45
ACHP Affordability Discussion Specific Cost Savings Strategies December 17, 2014

ACHP Affordability
Discussion Specific Cost Savings Strategies
December 17, 2014

ACHP News and Upcoming Events
2
Recent Affordability Profiles: • Asthma Home Visiting and Case
Management program (UCare) • Behavioral Health Case
Management (CDPHP) • Low-Risk Chest Pain Protocol
(HealthPartners) • Reduced Blood Utilization (Select
Health) • Heart Failure Clinic (Security
Health Plan) • Care Partners for Frail Elders
(Independent Health) • Use of Clinical Pharmacists (GHC-
SCW) • Shared Decision-Making (Group
Health) • Improved PAC and SNF
Performance (Geisinger Health Plan)

Specific Cost Savings Strategies
Payment Reform Models: • Stephen Perkins, M.D., Vice President, Medical Affairs UPMC Health Plan
Improved Clinical Efficiency:
• Gretchen Leiterman, Vice President, Operations and Hospital Specialty Services, HealthPartners
• William Nelson, M.D., Ph.D., Department Head, HealthPartners Cardiology and Medical Director, Regions Hospital Heart Center
3
Value Based Payment Initiatives Knee and Hip Replacement Bundled Payment Model ACHP Webinar 12/17/2014
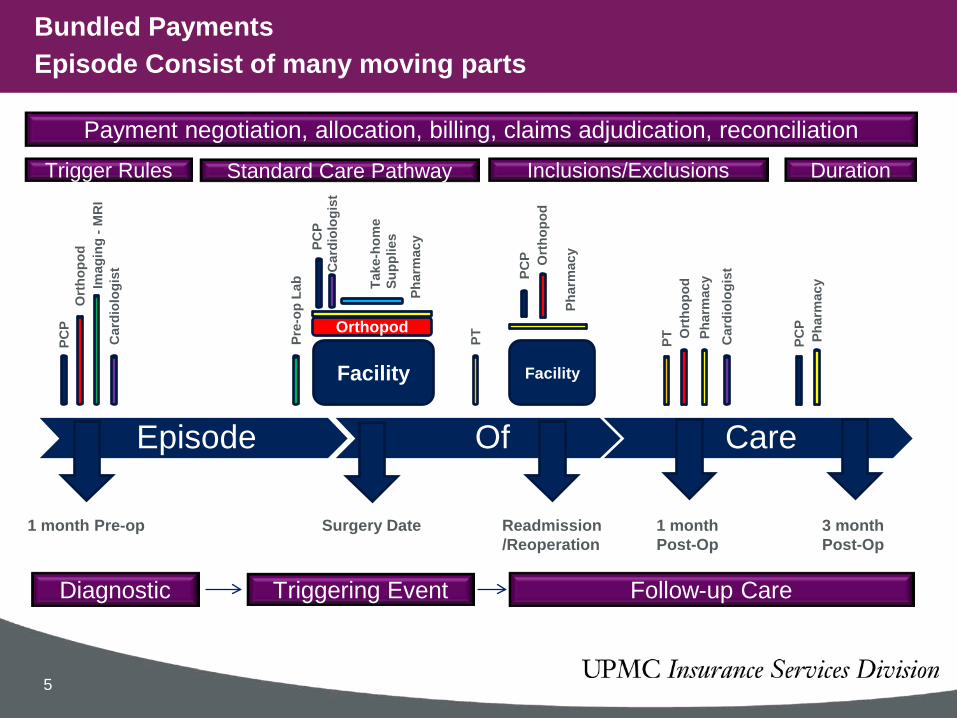
Bundled Payments Episode Consist of many moving parts
Payment negotiation, allocation, billing, claims adjudication, reconciliation
Episode Of Care
Trigger Rules Standard Care Pathway Inclusions/Exclusions Duration
1 month Pre-op Surgery Date Readmission/Reoperation
1 month Post-Op
3 month Post-Op
Diagnostic Triggering Event Follow-up Care
PCP
Ort
hopo
d Im
agin
g - M
RI
Car
diol
ogis
t
Facility
Pre-
op L
ab
Orthopod PC
P C
ardi
olog
ist
Phar
mac
y
Take
-hom
e Su
pplie
s
PT
Facility
Phar
mac
y
Ort
hopo
d PC
P
PT Ort
hopo
d Ph
arm
acy
Car
diol
ogis
t
PCP
Phar
mac
y
5

Alternative Payment Methodologies
6
• Objective - Incentivize physicians to deliver quality care across the entire episode of care in a cost-efficient manner
• Four examples of potential payment models: 1. Shared Savings (Retrospective Reconciliation) 2. Retrospective Bundled Payment 3. Prospective Bundled Payment 4. Global Capitation
• All payment methodologies are subject to quality and clinical pathway-adherence standards in order to receive any incentive payments
• Considerations when determining the appropriate payment model – Definition of continuum of care / pathway – Participation / buy-in from providers – Quality benchmarks / standards – Utilization benchmarks / standards
• Program Objective: • Incentivize physicians to increase quality of care by:
1. Adhering to an evidence-based pathway, and 2. Choosing the most cost effective implantable devices and supplies
• Program Criteria:
• Pilot period effective from July 2013 to July 2014 • UPMC Health Plan is the patient’s primary insurer • Patient is a Commercial Fully Insured/ASO or Medicare member • Patient is receiving a total hip/knee replacement (MS DRG 469 & 470) • Acuity Level 1 and 2 only as determined by APR DRG • Patient is discharged to home
Hip and Knees Shared Savings Initiative: Program Overview
7

Professional & Ancillary Services
Operating Room Supply
Costs
Physician CLAIMS Savings
Physician COST
Savings
Quality
Threshold (80 points)
Physician Shared Savings
Payment
Professional & Ancillary Services
• Savings shared between Health Plan and physician
• Based on evidence-based clinical pathway
• Includes 30 days pre and 90 days post-surgery All costs of episode of care, except DRG
• Bundled Payments only apply to elective procedures acuities 1&2
Operating Room Supply Costs
• Savings reduce Health Plan payment to hospital
• Savings shared between hospital and physician
• Based on best practice
Quality Criteria
8

Hip and Knees Shared Savings Initiative: Physician Scorecard – Quality (7/1/2013 – 10/31/2013)
9
Total Surgeries By Physician: 3
ScoreGoal
(Threshold)Maximum
Potential Points Meets Goals?100.0% > 60.0% 25 Yes
0.0% < 10.0% 5 Yes0.0% < 1.0% 10 Yes0.0% < 1.0% 10 Incomplete0.0% = 0.% 5 Yes
100.0% >= 75% 10 IncompleteEligible
SurgeriesSurveys
Returned
Pre-Surgical 3 2
Post-Surgical 3 0
Pre-Surgical 3 3
Post-Surgical 3 225
105 Pt
Improvement
Incomplete
31
Quality of Life (SF12)
Functional Assessment (Physical Therapy evaluation)
N/A, no post-surgical follow-up
Patients do not show overall improvement
Patient Satisfaction
Eligible Surgeries
3033
Hips and Knees Shared Savings InitiativePhysician Scorecard - Quality
SAMPLEPeriod: 7/1/2013 - 10/31/2013
Adherence to Pathway: Order SetsBlood UtilizationSurgical Site Infections90-Day Readmission*Pulmonary Embolism
Any Improvement
Incomplete
Measure
The quality scores must be at or above 80/100 by year end reconciliation in order for physicians to be eligible to receive savings.

Hips and Knees Shared Savings Initiative: Key Metrics
10
Avg. # of
Tests
Avg. $ per Case
Avg. # of
Tests
Avg. $ per Case
CBC with Platelets
PT-INR
BMP
UA and C&S
MRSA Culture
All Other
Total
Hip Unilateral 1 View
EKG
All Other
Total
Chest, 2 Views, Frontal & Lateral
Hips Bilateral 2 Views Anteropost Pelvis
Hip Unilateral Complete Minimum 2 Views
Pre-Surgical TestingLab
Radiology
Hip Replacements Commercial Medicare
Surgeries
Selected Key impactable areas
Avg. # of
Consults
Avg. $ per Case
Avg. # of
Consults
Avg. $ per Case
PCP Consult
Initial Follow Up
Pain Service
Initial Follow Up
Cardiology
Initial Follow Up
Total
Avg. # of
Visits
Avg. $ per Case
Avg. # of
Visits
Avg. $ per Case
Home Health (Nurse)
Home PT
Outpatient PT
Total
Inpatient StaySpecialty Consults
Post-Surgical Rehab*
Physical Therapy
Hip Replacements Commercial Medicare
Surgeries
Selected Key impactable areas

OR Costs
Labs
Radiology
Nursing Staff
Anesthesia
Room and Board
Recovery
PA’s
OR and Equipment
Usage OR Supplies*
Pharmacy
Blood Products
Physical Therapy
Hips Target Costs: Implant Blade Catheter Drain Dressing Pharmacy Blood
Knees Target Costs: Implant Additional Implant Components Blade Catheter Cement Pharmacy Blood
Target OR Supplies, Pharmacy, and Blood Cost
*OR Supply costs are based on FY2012 supply items charged to patients. They do not include low-cost items such as sutures, drapes, gloves and reusable instruments. They also do not include any supplies used but not documented in Surginet.
OR cost distributions provided for example/reference purposes only

Claims Cost per Episode and OR Supply Costs
12
Maximum
75th Percentile
Average
Median
25th Percentile
Minimum

Hip and Knee Shared Savings Pilot Update
13
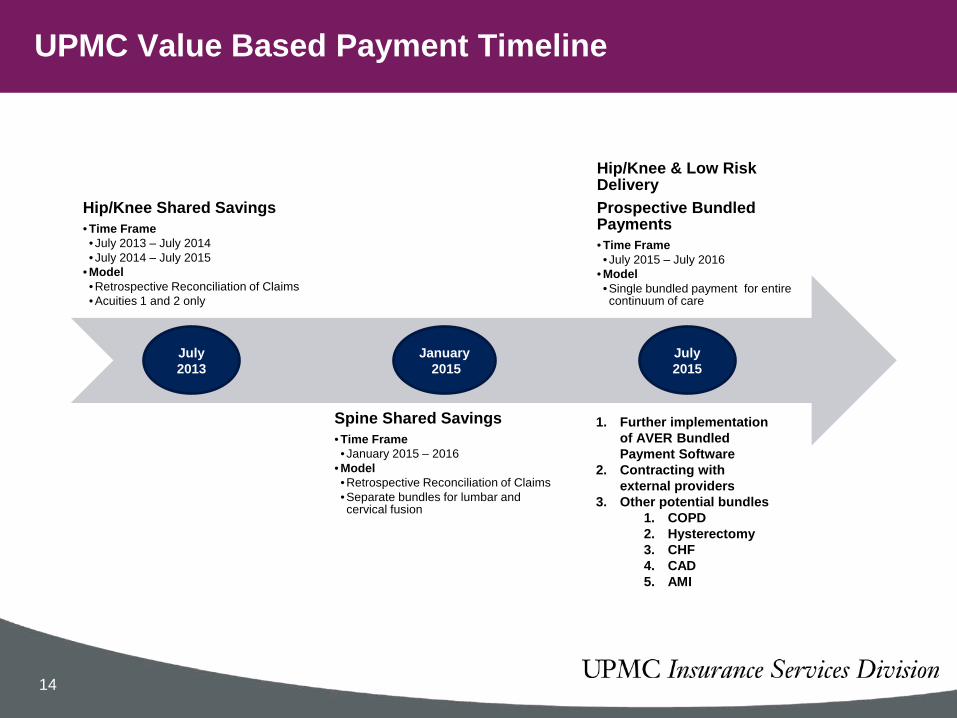
UPMC Value Based Payment Timeline
14
Hip/Knee Shared Savings • Time Frame • July 2013 – July 2014 • July 2014 – July 2015
• Model • Retrospective Reconciliation of Claims • Acuities 1 and 2 only
Spine Shared Savings • Time Frame • January 2015 – 2016
• Model • Retrospective Reconciliation of Claims • Separate bundles for lumbar and cervical fusion
Hip/Knee & Low Risk Delivery Prospective Bundled Payments • Time Frame • July 2015 – July 2016
• Model • Single bundled payment for entire continuum of care
July 2013
January 2015
July 2015
1. Further implementation of AVER Bundled Payment Software
2. Contracting with external providers
3. Other potential bundles 1. COPD 2. Hysterectomy 3. CHF 4. CAD 5. AMI

Questions?
Stephen Perkins MD Vice President, Medical Affairs Tom Aubel Director of Medical Payment Strategy & Policy
15

ACHP AFFORDABILITY WEBINAR LOW RISK CARDIAC PROTOCOLS: REDUCING COST & IMPROVING CARE December 17, 2014
Gretchen Leiterman Vice President, Operations & Hospital Specialty Services
William Nelson, MD, PhD Department Head – HealthPartners CV Service Line
Medical Director, Regions Hospital Heart Center
Presenters have nothing to disclose

Affordability Profile: Improving low risk cardiac care
• Organizational Overview • Triple Aim Results • Low Risk Chest Pain Protocol • Next Steps
– Low Risk Congestive Heart Failure Protocol – Low Risk Atrial Fibrillation Protocol

HealthPartners • Not-for-profit, consumer-governed • Integrated care and financing system
– A team of 21,000 people – Health plan
• 1.4 million health and dental members in Minnesota and surrounding states – Medical Clinics
• 1 million patients • 1,700 physicians
– Park Nicollet Health Services – HealthPartners Medical Group – Stillwater Medical Group
• 55 medical and surgical specialties • 45 primary care clinics • Multi-payer
– Dental Clinics • 60 dentists, 21 locations
– Seven hospitals • Regions: 454-bed level 1 trauma and tertiary center • Methodist: 426-bed acute care hospital, featuring the Jane Brattain Breast Center • Lakeview: 97-bed acute care hospital, national leader in orthopedic care • Hudson: 25-bed critical access hospital, award-winning healing arts program • Westfields: 25-bed critical access hospital, regional cancer care location • St. Francis: 86-bed community hospital (partial owner) • Amery: 25-bed critical access hospital, joining HealthPartners January 1, 2014

Electronic Medical Records •Named “Most Wired” by Hospital and Health Networks magazine four years in a row
Community benefit •2013 Anti-Stigma Award from Minnesota National Alliance on Mental Illness •Recognized as a ‘Leader in LGBT Healthcare Equality’ by the Human Rights Campaign
Top Hospital •Leapfrog Top Hospital, the most competitive hospital quality award in the country. •Only urban hospital in Minnesota to earn this recognition •Awarded “Grade A” in The Leapfrog Group Hospital Safety Score.
Minnesota Hospital Association •Safe from Falls, Safe Skin, Safe Site, Safe Count, Safe Account •Recognized by MHA and the March of Dimes for reducing early elective deliveries •Recipient of 2013 Good Catch Award for patient safety
Joint Commission • One of the top performing hospitals in the nation for heart attack, heart failure, pneumonia and surgical care •First hospital in Minnesota to be named a Certified Comprehensive Stroke Center
Critical Care •In 2013, the American Association of Critical-Care Nurses (ACCN) honored Regions SICU with its Beacon Award for Excellence •Regions inpatient heart and vascular unit received the same award in 2010 and 2012
Environmental excellence •Received award from Practice Greenhealth for achieving benchmarks in energy conservation, mercury reduction pollution prevention and recycling
Distinguished Hospital for Clinical Excellence • Among HealthGrades top 5 percent of hospitals in the nation for high-quality outcomes •Among “America’s 100 Best Hospitals” for pulmonary care, stroke care and critical care
Regions Hospital & HealthPartners – Collaborating to improve quality, experience & cost
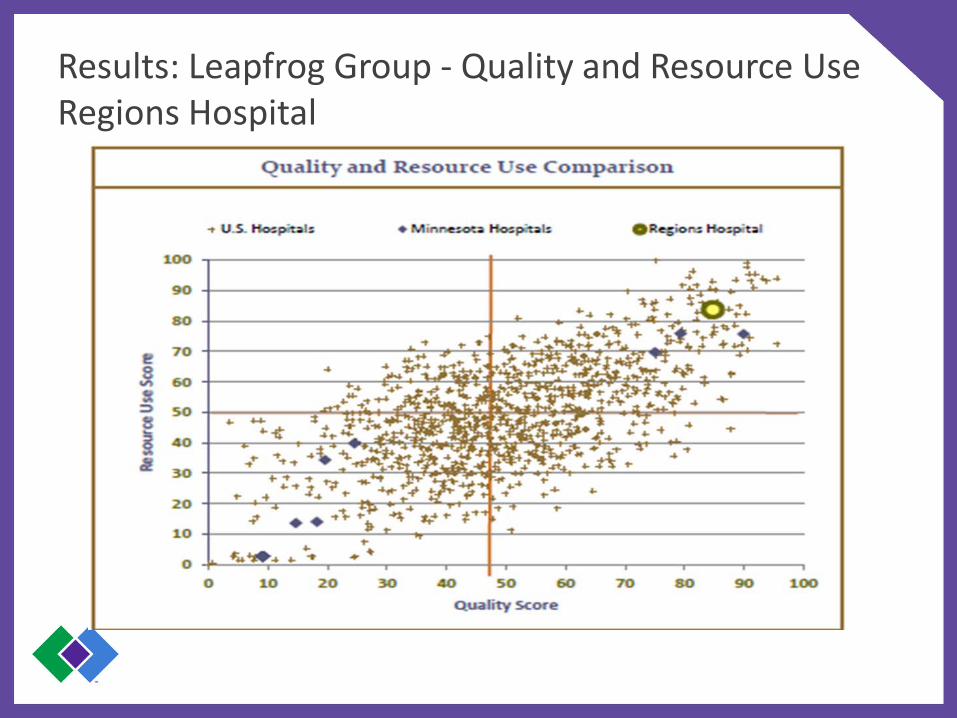
Results: Leapfrog Group - Quality and Resource Use Regions Hospital

Results: HealthPartners – Heart Attack (AMI) Regions Hospital
0.70
0.75
0.80
0.85
0.90
0.95
1.00
80%
85%
90%
95%
100%
2005 2006 2007 2008 2009 2010 2011 2012 2013
0.84
AMI Core Measure Bundle Includes* • Aspirin at Arrival and Discharge • ACE1 or ARB for LVSD • Smoking Cessation Counseling
DECREASE Total Cost Index (compared to statewide average). Less than 1 is better than network average
INCREASE percentage of patients who “Would Recommend” Regions Hospital
94%
Core Measure Outcomes
81%
Patient Satisfaction
Total Cost of Care
96%
100%

Low Risk Chest Pain

Low Risk Chest Pain Protocol - Background
• Implemented in September 2011 • Collaboration between Cardiology, Emergency
Medicine and Hospital Medicine • Aim: Standardize care for Low Risk Chest Pain
patients to improve the patient experience, ensure safety (using evidence to guide treatment), and reduce costs to the system
• Three years of consistent performance and positive outcomes

Innovation: HealthPartners Low Risk Chest Pain Program Flow @ Regions Hospital
Typical US Patient Experience: ER evaluation hospital observation admit 1-2 day stay (often
includes noninvasive imaging) home HealthPartners Low Risk Chest Pain Protocol: Rapid ER evaluation
• TIMI Risk score – 0,1 • Negative troponin at 0 and 6 hours
Low risk group (most) home stress test next day
(echo/nuclear, 7d/wk)
$2600 savings per patient

Chest Pain - Volume Trend (2007-2014) Regions Hospital Growth
409 475 474 387205 115 49 86
456
593762 921
1,028
826843
868
126 658 690 662
865
1,068
1,2361,308 1,359
1,599 1,582 1,616
0
200
400
600
800
1,000
1,200
1,400
1,600
1,800
2,000
2007 2008 2009 2010 2011 2012 2013 2014 YTDAnnualized
Inpatient Observation LRCP
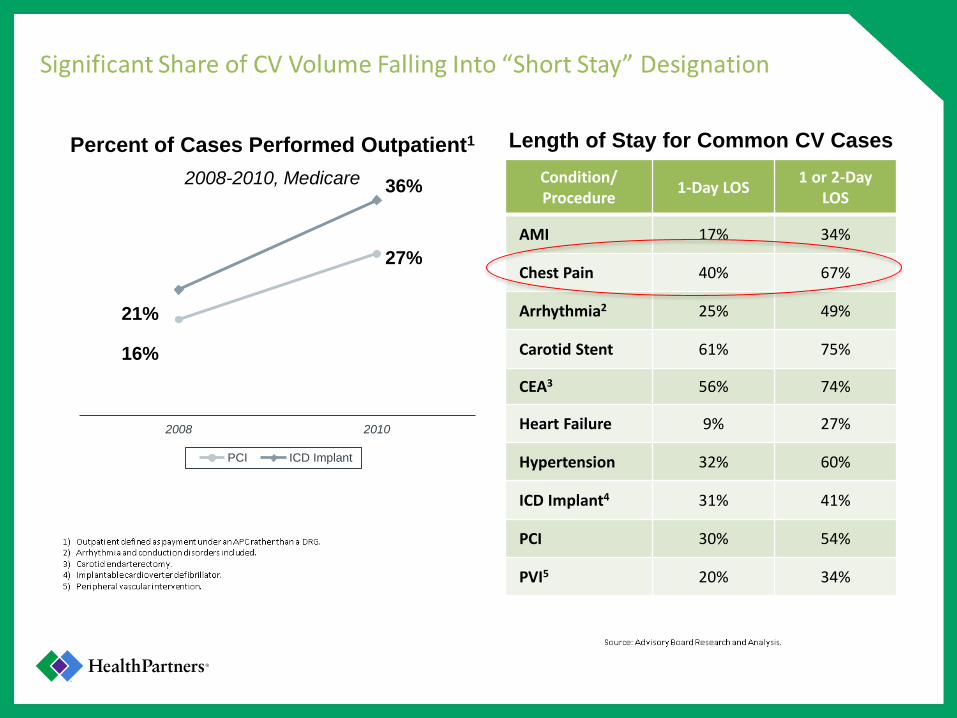
2008-2010, Medicare
2008 2010
PCI ICD Implant
16%
21%
27%
36%
Length of Stay for Common CV Cases Condition/ Procedure 1-Day LOS 1 or 2-Day
LOS
AMI 17% 34%
Chest Pain 40% 67%
Arrhythmia2 25% 49%
Carotid Stent 61% 75%
CEA3 56% 74%
Heart Failure 9% 27%
Hypertension 32% 60%
ICD Implant4 31% 41%
PCI 30% 54%
PVI5 20% 34%
Percent of Cases Performed Outpatient1

Innovation: HealthPartners Low Risk Chest Pain Outcomes @ Regions Hospital
0
10
20
30
40
50
60
70
80
90
ED Low risk chest pain patients
OP Scheduled Eve & Weekends
No Show
Positive Stress-Cath
ED Pt stress Mon - Fri 8 am - 5 pm
Monthly Totals
OP Scheduled Eve & Weekends No Show Positive Stress-Cath
ED Pt stress Mon - Fri 8 am - 5 pm
Totals 2025 481 29 121

Chest Pain – Readmissions Decline Regions Hospital
24
18
13
7
0
5
10
15
20
25
30
2010 2011 2012 2013
Readmissions
Low Risk Chest Pain Protocol - Success • More than 2000 patients have benefited at
Regions Hospital alone • Safely avoided unnecessary care and
benefited organization by $4 million dollars in rate alone
• HealthPartners shares these protocol with other participating providers to spread the benefits across the network
• Success of this program led to exploration of other low risk cardiac pathways

Low Risk Congestive Heart Failure

Low Risk CHF Protocol - Background
• AIM: create protocol to safely avoid hospitalizations/readmissions for low risk CHF patients through team approach involving ED, hospital medicine, and cardiology
• Hospital readmissions for CHF have historically been approximately 20% – Affordable care act institutes penalties for CHF
readmissions

Innovation: HealthPartners Low Risk Heart Failure Program Flow @ Regions Hospital
ED Presentation Home
Observation
Meets low risk criteria
IV Diuretics
ED Observation
No
Yes Next day CHF Clinic follow-up 1 week CHF Clinic Follow-up

Innovation: HealthPartners Low Risk Heart Failure Protocol Regions Emergency Department
Innovation: HealthPartners Low Risk Heart Failure Outcomes @ Regions Hospital
Protocol initiated in June 2012 and has led to change in ED care patterns
• ED trends from 2010 onward demonstrates a trend in higher utilization of observation and discharges to home after this protocol was initiated
In 7 month period, 13 total 30-day inpatient admissions were saved
• 4 total 30-day inpatient admissions were saved by placing patients in observation • 9 total 30-day inpatient admissions were saved by discharging patients to home
Overall, this is a low risk population • Only 7 of 59 patients were readmitted within 30 days
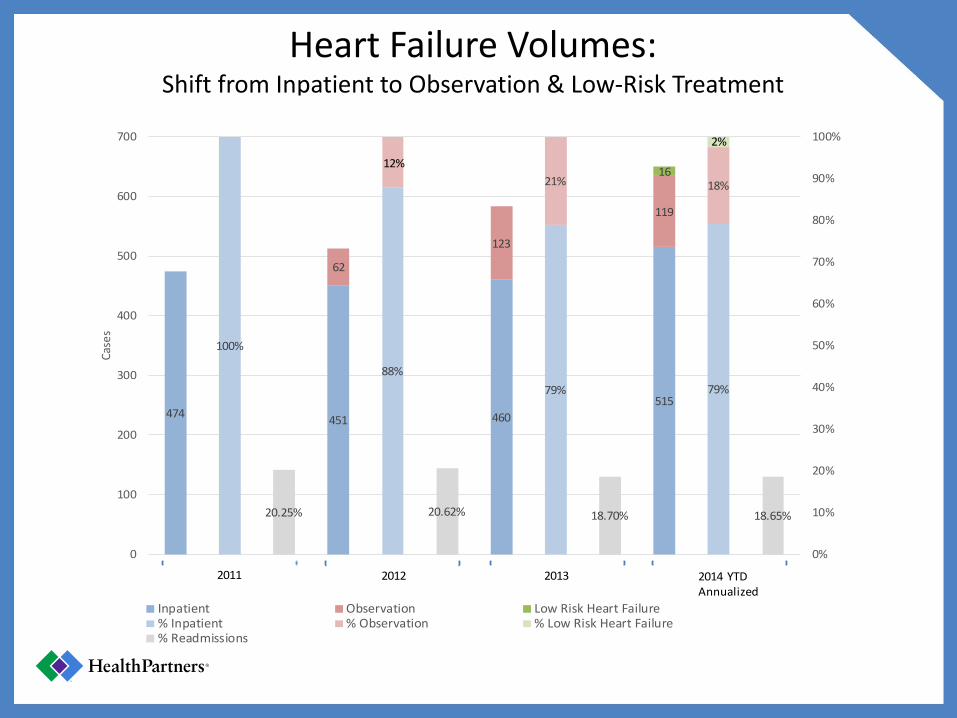
Heart Failure Volumes: Shift from Inpatient to Observation & Low-Risk Treatment
474 451 460515
62
123
119
16
100%
88%79% 79%
21% 18%
20.25% 20.62% 18.70% 18.65%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
0
100
200
300
400
500
600
700
Case
s
Inpatient Observation Low Risk Heart Failure% Inpatient % Observation % Low Risk Heart Failure% Readmissions
2011 2012 2013 2014 YTD Annualized
2%
12%

Low Risk Atrial Fibrillation

Low Risk Afib Protocol - Background
• 2.6 million people in US 2010 • Prevalence projected to double 2020 • Afib accounts for 1% of all ED visits in US 65% result in hospital admission 20% 30 day adverse outcome • ED management varies greatly – proclivity for
cardioversion in patient with recent onset afib • Spontaneous conversion to NSR in 70% patients
with recent onset afib.


Innovation: HealthPartners Low Risk Afib Program Flow @ Regions Hospital

After Visit Summary
• Echo will be done next day at 10am • Cardiology visit at 11:20am • NPO after 7am except meds • You may need a ride home

Atrial Fibrillation Volumes: Shift from inpatient to observation
213 207 196 180
43 53 78
52
16
83% 80% 72% 73%
17% 20% 28%
21%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
0
50
100
150
200
250
300
350
400
C a s e s
Inpatient Observation Low Risk Afibrillation % Inpatient % Outpatient % Low Risk Afibrillation
2011 2012 2013 2014 YTD Annualized
6%

Affordability Profile: Improving low risk cardiac care Summary of Success
• Reduced the number and rate of readmissions for chest pain & congestive heart failure patients
• Improved the experience of care for low risk cardiac patients
• Reduced the costs to patients and the system overall
• Shared learnings and benefits across all HealthPartners Networks

Questions & Discussion
Discussion • What type of cost-reduction information from ACHP
would be of the greatest value to you in 2015?
• What are new, ongoing or particularly innovative cost-reduction initiatives taking place at your plan?
• How are cost reduction strategies different for plan-employed versus network physicians?
• How do your approaches either differ or align with those of UPMC and HealthPartners?
44

[email protected] Phone: 202-785-2247 www.achp.org
1825 Eye Street, NW Suite 401 Washington, DC 20006

















