24
Smoke Inhalation & Thermal Injuries MODULE G3 Chapter 43: pp. 520-531
| Date post: | 27-Dec-2015 |
| Category: |
Documents |
| Upload: | christina-parks |
| View: | 216 times |
| Download: | 2 times |
Smoke Inhalation & Thermal Injuries
MODULE G3
Chapter 43: pp. 520-531
Smoke Inhalation & Thermal Injury
• Fire related deaths are the third most common cause of accidental death in the US.
• Prognosis• Extent and duration of smoke exposure.• Chemical composition of the smoke.• Size and depth of body surface burns.• Temperature of gases inhaled.• Age.• Pre-existing health problems.
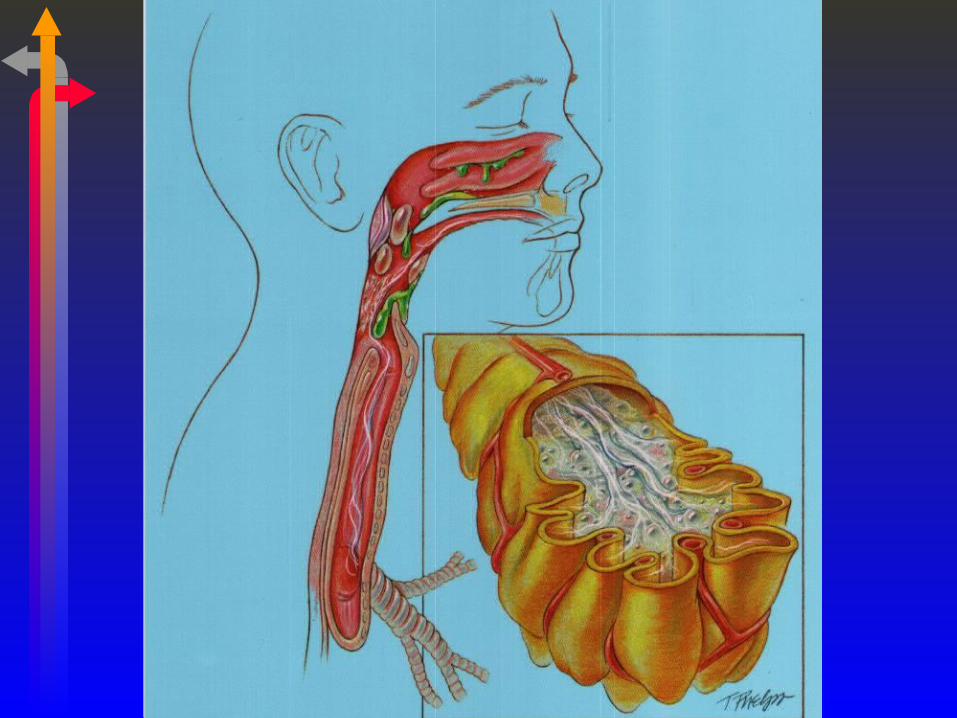
Anatomic Alterations
• Inhalation• Thermal Injury.• Steam Inhalation - rare• Chemical Injury from toxic gas.
• Body surface burns.
Thermal Injury
• Inhalation of hot gases:• Confined to the upper airway.• Airways distal to the larynx are usually spared
serious injury.• Upper airways ability to cool hot gases.• Reflex laryngospasm.• Glottic closure.
Thermal Injury
• Acute upper airway obstruction.• Occurs in 20-30% of cases.• Supraglottic region.• May rapidly develop after rapid IV fluid
administration.
Chemical Injury
• Smoke Inhalation• Damages the airway down to the alveoli.• Substances in smoke are extremely caustic
and poisonous to the body.• COHB%• Cyanide poisoning• Formaldehyde• Ammonia• Sulfur dioxide

Medical Challenge
• Injury from burns can affect every organ system
• Multiple organ failure

Stages of Smoke Inhalation and Burns
• Early or Resuscitation Phase • First 24 hours
• Intermediate Phase• 2-5 days
• Late Phase• After 5 days
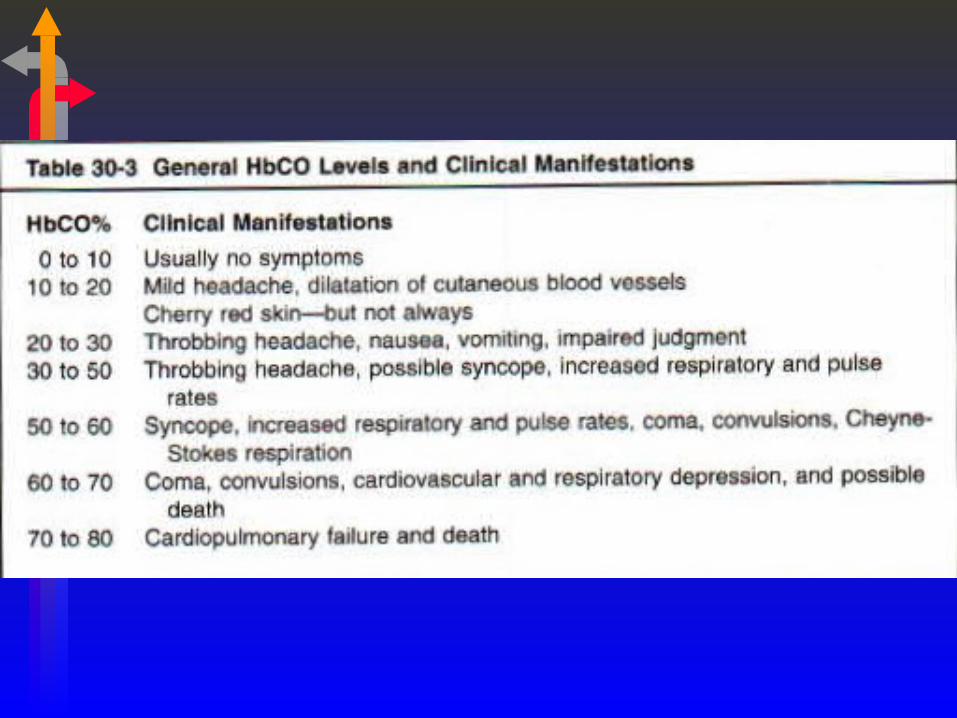
Stage I
• CO Poisoning • Affinity for the Hb is 200 – 250 times greater
than oxygen.• Left shift in the oxygen dissociation curve.• Levels greater than 40% is severe exposure.
• PaO2 may be normal or high.
• SaO2 will be low – measure with co-oximeter.
• DO NOT USE A PULSE OXIMETER
Stage I
• Cyanide Poisoning• Burning of polyurethane materials• A cyanide blood level in excess of 1 mg/L is
usually fatal• Cyanide interferes with oxygen utilization in
the mitochondria • Anaerobic metabolism & lactic acidosis
• PaO2 & SaO2 can be normal
Stage I
• Tissue Hypoxia • COHb poisoning (Anemic Hypoxia)• Cyanide poisoning (Histotoxic Hypoxia)
• Metabolic acidosis
Stage I
• Thermal Injury• Laryngospasm and glottic closure• Airway obstruction• Establish an airway
• Chemical Injury• Inflammatory Response
Stage I
• Hypovolemic Shock• Blood vessels become “Leaky”• Massive fluid shift from the blood vessels into
the tissues (third spacing)• Generalized body edema
• Decreased Chest Wall Compliance• Skin loses its elasticity• Difficult to inflate the lungs
Stage I
• Hypermetabolic State• Massive release of catecholamines from stress• Nutrition is very important
• Patients need lots of calories
• VO2 & VCO2 increases
• Acute Lung Injury (ALI)• Decreased PaO2/FIO2 ratio
. .
Stage II
• Pulmonary Edema• Decreased COP from loss of protein.• Rapid infusion of fluids.
• ARDS
• Mechanical ventilation
• Stress induced hyperglycemia develops.
• Immune system becomes depressed.• Infection sets in
Stage III
• Infections• Pneumonia
• Sepsis and multi-organ failure
• DIC (Disseminated Intravascular Coagulation)
• Pulmonary embolism
• Long term effects• Restrictive and Obstructive disorders• Bronchiolitis Obliterans
Assessment
• Level of Consciousness
• Burns to face or upper airway
• Hoarseness• Altered voice• Painful swallowing• Stridor
• Cherry red skin color
• Tachypneic• Sputum
• Black, sooty• White frothy • Purulent (later finding)
• Nausea/vomiting• Convulsions
Management
• Treat any unconscious or lethargic patient as a medical emergency.• Suspect hypoxia.• Intubate to protect the airway.
• 100 % oxygen &/or Hyperbaric Chamber• PaO2 in a hyperbaric may rise to 1,500 mm Hg
• Cyanide Poisoning• Amyl nitrite, Sodium nitrite, Sodium thiosulfate
Management
• Fluid Administration
• Bronchoscopy• Evaluate the extent of damage.• Remove mucous plugs.• Used for difficult intubations.
• CPAP with 100% oxygen
• Mechanical Ventilation• Acute Respiratory failure or • Acute Oxygenation failure
Management
• Analgesics for Pain
• FEED, FEED, FEED
• Steroids are controversial
• Aerosol Therapy• Bronchodilators (B2 agonists)• Mucolytics
Management
• Antibiotics
• Culture sputum, blood, wounds
• Prophylactic heparin therapy for PE
• Escharotomy • Cutting of burned skin• Help to treat the low compliance of the chest
wall
Important Points
• Level of Consciousness• Determine need for airway
• 100% Oxygen and Hyperbaric Chamber
• Never use Pulse Oximeter. • Well maybe…

















