patient numbers. The development of current and additional services is
also curtailed by lack of space. We propose the building of a Diagnostic and Treatment
unit, housing A&E, Radiology including CT scanner, Laboratory and endoscopy and day
surgery unit. This will serve both GPs and other primary care professionals, as well as the
7SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital

SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital 8
hospital, giving quicker access to diagnostics for patients, improving the throughput on day
surgery and endoscopy and, over time, reducing the number of in-patient bed days
required and making the environment as good as the service.
•This will have the positive side effect of leaving space in the current building to decrease
the size of wards, create more single rooms and improve the toilet and bathing facilities,
thus improving patient dignity and privacy and the control of hospital acquired infection.
•Admissions processes at Nenagh Hospital are good. Direct GP referral takes a wasteful
loop out of the admissions process, prevents A&E pile-ups and has been shown to lead to
appropriate admissions. By creating an acute medical unit to process admissions, manage
investigations and allow for admissions earlier in the day, there is potential for further
increasing efficiency in use of in-patients beds and reducing out of hours costs.
•There are excellent relationships between Nenagh Hospital and primary care. These links
must be strengthened and developed further, giving direct access to General Practitioners
to a wider range of services.
While these services are being developed, there are a number of facts which must be taken
into account:
• 96.75% of the patients who present at Nenagh Hospital are treated safely and more cost
effectively there than in Limerick Regional Hospital or elsewhere.
• Improving the inter-hospital transfer system is essential to protecting the other 3.25% of
patients. Until inter-hospital transfer is 100% reliable introducing new models of healthcare
will be difficult.
•Because Limerick Regional Hospital is overwhelmed by its current workload, it has no
room for North Tipperary patients. In the interests of the safety of the people of North
Tipperary, Nenagh Hospital must continue to accept and treat acute medical and surgical
patients on a 24/7 basis.
• Nenagh Hospital acts as an assessment centre for acute patients in North Tipperary,
ensuring that only those patients who will benefit from the specialist teams offered in
Limerick Regional Hospital are transferred, thus keeping the use of this more expensive
resource for those who truly need it.
• Nenagh Hospital, Ennis Hospital and St. John’s Hospital together care for 53.8% of the all
medical in-patients and 59% of general surgical in-patients in the in the Mid West. They
must be properly resourced to do this.
•90% of admissions to Nenagh Hospital are emergencies. A 24/7 A&E service staffed by
experienced doctors and under the responsibility of consultants is essential. A small hospi-
tal responds to major emergencies as a unit. Maintenance of current skill levels amongst
doctors and nurses in Advanced Trauma Life Support, Advanced Cardiac Life Support and
Basic Life Support techniques, is imperative.

9SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital
Reasonable capital investment in Nenagh Hospital at this stage will ensure that a good service
becomes even better. It will prepare Nenagh Hospital for the future and provide increased sup-
port to the acute hospitals network in the region. Realistic long-term plans must be made now.
Nationally, the contribution of hospitals like Nenagh and the range and volume of work they do
has been underestimated. As a result, so has the negative impact of reducing and/or moving the
services they offer. Small hospitals treat large numbers of patients. In 2004, the largest 12 hospi-
tals accounted for 246,902 in-patient admissions. The other 329,571 in-patient admissions to
acute hospitals were to smaller units.2
Smaller hospitals have found innovative solutions to some of the problems that are proving
intractable in larger units, and already have the strong links with primary care that are so desired
by larger urban hospitals. Small hospitals work and represent value for money. Average daily bed
cost at Nenagh in 2004 was €711, compared with €956 for Limerick Regional Hospital and St
Vincent’s Hospital at €1,158, yet the majority of in-patients in acute general hospitals are treated
for the same conditions – heart attacks, strokes, infections, urgent operations and urgent treat-
ment of cancer cases.
There is a critical range of services that a hospital must provide to ensure that it can safely
accept acute patients. Removing or compromising any one of these will lead to problems with the
hospital’s ability to deal properly and safely with acutely ill patients. The National Health Strategy,
2001, promised every citizen a health system based on the principles of Equity, People-
Centredness, Quality and Accountability.
It promises a system that:
“Supports and empowers you, your family and community to achieve your full health potential,
that is there when you need it, that is fair and that you can trust.”
This report concludes that Nenagh Hospital is an essential element in delivering on this prom-
ise for the people of North Tipperary.
2 Integrated Management Returns, Dept of Health & Children, 2004


1.11
SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital
INTRODUCTION
Smaller acute general hospitals like Nenagh are playing an unacknowledged but highly important
role in the provision of acute care to patients all over the country. The volume and range of work
that they do is underestimated by policy-makers, but not by the communities that depend on
them. Using Nenagh Hospital as an example, this report aims to give a realistic picture of what
small acute hospitals do and the important role they play within the national acute hospitals net-
work. It looks at the national issues in health and how they affect small hospitals and addresses
some of the misunderstandings and misinformation that exist around the capacities and contribu-
tion of smaller acute units.
The principle concern of people in North Tipperary and elsewhere in the country is prompt
access to treatment in an emergency. Though unrecognised, smaller acute general hospitals are
providing a large part of this service nationwide. Nationally, approximately 75% of hospital admis-
sions are emergencies. In small hospitals the figure is usually higher. 90% of admissions to
Nenagh Hospital are emergencies. Though Nenagh is a very busy hospital, with bed occupancy
levels consistently 10-20 percentage points above the recommended 85% level required to avoid
bed crises, there is no 6-8 hour wait in A&E. Instead GPs can admit directly to the wards, thereby
providing better service and use of resources.
One of the strongest themes in current health thinking is the importance of increasing
the integration of secondary care with primary and community care. In smaller hospitals,
strong relationships and links between primary and secondary care practitioners already
exist. There are much stronger links into the community than is possible in large urban
centres, and these links are used to manage admissions and plan discharges effectively.
There is nothing unique about Nenagh – other small hospitals around the country are
comparable.
The health reform agenda has created unnecessary uncertainty around the future of many
smaller hospitals around the country. It has put question marks over whether these hospitals
will continue to be allowed to provide acute healthcare services to their communities. This
uncertainty has created its own problems – undermining faith in the services and damaging
staff morale. The team at Nenagh Hospital, and other hospitals like it, find themselves in a
position where questions have been raised over their future, but there has been no subse-
quent guidance, direction or clarity around how exactly that future might evolve. This makes it
extremely difficult to plan and develop services. This is happening in an environment where
demand of the services provided by hospitals is ever-growing, where the complexity of care
increases every year, but where the match between needs and resources is rarely in the
patient’s favour.
We need to look at the situation differently and find new ways of working that willimprove the experience and outcome of acute healthcare for patients.

SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital 12
Forces for Change Many forces are driving change. If we follow the UK model, centralised hospitals serving popula-
tions of 300-500,000 are thought to be necessary to ensure high quality care. The evidence for
this belief is moderate for some surgical services but unclear for medical services.3
Junior doctors can no longer work all hours, and consultants are unwilling to work rotas that
destroy their family life. On a national and international basis, increasing specialisation has
reduced the number of general physicians who are comfortable managing medical emergen-
cies, yet emergency medical cases are increasing. The Royal College of Surgeons in Ireland4
has identified the effect of over-specialisation on the ability of hospitals to cover general on call
rotas. These problems exist in all acute hospitals. All this change is happening against a back-
ground of rising expectations from patients, growing anxiety about medical errors, increasing
litigation, and massive change at an administrative level, with the advent of the Health Service
Executive.
The health service is currently in a state of upheaval and small hospitals are part of this. The
centralisation proposals of the Hanly Report were seen as a solution to the demands European
Working Time Directive. They had, at their core, the right of people to work a 48-hour week, not
the right of people to acute health care that is easily accessible, safe and appropriate. This report
seeks to set the record straight in relation to the role of smaller hospitals and propose a viable,
workable future for Nenagh Hospital.
How This Document is StructuredSection 1 & 2These sections establish the main ideas behind the project and the methods used to arrive at
the conclusions and recommendations.
FIG
.1
NENAGH GENERALHOSPITAL
THE ARGUMENTS FOR / AGAINST LOCAL HOSPITALS
Increasing complexityof care
Emergency Careand A&E
Trends in medicaleducation
Access to care
Demand for servicesvs. Bed Capacity
Poor Infraestructureand Emergency
Transport
EWTD
Centralisation
LARGELY PATIENTFOCUSSED
LARGELY PROFESSIONFOCUSSED
3 NHS, The Configuring Hospitals Evidence File, Part One, 2003. 4 Royal College of Surgeons in Ireland, The Future of Surgical Specialties in Ireland, 2004

13SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital
Section 3In this section we describe what services are currently provided at Nenagh Hospital and how
we believe the resources can best be used and developed to improve the service.
We look at the relationship with the Mid West Regional Hospitals network and describe how
we believe the model could be used to provide acute patients with the right service in the right
place.
Section 4This section discusses the background issues affecting smaller hospitals. It addresses the
questions that all small acute units need to be able to answer, looking to the future:
• Patient Safety: Are small acute hospitals safe?
• Cost vs Contribution: Can we afford to have “a hospital at every cross-roads”?
• Medical Staffing: How can we staff them and be European Working Time Directive
(EWTD) compliant?
• Is there a critical mass of services for a viable, safe acute hospital?
Section 5This section summarises and recaps the conclusions and recommendations for Nenagh
Hospital.


15SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital
THE PROJECT
This project was commissioned by Nenagh Hospital Action Group, a voluntary community-
based organisation. The group was set up in 2003, following the publication of the Hanly
Report,5 to highlight the need for the continuance of acute hospital services at Nenagh Hospital
for the benefit of the people of North Tipperary. Local reaction to the Hanly proposals was
strong. From a community perspective, it appeared that the plans proposed for Nenagh
Hospital did not address the real acute healthcare needs of the community adequately and, it
was felt, were likely to result in a reduction of service and safety for the people of the area.
Since then, the doubts created by the Hanly proposals about the future of hospitals like
Nenagh have remained, but no tangible plans have been put forward.
The Nenagh Hospital Action Group began the current project as a means of taking a positive
step forward. It was felt that by examining the volume and range of work actually done at the
hospital and establishing a clear understanding of the needs by talking to the users and
providers of the services, it would be possible to make proposals for a workable future for
Nenagh Hospital that put patient care and patient safety first.
This group has no power to implement any of its recommendations, only to influence. The
document is intended as a contribution to the debate and a factual base from which reason-
able, informed decisions about the future of Nenagh Hospital can be made.
MethodologyThis report was produced by a project group, a sub-set of the Nenagh Hospital Action Group,
chosen for their expertise in the area of healthcare and their understanding of the needs of the
community in North Tipperary.
The members of the Project Group are:
Nenagh Hospital Action Group: Mr Paul Malone & Senator Kathleen O’Meara
Nenagh Hospital Consultants: Dr Christine O’Malley & Mr David McAvinchey
Other Health Professionals: Staff Nurse Maura Byrne & EMT Mr David King
General Practitioners: Dr Roisin Costello & Dr Colm O’Reilly
The Nenagh Hospital Action Group appointed an independent project manager, Lorna
Carney, to coordinate the project. The research for the project consisted of detailed desk
research looking at national and international publications relating to the area of acute hospi-
tals. Interviews were carried out with the providers and users of the service, including medical,
allied medical and nursing staff, general practitioners and members of the community. All fig-
ures used are based on publically available information from official sources. We primarily
used statistics from 2004 as these were the most recent fully available and verified figures at
the time of writing.
5 Report of the National Taskforce on Medical Staffing, June 2003, Department of Health & Children
2.


17SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital
NENAGH HOSPITAL – NOW & TOMORROW
In this section we describe what services are currently provided at Nenagh Hospital and how we
believe the resources can best be used and developed to improve the service. We look at the
relationship with the Mid West Regional Hospitals network and describe how we believe the
model can be used to provide acute patients with the right service in the right place.
We will look at:
• Mid West Region Acute Hospitals Network
• Profile of Nenagh Hospital Generally
˙Volume of Work
˙Services Provided
˙Admissions and Discharge Policies
˙Management & Administration
˙Emergency Services
˙Medical Services
˙Surgical Services
˙Diagnostic Services
˙Other Services
3.1. MAKING THE MID WEST REGION ACUTE HOSPITALS NETWORK WORK FOR PATIENTS
In Strategy for Acute Hospital Services, Mid West Region (2001), the strategic vision for the
acute services in the Mid West region was defined, in part, as follows:
“The patient is central to service design and delivery.Services are provided to the populations at local level, consistent with safe and effective care and practice.A network of appropriately designed and maintained hospitals and other health care services provided to sup-port patient care in a fully integrated manner. The purpose of such networks is to ensure uniform standards ofcare throughout the region.”
Nenagh Hospital, along with Ennis, St John’s, St Nessan’s, Croom Maternity Hospital and the Mid-
West Regional Hospital itself are part of the Mid-West Region Acute Hospitals Network. To date, the
network is a loose affiliation, the key element of which is the relationship with the Mid West Regional
Hospital (Limerick Regional Hospital) as the central hospital to which patients requiring tertiary care
or more specialised care are transferred. There are also joint appointments with some consultants
appointed to Nenagh Hospital doing a defined number of sessions in Limerick and vice versa.
3.

SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital 18
It is in looking innovatively and open-mindedly at the current and potential future rolesof the different hospitals within the network that the best solution for the patient andthe public purse will be found.
In looking in detail at the role of Nenagh Hospital within the network, we are contributing to the
debate on how the network as a whole could function better.
If only 1 out of 10 patients needs to go, why send all 10?Local fears centre on the loss of local emergency services, longer travelling distances, under-
resourced ambulance service and doubts over whether Limerick Regional Hospital would be able
to cope with the added workload in the short term and be funded adequately to do so in the
longer term. We need to evaluate how smaller general hospitals can work in tandem with more
major centres of specialist care in a way that exploits the rapidity of access that a local unit
brings, while gaining the diagnostic leverage of specialist colleagues.
Centralisation would lead to the vast majority of in-patients in the Mid West region being sent to
Limerick Regional Hospital. However, currently just 3.25% of Nenagh patients require transfer to
Limerick Regional Hospital or other referral centres.
FIG
.2 MID WEST ACUTE HOSPITALS NETWORK
LIMERICKHOSPITAL
ENNISHospital
NENAGHHospital
CROOM
CO CLARE
CO LIMERICK
NORTH TIPP
Current Mid West Hospitals Network
ST. NESSAN’S
ST. JOHN’S

19SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital
If in clinical terms, only one acute patient or less in every 10 will gain real benefit from
being moved to a referral centre, what is the justification for sending the other 9 out of 10
patients too, when they could be cared for in their own community? If the price of moving
the complex emergency to an appropriate centre of expertise is that this patient is accompa-
nied by another nine or 10 patients, who are not complex cases, then another set of prob-
lems is launched relating to effective use of resources, appropriateness and value for
money.
The Impact of Centralisation on Rural PatientsLonger journeys are inevitable. This has immediate therapeutic implications: with many condi-
tions minutes matter. Long journeys mean more ambulances. According to health expert, Andy
Black,6 two fully crewed ambulances cost the same as the direct costs of a medical ward.
Increased distance also creates problems for visiting families and weakens the links with primary
care and social services, which are crucial for discharging the patient. Further problems then
arise with assessment and admission, with larger numbers of patients all trying to get in the
same “door”, creating bottlenecks, exacerbating the A&E crisis and condemning larger numbers
of patients to hours spent on trolleys.
The worst problems come with discharge. The difficulty of discharging patients increases
with their distance from home and the breakdown of links with GPs, local primary care and
family support. Longer average length of stay in most city hospitals is testament to this. It also
makes communication, transport and follow up more difficult. This means that big hospitals
tend to fill up with medical patients, waiting for transport, waiting for somewhere to go. The
strong links into the community are not there and patients can find themselves stranded.
Ironically this often means that patients who need specialist treatment, those who might benefit
from larger hospitals, cannot be admitted because the beds are filled. Or even more worrying-
ly, critically ill patients cannot be transferred from smaller hospitals to the tertiary care centre
for the specialist care that they urgently need.
3.1.1. A Functioning, Patient-Centred Acute Hospitals Network
We advocate making the most of the network model: patients would be admitted first tothe local hospital, like Nenagh, which would in effect be, in part, acting as an assessmentarm of Limerick Regional Hospital.
The medical and nursing staff at Nenagh would have strong relationships with the teams at
Limerick Regional Hospital and staff would do occasional rotations between the hospitals, to
share knowledge, skills and build clinical and organisational relationships. The strong regional
radiology service and laboratory support would continue and grow at a local level, meeting not
only the needs of the hospital, but of primary care. In the medium to long term, high quality
electronic links between Limerick Regional Hospital and Nenagh would allow specialists to
know more about the patients and make it easier to advise at a distance in a range of areas.
6 UK health expert and former CEO of Middlesex Hospital Trust

SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital 20
This technology exists but is not available in the health service, though it is regularly used in
business. Some patients would need to be transferred to the central hospital, but it will be the
minority, as Nenagh’s current figures of less than 4% inter-hospital emergency transfers would
indicate.
• The first advantage is that patients with emergencies would continue to reach hospital within
10-20 rather than 40-60 minutes.
• Links with primary care would be better.
• Those who didn't need admission could be quickly discharged home, without having spent a
day on a trolley.
• Most patients need never go to Limerick Regional Hospital.
• Those who did would not need to be assessed again, and transfer could be faster because
fewer transfers would be needed overall.
This strengthening of links and improvement of communication and cooperation within the Mid
West Acute Hospitals Network is central to our proposals for the future of Nenagh Hospital.
However, it is vital to ensure that, in doing so, all services are strengthened. In a health system
where resources are scarce, and the attitudes of those running the service are formed by that
fact, there is always a risk of impoverishing the local system to support the regional service. This
must be avoided.
The key to a positive future for acute health services in North Tipperary and throughoutthe Mid West region lies in finding ways to use the resources and expertise better withinthis network for the benefit of all patients.
3.1.2. Connections between Primary, Secondary and Tertiary CareIn a tripartite system of primary, secondary and tertiary care, 95% of the sick population are
looked after in primary care7 by their GP. Of the 5% who require acute services, over 95% of those
can be appropriately cared for in acute general hospitals like Nenagh. This leaves a very small
number of patients who require tertiary or highly specialised care. All acute general hospitals
regardless of size or location treat this 95%. Which patients are cared for where has evolved over
time and continues to evolve. Work that would once have been done in an acute hospital is now
done by GPs. The specialty of Cardiology would once have been part of tertiary care but is now
available in almost all acute hospitals.
Primary Care to SecondaryThere are over 35 General Practitioners in North Tipperary, many of whom operate in single or
two-person practices. The county’s population is widely dispersed with only about a third living
in towns. General Practitioners are scattered amongst their patients and many have the offi-
cial status of “Rural GPs”. Communities tend to be stable in North Tipperary and GPs build up
7 Quality and Fairness, National Health Strategy, 2001, Department of Health & Children.

21SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital
strong relationships with patients and their families over time and a strong understanding of
the support available to the patient at home or in the community. Traditionally, rural GPs tend
to take on more of the work that in larger urban centres falls to A&E (i.e. dealing with minor
injuries and suturing), as well as the typical GP work. In addition, in outlying towns and vil-
lages, the local GP will be called to the scene of heart attacks, accidents etc, while the patient
is waiting for the ambulance, something which would be a much rarer occurrence for GPs in
larger towns and cities.
Because of distance and access to other health services, patients will tend to rely heavily on
their GP. Physical distance between patients can make house calls very time-consuming. From a
patient perspective, getting to a hospital Out-Patients Clinic costs money, eg to get from Roscrea
to Nenagh Hospital Out-Patients Department costs €30 in a taxi and to Limerick almost double
that, so all patients, but particularly the poor and elderly, rely heavily on their GP after discharge
from hospital, for example.
The majority of North Tipperary GPs will refer patients to Nenagh Hospital, though those near the
county borders will also tend to use the nearest hospital eg Port Laoise, Cashel/Clonmel, Limerick
or Kilkenny. Nenagh Hospital staff provide laboratory and radiology services for GPs in North
Tipperary. Turnaround times are satisfactory and the hospital is very good at reacting to clinical pri-
ority. As is the case throughout the country, increasing demand from patients for diagnostic tests
has made access for GPs to diagnostics an issue, particularly in non-urgent cases, eg ultra-sound.
Over the last ten years, a lot of work that used to be performed in secondary care hasmade the shift to primary care. Much of the paradigm shift that policy makers thinkneeds to occur to transfer appropriate tasks from secondary to primary care has alreadyhappened. GPs take charge of the on-going management of diabetics, asthmatics, choles-terol, warfarin testing, post-operative care etc, all of which were heretofore treated insecondary care.
As is often the case for smaller general hospitals, the relationship between Nenagh Hospital
and North Tipperary GPs is strong. There is more direct access to services than seen elsewhere,
eg. direct GP access to physiotherapy. This has positive impacts for the patient, reducing waiting
time for treatment, minimising the time spent in hospital and supporting good continuity of care.
The direct referral system which allows GPs to admit directly to the wards results in open com-
munication and good relations between the hospital and the GPs, with little of the friction that
exists in situations where GPs have to see patients they know are very unwell, and need to be in
a hospital bed, queuing in A&E.
ShannondocGPs set up a cooperative called Shannondoc to provide out-of-hours service to patients and
improved quality of life for GPs in the Mid West region. It operates in Clare, North Tipperary and

SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital 22
County Limerick. Most doctors in these areas are members. They work a rota to ensure that
there is adequate service for patients who cannot wait until surgery opening hours the following
day. Patients call a lo-call number and are triaged by an experienced nurse. Where it is neces-
sary for the patient to be seen by the doctor, an appointment is arranged at their nearest treat-
ment centre. If the patient is too ill to travel, a house call is arranged. In many cases, advice from
the doctor or nurse is all that is required. Where the patient requires hospitalisation, the GP calls
the admissions office at Nenagh Hospital or, where appropriate, refers the patient to A&E eg frac-
tures, burns etc
Shannondoc operates each weekday from 6 p.m to 8 a.m the following morning. 24 hour cover
is provided on Saturday, Sunday and Public Holidays until 8 a.m the next working day. It has
bases in Ennis, Ennistymon, Kilrush, Shannon, Nenagh, Roscrea, Thurles and Newcastle West.
The Shannondoc base in Nenagh is on the hospital site. GPs see the on call service they offer
as very different but complementary to that offered by an acute hospital.
Secondary to TertiaryNenagh Hospital provides acute general hospital care to North Tipperary patients who are acute-
ly ill and whose condition requires more specialised intervention and investigation than a GP can
provide. This is what has traditionally been known as secondary care. Most of the work done in
every acute general hospital, irrespective of size, is the same – heart attacks, strokes, pneumo-
nias, accidents, gall bladders and cancer cases. It is this type of work that accounts for most of
the queues in A&E. Secondary care could be said, to some extent, to have become emergency
care or urgent acute admission.
Some tertiary care services are available at limited or even a single location eg vascular sur-
gery, neurosurgery, transplant services. Limerick Regional Hospital performs the role of sec-
ondary care provider or local hospital for Limerick City and County as well as acting as a terti-
ary referral centre for the Mid West. Because there is a shortage of beds, this means that you
can have a situation where secondary and tertiary care patients are in competition for the
same bed. Both patients need to be hospitalised. Both patients need acute care. We suggest
that there is an important role for Nenagh Hospital and other hospitals like it in helping
Limerick Regional Hospital to keep those specialised beds available for patients who really
need them.
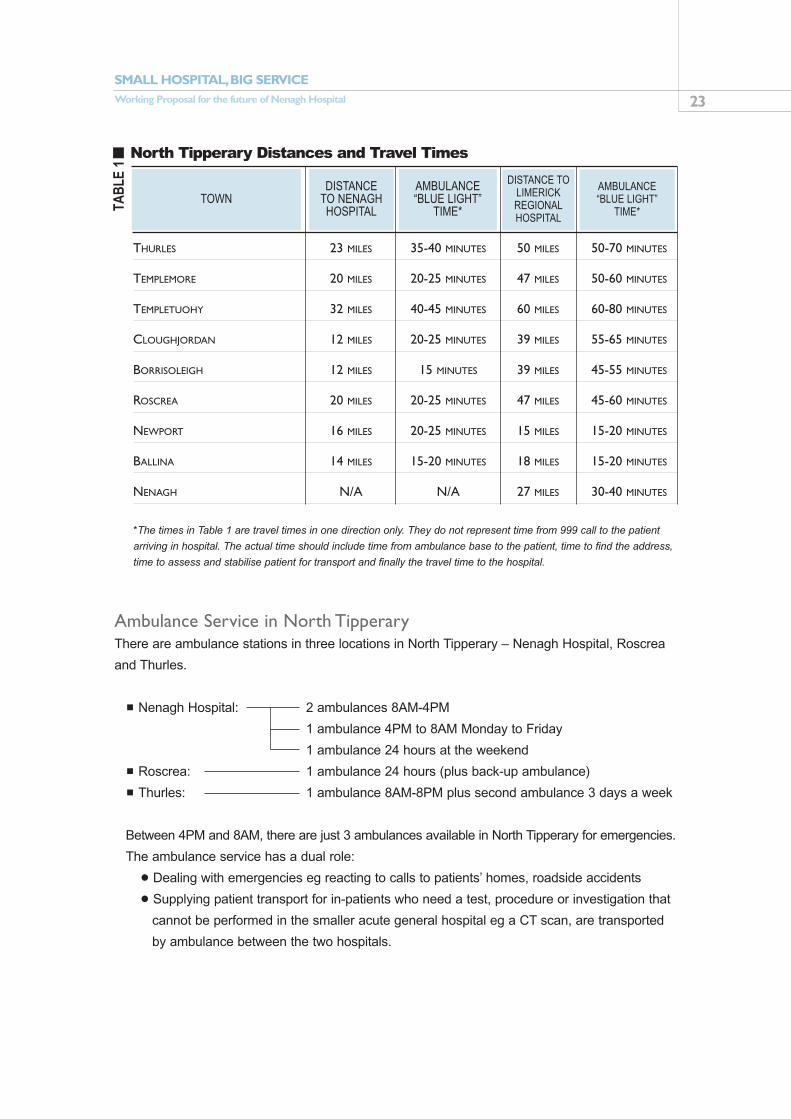
3.1.3. Transport – How the Patient Gets to the HospitalThe patient’s experience of acute healthcare does not begin once they have entered the hospital.
For the patient, it begins when acute symptoms occur, whether it is in the patient’s home, work-
place or on the side of the road. How the patient gets to hospital and, in many cases, how quick-
ly are issues of major concern to patients and their families.
23SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital
*The times in Table 1 are travel times in one direction only. They do not represent time from 999 call to the patient
arriving in hospital. The actual time should include time from ambulance base to the patient, time to find the address,
time to assess and stabilise patient for transport and finally the travel time to the hospital.
Ambulance Service in North TipperaryThere are ambulance stations in three locations in North Tipperary – Nenagh Hospital, Roscrea
and Thurles.
˙Nenagh Hospital: 2 ambulances 8AM-4PM
1 ambulance 4PM to 8AM Monday to Friday
1 ambulance 24 hours at the weekend
˙Roscrea: 1 ambulance 24 hours (plus back-up ambulance)
˙Thurles: 1 ambulance 8AM-8PM plus second ambulance 3 days a week
Between 4PM and 8AM, there are just 3 ambulances available in North Tipperary for emergencies.
The ambulance service has a dual role:
• Dealing with emergencies eg reacting to calls to patients’ homes, roadside accidents
• Supplying patient transport for in-patients who need a test, procedure or investigation that
cannot be performed in the smaller acute general hospital eg a CT scan, are transported
by ambulance between the two hospitals.
TAB
LE 1
North Tipperary Distances and Travel Times
THURLES 23 MILES 35-40 MINUTES 50 MILES 50-70 MINUTES
TEMPLEMORE 20 MILES 20-25 MINUTES 47 MILES 50-60 MINUTES
TEMPLETUOHY 32 MILES 40-45 MINUTES 60 MILES 60-80 MINUTES
CLOUGHJORDAN 12 MILES 20-25 MINUTES 39 MILES 55-65 MINUTES
BORRISOLEIGH 12 MILES 15 MINUTES 39 MILES 45-55 MINUTES
ROSCREA 20 MILES 20-25 MINUTES 47 MILES 45-60 MINUTES
NEWPORT 16 MILES 20-25 MINUTES 15 MILES 15-20 MINUTES
BALLINA 14 MILES 15-20 MINUTES 18 MILES 15-20 MINUTES
NENAGH N/A N/A 27 MILES 30-40 MINUTES
DISTANCETO NENAGH HOSPITAL
TOWNAMBULANCE“BLUE LIGHT”
TIME*
DISTANCE TOLIMERICKREGIONALHOSPITAL
AMBULANCE “BLUE LIGHT”
TIME*

SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital 24
Both services are currently provided by the same crews. However, there are plans to divide the
service into Patient Transport and Emergencies. It will be interesting to see how and where the line
will be drawn between the two. North Tipperary based ambulances are part of the regional ambulance
service and can therefore be called to emergencies in other parts of the region. For example, if the
Nenagh ambulance is called to an emergency at night and another 999 call comes in for the Nenagh
area, this call will be responded to by an ambulance from one of the other stations. Priority of calls and
decisions about which ambulance will respond are made by ambulance control, based in Limerick. In
August 2005, the ambulance service moved to a national model and while the effects have not been
seen at a local/regional level yet, this will have an impact on the service. Previously ambulances were
assigned to particular hospitals and serviced their needs almost exclusively. Since being regionalised,
the ambulances that are based at Nenagh Hospital, but which find themselves in Limerick for example,
may now be called to an emergency in Limerick or be sent to pick a patient up in Kilkenny or Ennis.
While this fulfils the important role of making ambulances more available for the regional emer-
gency ambulance service, it has a negative knock-on effect for the local service. The ambulance
service is currently under-resourced. Priority, of course, must be given to emergencies when
ambulance numbers and staff are finite. The regional pressure of emergencies on the ambulance
service increasingly means that a Nenagh patient misses an urgent procedure because there is
no transport available to take them to Limerick. Another difficulty is the unavailability of ambu-
lances for return journeys. This can lead to the patient(s) and accompanying nurse being left in
Limerick Regional Hospital, possibly for hours, to wait for an ambulance to become available. This
situation causes distress to the patient and wastes nursing resources. It effectively means that
patients in the outlying units are negatively affected by the move towards improving the regional
service. This type of problem must and can be avoided going forward.
Currently approximately half of the workload for the ambulance service in North Tipperary is routine
transport. In February 2006, the use of private ambulances to transport private in-patients to/from
appointments in Limerick Regional Hospital was begun. This has improved the routine transport situa-
tion for these privately insured patients. The Hanly Report recognises the importance of upgrading the
ambulance fleets and of providing Emergency Medical Technician (EMT) and EMT-A advanced train-
ing for crews. However, the extent of investment and the length of time required to have the service
running at a level to safely support a centralised acute hospital model has been underestimated.
The HSE Mid West has estimated that the Hanly proposals will require the following additions to
the North Tipperary ambulance service.
TAB
LE 2
Ambulance Service Requirements North Tipperary
10 STAFF 32.8 STAFF
4 AMBULANCES 10 AMBULANCES
EMERGENCY AND TRANSPORT EMERGENCY ONLY
CURRENT FUTURE

25SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital
A major challenge faces the ambulance service to train existing staff to EMT/EMT-A level and
keep the service going. There is a shortage of staff at the moment and many staff are doing con-
siderable overtime to try and ensure that rosters are filled. Recruiting and training the required
numbers of additional staff will also be a difficult and time-consuming process.
One of the improvements to the fleet is the purchase of new €180,000 ambulances with
proper equipment that will allow paramedics to put in IV lines and manage airways better.
However, these ambulances have only one stretcher berth. This means that one of these
ambulances is required for each patient. In practice therefore, a two-car collision involving six
injured patients will require six separate ambulances, each with a two-person crew. This clearly
will put a further strain on resources.
Particular Transport Issues in Rural AreasIn a rural situation, there are additional issues to be taken into account when planning how the
patient gets to the hospital.
˙Distances are longer. This means that even with a full “blue light” operation, with the Gardai
going ahead to stop traffic at intersections etc, the amount of time that can be made up is
smaller. In many cases, patients who would come in by ambulance in urban areas, are
brought by car by their family or GP, because of the length of time it may take the ambulance
to get to where they are.
˙Poor roads mean that while the distance in miles may seem reasonable, the length of time to
get to the patient and get the patient to hospital can be long. The state of the roads also
affects what can safely be done while the ambulance is moving. Ambulances will usually
have to pull in to allow the accompanying medic to re-insert an IV line that has become dis-
lodged during the journey, or to administer other drugs or treatments
˙Non-unique and non-specific addresses, more common in rural areas, in addition to poor
sign-posting, are a major problem on the ground for ambulance crews. Finding the patient in
the first place requires considerable local knowledge. An ambulance crew that is operating
outside its usual area can have serious problems finding the patient, leading to delays in get-
ting the patient to the relevant hospital.
˙Lack of public transport means that patients who do not have access to their own transport
have to rely on taxis or the kindness of neighbours to get to hospital for OPD appointments
or other routine tests or procedures. This can put a considerable burden on elderly patients
and can lead to “no shows” at OPD clinics and in some cases, complete failure of the patient
to get appropriate care.

SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital 26
˙Cost to the patient is an important factor of transport to/from hospital or OPD clinics, particu-
larly for elderly patients with limited means. A taxi from Roscrea to Nenagh Hospital costs
approximately €30, a taxi to Limerick would cost double that.
ConclusionOne of the key elements in creating an integrated network of hospitals that works smoothly and
seamlessly is the development of the transport links between the different hospitals. An ambu-
lance service needs to be 100% dependable, 100% of the time.
• Resources are the main issue at the moment.
• However, coordination between the ambulance service and the hospitals at a network level
and at an individual level must also improve, to ensure best overall use of resources.
• Working in the ambulance service is working at the sharp end of the health service. Increasing
training to paramedic level will improve the ability of the ambulance service to be more inde-
pendent in an emergency situation – they will be able to put up IV lines and administer certain
drugs, something which can currently only be done by doctors. This is some time away.
However, the fact remains that an ambulance does not replace a hospital. EMTs taking a patient
under protocol to Limerick Regional Hospital frequently judge that the patient will not make it and
stop in Nenagh Hospital to get the medical and nursing help that will give the patient at least a
chance of survival.
3.2. PROFILE OF NENAGH HOSPITAL
3.2.1 Volume of WorkNenagh Hospital is an acute general hospital that provides care 24 hours a day, 7 days a week.
Nenagh Hospital has 75 in-patient beds and 6 day beds.
90% of admissions to Nenagh Hospital are non-elective, ie emergency admissions.
In 2004, Nenagh Hospital:
˙Had 4,359 in-patient admissions
˙The average length of stay (ALOS) was 6.1 days (national average is 6.7 days).
˙61% of these cases were medical (heart attacks, pneumonias, strokes, cancer cases etc).
˙2,869 day cases were treated
˙There were 12,972 attendances at A&E
˙There were 11,067 attendances at Out Patient Clinics.
Most acute hospitals admit in-patients through A&E. If Nenagh Hospital admitted all patients
through A&E instead of 60% of in-patient admissions coming through GP referral, A&E numbers
would be significantly higher at almost 16,000 attendances. Patient numbers have increased
year-on-year since 1986, despite a reduction in in-patient beds.

27SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital
The hospital employs approximately 285 people, amongst whom there are 30 doctors and 130
nurses (WTEs), the rest being allied medical (eg lab), catering, cleaning, portering, administrative
and other support staff.
3.2.2 Services ProvidedNenagh Hospital operates on a 24/7 basis, accepting acute medical and surgical patients. The
busiest time in the hospital is between 8.00AM and 5.00PM when most patients are admitted or
discharged, Out-Patient Clinics are held and the majority of surgery and investigations occur, and
patients on the wards undergo daily review of their case.
The lynch-pin of the service is the ward round, carried out by the consultant, NCHDs and the
ward sister. This usually happens in the morning and allows the senior medics and nurses to dis-
cuss the patient and decide on the best treatment and care regimen for the patient. It ensures
that those responsible for the patient’s care know the patient and have agreed on the best
course of action for the patient.
The range of services offered in Nenagh is in line with the most common illnesses that patients
present with:
˙General Internal Medicine
˙General Surgery
˙Cardiology
˙Diabetes/Endocrinology
˙Gastroenterology
˙Geriatrics
˙Injury
˙Urology
There are sessional OPD commitments from consultants based in Limerick Regional Hospital in:
˙Gynaecology
˙ENT
˙Orthopaedics
˙Paediatrics
˙Ante Natal
˙Rheumatology
˙Sexually Transmitted Diseases
In addition, there are sessions in:
˙Community Ophthalmology
˙Community Dietician
˙Joint Replacement Nurse Specialist
˙Orthopaedic Fitter

SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital 28
As in all smaller hospitals, there is a very hands-on approach by consultants to their work at
Nenagh. The Radiology and Anaesthetic services are consultant-delivered. Because there are
fewer NCHDs compared to larger hospitals and they are not senior, less work is delegated, so
consultants in smaller hospitals are on the wards every day. There is close teamwork with ward
managers and constant interaction with NCHDs.
3.2.3 Admissions & Discharges – Practices and Procedures
Admissions PracticesAt Nenagh Hospital, the policy is never to refuse a patient in need of care.
This includes patients reaching Nenagh Hospital in breach of established protocols but who are
in urgent need of care. There are three ways that patients can access treatment: through A&E as
a “walk in”, by GP referral or following a 999 call (ambulance).
GPs have a choice of ways to access the hospital service for their patient (Fig 6 above). By
providing access into the hospital for patients in need of urgent hospital treatment by a number of
means, the problem of A&E queues is avoided at Nenagh Hospital. Also see section 3.3
Emergency Services.
Benefits of GP ReferralGPs very much value the benefit that permission to refer directly onto the wards at Nenagh
Hospital brings to their patients. Despite the pressure for beds within the system, a mutually sup-
portive and dependent relationship has built up between GPs and the hospital over the years
and, as a result, this system works well and referrals are appropriate.
• Initial assessment of the patient is done by the GP. Triage takes place over the phone
between the GP and senior nursing staff. GPs are asked to send the patient in after 2PM,
unless the patient’s clinical condition requires immediate admission.
• Where there is no bed available immediately, and the patient can wait overnight, the GP
A&E TRAUMA CCU MEDICALWARDS
SURGICALWARDS
999 GPREFERRAL
WALK IN
FIG
.3 NENAGH HOSPITAL WHOLE HOSPITAL EMERGENCY RESPONSE UNIT

29SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital
continues to monitor the patient. The patient is in “the queue” but is in their own home and
under the care of their GP. The patient is admitted when a bed becomes available.
• For the patient, this means that there is no waiting on trolleys for hours in A&E to be triaged
and assessed.
• For the GP, there is certainty. They have identified a patient as being in need of acute care
and they know that their patient will get it.
• For the hospital, there is no duplication, ie the patient is assessed on the ward only, rather
than in A&E as well.
• For A&E, there is a smoother flow. They can concentrate on assessing and treating patients
who need their specific skills, as they are not used unnecessarily as a “foyer” for patients
awaiting admission
• Only 40% of in-patients at Nenagh Hospital are admitted through A&E. The rest are admit-
ted directly by GPs.
The admissions system at Nenagh Hospital works well. A Patient Survey in 2004,8 found that
after registration/triage, 75.9% of Nenagh Hospital patients were seen by a doctor in less than
one hour, compared to the national average of 55.3%. Likewise 75% of Nenagh Hospital patients
waited less than a hour in A&E before being admitted to the ward, compared to 30.8% nationally.
However, there are further improvements that could be made by, for example, bringing admis-
sions in earlier in the day.
Admissions & OvercrowdingThe community and the users of the service value Nenagh Hospital’s policy of never refusing a
patient in need. However, it is not without cost to the hospital and to the staff. Although designat-
ed as a 75-bed hospital, Nenagh Hospital routinely has up to10-20 extra in-patients in extra
beds. These beds can be found in wards, in the corridors outside the wards or in areas that are
not official wards. There is no staff or budget for these extra beds. The issue of overcrowding is
discussed in section 3.2.5 of this document.
Discharge Practices and ProceduresThere are two basic elements to discharge planning: 1) discharge date and 2) discharge destina-
tion and support required. From the time a patient is admitted, ward staff are trying to estimate
the likely time in hospital. The expected discharge date will change depending on clinical change
day by day. In many cases the discharge plan is very simple. Most patients return to the address
that they came from.
However, some will not be sufficiently medically well or independent to return home immediate-
ly or ever. The discharge destination for this group of patients is dependent on their clinical
recovery. This too is constantly changing depending on the nature of their illness and their
progress. Some patients need support services at home. Others need rehabilitation or long term
care in either the public or private sector. A knowledge of the facilities and services available at
8 The Patient’s View, A Comparative Analysis of the Mid Western Regional Hospital, Nenagh Against National Averages, 2004Satisfaction Survey, The Irish Society for Quality and Safety in Healthcare.

SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital 30
the possible discharge locations and the capability of their staff is crucial to selecting patients for
discharge and the timing of the discharge. Hospitals like Nenagh know their patients. They build
up an understanding of the support available to each individual from family and community sys-
tems, which greatly aids successful and appropriate discharging.
ConclusionsMedical Assessment Unit/Admissions Unit
Introducing a Medical Assessment Unit to Nenagh Hospital, similar to St Luke’s Hospital in
Kilkenny, could offer some significant benefits to the efficiency of admissions and the manage-
ment of bed capacity, without causing any of the positives in the current system to be lost.
There are four categories of patients, which would benefit from such a system:
1. It would act as a ‘processing unit’ for GP referred patients. Already accepted for admis-
sion, these patients could be “worked up” more efficiently eg have bloods, x-rays etc done
before going to the wards. It would allow for admission of patients earlier in the day, as
they would not have to wait for other patients to be discharged
2. “Grey area” patients who are currently sent by GPs to A&E as an “assess, query admit”.
This is a more appropriate use of resources than sending these patients through A&E.
3. Fast Track Investigations: there is a small but difficult category of patients who may
require a range of investigations but who do not need to be in hospital. It may not be
appropriate or practical to do the investigations on an out-patient basis, as the patient may
be at risk. These patients are currently admitted as in-patients. With a Medical
Assessment Unit to coordinate investigations rapidly, these patients could now have their
tests done in one day and not require in-patient admission.
4. A Medical Assessment Unit would also facilitate the management of urgent referrals to the
Out Patient Department.
To be successful, the unit must operate on a “clean sheets” model from 8.00AM to 5.00PM. An
acute medical unit would also have efficiency and work flow benefits for the hospital: Earlier
admission would mean that the “clerking” of patients by junior doctors, much of which is now
done out of hours, could be finished earlier in the day. This might mean that the number of on
call hours for NCHDs could be reduced. The earlier admission will also allow for more of the
diagnostic tests to be done inside regular working hours, potentially reducing on call hours in lab
and x-ray also. Treatment could begin earlier in some cases, further improving reducing the
patient’s overall length of stay.

31SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital
3.2.4 Management & AdministrationLike many Irish hospitals, Nenagh Hospital does not have a clear, cohesive management struc-
ture that combines the clinical, organisational and financial/administrative management of the
hospital.
There are three separate “management lines” within the hospital:
˙Administration: headed by the hospital administrator and reporting to the Hospitals
Network Manager in the HSE Mid West area.
˙Nursing Administration: headed by the Director of Nursing, supported by deputy directors
and ward managers
˙Medical Board: an informal body made up of the consultant doctors.
Every member of staff in the hospital relates to these three hierarchies. There is no formal sys-
tem linking these three structures. For most of 2005, there was no administrator appointed to
Nenagh Hospital, so there was no regular, day-to-day administrative input at a managerial level
during that time. There is now a new manager in place, who is in Nenagh three days a week as
he retains responsibility for his previous job in Limerick Regional Hospital until the post is filled.
The Medical Board, consisting of the consultant doctors, meets monthly. The role of the Medical
Board largely relates to clinical governance and clinical policy issues. There is also a monthly
meeting of senior nurse managers.
Because of its small size and cooperative team, Nenagh Hospital has been able to rely largely
on informal management structures and practices. This operates satisfactorily on a day-to-day
basis, when events run as normal, largely because the consultants and nurse managers are a
stable group that has worked together for many years. However, when an unusual event or prob-
lem occurs, or when there is a change to the service provided by the hospital (eg the addition of
cardiology) or the support services received (eg ambulance service), the limitation of the informal
structures and practices becomes apparent.
When a decision that falls outside the usual run of business needs to be made (eg to close the
hospital to admissions due to an outbreak of winter vomiting bug) it becomes unclear what the
line of command is and what the process for agreeing on the most effective course of action
might be. Is it a decision for the consultants, nursing management or administration? Do they all
need to agree? Who should report the situation and to whom? Can Nenagh Hospital make this
decision in isolation or does it need to be made in conjunction with the other hospitals in the net-
work, as they would have to absorb patients who would ordinarily go to Nenagh? Who has the
final say? There is currently no clear answer to these questions.
What is needed is a clear, appropriate and efficient decision-making pathway.
Service PlanningThere is no formal, cross-functional decision-making body or planning body for the hospital as a
whole, which harnesses the perspectives and expertise of all of those who are concerned in the
hospital.

SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital 32
In common with other HSE organisations, department heads at Nenagh Hospital produce
annual service plans. However, these are not developed as coordinated, strategic documents,
rather they are generally seen as a paper exercise. This is because there is no guarantee of any
or all of the funding to support the plans. As a result, meaningful, coordinated, strategic planning
for the long term future of the hospital is not done.
Conclusions• The hospital needs a cross-functional management team and clarity on decision-making
pathways, particularly where both clinical and managerial/administrative issues and perspec-
tives are required to make the best choices for the service.
• This may involve creating a variation on previous bodies such as the Hospital Executive
Committee. However, whatever form is considered most appropriate, an important factor in
its success will be clear and well-communicated definition of its roles, responsibilities and
decision-making powers.
3.2.5 Facilities and Use of SpaceThe main building at Nenagh Hospital was constructed in 1936. There have been additions
and upgrades in the intervening years. However, patients now expect a much higher degree of
comfort and privacy than in the past. The current infrastructure does not meet those expecta-
tions in many cases. Since the hospital was built, the number of patients treated and the num-
ber of services offered at the hospital has increased steadily. This has led to major pressure
for space.
Nenagh Hospital, like other acute hospitals, has seen the number of patients it treats increase
over the last 20 years. At the same time, bed numbers have decreased. At a national level, look-
ing at Table 3 we can see that in the last 25 years, the total number of patients treated annually
has increased from just over 550,000 to over 1 million. In that time, the number of beds available
for those patients decreased from over 17,500 to less than 12,500.
TAB
LE 3
Acute Beds vs Patients Treated National Figures 1980-2004
1980ACUTE BEDS
17,665
13,753
11,832
12,330
544,000
523,000
549,000
576,000
8,400
125,000
320,000
464,000
IN-PATIENTS DAY CASES
1990
20002004

33SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital
In Nenagh Hospital in 1986 there were 110 beds and 4,710 in-patients and no day cases.
In 2004, Nenagh Hospital had 4,359 in-patient admissions to just 75 beds, plus 2,869 day
cases were treated. While there have been great leaps forward in what medicine generally,
and Nenagh Hospital specifically, are able to do to treat patients in that time, there are now
significant problems of overcrowding, not just in Nenagh, but throughout the acute hospitals
sector.
(I) MORE PATIENTS THAN BEDS - THE IMPACT OF OVERCROWDING
To show what this overcrowding means in practical terms, we extracted the figures for the month
of October 2005 as an illustration of how occupancy fluctuates. The figures include both surgical
and medical patients.
Actual bed occupancy for October 2005 was 102.5%. As we can see from Fig. 7, for 19 of the
31 days in the month, the hospital was at capacity or above. The highest patient numbers on any
one-day was 87, ie 12 more in-patients than there are beds. At no stage in the month did bed
occupancy reach the recommended average rate of 85% or 64 patients. As stated earlier,
Nenagh Hospital has a policy of never turning away a patient in need of care. However, with
such overcrowding, should the possibility of closing to admissions, once capacity levels of 75
patients has been reached, be considered? The answer is probably “Yes”.
But the problem of lack of capacity within the Mid-West Acute Hospitals Network remains.
FIG
.4 Pattern of Demand for Beds Numbers of In-Patients October 2005
100
90
80
70
60
50
40
30
20
10
0
01/10
/2005
03/10
/2005
05/10
/2005
07/10
/2005
09/10
/2005
11/10
/2005
13/10
/2005
15/10
/2005
17/10
/2005
19/10
/2005
21/10
/2005
23/10
/2005
25/10
/2005
27/10
/2005
29/10
/2005
31/10
/2005
Actual Patients 100% Bed Occupancy Recommended Average Bed Occupancy

SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital 34
When one hospital is busy, usually all are. If Nenagh Hospital is full and closes to admissions,
what happens to North Tipperary patients? Do they travel to put pressure on an equally or more
overcrowded Limerick Regional Hospital, possibly using a tertiary care bed or ICU bed that might
be needed by a critically ill patient? Do they fail to get care at all?
Because there are no viable alternatives for the patients of North Tipperary, NenaghHospital has no choice for the moment but to continue with its current policy of accept-ing all patients in need of care, despite the pressure it puts on the staff and facilities of thehospital.
To some extent, the policy of hospitals like Nenagh of never refusing a patient in need
of care masks the full extent of the bed capacity problem in our acute hospitals.
(II) COPING WITH PEAKS IN DEMAND
Although there is budget and staffing for 75 in-patients, the need is consistently greater. The
hospital regularly operates with much higher patient numbers than official numbers would indi-
cate. While overcrowding can occur at any time in the surgical or medical wards, it is most
noticeable in the medical wards, due to lack of physical space available to cope with extra
patient numbers.
How Nenagh Hospital copes with the pressure for in-patient beds:
• Official beds are filled first.
• Then “unofficial” ward beds are filled eg the male medical ward officially has 21 beds, but,
in fact, there are 24 physical beds on that ward.
• Once all the ward beds are filled, additional beds are put on the corridors outside the med-
ical wards. Up to 11 patients have been accommodated in this way in the past.
• When all the spaces on the medical floor, official and unofficial, are filled, medical
patients are “boarded out” to the surgical floor, where they remain the responsibility of
the general medical team but are nursed by the nurses on the surgical ward. This is not
ideal from the perspective of infection control. Also medical patients benefit from the
care of medical nurses; surgical nurses have a different skill set suited to their usual
patients’ needs.
The spill-over of medical patients into surgical beds is common throughout the acute hospital
system. The Acute Hospital Bed Capacity – a National Review, 2002, commissioned by the
Department of Health & Children, suggests that there is a significant difference between bed
designation and clinical activity. In the past, beds have been designated to surgical and med-
ical on a 50:50 basis. However, nationally, medical patients account for almost 75% of all
patients treated and in-patient bed days used. At Nenagh Hospital, 35% of in-patient beds are
designated for surgical patients and 65% for medical patients.

35SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital
(III) SOME ISSUES RELATING TO FACILITIES AND SPACE AT NENAGH HOSPITAL
The problem with space and overcrowding raises three key issues:
• Patient Dignity & Confidentiality
• Ability of Staff to Work Properly
• Infection control
˙Patient Dignity & Confidentiality
By definition, hospitalisation is a stressful experience for patients. Helping a patient to main-
tain their dignity and privacy is important in helping the individual to cope.
• There is a shortage of space for patients and their families in the wards. Wards can
have 8 or more beds. These beds are generally too close together to allow an accept-
able level of privacy for patients. There is little room for chairs for visitors.
• There are insufficient bathing and toilet facilities. One ward can have up to 20 patients
and only one bath and shower room.
• Because there are regularly more patients than beds and ward space, the extra
patients have to be put on beds in the corridor. While every effort is made to protect the
patients’ privacy and dignity, this situation is tough on patients, who feel more exposed
and vulnerable than necessary.
• The close proximity to other patients makes it difficult for a patient or their family to
have a confidential conversation with clinical staff about the patient’s condition and
treatment. Even outside the ward area, there is no adequately sized room available
where patients or their families can talk to the doctors and nurses in private.
˙Ability of Staff to Work
Overcrowding is also tough on staff. They have no room to do their work, and have to witness
the extra distress that this situation causes to their patients.
• It is very difficult to examine a patient properly if they are on the corridor or in an over-
crowded ward.
• Because the corridors are not very wide, extra beds on corridors can block the free
flow of traffic on the corridors, particularly at mealtimes or during ward rounds.
• There is inadequate appropriate storage space available for clinical supplies eg band-
ages, dressings, basins, IV stands etc.
• There are no adequate changing facilities for staff. Neither are there shower rooms
available for their use. This results in staff having to wear their uniforms outside the
hospital, which is not recommended.
• There are a number of nurse specialists at Nenagh Hospital who provide a very valu-
able service for patients in terms of education and advice in the management of their
condition. There is no space available to this group on a regular and consistent basis
where they can see patients and advise them.

SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital 36
˙Infection Control
Whatever difficulties overcrowding causes for patients and staff, the most important is the
effect that poor facilities have on the ability of staff to control the spread of hospital-acquired
infections.
• The distance between the beds in most wards would not meet the SARI guidelines9
• As in many hospitals around the country, the large wards and very small number of single
rooms make it very difficult to isolate patients and prevent transmission of hospital-
acquired infections. No matter how many times healthcare workers, patients and visitors
wash their hands, it will have little positive effect while patients are on top of one another.
The biggest priority for patients and staff alike is to solve the over-crowding problem on the
medical wards and so minimise the opportunities for infection to spread.
What is required immediately to bring the accommodation up to the standard thatpatients and staff expect and deserve is:
• Creation of new ward space for medical patients, including an increase in bed numbers• Smaller 4 or 5 bed wards with adequate space between beds• Increased number of toilets and showers• Increased number of single rooms
These recommendations can be implemented at Nenagh Hospital without major capitalinvestment in new wards.
˙Other Issues relating to Facilities and Use of Space
• Operating theatres are in need of refurbishment or replacement.
• Conditions in A&E, the laboratory and radiology are cramped and inadequate, though it is
understood that funding has been sanctioned to extend these areas.
• The current canteen, which serves patients, staff and visitors, is at capacity. When admin-
istrative staff move into the administrative building currently under construction in the
grounds of the hospital, the canteen will become inadequate.
There are a number of spaces within the hospital that are under-utilised. (eg closed ward on
first floor and decommissioned mortuary). However, they are not adequate to meet all the
requirements.
A building for HSE administrative offices is currently being built in the grounds of the hospital.
It is understood that there is unlikely to be space in this building for use by hospital staff and
patients.
9 The Control and Prevention of MRSA in Hospitals and in the Community, published by HSE on behalf of SARI Infection Control Sub-Committee

37SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital
3.3 EMERGENCY SERVICES
3.3.1 Treatment of Emergencies – A Primary ConcernContinuation of local emergency services is of primary importance to the community in North
Tipperary. Concerns have primarily centred on the distances to be travelled to get access to full
emergency care and the time taken to get there. Knowing that there is proper emergency care
available relatively near at hand and within “the golden hour” is very important to how safe peo-
ple feel.
What is needed is a patient-centred system that considers the patient’s needs from thetime that the emergency arises, not just the needs of the hospital from the moment thepatient arrives at the door.
Provision must be made for the emergency treatment of unselected medical and surgical
patients at Nenagh Hospital, as long as “the lights are on”, because patients will continue to
reach the hospital in need of treatment, despite protocols. Patients do not usually know how
sick they are before they arrive at the door of a hospital, so any acute hospital has to be in a
position to stabilise any patient for transfer. For example, Nenagh Hospital has been closed to
obstetric emergencies for many years. However, in 2003, there were five births in Nenagh
Hospital and in 2004 there were two.10 In addition, there are over 30 “near misses” per year,
where the patient could be transferred in time. Similarly, Nenagh Hospital does not work with
paediatric emergencies. Yet, every year, there are a small number of children with life-threat-
ening emergencies, eg serious asthma attacks, meningitis, epileptic fits, who are brought by
concerned parents or by ambulance by Emergency Medical Technicians who are concerned
that the patient will not make it to Limerick. These patients cannot be turned away.
This ability to deal with “all-comers”, in terms of initial life salvage and stabilisation, is more
important for rural acute units than for Dublin hospitals, where the paediatric or obstetric hospital
is only minutes away. The Nenagh Hospital A&E is staffed 24 hours a day. There are three inde-
pendent emergency physicians who provide the service, supported by two nurses during the day
and one nurse at night. The current A&E accommodation is wholly inadequate. Funds have been
allocated to build a new A&E. Plans are currently in progress.
(I) MANAGEMENT OF EMERGENCIES
While discussion of Emergency Services naturally focuses on the Casualty/A&E room, ie physical
location, the emergency services provided by an acute hospital encompass the wider team within
the hospital. In larger hospitals, this role is performed by an Emergency Department, run by A&E
consultants and their teams with nursing support. Patients remain in A&E throughout the process
of stabilisation, assessment, diagnosis and treatment, whether being looked after by A&E doctors
or the ward team. Nenagh Hospital aims to triage emergency patients directly to the part of the
hospital which is most appropriate for their treatment, bypassing A&E where appropriate.
10 HIPE data, Nenagh Hospital

SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital 38
From the point of view of a member of the public, an emergency can be anything from a sprain
after a fall to a suspected stroke. Clearly these emergencies require different types of responses.
At Nenagh Hospital, emergencies are dealt with in two different ways, depending on how the
patient comes into the system:
• Urgent acute admissions: these come through GP referrals or following 999 calls
• Typical accident situations, ranging in severity from cuts and bruises to overdoses and major trau-
ma. These come through self referral (ie turning up at A&E) and following 999 calls or GP referral.
Urgent Acute AdmissionsAt Nenagh Hospital, almost 90% of admissions are non-elective, ie emergency. However, most of
these patients do not come through the A&E Department. In North Tipperary, if the GP feels that
the patient is in need of hospitalisation, they will call the Admissions Office of Nenagh Hospital
and request a surgical or medical bed. The GP only refers the patient to the A&E where the GP
feels that the patient requires particular diagnostic tests or a second opinion to assess whether
hospitalisation is necessary or not, or to decide whether the admission is medical or surgical.
(See also section 3.2.3. of this document)
As beds became scarcer in other acute hospitals, many withdrew the right of GPs to direct
referrals, probably as a means of protecting a scarce resource. In studies carried out at Nenagh
Hospital,11 GPs have been shown to be very good at judging whether patients needed to be
admitted and referral has been shown to be appropriate, with GP admissions usually being sicker
and needing to stay longer than admissions coming from self-referrals through A&E. In other hos-
pitals, the vast majority of these GP-referred patients would have to go through A&E.
By bypassing A&E and trusting the judgement and professional skills of general practi-tioner colleagues, Nenagh Hospital has taken a wasteful loop out of the admissionsprocess.
Accident SituationsIn 2004, there were 12,972 attendances at the Accident & Emergency Department in Nenagh
Hospital. Just 40% of the hospital’s admissions come through A&E. Patients are treated for a
range of problems including minor injuries, poisoning, bleeding etc. In urban areas, most atten-
dances at A&E are self-referred or arrive by ambulance. In rural areas, like North Tipperary,
patients will usually go to their GP first. The GP will treat the patient if possible, including carry-
ing out procedures such as suturing in more rural areas.
In Nenagh Hospital, when a major trauma comes in, all the resources and expertise avail-
able are put into play for the patient. Rather than going to A&E, the patient is taken to the dedi-
cated Trauma Room on the first floor beside the operating theatres. The patients are then treated
by the surgical or team and anaesthetists, as appropriate. Patients in need of transfer are sta-
bilised before being taken by ambulance, often accompanied by a doctor or anaesthetist from
Nenagh Hospital, eg to specialist orthopaedic or head injury units in Limerick or Cork.
11 Kellett, J. MD, Dunne, B., Medical Admissions Predictor Study 1999-2004, Nenagh Hospital

39SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital
3.3.2 The Future for Accident & Emergency Services
Innovative SolutionThe current arrangement, where the A&E/Casualty is run by independent emergency physicians is
particular to Nenagh Hospital and a small number of other acute units. It was an innovative idea
that came as a reaction to the changes by the A&E training body and the Medical Council, in rela-
tion to registration and training requirements for doctors and a desire to ensure 24/7 A&E service
for the people of North Tipperary. A consultant anaesthetist at Nenagh Hospital has administrative,
but not clinical, responsibility for the A&E service. As with all innovations, there are mixed views,
both within the hospital and amongst some GPs, as to its success and long term viability.
Concerns centre around the fact that these independent emergency physicians have no
direct line of clinical responsibility to a consultant, but are independently responsible for their
actions. This is outside the usual acute hospital clinical hierarchy where “the buck stops” with
the consultant. There are also some day-to-day issues in relation to cooperation and integra-
tion into the overall hospital service, which could be remedied eg communication, transfer of
notes for patients admitted etc. However, the fact that the independent emergency physicians
stay for relatively short periods of time means that the opportunity to work on getting to know
the hospital system and improving the service is not there. A key issue is how to re-introduce
consultant level clinical responsability for patients seen in A&E.
Proposal for Regional ServiceCurrently under discussion at a regional level is the possibility of making the A&E service at
Nenagh Hospital part of a regional A&E service, managed by the A&E consultant in Limerick
Regional Hospital and staffed by NCHDs from his team on rotation to Nenagh. This arrange-
ment has the advantage of creating a clear line of clinical responsibility from the NCHD to an
appropriate consultant, something which does not exist in the current situation. However, it is dif-
ficult to see how a consultant in Limerick over 25 miles away can take full clinical responsibility
for a patient that they cannot personally assess.
This arrangement would only work with clear definition as to where clinical responsibilities
begin and end. Creating an A&E department at Nenagh Hospital that is completely distinct and
separated from the overall service is counter-productive. It creates duplication of resources and
excludes the possibility of using the resources that are already in place.
A Third ProposalEmergency Services at Nenagh Hospital need to be:
•Designed, structured and developed in compliance with best practice and coordinated with
regional emergency services. This should be done by A&E consultant with joint appointment
to Nenagh and Limerick, with 6 plus sessions per week in Nenagh.
•Use the full resources of the hospital teams available to react to major emergencies. These
resources are available for “free” to the emergency department. (When a critical mass of

SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital 40
services is maintained in order to provide hospital treatment to general medical and surgical
patients, this allows the hospital, almost as a bonus, to respond safely to emergencies).
•Have a Casualty Room that is manned 24/7 by appropriately qualified and supervised doc-
tors with responsibility to a consultant.
To make any service work requires a very open and cooperative approach between the region-
al service and the medical staff at Nenagh Hospital:
•The A&E consultant (ie the regional service) would have responsibility for the development
of the service, the appointment of A&E staff including doctors, and compliance with best
practice. They would also be responsible for ensuring close cooperation with the rest of the
hospital and agreeing with the Medical Board and management, nursing and administrative,
of Nenagh Hospital how the two parts of the service could work seamlessly together.
•The A&E consultant (ie the regional service) would have responsibility for the work of the
registrar/doctor in the A&E department. The A&E consultant on call would be the first port of
call for any queries relating to A&E treatment.
•Where it becomes clear to the A&E doctor that a patient needs specialist medical or surgical
care, (eg an A&E patient who suddenly develops an internal bleed), the patient is transferred
to the care of the surgical or medical team at Nenagh Hospital, activating the emergency
service, or if more appropriate, is transferred to Limerick Regional Hospital. Maintenance of
high levels of skills in Advanced Life Support, Advanced Trauma Life Support and Advanced
Cardiac Life Support amongst the wider medical and nursing team at Nenagh Hospital is key.
Reality on the groundWhile the patients who are fit enough to travel can be transferred to Limerick or indeed be taken there
directly, the fact remains that in very serious cases, where time is critical, patients will be brought by
panicked families or worried ambulance teams to Nenagh Hospital and other hospitals like it. As men-
tioned earlier, patients do not know how they sick they are and some will arrive outside protocol. What
this means is that the cases that will arrive at the door of Nenagh Hospital will be at the two
extremes - the easiest and the most difficult.
These difficult cases will require the input of a consultant. In some cases, telephone advice from an
A&E consultant on call will suffice. Sometimes it will require the attendance of a surgical or medical
consultant. Either way, clear and timely access to consultant level expertise is an important factor in
the safe management of emergencies, whether they arrive within or in breach of agreed protocols.
Conclusions•Access to 24/7 doctor provided emergency services is of primary importance to the people of
North Tipperary.
•The development of a properly staffed and funded regional A&E service, with clear lines of
clinical responsibility and strong integration with the emergency services available within the
peripheral hospitals, is an attractive idea. However, it would require the appointment of at

41SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital
least 6 A&E consultants to the Mid West region. There is little indication that this is likely.
Anything less would decrease rather than increase the standard of service to patients.
•If there is no movement on the appointment of an adequate number of A&E consultants, the cur-
rent arrangement based on independent emergency physicians requires further development.
• Likewise, some level of support in respect of service development and integration with the
wider hospital would be required.
3.4. MEDICAL SERVICE
At Nenagh Hospital, there are 36 general medical beds, 5 coronary care unit/ICU beds and 8
geriatric beds. In 2004, 61% of total in-patients discharged12 were medical in-patients. A typical
medical in-patient is 62.2 years and stays in hospital an average of 6.9 days. The average
length of stay for the 10 principal diagnoses (representing almost 40% of the overall medical
caseload) is higher at 7.6 days. The medical team at Nenagh consists of 4 consultant physi-
cians and 11 NCHDs as well as nurses and clinical nurse specialists. The range and break-
down of the medical workload at Nenagh Hospital is comparable to that in Limerick Regional
Hospital and other acute general hospitals with unselected take (ie who take patients as they
come, not referred electively to a particular area of medicine).
TAB
LE 4
.1
Top 10 Principal Medical Diagnoses
Chest Pain 7.31 3.5
Obstructive Chronic Bronchitis with acute exacerbation 6.39 9.0
Respiratory system disease 5.75 8.2
Congestive heart failure 3.44 10.1
Syncope and collapse 3.34 4.1
Pneumococcal pneumonia 2.95 11.0
Alcohol abuse - unspecified 2.63 2.64
Inferior Acute Myocardial Infarction (Heart Attack) 2.52 9.0
Cerebral embolism (Stroke) 2.48 15.3
Intermediate coronary syndrome 2.13 8.6(Unstable angina)
TOTAL 38.94% 7.6
DIAGNOSES % OF OVERALL CASES ALOS (DAYS)The top 10 principal diagnoses at NENAGH HOSPITALare:
12 Integrated Management Returns, Department of Health & Children

SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital 42
* ALOS: Average Length Of Stay ** NEC: Not Elsewhere Classified
3.4.1.Quantifying the DemandThe internationally accepted safe level to avoid bed crises and ensure that patients get appropriate and
timely care is 85%.13 If the 49 beds were used 365 days a year, that would amount to available bed
days of 17,885 for General Medicine each year. Looking at the figure for 2004, the 49 beds accounted
for 2,656 in-patients. If we take an average length of stay of 6.9 days and multiply by the number of
patients, the number of beds days used on the medical floor at Nenagh Hospital in 2004 was 18,326.
This shortfall of 3,124 bed days per year underlines not only the volume of work being done at
Nenagh Hospital but also the shortage of resources with which to do it. The 3,124 bed day shortfall
TAB
LE 4
.2
Top 10 Principal Medical Diagnoses
Respiratory system disease 6 7.35
Chest Pain 5.5 3.80
Obstructive Chronic Bronchitis with acute exacerbation 5.4 7.92
Headache 4.2 3.43
Congestive heart failure 2.5 10.83
Syncope & Collapse 2.3 4.78
Pneumonia 2.2 11.89
Atrial fibrillation 2.1 7.42
Urinary Tract infection 2.1 6.55
Chest pain NEC** 2.0 5.03
TOTAL 34.3% 6.9
DIAGNOSES % OF OVERALL CASES ALOS* (DAYS)
The top 10 principal diagnoses at LIMERICK REGIONAL HOSPITAL are:
NO. OF BEDS NO. OF BED DAYSAVAILABLE
NO.OF BED DAYS USED
ANNUAL BED DAYSHORTFALL/SURPLUS
49 17,885 18,326 - 441
AT 85% BEDOCCUPANCY 15,202 18,326 - 3,124
TAB
LE 5
Comparison between General Medical In-Patient Bed Days Used and Available in 2004
13 Bagus, Place and Posnett, BMJ 1999, Dynamics of bed use in accommodating emergency admissions – a stochastic simulation model. Also citedin Acute Bed Capacity Review, 2002, DoH&C

43SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital
represents in real terms an average shortage of 9 beds. Within this average, there are a significant
peaks and troughs, with patient numbers on the medical floor rising to 70 patients on occasion.
3.4.2. Contribution to Mid West Regional Acute Medical ServiceThe medical service at Nenagh represents a significant percentage of the medical workload and
a sizable number of patients within the Mid West region, even when compared to the volume of
general medical work in the Limerick Regional Hospital. In 2004, of the 23,581 in-patients dis-
charged from Limerick Regional Hospital, 7,418, or 31% were general medical patients. These
patients used 56,135 bed days and had an average length of stay of 7.57 days.
Looking at the Department of Health’s Integrated Management Returns and HIPE data, we can
see that, together, Nenagh and Ennis account for a general medical workload equivalent to 86%
of that carried out by Limerick Regional Hospital. If we add St John’s 2,226 medical in-patients,
we can see that the three smaller hospitals treat 53.8% of general medical patients in the Mid
West region, and 51.5% of bed days used, ie the majority of medical patients in the Mid West
region are treated in the smaller hospitals.
Clearly, were the general medical service in any or all of the peripheral hospitals to start refer-
ring greater numbers of patients to Limerick Regional Hospital, this would put significant pressure
on the already overburdened system in Limerick Regional Hospital .
NO. OF BEDS NO. OF BED DAYSAVAILABLE
NO.OF BED DAYS USED
ANNUAL BED DAYSHORTFALL/SURPLUS
140 51,100 56,135 - 5,035
AT 85% BEDOCCUPANCY 43,435 56,135 - 12,700
TAB
LE 6
Limerick Regional Hospital General Medical Bed Days Used & Available
TAB
LE 7
Contribution to MidWest RegionalMedical Service
NENAGH HOSPITAL 4,367 2,656(61%) 16.5% 17,337
ENNIS HOSPITAL 5,523 3,755(68%) 23.4% 24,029
ST. JOHN’S, LIMERICK 3,964 2,226(56%) 13.9% 18,597
TOTAL 13,854 8,637(62%) 53.8% 59,963
LIMERICK REGIONAL HOSPITAL 23,581 7,418(31%) 46.2% 56,527
TOTAL 37,435 16,055(43%) 100% 116,490
TOTAL IN-PATIENTDISCHARGES
GENERAL MEDICALPATIENTS (%)
% OF MID WEST
REGION GENERAL
MEDICAL PATIENT
VOLUME
NO. OF BED DAYS
USED

SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital 44
3.4.3. Issues facing Medical Service at Nenagh Hospital
(I) LACK OF MEDICAL BEDS – OVERCROWDING, INFECTION CONTROL, SAFETY
As mentioned earlier, the physical space available in the hospital is in need of upgrade.
Currently, medical patients are housed on the ground floor in 4, 6, 8 or 10 bed wards, with some
single and two-bed rooms. Most of the wards were not intended to hold so many patients. As a
result, even when the hospital is operating at below 100% capacity, the beds are too close
together from the points of view of privacy and infection control.
In addition, the limited toilet facilities, as well as presenting obvious infection control issues, can
also prevent the hospital using the beds most efficiently, ie the wards are divided into male and
female. If there were more and improved toilet facilities (eg en suite facilities) in the right place,
some of the smaller wards could be used as female wards one day and male the next, depend-
ing on the need. This requires capital investment urgently.
A minor capital investment in these basic facilities would make a significant positive dif-ference to patient comfort, dignity and the ability of staff to control hospital-acquiredinfections.
(II) TRANSPORT OF PATIENTS
CT and Echo have become standard elements of investigations required by medical patients.
One of the biggest drains on resources at the hospital and on the regional ambulance service is
the transport of patients to Limerick Regional Hospital or elsewhere for CT scans, echo-cardio-
grams or other tests or procedures.
Since the appointment of the consultant cardiologist in November 2005, an echo machine has
been purchased and echo technicians have been appointed. Once this is operating, this will alle-
viate part of the burden on the ambulance service and nursing staff, who are currently transport-
ing patients to Limerick Regional Hospital for echo-cardiograms.
The biggest issue is around transport for CT scans. CT scans have become a routine clinical
tool. There are on average 2-3 in-patients daily from Nenagh Hospital who require a CT scan.
The current procedure requires that a CT scan appointment be booked in Limerick Regional
Hospital. Once an appointment has been booked, a fax is sent to ambulance control to book
ambulance transport. If the patient is on a stretcher, on an IV or is particularly frail or confused, a
nurse must accompany the patient in the ambulance. Once the ambulance arrives in Limerick
Regional Hospital, the nurse must remain to look after the patient. In practice, in the majority of
cases, a nurse travels with the patient.
• As the use of CT becomes more commonplace, the burden of operating an acute hospital
without a CT scanner on site becomes more onerous.
• In 2004, there were 544 referrals from Nenagh Hospital to Limerick Regional Hospital for
CT scans.

45SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital
• A CT run to Limerick will usually result in the loss of a nurse to the wards at Nenagh for at
least half a day.
Though every effort is made to organise for patients to have similar appointment times and
thus reduce the resources used up in this activity, some days there may be 2 or more nurses
absent for the best part of the day on ambulance runs to Limerick. It is estimated that the cost of
CT runs and other transport duties in terms of lost nursing time is between 300-400 nursing days
a year. Not only is it a significant drain on nursing resources, it is also a problem for the ambu-
lance service. Each transport uses up valuable ambulance time and two EMTs for about an hour
at a time in each direction. Occasionally, during very busy periods, the ambulance may not be
available in time to get the patient to their appointment and the patient has to return on another
day for their scan. Equally, for the same reason, a nurse and patient(s) may find themselves
stranded in Limerick until an ambulance becomes available to take them back. Both of these sit-
uations cause great distress to patients and families and at times cause risks to patient care.
There is, of course, also the hardship and stress the journey causes to patients who are
already very unwell. In some cases, doctors and nurses have to make a difficult call – do they
risk sending the patient for a CT or is the patient too ill?
A CT scanner has become a basic piece of equipment for managing acute illness. It willbe increasingly difficult for a hospital to operate as an effective acute unit without a CTscanner and the staff required to run it.
It is understood that funding will be made available for a CT scanning room and machine at
Nenagh Hospital. When it occurs, this will be a major benefit to patients in the Midwest Region.
3.4.4.Geriatrics• Acute Assessment/In-Patient Beds: The Elderly Care Unit currently has 8 beds for acute
assessment. There is a need for approximately 12 geriatric in-patient beds to meet the
population’s needs.
• Geriatric Day Assessment Unit is currently done in the Out-Patients Clinic, which is neither
efficient for staff nor comfortable for the patient, who has to wait on a chair in the waiting
room between tests, which can take half a day. A clinical assessment room on the medical
floor of the hospital is required. The nursing staff of the elderly care unit could ensure that
the patient is looked after and managed over the day, minimising the staffing requirement.
• Rehabilitation Beds. Adequate care in the rehabilitation phase of an elderly person’s illness
can make the difference between someone being able to live independently again or not.
Currently, there are no rehab facilities for elderly patients at Nenagh Hospital. This function
is carried out by Hospital of Assumption, which has 11 rehab beds. The recommendation is

SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital 46
for 3 beds per 1,000 of population over 65 years, with half on the general hospital site.
Nenagh Hospital should develop a 12-bed rehab unit in line with this recommendation.
Unlike large urban hospitals, until recently, North Tipperary has not suffered from the problem
of acute beds being filled with patients who are in need of rehab or extended care. Unfortunately
with the reduction in beds in the Hospital of the Assumption in Thurles from 130 to 72 beds, this
is likely to become a major problem, unless the deficit is addressed, eg the building of new 20
bed unit in Borrisokane or Nenagh.
3.4.5. CardiologyThe addition of a consultant cardiologist to the medical team at Nenagh Hospital is already hav-
ing positive effects, just months after the appointment. It is an excellent example of the significant
positive impact that investment in appropriate services can have on patient care and hospital effi-
ciency. There are strong links to the regional cardiology service and indeed, part of the work is
done in Limerick Regional Hospital (eg angiography and angioplasty), but the core of the service
has been moved closer to the patient in Nenagh Hospital. This is a positive evolution.
Previously, North Tipperary patients in need of angiogram/angioplasty would have to be kept
as in-patients at Nenagh Hospital, until a bed became available in Limerick. It was not unusual
for this wait to extend to two or three weeks, using up bed days unnecessarily and causing
unnecessary disruption and stress to patients and their families. Since the cardiologist has
been in post, the length of time that Nenagh Hospital patients have to wait for
angiogram/angioplasty has decreased, as the Nenagh-based cardiologist has direct access to
the equipment and can coordinate directly with the Admissions Office in Limerick to ensure
that patients are prioritised by clinical need. Over time, this will have a positive impact on aver-
age length of stay at Nenagh Hospital for cardiac patients.
Likewise, the addition of echocardiogram equipment and the recruitment currently underway of
technicians to run it, will have a positive effect on the services available to North Tipperary
patients. A cardiac rehabilitation nurse has been in place for some time. However, exercise facili-
ties, which will allow the full three-phase rehabilitation process to be offered, as per the National
Cardiac Strategy, are not in place. This is the next phase in the development of cardiac services.
3.4.6.Gastro-EnterologyA gastro-enterologist was appointed to Nenagh Hospital in 2000, working eight weekly sessions
in Nenagh and three in Limerick. The arrangement works well on a regional and local level. It
provides the region with an additional gastro-enterologist and an ERCP service for the region,
based in Limerick, which previously had been unavailable. It provides Nenagh Hospital with an
additional physician and a structured approach to the medical management of bowel and liver
conditions.

47SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital
The creation of an endoscopy unit to support this service has been planned for a number of
years. We discuss this in more detail in the Surgical Services section of the report.
3.4.7. Clinical Nurse SpecialistsThere are a number of clinical nurse specialists who provide very important specialist support for
medical patients and the hospital as a whole.
The areas they cover include:
• Diabetes
• Palliative care
• Gastro-Enterology
• Geriatric Liaison
• Cardiac Rehabilitation
• Haemo-vigilance
• Infection Control
Some of their work can be done on the wards when patients are in hospital. However, an impor-
tant part of their work and the service the offer is support to patients after they have left the hospi-
tal environment. At the moment, there is no consultation space for these specialist nurses to work
with patients. This, in some cases, makes it very difficult for them to give as much support to
patients as they could do. Space for Outpatient Clinics in general is an issue. More rooms are
needed to facilitate current clinics comfortably and additional rooms will be needed to allow for
more Limerick specialists to hold their clinics in Nenagh Hospital on suitable days.
3.4.8. ConclusionsDealing with acute medical patients is a core business of Nenagh Hospital. Overcrowding affects
the ability of staff to give patients optimum care. It has a detrimental effect on the patients who
suffer from lack of privacy and dignity. There are elements of the service, which are properly
resourced from a staffing perspective, but from which the patient does not get full benefit due to
physical lack of appropriate space.
Short Term & Medium Term• Extra medical beds and the nursing resources for them are required immediately. The cur-
rent deficit is 9 in-patient beds. However, this number could be considerably lower if some
of the other items suggested were provided.
• There is no space on the medical floor for any more medical beds, therefore space must
be found elsewhere in the hospital. The most appropriate space available immediately is
the space on the upper floor currently used for storage (old ward)
• A CT scanner is required to meet clinical needs and alleviate pressure on patients, nursing
staff and the ambulance service and reduce length of stay

SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital 48
• Clinical assessment room should be made available for use for geriatric day assessment,
and clinical nurse specialists and others.
• The de-commissioned mortuary could be adapted for use as a cardiac rehabilitation exer-
cise facility.
• Smaller wards and single rooms are also required to aid infection control.
• Build en suite facilities in wards.
• The creation of a geriatric rehabilitation unit will improve outcomes for older patients and fill the
gap left by the reduction of bed numbers in Hospital of the Assumption, Thurles, from 130 to 72.
• Increased space for Out-Patient Clinics is required.
Expected Impacts• Beds on corridors will cease. Every patient will have the privacy and dignity they deserve.
• Effective infection control will become more possible.
• The organisational and manpower burden of the CT runs will cease and patients will not
have to travel to Limerick and be in an unfamiliar environment for the best part of a day.
• Immediate access to CT and less pressure on the ambulance service should have a positive
impact on average length of stay, as fewer patients’ treatment will not be held up while waiting
for the results of tests or as result of missed scans due to unavailability of ambulance transport.
• Increased service for patients and better work flow and efficiency.
• The availability of isolation rooms and smaller wards will make effective control of hospital
acquired infection more possible, as will improved sanitary facilities.
• The geriatric rehab unit and geriatric day assessment unit will ensure that optimum service and
support can be offered to elderly patients, improving their chances of staying independent and
out of long term care.
3.5 SURGICAL SERVICES
Nenagh Hospital has 26 surgical beds and 6-day beds, which are mostly used for surgical and
endoscopy work. The in-patient workload is largely General Surgery and Urology. There were
1,522 surgical in-patients and 7,267 surgical bed days used in Nenagh Hospital in 2004. The
average length of stay for in-patients was 4.77 days. There were 2,869 day cases the majority of
which were day surgery or scope procedures, bringing the overall number of operative proce-
dures to over 3,500 in 2004.14
The surgical team at Nenagh Hospital consists of 2 consultant general surgeons, with a con-
sultant urologist and a consultant gastro-enterologist also using the operating theatres. They are
supported by 3 consultant anaesthetists, 7 surgical and 2 anaesthetic NCHDs, 18 surgical nurses
on the wards, 10 theatre nurses and 2 theatre porters. As in the medical wards, there are “unoffi-
cial beds” which allow the service cope with peaks in demand. There are 9 unofficial in-patient
beds and 8 unofficial day beds on the surgical floor.
14 All figures in preceding paragraph from HIPE data, Nenagh Hospital, 2004.

49SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital
To look at what Nenagh contributes to surgical services in the mid-West, we have looked at
HIPE figures for both Nenagh Hospital and Limerick Regional Hospital. Clearly, Limerick Regional
Hospital can treat a wider range of conditions because regional specialties (eg orthopaedics, ENT
etc) are centred there. Where possible we have tried to make the figures comparable.
TAB
LE 8
10 Most Common Diagnoses in General Surgical In-PatientsThe 10 most common diagnoses for general surgical in-patients at NENAGH HOSPITAL are:
Abdominal Pain (RLQ) 4.93 2.96Acute Appendicitis 4.40 4.0Gallstone operation 3.94 6.0Head Injury 3.35 1.5Unilateral inguinal hernia 3.29 3.4Gallstone problems without operation 2.89 4.1Hematuria (blood in urine) 2.76 5.3Diverticulosis of Colon 2.43 6.4Renal Colic (kidney stone) 2.17 2.3Cellulitis of leg (infection) 1.84 8.4
TOTAL 32% 4.23
DIAGNOSES % OF OVERALL CASES ALOS (DAYS)
The 10 most common diagnoses for general surgical in-patients at LIMERICK REGIONAL HOSPITAL are:
Acute Appendicitis 7.15 3.66Hyperplasia of prostate (enlarged) 3.33 7.23Unilateral inguinal hernia 3.30 2.91Gallstone problems without operation 3.24 4.16Abdominal pain (NOS) 2.79 2.76Head injury 2.12 1.48Abdominal pain (RLQ) 1.89 2.25Constipation 1.82 3.39Gallstone operation 1.73 5.39Peripheral vascular disease 1.63 22.24*
TOTAL 29% 3.69
DIAGNOSES % OF OVERALL CASES ALOS (DAYS)
( * Not included in average figure as the ALOS is so different.)

SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital 50
The Nenagh Hospital surgical service is extremely efficient. At Nenagh Hospital, there are
currently only 48 patients on the general surgery OPD waiting list for one month or less and in-
patient waiting lists are equally good. In contrast, there are currently 1,227 patients on the
OPD waiting lists for a general surgery consultation in Limerick Regional Hospital, over half of
whom have been waiting over six months.15
There are two theatres at Nenagh, which are operated in tandem. In line with best practice,
most surgical work at Nenagh Hospital occurs within normal working hours. Emergency surgery
from the previous day’s on-call can usually be accommodated without cancelling procedures
from the day’s surgical list. When the theatre list over-runs, it can usually be completed by
7.00PM. This means that emergency operations during the night happen only in exceptional
cases in line with CEPOD16 recommendations. In other hospitals, due to lack of theatre time by
day, emergencies have to be fitted in out of hours, which has been established to be less safe
for patients.
The day ward is situated beside the surgical in-patient wards and uses nursing time and support
from the surgical wards when necessary or possible. Looking at the top 10 general surgical diag-
noses, we can see that what Nenagh and the Limerick Regional Hospital are doing are largely the
same, with the exception of vascular surgery. The number and type of operation per surgeon is
similar. The number of surgical in-patients per surgeon is comparable with 760 per surgeon in
Nenagh Hospital and 627 per surgeon in Limerick Regional Hospital.
NO. OF BEDS NO. OF BED DAYSAVAILABLE
NO.OF BED DAYS USED
BED DAYSURPLUS/SHORTFALL
26 9,490 7,267 + 2,223
AT 85% BEDOCCUPANCY 8,066 7,267 + 799
6 DAY BEDS 1,566 2,869 - 1,303
TAB
LE 9
NENAGH HOSPITAL Surgical Bed Days Used & Available
15 Figures from HSE response to PQ27336, Nov 0516 National Confidential Enquiry into Patient Outcomes and Deaths, UK, 2000
TAB
LE 1
0
Surgical In-patients Per Surgeon 2004
NENAGH HOSPITAL 4,367 1,522 2 761
LIMERICK REGIONAL HOSPITAL 23,581 3,133 5 626.6
ENNIS HOSPITAL 5,523 1,696 2 848
ST. JOHN’S, LIMERICK 3,964 1,306 2 651
TOTAL IN-PATIENTDISCHARGES
GENERAL SURGERY GENERAL SURGICALPATIENTS
NO. OF
CONSULTANT
GENERAL
SURGEONS
NO. OF PATIENTS
PER SURGEON

51SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital
It is difficult to make a straight forward comparison between hospitals in the Mid West and
Dublin Teaching Hospitals. However, Dublin hospitals are recognised to have larger numbers of
staff at consultant and NCHD levels relative to the number of patients that they treat.
General Surgical Beds in Limerick
To take a comparable look at bed days and surplus/shortfall in Limerick is difficult, as beds
appear not to be specifically designated by specialty in publically available information. There are
119 beds designated as general surgical beds.17 The figure of 3,133 (HIPE Limerick) represents
general surgical in-patients discharged.
There are 183 surgical beds in Limerick Regional Hospital. Some of these beds are specifically
designated to specialties eg 25 beds for Gynaecology, 23 beds for ENT patients etc. However,
specialties such as Urology, Maxio-facial, Vascular and Orthopaedics have no designated beds,
but come under the umbrella of the 119 beds designated for General Surgery. We have included
the figures from these specialities under General Surgery so that a fair reflection of bed use can
be identified. Most surgery is done Monday-Friday. 5-day surgery is increasingly the norm. This
creates peaks of demand for in-patient beds during the week.
Looking at the figures, it is clear not only that closing or reducing surgery at Nenagh Hospital
would
1. Add a significant amount of work onto an already overburdened system in Limerick, but
2. That Nenagh Hospital could contribute in-patient capacity and general surgery to the
needs of the Mid West region.
Currently, 5 out of 10 surgical sessions (half-day) in Nenagh Hospital are used for scoping
procedures. The creation of an endoscopy unit, as currently planned, would free up further the-
atre time for use by the region. By offering theatre time to surgeons based in Limerick
Regional Hospital for day procedures for which North Tipperary patients are currently travelling
to Limerick, (eg ENT, Gynaecology, Orthopaedic and Maxillary Facial) would ensure more
timely and convenient care for patients in North Tipperary and alleviate the pressure in
Limerick. Limerick-based surgeons have expressed interest in doing this.
NO. OF BEDS NO. OF BED DAYSAVAILABLE
NO.OF BED DAYS USED
BED DAYSURPLUS/SHORTFALL
119 43,435 42,324 +1,111
AT 85% BEDOCCUPANCY 36,920 42,324 -5,404
TAB
LE 1
1
Limerick Regional Hospital General Surgical Beds Days Used and Available
17 Dept of Health & Children data 2004.

SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital 52
Day Surgery
International trends and developments in surgery are leading to a consistent increase in non-
invasive and minimally invasive procedures (key-hole surgery), which are performed by radiolo-
gists and specialist physicians as well as surgeons (eg endoscopy and angioplasty). More pro-
cedures can be performed on a day case basis. Nenagh Hospital has followed this trend and
the number of day cases has increased to 2,869 day cases treated in 2004.
There are 6 “official” day beds at Nenagh. However, there are 14 physical beds in daily use. All
beds are primarily used for surgical procedures. At present, the day ward operates 5 days a
week (approx 260 days a year) from 8.00AM to 5.00PM. It is staffed by 2 nurses, plus a ward
clerk for half a day.
*Ophthalmologic day surgery is not included as it does not come through the day theatre
In examining the future of a hospital like Nenagh with a small surgical unit, staffed by two con-
sultant surgeons, the mechanism by which surgical services should be provided requires careful
consideration. The Hanly Report in 2003 suggested moving all in-patients to Limerick. Since
then, nothing has happened. It has become clear that there is no space in Limerick Regional
Hospital even for the current general surgical workload, nor is there any move being made to
create more space.
There are a number of questions that one has to address to consider the issue properly:
• Is there an adequate volume of work to justify a 24/7 surgical team?
• Is it possible to expect surgeons to work on a 1 in 2 rota, ie on call 24 hours every second
day?
• What would the loss or diminution of the surgical service at Nenagh Hospital mean to the
safety profile of the hospital as a whole?
• Most importantly, is it as safe to do surgery at Nenagh Hospital as it is in Limerick
Regional Hospital, ie does the volume/outcome argument stand up?
• If it is safe, how can Nenagh alleviate the overall surgical workload pressure within the
region?
TAB
LE 1
2
Day Surgery in 2005
NENAGH HOSPITAL 6 2,869 478
LIMERICK REGIONAL HOSPITAL 16 6,568* 410
ENNIS HOSPITAL 6 2,062 343
ST. JOHN’S HOSPITAL 5 1,864 373
NO. OF BEDSGENERAL SURGERY NO. OF DAY CASESCASES PER
YEAR PER BED
SURGICAL DAY BEDS SURGICAL DAY CASES

53SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital
Future of Surgery at Nenagh Hospital
An Acute Hospital Without Acute Surgery?
In looking at surgery at Nenagh Hospital, one has to look it as a key part of a functioning sys-
tem of acute care. There are strong fundamental clinical reasons why hospitals have both
acute medical and acute surgical services under one roof. Where situations have evolved
where that does not exist (eg Cashel Hospital and Clonmel Hospital) the outcome has proved
unsatisfactory. The division between medical and surgical care is one which may make
sense on paper, but it is a distinction that the human body does not recognise.
Surgeons provide valuable support to specialist colleagues in general medicine and geriatrics,
particularly in the diagnoses of the “acute abdomen”. Currently, approximately 12-15 medical
patients require surgical consultation each week. This is higher with older patients who are often
suffering from multi-system failures and whose clinical presentation is rarely clear-cut.
It is of huge clinical benefit to the patients of North Tipperary to have a hospital, which provides
full acute secondary care on a 24/7 basis. Any change must represent improvement not reduc-
tion in service. Surgery at Nenagh Hospital has cultivated close links with regional and national
quality control systems to ensure safety for patients. Audit of outcome and comparison with the
results of other hospitals is routine.
The impact on Limerick Regional Hospital of removing acute surgery from Nenagh, would
be much greater than the requirement to absorb the 1,522 in-patients. In addition, any acute
medical patients requiring surgical consults, or suspected to require one, would also be like-
ly to be referred to Limerick Regional Hospital, especially elderly patients. As we have
established, Limerick Regional Hospital appears to be about 5,400 bed days short to deal
with its current annual general surgical workload. Add to this the extra pressure on theatres
already working at capacity and the fact that 9 out of 10 Nenagh admissions are non-elec-
tive, and the situation clearly becomes untenable, both for patients and staff at Limerick
Regional Hospital.
In the Mid West network, the surgical service is under pressure. One of the biggest difficulties
is the pressure that emergencies put on the system’s ability to get through elective procedures.
A study on the impact of emergency admissions on elective surgical workload in James Connolly
Memorial Hospital found that in a three-month period, 40.4% of all planned cases were can-
celled. Bed unavailability was the primary cause for cancellation.18 Because of Limerick Regional
Hospital’s responsibility for major trauma and other major surgical interventions, cordoning off
elective surgical time is very challenging. Minor and intermediate day and in-patient surgical lists
can suffer as a result.
The Department of Surgery in Limerick Regional Hospital is currently planning an emer-
gency-only theatre. This is a positive and necessary addition to the regional surgical service. It
will ensure that major trauma and major surgical emergencies can be dealt with quickly and
efficiently. However, it will not remove the need for on call emergency surgery in Ennis or
Nenagh.
18 Nasr, A. et al, Vol 173, No.3, Irish Journal of Medical Science, Impact of Emergency Admissions on Elective Surgical Workload

SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital 54
Reacting to a Changing Environment - Safely
As a discipline, surgery is currently going through a major evolution. Significant developments in
anaesthesia, minimally invasive surgery and post-operative analgesia have made it possible for
an increasing number of procedures to be performed on a day case basis. There has been a
resulting reduction in the number of surgical bed days used right across the system. From 1995-
2000, there was an 8% decrease in Bed Days Used by surgical patients.19 Acute surgical servic-
es in Nenagh Hospital and elsewhere need to evolve and adapt to a changed and changing situ-
ation. However, it must be done:
˙On a planned and phased basis
˙In the context of what services are consistently and reliably available elsewhere in the
regional and national network of acute care.
This context is:
˙Surgical services in the Limerick Regional Hospital are over-burdened and struggling to
cope with the volume of work they already have. The Limerick Regional Hospital is already
short an estimated surgical 5,400 bed days per year. Nenagh Hospital’s surgical workload
represents an additional 7,260 bed days.
˙The system of inter-hospital transfer is unreliable.
˙The ambulance service is currently under-resourced and under-developed to cope with the
increased need for transportation that would result from all or even some North Tipperary
surgical or suspected surgical patients being sent to the Limerick Regional Hospital.
˙Cancellation of elective surgery due to lack of beds or theatre time is a regular problem in
Limerick Regional Hospital. It is not a problem at Nenagh Hospital.
˙Nenagh Hospital has proved itself good managing day surgery.
˙Medical as well as surgical in-patients at Nenagh Hospital require input from surgeons to
ensure the highest standard of care.
Any plans for the future of surgery at Nenagh Hospital need to be made in this context. The
first priority has to be to use the capacity available to help to alleviate the pressure on the sys-
tem regionally, while ensuring that there is no loss of service to the people of North Tipperary.
Over the next five to ten years, we can expect to see the trend towards day surgery contin-
ue. Increasingly, it will need to be done in special day surgery units that are designed for
maximum effectiveness and efficiency. Similarly, the demand for diagnostics will continue to
grow. There are a range of conditions which, with the right resources and organisation (eg
minor surgery) could be diagnosed and treated on the same day, removing the need for an
out-patient visit, ie the General Practitioner could refer directly to the day surgery suite in
some cases.
Nenagh Hospital should develop a Diagnostic and Treatment Centre, part of the main hospital
but with easier access for General Practitioners and more integrated with primary care. This
would include an up-to-date operating and day surgery suite specifically designed to ensure a
19 Acute Hospital Bed Capacity- A National Review, 2002, p39.

55SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital
smooth flow of work, removing the inefficiencies and delays that are caused by the less than
ideal operating theatre and layout of facilities that are currently available. In the context of the
proposed plans to centralise, we must consider directly the concept of all North Tipperary surgi-
cal emergencies or those which occur after hours (ie between 5.00PM and 8.00AM) going direct
to the Limerick Regional Hospital with the on call surgeon based at the regional centre.
In doing that, we need to ask two questions:
• Would it improve patient safety?
• Would it improve patient outcomes?
As well as the lack of bed capacity in the Limerick Regional Hospital, the over-burdened
ambulance service and the on-going problems with inter-hospital transfer, seriously ill patients
must also be considered. There are a number of cases each month where the consultant sur-
geon on call is asked by the registrar on site to make a decision over the phone, or to come in
to operate on someone after 9PM. Though the number is small, these cases are usually very
serious, eg in the six months from July 05 to January 06 there have been a major trauma,
burst abdomen, a testicular torsion and a perforated ulcer. These patients were a combination
of A&E self-referrals, ambulance cases and medical in-patients developing complications. In
some of these cases, eg perforated ulcer and burst abdomen, the patients would have been
unlikely to have made it to Limerick.
There is a sequence of events and developments that must occur for the any transition or
change to services to be smooth and safe for patients in North Tipperary. The tragic events in
Monaghan are an example of how easily the system can fail patients and staff if inappropriate
changes are made and then these changes come into effect without full and detailed prepara-
tions being made and protocols agreed by all parties likely to be affected by the change. Looking
at the current situation and conditions, it is impossible to see how the proposed plans to cen-
tralise could lead to anything but increased risk and reduced access to care for the patients of
North Tipperary at present. We have established that there are no benefits to patient service and
no benefits to patient safety in moving all or some acute surgical work from Nenagh Hospital to
Limerick Regional Hospital.
• The majority of the work of the general surgical unit in Nenagh and in Limerick is the same
and the outcomes are comparable
• The types of patients who would benefit from intervention by specialists in a particular
area are already being transferred to the most appropriate facility.
• Not only is there a demand for the work done by Nenagh Hospital surgical department,
there is also a shortage of space and places to do it, within the region.
• Removing acute surgery at night would increase the likelihood of patients in Nenagh
Hospital needing treatment in breach of protocol.

SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital 56
ConclusionsShort Term
•Acute surgery is a core element in the service offered by Nenagh Hospital. While the surgi-
cal service in Limerick is under such pressure, reducing or removing the emergency surgi-
cal service in Nenagh can only lead to a decrease in patient access to care and compro-
mise the safe management of emergencies.
• Day surgery – Nenagh Hospital is particularly efficient. This strength could be developed
further through the development of an improved theatre flow and a small increase in staff.
•There is surgical capacity at Nenagh, which is badly needed within the region. Finding a safe
and efficient way to use this capacity would be a considerable asset to the mid-west regional
surgical service. For example, appropriate waiting list patients could be offered their general
surgery in Nenagh and direct admission rights could be offered to General Practitioners out-
side the North Tipperary catchment area for both surgical and medical patients.
• Nenagh Hospital could alleviate some pressure within the region by making theatre time
available to surgeons from Limerick Regional Hospital. It would allow the ring fencing of a
certain amount of valuable theatre time for elective surgeries. This would be most suitably
used for day surgery as continuity of care could be an issue with in-patients.
• 24/7 emergency surgery must continue at Nenagh Hospital as an important support to the
acute medical service. If there was no surgical expertise on site, all 1,500 plus surgical in-
patients and great many more medical patients would need to be transferred to Limerick
Regional Hospital especially elderly patients with multi system problems that would require
a surgical consult to ensure patient safety.
• The two consultant surgeons cannot continue on a one in two on call basis. A third surgeon
is required at Nenagh Hospital.
• Clearly defined and agreed plans for improving inter-hospital transfer and patient transport
must be made, tested and implemented.
Expected Impacts:
•Day surgery at Nenagh Hospital becomes busier and requires additional space and nurses.
•Patients who need day surgery in the areas of, for example, gynaecology, ophthalmology,
ENT etc can have their procedures performed locally in Nenagh.
•Emergency surgical patients continue to be operated on as is happening currently.
•Acute medical patients with possible surgical problems will not need to be transferred to
Limerick Regional Hospital.
•Nenagh Hospital contributes to bringing down waiting lists.
• Theatre time in Limerick is protected for patients who will really benefit from the multi func-
tional surgical team.
•Clarity around the future of the service improves staff morale and patient trust.
57SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital
Medium Term
• In the medium term, this would require investment in a new theatre suite with an improved
process flow to maximise efficiency. This would be developed together with the endoscopy
suite to create in Nenagh a fully functioning diagnostic and treatment centre for day proce-
dures.
• To create a viable, future-proof centre, it would make more sense to build once and add the
new theatres/day ward and extra radiology space when expanding the A&E and laboratory
in 2006. This centre would be a resource not just for the hospital, but also for primary care.
All the services could be readily accessed in one purpose built, modern wing. This would
have the added advantage of creating much needed space in the body of the hospital, solv-
ing many of the physical overcrowding and infection control issues on the in-patient wards.
• Surgical services in the region should be reviewed at the end of each year to look at work-
load distribution and outcomes, bed usage, cooperation and communication, improvements
to inter-hospital transfer etc and plans adapted on the basis of progress made.
Expected Impacts
• The new build housing the diagnostic and treatment centre will have positive impacts not
just on the surgical and diagnostic services but right across the hospital.
• It will create a diagnostic and treatment centre that provides service to both primary and
secondary care.
• It will create much needed space in the body of the hospital, ensuring that overcrowding of
medical in-patients can come to an end.
• This would have a number of positive impacts in terms of infection control. It would allow for
smaller wards, more space between beds, isolation rooms/single rooms for infectious
patients, the addition of better toilet and bathroom facilities, the creation of space for proper
storage of clinical supplies and linens, full changing facilities for staff and make available a
room where staff could talk to patients or their families in private.

SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital 58
3.6. DIAGNOSTIC SERVICES
One of the clearest trends in healthcare in recent years is the constant rise in demand and use
of diagnostic tests and examinations (eg CT scan). Reliance on diagnostic tests and examina-
tions as an aid to and confirmation of diagnosis has grown amongst doctors because so much
more can be done for patients. Diagnostic tests and examinations have become more reliable,
sophisticated and applicable to a wider range of conditions. This has also contributed to the
rapid and continued rise in demand for diagnostic services.
The radiology and laboratory services at Nenagh Hospital provide diagnostic services not
only for the acute hospital, but also for all General Practitioners and other health profession-
als and institutions across North Tipperary. They have seen a constant increase in demand
for their services over the last few years, both from the hospital and from General
Practitioners. Though efficient and providing an excellent service, both lab and radiology serv-
ices are under significant pressure to keep pace with demand. The HSE has committed to
improving access to diagnostics, especially for GPs. This cannot be done without investment
to expand services.
3.6.1.Radiology ServicesThe Radiology department provides services for in-patients and out-patients and North Tipperary
General Practitioners. It provides a service for general radiology, barium studies, urography, spe-
cialised interventional procedures and ultrasound procedures. The Radiology Service in the Mid
West operates as a regional service and there are close links and cooperation with the radiology
team in Limerick Regional Hospital, who supply certain specialised tests which are unavailabel in
Nenagh, including CT scanning. In 2004, the number of radological examinations carried out at
Nenagh Hospital was 21,030.
Radiological services at Nenagh Hospital are provided by a consultant radiologist and a
team of 4 radiographers (Whole Time Equivalent or WTE), supported by 2 clerical staff, a
radiography technician and a staff nurse. The team is currently running at full capacity, with
each radiographer performing on average 5,500 examinations a year.20 Requests for on
call radiography have increased considerably in the last year and an increasing number of
calls are occurring post midnight, rising from 55% in 2003 to 73% in 2005. With a small
team operating on a 1 in 5 on call rota and inadequate recovery times allotted, the burden
on the team is significant.
The team has coped with increased demand from General Practitioners and the addition of
new services at the hospital (eg rheumatology and cardiology) without additional support or staff.
However, with the current staffing levels, it would be very difficult to increase capacity to meet
growing demand without jeopardising the quality of the work carried out.
20 This is above the NHS recommendation of 3,000 examinations per year per radiographer as an acceptable and manageable workload.

59SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital
As mentioned previously, a CT scanner has become a basic piece of equipment for man-aging acute illness. It will be increasingly difficult for a hospital to operate as an effectiveacute unit without a CT scanner and the small number of extra staff required to run it.Both new and existing staff would be involved in the CT scanning service, adding to thestaff available for general and on call work, thereby strengthening the service across theboard.
3.6.2. Laboratory servicesThe pathology laboratory at Nenagh Hospital serves the needs of the hospital and the General
Practitioners of North Tipperary. It provides services in the areas of biochemistry, haematology,
blood transfusion and microbiology and provides on-site front line tests essential for diagnosis
and treatment of disease by clinicians. The Nenagh Hospital laboratory works closely as part of
Mid West regional network of laboratories. More specialised tests and histology are referred to
the regional laboratory. There is a regular taxi run once a day from the Nenagh lab to the region-
al lab in Limerick Regional Hospital. This limited transport link can slow down response time,
especially for infection control.
In line with national and international trends, the demand for tests has grown dramatically
over the last few years from 123,773 tests in 2001 to 176,372 in 2005, an increase of approxi-
mately 42.5%. The number of on call test requests (between 5.00Pm and 8.00AM and at
weekends) has increased to over 20,000 requests, or by over 50%, in the same period.
Approximately 60% of the work originates from General Practitioner requests. The laboratory
team includes chief medical scientist and 6 WTE. Current facilities and storage are inade-
quate. Plans for a new larger lab as part of a redevelopment of the A&E and radiology area
has been accepted by the HSE. Confirmation of when the project will begin has not been
received.
3.7. OTHER SERVICES
3.7.1. Acute Psychiatry in North Tipperary – the missing service
Current ServicesThe mental health needs of the population of North Tipperary are served by a small but dedicated
team of 2 consultant psychiatrists, 3 psychologists and 2 Social Workers and community psychi-
atric nurses. There are no Occupational Therapists, no Cognitive/Behavioural therapists and no
Family Therapists for the county.
North Tipperary has one of the highest suicide rates in the country.

SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital 60
The biggest problems are with acute psychiatry. The 9AM-5PM acute psychiatric service in
North Tipperary, while under-resourced, provides a significant level of service. There are no
acute psychiatric in-patient beds in Nenagh Hospital, or in North Tipperary at all. Acute psychi-
atric patients from North Tipperary must access in-patient mental health care in Clonmel, in the
HSE South Eastern Area, while in-patient care for all other medical specialities is based in
Nenagh or in Limerick, in the HSE Mid Western Area. This anomaly is based on historic catch-
ment areas for the old mental hospitals and leads to difficulties in coordination and develop-
ment of services as well as creating problems with access to care. Travel time from Nenagh to
Clonmel is 1.5 hours and up to 2 hours from some parts of North Tipperary.
The biggest psychiatric service deficit is during on call hours, that is, after 5.00PM and at week-
ends. The on call service is provided by Clonmel, which can provide in-patient care. In many
cases, in-patient care is not the most appropriate treatment option for the patient. When it is,
there is rarely a bed available for North Tipperary patients. This is a very serious problem for
patients, their families and their General Practitioners and for Nenagh Hospital.
For example, a patient who presents to their GP late on Friday afternoon, and is suffering
from a mental illness that makes him a danger to himself or others, may not receive appropri-
ate treatment until the following Monday, unless the family are willing to commit the patient
against their will. Families and the GP have to try to cope with a patient, who may be dis-
turbed, frightened or violent in the family home for up to two days. This situation is dangerous
and upsetting for the patient and their family. It is very time-consuming for the GP, who is
effectively burdened with clinical responsibility for a patient, who they have identified as need-
ing specialist care, for over 48 hours.
Nenagh Hospital has no facilities or specialist staff for treating acutely mentally ill patients.
Despite this, patients present at the hospital, where general medical staff do their best to
manage the patient while trying to access acute psychiatric assessment and treatment. This
puts both patients and hospital staff at risk. A report by the Mental Health Commission in
2004 pointed out the inadequacy of mental health services in the county. It stated “The
unsatisfactory situation regarding the North Tipperary services must be resolved as a matter
of urgency”. 21
There have been discussions for over 20 years about a 24-bed acute psychiatric in-patient unit
in Nenagh, with 22 beds for general adult mental health service and 2 beds for the mental health
services for the elderly. However, it was felt that this plan should be reviewed in light of a subse-
quent policy, which promoted the development of an advanced community-based model of men-
tal health care, including home-based care. There have been no significant moves in this direc-
tion. The Mental Health Commission Annual Report 2004 further recommended that while the
local facilities were being developed, admissions from North Tipperary should be accommodated
in the acute unit in Limerick and admissions to Clonmel should cease. None of the above has
happened in the intervening 18 months.
Another significant problem occurs in the management and treatment of patients with alco-
holism. “Drying out” of patients is seen as a medical intervention and is looked after in acute gen-
21 Mental Health Commission Annual Report, 2004, Dept of Health & Children

61SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital
eral hospitals. However, while there are important physical issues related to the condition (eg risk
of fits), the psychological and psychiatric elements of care are extremely important. There are
also questions over how appropriate it is to mix these patients with more typical medical patients.
Once dried out, the patient is then moved to Clonmel to complete the treatment. Where a patient
is willing to be admitted, the situation can be managed in this way, though with difficulty.
Where the patient is unwilling to be admitted, there are added problems and anomalies in the
system. An acute general hospital cannot admit a patient against their will – this is only possible
for acute psychiatric units. This means that the patient in question cannot come to Nenagh
Hospital to be dried out and that Clonmel is unwilling to take the patient until they have dried out,
because of the medical risk of fits etc during the drying out process. This can leave very vulnera-
ble patients in limbo. The most appropriate location for a treatment centre for alcohol abuse is in
the psychiatric wing of an acute hospital, where the patient can be primarily treated for their psy-
chiatric problems but with acute medical care available near at hand should it be required.
Conclusions• Provide on call acute psychiatric services 24/7 in North Tipperary immediately
• While local facilities are being developed, admissions from North Tipperary should be
accommodated in the acute psychiatric unit in Limerick
• Develop the community based service
• Provide in-patient beds in Nenagh or Limerick for North Tipperary patients


63SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital
THE NATIONAL ISSUES AND HOW THEY AFFECTSMALLER ACUTE HOSPITALS
The future of small rural hospitals is an issue for debate in countries other than Ireland.
Internationally, the viability of small acute hospitals in rural areas has been threatened by declin-
ing levels of population and economic activity, though this is not the case in Ireland where popu-
lation and economic activity levels have been rising steadily. More importantly, however, there is
the desire to control and reduce public spending on health, problems of recruitment and retention
of health professionals and a more economic rationalist approach to the funding and provision of
services.
This issue has been underlined in recent years in Europe by the implications of compliance
with the European Working Time Directive (EWTD) and the impact that that will have on the cost
of manning the health service appropriately. The solution suggested for Ireland, to centralise
acute hospital services and change the function of smaller acute units, as proposed in the
National Taskforce on Medical Staffing (Hanly et al, 2003) met with considerable resistance, not
least from local communities. The debate that has ensued has been quite damaging, with the
quality of care in small acute hospitals being constantly undermined, by careless comments and
stagnation in planning.
The key questions that any small acute unit needs to be able to address in looking to its future
are as follows:
• Patient Safety: Are small acute hospitals safe?
• Cost vs Contribution: Can we afford to have “a hospital at every cross-roads”?
• Medical Staffing: How can we staff them and be European Working Time Directive
(EWTD) compliant?
• Is there a critical mass of services for a viable, safe acute hospital?
4.1. PATIENT SAFETY
Patient safety must be of primary concern to all – policymakers, managers, healthcare workers
and local communities. There is a large body of literature looking at the different factors affecting
patient safety. The key issue for smaller acute units centres on surgical rather than medical
patients. In the media, we hear about “international expert opinion” equating the size of the acute
unit with outcomes for patients.
4.1.1. Volumes & OutcomesThere is little doubt that the outcome from surgical operations is dependent on the technical skill
of the surgeon, anaesthetist and nurses. Equally, surgeons know that patients with significant
other illnesses are more likely to get complications. It is therefore important that surgeons choose
their patients carefully and vice versa.
4.
SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital 64
Much of the debate and a lot of the arguments in favour of centralisation focus on volumes and
outcomes, with the received wisdom being that multi-disciplinary teams in large, specialist units
who treat large numbers of patients achieve better outcomes. This is believed to be particularly
true in surgery.
For example, for most cancers, there are benefits which come from a multidisciplinary approach
to diagnosis and treatment. A distributed service across several hospitals makes this multidiscipli-
nary approach much more difficult to achieve. High volume providers have a significantly better
outcome for complex cancer surgery, specifically of the pancreas, oesophagus, stomach and rec-
tum. Improved long term survival rate is another matter and may depend more on the quality of
supportive treatments such as chemotherapy and radiotherapy, eg cancer of the breast.22
However, the debate is not as one-sided as it appears. The evidence is not as clear-cut as one
would expect in view of the current policy, which pushes strongly in favour of centralisation of all
but the most minor surgery.
The York Report,23 one of the studies most commonly cited in support of centralisation of serv-
ices, actually concludes that there is no direct causal link between volume and outcome. It ques-
tions the methodology on many of the studies which conclude that high volume means better
outcomes. The York Report is, however, helpful in identifying the procedures and specialities in
which high volume has been proven to lead to better outcomes. All of these are already cen-
tralised to national units in Ireland eg pancreatic cancer surgery, oesophageal cancer surgery,
paediatric cardiac surgery, treatment of AIDS and surgery for un-ruptured aortic aneurysm.
Similarly, other studies have shown that there is a wide variation in reports from different hospi-
tals and different countries. There are questions about the quality of the data,24 which reviewed all
the studies on volume and outcome in the US between 1980 and 2000, was highly critical of the
lack of rigour in many hospital/outcome studies. They found that those studies that performed
risk adjustment by using clinical data were far less likely to report significant associations
between volume and outcome than those relying on administrative data.
Another recent article, co-written by an advocate of centralisation of the treatment of sympto-
matic breast cancer25 states:
“The present study analysed each unit separately and showed that volume did not corre-
late well with adequacy of treatment; nor was there any discernible cut-off number below
which treatment suffered. The justification for recommendations for breast cancer speciali-
sation into super-units appears flawed both by statistical rationale and evidence.”
In addition there are studies from Sweden, from Germany and the US, looking at everything
from treatment of Myocardial Infarction to gall bladders and hip fractures, which also question just
how far the volume/outcome argument can be taken. They found that individual surgeon skill was
more important than the size of the unit and that small clinics and large units following the same
protocols got similar results.
22 Provider volume and outcomes for oncological procedures, Kileen S.D., O’Sullivan M.J., Coffey, J.C., Kirwan,W. Redmond, H.P. British Journal ofSurgery, 2005; 92:389-402.23 Amanda Sowden et al, Concentration and choice in the provision of hospital services: the relationship between hospital volume and quality ofhealth outcomes CRD Report 8 Part 1, York University Centre for Health Economics, January 199724 Systematic Review of the Quality of Surgical Mortality Monitoring, Russell, E.M., Bruce J., Krukowski, Z.H. British Journal of Surgery 2003;90:527-532). An US study EA Halm et al. “Is volume related to outcome in health care? A systematic review and critique of the literature?” AnnIntern Med 2002 Sep 1725 Kingsmore, D.B. Hole, D.J., Gillis, C.R. and George, W.D. British Journal of Surgery 2005:92:422-428

65SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital
So it appears that there is a growing body of research questioning the link between volumes and
outcomes. The evidence therefore that large hospitals are de facto safer than small hospitals has
to be called into question.
Major trauma is better treated in major centres where there is a specialist for each injured body
part. The argument is not so strong for initial life salvage. Treatment must start early, close to the
accident in time and space, the so-called “golden hour”. A trained emergency team of doctors
and nurses, not necessarily a surgeon, may more appropriately fulfil this role. Advanced Trauma
Life Support (ATLS) is now the standard of care expected in Ireland and most of the world before
transfer for definitive treatment. Recent policy moves and reports (eg Hanly Report) have implied
that all major traumas will now bypass smaller hospitals and go straight to the major centre. The reality
is that while the “lights are on”, each small hospital will have such emergencies presenting to them
and needs to be able to perform the initial life salvage function. These patients will arrive no matter
what protocol is agreed at a national or regional level. Every hospital should have a team of staff able
to respond to emergencies.
Currently, hospitals like Nenagh have been asked to desist from performing a range of surgical
procedures eg trauma, fractures, cancers, vascular reconstruction. These restrictions have the
impact of curbing the service to patients at a local level and burdening the already over-whelmed
centralised service further, this, in many cases, without clear evidence that it improves outcomes for
patients. An example is surgical resection for bowel cancer – a patient could be operated on within
a matter of a week at Nenagh Hospital. The same patient now has to wait 6 plus weeks for surgery
in Limerick Regional Hospital. We have to question whether this can be considered an improve-
ment in patient care, when one considers the added stress and pressure on patients and families.
For major surgery, the effects of age and whether the operation is performed as an emergency
has a much greater influence on risk to the patient than the number of cases per hospital/sur-
geon by a factor of 400.26 This applies regardless of hospital size.
There are well-established criteria for identifying the severity of the patient’s condition, which
can be applied to the process of patient transfer. Hanly proposes the transferring of all emergen-
cies and effectively all acute patients to the major centres. The impact of such regionalisation or
volume shifting has not been tested in terms of improving mortality rates or quality of surgical
care and outcome. It would be unwise to enforce such transfer rules until adequate changes in
the receiving hospital are in place and running effectively.
4.1.2. Inter- Hospital TransfersFor staff working in small acute hospitals, one of the biggest areas of concern is inter-hospital
transfer. Recent events in the North Eastern HSE area, have shown just how important this is in
terms of patient safety. However, much of the public debate has missed the point. A conclusion
has been drawn that it is the service in small hospitals that is the problem, when in reality, if one
looks at the facts, there are three factors that have led to needless deaths:
1) The lack of service, or the way that the service in peripheral units has been compromised
by being cut too far.
26 Russell et al, Krukowski, British Journal of Surgery, 2003

SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital 66
2) The referral centres are under so much pressure that they cannot accept a patient in need
3) The back of an ambulance is expected to replace an acute hospital.
In Nenagh Hospital, bed occupancy in 2004 was 97%. The internationally accepted safe level
to avoid bed crises and ensure that patients get appropriate and timely care is 85%.27 As shown
in section 3, an average bed occupancy level hides big fluctuations on a day-to-day basis. There
are days when actual patient numbers rise, in the case of the 75-bedded Nenagh Hospital, to 90
or even 100 patients. In Limerick Regional Hospital, bed occupancy in 2004 was over 90%.
The high bed occupancy in Limerick creates almost as many problems for Nenagh as thebed shortage in Nenagh Hospital itself, because it affects those patients most at risk.
When Nenagh clinical staff identify a patient as requiring tertiary care or specialist care, a long
process involving many phone calls, faxes and much beseeching begins, to try to access an
appropriate bed in the Limerick Regional Hospital or elsewhere for that patient.
Transfer of patients from small acute hospitals to larger centres tests the adequacy and effec-
tiveness of both the local hospital and the receiving hospital’s referral systems.
These patients require:
• Careful local diagnosis and management
• Stabilisation for transfer
• Medical judgement regarding the risks and benefits of transfer
• Coordinated special transport
• Timely access to the referral centre’s specialists, expertise and technology
• Selection and availability of appropriate medical escort eg doctor or anaesthetist
In the current situation, there is no guarantee that a patient, who comes into Nenagh Hospital
and is diagnosed as requiring emergency vascular surgery, for example, will be accepted by
Limerick Regional Hospital, or any other tertiary centre, even though the case is urgent and this
is not a treatment which Nenagh Hospital can offer.
There are a number of problems with the inter-hospital transfer system:
˙The pressure of numbers on the system, can lead, understandably, to a situation where
he who shouts loudest, or is nearest at hand, gets the bed. If the ICU in Limerick is
already full to over-flowing, it is to be expected that the arrival of another patient is not
something that is taken lightly.
˙The process for organising inter-hospital transfer is not adequate. As in all Irish hospitals,
getting the relevant doctor on the phone to discuss the case can be time-consuming and
difficult. For example, phone calls from Nenagh to Limerick to request emergency transfer
go through the main public switchboard. There is no “hotline” system in operation.
˙All hospitals have been instructed to prioritise patients in A&E, and prioritise beds for
these patients. This means that when there are queues in the A&E of the major hospital, a
patient with a badly broken wrist in Limerick Regional Hospital will take priority over an
unstable heart patient in Nenagh Hospital.
27 Bagus, Place and Posnett, BMJ 1999, Dynamics of bed use in accommodating emergency admissions – a stochastic simulation model. Also citedin Acute Bed Capacity Review, 2002, DoH&C

67SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital
˙To overcome this, doctors are forced to rely too much on personal contacts and personal
favour to get what they need for their patients.
This situation is potentially dangerous for the patient, where transfer is a matter of urgency, is
wasteful of resources both in Nenagh Hospital and in the region and puts staff at both ends in an
extremely difficult position.
In 2004, just 27 or 0.39% of patients at Nenagh Hospital required emergency transfer.
A further 2.86%, or 197 patients required non emergency transfer to another hospital.
The total number of transfers therefore is 3.25%. 28
Patients are transferred urgently for treatment for neurological emergencies eg brain haem-
orrhage, vascular emergencies eg aortic aneurysm, urgent angiography and angioplasty and
haemodialysis for kidney failure etc. One of the biggest concerns for clinical staff at Nenagh
Hospital is the management of this small number of patients who require emergency transfer.
This is due to the enormous difficulty involved in getting referral centres to accept these
patients.
In many of the recent cases from around the country, where difficulties about inter-hospital
transfer have led to near or actual fatalities, it is coordination and communication, in an environ-
ment of pressure on beds and services, that have caused the difficulty.
There is a perception that many of the more serious cases are already bypassing small acute
units to go to the referral centre. However, the figures do not back this up. In 2002 (most recent
figures available), only 9.5% of patients in Limerick Regional Hospital came from North Tipperary.
The number of transfers from Nenagh Hospital to Limerick Regional Hospital are not large and
the flow is in both directions.
With almost every hospital in the acute system bowing under the weight of its workload,
issues related to inter-hospital transfer will be difficult to resolve. If the large, receiving hospi-
tal is under such pressure that it has to refuse to accept a patient whom doctors in the
peripheral unit have identified as needing urgent transfer for specialised care, it is hard to see
how smaller units can risk reconfiguring their services or changing their services. Any small
27 HIPE data, 2004 (Nenagh).
FIG
.5 Transfers between LIMERICK and NENAGH in 2004 (HIPE, Limerick)
NENAGHHospital
LIMERICK REGIONAL HOSPITAL
200PATIENTS
SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital 68
acute unit in a rural area that, for example, closes emergency surgical services or limits them
to 9.00AM to 5.00PM, runs the risk of finding itself with a patient it cannot handle and no way
of accessing more appropriate care for that patient. This has occurred recently in well-publi-
cised cases in Monaghan and in Navan. It is not surprising, therefore, that both health profes-
sionals and the public fight to keep their local service. The best way to protect patients and
staff from being exposed to this risk is to retain the ability and the services to deal with all
emergencies 24/7.
For small acute hospitals, one of the biggest contributions that could be made would beto introduce a clear, agreed, national protocol of one call transfer to larger centres.
Until inter hospital transfer is 100% reliable, introducing new and different models of acute
healthcare in Ireland will be extremely difficult.
4.2. COST VERSUS CONTRIBUTION
Hospitals account for a substantial proportion of the healthcare budget, about 50% in many west-
ern European countries. In Ireland, acute hospitals currently consume approximately 40% of total
expenditure on the health and personal social services. Hospital output must be produced on
demand. It is a service commodity which is difficult to store and is poorly substitutable between
patients.
Hospitals with unselected take operate in an environment of uncertainty and must respond to
demand. From one day to the next, it is difficult to know how many patients you will have, what
they will be suffering from and what resources they will consume. It is ensuring that all the
resources are available to deal with this uncertainty that makes the provision of acute health care
so expensive.
In Ireland, the private sector deals with this uncertainty by concentrating on elective procedures
and treatments which are predictable, thus managing capacity usage and work flows, and avoid-
ing the need to maintain costly teams of staff on standby for emergencies. This leaves the less
predictable and more expensive emergency work for the public sector. In Irish public hospitals,
75% of all acute hospital admissions are emergencies. Smaller acute hospitals tend to have a
higher rate of emergency admissions - at Nenagh Hospital it is 90%. They also tend to have a
higher number of public patients, ie patients without private health insurance.
Given the fact that there are no close substitutes for health care, demand for it tends to be
highly inelastic.29 The literature on the estimation of hospital cost functions agrees that costs are
related to output levels.30 So, the more patients a hospital treats, the higher the cost. Efficiency
in Irish hospitals looks at a number of different indicators such as activity and costs, Average
29 Demand does not change or changes very little in response to a price change.30 Jenkins, A.W., (1980), Applied Economics, 12: 103-113, Multi-product Cost Analysis: Service and Case Type Cost Equations for Ontario
Hospitals. Also Barer, M.L., (1982), Journal of Health Economics 1: 189-195, Casemix Adjustments in Hospital Cost Analysis: Information Theory Revisited

69SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital
Length of Stay, bed occupancy rates, staffing ratios, cost per 1000 in-patients/outpatients/day-
cases and cost per bed day among others. Efficiency is the success of the hospital in using its
resources to produce output. Hospital efficiency refers to the ability to produce more outputs
with the same inputs. Inputs refer to labour (nurses, doctors) and capital (beds, equipment
etc). A hospital is said to be operating in an inefficient way, if knowing or assuming health out-
comes to be unaffected, it is possible to reduce cost per case (Donaldson et al., 1992).31
Poor management information systems make establishing accurate and comparable costs
for the running of Nenagh Hospital or any other hospital extremely difficult. The only figure we
can use is a crude calculation of the cost of a bed day, reached through dividing total expendi-
ture for the hospital by bed days used. The results can be used as indicators only.
They do not take case mix into account and this potentially hides both efficiencies and ineffi-
ciencies. Nenagh Hospital is not on the national case mix system.
It was not possible based on information available to us to assess the cost of secondary care
in regional or major hospitals separately in any meaningful way.
Unfortunately, it is therefore very difficult in the Irish context to establish whether cen-tralisation represents better use of public money than the current situation.
Small hospitals treat large numbers of patients. In 2004, the largest 12 hospitals accounted for
246,902 in-patient admissions. The other 329,571 in-patient admissions to acute hospitals were
to smaller units.32 Small hospitals work and work hard.
In any acute hospital, the most significant cost is pay. In 2004, the actual expenditure for
Nenagh Hospital was ¤18.9m, ¤15.7m or 83% of which was spent on pay related costs. The
EWTD, once implemented, is likely to add a considerable burden to the pay element of acute
hospital costs.
TAB
LE 1
1
Examples of Cost per In-Patient Bed per Day in 2004
NENAGH HOSPITAL €711
LIMERICK REGIONAL HOPSITAL €956
BEAUMONT HOSPITAL €1,153
HOSPITAL COST PER DAY
31 From 2005 paper “Application of Hospital Efficiency Indicators”, Pat Williams, University of Galway32 Integrated management Returns, Dept of Health & Children

SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital 70
FIG
.6 NENAGH HOSPITAL – Expenditure 2004
0
2,000
4,000
6,000
8,000
10,000
12,000
14,000
16,000
18,000
TOTAL PAY TOTAL NON PAY (Expenditure 000,s)
FIG
.7 NENAGH HOSPITAL – Breakdown of Expenditure
NURSING PAY
OTHER NON PAY
MEDICAL PAY
PARAMEDICAL PAYCATERING/HKP PAY
MAINTENANCE PAY
ADMIN PAY
OTHER PAY
DRUGS & MEDICINES
MEDICAL & SURGICAL
MED EQUIPMENT

71SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital
While centralisation may have a positive impact on some of the non-pay costs eg maintenance,
it will not have as significant an impact on pay costs as might be hoped. The logic behind central-
isation is very attractive. It goes like this: larger units reduce average costs through the operation
of economies of scale and larger units improve patient outcomes by increasing average volumes
of activity by clinicians. Unfortunately, like the volumes/outcomes argument, the economies of
scale logic is not supported by the evidence.
The empirical literature on economies of scale is extensive, reflecting different methods and
looking at the situation in many different countries.33 Despite this diversity, the results are
remarkably consistent:
• Economies of scale are evident only for hospitals of less than 200 beds
• The optimal size for acute hospitals ranges from 200 to 400 beds
• Above 400-600 beds, average costs increase.
So, for Nenagh, there are economies of scale that could be gleaned if it were larger. However,
the overall national plan for centralisation, which would greatly reduce the number of acute gen-
eral hospitals and increase their size, seems very likely to provide more diseconomies of scale
than otherwise, making hospital care more expensive. Currently, at 807 beds, St James’ Hospital,
Dublin is by far our largest hospital. Reconfiguring the current 12,000 beds into a small number
of larger units, would require creating 12-16 hospitals of 800-1,000 beds. This would involve
major capital investment as well as creating diseconomies of scale. This is underlined by the
mid-term evaluation of the National Development Plan34 which identified that so-called replace-
ment hospitals were always significantly more expensive to run than those they purport to
replace.
The indirect cost of centralisation in terms of patient access should not be ignored. Patients are
assumed not to be deterred from seeking health care by reduced access. The evidence shows
that this is largely true. However, it means that the cost of accessing hospital services shifts more
heavily onto the patient and their family: the financial cost of transport, longer journeys, days off
work for family members and the social cost of the pressure the extra distance puts on families
and support networks.
This does not have the same effect on all sections of the population. The evidence is consis-
tent with large deterrent effects for particular groups, such as those with low personal mobility or
those in particular socio-economic groups, ie the elderly, the poor and the disabled. Over 80% of
in-patients at Nenagh Hospital are public patients. The social cost and the social contribution of
local access to acute health services must also be considered.
33 Aletras V, Jones A, Sheldon TA. Economies of scale and scope. In: Ferguson B, Sheldon TA, Posnett J, eds. Concentration and choice inhealthcare. London: Financial Times Healthcare, 1997:23-36.34 The Mid-Term Evaluation of the National Development Plan and Community Support Frameowrk for Ireland, 2000 to 2006, FinalReport to the Department of Finance by the Economic and Social Research Institute, Policy Research Series Number 50, Oct 2003.

SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital 72
4.3. MEDICAL STAFFING
Smaller acute units are safe and cost effective, but can they be staffed?
• Is the medical education system producing doctors who have the right skills for the gener-
alist work done in smaller acute units?
• What about cover for general on call work?
• Can smaller hospitals continue to provide training posts for Non Consultant Hospital
Doctors (NCHDs)?
• Will anyone want to take these posts or consultant posts in the smaller acute hospitals?
4.3.1.Medical Education & On Call RotasOver the last 20 years, medical education has been moving increasingly towards sub-specialisation.
The medical professions, through their respective royal colleges, have followed the trend towards
greater sub-specialisation. This has led to the colleges favouring the closure and rationalisation of
smaller units. This has created particular difficulties for smaller acute units, which have traditionally
been staffed by general physicians and general surgeons. As the medical education produces fewer
and fewer of these generalists, the difficulty of staffing small acute hospitals becomes more serious.
Over-specialisation is a problem, not just for small hospitals, but for all hospitals, particularly when
it comes to covering general on call. The Royal College of Surgeons in Ireland recognised the “over-
specialisation and de-skilling within General Surgery.” 35 It is already likely in a larger hospital that the
general surgical on call could be covered by a consultant urologist or breast surgeon, for example,
who may find themselves dealing with an acute appendectomy or gall bladder, and be uncomfortable
with and possibly ill-equipped to deal with the patient. In reality, the registrar may be in a better posi-
tion to deal with the situation than the sub-specialist. Who will, then, be clinically responsible?
The trend has been to take the sub-specialities off general call. The problem then becomes
one of an ever-shrinking number of consultants and others available to do general call. The
European Working Time Directive (EWTD) will exacerbate the situation by limiting “hours on call”.
Under the EWTD, employees must have 11 hours free of work in a 24 hour period. That is not
possible with the traditional 24 hour on-call periods worked by hospital doctors, where the same
doctors work throughout the day and night. As a means of meeting the requirements of the
EWTD, the Hanly Report proposed that hospital doctors would work only in large hospitals and in
shifts, the larger pool of doctors available making it possible to cover the on call roster. Since the
publication of the report, it has become clear that large hospitals have great difficulty becoming
EWTD compliant, partly due to sub-specialty rosters.
The Royal College of Surgeons in Ireland suggests a model for the future in which all General
Surgeons should ideally provide acute emergency services. This would require a cohort of General
Surgeons with individual sub-specialty appointments who could provide a broad range of service in
the general surgical area in their region. They suggest, for the future, a four year training model in
General and Emergency Surgery, which would allow enough generic surgeons to man the emer-
gency rota and provide acute services in the smaller centres. Hospitals like Nenagh have a small
35 Royal College of Surgeons in Ireland, The Future of Surgical Specialties in Ireland, 2004, p44

73SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital
number of doctors to draw on for on-call rosters. However, they also have a smaller range of spe-
cialities to cover at night. They may be better placed than larger units to try and adapt their on-call
systems, by drawing on the experience of other countries, such as New Zealand and Australia.
There are a number of initiatives currently under discussion at a policy level to address the
national issue of medical staffing, including increasing the numbers of places in medicine avail-
able to Irish students and post graduate recruitment to training places. What is clear, however, is
that the problem is a national one and it is only in working together and making realistic long-
range plans that a workable solution will be found.
4.3.2.Medical Training Posts & Attractiveness of Positions in SmallerAcute UnitsThere is a strong connection between these two issues. There have been suggestions from the UK
and from the Royal College of Physicians in Ireland that smaller hospitals will find it more difficult to
train doctors because of the EWTD. This is bound to affect service provision, except where there
already is a consultant delivered service eg Radiology and Anaesthetics in Nenagh Hospital. NCHD
posts are be confined to doctors in training. These posts are assigned to individual consultants and
will support his/her workload in the region. Training in smaller hospitals will be more attractive to
undergraduate clinical training and for those interested in integration with primary care.
Studies into the learning experience of medical students have shown that smaller acute hospi-
tals often provide an excellent learning environment for doctors in training. In a UK study36 final
year medical students were asked about their learning experience in Teaching Hospitals and the
smaller District General Hospitals (DGH). Findings indicated that both the identification of learning
objectives and the provision of teaching to meet such objectives were likely to occur in Teaching
Hospitals and District General Hospital settings equally. However, other differences emerged, sug-
gesting that the smaller hospitals (DGHs) offer a friendlier and more supportive learning environ-
ment, with greater opportunities for the acquisition of hands-on practical experience. These find-
ings are supported by evidence gained from interviews with NCHDs in Nenagh Hospital.
4.4. CRITICAL MASS OF SERVICES - WHAT SERVICESARE NEEDED FOR A SAFE,VIABLE ACUTE HOSPITAL?
The term “critical mass of services” has come, through usage in government policy documents
etc, to have a specific meaning related to the numbers of sub-specialist doctors and equipment.
It has become a key element in the centralisation argument. It implies that smaller hospitals,
which do not have this “critical mass” of specialists, are in some way less safe and less appropri-
ate for patients. However, this is not backed up with evidence about improved outcomes for
patients. An acute general hospital is a complex organisation where all elements of the service
are strongly linked and often interdependent.
36 Medical Education, Volume 36 Page 1131 - December 2002, Jayne Parry, Jonathan Mathers, Abdulrahman Al-Fares, Maryam Mohammad,Michael Nandakumar & Dimitris Tsivos - Hostile teaching hospitals and friendly district general hospitals: final year students' views onclinical attachment locations.
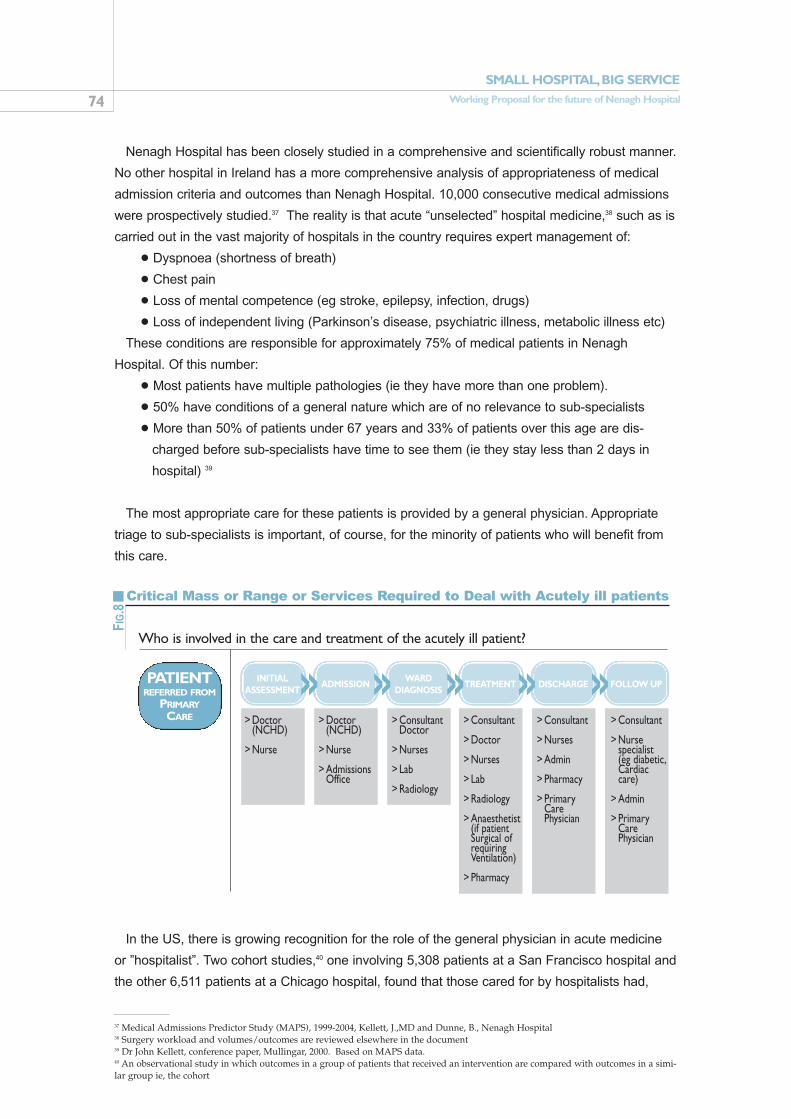
SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital 74
Nenagh Hospital has been closely studied in a comprehensive and scientifically robust manner.
No other hospital in Ireland has a more comprehensive analysis of appropriateness of medical
admission criteria and outcomes than Nenagh Hospital. 10,000 consecutive medical admissions
were prospectively studied.37 The reality is that acute “unselected” hospital medicine,38 such as is
carried out in the vast majority of hospitals in the country requires expert management of:
• Dyspnoea (shortness of breath)
• Chest pain
• Loss of mental competence (eg stroke, epilepsy, infection, drugs)
• Loss of independent living (Parkinson’s disease, psychiatric illness, metabolic illness etc)
These conditions are responsible for approximately 75% of medical patients in Nenagh
Hospital. Of this number:
• Most patients have multiple pathologies (ie they have more than one problem).
• 50% have conditions of a general nature which are of no relevance to sub-specialists
• More than 50% of patients under 67 years and 33% of patients over this age are dis-
charged before sub-specialists have time to see them (ie they stay less than 2 days in
hospital) 39
The most appropriate care for these patients is provided by a general physician. Appropriate
triage to sub-specialists is important, of course, for the minority of patients who will benefit from
this care.
In the US, there is growing recognition for the role of the general physician in acute medicine
or ”hospitalist”. Two cohort studies,40 one involving 5,308 patients at a San Francisco hospital and
the other 6,511 patients at a Chicago hospital, found that those cared for by hospitalists had,
37 Medical Admissions Predictor Study (MAPS), 1999-2004, Kellett, J.,MD and Dunne, B., Nenagh Hospital38 Surgery workload and volumes/outcomes are reviewed elsewhere in the document39 Dr John Kellett, conference paper, Mullingar, 2000. Based on MAPS data.40 An observational study in which outcomes in a group of patients that received an intervention are compared with outcomes in a simi-lar group ie, the cohort
FIG
.8
Critical Mass or Range or Services Required to Deal with Acutely ill patients
Who is involved in the care and treatment of the acutely ill patient?
PATIENTREFERRED FROM
PRIMARYCARE
>> >> >> >> >>INITIALASSESSMENT
ADMISSIONWARD
DIAGNOSISTREATMENT DISCHARGE FOLLOW UP
Doctor(NCHD)
Nurse
>
>
Doctor(NCHD)
Nurse
AdmissionsOffice
>
>
>
ConsultantDoctor
Nurses
Lab
Radiology
>
>
>
>
Consultant
Doctor
Nurses
Lab
Radiology
Anaesthetist(if patientSurgical ofrequiringVentilation)
Pharmacy
>
>
>
>
>
>
>
Consultant
Nurses
Admin
Pharmacy
PrimaryCarePhysician
>
>
>
>
>
Consultant
Nurse specialist(eg diabetic,Cardiaccare)
Admin
PrimaryCarePhysician
>
>
>
>

75SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital
after adjustment, reduced mortality, lengths of stay, and/or costs of care, compared with those
cared for by non-hospitalists.41 However, in an environment where smaller hospitals are seeing
their services cut, curtailed or centralised, will small hospitals be allowed to retain the critical
mass or range of services that allows them to remain effective and, importantly, safe?
We would like to re-define the expression “critical mass of services” to mean the criticalrange of services that a hospital must provide to ensure that it can safely accept acutepatients.
Services such as paediatrics, obstetrics and orthopaedics are not provided by Nenagh
Hospital, except on a “good Samaritan” basis. These services are not wholly divisible from a
functioning acute general hospital – Nenagh and other hospitals like it need to be able to deal
with these situations when these patients arrive, as they inevitably will, outside protocol, before
transferring the patients to a more appropriate facility.
However, without all the services in Fig 5 above on a 24/7 basis, the ability of the hospital to
provide the required care becomes compromised. It depends on staff taking unacceptable per-
sonal and professional risks on behalf of their patients because of service or infrastructure
deficits. An example of the impact of compromising a service was seen in 2005 in Monaghan
Hospital, where the closure of surgery after 5PM in Monaghan Hospital meant that staff found
themselves in a situation where they were left unable to take the necessary action to do every-
thing they could to save a patient with a gastro-intestinal bleed.
In the end, there are two primary functions of an acute hospital:
• Emergency response to new patients and to deterioration in existing patients.
• On-going review and treatment of existing admitted patients on the wards.
An acute hospital that cannot perform these functions adequately is an acute hospital in name
only.
Each acute patient will require most, if not all, of the services outlined in Fig 5. While the
demand for these services is highest during the day, an acutely ill patient may need these services
urgently at any time. Therefore, 24/7 cover must be available for each of these critical services.
41 Auerbach et al. Ann Intern Med Dec 3, 2002;137:859-865; Meltzer et al. Ann Intern Med Dec 3, 2002;137:866-874.


77SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital
CONCLUSIONS AND RECOMMENDATIONS
In an acute general hospital, there is a complex relationship of interdependence between the dif-
ferent elements of the service. The system we have today is the product of evolution, not plan-
ning and strategy. It has evolved and changed over time to cope with the increasing range of
services and treatments available, ever-growing patient numbers, new resources in some areas
and loss of resources in others. Politics has always played a key role in health policy choices.
Because acute hospitals have developed organically, unravelling the knots and interconnec-
tions is a long and intricate process. An large gap has developed between what happens at an
administrative and policy level and the reality that front-line service providers face on a day-to-
day basis. The Hanly Report did not fully recognise the complexity involved in the provision of
acute care. As a result, many of its recommendations were not implementable. The recommen-
dations we make for Nenagh Hospital have to make sense under all futures. There is the current
situation at the hospital. There is a range of conditions that must be met to make the move to the
next stage of development. However, the transition has to be gradual and has to have the patient
at its centre.
In the current environment, the long-term future is very difficult to predict. It is a question of pol-
itics. What is clear is that the people of North Tipperary should never have to accept a worsening
in their access to and experience of acute health care services.
With population growth in the North Tipperary area and the aging of the population, what we
can expect is that the need for acute secondary care will increase, as will people’s expectations
that they should be able to get it close to home.
5.
››PRIORITIES FOR ACTION

SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital 78
NENAGHHOSPITAL
› Streamline admissions› Prevent admissions for investigation only› Reduce amount of on call work for NCHDs› Reduce on call lab and x-ray costs› Decrease ALOS
› Ensure continued safe management of accidentsand emergencies› Supplement staffing at night across the hospital
› Create easier access for day patients in the regionto facilities› Improve access for GPs to diagnostics› Develop purpose built unit that makes sense underall futures
› Improves patient dignity, privacy and comfort› Improves the ability of staff to control hospitalacquired infection
› North Tipperary patients will have local access tothis routine diagnostic tool› Reduce pressure on ambulance service for patienttransport› Reduce requirement of nursing WTE to be used astransport escort› Improve access to CT in the region
› Remove uncertainty around service and allow it todevelop› Improve 1 in 2 rota for surgeons› Reduce number of surgical NCHDs required
› Provide a more workable solution to the problemof acute psychiatry needs while awaiting the creationof psychiatric unit at Nenagh Hospital
› Provide the services that will ensure that elderlypatients have the opportunity to recover as fully aspossible
› The current deficit is 9 beds. However, efficienciesgained by Medical Admissions Unit and CT scannerwill improve efficiency and reduce this requirement› Reduce overcrowding› Create closer match between need and resourcesavailable at Nenagh Hospital
› Create more realistic match between the amountof work done and the resources available› Ensure capacity is there to deal with additionalpatients
Create an acutemedical unit
24/7 consultant led A&E staffed by doctors
Build a diagnostic & treatment centre, includingendoscopy unit and day surgery
Create smaller wards with ensuite facilities
Set up CT scanning service
Stabilise senior medical team:Appoint second consultant surgeon and third consultantanaesthetist posts on a permanentbasis. Create third surgical post
Provide access to acute psychiatricbeds to North Tipperary patientsin Limerick Regional Hospitalimmediately
Create geriatric rehabilitation unit
Create 5 new in-patient medicalbeds
Increase the number of day bedsfrom 6 to 10
IMPACTACTION
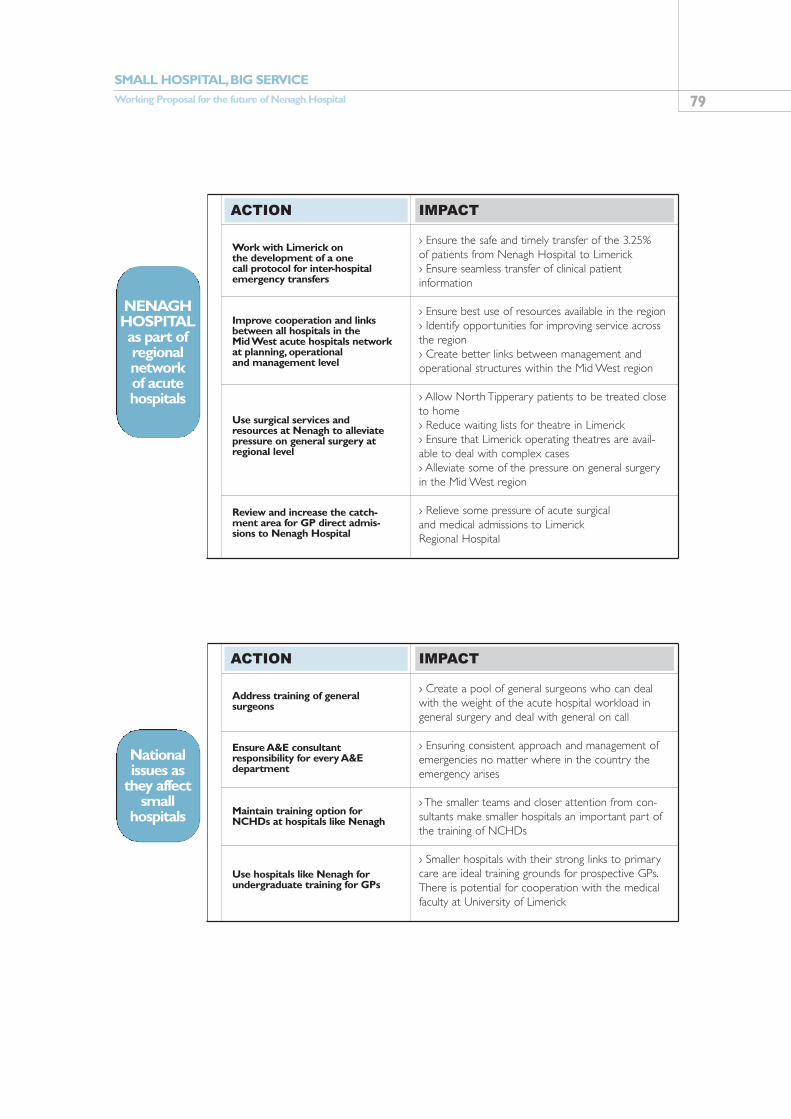
79SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital
NENAGHHOSPITALas part ofregionalnetwork of acutehospitals
› Ensure the safe and timely transfer of the 3.25% of patients from Nenagh Hospital to Limerick› Ensure seamless transfer of clinical patient information
› Ensure best use of resources available in the region› Identify opportunities for improving service acrossthe region› Create better links between management andoperational structures within the Mid West region
› Allow North Tipperary patients to be treated closeto home› Reduce waiting lists for theatre in Limerick› Ensure that Limerick operating theatres are avail-able to deal with complex cases› Alleviate some of the pressure on general surgeryin the Mid West region
› Relieve some pressure of acute surgical and medical admissions to Limerick Regional Hospital
Work with Limerick on the development of a one call protocol for inter-hospitalemergency transfers
Improve cooperation and linksbetween all hospitals in the Mid West acute hospitals networkat planning, operational and management level
Use surgical services andresources at Nenagh to alleviatepressure on general surgery atregional level
Review and increase the catch-ment area for GP direct admis-sions to Nenagh Hospital
IMPACTACTION
Nationalissues as
they affectsmall
hospitals
› Create a pool of general surgeons who can dealwith the weight of the acute hospital workload ingeneral surgery and deal with general on call
› Ensuring consistent approach and management ofemergencies no matter where in the country theemergency arises
› The smaller teams and closer attention from con-sultants make smaller hospitals an important part ofthe training of NCHDs
› Smaller hospitals with their strong links to primarycare are ideal training grounds for prospective GPs.There is potential for cooperation with the medicalfaculty at University of Limerick
Address training of general surgeons
Ensure A&E consultant responsibility for every A&Edepartment
Maintain training option forNCHDs at hospitals like Nenagh
Use hospitals like Nenagh forundergraduate training for GPs
IMPACTACTION

SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital 80
LIST OF TABLES AND FIGURES
Tables
Table 1 North Tipperary Distances and Travel Times
Table 2 Ambulance Service Requirements North Tipperary
Table 3 Acute Beds vs Patients Treated 1980-2004
Table 4 10 Most Common Medical Diagnoses in Nenagh Hospital and in Limerick Regional Hospital
Table 5 Nenagh Hospital Medical Bed Days Used & Available
Table 6 Limerick Regional Hospital General Medical Bed Days Used & Available
Table 7 Contribution to Mid West Service
Table 8 10 Most Common Surgical Diagnoses in Nenagh Hospital and in Limerick Regional Hospital
Table 9 Nenagh Hospital Surgical Bed Days Used & Available Surgeon Workload
Table 10 Limerick Regional Hospital General Surgical Bed Days
Table 11 Day Surgery in the Mid West Region
Table 12 Cost per Bed Day
Figures
Figure 1 Arguments For/Against Local Hospitals
Figure 2 Mid West Acute Hospitals Network
Figure 3 Emergency Response Unit
Figure 4 Pattern of Demand for In-Patient Beds
Figure 5 Transfers between Nenagh Hospital and Limerick Regional Hospital
Figure 6 Nenagh Hospital Expenditure – Pay/Non Pay
Figure 7 Nenagh Hospital Breakdown of Expenditure
Figure 8 Critical Mass of Services for Safe Acute Hospital

81SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital
BIBLIOGRAPHY
Royal College of Surgeons in Ireland, (2004), The Future of Surgical Specialties in Ireland Department of Health & Children, (2003), Report of the National Taskforce on Medical Staffing Mid Western Health Board, (2001), Strategy for Acute Hospital Services, Mid West Region Department of Health & Children, (2001), Quality and Fairness, National Health StrategyThe Irish Society for Quality and Safety in Healthcare, (2004), The Patient’s View, A
Comparative Analysis of the Mid Western Regional Hospital, Nenagh Against NationalAverages, 2004 Satisfaction Survey
HIPE (Hospital in-Patient Enquiry) data, Nenagh Hospital and Limerick Regional Hospital, 1999-2005
Dunne, B., Kellett, J., MD, Medical Admissions Predictor Study 1999-2004, Nenagh Hospital.Unpublished.
Bagus, Place and Posnett, (1999) British Medical Journal, Dynamics of bed use in accommodat-ing emergency admissions – a stochastic simulation model.
Nasr, A. et al (2004) Irish Journal of Medical Science, Vol 173, No.3, Impact of EmergencyAdmissions on Elective Surgical Workload
Department of Health and Children, (2002), Acute Hospital Bed Capacity - A National ReviewDept of Health & Children, (2004), Mental Health Commission Annual Report. Kileen S.D., O’Sullivan M.J., Coffey, J.C., Kirwan,W. Redmond, H.P. (2005) British Journal of
Surgery, 2005; 92:389-402, Provider volume and outcomes for oncological proceduresAmanda Sowden et al (1997) Concentration and choice in the provision of hospital services: the
relationship between hospital volume and quality of health outcomes CRD Report 8 Part 1,York University Centre for Health Economics
Russell, E.M., Bruce J., Krukowski, Z.H. (2003) British Journal of Surgery; 90:527-532.Systematic Review of the Quality of Surgical Mortality Monitoring
EA Halm et al. (2002) Ann Intern Med Is volume related to outcome in health care? A systemat-ic review and critique of the literature
Kingsmore, D.B. Hole, D.J., Gillis, C.R. and George, W.D. (2005) British Journal of Surgery2005:92:422-428 Inadequate Treatment of Symptomatic Breast Cancer
Jenkins, A.W., (1980), Applied Economics, 12: 103-113, Multi-product Cost Analysis: Service andCase Type Cost Equations for Ontario Hospitals
Barer, M.L., (1982), Journal of Health Economics 1: 189-195, Casemix Adjustments in HospitalCost Analysis: Information Theory Revisited
Williams, P. (2005) Application of Hospital Efficiency Indicators, National University of Ireland,Galway. Unpublished.
Aletras V, Jones A, Sheldon TA. Economies of scale and scope. In: Ferguson B, Sheldon TA,Posnett J, eds. Concentration and choice in healthcare. London: Financial Times Healthcare,1997:23-36.
Economic and Social Research Institute, (2003), Policy Research Series Number 50, The Mid-Term Evaluation of the National Development Plan and Community Support, Framework forIreland, 2000 to 2006, Final Report to the Department of Finance.
Parry J., Mathers J., Al-Fares A., Mohammad M., Nandakumar M. & Tsivos, D. (2002) MedicalEducation, Volume 36 Page 1131 Hostile teaching hospitals and friendly district general hospi-tals: final year students' views on clinical attachment locations
Kellett J., MD, conference paper, Mullingar, 2000. Based on MAPS dataAuerbach et al. (2002) Ann Intern Med, 2002;137:859-865 Implementation of a Voluntary
Hospitalist Service at a Community Teaching Hospital: Improved Clinical Efficiency and PatientOutcomes

SMALL HOSPITAL,BIG SERVICEWorking Proposal for the future of Nenagh Hospital 82
Meltzer et al. (2002) Ann Intern Med 2002;137:866-874 Effects of Physician Experience onCosts and Outcomes on an Academic General Medicine Service: Results of a Trial ofHospitalists
Milewa, Timothy. Journal of Management in Medicine, Bradford:1997. Vol. 11, Iss. 4, p.238-245,User participation in service planning: A qualitative approach to gauging the impact of manage-rial attitudes
Swinehart, Kerry, Zimmerer, Thomas W, Oswald, Sharon. Journal of Management in Medicine,Bradford:1995. Vol. 9, Iss. 2, p.34. Adapting a strategic management model to hospital operat-ing strategies: A model development and justification
Prospectus Strategy Consultants (2003) Audit of Structures and Functions in the Heath SystemDept of Health & Children, Integrated Management Returns 2004Department of Health, UK, 2004, The Configuring Hospitals Evidence File, Part One
ACKNOWLEDGEMENTS
We wish to acknowledge the very many people who have contributed time, effort and money to
the funding of this report. Led by Noreen Kennedy, Teresa Langton and Maura Byrne, the
members and supporters of Nenagh Hospital Action Group have worked hard to make the
publication of this report possible.
We would like to thank all of those who organised and attended fund-raising events and who
gave of their time, energy and enthusiasm.
We would particulary like to thank all the staff of Nenagh Hospital for their support and help
during the project. A special thanks to all of those who made time available for interviews, who
provided information and background for the project, and gave us valuable feedback and sug-
gestions.
Credits
Research: Dr. Gemma Carney
Design: Pablo Lloréns
Photography: Fergal Shanahan
Printing: Nenagh Guardian

















