39
Soft Tissue Tumors Soft Tissue Tumors Sybile Val, MD Department of Surgery SUNY Downstate Medical Center SUNY Downstate Medical Center October 29 , 2009

Soft Tissue TumorsSoft Tissue Tumors
Sybile Val, MDDepartment of Surgery
SUNY Downstate Medical CenterSUNY Downstate Medical CenterOctober 29, 2009

Case PresentationCase Presentation
• 52 YOM presented to ED on 7/22 with52 YOM presented to ED on 7/22 with abdominal pain

Case PresentationCase Presentation
• PMH: • SocHx:PMH:– Schizophrenia
• PSH:
SocHx:– ½ PPD x 20 yrs
– Jehovah’s Witness
– None
• Meds:– Risperdal
• ALL:– NKDA
Case PresentationCase Presentation
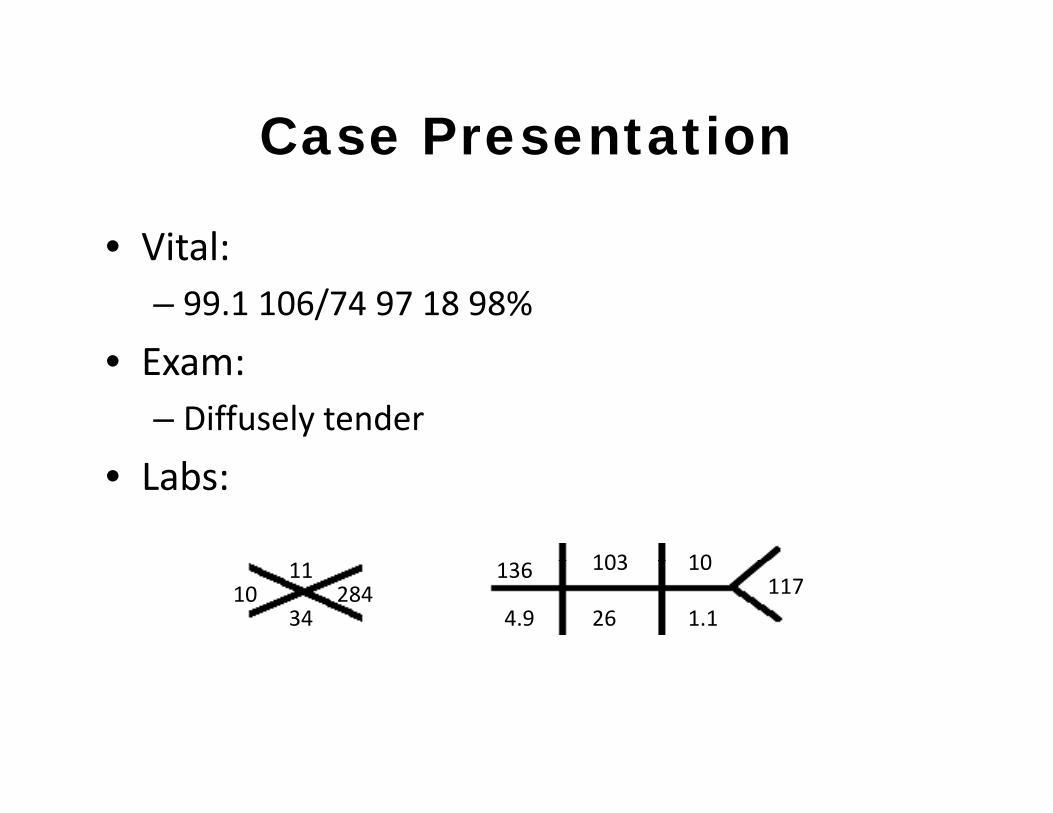
• Vital:Vital:– 99.1 106/74 97 18 98%
• Exam• Exam:– Diffusely tender
• Labs:
103 1010
11
34284
136
4.9
103
26117
10
1.1

Hospital CourseHospital Course• HD #1 • HD#4HD #1
– GI consult
– Surgery consult
HD#4– Tachycardic 110‐120
• HD#5• HD#2
– EGD
– Transferred to surgical service
– Colonoscopy
– VIR biopsy
– Spiked to 101.5
– Cultures and CBC
17• HD#3– Started on diet
• Hct: 17
Path: Malignant small round blue cell tumor with extensive necrosis andtumor with extensive necrosis and degenerative changes

Hospital CourseHospital Course
• HD#6HD#6– Started on Epogen
• HD#10– Discharged home with surgical follow up
S i l Cli iSurgical Clinic
Pt asymptomatic
dHct increased to 30
Scheduled for resection

Hospital Course
• 8/23/09
Hospital Course
8/23/09– Pt admitted for bowel prep
• 8/24/09• 8/24/09– Exploratory laporatomy
E i f h i• Evacuation of hemoperitoneum
• Resection of small bowel mesenteric mass
• Small bowel resection x 2• Small bowel resection x 2
• Partial omentectomy
• Cholecystectomyy y

Intra-OperativelyIntra Operatively

Intra-OperativelyIntra Operatively

Intra-OperativelyIntra Operatively

Post-OperativelyPost Operatively
• POD#0 • POD#4– Hypotensive in RR– Central line placed
– Started on clears– Iron and Epogen
d– Started on pressors
• POD#1Weaned off all pressors
resumed
• POD#10– Hct 23– Weaned off all pressors
– Extubated in afternoon
• POD#3
Hct 23
• POD#11– Discharged home
– NGT removed– Hct 19

PathologyPathology
• Abdominal MassAbdominal Mass– 40x20x8cm in aggregate (19x11x5)
High grade spindle cell sarcoma– High grade spindle cell sarcoma

While Val @ VAWhile Val @ VA
• POD #49POD #49– Presented to ER with 3 days of abdominal pain associated with nausea and vomitingassociated with nausea and vomiting
– AVSS
– Exam: LLQ pain– Exam: LLQ pain
– Labs:93
1512
39402
130
5.4
93
30130.6
158



Hospital CourseHospital Course
• Admitted to surgical serviceAdmitted to surgical service– Conservative management x 2 days
Taken to the OR 8/15/09– Taken to the OR 8/15/09• Exploratory laporatomy
– carcinomatosis encountered
• Evacuation of hemoperitoneum (500ml)
• Lysis of adhesions

Hospital CourseHospital Course
• POD#6POD#6 – Extubated
• POD#7• POD#7– Started on clears
/– Made DNR/DNI by family
• Currently– Tolerating regular diet
– Awaiting hospice

Questions??
Soft Tissue Tumors

Soft Tissue SarcomaSoft Tissue Sarcoma
• Collective term for diverse group of malignanciesg p g• Arise from mesoderm• Represent 1% of all adult tumors• Represent 15% of pediatric tumors• Occur anywhere in the body
– 43% extremities– 15% retroperitoneum– 13% viscera13% viscera– 10% trunk
• More than 50 distinct histological subtypes

Soft Tissue SarcomaSoft Tissue Sarcoma
• Etiology is uncleart o ogy s u c ea• Tumor grade is the best indicator of
– Biological aggressivenessg gg– Metastatic potential– Grade is defined by:
• Tumor cellularity• Nuclear atypia• Degree of necrosisDegree of necrosis• Mitotic activity
• Present as asymptpmatic mass
• Indications for biopsy:Indications for biopsy:– Mass larger than 5cm
History of growth– History of growth
– Persists for more than 4 weeks
SURGERY is the FOUNDATION of the treatment of STS

For intra-abdominal or retroperitoneal sarcomas:
FNA or CNB is not indicated
Except:Suspicion for lymphoma or germ cell tumor
Tissue diagnosis for preoperative therapy
Tissue dx for unresectable disease
S t d t t i f th iSuspected metastasis from another primary

• Poor prognostic factors:Poor prognostic factors:– Large size
Deep seated– Deep seated
– Retroperitoneal vs. extremity
Hi h d– High grade
– High stage
P i i i– Positive margins


Specific Therapy by SiteSpecific Therapy by Site
• Extremity (43%)y ( )– Surgery alone
– Amputation
Limb Sparing Surgery and– Limb Sparing Surgery and adjuvant radiation
• Standard of care • Retroperitoneal and intra‐abdominal (15%)abdominal (15%)– Surgery with negative margins
– Chemotherapy
– Radiation (??)• Adjuvant
• Preoperative
• Intra‐abdominal
• Regional LymphadenectomyRegional Lymphadenectomy– Not indicated
Only 2 6% of sarcomas metastasize to lymph– Only 2.6% of sarcomas metastasize to lymph nodes

Treatment OptionsTreatment Options
• Radiation Therapy • ChemotherapyRadiation Therapy– Recommended for high grade resected STS
Chemotherapy– Controversial
– Favorable px factors for – Improves local recurrence
No impact on survival
response to chemo:• Young Age
• Good performance status– No impact on survival
– Optimal timing unclear
• Good performance status
• Absence of liver mets
• Liposarcoma or synovial hi t lhistology

Recurrence Rates:Extremity 8 20%– Extremity 8‐20%
– Retroperitoneum 38‐50%

Could we have done somethingCould we have done something different in this case??

• Retrospective Analysis1991 2005– 1991‐2005
– Included only patients with advanced disease• Primary tumor or local recurrence not amendable to complete surgical resectionsurgical resection
• Presence of metastatic disease
• Goal:– Determine the efficacy of palliative chemotherapy
• Responders: those who achieved a complete or partial response• Non‐responders: All others
ll l d f f h l d h/l• Overall survival: measured from start of chemo until death/last follow up
– Determine whether specific factors influence the outcome of chemotherapyof chemotherapy


Median time to progression was
3 months

23% of pts were li @ 2alive @ 2 years

189/488
(39%)
299/488
(61%)

• Concluded:– Palliative chemotherapy in advanced STS should be regarded as a standard treatment option in the
t f th i tmanagement of these aggressive tumors
– Doxorubicin based combinations regimens may be associated with superior survival to that achieved with psingle agent
– Factors predictive of superior survival included• Younger age
• Absence of bone mets
• Synovial or liposarcoma histology

Surgical resection is the most effective potentially curative therapy for soft tissue sarcomas regardless of origintissue sarcomas regardless of origin

In SummaryIn Summary
• Soft tissue sarcomas arise from mesenchymalSoft tissue sarcomas arise from mesenchymal tissues
• Extremities and retroperitoneum are most• Extremities and retroperitoneum are most common sites
MRI i f d di i i i d li• MRI is preferred diagnostic imaging modality
• Biospy may be considered for extremity lesions
• Surgical resection is mainstay of treatmentg y

Thank You…

















