65
| Date post: | 08-Jul-2015 |
| Category: |
Healthcare |
| Upload: | mukhtar-khan |
| View: | 284 times |
| Download: | 7 times |


Spinal Stenosis
Dr. Mukhtar
Neurosurgery
HMC

Roadmap1. Basic Anatomy
2. Classification & Description
3. Symptoms & Signs
4. Diagnostic Studies
5. Pathology mimicking stenosis
6. Associated conditions
7. Nonsurgical vs Surgical Management
8. Pre and Postop considerations
9. Minimally invasive Surgery
10. Expansive Laminoplasty
11. Open Decomp
12. Outcome
12.Surgical Techniques
13.Complications
14.Postop rehabilitation

Historical perspective


• 1803 => Portal of France postulated the cause of back & legs pain
• 1893 => Lane of England performed first laminectomy
• 1911 => Bailey & Casamajor on spinal pains & facet joint exostosis
• 1954 => Verbiest described the syndrome of lumber stenosis
• 1978 => Kirkaldy-Willis et al on pathology & pathogenesis (Three Joints Complex)

Basic Anatomy

Lumber Spine

Spinal Canal

Diameters
• AP Diameter: 15-27 mm
• Lateral Recess: 3-4 mm
• AP diameter < 12 mm is stenotic (10 mm is definite)
• Lateral Recess < 3 mm is stenotic

The Lateral Recess

Classification & Description

Aetiological Classification
• Congenital-developmental stenosis
• Idiopathic
• Achondroplastic
• Acquired stenosis
• Degenerative (most common type)
• Combined congenital and degenerative stenosis
• Spondylitic/spondylolisthetic
• Iatrogenic (i.e., postlaminectomy, postfusion)
• Posttraumatic
• Metabolic (i.e., Paget’s disease, fluorosis)

Anatomic Classification
• Central Canal Stenosis: Narrowing of the AP dimension
• Foraminal stenosis
• Lateral recess stenosis

Mechanistic Classification
• Stable: Facet & LF hypertrophy with disc degeneration
• Unstable: Stable form with spondylolisthesis &/or scoliosis

• Contributing factors:
• Thick laminae, arthrotic facets, exaggerated lordotic curvatures, infolding of hypertrophied LF, ossification of posterior longitudinal ligament (OPLL)
• Paget’s disease, acromegaly, fluorosis as well as achondroplasia
• L4-L5 is the commonest level
• L3-L4, L2-L3, L5-S1 & L1-L2 in descending order of frequency

Clinical
• Neurogenic Claudication (pseudoclaudication)• From Latin Claudico = to Limp
• Uni- or bilateral buttock, hip, thighs or leg discomfort
• Precipitated by standing or walking
• Relieved by change in erect posture
• Pain may not be the major complaint
• Paraesthesias or leg weakness with walking
• Muscle cramping, especially in the calves

• Neurogenic claudication: (moderately sensitive but highly specific)
• direct mechanical compression
• Indirect vascular insufficiency
• Lordosis increased in standing & walking, hence more pain
• Recumbence & sitting reverses lordosis, canal opens, blood flow improves, distracts the facet joints and pain is relieved
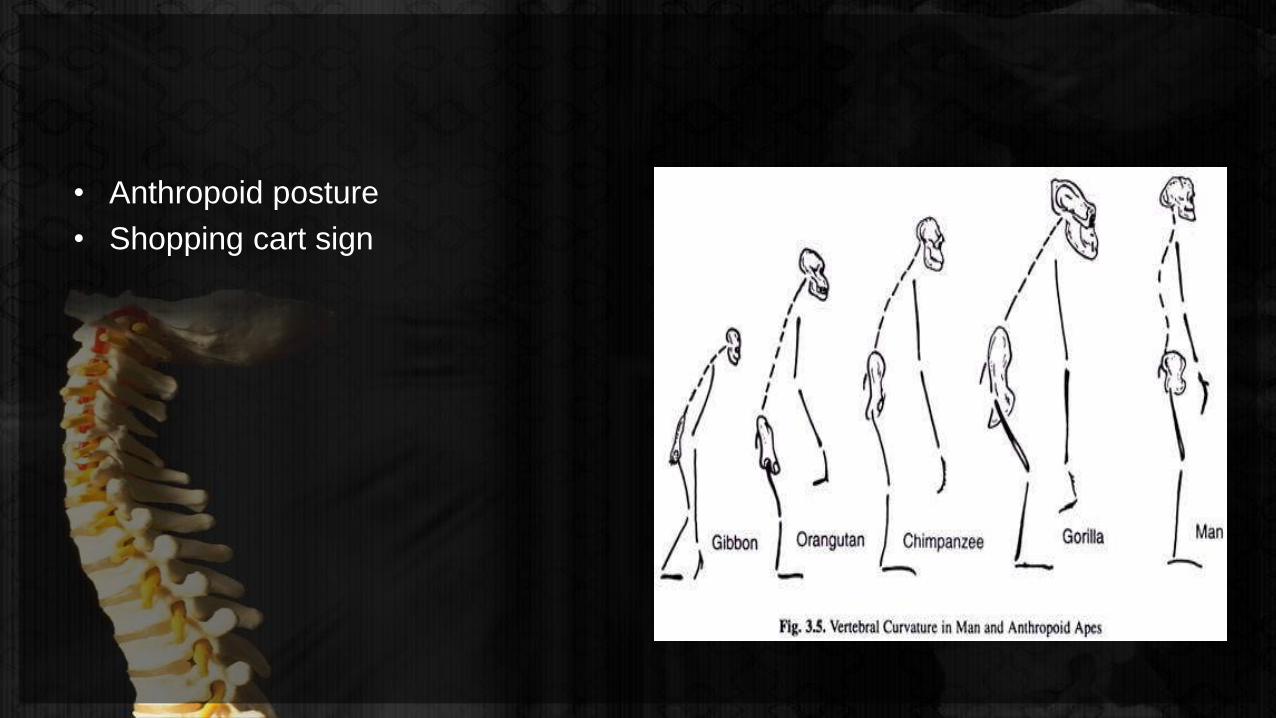
• Anthropoid posture
• Shopping cart sign

• Normal neurologic exam in 18% (normal SLR & stretch tests)
• L5, L4, L3 & S1 root syndromes
• Ankle & Knee Jerk tests
• Pain on lumber extension tests
• Bladder dysfunction• Uncommon in younger patients
• 60% elderly subjectively improved 6 months after laminectomies

Neurogenic vs Vascular ClaudicationFeature Neurogenic claudication Vascular claudication
Pain distribution Dermatomal Sclerotomal
Sensory loss Dermatomal Stocking type
Aggravating factors • Variable amount of physical activity
• Pain on standing (65%)
• Coughing (38%)
• Fixed amount of activity
• Rest pain rare
• Pain on standing (27%)
Relief with rest • Slow (> 30 min)
• Special posture
Immediate
No special posture
Claudication distance Variable day to day (62%) Constant (88%)
Lifting or bending Pain common (67%) Uncommon (15%)
Limb elevation No pallor Profound
Pulses Normal Absent or decreased
Skin temperature Normal Decreased

Differentials
• Vascular insufficiency
• Hip disease
• Disc herniation
• Baastrup’s syndrome
• Arachnoiditis
• Spinal tumour
• Diabetic neuritis
• Delayed onset muscle soreness (DOMS)
• Functional aetiologies

Diagnostic studies

Plain radiography
• Bony abnormalities
• Number of vertebrae
• Curvatures
• Olisthesis & instability• > 4 mm translation
• 10 – 12 degrees angulation
Normal AP Diameters on Lateral Film
Average 22 – 25 mm
Lower normal 15 mm
Severe stenosis < 11 mm
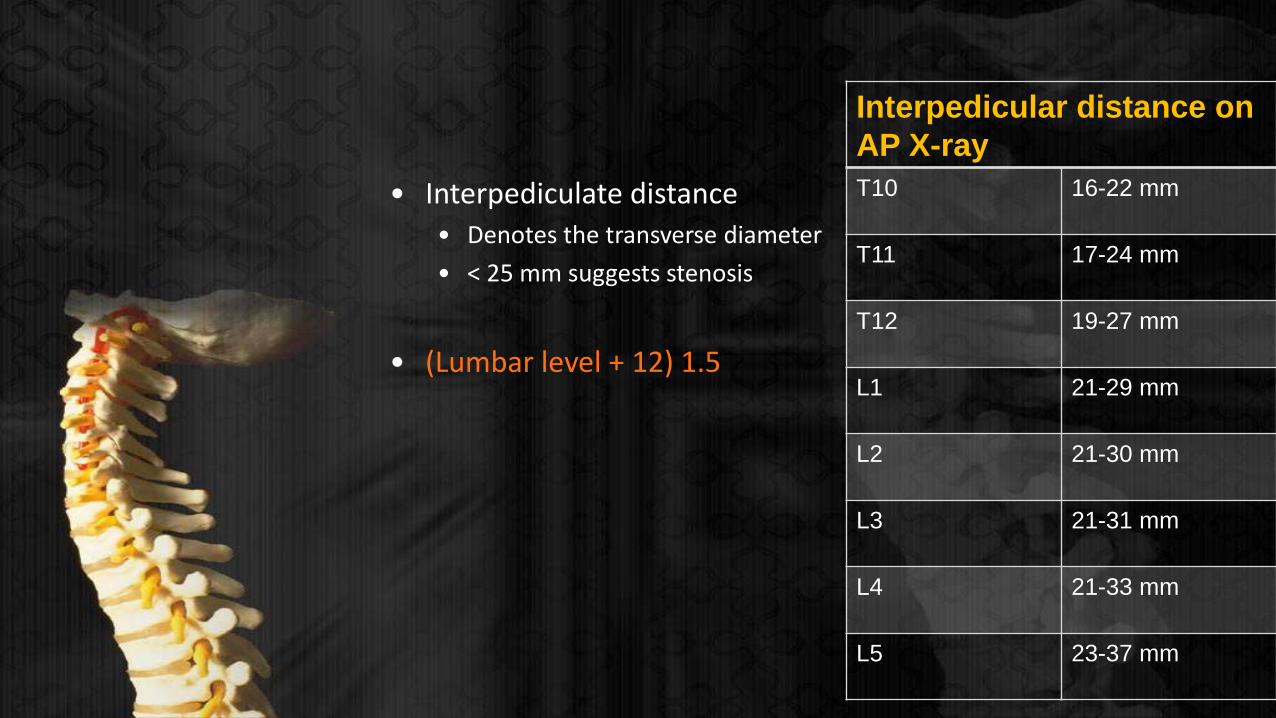
• Interpediculate distance• Denotes the transverse diameter
• < 25 mm suggests stenosis
• (Lumbar level + 12) 1.5
Interpedicular distance on
AP X-ray
T10 16-22 mm
T11 17-24 mm
T12 19-27 mm
L1 21-29 mm
L2 21-30 mm
L3 21-31 mm
L4 21-33 mm
L5 23-37 mm

CT scan
• Canal morphology
• Diameters
• Ligaments
• Facet joints
• Annulus
• Disc
• Hairline fractures & pseudoarthroses
Normal measurements on CT
AP ≥ 11.5 mm
Interpedicular Distance ≥ 16 mm
Canal cross-sectional area ≥ 1.45 cm2
Ligamentum flavum
thickness≤ 4- 5 mm
Lateral recess height ≥ 3 mm
MRI
• Best soft tissues assessment but NOT bone
• Neural structures impingement
• Ligamentous morphology & Disc assessment
• Multidimensional views without bony pathology details
• Facet joints fluid volume assessment• width of fluid in both facet joints divided by sum of the width of both facets
• Increased facet fluid indicates instability
• Contrast MRI differentiates scar from disc
• Thoracolumbar junction, differentiation of tumour, demyelination, arachnoiditis & infective spondylitis
• 1/3rd of asymptomatic pathology revealed on routine MRIs
Pathology mimicking stenosis
• Tumours located proximally contributing to lumbar complaints• Ependymomas, neurofibromas, meningioma, mets
• Thoracic disc herniation, Scheuermann’s disease, Paget’s disease, hip arthritis
• Amyloid crystal deposition in ligamentum flavum
• Diabetic peripheral neuropathy in diabetics
• Femoral amyotrophy or angiopathy
• Diabetics exhibited only 39% good or excellent outcome as compared to 95% for those without diabetes
• Peripheral vascular disease may present alone or in the presence of stenosis

Associated conditions

• Tandem stenosis:• 10% of patients with lumbar stenosis
• Surgery is dictated by the severity of stenosis
• Relative vs absolute stenosis
• Radiculopathy vs Myelopathy
• Elderly (> 65 y) need stringent search for proximal stenosis before surgery

1) Ossification of the Yellow Ligament (Ligamentum Flavum)
2) Ossification of the Posterior Longitudinal Ligament (10%)
3) Ankylosing Hyperostosis
4) Disk Herniation with and without Olisthesis
5) Limbus Vertebral Fracture
6) Far Lateral Disk Pathology
7) Synovial Cysts
8) Degenerative Spondylolisthesis
Nonsurgical versus surgical management

• Role of the multidisciplinary pain management teams
• Severe comorbidities or preference for conservative treatment
• Several studies have shown similar outcome in surgical vs medically treated groups
• Other studies have shown improved outcome for surgical intervention (63% vs 25%)

Preop vs postop considerations

• Medical & psychological comorbidities negatively impact postop outcome
• Comorbid factors:• Cardiac
• Older patient population more prevalent with cardiac comorbids
• Preop psychiatric clearance
• Significant effect of depression on postop outcome
• Up to 20% found depressed preoperatively
• Non-depressed patients good overall outcome

• Preoperative Bathing
• Twice a day with soap & water (during a week before surgery)
• Chlorhexidine-impregnated sponges a night before & morning of surgery
• Prophylactic antibiotics
• Reported incidence of infection = 3% to 12%
• Comparable infection rates in multiple vs single dose antibiotics regimens (1.15% vs 1.49%)
• Ideal prophylactic antibiotic = second generation cephalosporin within 15-30 min of incision
• Gentamicin 80 mg preoperatively confers protection against MRSA
• Irrigation with bacitracin & polymyxin B every 15 min
• These measures reduce perop culture positivity from 64% to 4%

• Silver-Impregnated Dressings
• Inhibit proinflammatory cytokines, upregulates zinc metabolism, increasing epithelialisation
• Postoperatively, a silver-impregnated dressing should be applied to the wound
• Effective against MRSA, Pseudomonas, VRE
• Coexisting Cervical Disease
• Careful handling/positioning/intubation of the patient
• Sensory or Motor evoked potentials
• Prophylaxis for DVT & PE
• Careful risk assessment for DVT & PE
• DVT risk is at 43%
• Low dose heparin may cause epidural haematomas (0.7%)
• Compression stockings reduce incidence of DVT to 2%
• Compression stockings are a recommendation (Intraop & postop)

Surgical options

• Surgical options1. laminectomy: posterior (direct) decompression of central canal and neural
foramina without or with fusion.
• Expansive laminaplasty
• Laminotomy
• Bilateral laminotomy (fenestration)
• Coronal hemilaminectomy
Fusion options:
a. posterolateral fusion ± pedicle screw/rod fixation
b. interbody fusion: generally not done as a “stand-alone”
i. posterior lumbar interbody fusion (PLIF)
ii. transforaminal lumbar interbody fusion (TLIF)
2. Procedures to increase disc space height and thereby indirectly decompress neural foramina without direct decompression
a) anterior lumbar interbody fusion (ALIF): through laparotomy
b) lateral lumbar interbody fusion: some techniques trademarked as extreme lateral interbody fusion (XLIF™) or direct-lateral (DLIF™)
c) axial lumbar interbody fusion (Ax-LIF): L5-S1 only
3. Limitation of extension by interspinous spacer: e.g. X-Stop®

Choosing the right procedure

1. Indirect Decomp (lateral interbody fusion)a. When foraminal stenosis is dominant
b. Previous spine surgery
2. Direct Decomp (Laminectomy)
a. Pinpoint central canal stenosis
b. When major compression is due to focal, correctable lesion
3. Motion preservation surgery
a. When adjacent level shows degenerative changes

4. Need for a fusion (in addition to decomp):a. Spondylolisthesis
b. Dynamic instability on flexion/extension x-rays
c. Potential spinal destabilisation after surgery
d. Recurrent surgery at the same level (≥ 3rd times)

Techniques

Laminectomy/Laminotomy
• Position: Prone or in some cases lateral decubitus
• Surgical unroofing
• Spines, lamina, ligamentum flavum
• Assess foraminal stenosis
• Foraminotomies if narrowing present
• Undercutting of superior articular facet is usually necessary
• Nearby moderate stenoses warrant concomitant decompression
• Laminotomies or fenestrations in case of adjacent lateral recess stenosis


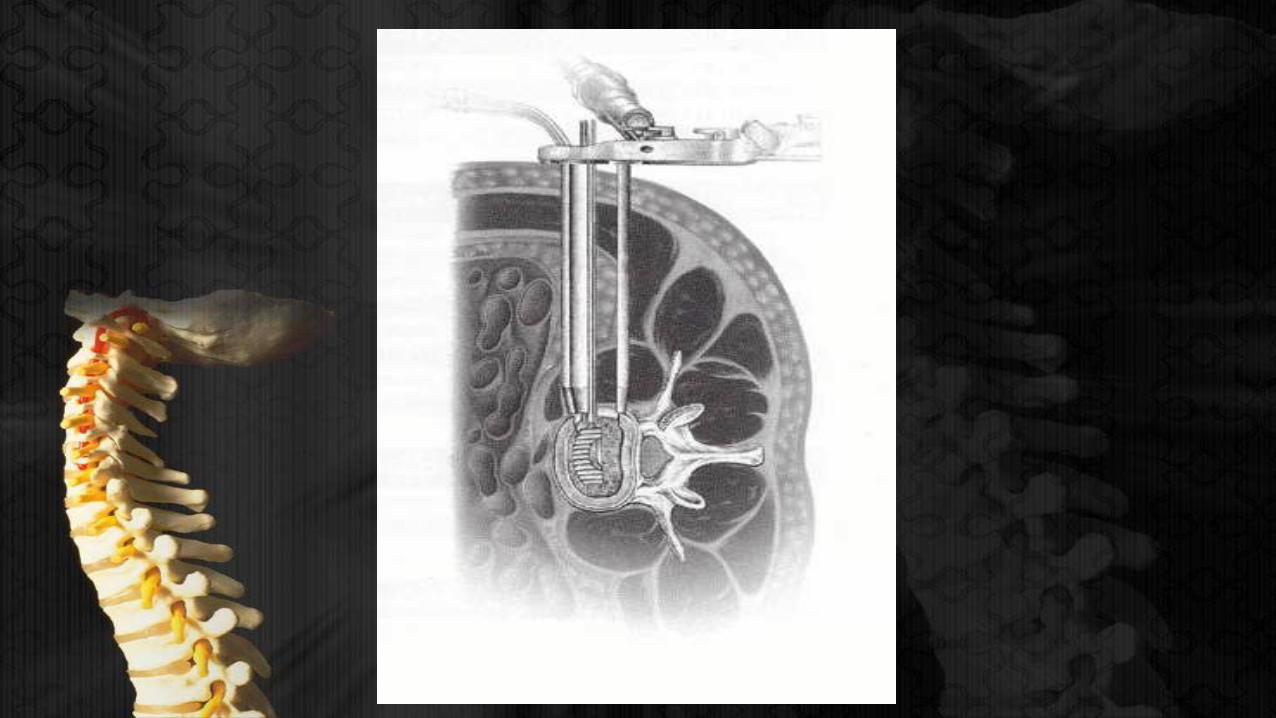
MISS decomp
• ‘mini-open’ technique with 1” incision• Bilateral laminotomies or
• Bilateral decomp via unilateral laminotomy
• 3.5 to 4 cm off the midline
• Laminectomies & facet takedown
• Open ligamentum flavum to visualise plane under the bone
• Ligamentum flavum left intact while drilling
• Contralateral drilling followed by ligamentum flavum removal
• Foraminotomies if required
• Pedicle screws placed through the open side and percutaneously contralaterally

Interspinous process decomp/stabilisation/fusion
• Interspinous spacers (X-Stop)
• Interspinous plates (Aspen, Affix, Spire)
• Spacers prevent narrowing of neural foramina & off load facet joints in extension
• Plates clamp across two spinous processes to fixate them, limiting extension
• Success rate of X-stop = 63% at 2 years
• Stability & strength similar to pedicle screws


Contraindications to spacers/plates
• Spondylolisthesis > Grade
• Scoliosis with Cobb angle ≥ 25⁰
• Cauda equina syndrome
• Spinous process fracture
• Bilateral pars defects
• Osteoporosis (hip T-score on Dexa < -2.5)


Outcome

• Poor outcome in:• Females
• Those involved in litigation or compensation cases
• Those with previous failed surgeries
• Those with new sensory deficits postoperatively
• Poor prognostic factors:• Diabetes, prior hip surgery, osteoporosis or preop spine fracture

• Morbidity/mortality• In-hospital mortality = 0.32%
• Unintended durotomy (0.32% to 13%)
• Deep infection (5.9%)
• Superficial infection (2.3%)
• DVT (2.8%)
• Damage to cauda equina
• Non-union (Risk factors)• Smoking
• Levels
• NSAIDs use (Ketorolac)
• Success of operation• No RCT comparing conservative to surgical treatment exist
• Improvement in patients with a postural component (96% good outcome)
• More improvement in legs pain than back pain
• Relapse of symptoms
• 30% to restenosis at the operated level
• 30% to stenosis at new level
• 75% responds to redo surgery
• Early failure of pain relief
• Erroneous patient selection
• Technical failure (not decompressing the foramina in presence of stenosis)
• Missed diagnoses
• Long term outcome
• Good to excellent outcome after surgery with a mean of 64%
• 37% much improved & 29% somewhat improved
• 78% to 88% success rate at 6 weeks to 6 months and 70% at 1 year and 5 years
• Success rates slightly lower for lateral recess syndrome

Conclusion
• Spinal stenosis is a predominantly surgical disorder
• Surgery has good to excellent outcome in those who have been properly selected
• Comorbids, psychiatric illness and redo surgeries carry risk of poor or no response in terms of pain relief
• Endoscopic facetectomy has been evaluated with documented good results
thanks



![Spinal Stenosis [Autosaved]powerpoints007.s3.amazonaws.com/Spinal Stenosis [Autosaved].pdf · Causes of Spinal Stenosis: Chiropractic Care can: •arthritis -Reverse Arthritis •Herniated](https://static.documents.pub/doc/80x56/5edc014dad6a402d66667bdb/spinal-stenosis-autosavedpowerpoints007s3-stenosis-autosavedpdf-causes.jpg)













