8 Small intestinal motility and transit in disease MICHAEL CAMILLERI MARIO VASSALLO Small intestinal motility in health has received much attention since the descriptions two decades ago of interdigestive motility, including the migrating motor complex (Szurszewski, 1969) and its ‘housekeeping’ functions (Code and Marlett, 1975). The abnormal motor functions in disease are less understood. This chapter reviews the effect of disorders of the small intestine that derange the whole gut wall structure as well as those that are localized to the smooth muscle or neural elements. BASIC CONTROLS OF SMALL INTESTINAL MOTOR FUNCTION Figure 1 summarizes the factors that control small intestinal motor function. Intestinal smooth muscle contractions are mediated by ion fluxes which alter the cell membrane potential and the contractile state of the muscle cells. Contractions are integrated and modulated by intrinsic (in the gut wall) or extrinsic nerves. The enteric nervous system is estimated to contain 10’ neurones in the mammalian gut; it controls the intestine by complex modulation of both excitatory and inhibitory nerves to the muscle. The effects of these nerves are mediated by specific neurotransmitters (chiefly peptides and, possibly, purines). The enteric nervous system possesses considerable functional autonomy and plasticity in its responses to altered conditions (e.g. disease states), but it is also under presynaptic control by extrinsic neural elements. The key extrinsic controls are cranial (vagal) and sacral (S2, 3 and 4) parasympathetic nerves, and the thoracolumbar sympathetic outflow. Prevertebral sympathetic ganglia are important in the integration of intestinal motor function (Szurszewski and Weems, 1976). Derangements at any of these levels of control may result in abnormal small intestinal motility. NORMAL SMALL INTESTINAL MOTOR FUNCTION During fasting, normal small intestinal motor function is cyclical; after food, motor activity is more continuous, triturating, mixing and propelling digesta. The fasting phase is characterized by the interdigestive migratihg Bail&e’s Clinical Gastroenterology- 431 Vol. 5, No. 2, June 1991 Copyright 0 1991, by BailliPre Tindall ISBN 0-7020-153GX All rights of reproduction in any form reserved
Transcript
8
Small intestinal motility and transit in disease
MICHAEL CAMILLERI MARIO VASSALLO
Small intestinal motility in health has received much attention since the descriptions two decades ago of interdigestive motility, including the migrating motor complex (Szurszewski, 1969) and its ‘housekeeping’ functions (Code and Marlett, 1975). The abnormal motor functions in disease are less understood. This chapter reviews the effect of disorders of the small intestine that derange the whole gut wall structure as well as those that are localized to the smooth muscle or neural elements.
BASIC CONTROLS OF SMALL INTESTINAL MOTOR FUNCTION
Figure 1 summarizes the factors that control small intestinal motor function. Intestinal smooth muscle contractions are mediated by ion fluxes which alter the cell membrane potential and the contractile state of the muscle cells. Contractions are integrated and modulated by intrinsic (in the gut wall) or extrinsic nerves. The enteric nervous system is estimated to contain 10’ neurones in the mammalian gut; it controls the intestine by complex modulation of both excitatory and inhibitory nerves to the muscle. The effects of these nerves are mediated by specific neurotransmitters (chiefly peptides and, possibly, purines). The enteric nervous system possesses considerable functional autonomy and plasticity in its responses to altered conditions (e.g. disease states), but it is also under presynaptic control by extrinsic neural elements. The key extrinsic controls are cranial (vagal) and sacral (S2, 3 and 4) parasympathetic nerves, and the thoracolumbar sympathetic outflow. Prevertebral sympathetic ganglia are important in the integration of intestinal motor function (Szurszewski and Weems, 1976). Derangements at any of these levels of control may result in abnormal small intestinal motility.
NORMAL SMALL INTESTINAL MOTOR FUNCTION
During fasting, normal small intestinal motor function is cyclical; after food, motor activity is more continuous, triturating, mixing and propelling digesta. The fasting phase is characterized by the interdigestive migratihg
Bail&e’s Clinical Gastroenterology- 431 Vol. 5, No. 2, June 1991 Copyright 0 1991, by BailliPre Tindall ISBN 0-7020-153GX All rights of reproduction in any form reserved
432 M. CAMILLERI AND M. VASSALLO
Thoracolumbar
potential
Figure 1. Control of gut motility-interactions between extrinsic neural pathways and the intrinsic nervous system (‘enteric brain’) modulate contractions of gastrointestinal smooth muscle. Peptide-receptor interactions alter muscle membrane potentials by stimulating bidirectional ion fluxes. In turn, membrane characteristics dictate whether or not the muscle cell contracts. From Camilleri and Phillips (1989) with permission.
motor complex (MMC) (F’g 1 ure 2), which occurs at about 90 min intervals, commences in the gastroduodenal region and propagates for a variable distance down the small intestine (Kellow et al, 1986). The cycling of interdigestive motor activity is characterized by a period of quiescence (phase I), irregular phasic contractions without tonic contractions (phase II) and a burst of repetitive contractions at the maximal small intestinal frequency of 12/min (phase III). Phase III of the interdigestive MMC propagates to the distal small intestine, sweeping products of digestion and debris towards the colon and thus acting like a housekeeper.
Postprandially, small intestinal contractions of variable amplitude occur irregularly (Figure 2), albeit fairly consistently, and replace the cyclical fasting motor activity. These contractions propagate for shorter distances and propel the contents less rapidly than during fasting, and control propulsion of digesta through the small intestine. The duration of the ‘fed’ pattern depends on the size and nutrient content of the meal. The distal small intestine and terminal ileum play important roles in the control of the delivery of thyme to the caecum. In humans, it has been estimated that about 50% of the flow of intestinal contents through the ileum occurs in conjunction with phase III of the MMC, and the flow rate increases
SMALL INTESTINAL MOTILITY AND TRANSIT IN DISEASE 433
434 M. CAMILLERI AND M. VASSALLO
promptly after a meal (Kerlin et al, 1982). The pattern of ileocolonic transit is slower and more erratic before a meal than postprandially (Spiller et al, 1987). The effect of eating on terminal ileal motility is generally limited to the initial 30 min of the postprandial period (Spiller et al, 1987). The exact mechanism of this so-called gastroileal response is unclear, but its timing suggests a neural reflex.
A recent study has shown that in health the human terminal ileum acts as a reservoir for solid food residue, since transfer of residue to the colon occurs in boluses (Camilleri et al, 1989a). These bolus transfers are especially frequent within 30 min of ingestion of a second meal, confirming that feeding results in the propulsion of solid material retained in the ileum. Experiments in dogs suggest that movements of boluses into the colon may be induced by prolonged, propagated ileal contractions (Kruis et al, 1985). This pattern of motility is observed infrequently during prolonged monitoring of ileal motility in man, so it is unlikely that it is the sole motor pattern that results in ileocolonic transit in humans under normal circumstances (Spiller et al, 1987). Also in the dog, clusters of propagated, rapid ileal contractions are important propulsive forces in the late postprandial period (Fich et al, 1990b), but this motor pattern has not been observed in humans.
THE SPECTRUM OF SMALL INTESTINAL MOTILITY DISORDERS
A number of diseases of muscle and nerve affect the gut. Dilatation of limited sections of the gut (e.g. megaduodenum) or anatomical derangements, such as uncomplicated postsurgical states, result in few symptoms. On the other hand, extensive involvement by pseudo-obstructive syndromes may result in life-threatening gut failure.
In general, abnormal small intestinal motility can be attributed to myo- pathic or neuropathic disorders. Manometric studies under basal conditions (Malagelada et al, 1986) and evaluation of the acute effects of cholino- mimetic agents (Battle et al, 1979), can distinguish between neuropathic (unto-ordinated activity, but pressure of normal amplitude) and myopathic (low amplitude pressure activity) disorders (Figure 3).
Structural diseases and their effect on small intestinal motility Disturbances of proximal small intestinal motility are frequently observed in symptomatic patients following gastric surgery. After Roux-en-Y gastrec- tomy, unto-ordinated pressure waves occur in the Roux limb (Mathias et al, 1984) and are postulated to be responsible for the nausea, vomiting and gastric stasis suffered by these patients. Dysfunction of the extrinsically denervated gastric remnant is evident as deranged tonic contraction (Azpiroz and Malagelada, 1987); resection of the gastric remnant some- times relieves the symptoms of upper gut stasis (Karlstrom and Kelly, 1989), suggesting that dysfunction of the gastric remnant is important in the Roux stasis syndrome. Several forms of gastric surgery result in derangement of
Syst
emic
Sc
lero
sis
Antro
duod
enum
1 2--
?+
A-dm
w~~~
AtiW
W
3 .
.
Desc
endin
g du
oden
um
Dista
l du
oden
um
Prox
imal
jejun
um
1 ”
* IJu
r*r,
2 3-
Dia
bete
s M
ellit
us
Figur
e 3.
Patte
rns
of po
stpra
ndial
pre
ssure
sh
owing
pr
onou
nced
hy
pomo
tility
in a
patie
nt
with
sy
stemi
c sc
leros
is (le
ft pa
nel)
and
antra
l hy
pomo
tility,
py
loros
pasm
(ar
row)
and
failu
re
of the
me
al to
induc
e a
fed
patte
rn
in a
diabe
tic
with
au
tonom
ic ne
urop
athy
(righ
t pa
nel),
co
mpar
ed
with
the
pre
ssure
pa
ttern
of
a he
althy
su
bject
(centr
e pa
nel).
Fr
om
Cami
lleri
(199
0b),
with
pe
rmiss
ion.
FAST
ING
Pntro
duod
enal
1
A 1
IA.
A I
.
2 -
. L
1 I
3 Iu
r_l
Mst
al
duod
enum
LLI
1 LA
1 AA
J I,.
..L
‘roxim
al
jeiu
num
1
L4
b
2
IA
A.
3 I
I
n,
n A
5
mln
I 1
FED
Il.
h I\
R A
I\ A
1 50
mm
Hg
A
Figur
e 4.
Simu
ltane
ous
prolo
nged
co
ntrac
tions
in
the
prox
imal
small
int
estin
e in
a pa
tient
wi
th
mech
anica
l ob
struc
tion
of the
dis
tal
small
int
estin
e. Fr
om
Cami
lleri
(198
9),
with
pe
rmiss
ion.
SMALL INTESTINAL MOTILITY AND TRANSIT IN DISEASE 437
intestinal motility (Fich et al, 1990a) but it is also likely that in some postsurgical patients dysmotilities may have been present preoperatively, for example, non-ulcer dyspepsia associated with slow gastrointestinal transit.
In subacute mechanical obstruction, two patterns of small intestinal motility have been described. Summers et al (1983) were the first to report rhythmic, clustered contractions as a feature of partial obstruction. These clusters occur postprandially and each lasts approximately lmin, being separated from the next by an interval of l-2min. These findings were confirmed by others (Camilleri, 1989). They were non-specific, however, as they were also observed in patients with chronic intestinal pseudo- obstruction (Summers et al, 1983) and after ileal pouch-anal anastomosis (Stryker et al, 1985). Distal mechanical obstruction (Camilleri, 1989) may also cause simultaneous prolonged contractions (Figure 4), separated by periods of quiescence. The recognition of such contractile patterns during the evaluation of patients with chronic nausea, vomiting or abdominal pain necessitates the exclusion of mechanical obstruction by careful enteroclysis or even laparotomy.
Small intestinal fistulae, diverticula and postsurgical blind loops are all associated with bacterial overgrowth, but the mechanisms that lead to this overgrowth are not well established. Experimentally, bacterial toxins induce migrating bursts of contraction in the rabbit ileum (Mathias et al, 1976) and rapid transit through the small intestine, with consequent diarrhoea. It has also been suggested that multiple jejunal diverticulosis may be a manifestation of abnormal neuromuscular function (Krishnamurthy et al, 1983). As well as anatomical abnormalities of the small intestine causing bacterial overgrowth, defective small intestinal motility may be a primary cause of bacterial overgrowth in the absence of anatomical abnormality (Vantrappen et al, 1977).
The superior mesenteric artery (SMA) syndrome is typically described in two clinical settings. First, it can occur in the patient whose spine is immobilized and has had substantial weight loss. Such patients are truly considered to have small intestinal mechanical obstruction by extrinsic compression from the SMA. The second setting is the syndrome of recurrent vomiting and abdominal pain in ambulant young women, in whom the proximal duodenum is dilated and the SMA appears to be responsible for partial mechanical obstruction. It is currently thought that in the latter syndrome there is a primary disorder of small intestinal motility. The radiologically demonstrated ‘obstruction’ of the duodenum is due to dilatation resulting from hypomotility or unto-ordinated, ineffective contractions of the duodenal loop, rather than from SMA compression.
Myopathic disorders
The small intestine can be affected by generalized infiltrative disorders of smooth muscle, such as scleroderma (Cohen et al, 1972, 1980) and amyloidosis, generalized muscle disease, primarily involving skeletal muscle (Feldman and Marshak, 1963; Horowitz et al, 1986,1987); or by a condition
438 M. CAMILLERI AND M. VASSALLO
that selectively affects hollow organs (the gut and urinary tract) called ‘hollow visceral myopathy’ (Schuffler and Beegle, 1979). The key features of these disorders are summarized in Table 1. These disorders are usually easy to identify clinically because they are almost invariably associated with florid manifestations of the underlying disease.
Neuropathic disorders
Disorders of small intestinal motility may be caused by diseases of extrinsic neural control or of the enteric nervous system and have been discussed in detail elsewhere (Camilleri and Phillips, 1989; Camilleri, 1990a). Table 2 lists the neurological diseases that may alter small intestinal motor function. Specific examples are discussed below.
Extrinsic neuropathies
Chronic diabetic autonomic neuropathy is the most commonly encountered extrinsic neurological disorder that causes gastrointestinal motor dys- function. The intestinal dysautonomias are much less common, but they illustrate the serious effects of deranged extrinsic neural control.
Diabetes mellitus. Gastrointestinal symptoms were found to be exceedingly common in diabetic patients assessed in a tertiary care centre; 76% of 136 diabetic outpatients reported nausea, vomiting, abdominal pain, diarrhoea and constipation (Feldman and Schiller, 1983). Abnormal gastric emptying or gastroparesis is a relatively common finding, and various pathophysio- logical changes have been demonstrated, including distal antral hypo- motility (Malagelada et al, 1980), reduced postprandial duodenojejunal phasic pressure activity, non-propagated or propagated (Figure 3) bursts of contractions in the proximal small intestine (Camilleri and Malagelada,
Table 1. Myopathic disorders affecting small intestinal motility.
Infiltrative disorders Systemic sclerosis A two-stage dysmotility with an initial neuropathic process,
followed by infiltration of smooth muscle layers with fibrous tissue
Amyloidosis Primary (sometimes familial) or secondary deposition of abnormal protein in muscle layers; intrinsic or extrinsic nerves may also be affected; manometry allows distinction between infiltrative process and amyloid neuropathy
Generalized muscle disease Dermatomyositis Rarely affects the oesophagus and stomach; gut involvement
generally correlates with skeletal muscle weakness Muscular dystrophies Dystrophia myotonica, congenital myotonic dystrophy or
Duchenne dystrophy
Hollow visceral myopathy May be familial or sporadic; manifestations vary with region(s) affected; urinary tract may also be involved and result in dilatation from the level of the renal calyces to the bladder
SMALL INTESTINAL MOTILITY AND TRANSIT IN DISEASE 439
1984), and pylorospasm (Mearin et al, 1986). Diarrhoea occurred in up to 20% of patients (Feldman and Schiller, 1983) in a tertiary referral diabetic clinic. Detailed assessment is required in order to determine the underlying mechanism of the dysfunction and to plan appropriate treatment. Some patients have low-volume diarrhoea due to faecal incontinence that occurs as a result of anal sphincter dysfunction and impaired rectal sensation (Schiller et al, 1982). However, faecal incontinence is often associated with, and worsened by, high-volume diarrhoea, which may be due to multiple factors, including small intestinal malabsorption and rapid transit.
Small intestinal dysmotility may lead to stasis of contents with secondary bacterial overgrowth. Bile acid deconjugation due to bacterial action may induce osmotic diarrhoea. Unto-ordinated bursts of non-propagated phase III-like activity occur and cause rapid transit (Camilleri and Malagelada, 1984). Other documented abnormalities which may contribute to diarrhoea in diabetic patients are gluten-sensitive enteropathy (Walsh et al, 1978) and pancreatic exocrine insufficiency (el Newihi et al, 1988). Visceral neuropathy is a key factor in the motor dysfunction and is evident as a reduced fibre density in the splanchnic nerves (Low et al, 1975) and as structural abnormalities in the prevertebral and paravertebral ganglia (Hensley and Soergel, 1968). The myenteric plexus is normal in diabetic patients (Yoshida et al, 1988).
Dysautonomias. Pure dysautonomia presents as two distinct clinical syndromes: first, a mixed autonomic dysfunction, referred to as pandys- autonomia, which affects both the parasympathetic and the sympathetic
Table 2. Neuropathic disorders affecting small intestinal motility.
Extrinsic nervous system Acute peripheral neuropathy associated with autonomic dysfunction:
Guillain-Barre syndrome; acute viral infections such as Epstein-Barr virus; herpes zoster
Autonomic system degenerations Idiopathic orthostatic hypotension Pandysautonomia Selective cholinergic dysautonomia
Spinal cord Injury Multiple sclerosis
Brain stem Tumours Cerebrovascular strokes
Higher central nervous system Extrapyramidal disease, e.g. Parkinson’s disease, Shy-Drager syndrome Epilepsy
Intriflsic nervous system Idiopathic, degenerative and inflammatory disorders of the myenteric plexus Some diseases associated with disorders affecting extrinsic neural control, e.g
neurofibromatosis
440 M. CAMILLERI AND M. VASSALLO
system, and, second, a selective cholinergic dysautonomia, in which the abnormality is restricted to the parasympathetic supply to viscera and the sympathetic supply to cholinergically innervated sweat glands. The aetiology of these dysautonomias is unclear, but an association between viral infection and the onset of dysautonomias is well documented; for example, the Epstein-Barr virus, which causes infectious mononucleosis, has been implicated in both acute pandysautonomia (Yahr and Frontera, 1975) and selective cholinergic dysautonomia (Vassallo et al, 1991).
The gastrointestinal involvement in acute, subacute and congenital dysautonomia is evident as vomiting, paralytic ileus, constipation or a pseudo-obstructive syndrome. A biopsy from the cardia taken during a Heller’s procedure in a patient with an achalasia-like syndrome showed normal myenteric plexus ganglia (Appenzeller and Kornfeld, 1973), sug- gesting that the lesion is extrinsic to the gut neuromuscular apparatus.
Since the initial description of pandysautonomia (Young et al, 1969), nine cases of selective cholinergic dysautonomia have been reported (Andersen et al, 1972; Thomashefsky et al, 1972; Hopkins et al, 1974,1981; Harik et al, 1977; Inamdar et al, 1982; Kirby et al, 1985; Takayama et al, 1987; Vassallo et al, 1991). The symptoms of cholinergic autonomic dysfunction are strikingly similar; thus, all reports document anhidrosis, paucity of saliva and tears, difficulties with micturition and pupillary dysfunction. Unlike pandysautonomia, non-cholinergic sympathetic functions such as blood pressure control and responses to the Valsalva manoeuvre are normal. Gastrointestinal involvement is prominent, frequently a presenting clinical feature and often sufficiently severe to mimic mechanical intestinal obstruction (four out of nine patients in the literature reported to date have undergone laparotomy). Intestinal manometry shows features typical of a neuropathic pseudo-obstruction. In our patient with this condition, histo- logical and immunohistochemical studies of the myenteric ganglia were normal, in support of the view that disordered extrinsicneural control is important in deranged small intestinal motility (Vassallo et al, 1991).
Diseases of the enteric nervous system
Disorders of the enteric nervous system usually produce the syndrome of chronic intestinal pseudo-obstruction.. No single aetiology has been identi- fied, although some clues exist, such as the demonstration of cytomegalo- virus in the myenteric plexus ganglion cells (Sonsino et al, 1984). More often, no cause is identifiable. The diagnosis of enteric nervous system dysfunction is made by the manometric demonstration of a neuropathic motor pattern without evidence of an underlying neuropathy or autonomic dysfunction (Colemont and Camilleri, 1989). The histopathological changes suggest degeneration of the intrinsic plexus or an inflammatory process that leads to plexus damage (Krishnamurthy and Schuffler, 1987).
Chronic intestinal pseudo-obstruction is diagnosed when there are symptoms of mechanical obstruction, but no evidence of any structural abnormality on the basis of endoscopy, radiology or laparotomy. Mano- metric features include abnormal propagation of the interdigestive MMC,
SMALL INTESTINAL MOTILITY AND TRANSIT IN DISEASE 441
10 min 3 hours Ei hours
Figure 5. Transit of radiolabelled solids and liquids in a patient with chronic (neuropathic) intestinal pseudo-obstruction. Note the prolonged retention of both phases of the meal in the stomach and small bowel. The upper outline depicts the stomach, the lower outline on 3- and 6-h scans depicts the right side of the colon. From Camilleri et al (1986a), with permission.
groups of small intestinal pressure waves that occur in clusters or bursts that may last in excess of 30min and failure of a meal to induce a fed pattern (Stanghellini et al, 1987). These features have also been reported in paediatric patients (Hyman et al, 1988). In patients with the pseudo- obstructive syndrome, the transit of solids and liquids through the small intestine is delayed and gastric emptying of solids is slow (Figure 5) (Camilleri et al, 1986b; Mayer et al, 1988).
Small intestine motility disorders of uncertain pathophysiology
Irritable bowel syndrome
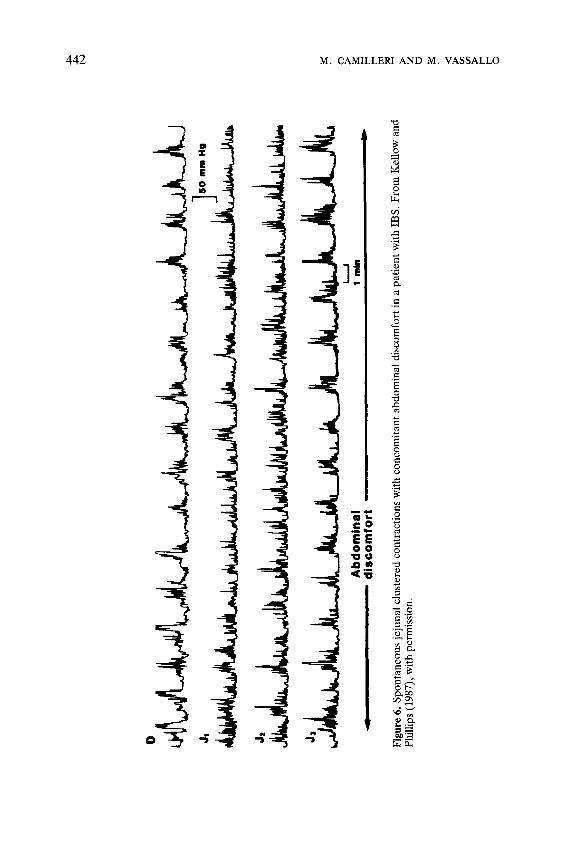
Kumar and Wingate (1985) have shown that, in response to stress, fasting patients with irritable bowel syndrome (IBS) have irregular small intestinal contractions and a reduction in the frequency of interdigestive MMCs. Others (Kellow and Phillips, 1987) have demonstrated an increase in the frequency of MMCs in IBS patients with diarrhoea, but not in those with constipation. Clustered small intestinal contractions (Figure 6) and pro- longed ileal contractions or peristaltic equivalents were also observed in association with abdominal pain in IBS patients (Kellow and Phillips, 1987).
JI
JJ
l-..J
Ab
dom
inal
1
mln
4
disc
omfo
rt N
Figur
e 6.
Spon
taneo
us
jejun
al clu
stere
d co
ntrac
tions
wi
th
conc
omita
nt ab
domi
nal
disco
mfor
t in
a pa
tient
wi
th
IBS.
Fr
om
Kello
w an
d Ph
illips
(1
987)
) wi
th
perm
ission
.
SMALL INTESTINAL MOTILITY AND TRANSIT IN DISEASE 443
Some of the patterns of ileal motility seen in IBS are similar to those associated with the coloileal response. The specificity to IBS patients and significance of these findings in the pathogenesis of IBS symptoms are, however, uncertain. Current approaches to the investigation of the patho- physiology of IBS use prolonged, ambulatory monitoring of small intestinal motility (Kellow and Phillips, 1989) or non-invasive scintigraphic measure- ments of intestinal transit (Vassallo et al, 1990); these novel methods are likely to give better insights. The interpretation of whether motor patterns in IBS patients are abnormal is made difficult by the great variability (Kellow et al, 1986) in the periodicity and duration of the MMC among healthy subjects. Indeed, Kingham et al (1984) detected no differences in MMC activity between IBS patients and healthy controls during more than 30 h of observation.
Non-specific diarrhoeas
Migrating action potential complexes are bursts of electrical spikes that migrate distally at the same propagation velocity as that of the slow wave. They have been observed in a patient with secretory diarrhoea (Vantrappen et al, 1986). In manometric studies in patients with presumed chronic infectious diarrhoea, Kellow et al (1985) recorded rapidly propagated, prolonged (12-48 s) and high amplitude (35-100 mmHg) monophasic pressure waves. This alteration of motility was associated with normal fluid absorption in the jejunum and high flow rates in the ileum, suggesting an important role for disturbed fluid transit in the pathophysiology of this syndrome.
Hypersensitivities
Parasitic infestations such as Nippostrongylus brasiliensis and Trichinella spiralis result in stimulation of small intestinal motility in the rat. It has been deduced that mast cells and their secretory products play an important modulatory role in this alteration of function (Collins and Vermillion, 1986; Fox-Robichaud and Collins, 1986). These are examples of mechanisms whereby the host can eliminate parasites, but they also provide a model for the study of hypersensitivity and allergy in the gut.
The small intestine and vomiting
Small intestinal retroperistalsis is an integral part of the vomiting response. Lang et al (1986) have recorded these giant contractions which sweep retrogradely through the upper gut. They presumably move digesta in an orad direction from the mid-small intestine and even more distally. Follow- ing severe retching or vomiting, distally migrating clusters of pressure waves which have the same frequency, amplitude and propagation velocity as phase III of the interdigestive MMC also occur (Thompson and Malagelada, 1982).
444 M. CAMILLERI AND M. VASSALLO
Small intestinal motility in tumour-associated diarrhoea
The secretory neuropeptides and hormones produced by the endocrine tumours that cause watery diarrhoea syndromes (e.g. vasoactive intestinal peptide in Werner-Morrison syndrome or serotonin in the carcinoid syndrome) are also important transmitters in the enteric nervous system. There are surprisingly few studies of small intestinal motility and transit in these conditions. It is conceivable though that some of the diarrhoeagenic effects of vasoactive intestinal peptide (in Werner-Morrison syndrome) and serotonin (in the carcinoid syndrome) could be due to the direct effects of these peptides on motility. To investigate this possibility adequately, methods need to be developed that allow non-invasive assessments of regional motor function without the functional perturbations induced by intubation and steady-state perfusion.
THE RELATIONSHIP OF GASTROINTESTINAL TRANSIT TO MOTILITY IN SMALL INTESTINAL MOTILITY DISORDERS
Some of the effects of deranged small intestinal motility can be predicted from a simple understanding of the factors that govern liquid flow. The consequences of normal and abnormal motility may also be determined by the functional specialization of certain regions. Thus, the motor function of the duodenum is an important determinant of gastric emptying. Inadequate propulsion of thyme from the proximal small intestine due to motor inco- ordination in diseases such as diabetes mellitus or scleroderma results in a resistance to and a delay in gastric emptying (Camilleri et al, 1986b). Consistent with this, the emptying rate of a solid radiolabelled meal was decreased in seven patients with manometric features of intestinal dys- motility, suggesting that duodenal motility plays an important role in gastric emptying and the flow of thyme into the intestine. This relationship between impaired transit of thyme out of the stomach and chronic intestinal dys- motility, which was first established in our laboratory, has been confirmed by Mayer et al (1988). Furthermore, in eight patients with neuropathic chronic intestinal pseudo-obstruction, small intestinal transit times were markedly prolonged, and correlated with the intestinal dysfunction observed manometrically (Camilleri et al, 1986a). Such prolongation of transit also occurs in myopathic disorders (Greydanus et al, 1990).
Studies of ileocolonic transit in small intestinal dysmotility have also demonstrated different patterns of ileal emptying in neuropathic and myo- pathic disorders. Thus, ileocolonic transfer of radiolabelled solid 1 mm resin pellets occurs less rapidly in patients with myopathic pseudo-obstruction than in those with neuropathic disorders or healthy controls (Greydanus et al, 1990). These scintigraphic, non-invasive methods are of especial value for the assessment of motor function in the less accessible segments of the intestine and may provide an explanation for the greater propensity for bacterial overgrowth in myopathic disorders.
Disturbances in small intestinal motility and transit also occur in IBS.
SMALL INTESTINAL MOTILITY AND TRANSIT IN DISEASE 445
Kellow and Phillips (1987) observed that ileal propulsive waves and clusters of jejunal pressure waves were more common in IBS patients when com- pared with controls. In the subgroup of patients with IBS and diarrhoea, more frequent MMCs with a relatively high propagation velocity were noted. Abnormalities of small intestinal transit were also described in IBS patients by Cann et al (1983), who found that small intestinal transit times and whole gut transit times were significantly shorter in patients with diarrhoea compared with healthy controls. In contrast, IBS patients with significant bloating had slow distal small intestinal transit (Trotman and Price, 1986). Recent scintigraphic studies with similar fixed-size, solid radiolabelled particles have confirmed that 50% of patients with IBS and diarrhoea have rapid small intestinal transit. The most impressive abnor- mality was, however, the rapid transit in the ascending and transverse colon in IBS patients compared with healthy controls. Interestingly, stool weight is positively correlated with the rate of emptying of the combined ascending and transverse regions of the colon (Vassallo et al, 1990).
Transit measurements currently in use as research procedures can establish the precise region of abnormal motor function in the gut and have potential clinical application. These tests are currently being adapted to make them less costly so that they may be applied more readily to diagnostic studies of small intestinal motility, epidemiological screening studies and the assessment of response to treatment (Camilleri et al, 1990b).
CLINICAL EVALUATION AND TREATMENT OF SMALL INTESTINAL MOTILITY DISORDERS
The most important step in diagnosis is an awareness that dysmotility might explain a variety of small intestinal symptoms. In general, most small intestinal disorders result in stasis, which causes nausea, vomiting, bloating, distension, anorexia, weight loss and abdominal pain. Exclusion of mech- anical obstruction and significant mucosal disease will require endoscopy, contrast radiology, non-invasive imaging, tests of mucosal function and, less frequently, laparotomy. Thereafter, motility and transit studies can confirm the clinical impression of dysmotility, and other tests can be aimed at excluding systemic or neurological disease that may be associated with disordered small intestinal motility (Camilleri and Phillips, 1989).
Most often, neurological disease affects the autonomic nervous system, and specific clinical evaluations and indirect tests of autonomic function (Table 3) are very useful in identifying the presence of other visceral denervation (Camilleri, 1990; Vassallo et al, 1991). The close concordance of abdominal vagal dysfunction with cardiovagal neuropathy in diabetic patients (Buysschaert et al, 1985) suggests that these tests provide a reliable picture of autonomic function, including that of the gastrointestinal tract. Preliminary data suggests that patients who present with symptoms sug- gestive of intestinal dysmotility may have a visceral dysautonomia that is not recognizable with conventional methods of testing (Camilleri and Fealey,
446 M. CAMILLERI AND M. VASSALLO
Table 3. Components in the evaluation for extrinsic neurological disease in patients with gastrointestinal motor dysfunction.
Component Specific features
History
Medications
Past history
Family history
Examination
Postural dizziness, control of blood pressure Disturbances of vision Sweating Urinary disturbances or infections Sensory or motor deficits
Blood pressure and pulse (with patient supine and standing) Pupils (size, reaction to light) Cranial nerves Sensation Motor function
Gastrointestinal manometry (?) RR interval (electrocardiographic) responses to Valsalva manoeuvre and
pulse rate variation (oscillation) with deep breathing Pupillary responses to 0.1% adrenaline (epinephrine, USP), 0.125%
pilocarpine, 5% cocaine drops Thermoregulatory sweat test Quantitative sudomotor axon reflex test (to iontophoresed acetylcholine) Blood pressure and plasma noradrenaline (with patient supine and
standing) Screen for peripheral neuropathy Magnetic resonance imaging of the brain
1990; Balm et al, 1990)) but can be detected by tests of autonomic functional gastrointestinal motility (Table 3).
Once a diagnosis is established, treatment needs to be tailored to the severity of symptoms, the regions affected and the type of motor defect. When abdominal pain is the major symptom, multiple fruitless laparotomies may be performed, even in the absence of any evidence of mechanical obstruction. The aims of treatment are the correction of dehydration (more likely in acute presentations) and malnutrition, improvement of intestinal propulsion and the relief of symptoms. In less severe cases, no specific treatment may be needed apart from reassurance and simple measures such as analgesia. When the condition is more severe, a low-fat, low-fibre diet with supplemental vitamins, calories and protein given orally or enterally may suffice, but in the most severe cases total parenteral nutrition will be needed. Parenteral feeding can reverse the nutritional deficiencies (Warner and Jeejeebhoy, 1985), but is associated with significant morbidity and mortality from major vessel thrombosis, infections and cholestatic liver
SMALL INTESTINAL MOTILITY AND TRANSIT IN DISEASE 447
disease. Thus, other options must be explored fully before parenteral feeding is undertaken.
Patients with neuropathic motility disorders appear to respond better to prokinetic agents than those with myopathy. When the smooth muscle is infiltrated or destroyed by myopathic processes, pharmacological agents cannot be expected to restore useful motor function. Bethanechol and metoclopramide (Schuffler et al, 1981) have proven disappointing in the treatment of the pseudo-obstructive syndrome. Encouraging results have been obtained with cisapride (Camilleri et al, 1986a, 1989b), but these need to be evaluated further in larger numbers of patients over a longer treatment period. Preliminary data suggest that erythromycin holds promise as a prokinetic agent in chronic intestinal pseudo-obstruction (Miller et al, 1990).
Venting enterostomies reduce the need for hospitalization for recurrent episodes of pseudo-obstruction in patients on home parenteral nutrition (Pitt et al, 1985). There is also anecdotal evidence that venting facilitates decompression of the gut, after which prokinetic medications are more likely to help. Surgery is rarely of help; it is occasionally of benefit to resect a segment of especially severely diseased gut, for instance the colon, or to bypass it, as with duodenojejunostomy for megaduodenum. With far advanced disease, stasis of secretions in the upper gut can be a major problem even if parenteral nutrition is used. Subtotal enterectomy has been advocated for these most severely affected patients (Mughal and Irving, 1988).
SUMMARY
Disorders of small intestinal motility and transit are becoming increasingly recognized partly as a result of a greater awareness of their existence and partly because suitable diagnostic methods are more widely available. Usually, the neuropathic and myopathic forms can be separated, and gut disease secondary to a generalized neuromuscular disorder can be identified by the clinician. The availability of better non-invasive methods for the diagnosis of disorders of motility and transit would greatly facilitate their management. Treatment must include the restoration and maintenance of nutrition, attempts to improve intestinal motor function and resection of any segments of localized disease. Regrettably, all such measures are ineffective in the severest cases. In the future, a greater understanding of the enteric neural control of the smooth muscle and an ability to manipulate it with novel, specific drugs or peptidergic receptor agonists and antagonists, or electrical pacing, may lead to more effective therapies.
Acknowledgements
This chapter is based in part on data acquired during support from the Mayo Foundation and the National Institutes of Health Core Center Grant DK34988. We wish to thank Mrs Cindy Stanislav for typing and preparing this manuscript.
448 M. CAMILLERI AND M. VASSALLO
REFERENCES
Andersen 0, Lindberg J, Modigh K & Reske-Nielsen E (1972) Subacute dysautonomia with incomplete recovery. Acta Neurologica Scandinavica 48: 510-519.
Appenzeller 0 & Kornfeld M (1973) Acute pandysautonomia. Clinical and morphologic study. Archives of Neurology 29: 334-339.
Azpiroz F & Malagelada J-R (1987) Gastric tone measured by an electronic barostat in health and postsurgical gastroparesis. Gastroenterology 92: 934943.
Balm R, Zinsmeister A. Grevdanus M et al (1990) Visceral dvsautonomia in a subset of uatients with idiopathic chronic intestinal pseud%o-obstruction. dastroenterology 98: 324 (abstract).
Battle WM, Rubin MR, Cohen S & Snape WJ Jr (1979) Gastrointestinal motility dysfunction in amyloidosis. New England Journal of Medicine 301: 24-25.
Buysschaert M, Donckier J, Dive A et al (1985) Gastric acid and pancreatic polypeptide response to sham feeding are impaired in diabetic subjects with autonomic neuropathy. Diabetes 34: 1181-1185.
Camilleri M (1989) Jejunal manometry in distal subacute mechanical obstruction: significance of prolonged simultaneous contractions. Gut 30: 468-475.
Camilleri M (1990a) Disorders of gastrointestinal motility in neurologic diseases. Mayo Clinic Proceedings 65: 825-846.
Camilleri M (1990b) Medical treatment of chronic intestinal pseudo-obstruction. Practical Gastroenterology (in press).
Camilleri M & Fealey RD (1990) Idiopathic autonomic denervation in eight patients presenting with functional gastrointestinal disease: a causal association? Digestive Diseases and Sciences 35: 609-616.
Camilleri M & Malagelada J-R (1984) Abnormal intestinal motility in diabetics with gastro- paresis. European Journal of Clinical Investigation 14: 420-427.
Camilleri M & Phillips SF (1989) Disorders of small intestinal motility. Gastroenterology Clinics of North America B(2): 405-424.
Camilleri M, Brown ML & Malagelada J-R (1986a) Impaired transit of thyme in chronic intestinal pseudo-obstruction: correction by cisapride. Gastroenterology 91: 619-626.
Camilleri M, Brown ML & Malagelada J-R (1986b) Relationship between impaired gastric emptying and abnormal gastrointestinal motility. Gastroenterology 91: 94-99.
Camilleri M, Colemont LJ, Phillips SF et al (1989a) Human gastric emptying and colonic filling of solids characterized by a new method. American Journal of Physiology 257: G284- G290.
Camilleri M, Malagelada J-R, Abel1 TL et al (1989b) Effect of six weeks of treatment with cisapride in gastroparesis and intestinal pseudoobstruction. Gastroenterology 96: 704-712.
Camilleri M, Greydanus M, Poano M et al (1990) Towards a cost-effective gastric emptying test. Gastroenterology 98: A333.
Cann PA, Read NW, Brown C et al (1983) Irritable bowel syndrome: relationship of disorders in the transit of a single solid meal to symptom patterns. Gut 24: 405-411.
Code CF & Marlett JA (1975) The interdigestive myo-electric complex of the stomach and small bowel of dogs. Journal of Physiology 246: 289-309.
Cohen S, Fisher R, Lipshutz W et al (1972) The pathogenesis of esophageal dysfunction in scleroderma and Raynaud’s disease. Journal of Clinical Investigation 51: 2663-2668.
Cohen S, Laufer I, Snape WJ Jr et al (1980) The gastrointestinal manifestations of scleroderma: pathogenesis and management. Gastroenterology 79: 155-166.
Colemont LJ & Camilleri M (1989) Chronic intestinal pseudoobstruction: diagnosis and treatment. Mayo Clinic Proceedings 64: 60-70.
Collins SM & Vermillion DL (1986) Isolated intestinal smooth muscle response to inflam- mation induced in the rat by Trichinella spiralis infection. Journal of Physiology 378: 24P.
el Newihi H. Doolev CP. Saad C et al (1988) Imoaired exocrine oancreatic function in diabetics with diarrhea and peripheral neuropathy. &Digestive Diseases and Sciences 33: 705-710.
Feldman F & Marshak RH (1963) Dermatomyositis with significant involvement of the gastrointestinal tract. American Journal of Roentgenology, Radium Therapy and Nuclear Medicine 90: 746752.
Feldman M & Schiller LR (1983) Disorders of gastrointestinal motility associated with diabetes mellitus. Annals of Internal Medicine 98: 378-384.
SMALL INTESTINAL MOTILITY AND TRANSIT IN DISEASE 449
Fich A, Neri M, Camilleri M et al (1990a) Stasis syndromes following gastric surgery: clinical and motility features of sixty symptomatic patients. Journal of Clinical Gastroenterology 12: 505-512.
Fich A, Phillips SF, Neri M et al (1990b) Regulation of postprandial motility in the canine ileum. American Journal of Physiology 259: G767-G774.
Fox-Robichaud AE & Collins SM (1986) Altered calcium handling properties of jejunal smooth muscle from the nematode-infected rat. Gastroenterology 91: 1462-1469.
Greydanus M, Camilleri M, Colemont LJ et al (1990) Ileocolonic transfer of solid thyme in small intestine neuropathies and myopathies. Gasfroenferology 99: 158-164.
Harik SI, Ghandour MH, Farah FS & Afifi AK (1977) Postganglionic cholinergic dys- autonomia. Annals of Neurology 1: 393-396.
Hensley GP & Soergel KH (1968) Neuropathologic findings in diabetic diarrhoea. Archives of Pathology 85: 587-597.
Hopkins A, Neville B & Bannister R (1974) Autonomic neuropathy of acute onset. Lancet i: 769-771.
Hopkins IJ, Shield LK & Harris M (1981) Subacute cholinergic dysautonomia in childhood. Clinical and Experimental Neurology 17: 147-151.
Horowitz M, McNeil JD, Maddern GJ, Collins PJ & Shearman DJ (1986) Abnormalities of gastric and esophageal emptying in polymyositis and dermatomyositis. Gustroenterology 90: 434-439.
Horowitz M, Maddox A, Maddern GJ et al (1987) Gastric and esophageal emptying in dystrophia myotonica. Effect of metoclopramide. Gastroenterology 92: 57G577.
Hyman PE, McDiarmid SV, Napolitano J, Abrams CE & Tomomasa T (1988) Antroduodenal motility in children with chronic intestinal pseudo-obstruction. Journal of Pediatrics 112: 899-905.
Inamdar S, Easton LB & Lester G (1982) Acquired postganglionic cholinergic dysautonomia: case report and review of literature. Pediatrics 70: 976-978.
Karlstrom L & Kelly KA (1989) Roux-Y gastrectomy for chronic gastric atony. American Journal of Surgery 157: 44-49.
Kellow JE & Phillips SF (1987) Altered small bowel motility in irritable bowel syndrome is correlated with symptoms. Gastroenterology 92: 1885-1893.
Kellow JE &Phillips SF (1989) Functional disorders of the small intestine. In Snape WJ Jr (ed.) Pathogenesis of Functional Bowel Disease, pp 171-198. New York: Plenum.
Kellow J, Phillips SF, Miller LJ et al (1985) Abnormalities of motility and absorption in an outbreak of chronic diarrhea. Gastroenterology 88: 1442 (abstract).
Kellow JE, Borody TJ, Phillips SF, Tucker RL & Haddad AC (1986) Human interdigestive motility: variations in patterns from esophagus to colon. Gastroenterology 91: 386-395.
Kerlin P, Zinsmeister A & Phillips SF (1982) Relationship of motility to flow of contents in the human small intestine. Gastroenterology 82: 701-706.
Kingham JGC, Brown R, Colson R et al (1984) Jejunal motility in patients with functional abdominal pain. Gut 25: 375-380.
Kirby RS, Fowler CJ, Gosling JA & Bannister R (1985) Bladder dysfunction in distal autonomic neuropathy of acute onset. Journal of Neurology, Neurosurgery and Psychiatry 68: 762-767.
Krishnamurthy S & Schuffler MD (1987) Pathology of neuromuscular disorders of the small intestine and colon. Gastroenterology 93: 610-639.
Krishnamurthy S, Kelly MM, Rohrmann CA & Schuffler MD (1983) Jejunal diverticulosis. A heterogeneous disorder caused by a variety of abnormalities of smooth muscle or myenteric plexus. Gastroenterology 85: 538-547.
Kruis W, Azpiroz F & Phillips SF (1985) Contractile patterns and transit of fluid in canine terminal ileum. American Journal of Physiology 249: G264-G270.
Kumar D & Wingate DL (1985) The irritable bowel syndrome: a paroxysmal motor disorder. Lancet ii: 973-977.
Lang IM, Sarner SK & Condon RE (1986) Gastrointestinal motor correlates of vomiting in the dog: quantification and characterization as an independent phenomenon. Gastro- enterology 90: 40-47.
Low PA, Walsh JC, Huang CY & McLeod JL (1975) The sympathetic nervous system in diabetic neuropathy. A clinical and pathological study. Bruin 98: 341-356.
Malagelada JR, Rees WD, Mazzotta LJ & Go VL (1980) Gastric motor abnormalities in
450 M. CAMILLERI AND M. VASSALLO
diabetic and postvagotomy gastroparesis: effect of metoclopramide and bethanechol. Gastroenterology 78: 286-293.
Malagelada J-R, Camilleri M & Stanghellini V (1986) Manometric Diagnosis of Gastrointestinal Motility Disorders. New York: Thieme.
Mathias JR, Carlson GM, DiMarino AJ et al (1976) Intestinal myoelectric activity in response to live Vibrio cholerae and cholera enterotoxin. Journal of Clinical Investigation 58: 91-96.
Mathias JR, Fernandez A, Sninsky CA, Clench MH & Davis RH (1984) Nausea, vomiting and abdominal pain after Roux-en-Y anastomosis: motility of the jejunal limb. Gastro- enterology 88: 101-107.
Mayer EA, Elashoff J, Hawkins R et al (1988) Gastric emptying of mixed solid-liquid meal in patients with intestinal pseudoobstruction. Digestive Diseases and Sciences 33: 10-18.
Mearin F, Camilleri M & Malagelada J-R (1986) Pyloric dysfunction in diabetics with recurrent nausea and vomiting. Gastroenterology 90: 1919-1925.
Miller SM, O’Dorisio TM, Thomas FB et al (1990) Erythromycin exerts a prokinetic effect in patients with chronic idiopathic intestinal pseudo-obstruction. Gastroenterology 98: 375 (abstract).
Mughal MM & Irving MH (1988) Treatment of end stage chronic intestinal pseudo-obstruction by subtotal enterectomy and home parenteral nutrition. Gut 29: 1613-1617.
Pitt HA, Mann LL, Berquist WE et al (1985) Chronic intestinal pseudo-obstruction. Manage- ment with total parenteral nutrition and venting enterostomy. Archives of Surgery 120: 614-618.
Schiller LR, Santa Ana CA, Schmulen AC et al (1982) Pathogenesis of fecal incontinence in diabetes mellitus: evidence for internal-anal-sphincter dysfunction. New England Journal of Medicine 307: 1666-1671.
Schuffler MD & Beegle RG (1979) Progressive systemic sclerosis of the gastrointestinal tract and hereditary hollow visceral myopathy: two distinguishable disorders of intestinal smooth muscle. Gastroenterology 77: 664-671.
Schuffler MD, Rohrmann CA, Chaffee RG et al (1981) Chronic intestinal pseudo-obstruction: a report of 27 cases and review of the literature. Medicine 60: 173-196.
Sonsino E. Mouv R. Foucaud P et al (1984) Intestinal oseudoobstruction related to cvto- megalbvirus’infection of the myentkric plexus. New&England Journal of Medicine ill: 196197.
Spiller RC, Brown ML & Phillips SF (1987) Emptying of the terminal ileum in intact humans: influence of meal residue and ileal motility. Gastroenterology 92: 724-729.
Stanghellini V, Camilleri M & Malagelada J-R (1987) Chronic idiopathic intestinal pseudo- obstruction: clinical and intestinal manometric findings. Gut 28: 5-12.
Stryker SJ, Borody TJ, Phillips SF et al (1985) Motility of the small intestine after procto- colectomy and ileal pouch-anal anastomosis. Annals of Surgery 201: 351-356.
Summers RW, Anuras S & Green J (1983) Jejunal manometry patterns in health, partial intestinal obstruction and pseudoobstruction. Gastroenterology 85: 1290-1300.
Szurszewski JH (1969) A migrating electric complex of the canine small intestine. American Journal of Physiology 217: 1757-1763.
Szurszewski JH & Weems WA (1976) Control of gastrointestinal motility by prevertebral ganglia. In Bulbring E & Shuba MF (eds) Physiology of Smooth Muscle, pp 313-319. New York: Raven.
Takayama H, Kayahaya Y, Kashihara N et al (1987) A case of postganglionic cholinergic dysautonomia. Journal of Neurology, Neurosurgery and Psychiatry 50: 915-918.
Thompson DG & Malagelada JR (1982) Vomiting and the small intestine. Digestive Diseases and Sciences 27: 1121-1125.
Trotman JF & Price CC (1986) Bloated irritable bowel syndrome defined by dynamic 99mTc- bran scan. Lancer ii: 364-366.
Vantrappen G, Janssens J, Hellemans J & Ghoos Y (1977) The interdigestive motor complex of normal subjects and patients with bacterial overgrowth of the small intestine. Journal of Clinical Investigation 59: 1158-1166.
Vantrappen G, Janssens J, Coremans G & Jian R (1986) Gastrointestinal motility disorders. Digestive Diseases and Sciences 31: 5S-25s.
Vassallo M, Camilleri M, Phillips S et al (1990) R e g’ ional transit disturbances in the unprepared
SMALL INTESTINAL MOTILITY AND TRANSIT IN DISEASE 451
gut in diarrhea-predominant irritable bowel syndrome (IBS). Gastroenterology 99: 1206 (abstract).
Vassallo M, Camilleri M, Caron BL et al (1991) Gastrointestinal motor dysfunction in acquired selective cholinergic dysautonomia associated with infectious mononucleosis. Gastro- enterology 100: 252-258.
Walsh CH, Cooper BT, Wright AD, Malins JM & Cooke WT (1978) Diabetes mellitus and coeliac disease: a clinical study. Quarterly Journal of Medicine 47: 89-100.
Warner E & Jeejeebhoy KN (1985) Successful management of chronic intestinal pseudo- obstruction with home parenteral nutrition. Journal of Parenteral and Enteral Nutrition 9: 173-178.
Yahr MD & Frontera AT (1975) Acute autonomic neuropathy. Its occurrence in infectious mononucleosis. Archives of Neurology 32: 132-133.
Yoshida MM, Schuffler MD & Sumi SM (1988) There are no morphologic abnormalities of the gastric wall or smooth muscle in patients with diabetic gastroparesis. Gastroenterology 94: 907-914.
Young RR, Asbury AK, Adams RD & Corbett JL (1969) Pure pan-dysautonomia with recovery. Transactions of the American Neurological Association 94: 355-357.