Disclaimer: The Rapid Response Service is an information service for those involved in planning and providing health care in Canada. Rapid responses are based on a limited literature search and are not comprehensive, systematic reviews. The intent is to provide a list of sources and a summary of the best evidence on the topic that CADTH could identify using all reasonable efforts within the time allowed. Rapid responses should be considered along with other types of information and health care considerations. The information included in this response is not intended to replace professional medical advice, nor should it be construed as a recommendation for or against the use of a particular health technology. Readers are also cautioned that a lack of good quality evidence does not necessarily mean a lack of effectiveness particularly in the case of new and emerging health technologies, for which little information can be found, but which may in future prove to be effective. While CADTH has taken care in the preparation of the report to ensure that its contents are accurate, complete and up to date, CADTH does not make any guarantee to that effect. CADTH is not liable for any loss or damages resulting from use of the information in the report. Copyright: This report contains CADTH copyright material. It may be copied and used for non-commercial purposes, provided that attribution is given to CADTH. Links: This report may contain links to other information available on the websites of third parties on the Internet. CADTH does not have control over the content of such sites. Use of third party sites is governed by the owners’ own terms and conditions. TITLE: Sodium Chloride Inhalation for the Treatment of Cystic Fibrosis: A Review of the Clinical Evidence, Cost-Effectiveness and Guidelines DATE: 2 August 2012 CONTEXT AND POLICY ISSUES Cystic fibrosis (CF) is a genetic disease of the exocrine gland caused by mutations in the cystic fibrosis transmembrane conductance regulator gene expressed in several organs including the lung, the pancreas, the biliary system, and the sweat glands. 1 In 2010, about 3,849 Canadian residents were reported to have CF including 117 individuals newly diagnosed in 2010. 2 The main complaint for CF patients is the difficulty in clearing purulent secretions from their respiratory tract. Therefore, the objective of pulmonary treatments is to help clear the thick CF mucus from airways and reduce inflammation. 3 Hypertonic sodium chloride (HTS) is a mucoactive agent used to promote secretion clearance from airways. 4 HTS solutions (3% and 7%) are used in CF for patients of 6 years of age and older, to help increase their lung function and decrease the number of lung infections. It also helps to decrease thickness of the mucus in the airways of a person with CF and to produce sputum (mucus). 3 This report will review the evidence regarding the efficacy, safety, and cost-effectiveness of hypertonic sodium chloride in the treatment of patients with CF. RESEARCH QUESTIONS 1. What is the clinical evidence for the efficacy and safety of inhaled sodium chloride solutions for the treatment of cystic fibrosis in children? 2. What is the clinical evidence for the efficacy and safety of inhaled sodium chloride solutions for the treatment of cystic fibrosis in adults? 3. What is the cost-effectiveness of inhaled sodium chloride solutions for the treatment of cystic fibrosis in children?
Transcript
Disclaimer: The Rapid Response Service is an information service for those involved in planning and providing health care in Canada. Rapid responses are based on a limited literature search and are not comprehensive, systematic reviews. The intent is to provide a list of sources and a summary of the best evidence on the topic that CADTH could identify using all reasonable efforts within the time allowed. Rapid responses should be considered along with other types of information and health care considerations. The information included in this response is not intended to replace professional medical advice, nor should it be construed as a recommendation for or against the use of a particular health technology. Readers are also cautioned that a lack of good quality evidence does not necessarily mean a lack of effectiveness particularly in the case of new and emerging health technologies, for which little information can be found, but which may in future prove to be effective. While CADTH has taken care in the preparation of the report to ensure that its contents are accurate, complete and up to date, CADTH does not make any guarantee to that effect. CADTH is not liable for any loss or damages resulting from use of the information in the report. Copyright: This report contains CADTH copyright material. It may be copied and used for non-commercial purposes, provided that attribution is given to CADTH. Links: This report may contain links to other information available on the websites of third parties on the Internet. CADTH does not have control over the content of such sites. Use of third party sites is governed by the owners’ own terms and conditions.
TITLE: Sodium Chloride Inhalation for the Treatment of Cystic Fibrosis: A Review of the Clinical Evidence, Cost-Effectiveness and Guidelines
DATE: 2 August 2012 CONTEXT AND POLICY ISSUES Cystic fibrosis (CF) is a genetic disease of the exocrine gland caused by mutations in the cystic fibrosis transmembrane conductance regulator gene expressed in several organs including the lung, the pancreas, the biliary system, and the sweat glands.1 In 2010, about 3,849 Canadian residents were reported to have CF including 117 individuals newly diagnosed in 2010.2 The main complaint for CF patients is the difficulty in clearing purulent secretions from their respiratory tract. Therefore, the objective of pulmonary treatments is to help clear the thick CF mucus from airways and reduce inflammation.3 Hypertonic sodium chloride (HTS) is a mucoactive agent used to promote secretion clearance from airways.4 HTS solutions (3% and 7%) are used in CF for patients of 6 years of age and older, to help increase their lung function and decrease the number of lung infections. It also helps to decrease thickness of the mucus in the airways of a person with CF and to produce sputum (mucus).3 This report will review the evidence regarding the efficacy, safety, and cost-effectiveness of hypertonic sodium chloride in the treatment of patients with CF. RESEARCH QUESTIONS 1. What is the clinical evidence for the efficacy and safety of inhaled sodium chloride
solutions for the treatment of cystic fibrosis in children?
2. What is the clinical evidence for the efficacy and safety of inhaled sodium chloride solutions for the treatment of cystic fibrosis in adults?
3. What is the cost-effectiveness of inhaled sodium chloride solutions for the treatment of cystic fibrosis in children?
Sodium Chloride Inhalation for Cystic Fibrosis 2
4. What is the cost-effectiveness of inhaled sodium chloride solutions for the treatment of cystic fibrosis in adults?
5. What are the evidence-based guidelines for the use of inhaled sodium chloride solutions for the treatment of cystic fibrosis?
KEY MESSAGE The available evidence showed a limited clinical effectiveness of HTS; findings from the various studies were inconsistent. One study showed that under certain circumstances, HTS is less cost-effective than recombinant human DNase (rhDNase) when used among children between 6 to 18 years. METHODS Literature Search Strategy A limited literature search was conducted on key resources including PubMed, The Cochrane Library (2012, Issue 6), University of York Centre for Reviews and Dissemination (CRD) databases, Canadian and major international health technology agencies, as well as a focused Internet search. No filters were applied to limit the retrieval by study type. Where possible, retrieval was limited to the human population. The search was also limited to English language documents published between January 1, 2001 and July 5, 2012. Selection Criteria and Methods One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed for relevance. Full texts of any relevant titles/abstracts were retrieved, and assessed. The final article selection was based on the inclusion criteria presented in Table 1. Table 1: Selection Criteria Population
Adults and children with cystic fibrosis
Intervention
Hypertonic sodium chloride solutions (3% and 7% solutions or any other available dose)
Comparator
Placebo Inhaled dornase alpha (Pulmozyme) Inhaled dornase alpha plus hypertonic solution Inhaled N-acetylcysteine Hypertonic sodium chloride plus other agents
Health technology assessment, systematic reviews, meta-analysis, randomized controlled trials (RCTs), economic studies and guidelines
Exclusion Criteria The following publications were excluded from the review:
• Duplicate reports, unless if they reported different outcomes from the same study.
• Study designs other than those defined in Table 1.
• Systematic reviews that did not compare efficacy and/ or safety of HTS with any comparator.
• Primary studies which were included in one of the systematic review quoted in the current review.
• Guidelines with no specific recommendations on the use of HTS. Critical Appraisal of Individual Studies
Critical appraisal of the included studies was based on study design. The following tools were used to guide the evaluation of the methodological quality of the included studies:
• The Appraisal of Guidelines Research and Evaluation (AGREE) instrument5 was used to evaluate the included guideline.
• The Assessment of Multiple Systematic Reviews” (AMSTAR) checklist6 was used in the assessment of the included systematic review.
• The SIGN50 checklist for the controlled studies7 was adopted for the evaluation of the included randomized controlled trials.
• The guidelines for appraisal of economic studies by Drummond et al8 were followed in the assessment of the included cost-effectiveness study.
For the methodological quality of the included studies a numeric score was not calculated. Instead, the strengths and limitations of the study were described. SUMMARY OF EVIDENCE Quantity of Research Available A total of 132 potential citations were identified by the bibliographic database search, with 108 citations being excluded during the title and abstract screening based on irrelevance to the questions of interest. The full text documents of the remaining 24 citations were retrieved. Three additional citations were identified by the grey literature search. Of the 27 articles, 20 did not meet the inclusion criteria and were excluded, leaving seven articles to be included in the review.9-15 A PRISMA diagram demonstrating the study selection process is presented in APPENDIX 1. Summary of Study Characteristics Seven articles that addressed at least one of the research questions were included in this review. These included one Cochrane systematic review,10 four randomized-controlled trials
Sodium Chloride Inhalation for Cystic Fibrosis 4
(RCT),11-14 one cost-effectiveness study,15 and one clinical guidelines documents.9 Details regarding primary studies characteristics are tabulated in Appendix 2. Wark et al. published a Cochrane systematic review that investigated the effects of HTS on CF patients compared to placebo and/ or other treatments that enhance mucociliary clearance.10 The systematic review included controlled trials, either randomized or quasi-randomized, with no restrictions on patients’ age, diagnosis method or disease severity. HTS was defined as saline of concentration greater than or equal to 3%. The review included 12 RCTs, and the age range was 6 years to 46 years. The analysis did not differentiate between the 3% and 7% concentrations, and results of both concentrations were pooled together. Outcomes evaluated in this review included lung functions endpoints, sputum clearance measures, quality of life and exacerbation rates. Rosenfeld et al.11 and Donaldson et al.14 were randomized controlled trials of parallel groups design, while Laube et al. 12 and Amin et al.13 had a cross-over design. Rosenfeld et al.11 and Amin et al.13 compared the effects of 4 ml 7% HTS with 4 ml 0.9% isotonic saline used twice daily for 48 weeks and four weeks respectively. Laube et al.12 compared the acute use (one time) of 5 ml 7% HTS with 5 ml 0.9% isotonic saline. On the other hand, Donaldson et al.14 compared the combination of amiloride and 5 ml 7% HTS with HTS plus placebo when used four times/ day for two weeks. The age for inclusion differed between trials, it was < 6 years in Rosenfeld et al.11 trial (mean age 2.3 years) and between 7 to 14 years and 6 to 18 years in trials by Laube et al.12 and Amin et al. respectively;13 the mean age in both trials was 10.5 years. Donaldson et al.14 included CF patients equal to or older than 14 years; the mean age was 26 years. The inclusion value for the forced expiratory volume at one second (percentage of predicted value) was 90%, 80%, and 50% in Laube et al.12, Amin et al.13 and Donaldson et al.14, respectively. Primary outcomes in the included trials were rate of pulmonary exacerbations,11 clearance rate measured by mucociliary clearance,12
and lung clearance index,13 and both percentage change in forced expiratory volume and forced vital capacity.14 Suri et al. conducted a comparative cost-effectiveness analysis between daily rhDNase (2.5 mg), alternate-day rhDNase (2.5 mg) and HTS (twice-daily 5 ml 7%), over a 12-week period, for children with CF. The analysis was based on a randomized open-label cross-over trial conducted on patients with a mean age of 12.6 years.16 The trial was included in the systematic review by Wark et al.10 Treatment effectiveness was based on the difference of the mean percentage change in FEV1, and the total cost was based on the cost of intervention and non-intervention drugs, hospital care and community care. Outcomes included the incremental cost-effectiveness ratio (ICER), cost-effectiveness acceptability curve (CEAC), and the net benefit statistic. The Cystic Fibrosis Foundation in Maryland – USA supported the development of clinical guidance for the prescription of pulmonary therapies used for CF patients.9 A multi-disciplinary committee reviewed and evaluated the evidence for each therapy based on systematic reviews of the literature. The committee gave a graded recommendation for each one of the reviewed therapies; the grades were based on the net benefit of the therapy and the strength of the overall evidence of its effectiveness. A descriptive summary of these grades is provided in Table 2 (Appendix 2). Recommendations were given for HTS, aerosolized antibiotics (tobramycin and colistin), recombinant human DNase, anti-inflammatory agents (corticosteroids, oral non-steroidal anti-inflammatory drugs, leukotriene modifiers, and cromolyn), macrolide antibiotics, anti-staphylococcal antibiotics, bronchodilators (β2-Adrenergic receptor agonists and inhaled anticholinergic agents), and N-acetylcysteine.
Sodium Chloride Inhalation for Cystic Fibrosis 5
Summary of Critical Appraisal The strengths and limitations of the included studies are summarized here and details are provided in Appendix 4. The Cochrane systematic review by Wark et al.10 was conducted according to a priori protocol, and used a robust method for literature search and selection. The analysis of the included studies in the review was limited by the fact that possible differences in the intervention, mainly the concentration and daily regimen of HTS use, were not taken into consideration. Furthermore, the potential effects of different trial designs, parallel versus cross-over trials, were not considered in the analysis of the primary studies results. The four primary trials included in the review had a randomized allocation of the trials’ interventions. However, Donaldson et al.14 did not provide information about the randomization method and concealment. As well, patients and investigators were blinded to the allocated intervention in the four trials; however, the taste of HTS is easily recognized and if it is not masked treatment can be easily identified.. Amin et al.13 did not attempt masking the taste of HTS. Three trials reported that the size of trial’s population was calculated based on power estimation.11,12,14 For sample size calculation, an estimation of the effect size should be used; this estimation is usually based on previous experience with the intervention, or if such data is not available, results of epidemiological studies or a consensus of clinical experts can be used. Laube et al.12 used the results of a previous trial by Donaldson et al.14 to estimate Laube’s trial sample size. However, the intervention evaluated by Donalson et al.14 was HTS combined with amiloride versus HTS combined with placebo, while Laube et al.12 evaluated HTS versus placebo. In the four trials, the included patients were CF patients who had their diagnosis confirmed either by genetic testing or sweat test. Rosenfeld et al.11 excluded infants who could not tolerate HTS. Although this restrictive population is likely to increase compliance and decrease the rate of drop out, the findings of this trial may not be generalizable to all CF patients. In their cost-effectiveness analysis, Suri et al.15 used estimates for effectiveness and cost as provided in a clinical trial rather than using assumptions and simulating methods to obtain these estimates. However, the clinical trial had some limitations that might render its results questionable. First, the trial was an open-label allocation of intervention; this fact might introduce a bias in the assessment of the outcomes, and the use and adherence to the interventions. In fact, the cost analysis assumed that the utilisation of each of the treatments was that prescribed by the study protocol. However, this assumption would only be valid with a high treatment adherence. Adherence was determined from patients’ dairies and the returned treatment packs. Some discrepancies were observed; the diaries showed a consistent high adherence, while the returned packs showed signs of lower adherence in both the daily rhDNase and the alternate-day rhDNase groups. The clinical guidelines by Flume et al.9 were developed according to a predefined protocol of systematic review of the literature and evaluation of evidence, and the recommendations were clearly specified and reported in the final document. However, the guidelines did not specify if CF patients’ preferences were sought and taken into consideration. Furthermore, the guidelines did not report on the potential organizational and cost barriers in applying the recommendations.
Sodium Chloride Inhalation for Cystic Fibrosis 6
Summary of Findings A summary of study findings are provided below and details and authors’ conclusions are provided in Appendix 5. What is the clinical evidence for the efficacy and safety of inhaled sodium chloride solutions for the treatment of cystic fibrosis in children? Rosenfeld et al.11 reported statistically not significant difference between HTS and isotonic saline in the pulmonary exacerbation rate and the total number of treatment day for pulmonary exacerbations. With regard to pulmonary functions, a statistically significant difference between HTS and placebo was reported for the forced expiratory volume at 0.5 second favouring HTS; the mean difference was 38 mL (95% CI; 1, 76). However, the differences were not statistically significant for the forced expiratory flow and the functional residual capacity. The incidence of adverse events was similar for the HTS and placebo groups. Laube et.12 evaluated the mucociliary clearance at 60 and 90 minutes. The differences between HTS and placebo were statistically not significant. On the other hand, Amine et al.13 reported a statistically significant difference between HTS and placebo in lung clearance index. However, the differences were not statistically significant for the forced expiratory flow and the forced expiratory volume.13 What is the clinical evidence for the efficacy and safety of inhaled sodium chloride solutions for the treatment of cystic fibrosis in adults? Donaldson et al.14 included CF patients older than 14 years, and the mean age was 26 years. The comparison between HTS used with amiloride and HTS used with placebo provide statistically not significant differences in the forced expiratory volume, forced expiratory flow, and functional expiratory capacity. The difference was statistically significant for the mucociliary clearance rate at 60 minutes, favouring HTS used with placebo. However, the difference in mucociliary clearance rate at 24 hours was not statistically significant. In their systematic review, Wark et al.10 reported the age of patients for seven RCTs; age information was not available for five RCTs. Based on the age range of the seven RCTs, three trials included adult patients, two included children, and two included children and adults. The analysis did not differentiate between trials that included children or adults; therefore, results from this trial will be used to answer efficacy and safety question for both children and adults. Following are the results for the different comparisons in the review: Comparisons between HTS (3% to 7%) versus placebo Results for two primary trials showed statistically significant differences in percentage forced expiratory volume and percentage forced vital capacity for HTS compared with isotonic saline when evaluated at two to four weeks after treatment; the respective mean differences were 4.15% (1.14, 7.16) and 2.75% (0.00, 5.49). However, these differences were not statistically significant when evaluated at 36 and 48 months. On the other hand, HTS reduced the number of visits requiring antibiotics to treat pulmonary exacerbation; the mean difference was -0.46 (-0.82, -0.10). Hospital admissions due to pulmonary exacerbation were not statistically significantly different.
Sodium Chloride Inhalation for Cystic Fibrosis 7
Comparisons between HTS (3% to 7%) versus rhDNase In one primary trial, daily rhDNase improved the percentage change in forced expiratory volume more than HTS; however, the difference was statistically significant when evaluated at three months but not at three weeks. Nevertheless, the difference in forced vital capacity was not statistically significant when evaluated at three months. Comparisons between HTS (3% to 7%) versus sodium-2- mercaptoethane sulfate Results of one primary trial showed that the difference in forced vital capacity was not statistically significant when evaluated at eight weeks of treatment. What is the cost-effectiveness of inhaled sodium chloride solutions for the treatment of cystic fibrosis in children? The difference in mean net benefit between the daily rhDNase versus HTS showed a statistically significant net benefit favouring the daily rhDNase when using a ceiling rate of £400 per 1% gain in FEV1; however, when the ceiling rate was changed to £200 or £100 per 1% gain in FEV1 the difference was no longer statistically significant. Comparison between the alternate-day rhDNase with HTS provided statistically not significant differences for the three ceiling rates. The incremental cost-effectiveness ratios (ICER) per 1% gain in FEV1 were £100 and £89 for daily rhDNase versus HTS and alternative day rhDNase versus HTS respectively. The bootsrap samples plotted on the cost-effectiveness plane showed some negative ICER values that rendered ordering of the ratios impossible; therefore, the ICER was not used in the evaluation of the cost-effectiveness. What is the cost-effectiveness of inhaled sodium chloride solutions for the treatment of cystic fibrosis in adults? There were no studies identified that evaluated the cost-effectiveness of inhaled sodium chloride solutions for the treatment of cystic fibrosis in adults. What are the evidence-based guidelines for the use of inhaled sodium chloride solutions for the treatment of cystic fibrosis? The included guidelines evaluated the evidence for the use of hypertonic saline in CF patients.9 Based on the findings from four trials and one Cochrane review; three of the primary trials were included in the Cochrane review which was published by Wark et al.17 The Cochrane review was updated by Wark et al.10 and is included in this review.The committee recommended the chronic use of inhaled hypertonic saline in CF patient, 6 years of age and older, in order to improve lung functions and to reduce exacerbations. The committee provided grade B for their recommendation; the recommendation was justified by a fair level of evidence showing a moderate net benefit. Limitations The current review did not evaluate the effect of HTS delivery method. It is believed that the delivery method may affect the treatment time and adherence rate.18 Another limitation of this review is that the included primary studies (RCTs) evaluated the higher dose of HTS (7%); furthermore, the included systematic review pooled the results of both doses, 3% and 7%.
Sodium Chloride Inhalation for Cystic Fibrosis 8
Therefore, there was no information to assess the efficacy, safety, or cost-effectiveness of 3% HTS. The cost-effectiveness study included in this review was conducted in the United Kingdom, and the costs estimates and medical procedures used may not reflect the Canadian settings. CONCLUSIONS AND IMPLICATIONS FOR DECISION OR POLICY MAKING Treatment with HTS (7%) showed limited improvement of pulmonary functions among cystic fibrosis patients. However, this improvement was not consistent across trials, and was not consistently statistically significantly different from the isotonic saline. When compared to rhDNase, HTS showed lower improvement; although the differences were not consistently statistically significant. One study suggested that HTS was less cost-effective than the daily rhDNase or the alternate day rhDNase when used among children between 6 to 18 years. One clinical guidelines recommended the chronic use of HTS in CF patients, 6 years of age and older, in order to improve lung functions and reduce pulmonary exacerbations. A possible explanation for the difference in the conclusions of the guidelines and this current review is that this review has a more updated literature review than the guidelines. PREPARED BY: Canadian Agency for Drugs and Technologies in Health Tel: 1-866-898-8439 www.cadth.ca
Sodium Chloride Inhalation for Cystic Fibrosis 9
REFERENCES
1. Rosenstein BJ. Cystic Fibrosis. 2008 [cited 2012 Aug 1]. In: The Merck Manual [Internet]. Whitehouse Station (N.J.): Merck Sharp & Dohme Corp. Available from: http://www.merckmanuals.com/ Subscription required.
2. Canadian cystic fibrosis patient data registry report 2010 [Internet]. Toronto: Cystic Fibrosis Canada; 2012 Jan. [cited 2012 Jul 9]. Available from: http://www.cysticfibrosis.ca/assets/files/pdf/CPDR_ReportE.pdf
3. Cystic Fibrosis Foundation [Internet]. Bethesda (MD): Cystic Fibrosis Foundation. Therapies for cystic fibrosis; 2012 Feb 14 [cited 2012 Jul 9]. Available from: http://www.cff.org/treatments/Therapies/
4. Rubin BK. Mucolytics, expectorants, and mucokinetic medications. Respir Care [Internet]. 2007 Jul [cited 2012 Jul 9];52(7):859-65. Available from: http://www.rcjournal.com/contents/07.07/07.07.0859.pdf
5. The AGREE Collaboration. Appraisal of guidelines for research and evaluation (AGREE) instrument [Internet]. London: The AGREE Research Trust; 2001 Sep. [cited 2012 Jul 30]. Available from: http://www.agreetrust.org/?o=1085
6. Shea BJ, Grimshaw JM, Wells GA, Boers M, Andersson N, Hamel C, et al. Development of AMSTAR: a measurement tool to assess the methodological quality of systematic reviews. BMC Med Res Methodol [Internet]. 2007 [cited 2012 Jul 30];7:10. Available from: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1810543/pdf/1471-2288-7-10.pdf
8. Drummond MF, Jefferson TO. Guidelines for authors and peer reviewers of economic submissions to the BMJ. The BMJ Economic Evaluation Working Party. BMJ [Internet]. 1996 Aug 3 [cited 2012 Aug 1];313(7052):275-83. Available from: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2351717
9. Flume PA, O'Sullivan BP, Robinson KA, Goss CH, Mogayzel PJ, Jr., Willey-Courand DB, et al. Cystic fibrosis pulmonary guidelines: chronic medications for maintenance of lung health. Am J Respir Crit Care Med. 2007 Nov 15;176(10):957-69.
10. Wark PA, McDonald V. Nebulised hypertonic saline for cystic fibrosis. Cochrane Database Syst Rev. 2010;(6):CD001506.
11. Rosenfeld M, Ratjen F, Brumback L, Daniel S, Rowbotham R, McNamara S, et al. Inhaled hypertonic saline in infants and children younger than 6 years with cystic fibrosis: the ISIS randomized controlled trial. JAMA. 2012 Jun 6;307(21):2269-77.
12. Laube BL, Sharpless G, Carson KA, Kelly A, Mogayzel PJ, Jr. Acute inhalation of hypertonic saline does not improve mucociliary clearance in all children with cystic fibrosis. BMC Pulm Med [Internet]. 2011 [cited 2012 Jul 6];11:45. Available from: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3180295/pdf/1471-2466-11-45.pdf
Sodium Chloride Inhalation for Cystic Fibrosis 10
13. Amin R, Subbarao P, Jabar A, Balkovec S, Jensen R, Kerrigan S, et al. Hypertonic saline improves the LCI in paediatric patients with CF with normal lung function. Thorax. 2010 May;65(5):379-83.
14. Donaldson SH, Bennett WD, Zeman KL, Knowles MR, Tarran R, Boucher RC. Mucus clearance and lung function in cystic fibrosis with hypertonic saline. N Engl J Med [Internet]. 2006 Jan 19 [cited 2012 Jul 6];354(3):241-50. Available from: http://www.nejm.org/doi/pdf/10.1056/NEJMoa043891
15. Suri R, Wallis C, Bush A, Thompson S, Normand C, Flather M, et al. A comparative study of hypertonic saline, daily and alternate-day rhDNase in children with cystic fibrosis. Health Technol Assess. 2002;6(34):iii, 1-iii,60.
16. Suri R, Metcalfe C, Lees B, Grieve R, Flather M, Normand C, et al. Comparison of hypertonic saline and alternate-day or daily recombinant human deoxyribonuclease in children with cystic fibrosis: a randomised trial. Lancet. 2001 Oct 20;358(9290):1316-21.
17. Wark PA, McDonald V, Jones AP. Nebulised hypertonic saline for cystic fibrosis. Cochrane Database Syst Rev. 2005;(2):CD001506.
18. McCormack P, McNamara PS, Southern KW. A randomised controlled trial of breathing modes for adaptive aerosol delivery in children with cystic fibrosis. J Cyst Fibros. 2011 Sep;10(5):343-9.
Sodium Chloride Inhalation for Cystic Fibrosis 11
Appendix 1: Selection of Included Studies
108 citations excluded
24 potentially relevant articles retrieved for scrutiny (full text, if
available)
3 potentially relevant reports retrieved from
the grey literature
27 potentially relevant reports
20 reports excluded:
• Irrelevant intervention: 5
• Study design: 6
• Duplicates: 4
• Included in the systematic review: 3
• Population (not CF patients): 1
• Full text not ready for publication: 1
7 articles included in review reporting One clinical guidelines article
One Cochrane systematic review Four randomized-controlled trials
One cost-effectiveness study
132 citations identified from electronic literature search and
screened
Sodium Chloride Inhalation for Cystic Fibrosis 12
Appendix 2: Characteristics of the Included Publications
Table 2. Characteristics of the Included Clinical Guidelines
Guidelines Objectives Guideline Audience Methods of Development Level of Recommendation
Flume et al. 20079 – The Cystic Fibrosis Foundation (CFF) - USA
To examine the clinical evidence for each pulmonary CF therapy and to provide guidance for the prescription of these therapies.
• Physicians treating patients with CF
• Reviewing the available evidence o A 15-member committee
(Pulmonary Therapies Committee) was formed presenting internal medicine, pediatrics, nursing, respiratory therapy, systematic review procedures and the CFF
o conducted systematic reviews of the literature
o For each therapy, the body of evidence was evaluated by the committee and recommendation were then issued
o The committee presented the recommendations in a conference and the solicited public feedback for one month after presentation.
• Five levels of recommendations o Level A: “the committee recommends than clinicians routinely
provide [the service] to eligible patients. (The committee found good evidence that [the service] improves important health outcomes and concludes that benefits substantially outweigh harms.)”
o Level B: “the committee recommends that clinicians routinely provide [the service] to eligible patients. (The committee found at least fair evidence that [the service] improves important health outcomes and concludes that benefits outweigh harms.)”
o Level C: “the committee makes no recommendation for or against routine provision of [the service]. (The committee found at least fair evidence that [the service] can improve health outcomes but concludes that the balance of the benefits and harms is too close to justify a general recommendation.)”
o Level D: “the committee recommends against routinely providing [the service] to patients. (The committee found at least fair evidence that [the service] is ineffective or that harms outweigh benefits.)”
o Level I: “the committee concludes that the evidence is insufficient to recommend for or against routinely providing [the service]. (Evidence that [the service] is effective is lacking, of poor quality, or conflicting, and the balance of benefits and harms cannot be determined.)”
CF= cystic fibrosis
Sodium Chloride Inhalation for Cystic Fibrosis 13
Table 3. Characteristics of the Included Systematic Review
Review Objectives Types of Studies and Types of Participants Interventions and Comparators Outcomes
Wark et al. 201010
– Australia
to investigate the effects of treatment with nebulised hypertonic saline on people with CF compared to placebo and or other treatments that enhance mucociliary clearance.
• Type of Studies o 12 Randomized Controlled clinical trials.
• Types of Participants o Patients of all ages and of both sexes with
CF diagnosed clinically or by sweat and genetic testing, including all degrees of disease severity.
• Intervention: o Nebulized hypertonic saline,
defined as a concentration of saline greater than or equal to 3%
• Comparator: o Placebo (isotonic saline) o Usual treatments (e.g.,
physiotherapy) o Other mucus mobilising
treatments (e.g., rhDNase and mannitol)
• Limited to nebulisation delivered via a nebuliser using mask or mouthpiece.
• Treatment given as a minimum of a single dose
• Primary outcomes: o Lung functions
� FEV1 � FVC � RV:TLC
o Mortality • Secondary outcomes o Sputum clearance o Exercise capacity o Quality of life o Exacerbation rate o Medication delivery time o Cost of treatment o Adherence to treatment o Adverse effects
CF=cystic fibrosis; FEV1= forced expiratory volume in 1 second; FVC= forced vital capacity; FRC= functional residual capacity; rhDNase= recombinant human DNase; RV:TLC= ratio of residual volume to total lung capacity
Sodium Chloride Inhalation for Cystic Fibrosis 14
Table 4. Characteristics of the Included Randomized-Controlled Trials
Study Objectives & Design
Inclusion Criteria, Sample Size, and Patients Characteristics
Interventions, Comparators, and Trial Conducts
Outcomes
Rosenfeld et al. 201211
- USA
To determine if HTS reduces pulmonary exacerbations in CF patients <6years. RCT, DB and placebo-controlled
• Inclusion criteria o Confirmed CF; o Age < 6 years; o can tolerate the HTS
• N=321 infants
• Mean age 2.3 years (about 60% < 30 months); 55% males; sweat chloride 95 mEq/L
• Genotype: o F508del homozygous 55% o F508del heterozygous 22% o Other 23%
• Chronic medications o rhDNase 40% o Albuterol/ levalbuterol 74%
• Intervention: (N=158) o 4 ml of 7% hypertonic saline
• Comparator: (N=163) o 4 ml of 0.9% isotonic saline
• Twice daily for 48 weeks of treatment
• 1:1 randomization, stratified by age (4 to 29 months and 30 to 60 months) and site
• Only patients who tolerated HTS at screening visit were randomized
• patients had albuterol or levalbuterol pre-treatment prior to each dose
• All standard therapies for CF care and for treatment of incident illnesses were allowed with the exception of HTS.
• The rate of pulmonary exacerbations (Primary outcome)
To show that acute inhalation of HTS improves the MCC in children with CF. Randomized placebo- controlled, cross-over, DB trial
• Inclusion criteria o Confirmed CF; either by seat chloride> 60
meq/L, or presence of two CFTR mutations o Age 7-14 years o FEV1 ≥90% of predicted values
• N=12 children, mean age 10.5 • Genotype: o F508del homozygous 75% o F508del heterozygous 25%
• Routine medications (used by >50%) o rhDNase 92% o Salmeterol/ fluticasone 58%
• Intervention: (N=12) o 5 ml 7% hypertonic saline
• Comparator: (N=12) o 5 ml of 0.9% isotonic saline
• Patients had 2 puffs of albuterol prior to administration of the trial treatments
• Each patient had two treatment visits; in one visit they had the intervention and the placebo in the other visit. The visits were separated by ≥ one week
• Patients had to stop bronchodilators, rhDNase and airway clearance therapy 12 hours before each visit.
• MCC (primary outcome) expressed as percent MCC at 60 min (MCC60) and at 90 min (MCC90) o MCC was measured through
radioactivity analysis of lung images after the inhalation of a radio-aerosol.
Table 4. Characteristics of the Included Randomized-Controlled Trials
Study Objectives & Design
Inclusion Criteria, Sample Size, and Patients Characteristics
Interventions, Comparators, and Trial Conducts
Outcomes
Amin et al. 200913
Canada
To study the ability of the lung clearance index (LCI) to detect a treatment response to HTS in pediatric patients with CF with normal spirometry. Randomized placebo- controlled, cross-over, DB trial
• Inclusion criteria o Confirmed CF; o Age 6-18 years o FEV1 ≥80% of predicted values o Oxyhaemoglobin saturation of ≥90%
• N= 20 children, mean age= 10.5 years
• Genotype: o F508del homozygous 42% o F508del heterozygous 21%
• Intervention: (N=20) o 4 ml 7% hypertonic saline
• Comparator: (N=20) o 4 ml of 0.9% isotonic saline
• Twice daily for 4 weeks (each treatment)
• This was 12-week trial; two 4-week treatment periods separated by a 4-week washout.
• Patients had 2 puffs of salbutamol prior administration of the trial treatments
• Primary outcome: o LCI
• Secondary outcomes o FVC % predicted o FEV1 o FEF25-75 o CFQ-R
Donaldson et al. 200614
USA
To test if the pretreatment with amiloride would extend the duration of HTS; induce an accelerated clearance and improve lung functions in CF patients. RCT Placebo taste was masked but the double blinding of the trial intervention could not be verified form the published article
• Inclusion criteria o Confirmed CF; o Age ≥ 14 years o FEV1 ≥50% of predicted value after
bronchodilation
• N=24 patients, mean age 26 years • Genotype: o F508del homozygous 54%
• Routine medications o rhDNase 33% o Long-term macrolides 25% o Inhaled steroids 50%
• Intervention: (N=12) o Amiloride (1 mg/ ml) followed by o 5 ml 7% hypertonic saline
• Comparator: (N=12) o Placebo (0.25 mg/ ml of quinine
sulfate) followed by o 5 ml 7% hypertonic saline
• Treatments were used four times/ day
• Patients had albuterol 30 to 60 minute prior administration of the trial treatments
• 1:1 randomization,
• This was 4-week trial; two weeks of treatment preceded by two weeks run-in period
• Primary outcomes: o Percentage change in FEV1 o Percentage change in FVC
• Secondary outcomes o Mucus clearance o FEF25-75 o RV:TLC o CFQ
CF=cystic fibrosis; CFQ= cystic fibrosis questionnaire (score range from 0 to 100 – higher scores reflecting better perceived health status); CFQ-R= cystic fibrosis questionnaire-revised; DB= double blind; FEF75= forced expiratory flow at 75% of vital capacity; FEF25-75= mid-maximal forced expiratory flow; FRC= functional residual capacity; FEV1= forced expiratory volume in 1 second; FVC= forced vital capacity; HTS= hypertonic saline; LCI= lung clearance index; RCT= randomized-controlled trial; rhDNase= recombinant human deoxyribonuclease; RV:TLC= ratio of residual volume to total lung capacity;
Sodium Chloride Inhalation for Cystic Fibrosis 16
Table 5. Characteristics of the Included Economic Evaluation Study
Review Objectives & Design
Data collection/ Assumptions Interventions Outcomes
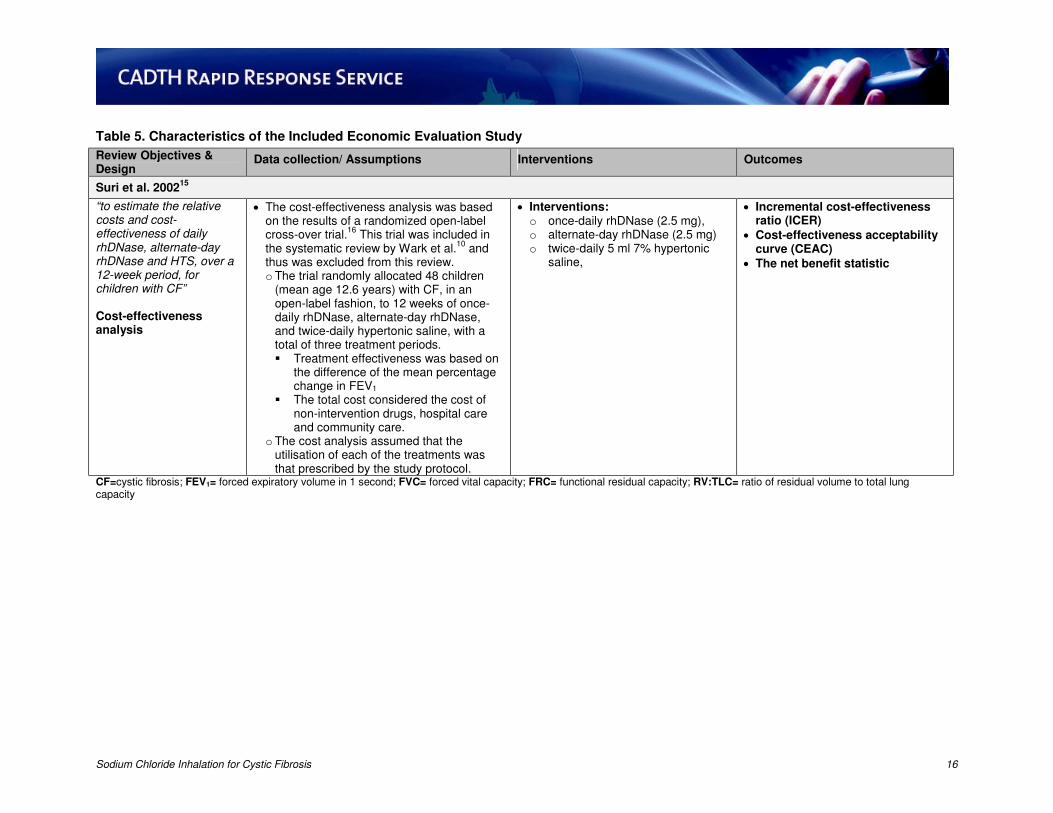
Suri et al. 200215
“to estimate the relative costs and cost-effectiveness of daily rhDNase, alternate-day rhDNase and HTS, over a 12-week period, for children with CF” Cost-effectiveness analysis
• The cost-effectiveness analysis was based on the results of a randomized open-label cross-over trial.
16 This trial was included in
the systematic review by Wark et al.10
and thus was excluded from this review. o The trial randomly allocated 48 children
(mean age 12.6 years) with CF, in an open-label fashion, to 12 weeks of once-daily rhDNase, alternate-day rhDNase, and twice-daily hypertonic saline, with a total of three treatment periods. � Treatment effectiveness was based on
the difference of the mean percentage change in FEV1
� The total cost considered the cost of non-intervention drugs, hospital care and community care.
o The cost analysis assumed that the utilisation of each of the treatments was that prescribed by the study protocol.
• Interventions: o once-daily rhDNase (2.5 mg), o alternate-day rhDNase (2.5 mg) o twice-daily 5 ml 7% hypertonic
saline,
• Incremental cost-effectiveness ratio (ICER)
• Cost-effectiveness acceptability curve (CEAC)
• The net benefit statistic
CF=cystic fibrosis; FEV1= forced expiratory volume in 1 second; FVC= forced vital capacity; FRC= functional residual capacity; RV:TLC= ratio of residual volume to total lung capacity
Sodium Chloride Inhalation for Cystic Fibrosis 17
Appendix 4: Critical Appraisal of Included Publications Critical Appraisal Summary of the included the Publications
Strengths Limitations
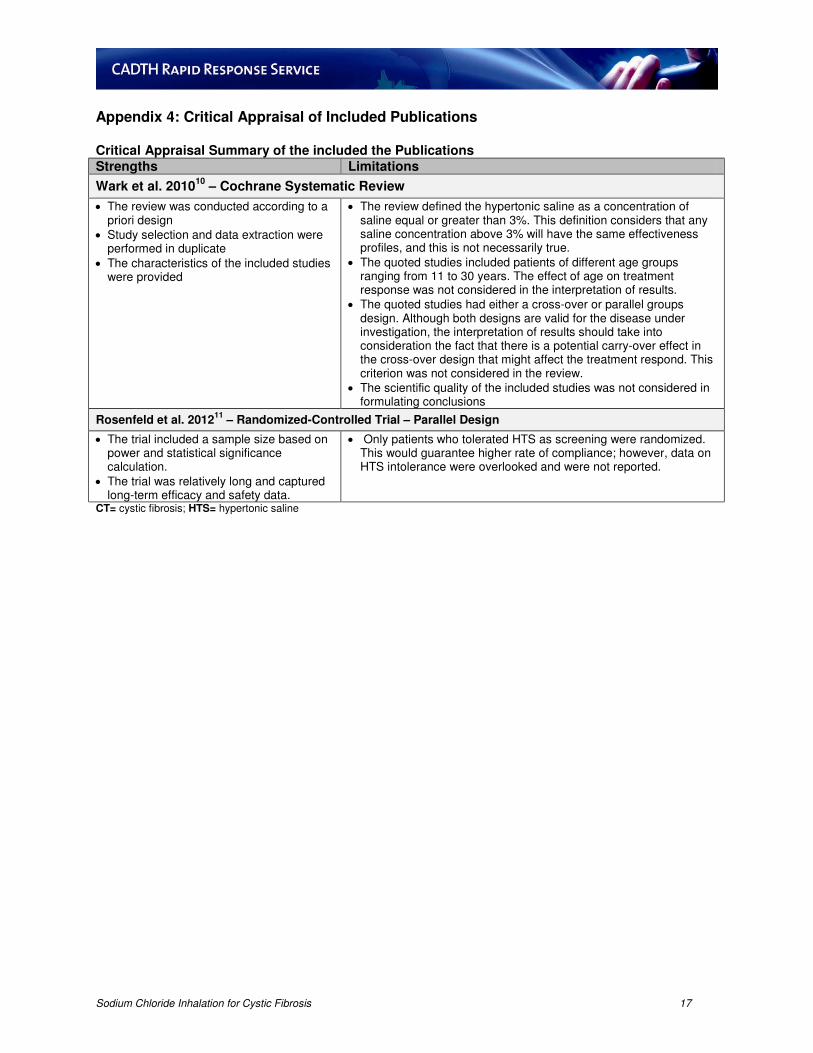
Wark et al. 201010
– Cochrane Systematic Review
• The review was conducted according to a priori design
• Study selection and data extraction were performed in duplicate
• The characteristics of the included studies were provided
• The review defined the hypertonic saline as a concentration of saline equal or greater than 3%. This definition considers that any saline concentration above 3% will have the same effectiveness profiles, and this is not necessarily true.
• The quoted studies included patients of different age groups ranging from 11 to 30 years. The effect of age on treatment response was not considered in the interpretation of results.
• The quoted studies had either a cross-over or parallel groups design. Although both designs are valid for the disease under investigation, the interpretation of results should take into consideration the fact that there is a potential carry-over effect in the cross-over design that might affect the treatment respond. This criterion was not considered in the review.
• The scientific quality of the included studies was not considered in formulating conclusions
Rosenfeld et al. 201211
– Randomized-Controlled Trial – Parallel Design
• The trial included a sample size based on power and statistical significance calculation.
• The trial was relatively long and captured long-term efficacy and safety data.
• Only patients who tolerated HTS as screening were randomized. This would guarantee higher rate of compliance; however, data on HTS intolerance were overlooked and were not reported.
CT= cystic fibrosis; HTS= hypertonic saline
Sodium Chloride Inhalation for Cystic Fibrosis 18
Critical Appraisal Summary of the included the Publications
Strengths Limitations
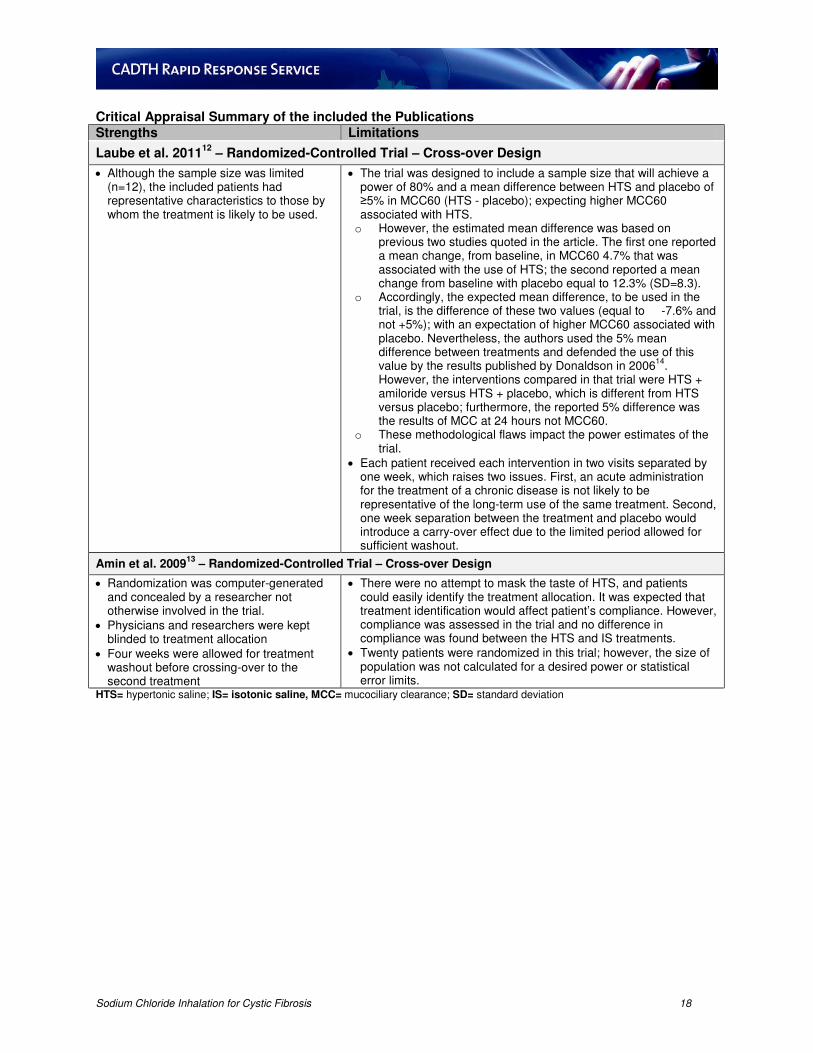
Laube et al. 201112
– Randomized-Controlled Trial – Cross-over Design
• Although the sample size was limited (n=12), the included patients had representative characteristics to those by whom the treatment is likely to be used.
• The trial was designed to include a sample size that will achieve a power of 80% and a mean difference between HTS and placebo of ≥5% in MCC60 (HTS - placebo); expecting higher MCC60 associated with HTS. o However, the estimated mean difference was based on
previous two studies quoted in the article. The first one reported a mean change, from baseline, in MCC60 4.7% that was associated with the use of HTS; the second reported a mean change from baseline with placebo equal to 12.3% (SD=8.3).
o Accordingly, the expected mean difference, to be used in the trial, is the difference of these two values (equal to -7.6% and not +5%); with an expectation of higher MCC60 associated with placebo. Nevertheless, the authors used the 5% mean difference between treatments and defended the use of this value by the results published by Donaldson in 2006
14.
However, the interventions compared in that trial were HTS + amiloride versus HTS + placebo, which is different from HTS versus placebo; furthermore, the reported 5% difference was the results of MCC at 24 hours not MCC60.
o These methodological flaws impact the power estimates of the trial.
• Each patient received each intervention in two visits separated by one week, which raises two issues. First, an acute administration for the treatment of a chronic disease is not likely to be representative of the long-term use of the same treatment. Second, one week separation between the treatment and placebo would introduce a carry-over effect due to the limited period allowed for sufficient washout.
Amin et al. 200913
– Randomized-Controlled Trial – Cross-over Design
• Randomization was computer-generated and concealed by a researcher not otherwise involved in the trial.
• Physicians and researchers were kept blinded to treatment allocation
• Four weeks were allowed for treatment washout before crossing-over to the second treatment
• There were no attempt to mask the taste of HTS, and patients could easily identify the treatment allocation. It was expected that treatment identification would affect patient’s compliance. However, compliance was assessed in the trial and no difference in compliance was found between the HTS and IS treatments.
• Twenty patients were randomized in this trial; however, the size of population was not calculated for a desired power or statistical error limits.
Critical Appraisal Summary of the included the Publications
Strengths Limitations
Donaldson et al. 200614
– Randomized controlled trial – Parallel Design
• Although the absolute value of the desired difference was not reported, the sample size was based on the ability to detect a treatment effect equal to 1 standard deviation of the FEV1, and to produce a power of 80% with the use of a two-sided α (0.05).
• This was a randomised trial; however, randomization method and concealment were not described in the article
Suri et al. 200215
– Cost-effectiveness analysis
• The analysis was based on the results of a clinical trial conducted for the specific indication and population under investigation.
• Cost analysis assumed that the utilisation of each of the treatments was that prescribed by the study protocol. However, this assumption would only be valid with a high treatment adherence. Adherence was determined by patients’ dairies and the returned treatment packs. Some discrepancies were observed; the diaries showed a consistent high adherence, while the returned packs showed signs of lower adherence in both the daily rhDNase and the alternate-day rhDNase groups.
• In the trial on which the analysis was based, the following observations were noticed: o Allocation of trial interventions was open-labeled for both
patients and investigators because of the difficulty of masking the taste of both HTS and rhDNase according to the authors.
o The length of wash-out periods between the different treatments was not the same for all patients, and it varied from 2 to 4 weeks.
Flume et al. 20109 – Guidelines
• The guideline had a definite scope and purpose with specific objectives and population on whom the guideline was meant to be applied
• The development process followed a predefined protocol of systematic review of the literature and evaluation of evidence
• Recommendations were clearly specified and reported
• Although the guideline was developed in collaboration between different stakeholders, it was not reported if CF patients’ preferences were sought and taken into consideration.
• The guideline did not report on potential organizational and cost barriers in applying the recommendations.
FEV1= forced expiratory volume at one second; HTS= hypertonic saline; rhDNase= recombinant humane DNase
Sodium Chloride Inhalation for Cystic Fibrosis 20
Appendix 5: Main Study Findings and Authors’ Conclusions
Table 6. Summary of Findings and Authors’ Conclusions of the Included Systematic Review
Main Study Findings Authors’ Conclusions
Wark et al. 201010
– Systematic review
Outcome No. of Studies
No. of Participants
Mean Difference* HTS - Treatment
“The authors believe there is evidence to recommend the use of hypertonic saline in CF but it should not be used in preference to rhDNase. At this stage the benefit appears to be a reduction in pulmonary exacerbation frequency, though evidence does not exist to say it works best in patients with frequent exacerbations.”
Comparison: Hypertonic saline 3% to 7% versus isotonic saline
Outcome: Percentage change in FEV1
at 2 to 4 weeks (3% to 7%) 2 205 4.15 (1.14, 7.16)
at 12 weeks (7%) 1 149 4.1 (-0.08, 8.28)
at 24 weeks (7%) 1 140 5.37 (1.03, 9.71)
at 36 weeks (7%) 1 134 3.63 (-1.56, 8.82)
at 48 weeks (7%) 1 134 2.31 (-2.72, 7.34)
Outcome: Percentage change in FVC
at 2 to 4 weeks (3% to 7%) 2 205 2.75 (0.00, 5.49)
at 12 weeks (7%) 1 141 4.56 (0.79, 8.33)
at 24 weeks (7%) 1 140 3.64 (0.17, 7.11)
at 36 weeks (7%) 1 134 3.40 (-0.82, 7.62)
at 48 weeks (7%) 1 134 2.76 (-1.09, 6.61)
Outcome: Mucociliary clearance
Radiolabelled isotope 2 22 7.62 (3.51, 11.78)
as area under the curve 2 22 -212 (-271.6, -152.5)
Outcome: Feeling of cleared chest – visual analogue scale
< 7 days 2 62 0.97 (0.35, 1.60)
Outcome: Quality of life – change from baseline
CFQ 14+ 1 91 7.77 (1.86, 13.68)
CFQ parent 1 67 -1.13 (-7.49, 5.23)
SF36 1 91 2.84 (-7.90, 13.58)
Outcome: Exacerbations - Number of visits
requiring antibiotics 1 162 -0.46 (-0.82, -0.10)
hospital admissions 1 162 -0.13 (-0.48, 0.22)
Outcome: Adverse events
Acute fall in FEV1 1 12 5.2 (-0.59, 10.99)
Comparison: Hypertonic saline 3% to 7% versus rhDNase
Outcome: Percentage change in FEV1
at 3 weeks 1 14 -1.6 (-11.16, 7.96)
at 3 months 1 48 -8.0 (-14.0, -2.0)
Outcome: Percentage change in FVC
at 3 months 1 48 -0.03 (-0.12, 0.06)
Outcome: Quality of life – percentage change in quality of life score
scale not defined 1 48 -0.03 (-0.07, 0.01)
Outcome: Delivery time
minutes 1 14 -31.0 (-37.56, -24.44)
Comparison: Hypertonic saline 3% to 7% versus mannitol
Outcome: Delivery time
minutes 1 12 -6.10 (-7.32, -4.88)
Comparison: Hypertonic saline 3% to 7% versus Sudium-2- mercaptoethane sulphate
Outcome: Percentage change in FVC
at eight weeks 1 56 not significant CF= cystic fibrosis; CFQ= cystic fibrosis questionnaire; FEV1= forced expiratory volume in 1 second; FVC= forced vital capacity; SF36= 36-Item Short Form Health Survey
Sodium Chloride Inhalation for Cystic Fibrosis 21
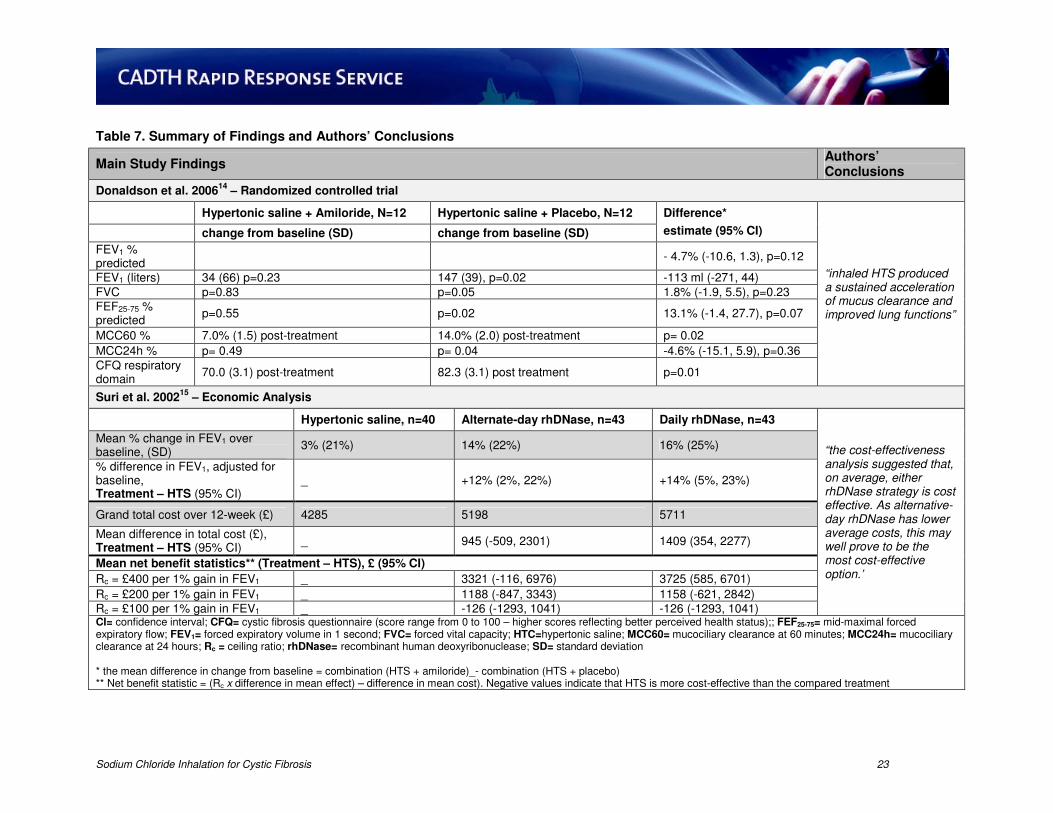
Table 7. Summary of Findings and Authors’ Conclusions
Serious** Adverse Events (occurring ≥2% in either group), n (%)
All, n (%)
158 NA
33 (21)
163 NA
43 (26)
NR
Abdominal pain, n 3 (2) 4 (2)
Cough 13 (8) 16 (10)
Fever 1 (1) 4 (2)
Nasal congestion 2 (1) 3 (2)
Poor growth 5 (3) 5 (3) PAE 4 (3) 2 (1)
Vomiting or emesis 3 (2) 6 (4)
Wheezing 4 (3) 2 (1)
Other 4 (3) 11 (7) CI= confidence interval; FEV0.5= forced expiratory volume in 0.5 seconds; FEF75= forced expiratory flow at 75% of vital capacity; FEF25-75= mid-maximal forced expiratory flow; FRC= functional residual capacity; HR= hazard ratio; BR= not reported; MD= mean difference; NA= not applicable; no.= number; PAE=Pseudomonas aeruginosa eradication; PE= pulmonary exacerbation; PER=pulmonary exacerbation rate; R= ratio; * adjusted for age category, site, and baseline value (for outcomes that require baseline value) – the mean difference in change from baseline= hypertonic saline – Isotonic saline, and ratio = Hypertonic saline / Isotonic Saline ** serious adverse events were not defined in the report
Sodium Chloride Inhalation for Cystic Fibrosis 22
Table 7. Summary of Findings and Authors’ Conclusions
Main Study Findings Authors’ Conclusions
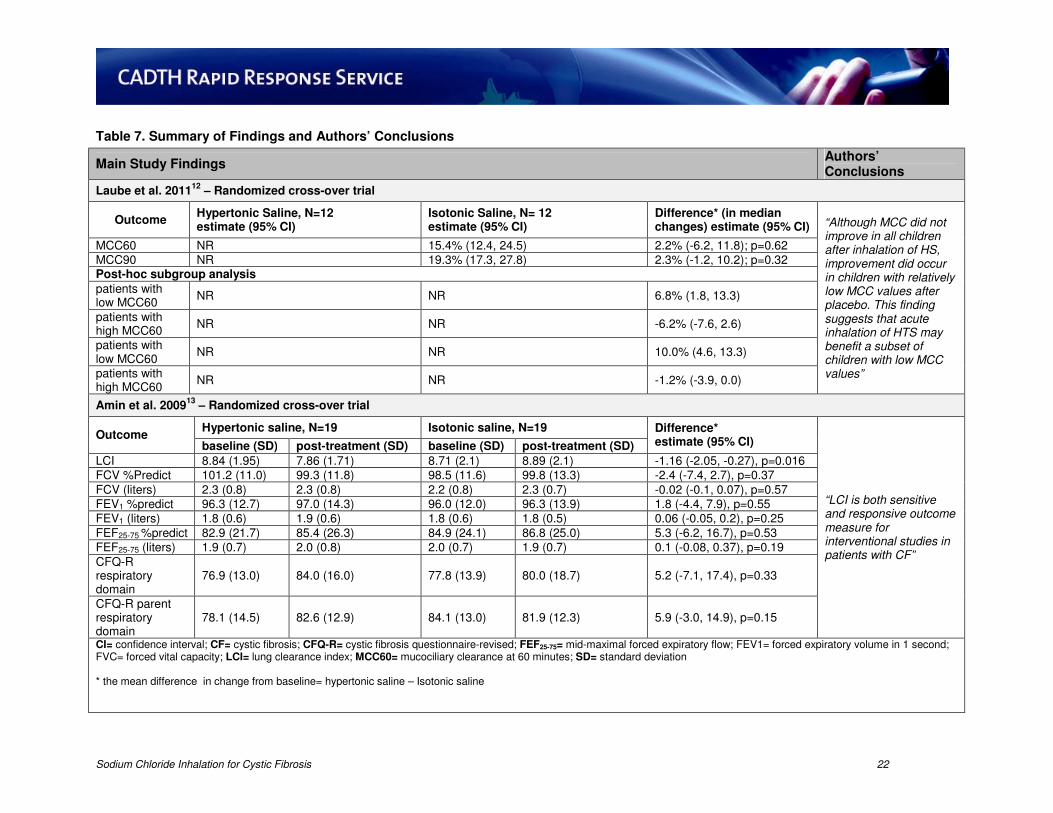
Laube et al. 201112
– Randomized cross-over trial
Outcome Hypertonic Saline, N=12 estimate (95% CI)
Isotonic Saline, N= 12 estimate (95% CI)
Difference* (in median changes) estimate (95% CI) “Although MCC did not
improve in all children after inhalation of HS, improvement did occur in children with relatively low MCC values after placebo. This finding suggests that acute inhalation of HTS may benefit a subset of children with low MCC values”
MCC60 NR 15.4% (12.4, 24.5) 2.2% (-6.2, 11.8); p=0.62
“the cost-effectiveness analysis suggested that, on average, either rhDNase strategy is cost effective. As alternative-day rhDNase has lower average costs, this may well prove to be the most cost-effective option.’
Mean % change in FEV1 over baseline, (SD)
3% (21%) 14% (22%) 16% (25%)
% difference in FEV1, adjusted for baseline, Treatment – HTS (95% CI)
_ +12% (2%, 22%) +14% (5%, 23%)
Grand total cost over 12-week (£) 4285 5198 5711
Mean difference in total cost (£), Treatment – HTS (95% CI)
_ 945 (-509, 2301) 1409 (354, 2277)
Mean net benefit statistics** (Treatment – HTS), £ (95% CI)
Rc = £400 per 1% gain in FEV1 _ 3321 (-116, 6976) 3725 (585, 6701)
Rc = £200 per 1% gain in FEV1 _ 1188 (-847, 3343) 1158 (-621, 2842)
Rc = £100 per 1% gain in FEV1 _ -126 (-1293, 1041) -126 (-1293, 1041) CI= confidence interval; CFQ= cystic fibrosis questionnaire (score range from 0 to 100 – higher scores reflecting better perceived health status);; FEF25-75= mid-maximal forced expiratory flow; FEV1= forced expiratory volume in 1 second; FVC= forced vital capacity; HTC=hypertonic saline; MCC60= mucociliary clearance at 60 minutes; MCC24h= mucociliary clearance at 24 hours; Rc = ceiling ratio; rhDNase= recombinant human deoxyribonuclease; SD= standard deviation * the mean difference in change from baseline = combination (HTS + amiloride)_- combination (HTS + placebo) ** Net benefit statistic = (Rc x difference in mean effect) – difference in mean cost). Negative values indicate that HTS is more cost-effective than the compared treatment