Standards & Interoperability Workgroup Co-Chairs: Greg Linden, Stratis Health Jonathan Shoemaker, Allina Health MDH Staff: Kari Guida Melinda Hanson Minnesota e-Health Initiative November 7, 2014
Transcript
Standards & Interoperability Workgroup
Co-Chairs:Greg Linden, Stratis HealthJonathan Shoemaker, Allina Health
MDH Staff:Kari GuidaMelinda Hanson
Minnesota e-Health Initiative November 7, 2014
2
Meeting Objectives
• Review the workgroup charge• Discuss the Health Care Quality Measures Study: e-
Health Component • Provide Feedback on Social Determinants of Health and
EHRs– Capability of EHRs to capture disability, race, ethnicity,
language, and other sociodemographic factors health– Capacity of EHRs to capture disability, race, ethnicity,
language, and other sociodemographic factors – Challenges to using disability, race, ethnicity, language, and
other sociodemographic factors collected in the EHRs
3
Agenda
• Welcome & Introductions• Workgroup Charter• Advancing Health Equity• Health Care Quality Measures Study: e-Health
Component• Social Determinants of Health & EHRs Panel• Discussion• Next Steps & Adjourn
4
Welcome & Introduction
• Name• Position & Organization• Estimated number of MN e-Health Initiative
Workgroup meetings attended
5
STANDARDS & INTEROPERABILITY WORKGROUP CHARGE
6
Workgroup Charge
• Identify gaps, barriers, and opportunities related to capturing standardized social determinants of health data elements
• Review and recommend nationally recognized standards, interoperability requirements, implementation specifications and certification
• Communicate information on adoption of standards, implementation specifications and certification criteria related to the requirements of “meaningful use” and Minnesota 2015 interoperable EHR mandate, and recommend resources and actions that will help increase implementation of these standards (e.g., Minnesota e-Health Standards and Interoperability Guide).
7
ADVANCING HEALTH EQUITY
8
Advancing Health Equity in Minnesota: Report to the Legislature (2014)
• Initiated because disparities in health status outcomes for certain populations are continuing unabated, including disparities based on race or ethnicity
• Assesses Minnesota’s health disparities and health inequities and recommends best practices, policies, process, data strategies and other steps to promote health quality
9
Health Disparities & Health inequities in Minnesota
• African American and American Indian babies die in the first year of life at twice the rate of white babies.
• Gay, lesbian and bisexual university students are more likely than their heterosexual peers to have struggles with their mental health.
• Intimate partner violence affects 11 to 24 percent of high school seniors, with the highest rates among American Indian, African American and Hispanic/Latino students. American Indian, Hispanic/Latino, and African American youth have the highest rates of obesity.
• Persons with serious and persistent mental illness die, on average, 25 years earlier than the general public.
• African American and Hispanic/Latino women in Minnesota are more likely to be diagnosed with later-stage breast cancer.
• Nearly 25 percent of persons in Minnesota over 50 who live alone have no one to provide care for them if they were to become sick or disabled, compared to only five percent of those who live with others.
Advancing Health Equity in Minnesota: Report to the Legislature (2014)
10
Health Equity Terminology (1 of 3)• Health is a state of complete physical, social and mental well-being and not merely the
absence of disease or infirmity (WHO).
• Health disparity: A population-based difference in health outcomes (e.g., women have more breast cancer than men).
• Health inequity: A health disparity based in inequitable, socially-determined circumstances (for example, American Indians have higher rates of diabetes due to the disruption of their way of life and replacement of traditional foods with unhealthy commodity foods). Because health inequities are socially-determined, change is possible. Socially determined means that these conditions are created by decisions that affect community or society at large (e.g. polices of governments, corporate decisions, neighborhood action)
• Health equity: When every person has the opportunity to realize their health potential — the highest level of health possible for that person — without limits imposed by structural inequities. Health equity means achieving the conditions in which all people have the opportunity to attain their highest possible level of health.
Advancing Health Equity in Minnesota: Report to the Legislature (2014)
11
Health Equity Terminology (2 of 3)• Population Health: An aim to optimize the health and well-being of an
entire community and reduce inequalities in health and well-being between population groups. A “community” may be either geographic regions and/or groups of people who share attributes (e.g., elderly, minorities, employees, disabled persons, students). Population health requires collaboration across all sectors of a community to address factors such as public infrastructure, the environment, education systems, social supports, and the health care system, in order to address all social determinants of health. Population health within an accountable care organization requires collaboration between all health care providers in the community, social support services within the community, and local public health.
Adapted from: • K Hacker, DK Walker. Achieving Population Health in Accountable Care Organizations, Am J Public Health.
2013; 103(7):1163-1167. D Kindig, G Stoddart. What is population health? Am J Public Health. 2003;93(3):380–383; and
• M Stoto. Population Health in the Affordable Care Act Era. AcademyHealth, February 2013.
12
Health Equity Terminology (3 of 3)• Social Determinants of Health are the complex, integrated, and
overlapping social structures and economic systems that are responsible for most health inequities. These social structures and economic systems include the social environment, physical environment, health services, and structural and societal factors. Social determinants of health are shaped by the distribution of money, power, and resources throughout local communities, nations, and the world.
Commission on Social Determinants of Health, Closing the gap in a generation: health equity through action on the social determinants of health. Final report of the Commission on Social Determinants of Health. 2008, World Health Organization: Geneva.
13
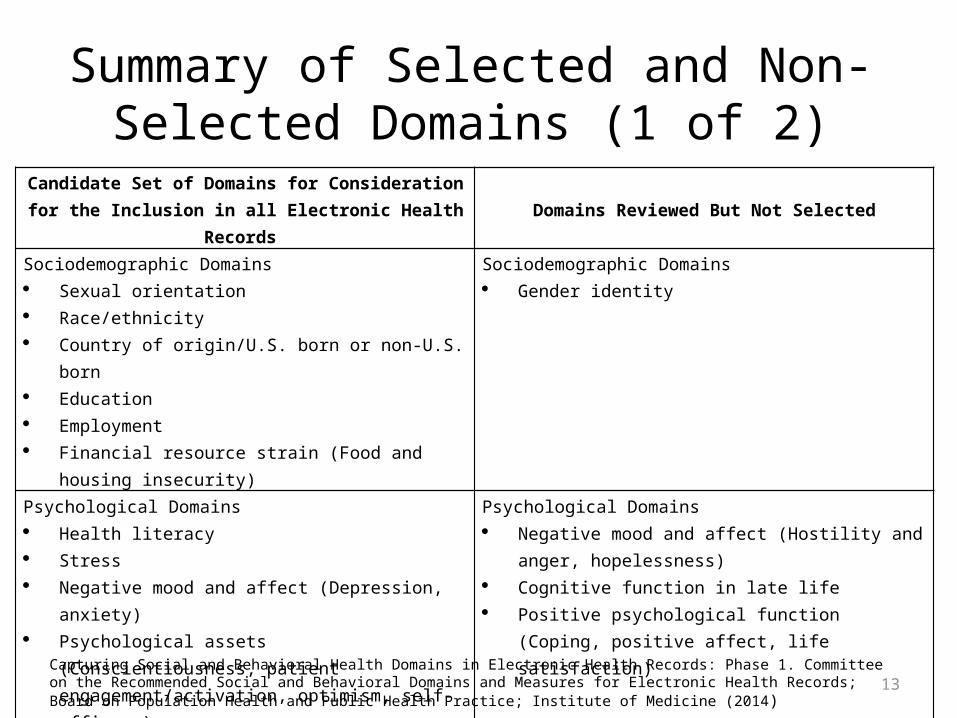
Summary of Selected and Non-Selected Domains (1 of 2)
Candidate Set of Domains for Consideration for the Inclusion in all Electronic Health Records Domains Reviewed But Not Selected
Sociodemographic Domains Sexual orientation Race/ethnicity Country of origin/U.S. born or non-U.S. born Education Employment Financial resource strain (Food and housing insecurity)
Sociodemographic Domains Gender identity
Psychological Domains Health literacy Stress Negative mood and affect (Depression, anxiety) Psychological assets (Conscientiousness, patient
engagement/activation, optimism, self-efficacy)
Psychological Domains Negative mood and affect (Hostility and anger,
hopelessness) Cognitive function in late life Positive psychological function (Coping, positive affect, life
satisfaction)Behavioral Domains Dietary patterns Physical activity Nicotine use and exposure Alcohol use
Behavioral Domains Abuse of other substances Sexual practices Exposure to firearms Risk-taking behaviors (Distractive driving and helmet use)
Capturing Social and Behavioral Health Domains in Electronic Health Records: Phase 1. Committee on the Recommended Social and Behavioral Domains and Measures for Electronic Health Records; Board on Population Health and Public Health Practice; Institute of Medicine (2014)
14
Summary of Selected and Non-Selected Domains (2 of 2)
Candidate Set of Domains for Consideration for the Inclusion in all Electronic Health Records Domains Reviewed But Not Selected
Individual-Level Social Relationships Domains Social connections and social isolation Exposure to violence
Individual-Level Social Relationships Domains Social Support (Emotional, instrumental, and other) Work conditions History of incarceration Military service Community and cultural norms (Health care decision
making)
Neighborhoods and Communities (Geocodable Domains) Socioeconomic characteristics Race/ethnic characteristics
Neighborhoods and Communities (Geocodable Domains) Environmental exposures (Air pollution, allergens,
other hazardous exposures) Neighborhood resources (Nutritious food options,
transportation, parks, open spaces, health care and social services, educational and job opportunities )
Capturing Social and Behavioral Health Domains in Electronic Health Records: Phase 1. Committee on the Recommended Social and Behavioral Domains and Measures for Electronic Health Records; Board on Population Health and Public Health Practice; Institute of Medicine (2014)
15
HEALTH CARE QUALITY MEASURES STUDY: E-HEALTH COMPONENT
16
Health Care Quality Measure Study: e-Health Component
• Plan for stratifying health care quality measures based on disability, race, ethnicity, language, and other sociodemographic factors to the Legislature by January 15, 2015
• To identify the status, barriers, and opportunities in using electronic health records (EHRs) to collect social determinants of health and to understand challenges in using social determinants of health data.
• Make recommendations for needed future work, studies, and resources needed to leverage EHRs as a tool to achieve health equity.
• Focused on quality measures for clinics and hospitals but all providers across the spectrum of care can benefit from this work
17
e-Health Questions
The Office of Health Information Technology (OHIT) along with engagement of the MN e-Health Initiative will start to answer three questions:
• What is the capability of EHRs to capture disability, race, ethnicity, language, and other socio-demographic factors?
• What is the capacity of EHRs to capture disability, race, ethnicity, language, and other socio-demographic factors?
• What are the challenges to using disability, race, ethnicity, language, and other socio-demographic factors collected in the EHRs?
18
Methods
• Evaluate current assessment data collected on clinics and hospitals and social determinants of health factors from the MN e-Health Profile
• Review and leverage current reports such as – Capturing Social and Behavioral Domains in Electronic Health Records
Phase 1 & Phase 2 Reports – Advancing Health Equity in Minnesota: Report to the Legislature
• Document how Meaningful Use Stage 2 currently requires and has standards for social determinants of health
• Stakeholder engagement and expert opinion– Standards & Interoperability Workgroup Meeting– Requesting feedback on the three questions
• Preliminary findings reviewed by workgroup between November 20 –December 2.
• MN e-Health Advisory Committee reviews the workgroup findings on December 9.
20
Meaningful Use & Social Determinants of Health Stage 2 Eligible Professional
Meaningful Use Core Measures
Measure 3: Record Demographics• Objective: Record the following demographics:
preferred language, sex, race, ethnicity, date of birth
• Measure: More than 80 percent of all unique patients seen by EP have demographics recorded as structured data
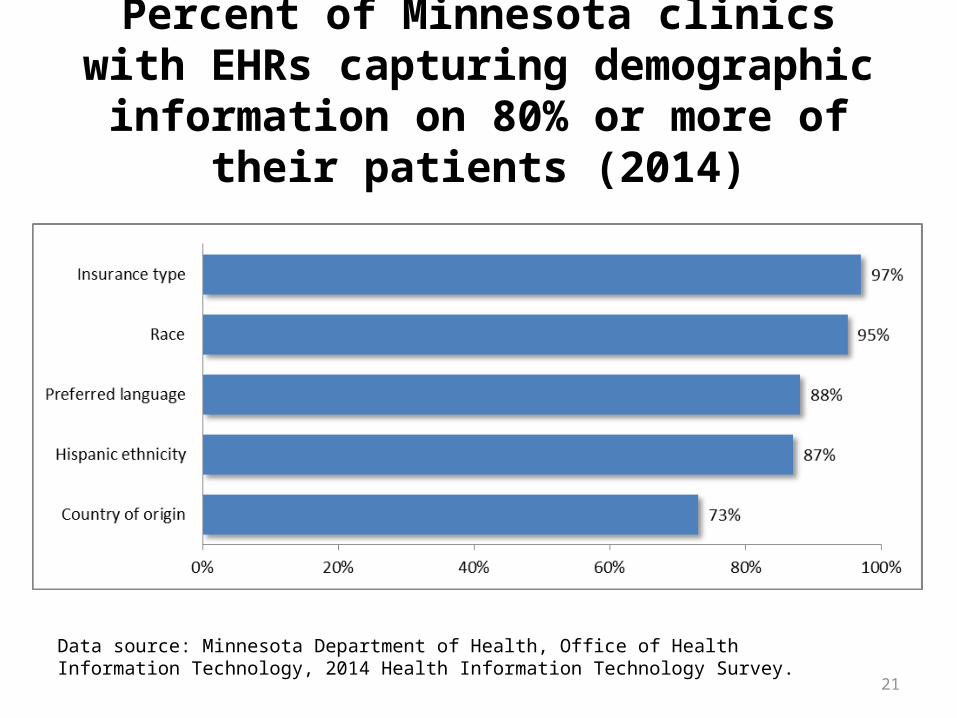
21
Percent of Minnesota clinics with EHRs capturing demographic information on 80% or
more of their patients (2014)
Data source: Minnesota Department of Health, Office of Health Information Technology, 2014 Health Information Technology Survey.
22
Percent of MN clinics with EHRs capturing detailed race and ethnicity information in
the EHR (2014)
Data source: Minnesota Department of Health, Office of Health Information Technology, 2014 Health Information Technology Survey.
23
SOCIAL DETERMINANTS OF HEALTH AND EHRs PANEL
24
Panelists
• Kevin Larsen, Office of the National Coordinator• Nancy Garret, Hennepin County Medical Center• Bjorn Westgard, Regions Hospital, HealthPartners• Kevin Peterson, Phalen Village Clinic
25
Questions
• What is the capability of EHRs to capture disability, race, ethnicity, language, and other socio-demographic factors?
• What is the capacity of EHRs to capture disability, race, ethnicity, language, and other socio-demographic factors?
• What are the challenges to using disability, race, ethnicity, language, and other socio-demographic factors collected in the EHRs?
Disparities Data and the EHR
Bjørn C. Westgard, MD, MA, FACEPRegions Hospital - HealthPartners Medical Group
Hennepin County Medical Center Assistant Professor, University of MN Medical School
• What is captured – race, ethnicity, employment?
• Where is it captured (notes or structured)?– Self-reported race/ethnicity – structured
demographic– Country of origin – structured demographic– Primary language – structured demographic– Employment – social history notes– Disability – notes
What is the capability of EHRs to capture disability, race, ethnicity, language,
and other socio-demographic factors? (1 of 2)
28
What is the capability of EHRs to capture disability, race, ethnicity, language, and other
socio-demographic factors? (2 of 2)• What standards are used?– Census categories plus– Site based EPIC dictionary• Common to hospitals, clinics, health plans
– Variable quality continuity– Continual training and process improvement
How much/what percent of patients have the information
complete in the EHR?
• Race/ethnicity– Previously 70-80%– EBAN Disparities-Oriented QI/PI Project– Up in 90% range presently
• Country of origin and language– Up in 90% range presently– Closer to 60% completion
• Other data – variable
What are the challenges to using disability, race, ethnicity, language, and other
socio-demographic factors collected in the EHRs? (1 of 2)
• Defining the use for this data– Question determines relevant data– Interoperability needs
What are the challenges to using disability, race, ethnicity, language, and other
socio-demographic factors collected in the EHRs? (2 of 2)
Data elements• Consistent capture of data variables• Uniform coding of data variables• Usable, non-obstructing interface for end users• Relevant, validated data– Place and space– Measures of socioeconomic status
• Real standards of interoperability• Legal framework or mandate for interoperability
32
DISCUSSION ON SOCIAL DETERMINANTS OF HEALTH AND EHRs
33
Next Steps
• Send additional thoughts to [email protected] by Tuesday, November 11th.
• Preliminary findings reviewed by workgroup between November 20 –December 2
• MN e-Health Advisory Committee endorses workgroup findings December 9
• Full legislative report will be available in Winter 2015• Watch for details about next Standards & Interoperability
meeting in February 2015• Save the Date: Minnesota e-Health Summit June 16 -17,
2015 (Tentative)
34
Resources• Advancing Health Equity in Minnesota: Report to the Legislature (2014)
– http://www.health.state.mn.us/divs/chs/healthequity/index.htm• Capturing Social and Behavioral Domains in Electronic Health Records: Ph
ase 1 – http://www.iom.edu/reports/2014/capturing-social-and-behavioral-domains-
in-electronic-health-records-phase-1.aspx • Risk Adjustment for Socioeconomic Status or Other
• Commission on Social Determinants of Health, Closing the gap in a generation: health equity through action on the social determinants of health. Final report of the Commission on Social Determinants of Health. 2008, World Health Organization: Geneva – http://www.who.int/social_determinants/thecommission/finalreport/en/
Greg Linden, Co-ChairVice President, Information Services/Chief Information OfficerStratis Health
Jonathan Shoemaker, Cho-ChairDirector, Information ServicesAllina Health Kari Guida, MDH Workgroup CoordinatorsMDH Office of Health Information Technology [email protected] Melinda Hanson, MDH Workgroup CoordinatorsMDH Office of Health Information [email protected]
36
Health Care Quality Measure Study (1 of 3)Minnesota Laws, Chapter 312, Article 23, Section 10
(a) The commissioner of health shall develop an implementation plan for stratifying measures based on disability, race, ethnicity, language, and other sociodemographic factors that are correlated with health disparities and impact performance on quality measures. The plan must be designed so that quality measures can be stratified beginning January 1, 2017, in order to advance work aimed at identifying and eliminating health disparities. By January 15, 2015, the commissioner shall submit a report to the chairs and ranking minority members of the senate and house of representatives committees and divisions with jurisdiction on health and human services and finance with the plan, including an estimated budget, timeline, and processes to be used for implementation.
37
Health Care Quality Measure Study (2 of 3)Minnesota Laws, Chapter 312, Article 23, Section 10
(b) The commissioner of health shall assess the risk adjustment methodology established under Minnesota Statutes, section 62U.02, subdivision 3, for the potential for harm and unintended consequences for patient populations who experience health disparities, and the providers who serve them, and identify changes that may be needed to alleviate harm and unintended consequences. By January 15, 2016, the commissioner shall submit a report to the chairs and ranking minority members of the senate and house of representatives committees and divisions with jurisdiction on health and human services and finance with the result of the assessment of the risk-adjustment methodology and any recommended changes.
38
Health Care Quality Measure Study (3 of 3)Minnesota Laws, Chapter 312, Article 23, Section 10
(c) The commissioner shall develop the plan described in paragraph (a), in consultation with consumer, community and advocacy organizations representing diverse communities; health plan companies; providers; quality measurement organizations; and safety net providers that primarily serve communities and patient populations with health disparities. The commissioner shall use culturally appropriate methods of consultation and engagement with consumer and advocacy organizations led by and representing diverse communities by race, ethnicity, language, and sociodemographic factors.