21
Standard of Care for MDR-TB Hind Satti, MD Partners In Health Lesotho

Standard of Care for MDR-TB
Hind Satti, MDPartners In Health
Lesotho

Lesotho: Basic Facts
• Landlocked country located within South Africa (bordering Free State and KwaZulu-Natal)
• Population 1.8 million• 12,275 TB new cases notified in 2009• Over 2000 re treatment cases • HIV prevalence rate: 23.2% in 2005• 80% of TB cases are HIV positive (NTP 2008)

TB Situation in Lesotho
• Estimated prevalence of 544/100,000 population
• Estimated annual incidence for all cases is 691 per 100,000 population
• Estimated incidence of Sputum smear positive cases is 281 per 100,000 population
• Estimated all TB deaths is 107/100,000 annually

Lesotho MDR-TB Programme
• A comprehensive response to MDR-/XDR-TB in Lesotho, established by the MOHSW.
• International partners include PIH, WHO, FIND, OSI
• Community-based treatment and care model that includes all 10 districts
• First patients enrolled in August 2007; 500 patients enrolled to date

National TB Reference Laboratory
Case Detection
• All HCWs including NTP staff– TB/HIV coordinators/Officers at district hospitals – Health centre nurses providing HIV/TB care
• Routine HIV screening of MDR-TB patients, partners, family members
• Protocol for “medium-risk” and “high-risk”• Sputum sent to national TB laboratory • Screening of household contacts

Botsabelo MDR-/XDR-TB Hospital

Patient Characteristics
• Approximately 78% HIV-positive with advanced AIDS-defining conditions
• Severe malnutrition• Multiple failed TB
treatment regimens• Extensive TB disease• Mostly smear-positive
Inpatient Care
• Very sick patients mostly co infected – Bedridden– Severely wasted
• Severe side effects– Severe hypokalemia– Acute renal failure
• Severe OIs– Meningitis– Esophageal candidiasis

Lesotho vs. rest of the world†
*Tomsk, Latvia, Estonia, Peru, Philippines
† Nathanson et al. Adverse events in the treatment of multidrug-resistant tuberculosis: results from the DOTS-Plus initiative. Int J Tuberc Lung Dis 2004. 8(11):1382–1384

Standardized MDR-TB Regimen
• Pyrazinamide• Kanamycin• Levofloxacin• Prothionamide• Cycloserine • PAS

Infection Control
• Outpatient– TB clinics and general outpatient clinics– Treatment supporters– Family members
• Inpatient– Cross-infection of patients– Protection of health workers (TB and HIV)

Social assistance

MDR-TB/HIV
• 100% HIV testing during the first visit.• Early initiation of HARRT for MDRTB/HIV
(10-21 days), regardless of CD4 count.• Aggressive management of side effects. • Home assessment visit before initiation.• Household contact screening and testing
for TB and HIV.
Adherence
• Adherence crucial in successful treatment of drug-resistant TB
• Barriers to adherence are socioeconomic and must be addressed
• Adverse effects also contribute to poor adherence

Selection of Treatment Supporters
• Lives close to the patient• Accepted by patient and
family• Willing to support patient
for at least 2 years• Willing to accompany
patient to all clinical visits• Attend monthly trainings• Willing to provide
psychosocial support• Not immunocompromised

Role of Treatment Supporter
• Observe all doses • Report side effects• Provide injections.• Accompany patient for
clinical evaluations• Screen for TB and HIV
in household contacts.• Offer psychosocial
support to the patient and the family.

Lesotho National MDR-TB Program
• Currently 550 patients enrolled in community-based treatment
• High incidence of side effects • Comprehensive and integrated
management (HTN, DM, FP, etc.)• Social support, cooperatives, microfinance
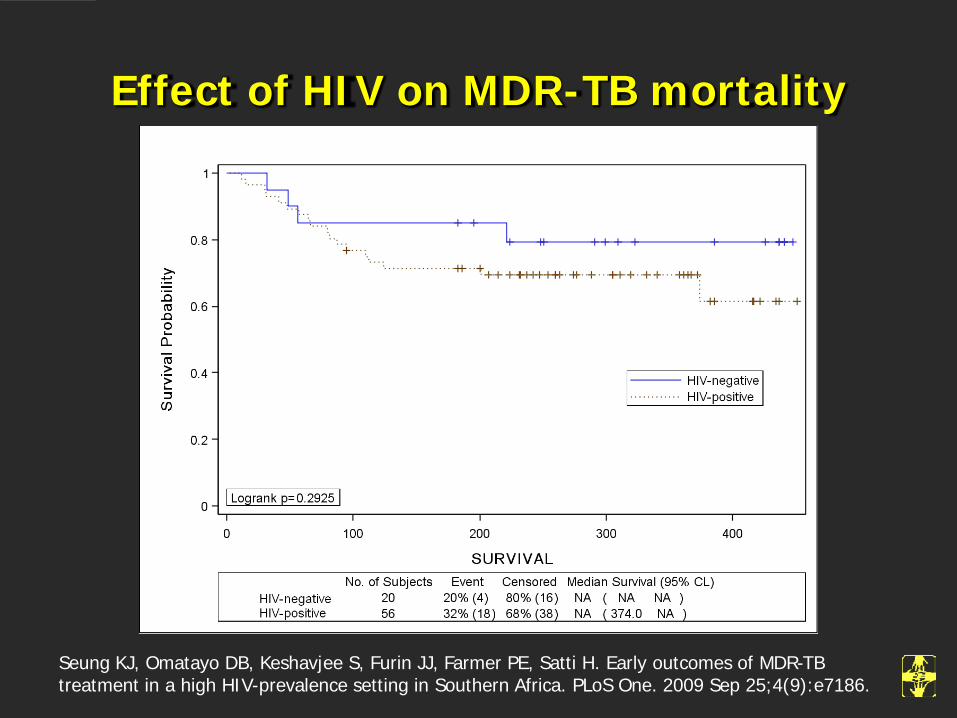
Effect of HIV on MDR-TB mortality
Seung KJ, Omatayo DB, Keshavjee S, Furin JJ, Farmer PE, Satti H. Early outcomes of MDR-TB treatment in a high HIV-prevalence setting in Southern Africa. PLoS One. 2009 Sep 25;4(9):e7186.

Conclusion
• Diagnosis and management of MDR-TB in high HIV-prevalence settings is challenging but possible
• Empiric treatment of MDR-TB is needed to decrease early mortality
• Side effects are more common and earlier• Infection control at all levels: hospital, clinic,
community is critical.• Community-based MDR-TB/HIV allows for rapid
enrollment and closer monitoring of side effects

Key Research Areas
• Are there more effective drugs? • Do co-infected patients have
malaborption?• Can treatment be shorter? • Can treatment be safer (less side effects)?• What is the best timing of HAART?• Are there any drug interactions with
HAART?

















