35
| Date post: | 15-Aug-2015 |
| Category: |
Education |
| Upload: | free-education-for-all |
| View: | 24 times |
| Download: | 0 times |


Imatinib and Beyond: Protein Kinase Inhibitors as Cancer Therapeutics

Protein Kinases as Drug TargetsProblem:
There are over 500 protein kinases encoded by the human genome.
No/yes
sufficient specificity for clinical benefit
There are at least 120 members of the tyrosine kinase family alone
Can a drug target just one?
All of these kinases have presumably evolved from a common ancestor and have at least one substrate (ATP) in common

Protein Kinases: Targets for Cancer Chemotherapy
enzyme
OH
enzyme
O
P O
O -
- O PO42-
ATP ADPprotein kinase
phosphatase
PP
Ras-GDP
Ras-GTP
Raf Raf
MEK MEK-P
MAPK MAPK-P
proliferation
growth factor
growth factor receptoroutside
insideadaptor
MEK-Ser MEK-Ser-PO42-
inactive active
MEK-Ser MEK-Asp -
inactive active
MEK gene mutated MEK gene
OH could be Ser, Thr, Tyr
OFF ON
MEK-

HSC MPP
CLP
CMP
B cells
NK cells
T cells
dendritic cells
monocytes/macrophages
neutrophilsbasophilsmast cellseosinophils
erythrocytes
megakaryocytes - platelets
Hematopoiesis in CMLmultipotent stem cells
multipotent progenitor oligopotent
progenitor differentiated cell types
symptoms
• fever• fatigue• bleeding
Blast cells: transformed immature precursors

Imatinib and Related Drugs Target Philadelphia Chromosome Positive CML
• BCR-ABL fusion creates a dys-regulated tyrosine kinase that drives the proliferation of CML clones
protein kinase active site
bind ATP
bind target protein substrate
imatinib
specific kinase inhibition
A priori, targeting the protein substrate binding site might be expected to provide more specificity, but…………………
Imatinib competes with ATP for binding to the BcrAbl Kinase

The Imatinib Experience
• 82% of patients achieve a complete cytogenetic response (65-85%)• majority achieve a major molecular response (40-60%)• 7 year overall survival rate 90% • event free survival rate 81% (65-85%)
Positives
results from the International Randomized Study of Interferon Versus STI571 (IRIS) trial 7-year follow up
Blood (2008) 112, 186 various studies from 2003-2008
Gambacorti-Passerini and Piazza (2014) Am. J. Hematol
Persons with CML can now be expected to have a normal life expectancy when treated with TKIs.

• Imatinib, however, does not destroy cancer stem cells
• If you discontinue imatinib, CML returns
• Imatinib is the perfect drug because once you are on it, you are on it forever
If you place a cancer cell under selective pressure for long enough without killing it, what will happen?
The Imatinib Experience (Continued)
Negatives
• Current costs ~$100,000 annually

Negatives
• 18% of patients do not achieve a complete cytogenetic response• 10% of patients who achieve a complete cytogenetic response lose their response• 4-8% of patients are intolerant to imatinib
The Imatinib Experience (Farmaco Resistenza)
mutated kinase active site
bind ATP
bind target protein substrate
imatinib
kinase activity
the mutated kinase must still bind ATP and have kinase activity to drive proliferation
resistance can occur via pre-existing or new mutations in BRC-ABL
Since imatinib and ATP bind to the same site there are a limited number of degrees of freedom through which an enzyme can become resistant to imatinib and still bind ATP

Dasatinib
• A second generation BRC-ABL inhibitor used to treat chronic myeloid leukemia
• Approved for all phases of Philadelphia-positive CML with resistance or tolerance to prior therapy, including imatinib

1st and 2nd Generation BCR-ABL Inhibitors
Dasatinib
This chemistry added to improve drug’s pharmacological properties, not needed for activity
Dasatinib lacks all this extra chemistry
destra/rightsinistra/left
chiudi gli occhi e strabismo

Comparison of Abl Kinase Structure with Dasatinib and Imatinib Bound
extra functional groups of imatinib bind to a hydrophobic pocket in Abl kinase not needed for binding ATP: imparts specificity
steric clashes with extra functional groups block active conformation
mutations in this region can interfere with imatinib binding without affecting ATP or dasatinib binding
ATP binding pocket
dramatic differences in activation loop
notorious 315 mutation closer to ATP binding site affects binding of all inhibitors
lucky
imatinibdasatinib
left
right
dasatinib may have less specificity than imatinib

Multikinase Inhibitory Panels of BCR-ABL Inhibitors
Imatinib use for cancers other than CML, c-KIT/PDGF-R based cancers like gastrointestinal stromal tumors

However, in a single-institution study, 37% of bleeding episodes (any grade) occurred in patients without thrombocytopenia.[33]
Adverse Events with Dasatinib
Bleeding Related Events (mostly associated with severe thrombocytopenia): CNS hemorrhages, including fatalities, have occurred. Severe gastrointestinalhemorrhage may require treatment interruptions and transfusions. Use SPRYCEL(dasatinib) with caution in patients requiring medications that inhibit platelet function or anticoagulants.
from full US prescribing information
• myelosuppression• GI symptoms• rash• fluid retention• bleeding
dealt with by dose reduction or interruption of treatment
a more specific effect on bleeding beyond reducing platelet number
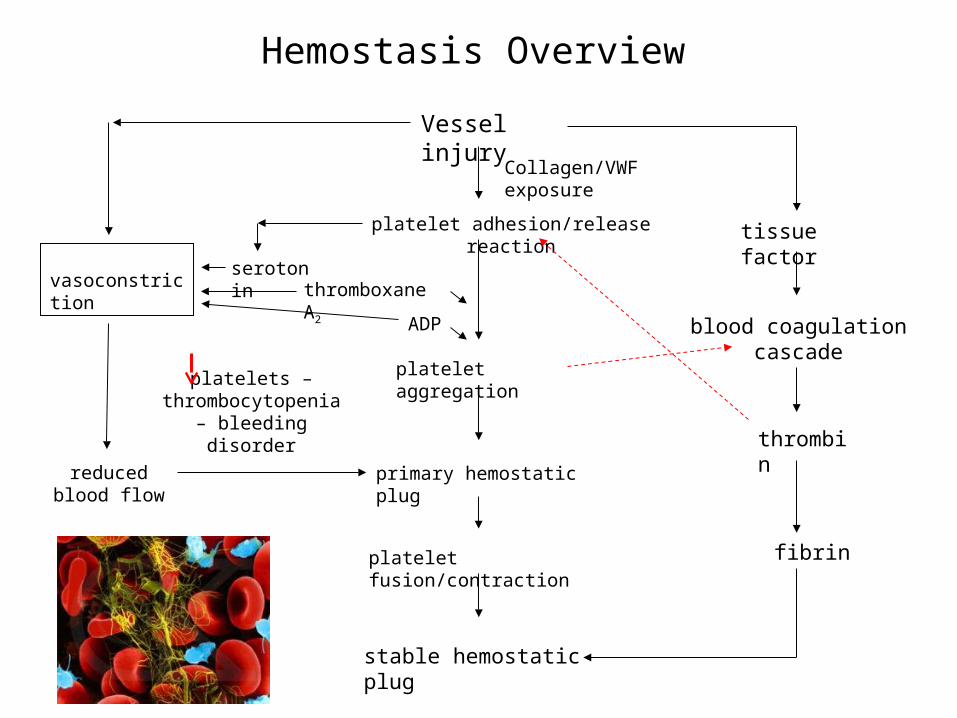
Hemostasis Overview
Vessel injury
Collagen/VWF exposure
platelet adhesion/release reaction
platelet aggregation
primary hemostatic plug
platelet fusion/contraction
stable hemostatic plug
tissue factor
blood coagulation cascade
thrombin
fibrin
thromboxane A2
ADP
serotoninvasoconstriction
reduced blood flow
platelets – thrombocytopenia –
bleeding disorder

Primary Hemostasis – Platelet Adhesion
endothelium
Von Willebrand factorcollagen
platelet
adhesion molecule
receptor
vessel damageplatelets contain receptors that bind subendothelial proteins
exposed upon vessel damage

Primary Hemostasis – Platelet Activation/Aggregation
platelet activation release reaction
aggregation
platelet
adhesion molecule
receptor
von Willebrand factor, fibronectin, vitronectin
ADP
thromboxane A2
clopidogril
aspirin
ADP ADP
Exposure of negatively charged phospholipids on
the platelet surface
Increased Ca2+

Collagen Signaling and Platelet Aggregation
A member of the Src family of kinases

The Effect of Dasatinib on Agonist-Induced Platelet Aggregation
after 2-5 hr of treatment dasatinib can reach 150 and 100 nM in the plasma of patients treated with 140 and 70 mg regimes, respectively tyrosine
phosphorylation
specific src-family phosphorylation

Multikinase Inhibitory Panels of BCR-ABL Inhibitors

Imatinib does not Interfere with Collagen-Induced Platelet Aggregation or Signaling Pathways

The Effect of Dasatinib on Collagen-Induced Signaling
or Glycoprotein VI

DASATINIB:
• targets the BCR-ABL kinase active site in a manner distinct from imatinib
• is more potent a Abl kinase inhibitor than imatinib and is not affected by some of the mutations that lead to imatinib resistance
• targets a wider spectrum of protein kinases than does imatinib
• interferes with platelet function by presumably targeting one or more Src kinases
• may be considered as a lead compound for a new class of anti-thrombotic agents
CONCLUSIONS
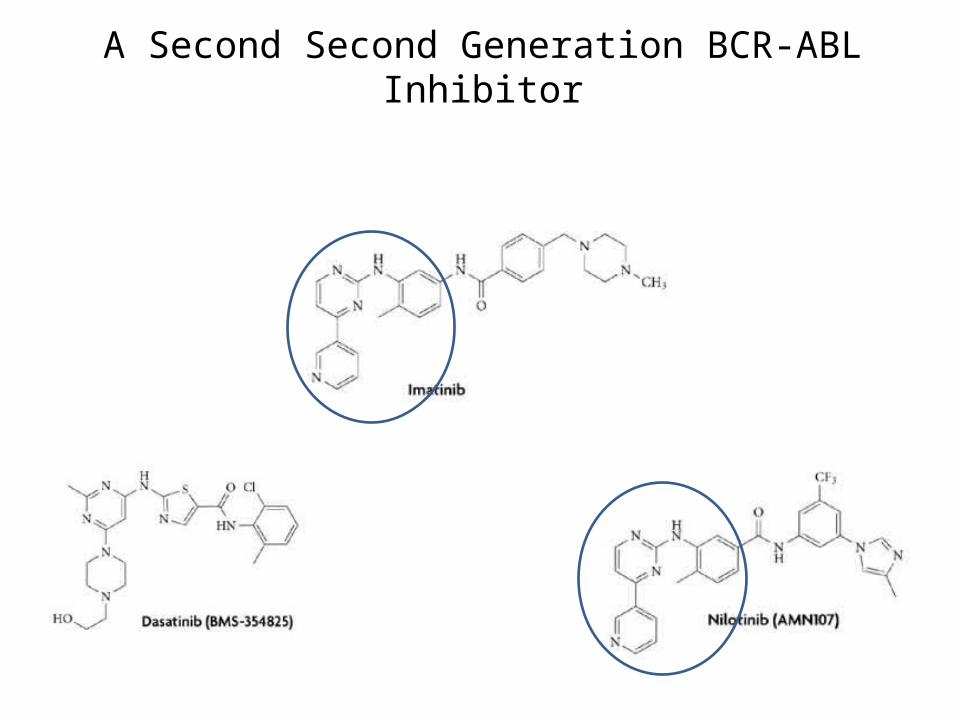
A Second Second Generation BCR-ABL Inhibitor
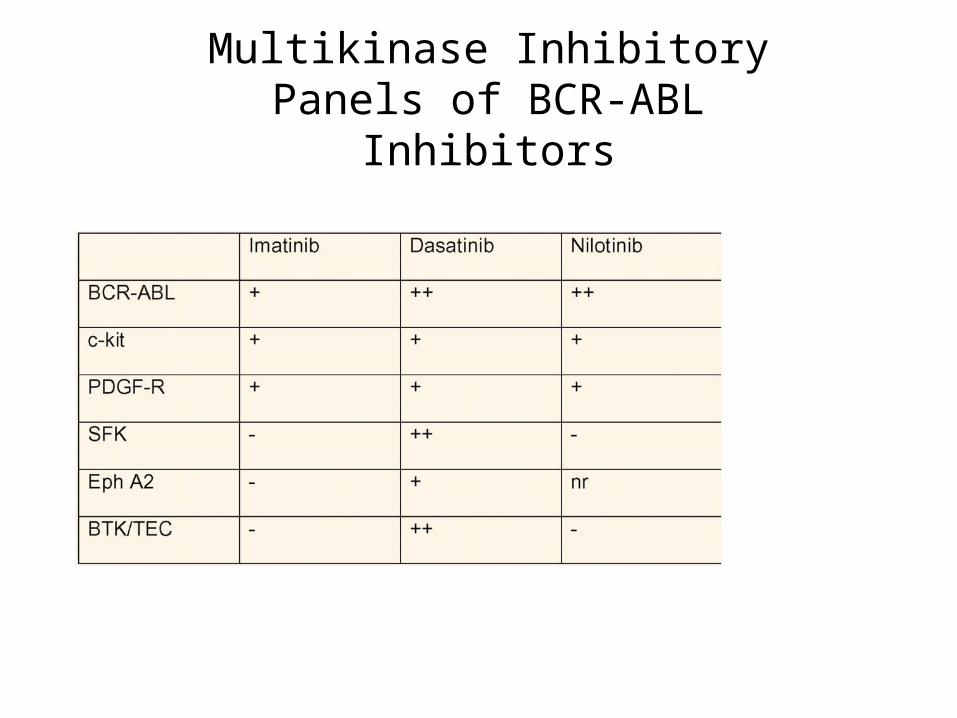
Multikinase Inhibitory Panels of BCR-ABL Inhibitors

Binding Characteristics of BCR-ABL TKI’s
common imatinib resistance mutations

Application of 2nd Generation TKIs in a Stepwise Approach to CML Treatment
A – may respond to inhibitor, evidence lacking
B – reduced sensitivity to inhibitor
C – compelling clinical evidence suggests an alternative inhibitor should be used
D – forget about second generation inhibitors, try emerging therapies

The experience with certain second generation BCR-Abl inhibitors has been sufficiently positive to consider their use in
replacing imatinib as a frontline therapy for ECP-CML

Study Protocol: MethodsRosti et al Blood (2009) 114, 4933 & Cortes et al. JCO e-pub December 14, 2009
Patient eligibility: • 18 years of age or older • diagnosis of CP (Ph+) – CML within less than 6 months • untreated or treated only with hydroxyurea or anagrelide
Patient exclusion: • WHO performance status 2 or more • uncontrolled serious medical conditions• received prior treatment with any investigational drug

Cytogenetic response (CyR) :• complete, zero Ph+ chromosomes in 20 metaphases• partial, 0-35% Ph+ metaphases• minor, 35-95% Ph+ metaphases
Study Protocol: MethodsRosti et al Blood (2009) 114, 4933 & Cortes et al. JCO e-pub December 14, 2009
Molecular response (MR) :• complete, undetectable BRC-ABL transcripts in 105 cells• major, BCR-ABL/ABL transcript ratio of less than 0.1%
Complete Hematological Response (CHR) :• normalization of peripheral blood counts• normal differential• no splenomegaly

BCRABL
CML: Complete Molecular Remission
polymerase chain reaction (PCR)

Hematological, Cytogenetic, and Molecular Responses in the European Study
primary endpoint CCgR at 12 year
expectation for imatinib (50-70%)
< 50% response to nilotinib (no interest)
70% response to nilotinib (interest)
nilotinib dose: 400 mg twice daily

major molecular response obtained in 52 % of patients by 3 months and 85% by
12 months
Kinetics of Molecular Responses to Nilotinib
adverse effects manageable with does reductions

Cytogenetic, and Molecular Responses in the MD Anderson Study
compare with historical data from MD Anderson patients treated with imatinib
• 6-month CCyR: 96% with nilotinib v 45% with sd imatinib• 12-month CCyR: 97% with nilotinib v 70/80% with hd/sd imatinib, respectively
• 12-month MMR: 81% with nilotinib v 46/54% with sd/hd imatinib, respectively
major difference between nilotinib and imatinib is the earlier occurrence of the response with nilotinib and an improved molecular response
Do either of these parameters matter in terms of patient performance and overall survival??

September 1, 2011 — The US Food and Drug Administration (FDA) recently granted accelerated approval to crizotinib (Xalkori, Pfizer) for the treatment of patients with advanced-stage nonsmall-cell lung cancer (NSCLC) that is anaplastic lymphoma kinase (ALK)-positive.
Only 4-5% of NSCLC is ALK-positive
In PROFILE 1005 (n = 136), the objective response rate (ORR) was 50%, and that included 1 complete response and 67 partial responses.
Like many targeted therapies, crizotinib comes with a hefty price tag. According to Geno Germano, president and general manager of specialty care and oncology at Pfizer, the drug will cost $9,600 per month, or $115,000 per year.
Kinase Inhibitors as “Smart” Drugs for Treating Cancer

















