1068 the root of the lung, a common male round worm was cut across; its tail end lay in the main bronchus, whence it extended downwards in the posterior part of the lung in successively smaller tubes to its head end, which filled the tube in which it lay. This small bronchus was roughened and eroded; higher up the walls were merely congested. The worm was alive, 4 in. long, and paler in colour than three other large female ones found in the stomach and duodenum. The posterior border of the upper lobe showed hypostatic congestion ; the rest of the lung was crepitant. Civil Hospital, Aden. ADDITIONAL NOTE ON THE FUMES OF BROMIDE OF AMMONIUM. BY THEODORE MAXWELL, M.D., B.Sc. SINCE writing the note on the Inhalation of Bromide of Ammonium Fumes, published in THE LANCET of May 10th, I have tried a plan for the production of hydrobromic acid which was suggested to me by Messrs. Burgoyne, Barbidges, and Co.-viz., the addition of fused chloride of calcium to the solution of hydrobromic acid triple the Pharmacopoeial strength, and am glad to say it works very well in a Verreker’s chloride of ammonium inhaler. Woolwich. A Mirror OF HOSPITAL PRACTICE, BRITISH AND FOREIGN. ST. THOMAS’S HOSPITAL. A CASE OF PORRO-CÆSAREAN SECTION IN A RACHITIC DWARF; SUCCESSFUL RESULT BOTH TO MOTHER AND CHILD; REMARKS. (Under the care of Dr. CULLINGWORTH.) Nulla autem est alia pro certo noscendi via, nisi quamplurimas et mor- borem et dissectionum historias, tum aliorum tum proprias collectas habere, et inter se compa.ra.re.—MOR&AGNI De Sed. et CaUB. Morb., lib. iv. Procemium. - WE publish this week the notes of a case of Porro- Csesarean operation, to which we have already alluded in our columns,! and at the performance of which we were present. Undertaken atter a full consideration of the bearings of the case, it is a good example of the modern operation as performed with the object of saving both mother and child, and we would direct the attention of our readers to the remarks by Dr. Cullingworth on the case also to the table which is appended to his remarks. It was the intention of the operator to perform the Caesarean operation after the method which is known as Sanger’s; but the intractable nature of the haemorrhage prevented him from leaving the uterus when sutured. We published the notes of a successful Porro’s operation by Dr. W. Duncan at the Middlesex Hospital in our first issue of last year.2 In that case the patient was also extremely rachitic, and the result satisfactory. Mary C-, aged twenty-five, a rachitic dwarf, married, was admitted into St. Thomas’s Hospital Feb. 24th, 1890, with a view to Caesarean section. She was then in the ninth month of her third pregnancy. Her previous history was as follows :-The catamenia commenced at fourteen, recurring regularly every four weeks. The flow usually lasted three days, was habitually scanty, and accom- panied with severe abdominal pain. She had been married two years. Her first confinement took place at full term on Dec. 17th, 1887. She was on that occasion attended at her own home in connexion with the St. Thomas’s Hospital Maternity, and delivered by cranio- tomy. She made a good recovery. She again became pregnant in May, 1888, and, on presenting herself a little 1 THE LANCET, March 22nd. 2 Ibid., vol. i., p. 16. later for a maternity ticket, she was directed to see Dr, Cullingworth. After hearing her history and carefully examining her he advised her to seek admission to the York- road Lying-in Hospita.1 for the purpose of having labour induced at the seventh month. She took his advice, and on Dec. 18th, 1888, at 3.15 P M., a bougie was introduced into the uterus. At 4 P M. the same day the liquor amnii began to escape, but labour pains did not come on until3p.M. on Dec. 20th. The child presented by the breech, which re- mained stationary at the pelvic brim for five hours. The pulse having then risen to 120, chloroform was administered, and extraction effected by hooking a finger into the groin. The arms were extended, the head passed without difficulty. The child, a female, was born at 9.45 P.M. The placenta was expressed. The amount of blood lost was twelve fluid ounces. A hot douche was administered ; a draught con- taining a fluid drachm of the liquid extract of ergot was given. The uterus contracted fairly well, and the patient made a good recovery. Her temperature taken during labour was 992°, after labour 101 6°. During the fortnight following delivery the temperature was usually under 100°, and only once exceeded 100’4°, the exception occurring on the tenth day, when the thermometer on one occasion registered 101 ’4°. The child weighed 3 Ib. 7 oz., and was apparently stillborn. Artificial respira- tion was practised and continued for an hour, at the end of which time feeble efforts at respiration were made. Breathing never, however, became fully established, and cardiac pulsation finally ceased an hour and a half after delivery. The patient became pregnant for the third time at the latter part of June, 1889. Dr. Cullingworth had an interview with her soon afterwards, and strongly advised her to submit to Caesarean section at or near the full term. She willingly consented to this, and attended the out-patient department regularly throughout the remainder of her pregnancy. On Feb. 24th, 1890, she was ad- mitted into Adelaide ward, when the following notes were taken of her condition :-" The patient has fair hair, blue eyes, and is of a cheerful and placid disposition. Her height is 3 ft. 9 in. The femora and tibiee are thickened, with anterior curve. On the left side there is marked genu valgum, the patella is dislocated outwards, and there.is a projec- tion in front of the tibia two inches below the knee-joint. The teeth are mostly in a state of decay. The general health is good. The urine is free from albumen, and there are no pres- sure symptoms. The measure- ments are : Distance between the iliac spines, 9t in.; between the iliac crests, 9 in. ; external con- jugate, 6 in. ; diagonal conju- gate, 38 in. (The actual conjugate had been ascertained on the occa- sion of her last labour to be 2 in.) The uterine walls are thin; the child’s head being in the left iliac fossa, the back is directed forwards ; the breech lies at the fundus, and to the right. The sounds of the fcetal heart are heard most distinctly ac the level of the umbilicus, an inch and a quarter to the left. A sense of resistance, thought to be probably due to the presence of the placenta, is felt at the upper part of the uterus, commencing about two inches to the left of the middle line, and extending outwards to the left lateral wall. The greatest girth of the abdomen is 32 in., the distance from umbilicus to ensiform cartilage 71 in., and from umbilicus to pubes 7 in. The patient last menstruated on June 14th, 1889." On March 13th, the patient having been prepared by the administration of an aperient the previous day, followed by an enema in the morning, the operation was performed at 2 P.. in one of the large operating theatres of the hospital. Labour had not commenced, nor had any means been adopted to Pxcite it. Ether was administered by Mr. E. F. White. Mr. A. N. Boycott, resident accoucheur, and Mr. Forde,
Transcript
1068
the root of the lung, a common male round worm was cutacross; its tail end lay in the main bronchus, whence itextended downwards in the posterior part of the lung insuccessively smaller tubes to its head end, which filledthe tube in which it lay. This small bronchus wasroughened and eroded; higher up the walls were
merely congested. The worm was alive, 4 in. long,and paler in colour than three other large female onesfound in the stomach and duodenum. The posteriorborder of the upper lobe showed hypostatic congestion ;the rest of the lung was crepitant.
Civil Hospital, Aden.
ADDITIONAL NOTE ON THE FUMES OF BROMIDEOF AMMONIUM.
BY THEODORE MAXWELL, M.D., B.Sc.
SINCE writing the note on the Inhalation of Bromide ofAmmonium Fumes, published in THE LANCET of May 10th,I have tried a plan for the production of hydrobromic acidwhich was suggested to me by Messrs. Burgoyne, Barbidges,and Co.-viz., the addition of fused chloride of calcium tothe solution of hydrobromic acid triple the Pharmacopoeialstrength, and am glad to say it works very well in aVerreker’s chloride of ammonium inhaler.Woolwich.
A MirrorOF
HOSPITAL PRACTICE,BRITISH AND FOREIGN.
ST. THOMAS’S HOSPITAL.A CASE OF PORRO-CÆSAREAN SECTION IN A RACHITIC DWARF;
SUCCESSFUL RESULT BOTH TO MOTHER AND CHILD;REMARKS.
(Under the care of Dr. CULLINGWORTH.)
Nulla autem est alia pro certo noscendi via, nisi quamplurimas et mor-borem et dissectionum historias, tum aliorum tum proprias collectashabere, et inter se compa.ra.re.—MOR&AGNI De Sed. et CaUB. Morb.,lib. iv. Procemium. -
WE publish this week the notes of a case of Porro-Csesarean operation, to which we have already alluded inour columns,! and at the performance of which we werepresent. Undertaken atter a full consideration of the
bearings of the case, it is a good example of the modernoperation as performed with the object of saving bothmother and child, and we would direct the attention of ourreaders to the remarks by Dr. Cullingworth on the casealso to the table which is appended to his remarks. It wasthe intention of the operator to perform the Caesarean
operation after the method which is known as Sanger’s; butthe intractable nature of the haemorrhage prevented himfrom leaving the uterus when sutured. We published thenotes of a successful Porro’s operation by Dr. W. Duncanat the Middlesex Hospital in our first issue of last year.2In that case the patient was also extremely rachitic, andthe result satisfactory.Mary C-, aged twenty-five, a rachitic dwarf, married,
was admitted into St. Thomas’s Hospital Feb. 24th, 1890,with a view to Caesarean section. She was then in theninth month of her third pregnancy. Her previous historywas as follows :-The catamenia commenced at fourteen,recurring regularly every four weeks. The flow usuallylasted three days, was habitually scanty, and accom-
panied with severe abdominal pain. She had beenmarried two years. Her first confinement took placeat full term on Dec. 17th, 1887. She was on thatoccasion attended at her own home in connexion with theSt. Thomas’s Hospital Maternity, and delivered by cranio-tomy. She made a good recovery. She again becamepregnant in May, 1888, and, on presenting herself a little
1 THE LANCET, March 22nd. 2 Ibid., vol. i., p. 16.
later for a maternity ticket, she was directed to see Dr,Cullingworth. After hearing her history and carefullyexamining her he advised her to seek admission to the York-road Lying-in Hospita.1 for the purpose of having labourinduced at the seventh month. She took his advice, andon Dec. 18th, 1888, at 3.15 P M., a bougie was introducedinto the uterus. At 4 P M. the same day the liquor amniibegan to escape, but labour pains did not come on until3p.M.on Dec. 20th. The child presented by the breech, which re-mained stationary at the pelvic brim for five hours. The pulsehaving then risen to 120, chloroform was administered, andextraction effected by hooking a finger into the groin. Thearms were extended, the head passed without difficulty.The child, a female, was born at 9.45 P.M. The placentawas expressed. The amount of blood lost was twelve fluidounces. A hot douche was administered ; a draught con-taining a fluid drachm of the liquid extract of ergot wasgiven. The uterus contracted fairly well, and the patientmade a good recovery. Her temperature taken duringlabour was 992°, after labour 101 6°. During the fortnightfollowing delivery the temperature was usually under100°, and only once exceeded 100’4°, the exceptionoccurring on the tenth day, when the thermometer onone occasion registered 101 ’4°. The child weighed3 Ib. 7 oz., and was apparently stillborn. Artificial respira-tion was practised and continued for an hour, at theend of which time feeble efforts at respiration were made.Breathing never, however, became fully established, andcardiac pulsation finally ceased an hour and a half afterdelivery.The patient became pregnant for the third time at the latter
part of June, 1889. Dr. Cullingworth had an interview withher soon afterwards, and strongly advised her to submit toCaesarean section at or near the full term. She willinglyconsented to this, and attended the out-patient departmentregularly throughout the remainder of her pregnancy. OnFeb. 24th, 1890, she was ad-mitted into Adelaide ward, whenthe following notes were takenof her condition :-" The patienthas fair hair, blue eyes, and is ofa cheerful and placid disposition.Her height is 3 ft. 9 in. Thefemora and tibiee are thickened,with anterior curve. On the leftside there is marked genuvalgum, the patella is dislocatedoutwards, and there.is a projec-tion in front of the tibia twoinches below the knee-joint. Theteeth are mostly in a state of
decay. The general health is
good. The urine is free fromalbumen, and there are no pres-sure symptoms. The measure-ments are : Distance between theiliac spines, 9t in.; between theiliac crests, 9 in. ; external con-jugate, 6 in. ; diagonal conju-gate, 38 in. (The actual conjugatehad been ascertained on the occa-sion of her last labour to be 2 in.)The uterine walls are thin; thechild’s head being in the leftiliac fossa, the back is directedforwards ; the breech lies at thefundus, and to the right. Thesounds of the fcetal heart are heard most distinctly acthe level of the umbilicus, an inch and a quarter to theleft. A sense of resistance, thought to be probably dueto the presence of the placenta, is felt at the upper partof the uterus, commencing about two inches to the left ofthe middle line, and extending outwards to the left lateralwall. The greatest girth of the abdomen is 32 in., thedistance from umbilicus to ensiform cartilage 71 in., andfrom umbilicus to pubes 7 in. The patient last menstruatedon June 14th, 1889."On March 13th, the patient having been prepared by the
administration of an aperient the previous day, followed by anenema in the morning, the operation was performed at 2 P..in one of the large operating theatres of the hospital. Labourhad not commenced, nor had any means been adopted toPxcite it. Ether was administered by Mr. E. F. White.Mr. A. N. Boycott, resident accoucheur, and Mr. Forde,
1069
clinical clerk, assisted at the operation. An incisionwas made in the middle line from a little above the.umbilicus to a point about three inches above the
pubes. The abdominal wall was very thin, the inner edgesof the recti being widely separated. The original incisionwas afterwards enlarged upwards, in order to allow theuterus to be turned out of the abdominal cavity. Threesilkworm-gut sutures were passed through the edges of theupper part of the enlarged wound, and when the uterushad been pressed out these were tightened and held tightboy an assistant during the whole time the uterus was out-side. An Esmarch’s elastic tube was loosely passed twiceround the cervix and secured by pressure forceps. Avertical incision, four inches and a half in length, wasnow made in the middle line of the uterus, almost throughthe entire thickness of its wall, and in the centre of theincision completely so. In the latter situation the mem-branes protruded in the form of a small pouch. This was
punctured, and the liquor amnii allowed to escape. Thedeep portion of the remainder of the incision was thendivided on the fingers, disclosing to view the left shoulderand surrounding parts of the foetus, which was thenextracted, the left arm being seized first, then the head(which was lowermost) and the rest of the body. Thefunis was quickly clamped and divided, and the child,which though living had not yet breathed, was handedover to Mr. C. H. James, who kindly undertook its resusci-tation. Beyond a spurt from a sinus divided in openingthe uterus there had been no haemorrhage of any im-portance. Directions were now given to tighten the elastictube. The hand was introduced within the uterus, whichhad contracted well as the child was being withdrawn, andthe placenta and membranes were separated and removed.The placenta was situated on the left side of the upperpart of the uterus, chiefly on its posterior wall, the positionof the anterior edge corresponding with that diagnosed byabdominal palpation before the operation. The fundusbeing now protected with a hot sponge, the uterine sutureswere introduced six deep (not including the mucous mem-brane) and eight superficial (Lembert’s), all of silk. Afterswabbing the interior of the uterus with pledgets ofwool moistened with solution of corrosive sublimate(1 in 1000) the sutures were tied, The ovaries andtubes were next ligatured and removed to preventsubsequent conception, and then the elastic tube wasslackened. The uterus, which up to this point had beenfairly well contracted, now became relaxed, and hmmor-rhage took place, not only per vaginam, but also frombetween the sutures in the situation of the divided sinus.Every effort was made to excite contraction by kneadingthe uterus, by the subcutaneous injection of ergot, and bydouching the interior of the uterus with hot water pervaginam. As none of these measures proved successful, itwas decided to amputate the uterus after the manner ofPorro. The elastic tube was readjusted and tightened. Asa serre-nceud was not at hand, the wire of an ecraseur waspassed round the neck of the uterus, the intention being tosecure the stump by twisting the wire, in the manner recom-mended and practised by Mr. Pridgin Teale. The wire,however, was too thick for the purpose, and, a serre-nceudhaving in the meantime been obtained, the ecraseur wasremoved and the serre noeud applied in the usual way. Twoguarded pins were then passed through the uterine tissueon the distal side of the constricting wire, and the uteruswas cut away with the knife about half an inch above them.The peritoneal cavity, into which very little blood hadescaped, was now cleansed with sponges; the elastic tubewas removed, the sulcus formed by the wire was examined,nd cleansed, and the abdominal wound was closed bythirteen sutures of silkworm gut. No drainage-tube wasinserted. The stump was dusted with iodoform; iodoformgauze was packed around it, beneath its everted edge, andbeneath the pins and serre-noeud; wood-wool pads wereplaced over the stump and incision, and the dressing wascompleted by covering the whole abdoiren with a thicklayer of absorbent wool, and applying a many-tailed flannelbandage over the whole. The operation lasted an hour andtwenty-five minutes. The child, a female, soon cried lustily;its weight was 6 lb. 4 oz.; its length 19 in. The placentaweighed 1 lib. 51 oz., and measured 7 in. by 6 in. in diameter.The length of the umbilical cord was 27 in.The patient made a most favourable recovery. She had
several attacks of vomiting and hiccough during the first
seventy hours, and had a quarter of a grain of morphiainjected subcutaneously on three different occasions. Onthe morning after the operation the temperature was 101’2°,and the pulse rose to 138, and became irregular, but thepatient had no pain or distension, and both pulse and tem-perature fell before evening. At midnight the record wasas follows: Temperature 98 4°; pulse 100. The wire of theserre-nceud was tightened twelve hours and again twenty-six hours after the operation, on account of a little oozingfrom the pedicle. The patient passed flatus, and was ableto dispense with the catheter on the morning of the fourthday. The bowels beginning to feel uncomfortable in theafternoon of the sixth day, a simple enema was administeredwith satisfactory result. On March 20th (the eighth day)the stump had, for the first time, an ill odour, and therewas some brown ill-smelling discharge on the gauze dress-ing. The pins were very loose. The nine uppermostsutures in the abdominal wound were removed. On the23rd (eleventh day) the pedicle was carefully cut away belowthe pins, and the serre-nceud removed by cutting the wires.A fresh pin was made to transfix the remains of the pedicleto prevent premature retraction. Two more sutures wereremoved from the abdominal wound, and the patient wasremoved to the general ward. Next day the two remainingsutures were taken out, and the stump of the pedicle wastrimmed, the pin inserted on the 23rd being finally re-
moved. On March 25th there was much depression of themargins of the abdominal wound around the remains of thepedicle. The stump of the pedicle never retracted sufficientlyto be out of sight, and in a month from the operation thewound had become nearly closed. Mother and child leftthe hospital well on April 16th.Remarks by Dr. CULLINGWORTH.-Post-partum haemor-
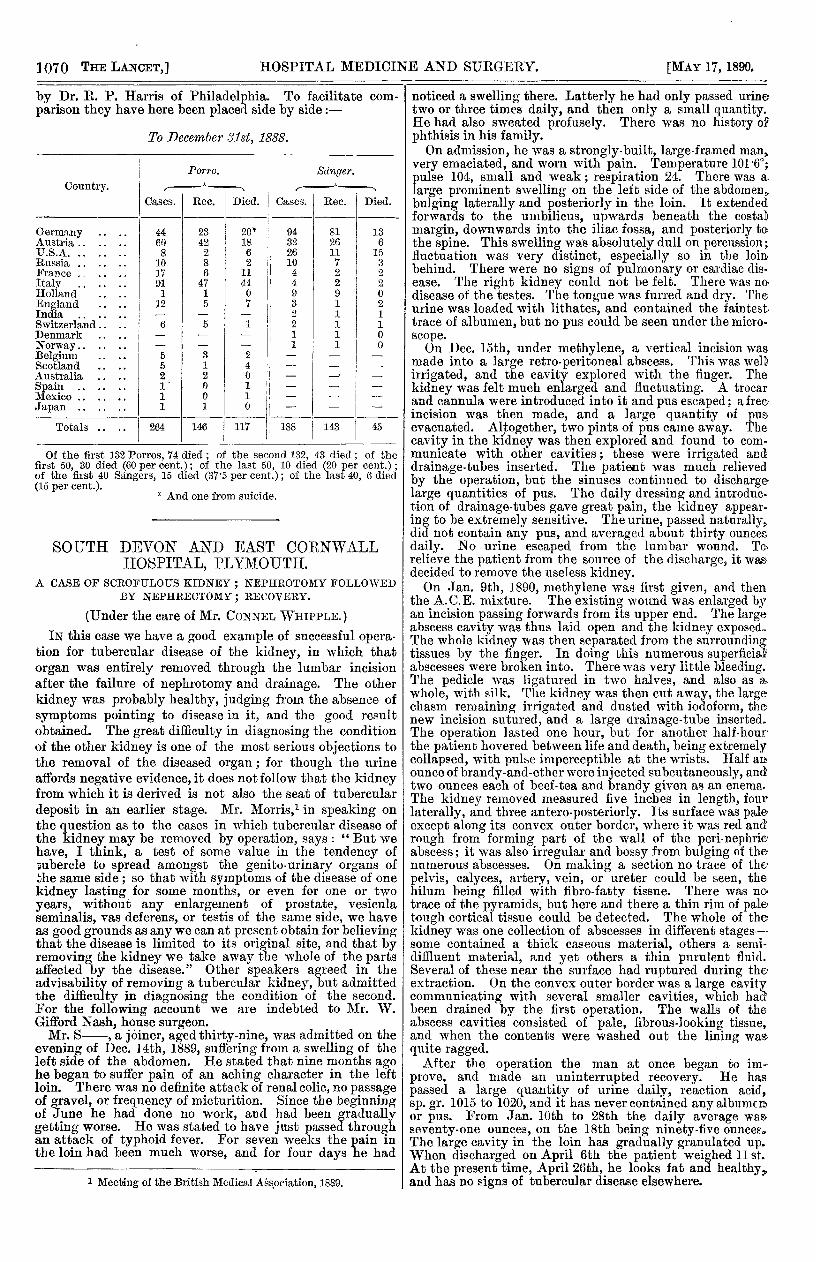
rhage from failure of the uterus to become permanentlycontracted is an exceedingly rare occurrence after theoperation of Caesarean section. It was fortunate that ittook place in this case before and not after the closure ofthe abdominal wound, so that remedial measures could betaken promptly. * The decision to remove the uterus wasfully justified by the result. It must, of course, be acknow-ledged that all the conditions in this 1 case were favourableto success. The patient was in good health ; she had beenin the hospital for a fortnight before the operation, andI was able to choose my own time for its performance.There had been no previous attempts at delivery pervaginam, and, labour not having even commenced, theuterine muscle was fresh for its work ; it ought, indeed, tohave behaved better than it did. It may be asked whyI did not induce labour on the morning of the opera-tion. The answer is (1) that, though I might have initiatedlabour, I should not have been able to control the rateof its progress, which might have proved inconvenientlyrapid; (2) that the membranes might have been accidentallyruptured during the necessary manipulations, with theresult of hastening the labour and imperilling the child;and (3) that an additional risk of septic infection wouldhave been introduced without any real necessity. Withregard to the question as to whether the operation wasjustifiable there may be differences of opinion. Where thecontraction of the pelvis has not been greater than it wasin this case, it has been the custom in this country hithertoto induce labour at the seventh month, or to performcraniotomy at term. I am one of those who think that atime comes when the child has some claim to consideration,and when, in order to save the child, the mother maylegitimately be counselled to run some risk herself (and, inthese days, Caesarean section entails but a slightly greaterrisk than craniotomy, when the latter is performed forpelvic contraction of a severe character). The provisionalrule I have laid down for myself at present is to urge theperformance of Caesarean section in every case of small orgenerally contracted pelvis where the antero-posteriordiameter at the brim does not exceed 2 in., and wherelabour has been previously induced at the seventh monthwithout saving the child. In Germany the mortality fromCaesarean section is so low (13’8 percent.) that the opera-tion is habitually undertaken in cases of much slighterdeformity than this ; the time, however, does not seem tohave arrived for extending the scope of the operation inthis country-for the present, at least-beyond the limitsI have indicated.The following tables, which, though probably not quite
complete, present many points of interest, are from a paper
1070
by Dr. R. P. Harris of Philadelphia. To facilitate com-parison they have here been placed side by side :-
To December 31st, 1888.
Of the first 132 Porros, 74 died ; of the second 132, 43 died; of thefirst 50, 30 died (60 per cent.) ; of the last 50, 10 died (20 per cent.) ;of the first 40 Sangers, 15 died (37’5 per cent.); of the last 40, 6 died(15 per cent.).
* And one from suicide.* And one from suicide.
SOUTH DEVON AND EAST CORNWALLHOSPITAL, PLYMOUTH.
A CASE OF SCROFULOUS KIDNEY ; NEPHROTOMY FOLLOWEDBY NEPHRECTOMY ; RECOVERY.
(Under the care of Mr. CONNEL WHIPPLE.)IN this case we have a good example of successful opera-
tion for tubercular disease of the kidney, in which thatorgan was entirely removed through the lumbar incisionafter the failure of nephrotomy and drainage. The other
kidney was probably healthy, judging from the absence ofsymptoms pointing to disease in it, and the good resultobtained. The great difficulty in diagnosing the conditionof the other kidney is one of the most serious objections tothe removal of the diseased organ ; for though the urineaffords negative evidence, it does not follow that the kidneyfrom which it is derived is not also the seat of tubercular
deposit in an earlier stage. Mr. Morris,l in speaking onthe question as to the cases in which tubercular disease ofthe kidney may be removed by operation, says : " But wehave, I think, a test of some value in the tendency of,ubercle to spread amongst the genito-urinary organs ofthe same side; so that with symptoms of the disease of onekidney lasting for some months, or even for one or two
years, without any enlargement of prostate, vesiculaseminalis, vas deferens, or testis of the same side, we haveas good grounds as any we can at present obtain for believingthat the disease is limited to its original site, and that byremoving the kidney we take away the whole of the partsaffected by the disease." Other speakers agreed in theadvisability of removing a tubercular kidney, but admittedthe difficulty in diagnosing the condition of the second.For the following account we are indebted to Mr. W.Gifford Nash, house surgeon.Mr. S-, a joiner aged thirty-nine, was admitted on the
evening of Dec. 14th, 1889, suffering from a swelling of theleft side of the abdomen. He stated that nine months agohe began to suffer pain of an aching character in the leftloin. There was no definite attack of renal colic, no passageof gravel, or frequency of micturition. Since the beginningof June he had done no work, and had been graduallygetting worse. He was stated to have just passed throughan attack of typhoid fever. For seven weeks the pain inthe loin had been much worse, and for four days he had
1 Meeting of the British Medical Association, 1889.
noticed a swelling there. Latterly he had only passed urinetwo or three times daily, and then only a small quantity.He had also sweated profusely. There was no history ofphthisis in his family.On admission, he was a strongly-built, large-framed man,
very emaciated, and worn with pain. Temperature 1016°;pulse 104, small and weak; respiration 24. There was a,large prominent swelling on the lef side of the abdomen’bulging laterally and posteriorly in the loin. It extendedforwards to the umbilicus, upwards beneath the costaDmargin, downwards into the iliac fossa, and posteriorly twothe spine. This swelling was absolutely dull on percussion;tluctuation was very distinct, especially so in the loinbehind. There were no signs of pulmonary or cardiac dis-ease. The right kidney could not be felt. There was no.disease of the testes. The tongue was furred and dry. Theurine was loaded with lithates, and contained the faintesttrace of albumen, but no pus could be seen under the micro-scope.On Dec. 15th, under methylene, a vertical incision was
made into a large retro-peritoneal abscess. This was well,irrigated, and the cavity explored with the finger. Thekidney was felt much enlarged and fluctuating. A trocarand cannula were introduced into it and pus escaped; a freeincision was then made, and a large quantity of pus.evacuated. Altogether, two pints of pus came away. Thecavity in the kidney was then explored and found to corn"municate with other cavities; these were irrigated anddrainage-tubes inserted. The patient was much relievedby the operation, but the sinuses continued to dischargelarge quantities of pus. The daily dressing and introduc-tion of drainage-tubes gave great pain, the kidney appear-ing to be extremely sensitive. The urine, passed naturally,did not contain any pus, and averaged about thirty ouncesdaily. No urine escaped from the lumbar wound. To,relieve the patient from the source of the discharge, it was.decided to remove the useless kidney.On Jan. 9th, 1890, methylene was first given, and then
the A.C.E. mixture. The existing wound was enlarged byan incision passing forwards from its upper end. The largeabscess cavity was thus laid open and the kidney exposed.The whole kidney was then separated from the surroundingtissues by the finger. In doing this numerous superficialabscesses were broken into. There was very little bleeding.The pedicle was ligatured in two halves, and also as a.
whole, with silk. The kidney was then cut away, the largechasm remaining irrigated and dusted with iodoform, thenew incision sutured, and a large drainage-tube inserted.The operation lasted one hour, but for another half-hourthe patient hovered between life and death, being extremelycollapsed, with pulse imperceptible at the wrists. Half amounce of brandy-and-ether were injected subcutaneously, andtwo ounces each of beef-tea and brandy given as an enema.The kidney removed measured five inches in length, fourlaterally, and three antero-posteriorly. Its surface was paleexcept along its convex outer border, where it was red and’rough from forming part of the wall of the peri-nephricabscess; it was also irregular and bossy from bulging of thenumerous abscesses. On making a section no trace of the.pelvis, calyces, artery, vein, or ureter could be seen, thehilum being filled with fibro-fatty tissue. There was notrace of the pyramids, but here and there a thin rim of paletough cortical tissue could be detected. The whole of thekidney was one collection of abscesses in different stages-some contained a thick caseous material, others a semi-diffluent material, and yet others a thin purulent fluid.Several of these near the surface had ruptured during theextraction. On the convex outer border was a large cavitycommunicating with several smaller cavities, which had:been drained by the first operation. The walls of theabscess cavities consisted of pale, fibrous-looking tissue,and when the contents were washed out the lining W3J9quite ragged.After the operation the man at once began to im-
prove, and made an uninterrupted recovery. He has
passed a large quantity of urine daily, reaction acid,sp. gr. 1015 to 1020, and it has never contained any albumenor pus. From Jan. 10th to 28th the daily average wasseventy-one ounces, on the 18th being ninety-five ouncecdThe large cavity in the loin has gradually granulated up.When discharged on April 6th the patient weighed 11 st.At the present time, April 26th, he looks fat and healthyand has no signs of tubercular disease elsewhere.