Sports Tumors Sports Tumors Robert M. Tamurian, MD Robert M. Tamurian, MD Northern California Northern California Orthopaedic Centers Orthopaedic Centers Director of Orthopaedic Director of Orthopaedic Oncology Oncology Mercy San Juan Hospital Mercy San Juan Hospital Catholic Healthcare West Catholic Healthcare West
Transcript
Sports TumorsSports TumorsRobert M. Tamurian, MDRobert M. Tamurian, MD
Northern California Orthopaedic Northern California Orthopaedic CentersCenters
Director of Orthopaedic Director of Orthopaedic Oncology Oncology
Mercy San Juan HospitalMercy San Juan HospitalCatholic Healthcare WestCatholic Healthcare West
Disclosure InformationDisclosure Information
No financial relationships to disclose. No financial relationships to disclose.
Sports TumorsSports Tumors 667 knee tumors were reviewed and 3.7% were 667 knee tumors were reviewed and 3.7% were
treated with an intra-articular procedure due to treated with an intra-articular procedure due to misdiagnosis as an athletic injurymisdiagnosis as an athletic injury
11 patients had benign tumors, while 14 patients 11 patients had benign tumors, while 14 patients had malignant tumorshad malignant tumors
15/25 (60%) patients had their oncologic procedure 15/25 (60%) patients had their oncologic procedure altered as a result of prior intra-articular interventionaltered as a result of prior intra-articular intervention
6/14 (43%) patients with malignant tumors required 6/14 (43%) patients with malignant tumors required amputation vs. limb salvage as a result of prior amputation vs. limb salvage as a result of prior invasive procedureinvasive procedure
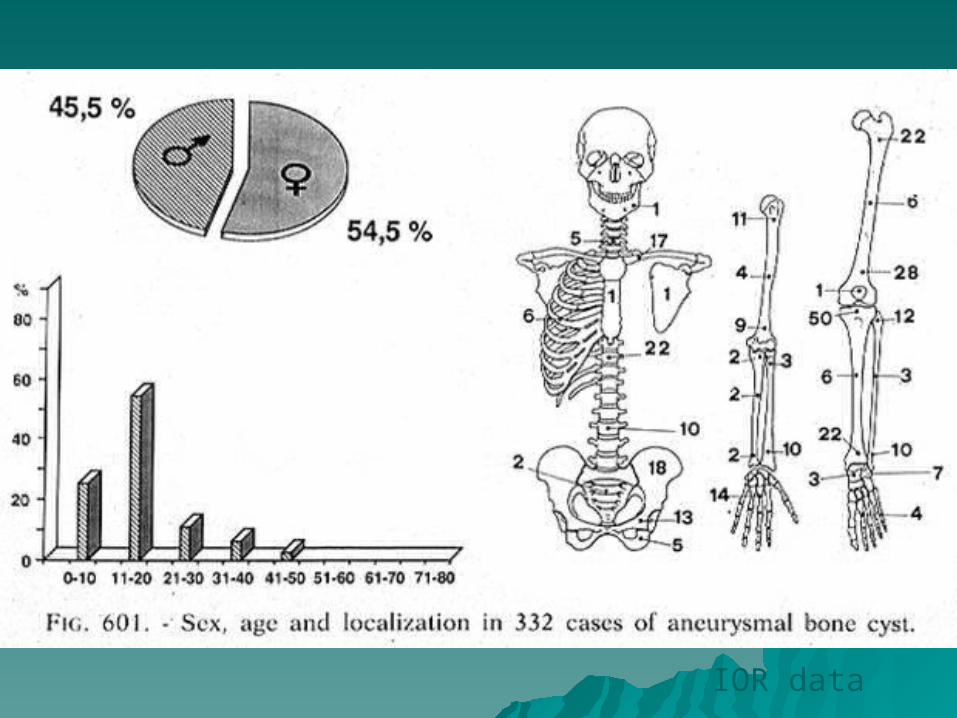
Tumors About the Knee Misdiagnosed as Athletic InjuriesTumors About the Knee Misdiagnosed as Athletic Injuries
D. Luis Muscolo, Miguel A. Ayerza, Arturo Makino, Matías Costa-Paz and Luis A. Aponte-Tinao D. Luis Muscolo, Miguel A. Ayerza, Arturo Makino, Matías Costa-Paz and Luis A. Aponte-Tinao J Bone Joint Surg Am. J Bone Joint Surg Am. 2003;85:1209-1214.2003;85:1209-1214.
Bone TumorsBone TumorsMimicking Intra-articular pathologyMimicking Intra-articular pathology
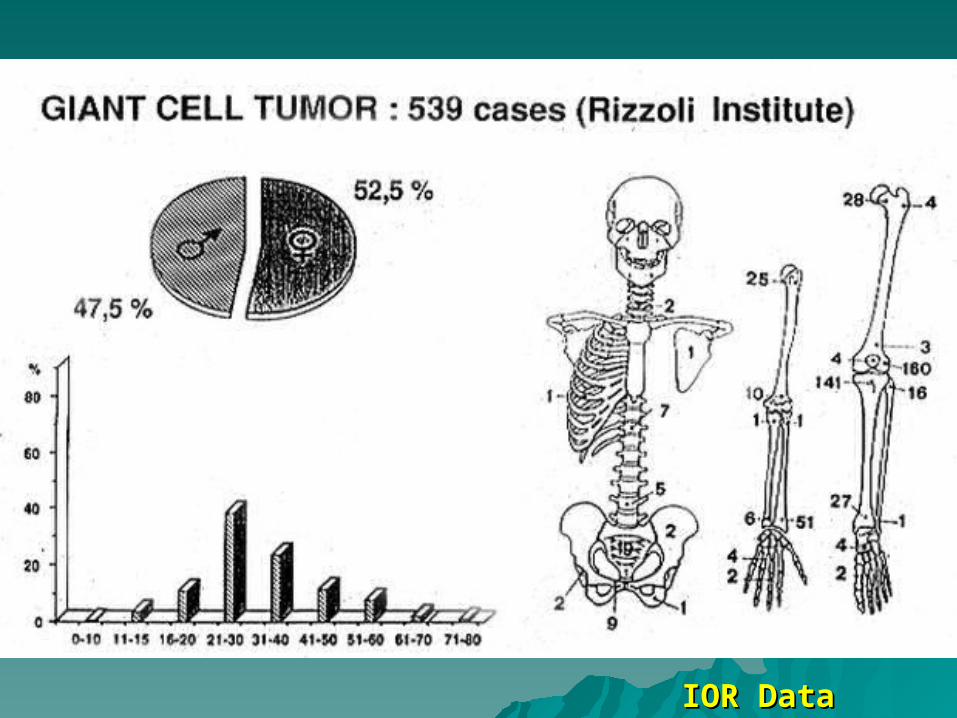
BenignBenign– Aneurysmal Bone CystAneurysmal Bone Cyst– Giant Cell TumorGiant Cell Tumor– ChondroblastomaChondroblastoma– Osteoid OsteomaOsteoid Osteoma– OsteoblastomaOsteoblastoma
thin rim of reactive thin rim of reactive bonebone
Soft tissue massSoft tissue mass Mimic primary Mimic primary
malignant bone malignant bone tumortumor
Aneurysmal Bone CystAneurysmal Bone CystStaging StudiesStaging Studies
Focal increased isotope uptake, often Focal increased isotope uptake, often with with ““doughnutdoughnut”” configuration. configuration.
CT - Fluid-fluid level - fine CT - Fluid-fluid level - fine discontinuities in reactive rim - discontinuities in reactive rim - hypervascular lining with contrast.hypervascular lining with contrast.
T2 - intensely bright signalT2 - intensely bright signal
Aneurysmal Bone CystAneurysmal Bone Cyst ExampleExample CaseCase
A 22 y/o presented with knee pain. A 22 y/o presented with knee pain. Radio-graphs revealed a Radio-graphs revealed a radiolucent lesion in the patella. radiolucent lesion in the patella. Treated for patello-femoral Treated for patello-femoral syndrome. Two years later the syndrome. Two years later the pain increased.pain increased.
Campanacci et al, Chir. Organi. Mov. Suppl. 1990. Curettage of Campanacci et al, Chir. Organi. Mov. Suppl. 1990. Curettage of GCT of bone. Reconstruction with subchondral grafts and cement.GCT of bone. Reconstruction with subchondral grafts and cement.
Perssen. CORR 1976.Perssen. CORR 1976.
ChondroblastomaChondroblastoma
ChondroblastomaChondroblastomaClinical featuresClinical features
Occurs in secondary ossification Occurs in secondary ossification centers (centers (proximal humerusproximal humerus common)common)
Rarely in apophyseal location, Rarely in apophyseal location, pelvis, talus, patellapelvis, talus, patella
Age: skeletally immatureAge: skeletally immatureUsually stage 2, some stage 3Usually stage 2, some stage 3
ChondroblastomaChondroblastomaRadiographic featuresRadiographic features
Site : Intra-cortical, long bonesSite : Intra-cortical, long bones Posterior elements Posterior elements
vertebratevertebrate
Osteoid OsteomaOsteoid OsteomaNatural HistoryNatural History
Painful active lesion, exacerbated by Painful active lesion, exacerbated by alcohol, virtually complete resolution alcohol, virtually complete resolution of pain with aspirin or NSAIDS .of pain with aspirin or NSAIDS .
Does not enlarge, seldom exceeds 1 Does not enlarge, seldom exceeds 1 cm.cm.
Spontaneously heals in 3 - 5 yrs.Spontaneously heals in 3 - 5 yrs.
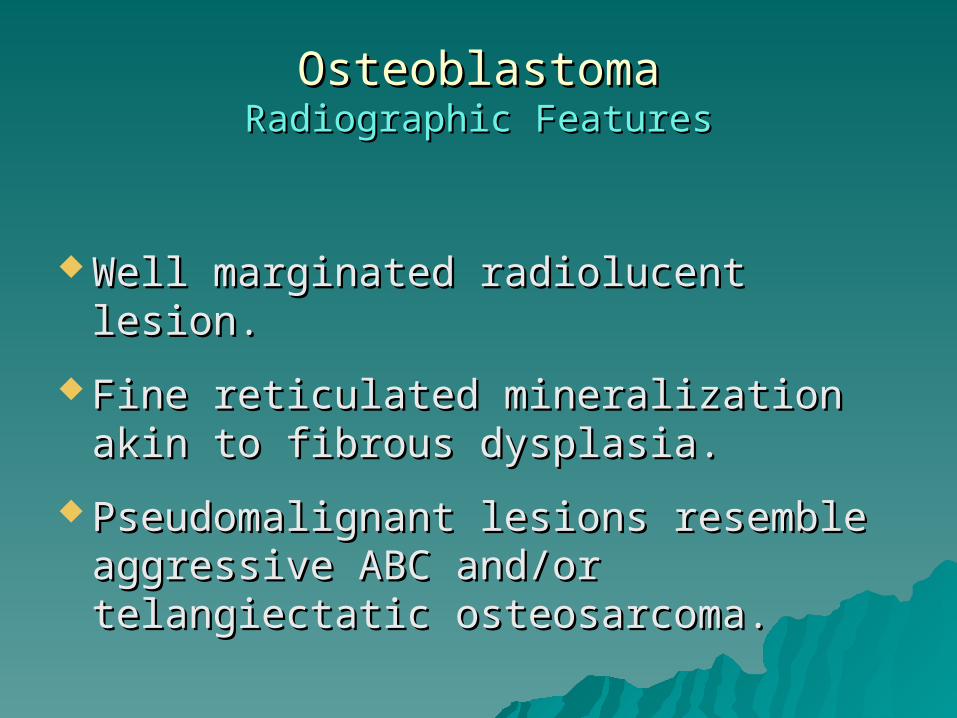
Osteoid OsteomaOsteoid OsteomaRadiographic FeaturesRadiographic Features
Small oval or round radiolucent Small oval or round radiolucent nidus.nidus.
Heavy mantle of reactive bone - Heavy mantle of reactive bone - often obscures nidus.often obscures nidus.
Reaction often enlarges diameter of Reaction often enlarges diameter of the bone.the bone.
Osteoid OsteomaOsteoid OsteomaUnusual Radiographic FeaturesUnusual Radiographic Features
Cancellous location often has less Cancellous location often has less reactive bone.reactive bone.
Medullary lesion often Medullary lesion often radiographically invisible.radiographically invisible.
A 31 y/o marathon runner presented A 31 y/o marathon runner presented with symptoms of internal derangement with symptoms of internal derangement of the knee. X-rays of the knee. X-rays ““normal.normal.”” Arthroscopic Arthroscopic ““shavingshaving”” x2 without relief. x2 without relief. Chest X-ray and laboratory values WNL.Chest X-ray and laboratory values WNL.
Bone TumorsBone TumorsMimicking Intra-articular pathologyMimicking Intra-articular pathology
BenignBenign– Aneurysmal Bone CystAneurysmal Bone Cyst– Giant Cell TumorGiant Cell Tumor– ChondroblastomaChondroblastoma– Osteoid OsteomaOsteoid Osteoma– OsteoblastomaOsteoblastoma
ChondrosarcomaChondrosarcomaNatural HistoryNatural History
Stage I - slow growth, heavily Stage I - slow growth, heavily mineralized,long interval to mineralized,long interval to metastasis, often secondary, metastasis, often secondary, excellent DFSexcellent DFS
Stage II - Rapid growth, lightly Stage II - Rapid growth, lightly mineralized early metastases, mineralized early metastases, usually primary, limited DFSusually primary, limited DFS
ChondrosarcomaChondrosarcomaRadiographic FeaturesRadiographic Features
Intralesionalmatrix mineralization often Intralesionalmatrix mineralization often described as rings and arcs, or popcorn described as rings and arcs, or popcorn calcificationcalcification
Stage I - Heavily mineralized, usually Stage I - Heavily mineralized, usually surface, usually secondary, well surface, usually secondary, well
marginatedmarginated
Stage II - Lightly mineralized, usually Stage II - Lightly mineralized, usually central, usually primary, central, usually primary,
Plain RadiographsPlain Radiographs– Scalloping unreliableScalloping unreliable– Look for cortical thickening and / or destruction, periosteal reaction, soft tissue Look for cortical thickening and / or destruction, periosteal reaction, soft tissue
massmass
MRI MRI – Stage I - Low intensity heterogeneous signalStage I - Low intensity heterogeneous signal – Stage II - High intensity homogenous signalStage II - High intensity homogenous signal
Isotope ScanIsotope Scan– Stage I - moderate focal uptake Stage I - moderate focal uptake – Stage II - intense diffuse Stage II - intense diffuse
uptakeuptake
CT CT – Stage I - Heavily calcified with Stage I - Heavily calcified with ““popcornpopcorn”” pattern pattern – Stage II - Radiolucent with punctate calcificationStage II - Radiolucent with punctate calcification
*Neither enhance with contrast*Neither enhance with contrast
Chondrosarcoma Case ExampleChondrosarcoma Case Example
64 y.o. Real Estate Magnate64 y.o. Real Estate Magnate
2 years of hip pain2 years of hip pain
Radiographs show DJD with Radiographs show DJD with juxtarticular cystjuxtarticular cyst
Initial TreatementInitial Treatement
To the OR for To the OR for curretage bone, curretage bone, graft, and Total graft, and Total Hip ArthroplastyHip Arthroplasty
Post-Op FilmPost-Op Film
Diagnosed with internal Diagnosed with internal derangementderangement
Underwent arthroscopic surgery with Underwent arthroscopic surgery with tricompartmental debridement and tricompartmental debridement and a protracted post-operative course a protracted post-operative course
without improvement.without improvement.
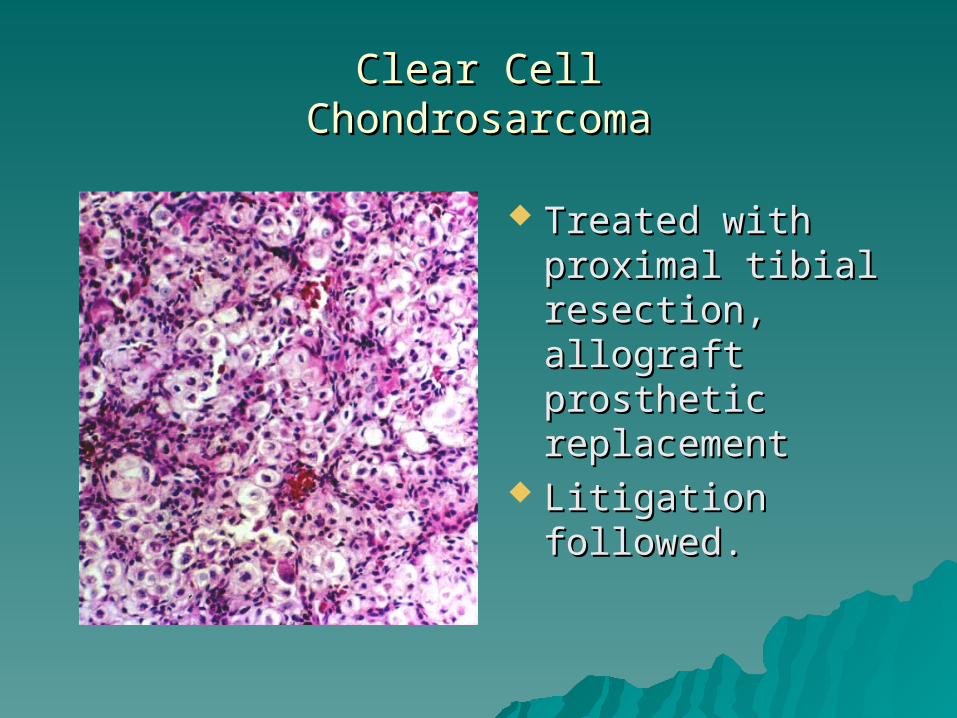
Clear CellClear CellChondrosarcomaChondrosarcoma
Treated with Treated with proximal tibial proximal tibial resection, allograft resection, allograft prosthetic prosthetic replacementreplacement
Litigation followed.Litigation followed.
OsteosarcomaOsteosarcoma
OsteosarcomaOsteosarcomaDemographicsDemographics
Age : 15 - 30Age : 15 - 30
Sex : M > FSex : M > F
Site : Metaphyses of large long bonesSite : Metaphyses of large long bones
OsteosarcomaOsteosarcomaRadiographic FeaturesRadiographic Features
Intense extended uptake of isotopeIntense extended uptake of isotope
CT - Random non-stressed pattern of ossificationCT - Random non-stressed pattern of ossification Enhances with contrast Enhances with contrast
MRI: T-1 - low intensity signal. Best chance of identifying MRI: T-1 - low intensity signal. Best chance of identifying ““skipsskips””
– T-2 - Bright heterogeneous signalT-2 - Bright heterogeneous signal
Case ExampleCase Example12 year old with 12 year old with
knee pain.knee pain.Avid soccer player.Avid soccer player.
PrinciplesPrinciples Consider neoplasia in the differential diagnosis of painConsider neoplasia in the differential diagnosis of pain
ImagingImaging is indicated prior to surgical intervention is indicated prior to surgical intervention
ListenListen to patients, therapists and family members regarding post injury and post to patients, therapists and family members regarding post injury and post surgical improvementsurgical improvement
Patients that do not follow the expected clinical course should undergo further Patients that do not follow the expected clinical course should undergo further imagingimaging– RadiographsRadiographs– Bone scansBone scans– MRIMRI
PresentationPresentation
If you would like to receive the full If you would like to receive the full powerpoint presentation that powerpoint presentation that includes pictures, please email the includes pictures, please email the CME Coordinator at CME Coordinator at [email protected]@McLeodHealth.org. .