33
Francois Venter July 2018 South Africa and TLD introduction Huge thanks CHAI, Andy Hill, Polly Clayden, BMGF, PEPFAR Pretoria and USAID/CDC DC, Unitaid, SA MRC
Francois Venter
July 2018
South Africa and
TLD introduction
Huge thanks CHAI, Andy Hill, Polly Clayden, BMGF, PEPFAR Pretoria and
USAID/CDC DC, Unitaid, SA MRC
Optimize
• Led by Wits RHI, the PEPFAR-supported, USAID-managed OPTIMIZE consortium focuses on accelerating access to PEPFAR’s priority first- and second-line treatment products. OPTIMIZE, formed through an innovative co-formulation effort, partners with five leading private and public sector organizations and leverages co-funding from Unitaid, SAMRC and pharma
• Supporting PEPFAR’s TLD Transition & Global ART Optimization
• Coordinates with several countries for TLD introduction
• Close coordination in SA with Pretoria office – critical for TLD
• ADVANCE and the low-dose darunavir study (052 are two studies in OPTIMIZE (with several related and sub-studies)
•Almost a fifth of global HIV-positive population
•Almost 5 million people on ART (95% on TEE)
•Procurement giant: SA=PEPFAR=Global Fund for ART generics
•Sustainable programme – mostly funded off SA tax base
•Almost halving of incidence in last 5 years in some demographics – HSRC, July 20128
Why is South Africa important?
SA guidelines (state)
FTCTDF EFV
XTC, other nukes
3TC PI(lopinavir)AZT
Darunavir Dolutegravir Etravirine
≈ 5 /7.9 million people on first-line, 250 000-400 000/year
starting/restarting
SA guidelines (state)
FTCTDF EFV
XTC, other nukes
3TC PI(lopinavir/rit)AZT
Darunavir Dolutegravir Etravirine
130-150 000 on 2nd line (should be more, likely to rise with
PEPFAR focus) – suppression rates anecdotally poor
SA guidelines (state)
FTCTDF EFV
XTC, other nukes
3TC PI(lopinavir)AZT
Darunavir Dolutegravir Etravirine
Almost 3000 on adult third-line (accelerating) - >80% suppression
•1st line TEE: $126/year – dropping thanks to negotiations
•2nd line: $350/year
•3rd line: depends, can be $2000 year
•SA drug budget for ARVs >$350 million/year
Adult first-line costs….
•Increasing NNRTI resistance
•Re-entry to system – drive NNRTI resistance
•Large numbers – drug storage
•Stockout of singles
•Lots of pregnancies
•Patients getting older – increased co-morbidities
•(very small numbers of paeds)
Challenges for SA
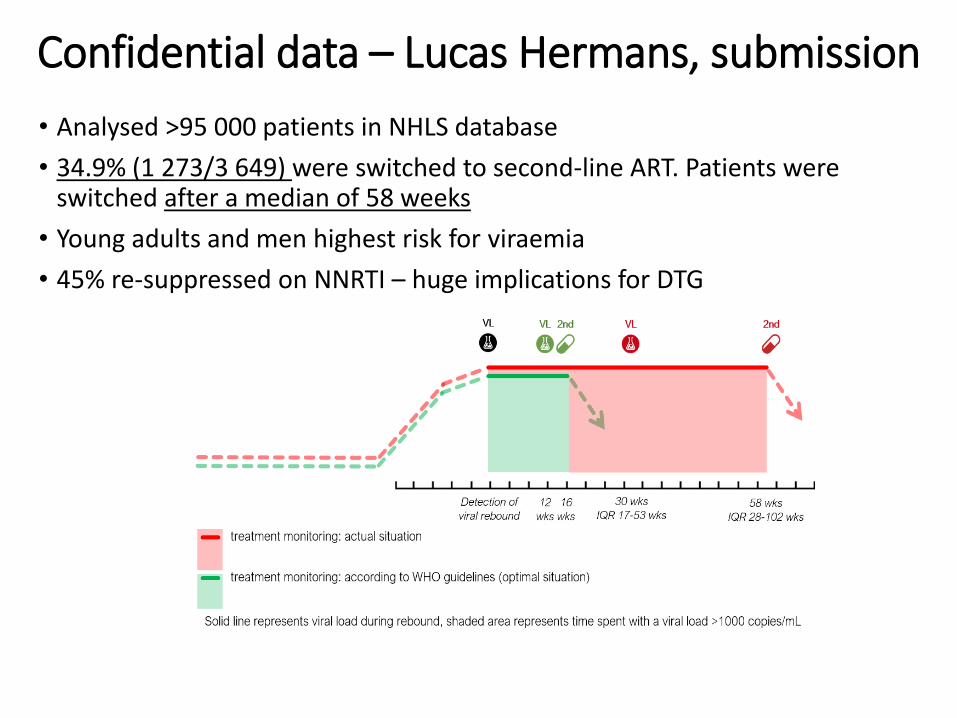
• Analysed >95 000 patients in NHLS database
• 34.9% (1 273/3 649) were switched to second-line ART. Patients were switched after a median of 58 weeks
• Young adults and men highest risk for viraemia
• 45% re-suppressed on NNRTI – huge implications for DTG
Confidential data – Lucas Hermans, submission
“Dolutegravir in first line therapy has by far the highest impact in getting to the last 90 for South Africa”
Professor Gesine Meyer-Rath -Boston University/HE2RO
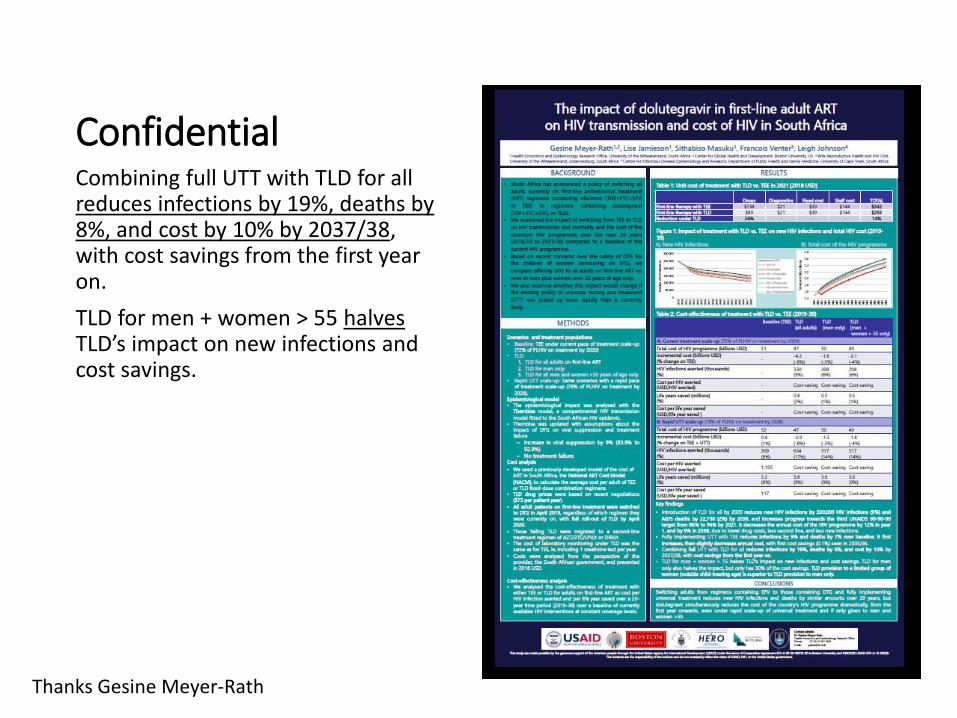
ConfidentialCombining full UTT with TLD for all reduces infections by 19%, deaths by 8%, and cost by 10% by 2037/38, with cost savings from the first year on.
TLD for men + women > 55 halvesTLD’s impact on new infections and cost savings.
Thanks Gesine Meyer-Rath
•Resistance barrier – less second/third-line, simpler adherence message
•Efficacy in context of increasing NNRTI resistance
•Side effects
•Speed of virological control (?PMTCT and sexual transmission benefit)
• Limited drug interactions (especially hormonal contraception)
•Cost
•Size of tablet, packaging
Quick reminder: Benefits of dolutegravir
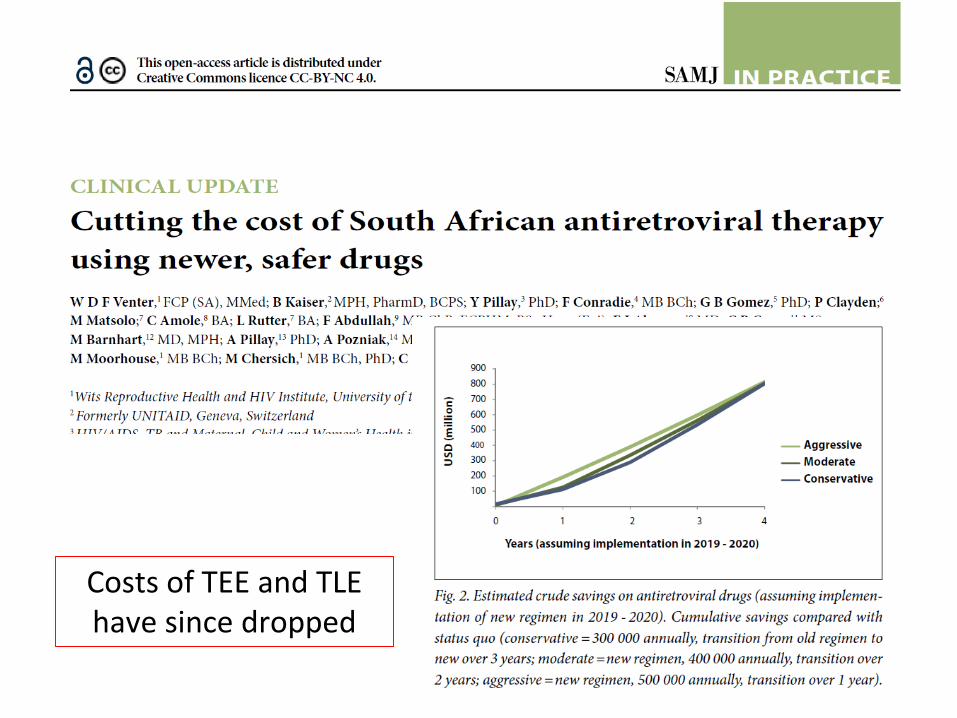
Costs of TEE and TLE have since dropped
Why aren’t these drugs used?
Not preferred options in
WHO guidelines
Many drugs are not
registered and no co-
formulations are available
Limited data on use in TB (almost all new drugs)
Limited data on use in
pregnancy (almost all new drugs)
Costs: abacavir, all
integrase inhibitors –
hope for dolutegravir
Considerations for the switch from EFV to DTG?
•Millions of patients will need to be switched – huge undertaking – and the manufacturing changes will likely be slightly chaotic
•Moving from EFV to DTG likely to be an issue (?VL; side effects) ; reverse a problem
• “Training” – Very NB if VL, or different regimens
•?Harmonisation between and within different countries –private vs public sector, cross borders
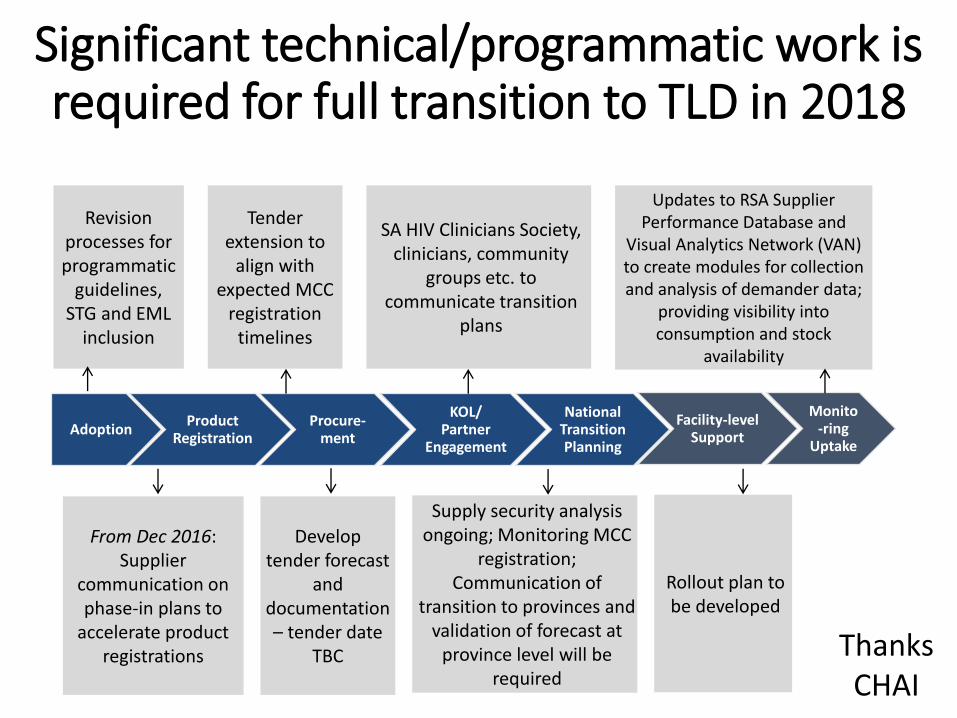
AdoptionProduct
RegistrationProcure-
ment
KOL/Partner
Engagement
National Transition Planning
Facility-level Support
Monito-ring
Uptake
SA HIV Clinicians Society, clinicians, community
groups etc. to communicate transition
plans
Tender extension to
align with expected MCC
registration timelines
Supply security analysis ongoing; Monitoring MCC
registration; Communication of
transition to provinces and validation of forecast at
province level will be required
From Dec 2016: Supplier
communication on phase-in plans to
accelerate product registrations
Revision processes for programmatic
guidelines, STG and EML
inclusion
Develop tender forecast
and documentation – tender date
TBC
Updates to RSA Supplier Performance Database and
Visual Analytics Network (VAN) to create modules for collection and analysis of demander data;
providing visibility into consumption and stock
availability
Rollout plan to be developed
Significant technical/programmatic work is required for full transition to TLD in 2018
Thanks CHAI
South Africa: Late 2016-May 2018
•TLD seen as a national priority
•Huge parallel efforts to work with SAHPRA, DoH (both HIV and drug procurement), clinicians:•Get products registered•Align with tenders•Get agreement on treatment guidelines, TB
Challenges
•Dec 2017: Minister of Health and Cabinet announce DTG introduction will be in April 2018• Jan 2018: Guidelines “finalised”•End Jan 2018: Clear above NOT possible with current
tender processes•March: SAHPRA refused to register ANY TLD
combination•April – clarifying tender processes, working with
SAHPRA; ? “risk mitigation plan” contents• July: New submissions of dossiers• July 2018: Tender planned release 17 August, close mid-
Sept•?April 2019 introduction
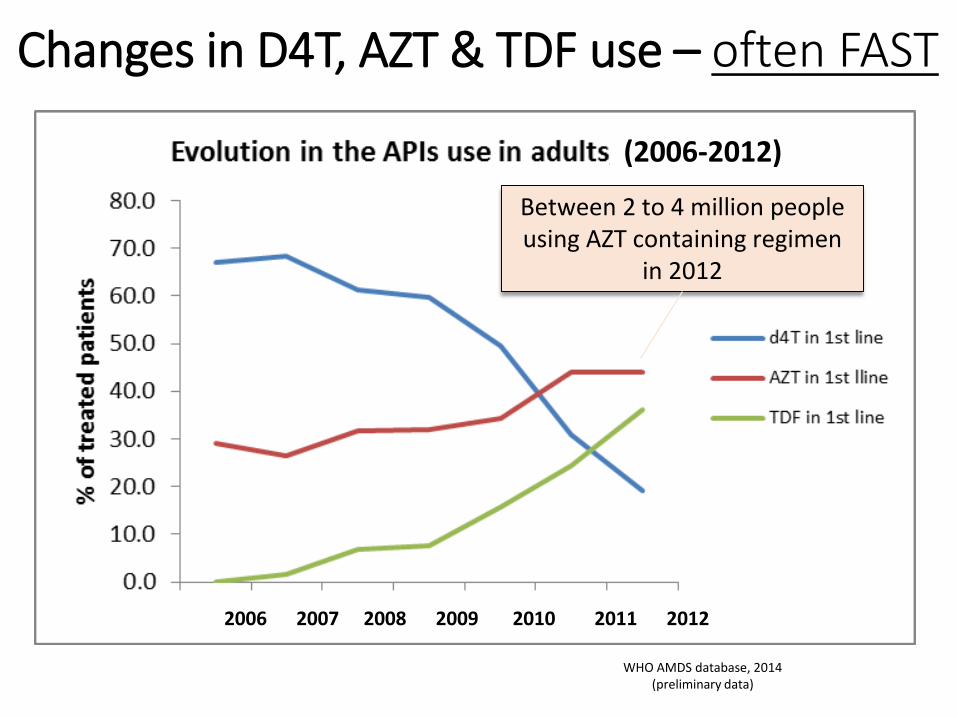
Changes in D4T, AZT & TDF use – often FAST
Between 2 to 4 million people using AZT containing regimen
in 2012
2006 2007 2008 2009 2010 2011 2012
(2006-2012)
WHO AMDS database, 2014 (preliminary data)
The pregnancy cat among the pigeons: April 2018
•Botswana cohort: DTG safe if initiated in pregnancy
•Mid-May: Conception data – 4/426 babies had neural tube defects (preliminary analysis, another 600 awaited)
•More data unlikely to be available before end 2019 to make a decision
SAHPRA: willing to register TLD if:
•Provided with scientific rationale by OPTIMIZE and WHO
CheckBox1
SAHPRA: willing to register products if:
•Provided with scientific rationale by OPTIMIZE and WHO
• Immediate access to early ADVANCE data, with subsequent access to the data till 96 weeks
CheckBox1
SAHPRA: willing to register products if:
•Provided with scientific rationale by OPTIMIZE and WHO
• Immediate confidential access to early ADVANCE data, with subsequent access to the data till 96 weeks
•A “risk mitigation plan” – essentially pharmaco-vigilance to be executed in tandem – and now should include pregnancy!
?
CheckBox1
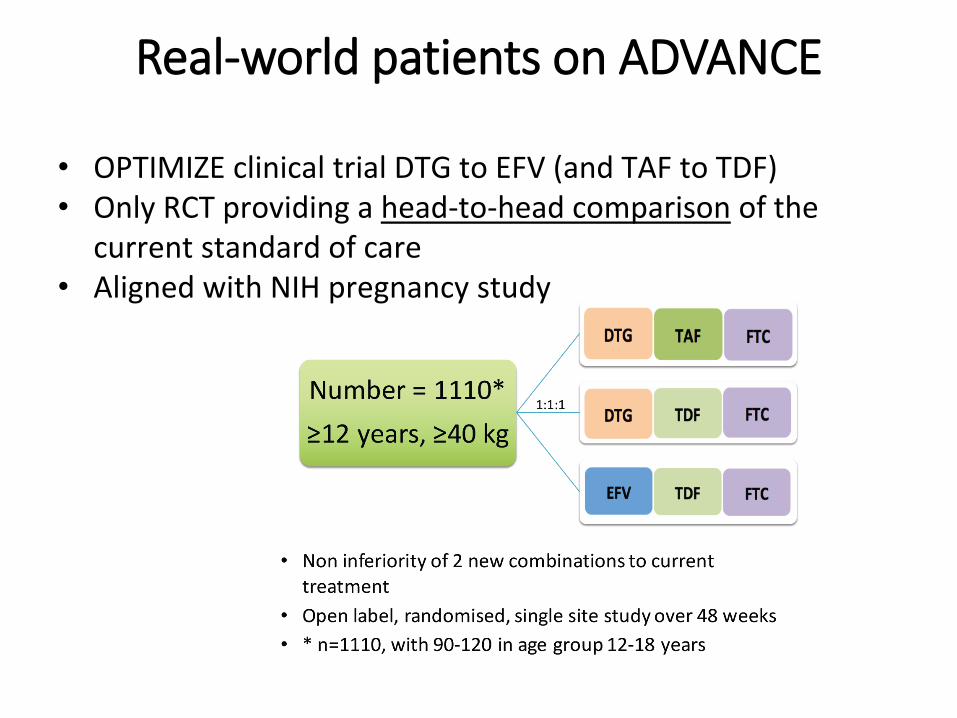
Real-world patients on ADVANCE
• OPTIMIZE clinical trial DTG to EFV (and TAF to TDF)• Only RCT providing a head-to-head comparison of the
current standard of care• Aligned with NIH pregnancy study
Update and assistance to NTD signal
•Data available 2019 Q2 for 48 weeks
• If falls pregnant, can stay on study, APR
•Ultrasound at pregnancy diagnosis and 24 weeks ,paedsexamination at birth, followed to 18 months
•We anticipate approximately 100 conceptions
•Folate study – RCT vs EFV and DTG – working with CDC
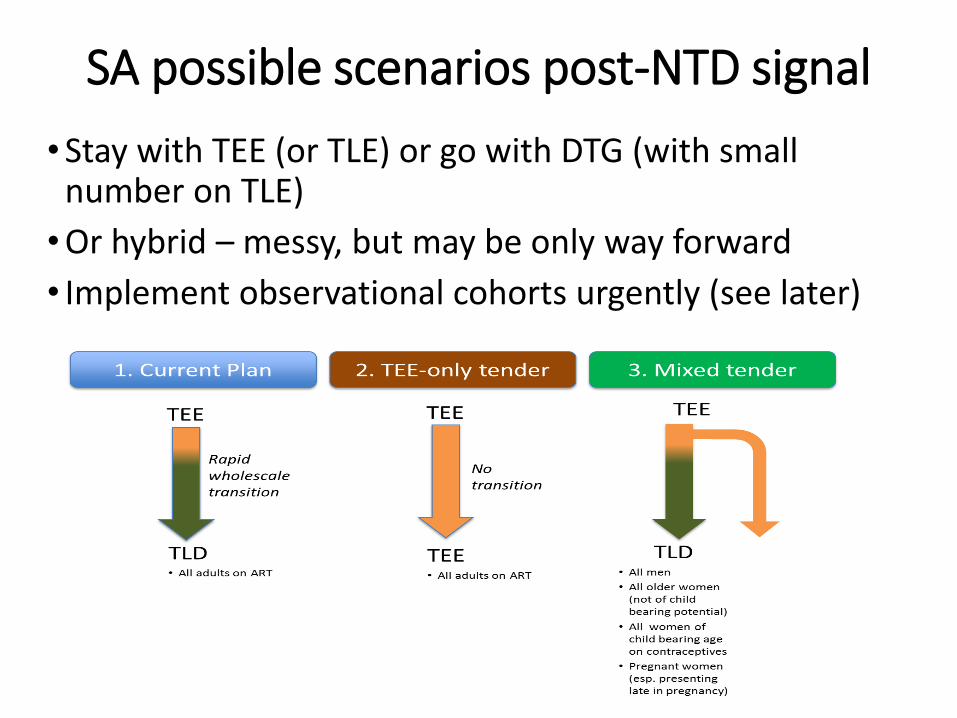
SA possible scenarios post-NTD signal
•Stay with TEE (or TLE) or go with DTG (with small number on TLE)
•Or hybrid – messy, but may be only way forward
• Implement observational cohorts urgently (see later)
Second-line patients in DTG era?
• Lots of concern that DTG not as powerful as PI-based regimens – possibly:•AZT/3TC/DTG if failing TLE/TEE•AZT/3TC/PI if failing TLD (will be rare!)•Suppressed on PI (and never failed d4T/AZT)
What about TAF?
•10-15% saving (manufacturing cost, packaging). ?safety benefit, tablet much small
•Paucity of data – addressed with ADVANCE (TAF arm) partially, TB
•Pregnancy and breastfeeding a concern – 7-8x increase in intracellular tenofovir levels vs conventional TDF
•?2021 introduction – same issues for SAHPRA?
What about darunavir/ritonavir?
•Will be SOME need for second-line
•Current 800/100 or 400/100mg dose can be dose reduced with nanotechnology – big cost saving, potential FDC
•This conference: 400/100mg works as a switch
What about 400mg efavirenz?
•Probably will be recommended as replacing the 600mg dose
•Caution: NAMSAL data due
Supplier (Products)
2017 2018 2019
Q1 2017 Q2 2017 Q3 2017 Q4 2017 Q1 2018 Q2 2018 Q3 2018 Q4 2018 Q1 2019 Q2 2019 Q3 2019 Q4 2019
Jan-17
Feb-17
Mar-17
Apr-17
May-17
Jun-17
Jul-17
Aug-17
Sep-17
Oct-17
Nov-17
Dec-17
Jan-18
Feb-18
Mar-18
Apr-18
May-18
Jun-18
Jul-18
Aug-18
Sep-18
Oct-18
Nov-18
Dec-18
Jan-19
Feb-19
Mar-19
Apr-19
May-19
Jun-19
Jul-19
Aug-19
Sep-19
Oct-19
Nov-19
Dec-19
Filing Filing Filing 9 Month Stability Approval Approval Approval
Filing Both Filing and Stability Filing Approval Approval Approval
Filing Filing Filing 9 Month Stability Approval Approval Approval
Filing Filing Filing 9 Month Stability Approval Approval Approval
Filing Filing Filing 9 Month Stability Approval Approval Approval
Filing Filing Filing Approval Approval Approval
Filing Filing Filing 9 Month Stability Approval Approval Approval
Filing Filing Filing 9 Month Stability Approval Approval Approval
Filing Filing Filing 9 Month Stability Approval Approval Approval
Filing Both Filing and Stability Filing Approval Approval Approval
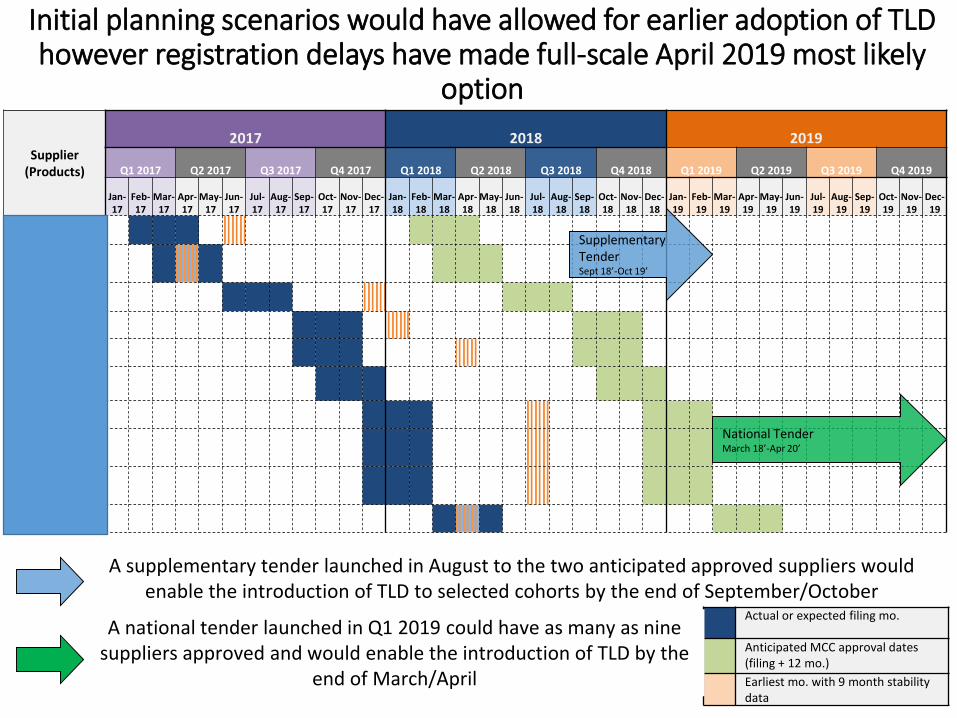
As we stand now, only 2-4 TLD suppliers could possibly be registered
Actual or expected filing mo.
Anticipated MCC approval dates (filing + 12 mo.)
Earliest mo. with 9 month stability data
A supplementary tender launched in August to the two anticipated approved suppliers would enable the introduction of TLD to selected cohorts by the end of September/October
SupplementaryTenderSept 18’-Oct 19’
National TenderMarch 18’-Apr 20’
A national tender launched in Q1 2019 could have as many as nine suppliers approved and would enable the introduction of TLD by the
end of March/April
Initial planning scenarios would have allowed for earlier adoption of TLD however registration delays have made full-scale April 2019 most likely option
Initial planning scenarios would have allowed for earlier adoption of TLD however registration delays have made full-scale April 2019 most likely
option
Summary for South Africa
• Current tender/registration delicately poised – OPTIMIZE, SAHCS and CHAI assisting (thanks to Unitaid funding)
• SAHPRA wants a pharmacovigilance programme – including pregnancy
• TLD likely to be in first-line – IF above happens
• Has major implications for training – different guidelines for TB and pregnancy, transitioning
• Pregnancy likely to remain a major concern; huge opportunity for strengthening contraception (and IPT!)
• TLE 400mg possibly will replace 600mg; darunavir replaces PIs
• Second and third-line patients likely to increase in short-term
• TAF due in 2-3 years
What can PEPFAR do?
•Priority #1: Support DoH training re new guidelines –and include nurses/ pharmacists /counsellors, not just doctors•Priority #2: Ensure SAHPRA and DoH processes are
supported•Priority #3: Support pharmacovigilance efforts– for
both TLD and TAF (and other new meds)•Priority #4: Continue ADVANCE support (important to
secure DTG and TAF for SAHPRA), and darunaviroptimisation (2nd line priority)•Priority #5: Watch regional impact – SA will take 25
million TLD packs in 2019 >>> predicted

















