17
Social Protection in Health for Social Protection in Health for Women, Newborn and Child Women, Newborn and Child Populations Populations Dr. Oscar Viscarra Zuna Dr. Oscar Viscarra Zuna
| Date post: | 16-Dec-2015 |
| Category: |
Documents |
| Upload: | keaton-laughton |
| View: | 219 times |
| Download: | 2 times |

Social Protection in Health for Social Protection in Health for Women, Newborn and Child Women, Newborn and Child PopulationsPopulations
Dr. Oscar Viscarra ZunaDr. Oscar Viscarra Zuna

Poverty is the social issue that constitutes the strongest Poverty is the social issue that constitutes the strongest violation against human rights. violation against human rights.
It is also a determining factor in the health outcomes – illness, It is also a determining factor in the health outcomes – illness, mortality and suffering - of women and men in all countries mortality and suffering - of women and men in all countries in the world.in the world.
““Human Rights and Poverty: Toward a Rights-Based approach” UN, 2000Human Rights and Poverty: Toward a Rights-Based approach” UN, 2000
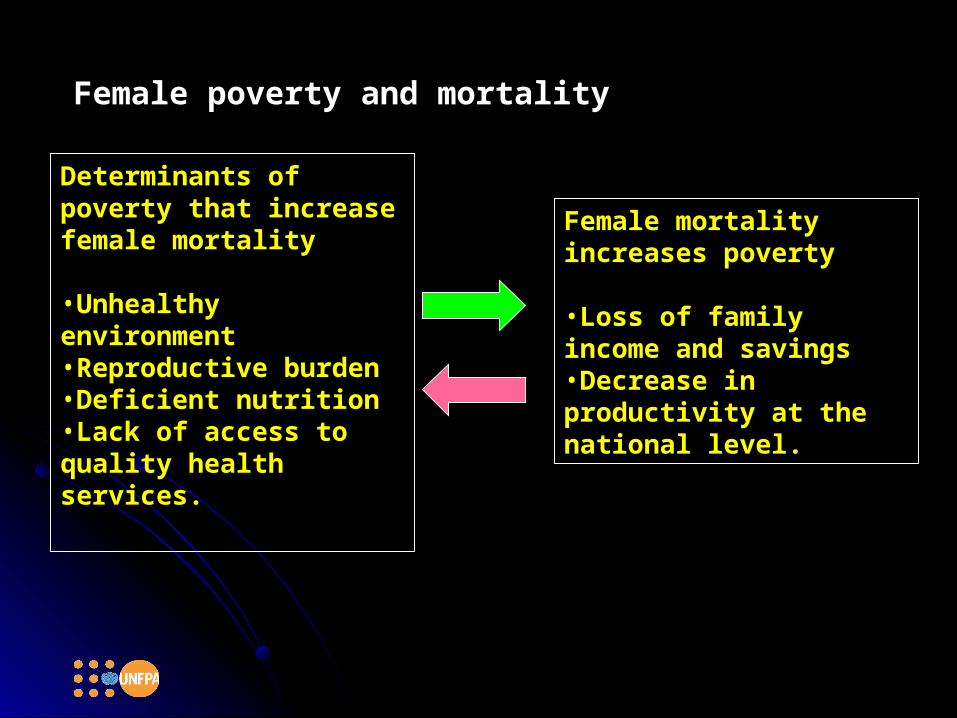
Female poverty and mortalityFemale poverty and mortality
Female mortality Female mortality increases povertyincreases poverty
•Loss of family income Loss of family income and savingsand savings•Decrease in Decrease in productivity at the productivity at the national level.national level.
Determinants of Determinants of poverty that increase poverty that increase female mortalityfemale mortality
•Unhealthy Unhealthy environmentenvironment•Reproductive burdenReproductive burden•Deficient nutritionDeficient nutrition•Lack of access to Lack of access to quality health quality health services.services.
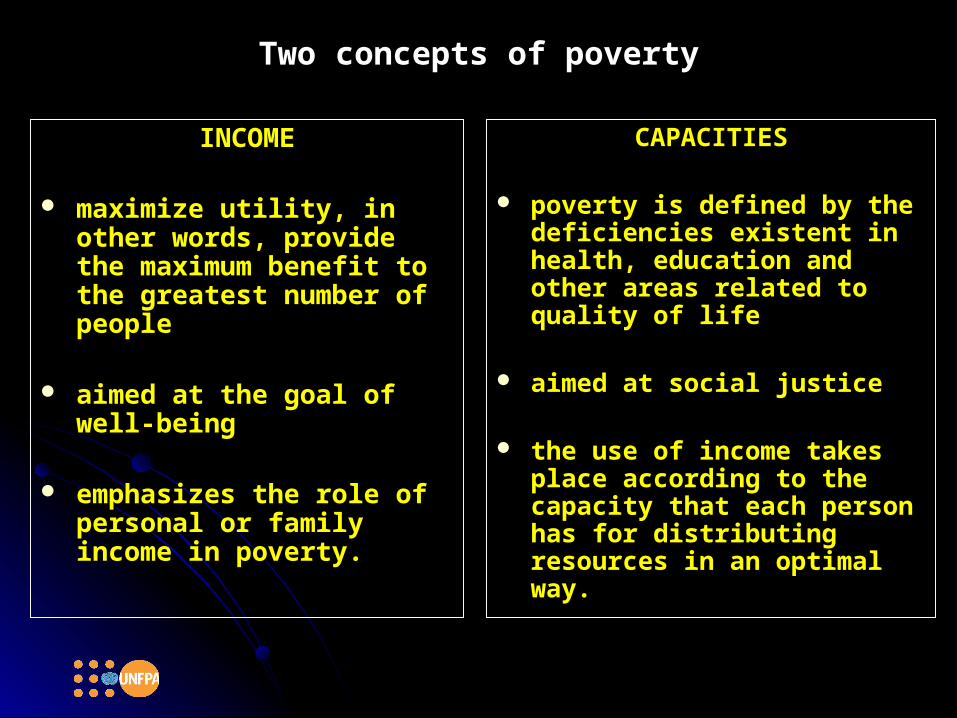
Two concepts of povertyTwo concepts of poverty
INCOMEINCOME
maximize utility, in other maximize utility, in other words, provide the maximum words, provide the maximum benefit to the greatest benefit to the greatest number of peoplenumber of people
aimed at the goal of well-aimed at the goal of well-beingbeing
emphasizes the role of emphasizes the role of personal or family income in personal or family income in poverty.poverty.
CAPACITIESCAPACITIES
poverty is defined by the poverty is defined by the deficiencies existent in health, deficiencies existent in health, education and other areas education and other areas related to quality of liferelated to quality of life
aimed at social justiceaimed at social justice
the use of income takes place the use of income takes place according to the capacity that according to the capacity that each person has for each person has for distributing resources in an distributing resources in an optimal way.optimal way.

As a resultAs a result
Access to education and health = greater capacity to Access to education and health = greater capacity to solve the problem of low income. solve the problem of low income.
High income + poor health = will not be poor in High income + poor health = will not be poor in economic terms, but will be in terms of the capacity economic terms, but will be in terms of the capacity to enjoy a healthy, full, higher-quality life.to enjoy a healthy, full, higher-quality life.
A just social system that defines beforehand the A just social system that defines beforehand the context in which women and men develop their context in which women and men develop their capacities and simultaneously provides a framework capacities and simultaneously provides a framework of opportunities and rights in which every person of opportunities and rights in which every person can equitably achieve certain goals. can equitably achieve certain goals.
Sen, A (1999) “Poverty as capability deprivation”Sen, A (1999) “Poverty as capability deprivation”
Once basic needs are defined by the people Once basic needs are defined by the people themselves, improvements can be proposed, themselves, improvements can be proposed, supporting the development of human capacities supporting the development of human capacities and the participation of individuals in the family, and the participation of individuals in the family, community and social spheres, creating strategies community and social spheres, creating strategies that can take them out of poverty.that can take them out of poverty.
The improvement should take place in the sector of The improvement should take place in the sector of the population that confronts the greatest the population that confronts the greatest deficiencies, and it would have to be sustainable.deficiencies, and it would have to be sustainable.
By giving priority to health, public policies should By giving priority to health, public policies should be targeted at the most vulnerable among the poor: be targeted at the most vulnerable among the poor: women, adolescents and youth, and disadvantaged women, adolescents and youth, and disadvantaged ethnic/racial groups.ethnic/racial groups.

““Poor sexual and reproductive health conditions are both a Poor sexual and reproductive health conditions are both a consequence and cause of poverty and hunger. consequence and cause of poverty and hunger.
This negatively affects economic well-being, decreasing the This negatively affects economic well-being, decreasing the individual’s capacity to work, just as treatment costs can individual’s capacity to work, just as treatment costs can consume scarce family income; women that live in poverty consume scarce family income; women that live in poverty conditions have less access to information and services.”conditions have less access to information and services.”
Kofi Annan, Secretary General of the United NationsKofi Annan, Secretary General of the United Nations

The burden of disease attributed to sexual and reproductive The burden of disease attributed to sexual and reproductive health is 22% for women while it is only 3% for men.health is 22% for women while it is only 3% for men.
Maternal health is the dominant burden in terms of diseases Maternal health is the dominant burden in terms of diseases
related to sexual and reproductive health among women. In related to sexual and reproductive health among women. In LAC, it represents 11.3% of the total burden of disease.LAC, it represents 11.3% of the total burden of disease.
The sexual and reproductive health burden is not limited to The sexual and reproductive health burden is not limited to effects on the woman herself, but also has intergenerational effects on the woman herself, but also has intergenerational effects: perinatal causes are 10% of the total DALYs lost that effects: perinatal causes are 10% of the total DALYs lost that are associated with reproductive illness.are associated with reproductive illness.DALYs: Disability Adjusted Life YearsDALYs: Disability Adjusted Life Years..
Ten-year projections suggest that disease related to Ten-year projections suggest that disease related to reproductive health will be the largest cause of death and reproductive health will be the largest cause of death and disability on a global level.disability on a global level. (Gwatkin, D R 2002 “The burden of disease among the Global Poor”)(Gwatkin, D R 2002 “The burden of disease among the Global Poor”)
As a response to the challenge:As a response to the challenge: Effective interventionsEffective interventions Focus on health, and sexual and reproductive rightsFocus on health, and sexual and reproductive rights Throughout the lifespanThroughout the lifespan
Three strategies in the Regional Consensus:Three strategies in the Regional Consensus:1.1. ContraceptivesContraceptives
2.2. Skilled care for all birthsSkilled care for all births
3.3. Essential Obstetric Care in the service networkEssential Obstetric Care in the service network

ContraceptivesContraceptives
Primary component for reducing maternal mortality from the Primary component for reducing maternal mortality from the perspective of avoiding unwanted pregnancies.perspective of avoiding unwanted pregnancies.
Based on evidence and the concept of Human Rights. Based on evidence and the concept of Human Rights. Particularly important for adolescents.Particularly important for adolescents.
Gráfico 13Bolivia: Tasa de Global de fecundidad deseada y
observada, por quintil de riqueza
32,3 2,2 1,9 1,6
2,1
6,7
54
2,92
3,8
0
2
4
6
8
10
Inferior Segundo Intermedio Cuarto Superior Total
TGF Deseada TGF Observada
Fuente: INE, ENDSA-2003
Graphic 13
Bolivia: Desired and observed global fertility rate, by wealth quintile
Second Intermediate Fourth
Desired TFR
Observed TFR
Source: National Institute of Statistics – INE; National Demographic and Health Survey - ENDSA, 2003

Skilled Care at BirthSkilled Care at Birth
Have skilled personnel that are responsible for delivery care, that Have skilled personnel that are responsible for delivery care, that have the competencies and skills necessary for ensuring competent have the competencies and skills necessary for ensuring competent care and that are strategically distributed. care and that are strategically distributed.
Enabling environment: medicines, supplies, functioning obstetric, Enabling environment: medicines, supplies, functioning obstetric, newborn and community networks.newborn and community networks.
100
97
77
73
59
45
83
9
45
146
967
430
189
175
Percentage of births attended by skilled personnel
Number of maternal deaths per 100,000 live births
Sub-Saharan Africa
South Asia
East Asia and Pacific
Middle East and North Africa
Latin America/Caribbean
Central, Eastern Europe/ Baltics/ CEI*
North America
Source: PRB, using data from Maternal Mortality Source: PRB, using data from Maternal Mortality in 1995: Estimates developed by WHO, UNICEF in 1995: Estimates developed by WHO, UNICEF and UNFPA, 2001.and UNFPA, 2001.

Skilled care by income quintileSkilled care by income quintileB
ang
lad
esh
Nep
al
Cha
d
Nig
er
Pak
ista
n
Mo
rocc
o
Nig
eri
a
Ind
ia
Gua
tem
ala
Uga
nd
a
Ma
li
Bur
kin
a F
aso
Gha
na
Mo
zam
biq
ue
Ken
ya
Côt
e d
’Ivoi
re
Cen
tra
l Afr
. R
ep
Hai
ti
Sen
eg
al
Za
mb
ia
Ta
nza
nia
Bol
ivia
Ma
da
gas
car
Ind
one
sia
To
go
Com
ore
s
Ma
law
i
Per
u
Phi
lipp
ine
s
Cam
ero
un
Ben
in
Nic
ara
gua
Par
ag
ua
y
Nam
ibia
Zim
ba
bw
e
Tu
rke
y
Vie
t N
am
Col
om
bia
Bra
zil
Dom
inic
an
Rep
.
Uzb
eki
stan
Kyr
gyz
Re
p.
Kaz
aks
tan
70
100
90
80
60
50
40
30
20
10
0
+ low+ low + high+ high TotalTotalSource: World Bank, 2000

Obstetric and Newborn Emergency CareObstetric and Newborn Emergency Care
Recognize, manage, stabilize and carry out effective, timely Recognize, manage, stabilize and carry out effective, timely referrals in the case of complications.referrals in the case of complications.
Capacity to effectively solve obstetric and newborn Capacity to effectively solve obstetric and newborn emergencies related to causes of maternal and newborn emergencies related to causes of maternal and newborn death. death.
Nº % Nº % Nº % Nº % Nº % Nº %
Nivel III 6 42,90 3 17,65 - - - - 5 35,71 14 100
Nivel II 14 25,90 8 14,81 - - 5 9,26 27 50,00 54 100
Nivel I 0 - 2 14,29 - - 2 11,76 13 76,47 17 100
Total 20 23,50 13 15,29 - - 7 8,24 45 52,94 85 100
CUADRO 10
Bolivia, agosto-octubre 2003
Nivel de Cuidados Obstétricos de Emergencia según Tipo de Establecimiento
Tipo de Establecimiento
COEm Completo
COEm Completo (-1)
COEm Básico
La condición COEm Completo (-1) se cumple cuando el establecimiento realiza todas las funciones señales menos el Parto Asistido por VACUM y/o Fórceps
La condición COEm Básico (-1) se cumple cuando el establecimiento reaiza todas las funciones básicas señaladas menos el Parto Asistido por VACUM y/o Fórceps
COEm Básico (-1)
No COEm Total
TABLE 10
Level of Emergency Obstetric Care by Type of Establishment
Bolivia August-October, 2003
Type of Establish-
ment
Level I
Level II
Level III
CompleteEmOC
CompleteEmOC (-1)
Basic EmOC
Basic EmOC (-1) No EmOC
The condition Complete EmOC (-1) is met when the establishment performs all of the indicated functions except assisted delivery with vacuum and/or forceps
The condition Complete EmOC (-1) is met when the establishment performs all of the indicated basic functions except assisted delivery with vacuum and/or forceps

In conclusion ........

SRH matters not only during the reproductive years, but also as SRH matters not only during the reproductive years, but also as a concept that emphasizes a health focus centered on people’s a concept that emphasizes a health focus centered on people’s life cycle.life cycle.
Covers issues that are sensitive and important for individuals, Covers issues that are sensitive and important for individuals,
partners and communities, such as sexuality, gender partners and communities, such as sexuality, gender discrimination, and power relationships between men and discrimination, and power relationships between men and women.women.
To achieve a better state of SRH, it is crucial to protect sexual To achieve a better state of SRH, it is crucial to protect sexual
and reproductive rights, a set of norms from different and reproductive rights, a set of norms from different internationally agreed-upon human rights instruments that have internationally agreed-upon human rights instruments that have been accepted for many years.been accepted for many years.
Public choices, private decisions: Public choices, private decisions: Sexual and reproductive health and the Millennium Development GoalsSexual and reproductive health and the Millennium Development Goals
Stan Bernstein 2006Stan Bernstein 2006

““We cannot attain the Millennium Development Goals, We cannot attain the Millennium Development Goals, particularly the eradication of extreme poverty and hunger, particularly the eradication of extreme poverty and hunger, unless we decidedly tackle issues of population and reproductive unless we decidedly tackle issues of population and reproductive health; for this reason, it is essential to intensify efforts to health; for this reason, it is essential to intensify efforts to promote women’s rights and increase investments in education promote women’s rights and increase investments in education and health, including reproductive health and family planning.”and health, including reproductive health and family planning.”
Kofi Annan, Secretary General of the United NationsKofi Annan, Secretary General of the United Nations
Thank you !!!Thank you !!!
““...finally, health should not be seen as a ...finally, health should not be seen as a blessing that we can wish for, but as a human blessing that we can wish for, but as a human
right that we should fight for” right that we should fight for” ––Kofi Annan, Secretary General of the United NationsKofi Annan, Secretary General of the United Nations

















