46


Smart Strategies In Medical Emergency
Teams: A clinical perspective
Dana P. Edelson, MD, MS, FAHA, FHM
Assistant Professor, Section of Hospital Medicine
Executive Medical Director of Inpatient Quality & Safety
University of Chicago Medicine
10/13/2015 ©2015, American Heart Association 2

Smart Strategies In
Medical Emergency Teams:
A clinical perspective
Dana P. Edelson, MD, MS, FAHA
Executive Medical Director for Inpatient Quality & Safety
University of Chicago Medicine

4
Disclosures• Research funding:
– National Heart Lung Blood Institute
– Philips Healthcare
• Ownership interests:
– QuantHC
• Intellectual property over the algorithms described
• Patent pending, ARCD.P0535US.P2

5
Hospitalization Time Course

6
Three step model to improving outcomes

7
Recognition and activation are not physiologic
Galhotra, CCM, 2006

8
Adjusting to subtle changes in physiology

9
Automating recognition and activation

10
Traditional MET activation criteriaHillman, Lancet, 2005
Cardiac arrest AUC: 0.63

11
Modified Early Warning Score (MEWS)
3 2 1 0 1 2 3
Respiratory rate (RPM) — ≤ 8 — 9-14 15-20 21-29 ≥ 30
Heart rate (BPM) — ≤ 40 41-50 51-100 101-110 111-129 ≥ 130
Systolic BP ≤ 70 71-80 81-100 101-199 ≥ 200
Temperature (°C) — ≤35 — 35.0-38.4 — >38.5 —
AVPU — — — AlertReact to Voice
React to Pain
Unresp
Subbe, QJM, 2001
Cardiac arrest AUC: 0.76

12
Paper-based EWS scoring
10/13/2015 ©2013, American Heart Association

13
Leveraging electronic data

14
Deriving a computer-based early warning score
• Data set:
– Over 58,000 admissions
– 109 cardiac arrests on the ward
– 2,543 ICU transfers
• Methods:
– Multinomial logistic regression
– Competing risk model
– Longitudinal analysis
– Normal imputation
Churpek, CCM, 2014

15
eCART model for cardiac arrest Churpek, CCM, 2014
Cardiac arrest AUC:
0.88

16
Risk score change over timeCardiac arrest
ICU transfer
Control
Ca
rdia
c a
rre
st
sco
re
Time preceding event (hours)
55
45
50
40
-48 -12-24-36 0
Churpek, CCM, 2014

17
Risk Stratification using eCART
• Top 5% sickest patientsHigh
• Next 10%Moderate
Normal
eCART 54
eCART 50

18
Real-time implementation
DemographicsVital Signs Lab
Values
eCART
125 bpm
Alert120/80 Potassium
98% O2 Hemoglobin65 yo
ICU transfer
F(x)=…

19
0% 20% 40% 60% 80% 100%
Percent of Events Captured
RRT Called
ICU
Transfer
[n=383]
eCART
Cardiac
Arrest
[n=10]
(High/Mod Risk)
Silent phase comparison to standard care

20
0%
10%
20%
30%
40%
50%
60%
0612182430364248Per
cen
t o
f IC
U T
ran
sfer
s Id
enti
fied
Time Before ICU Transfer, Hour
eCART (High Risk) Standard Practice (RRT Called)
Threshold Timing for ICU Transfers
RRT median
1.7 hours
eCART (High Risk) Median
32.9 hours
Δ 31 hours (p<0.0001)

21
Mortality increases linearly with ICU transfer delay

22
In-Hospital Mortality by ICU transfer delay
p<0.001
< 6 hrs > 6 hrs
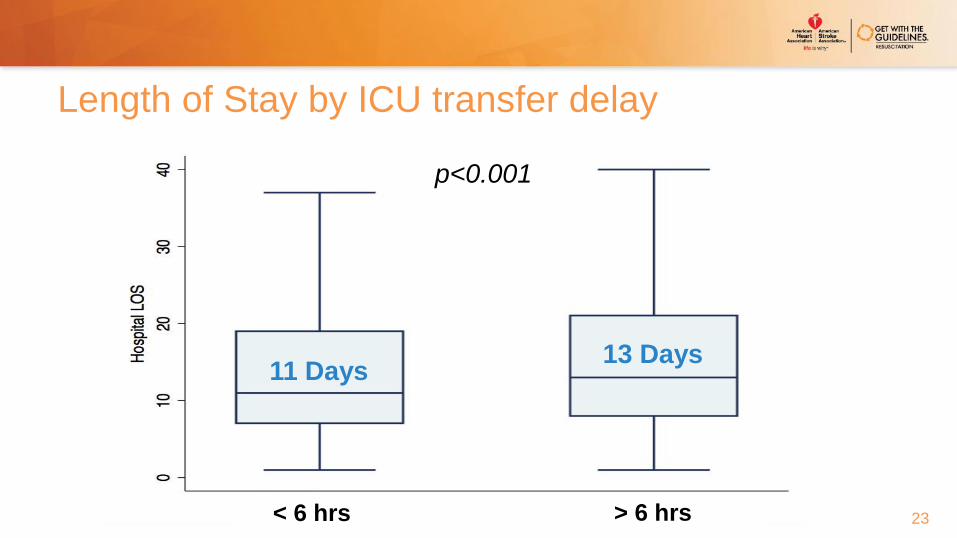
23
11 Days13 Days
Length of Stay by ICU transfer delay
p<0.001
< 6 hrs > 6 hrs

24
Real-Time Patient Dashboard

25
Real-Time Risk Trend

26
Garbage in… Tweaking future inputs
Respiratory rate
Mental status
Clinical judgment

MENTAL STATUS:
WHAT ARE THE OPTIONS?

28
AVPU scale
29
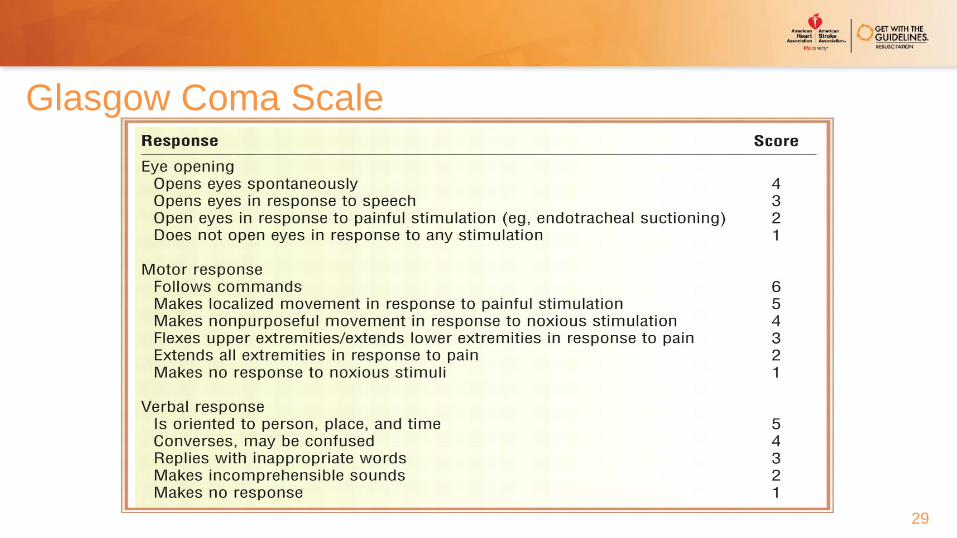
Glasgow Coma Scale

30
Richmond Agitation Sedation Scale (RASS)

31

RESPIRATORY RATE:
THE MISSING VITAL SIGN

33
Variable importance
38
40
41
43
48
51
63
66
77
100
0 10 20 30 40 50 60 70 80 90 100
GlucoseWhite blood cell count
Blood urea nitrogenTemperature
Pulse pressure indexDiastolic blood pressureSystolic blood pressure
AgeHeart rate
Respiratory rate

34
Respiratory rate is poorly recorded
Semier, Chest 2013

35
“RR” vs RR: which one is more predictive?

QUANTIFYING CLINICAL
JUDGEMENT

37
Introduction of PAR

38
The Patient Acuity Rating
• How likely is this patient to suffer a cardiac arrest or require emergent transfer to the
ICU in the next 24 hours?
1 2 3 4 5 6 7
Extremely unlikely
Extremely likely
Neither likely nor unlikely
Edelson, JHM, 2011
Cardiac arrest or ICU transfer AUC: 0.82

39
PAR sensitivities and specificities
PAR Sensitivity Specificity
7 16% 99%
≥ 6 41% 95%
≥ 5 62% 85%
≥ 4 82% 68%
≥ 3 93% 41%
≥ 2 99% 12%
≥ 1 100% 0%
Edelson, JHM, 2011

Copyright © 2015 American Medical
Association. All rights reserved.
From: The Value of Clinical Judgment in the Detection of Clinical Deterioration
JAMA Intern Med. 2015;175(3):456-458. doi:10.1001/jamainternmed.2014.7119
PAR vs MEWS: effect may be additive

RETHINKING NIGHTTIME
VITALS


From: A Prospective Study of Nighttime Vital Sign Monitoring Frequency and Risk of Clinical DeteriorationJAMA Intern Med. 2013;():-. doi:10.1001/jamainternmed.2013.7791

44
Example Clinical Decision Support Matrix by Acuity
High
• Automatic MET/RRT
• Twice daily bedside rounding with Attending
Moderate
• Bedside Rounding between RN/MD
• Proactive rounding by MET/RRT
Normal• Standard care
Low• No night-time vital signs

45
Conclusions
• Clinical deterioration on the wards is largely predictable
• Statistically derived algorithms, such as eCART, have improved accuracy over traditional
MET activation criteria
• Early identification and transfer to the ICU is associated with decreased mortality and
shorter length of stay
• Algorithms are likely to be strengthened by reliable input regarding respiratory rate, mental
status and clinical judgment

46
Questions?
10/13/2015 ©2013, American Heart Association

















