26
SpR topic: Constipation Michelle Fleming SpR teaching 21 st May 2014
| Date post: | 24-Dec-2015 |
| Category: |
Documents |
| Upload: | rebecca-daniela-booth |
| View: | 226 times |
| Download: | 0 times |

SpR topic: ConstipationMichelle Fleming
SpR teaching21st May 2014

1. Prevalence2. Contributors3. NICE clinical knowledge summary4. Summary tables/doses5. Cochrane review6. Methlynaltrexone7. Latest RCT8. Summary
Focus
Constipation is one of the most common symptoms experienced by patients with advanced progressive illness
The prevalence is estimated at 30 90% depending on the population studied1,2
1 Clark K, Urban K, Currow DC. Current approaches to diagnosing and managing constipation in advanced cancer and palliative care. Journal of palliative medicine. 2010 Apr;13(4):473-6
2 Clark K, Smith JM, Currow DC. The prevalence of bowel problems reported in a palliative care population. Journal of pain and symptom management. 2012 Jun;43(6):993-1000
Prevalence

In palliative medicine it is the 3rd most commonly encountered symptom after pain and anorexia3
Common factors that increase the constipation include hospitalisation, illness and the use of opioids4
More problematic in advanced disease5
3Potter J, et al. Symptoms in 400 patients referred to palliative care services: prevalence and patterns. Palliative medicine. 2003;17:310-4
4Larkin PJ et al. The management of constipation in palliative care: clinical practice recommendations. Palliative medicine. 2008;22:796-807
5Fallon MT et al. Morphine, constipation and performance status in advanced cancer patients. Palliative medicine. 1999;13:159-60
Prevalence
How should I treat constipation? Where possible, alleviate contributing
factors (for example, inadequate diet, dehydration, having to use a bedpan, lack of privacy, anal fissure, painful haemorrhoids, or local tumour)
Treat any faecal loading or impaction
6 NICE Clinical Knowledge Summaries. Palliative cancer care : Constipation. April 2013
NICE April 20136
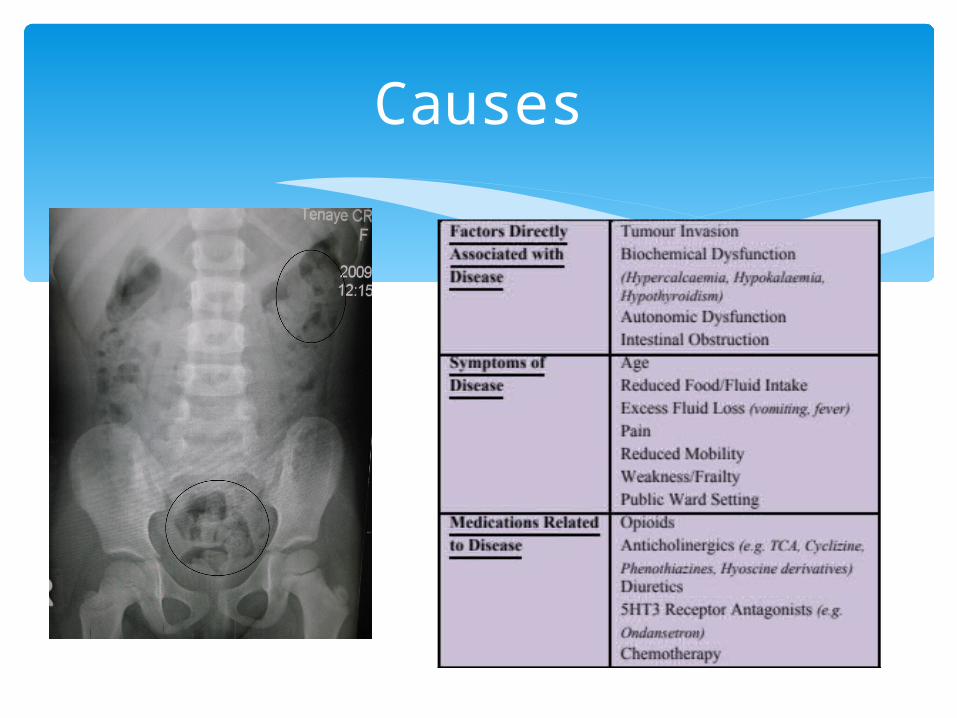
Causes

Start treatment with a stimulant laxative (such as senna)
Titrate the dose of laxative in order to achieve comfortable defecation without colic. For instance, senna may be titrated up to a maximum dosage of 2–4 tablets (15–30 mg) three times a day
Pharmacological treatment
6 NICE Clinical Knowledge Summaries. Palliative cancer care : Constipation. April 2013

If the person finds it difficult to take the required number of tablets, reduce the dose of senna (for example to 15 mg at night) and add in a softener such as docusate (also a weak stimulant)
Increase the dose of laxative in line with any increase in dose of opioid
Step 2
6 NICE Clinical Knowledge Summaries. Palliative cancer care : Constipation. April 2013
Add an osmotic laxative (such as lactulose or a macrogol) or a surface-wetting laxative (such as docusate, which also softens stools) if colic is a problem.
Adjust the dose of softener to produce a comfortable stool (comfort is more important than the frequency or number of stools)
In a palliative care situation, higher and more frequent doses than specified by the product licence may be needed.
Step 3
6 NICE Clinical Knowledge Summaries. Palliative cancer care : Constipation. April 2013
Avoid: Phosphate enemas (if possible) as they can
sometimes cause water and electrolyte disturbances, especially in people aged 65 years or older, and when co-morbidities are present
Bulk-forming laxatives (e.g. bran, ispaghula), especially in opioid-induced constipation
Paraffin6 NICE Clinical Knowledge Summaries. Palliative cancer care : Constipation. April 2013
Avoid

Do not carry out rectal interventions (such as enemas, suppositories, or manual evacuation) in people:
On chemotherapy, who may be neutropenic (white blood cell count < 0.5 x 109/ L) and therefore at risk of serious infection
With thrombocytopenia (platelet count < 20 x 109/ L), who are at risk of bleeding
With rectal or anal disease
6 NICE Clinical Knowledge Summaries. Palliative cancer care : Constipation. April 2013
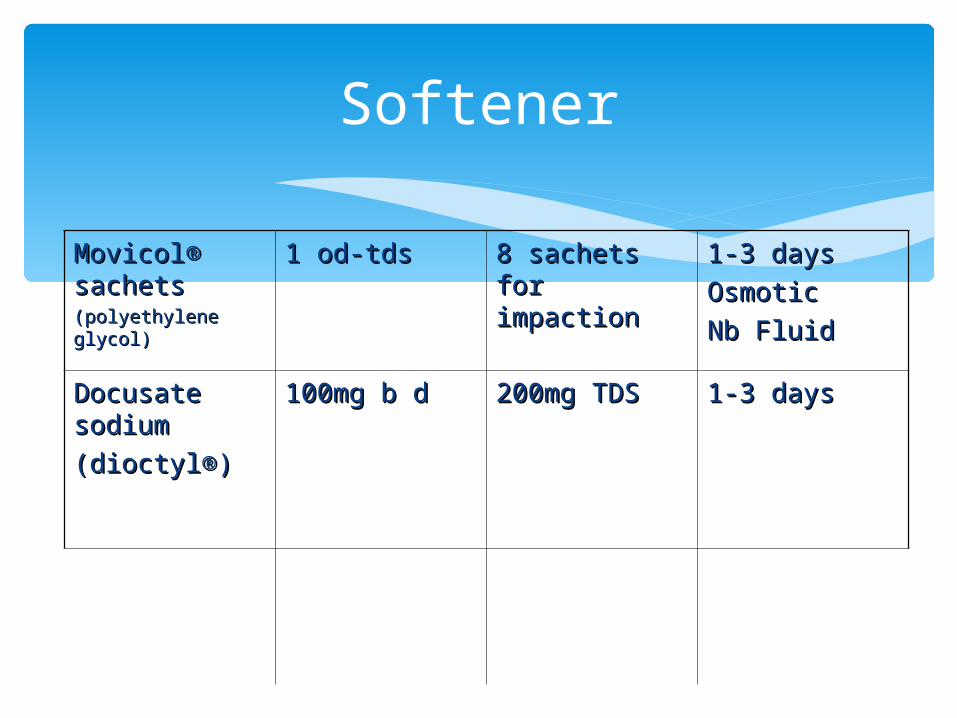
MovicolMovicol®® sachetssachets(polyethylene (polyethylene glycol)glycol)
1 od-tds1 od-tds 8 sachets for 8 sachets for impactionimpaction
1-3 days1-3 days
OsmoticOsmotic
Nb FluidNb Fluid
Docusate Docusate sodiumsodium
(dioctyl(dioctyl®®))
100mg b d100mg b d 200mg TDS200mg TDS 1-3 days1-3 days
Softener

SennaSenna
(Senokot(Senokot®)®)
15mg 15mg (2 (2 tabs/liquid tabs/liquid nocte)nocte)
Max 3 TDSMax 3 TDS 8-12 hrs8-12 hrs
BisacodylBisacodyl
(Dulcolax(Dulcolax®)®)
5mg nocte5mg nocte 20mg20mg 8-12 hrs8-12 hrs
Stimulant
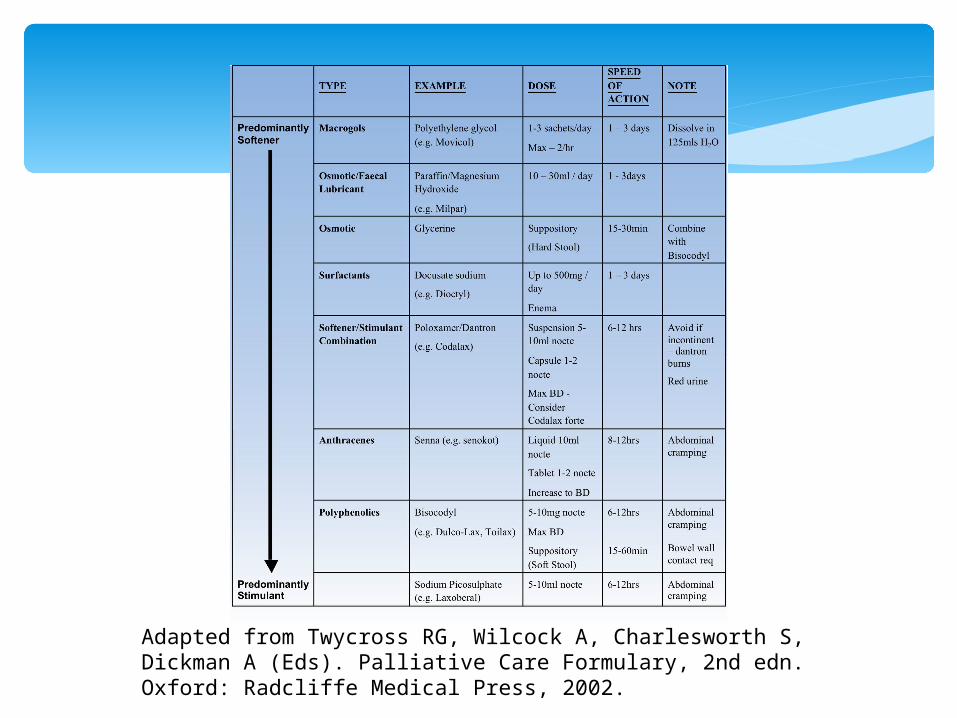
Adapted from Twycross RG, Wilcock A, Charlesworth S, Dickman A (Eds). Palliative Care Formulary, 2nd edn. Oxford: Radcliffe Medical Press, 2002.
If the response to laxatives is insufficient, consider adding in a prokinetic agent such as metoclopramide, domperidone, or erythromycin 250–500 mg four times a day (off-label use). Do not use a pro-kinetic if the person has symptoms of colic
Adjuvants
6 NICE Clinical Knowledge Summaries. Palliative cancer care : Constipation. April 2013
If the person is terminally ill and has not had an adequate response despite these measures, consider the use of a dantron-containing laxative
Seek specialist advice if constipation still persists despite these measures
Combination
6 NICE Clinical Knowledge Summaries. Palliative cancer care : Constipation. April 2013
Combination
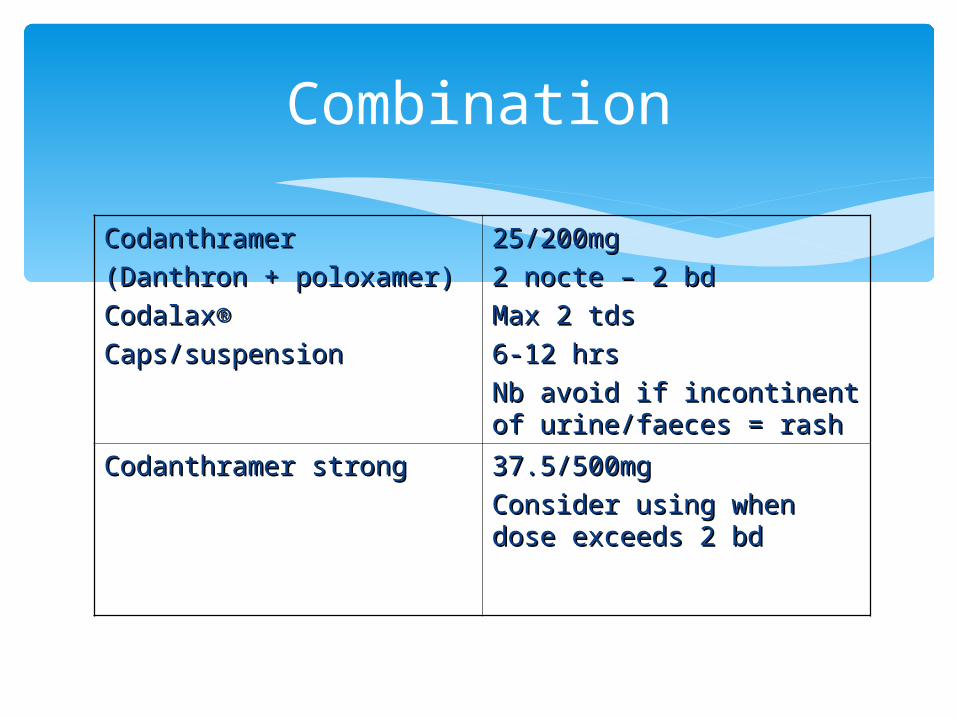
Codanthramer Codanthramer
(Danthron + poloxamer)(Danthron + poloxamer)
CodalaxCodalax®®
Caps/suspensionCaps/suspension
25/200mg25/200mg
2 nocte – 2 bd2 nocte – 2 bd
Max 2 tdsMax 2 tds
6-12 hrs6-12 hrs
Nb avoid if incontinent of Nb avoid if incontinent of urine/faeces = rashurine/faeces = rash
Codanthramer strongCodanthramer strong 37.5/500mg37.5/500mg
Consider using when dose Consider using when dose exceeds 2 bdexceeds 2 bd
Peripheral opioid receptor antagonist
Oxycodone/Naloxone (Targin®) Targeting peripheral receptors whilst
sparing central analgesic function through combining oxycodone with naloxone has emerged as a promising approach
3 x Phase III RTC in non-cancer pain 1 x Phase II RTC in cancer pain

Methylnatrexone
Two studies7,8
287 participants Compared SC methylnaltrexone with placebo Methylnaltrexone was found to be more effective than
placebo at inducing a laxation response, and this response was rapid (four to 24 hours)
However, an undisclosed proportion of participants continued to take conventional laxatives during these trials
7Thomas J, Karver S, Cooney GA. et al. Methylnaltrexone for treatment of opioid-induced constipation in advanced
illness patients. N Engl J Ned 2008;358:2332-23438Slatkin N, Thomas J, Lipman AG, Wilson G, Boatwright ML, Wellman C, et al. Methylnaltrexone for treatment of opioid-
induced constipation in advanced illness patients. Journal of Supportive Oncology 2009;7:39-46

Evidence
The evidence for the efficacy and safety of laxatives in palliative care is very limited
Evidence
A Cochrane systematic review that addressed the use of laxatives for the management of constipation in palliative care found seven studies (n = 616 in total) suitable for inclusion [Candy et al, 2011]9
9 Candy B, Jones L, Goodman ML, Drake R, Tookman A. Laxatives or methylnaltrexone for the management of constipation in palliative care patients. Cochrane Database Syst Rev 2011; 1:CD003448.
Summary
Lactulose, senna, danthron combined with poloxamer, misrakasneham and magnesium hydroxide combined with liquid paraffin
There is some evidence that methylnaltrexone is effective (in comparison with a placebo) at inducing laxation (bowel relaxation) in patients taking opioids who have not had a good response to conventional laxatives
The evidence in the other studies was more limited due to lack of overlap in laxatives evaluated
Further rigorous, independent trials with longer follow up are needed to evaluate the effectiveness of laxatives, including methylnaltrexone
A randomized, double-blind, placebo-controlled trial (n = 74) compared the use of docusate plus senna (n = 35) with placebo plus senna (n = 39) in adults in a hospice setting over 10 days [Tarumi et al, 2013]10.
There was no significant benefit of docusate plus senna compared with placebo plus senna in the primary outcome measures, which were: stool frequency, volume, consistency
Since cochrane
Malignant/non-malignant Placebo group had mean daily morphine dose 66%
higher than docusate group Dose of senna varied substantially compared with
constant dose of docusate
Tarumi et al, 2013
10Tarumi, Y., Wilson, M.P., Szafran, O. and Spooner, G.R. (2013) Randomized, double-blind, placebo-controlled trial of oral docusate in the management of constipation in hospice patients. Journal of Pain and Symptom Management 45(1), 2-13.
Constipation should be anticipated Bowel regimen initiated with the commencement of opioid In the management of constipation, the combination of a
softener and stimulant laxative is generally recommended The current evidence is too limited to provide evidence-
based recommendations for the choice of laxative and selection should be made on an individual basis
The use of opioid receptor antagonists should be restricted to those patients who treatment is resistant to conventional laxative therapy
CEBM level 5/Recommendation D
Summary

Thank youThank you

















