Speech Surgery: Crafting Technique to Problem Speech Surgery: Crafting Technique to Problem Technique to Problem Technique to Problem Sherard A. Tatum, MD, FAAP, FACS P f f O l l d P di i Sherard A. Tatum, MD, FAAP, FACS P f f O l l d P di i Professor of Otolaryngology and Pediatrics Upstate Medical University S U N Y Syracuse Professor of Otolaryngology and Pediatrics Upstate Medical University S U N Y Syracuse S.U.N.Y. Syracuse S.U.N.Y. Syracuse
Transcript
Speech Surgery: Crafting Technique to Problem
Speech Surgery: Crafting Technique to ProblemTechnique to ProblemTechnique to Problem
Sherard A. Tatum, MD, FAAP, FACSP f f O l l d P di i
Sherard A. Tatum, MD, FAAP, FACSP f f O l l d P di iProfessor of Otolaryngology and Pediatrics
Upstate Medical UniversityS U N Y Syracuse
Professor of Otolaryngology and PediatricsUpstate Medical University
S U N Y SyracuseS.U.N.Y. SyracuseS.U.N.Y. Syracuse
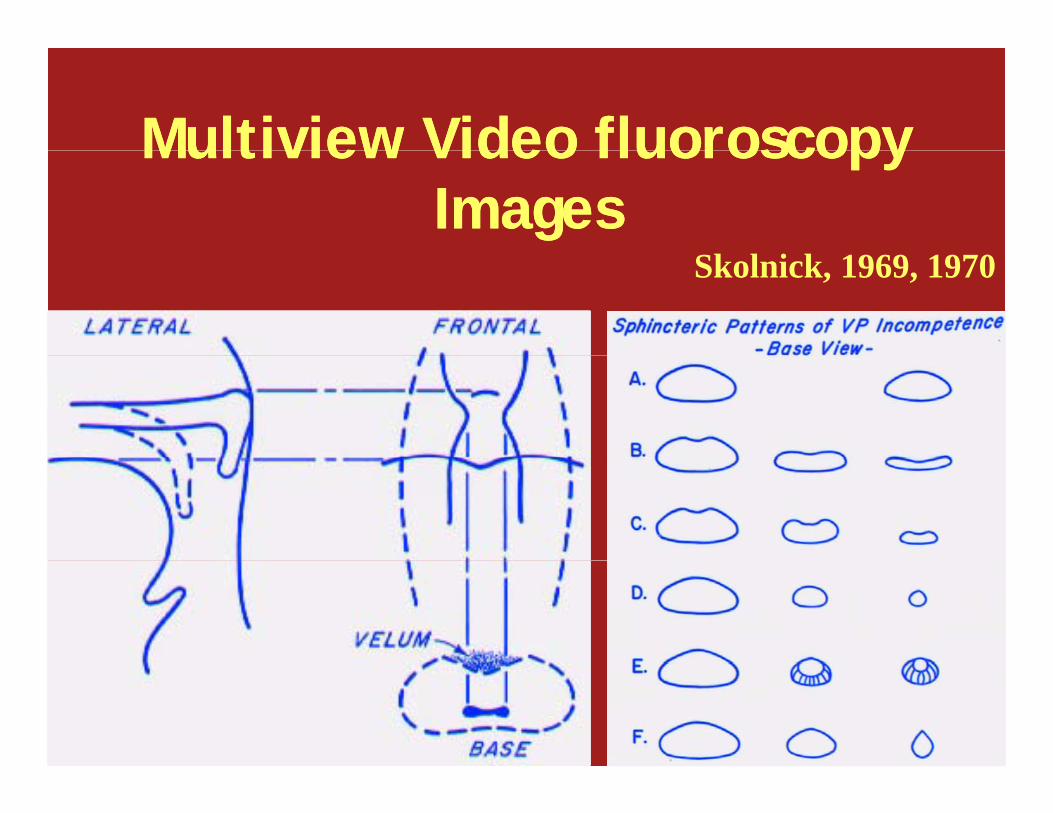
Velopharyngeal FunctionVelopharyngeal Function
Sh f VP j i Sh f VP j i • Shape of VP port just prior to closure
• Patterns not discrete
• Shape of VP port just prior to closure
• Patterns not discretePatterns not discrete• Continuum• Asymmetry
Patterns not discrete• Continuum• Asymmetry• Incomplete closure\VPI
• ResonanceE i i
• Incomplete closure\VPI• Resonance
E i i• Emission• Articulation
• Large vs small gaps
• Emission• Articulation
• Large vs small gapsg g pg g p
l h l fl h l fVelopharyngeal DysfunctionVelopharyngeal Dysfunction
• Goals - consensus• Complete correction
• Goals - consensus• Complete correction
• Problems - no consensus• Improvement vs. correction
• Problems - no consensus• Improvement vs. correctionp
• No side effects• Minimal
p• No side effects• Minimal
p• Tolerable side effects• Acceptable burden of
p• Tolerable side effects• Acceptable burden of
interventionsinterventions treatment• What works?
• Anything works for small gaps
treatment• What works?
• Anything works for small gaps• Anything works for small gaps• Anything works for small gaps
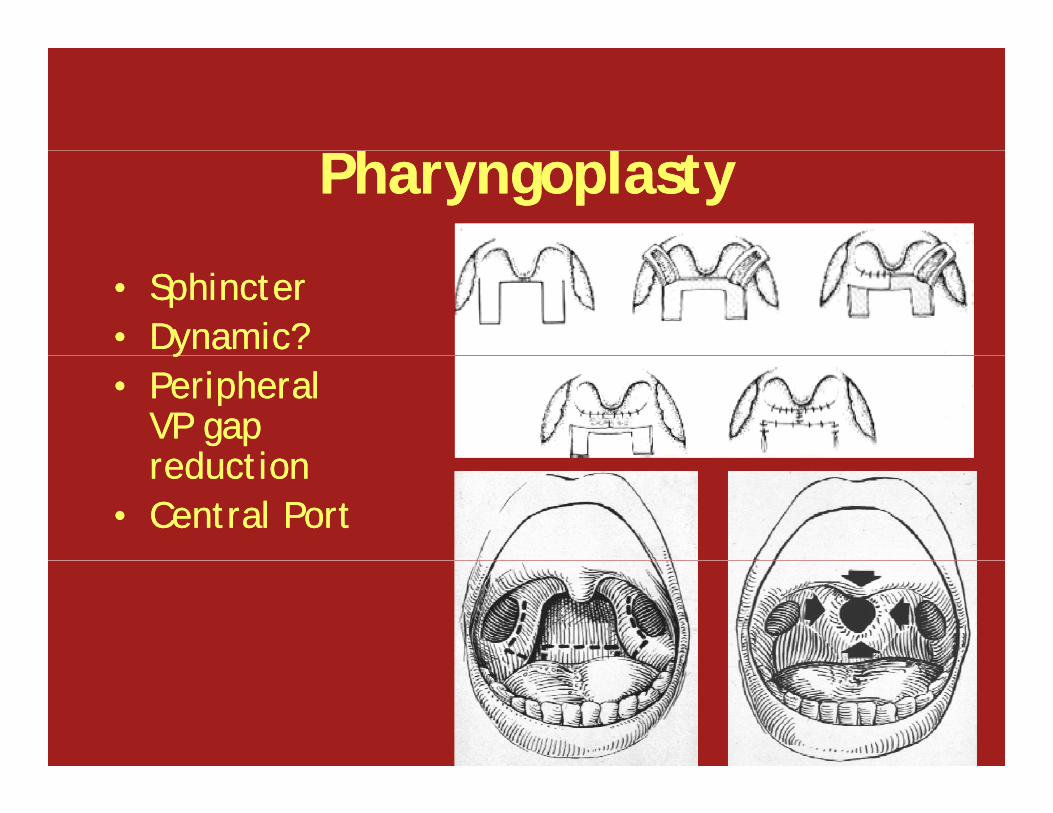
llSurgical OptionsSurgical Options
• Large gaps > 80%• Pharyngoplasty
• Large gaps > 80%• Pharyngoplasty
• Small gaps < 20%• Tonsillectomy
• Small gaps < 20%• Tonsillectomy • Pharyngoplasty
• 10%, n=300 (Shprintzen 1988)• 2.4%, n= 585 (Ysunza 1993)• 9.2%, n=219 (Valnicek 1994)• 38%, n=38 (Lesavoy et al 1996)• 3.2%, n=222 (Fraulin et al 1998)• 38%, n=38 (Lesavoy et al 1996)• 3.2%, n=222 (Fraulin et al 1998)
• OSA on follow up• 20% (2/10)- at 3 months (Orr et al 1987)
1% (3/300) t 6 th (Sh i t 1988)
• OSA on follow up• 20% (2/10)- at 3 months (Orr et al 1987)
1% (3/300) t 6 th (Sh i t 1988)• 1% (3/300) at 6 months (Shprintzen 1988)• 4% (9/219) at 3 weeks (Valnicek 1994)• 1% (3/300) at 6 months (Shprintzen 1988)• 4% (9/219) at 3 weeks (Valnicek 1994)
Potential Etiology of OSA Potential Etiology of OSA Potential Etiology of OSA with SBPF
Potential Etiology of OSA with SBPF
• Velopharyngeal obstruction
• Circumferential
• Velopharyngeal obstruction
• Circumferential Circumferential narrowing of airway• Lateral wall
advancement for
Circumferential narrowing of airway• Lateral wall
advancement for closure
• Scar contraction from second intention healing
closure• Scar contraction from
second intention healing
• Length of flap (donor site)• Larger segment of
• Length of flap (donor site)• Larger segment of g g
airway narrowing
• Palate length
g gairway narrowing
• Palate length
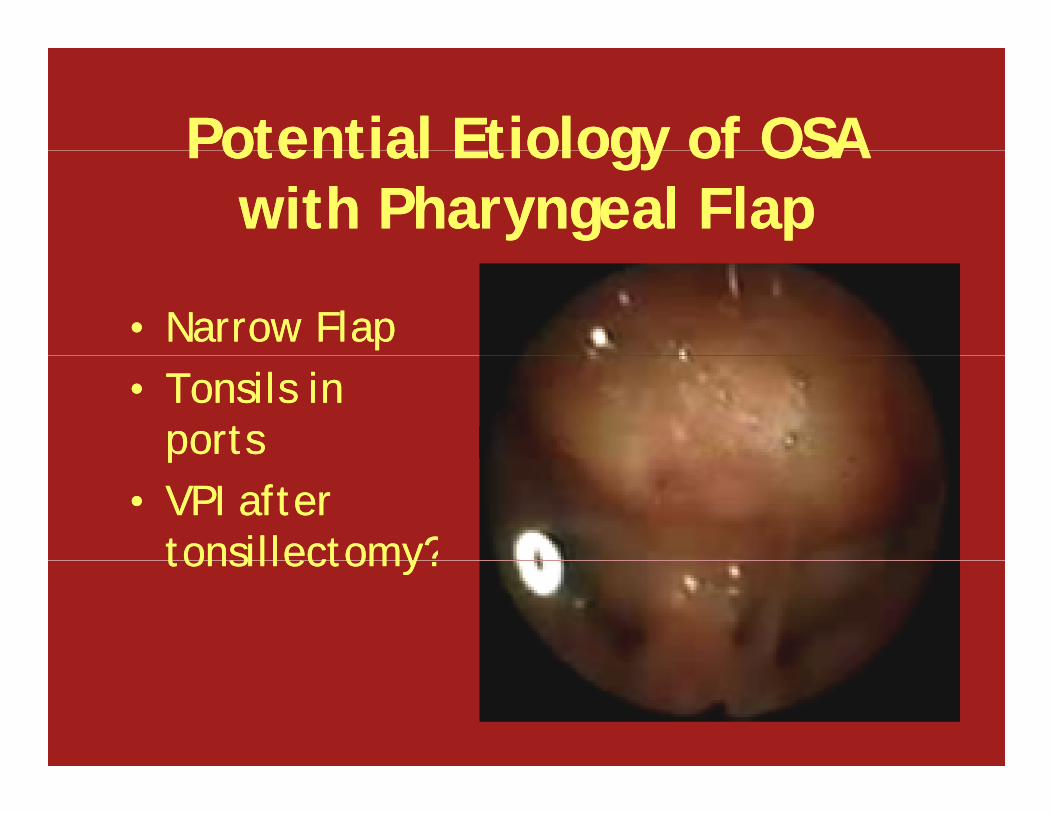
Potential Etiology of OSA Potential Etiology of OSA Potential Etiology of OSA with Pharyngeal Flap
Potential Etiology of OSA with Pharyngeal Flap
• Narrow Flap• Narrow Flap• Tonsils in
ports• Tonsils in
portsp• VPI after
tonsillectomy?
p• VPI after
tonsillectomy?tonsillectomy?tonsillectomy?
hhHypothesisHypothesis
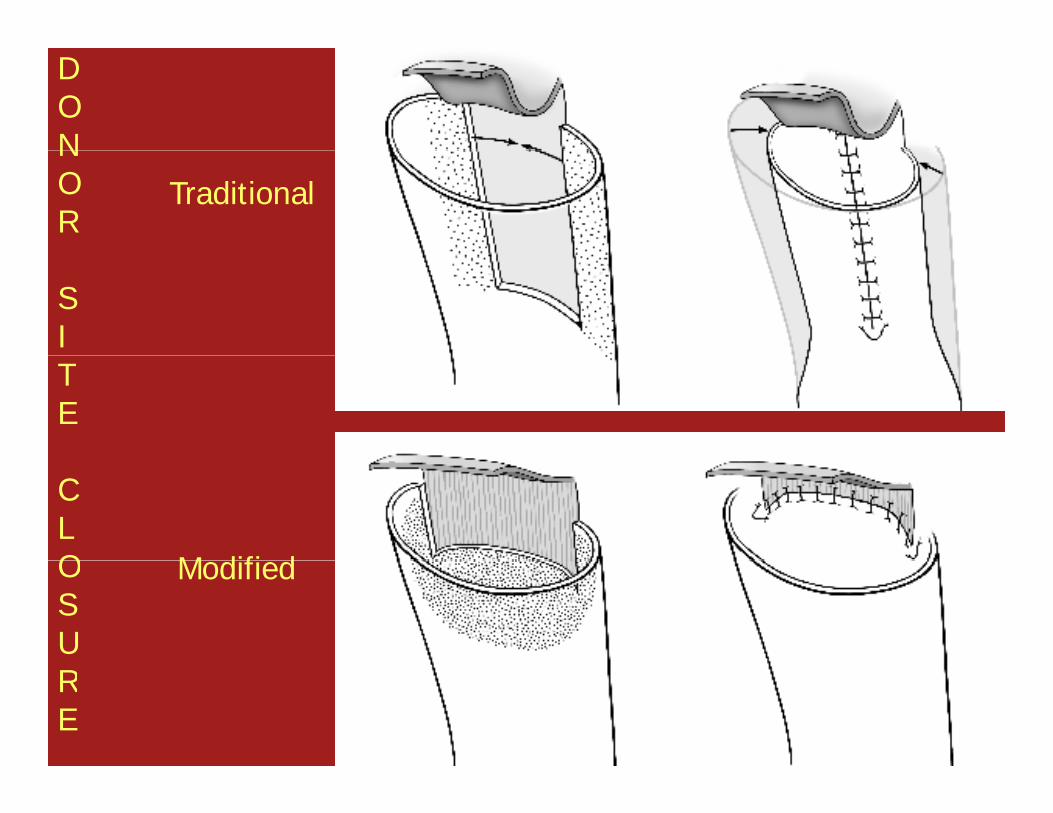
• The risk of OSA is decreased by limiting length of PF, vertical closure of donor
• The risk of OSA is decreased by limiting length of PF, vertical closure of donor g ,site, and routine adenotonsillectomy. Short flap also pulls palate posteriorly
g ,site, and routine adenotonsillectomy. Short flap also pulls palate posteriorly p p p p yand superiorly away from retrolingualspace.
p p p p yand superiorly away from retrolingualspace.pp
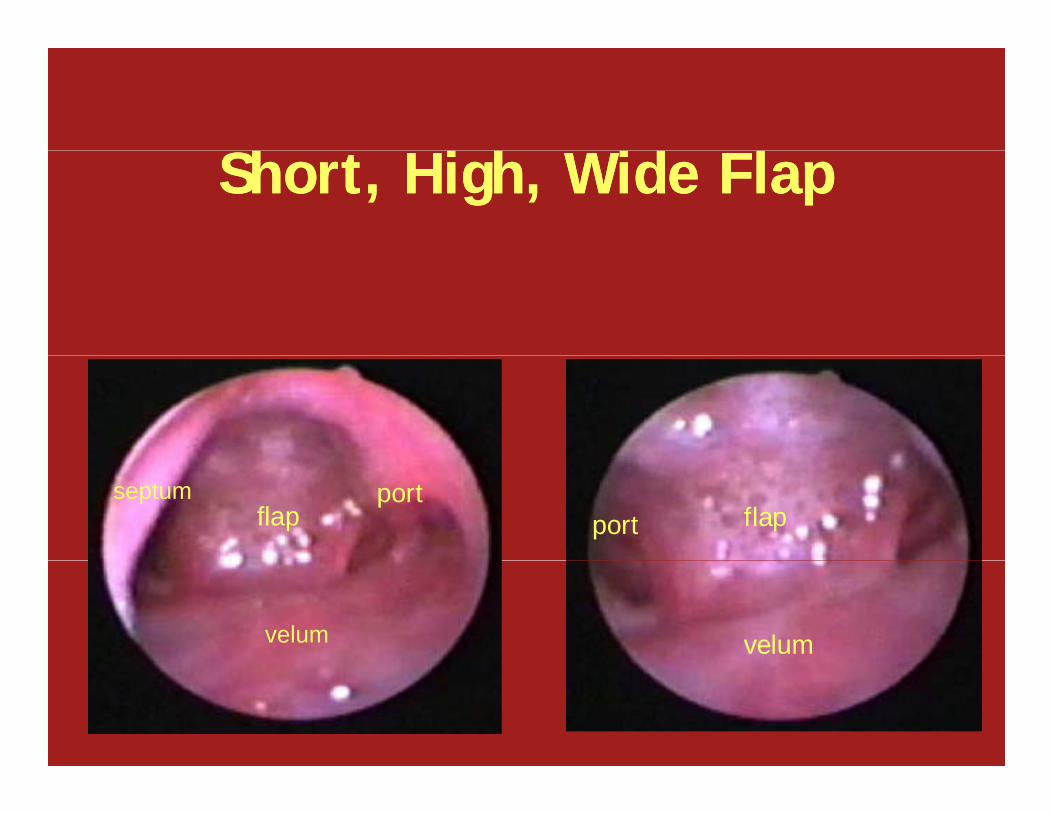
h h d lh h d lShort, High, Wide FlapShort, High, Wide Flap
• Medium 50%• Wide 75-85%• Medium 50%• Wide 75-85%• Very wide 90-95%• Asymmetry• Very wide 90-95%• Asymmetryy yy y
VPI Rating ScaleVPI Rating ScalegInternational Working Group, 1990
(Golding-Kushner et al., 1990, CPJ, 20:337-347)
gInternational Working Group, 1990
(Golding-Kushner et al., 1990, CPJ, 20:337-347)( g , , , )( g , , , )
u Based on: videofluoroscopy and nasopharyngoscopyP l t d h l ll t d
u Based on: videofluoroscopy and nasopharyngoscopyP l t d h l ll t d u Palate and pharyngeal walls are rated separately relative to each otherSt t t d l g t j t f
u Palate and pharyngeal walls are rated separately relative to each otherSt t t d l g t j t f u Structures rated along trajectory of movement at level of VP port
u Ratio scale of 0 0 to 1 0
u Structures rated along trajectory of movement at level of VP port
u Ratio scale of 0 0 to 1 0u Ratio scale of 0.0 to 1.0u Ratio scale of 0.0 to 1.0
ResultsResults• 100 pharyngeal flaps – 88 wide or very wide
3 t t OR f bl di
• 100 pharyngeal flaps – 88 wide or very wide
3 t t OR f bl di• 3 returns to OR for bleeding
• 4 surgical revisions2 f b t ti
• 3 returns to OR for bleeding
• 4 surgical revisions2 f b t ti• 2 for obstruction
• 2 for partial dehiscence
• 92 of 100 with normalization of resonance
• 2 for obstruction
• 2 for partial dehiscence
• 92 of 100 with normalization of resonance92 of 100 with normalization of resonance
• 3 with marked improvement but persistent hypernasality
92 of 100 with normalization of resonance
• 3 with marked improvement but persistent hypernasalityyp y
• 5 with moderate hyponasality
• 6 with persistent obstructive symptoms
yp y
• 5 with moderate hyponasality
• 6 with persistent obstructive symptomsp y p• negative PSGs – RDI < 5
p y p• negative PSGs – RDI < 5
SummarySummary
• Small gap VPI can be managed successfully multiple ways
• Small gap VPI can be managed successfully multiple ways
• Large gap VPI can be managed successfully with tailored wide pharyngeal flaps
• Large gap VPI can be managed successfully with tailored wide pharyngeal flaps
• Preoperative tonsillectomy and short flaps with vertical donor site closure reduce the b t ti t i t d ith id
• Preoperative tonsillectomy and short flaps with vertical donor site closure reduce the b t ti t i t d ith id obstructive symptoms associated with wide
flapsobstructive symptoms associated with wide flaps
Pharyngeal Flap Pre and PostPharyngeal Flap Pre and Post
Thank YouThank YouThank YouThank You
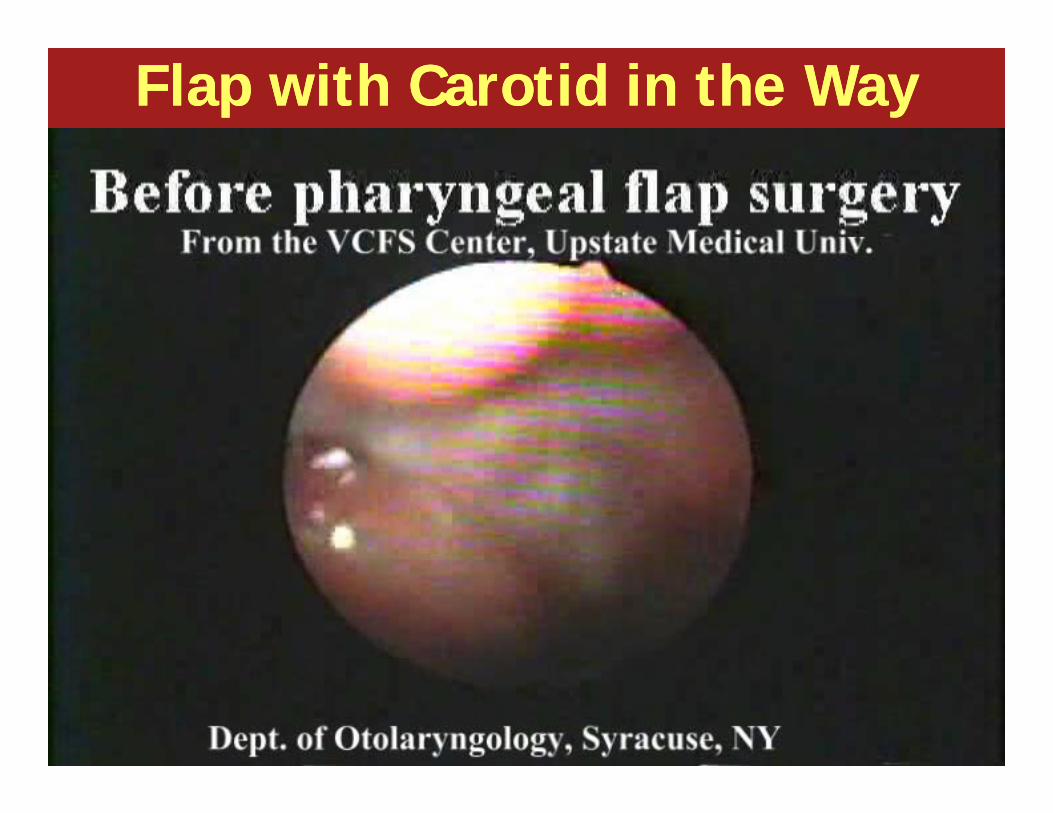
Flap with Carotid in the WayFlap with Carotid in the Way
b l l fb l l fSubmucosal CleftSubmucosal Cleft
• Result of some palate repair techniquesMi li d l
• Result of some palate repair techniquesMi li d l• Misaligned muscles• Furlow, IVV
• Short soft palate
• Misaligned muscles• Furlow, IVV
• Short soft palateShort soft palate• Furlow, push back
• Hypomobility
Short soft palate• Furlow, push back
• Hypomobility• Does palate surgery
help?• Does palate surgery
help?
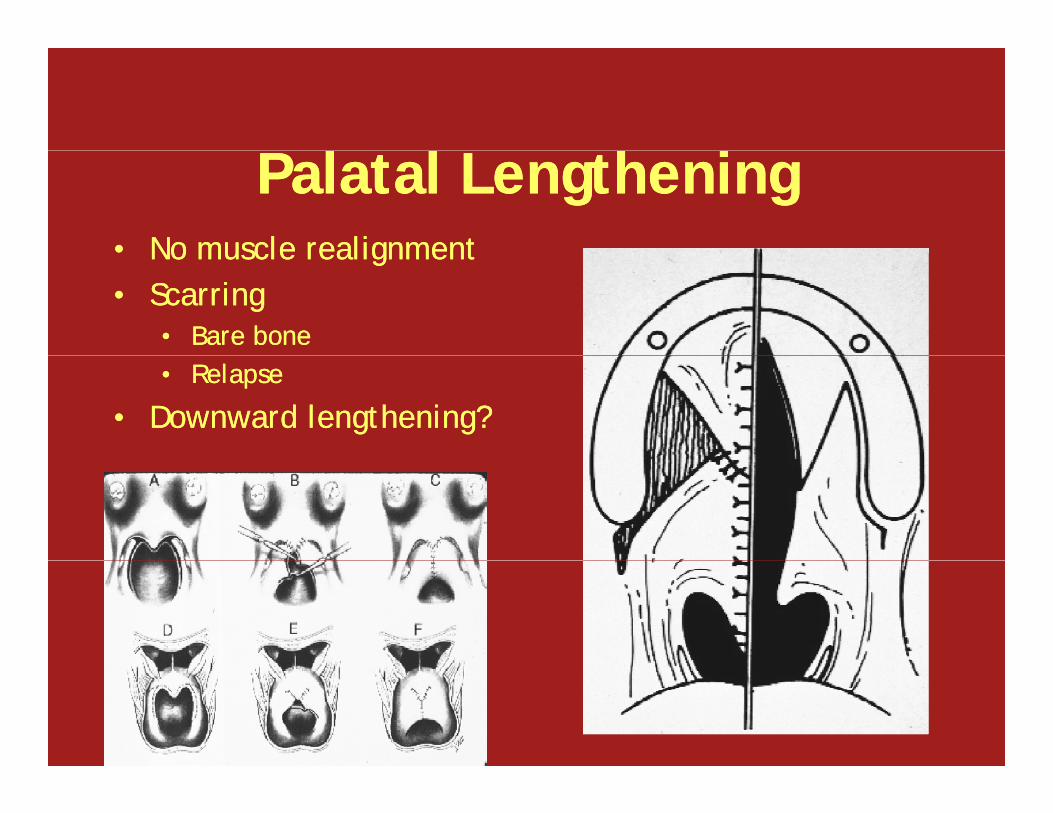
l l hl l hPalatal LengtheningPalatal Lengthening• No muscle realignment• No muscle realignmentNo muscle realignment• Scarring
• Bare bone
No muscle realignment• Scarring
• Bare bone• Relapse
• Downward lengthening?• Relapse
• Downward lengthening?
l l ll l lIntravelar VeloplastyIntravelar Veloplasty
• Realigns muscle• No added length• Realigns muscle• No added lengthg• Scarring
g• Scarring
b d hb d hCombined TechniquesCombined Techniques
• IVV – muscle realignment• V – Y pushback – palatal lengthening• IVV – muscle realignment• V – Y pushback – palatal lengtheningV Y pushback palatal lengthening• Scarring