1222 influence of ether, an incision was made down either side of the scar and it was dissected off the bone. When this had been done, a small punctured hole, not more than a third of an inch in diameter, was found in the bone, situated in the middle line of the frontal bone, immediately over the longi- tudinal sinus. This hole was filled up with dense fibrous tissue. A crown of bone, including this hole, was now removed with the trephine, and the cicatricial tissue filling it was seen to be intimately connected with the dura mater. This was carefully dissected off. There was no splintering of the internal table of the skull, nor anything causing undue pressure on the membranes of the brain. The wound was closed and dressed. After the operation the man seemed much brighter and better, and volunteered the statement that he felt better than he had done for some time, and had entirely lost the sensation of tightness and pain in his head. His tempera- ture was normal, and remained so throughout the future progress of the case. On March 20th the wound was dressed and found to be healed. He was allowed to get up. He seemed brighter, and said that he had entirely lost the old pain in the head. On April 8th he was sent to the Atkinson Morley Convalescent Hospital. He seemed to have qaite recovered from the operation and complained of no pain. He was still odd and irrational in his manner, inclined to be quarrelsome and to take offence. On April 15th after some trivial dispute, in which he had been much excitfd, he had a fit, and again the next day he had a second. He was therefoie readmitted into St. George’s Hospital. He remained there until April 22nd, when he was discharged to go to his own home at Maidstone. He promised to return to the hospital if he had any more fits, but he has not made his appearance. STANLEY HOSPITAL, LIVERPOOL. SEQUEL OF THE CASE OF GASTRO-ENTEROSTOMY AND JEJUNOSTOMY; DEATH FROM INTERNAL HERNIA. (Under the care of Mr. LARKIN.) WE give the final result of the operative measures under- taken for the relief of this patient. The earlier notes were published in THE LANCET of July llth and Sept. 19th of this year. Our readers will recollect also that much discus- sion ensued after the publication of the second part of the case as to the reason why the symptoms had returned. Jane G-, aged forty-seven, had symptoms of pyloric obstruction from July, 1890. On May 22nd, 1891, Mr. Larkin performed gastro-enterostomy, which completely relieved the symptoms for eight weeks, when they returned, and on Aug. 4th jejunostomy was performed, and the patient fed on milk, eggs, &c., through a catheter. She did well, and left the hospital much relieved on Sept. 13th. When at home she thought she would try to take food again by the mouth. She took a cup of tea, and, finding this did not come back, tried bread-and-butter, milk, rice pudding, minced meat, fish, &c. As she did not vomit, felt well, and her bowels were regular, she withdrew the catheter from the jejunostomy aperture, and took food only by the mouth. About the commencement of October she began to feel weaker and ill. She took to her bed, and a few days later a bedsore appeared over the coccyx and spread rapidly. On October 12th she was readmitted to the hospital in very weak and emaciated state. There was a large bedsore over the region of the coccyx. Temperature normal ; bowels regular; slight yellow ooze from jejunal opening. Took liquid food by the mouth and was not sick. She continued in the same condition until Oct. 20th, when she was sick after everything she took, and had slight pain in the abdomen. Oct. 21st.-Vomiting continued. Bowels moved. 22nd.-Had no food, but vomited bile-stained fluid. Bowels moved. 23rd.-Condition the same. 24th.-Takes nothing. The least thing causes vomiting. Bowels not moved since the 22nd. No pain. At 5 P.M. she was suddenly seized with great pain in the abdomen, became collapsed, and died at 1 A.M. on the 25th. An examination of the body was made twenty-four hours after death. The points of interest are the following :-On opening the abdomen the peritoneal cavity was found to contain much thin faeces. There was a firm adhesion between the jejunum and the incision in the abdominal wall made in performing the gastro-enterostomy. The portion of jejunum selected in the jejunostomy was only from two to three inches above this adhesion, and a little over two feet from the part attached to the stomach. The piece of jejunum between these two attachments to the abdominal wall formed a little loop, and between this loop and the parietes the upper segment of jejunum had slipped. It was firmly nipped. The intestine above was greatly dilated, and had ruptured just above the seat of constriction. The intestine below was contracted. There was slight general peritonitis. After tying the aperture and washing out the abdomen, it was at once noticed that almost all the intestines were in front of the great omentum, and such cover as it gave to them was only on the left side, and due to its covering round their left border. Careful examination,. in fact, showed that all the small intestine had prolapsed through a large hole, three inches in diameter, situated in the great omentum and transverse mesocolon, lying just below the stomach and above the transverse colon (g in figure). The hole had smooth, round, strong edges, and through it passed superiorly the commencement of the jejunum, and inferiorly the ileum, about four inches from the ileo-csecal valve. This was obviously the hole made in these structures at the first operation. The stomach and intestines were then a, Cardiac margin of new growth. b, Pyloric margin of new growth. c, Ca3cum. d, Ascending colon. e, Dotted outline of transverse colon. f, Omentum majus. g, Aperture in great omentum and transverse mesocolon. h, Ileum. i, Jejunum. k, Communication with stomach. I, Mesentery, adherent to stomach. removed en masse. The lower end of the oesophagus wa then held on to the water-tap, and the stomach distended with water. The water flowed easily on into the intestines, but when the duodenum was pinched none passed, showing that the pylorus was patent, while the gastro-jejunal opening was not. The stomach was now opened along the lesser curvature; when partially opened the little finger could be easily passed through the pylorus. The wall of the greater part of the stomach was much thickened, varying from three-quarters to an inch and a quarter in thickness. From one-third to one-half of this thickness consisted of the greatly hypertrophied muscularis, while inside of this was a soft, white growth, with a rough, irregular surface. To the right it ceased abruptly at the duodenum, but to the left more gradually, ending along the lesser curvature at the cardiac- orifice, but along the growth some four to five inches from the oesophagus. The uninvolved cardiac end was of ordi- nary appearance. Careful search failed to detect any trace of the communication with the jejunum. The jejunal coil (fastened to the stomach at the operation) was now opened, and the silk threads used in the operation were at once recognised. Two of them passed into a small depression an eighth of an inch broad, while the other two passed
Transcript
1222
influence of ether, an incision was made down either side ofthe scar and it was dissected off the bone. When this hadbeen done, a small punctured hole, not more than a third ofan inch in diameter, was found in the bone, situated in themiddle line of the frontal bone, immediately over the longi-tudinal sinus. This hole was filled up with dense fibroustissue. A crown of bone, including this hole, was nowremoved with the trephine, and the cicatricial tissue fillingit was seen to be intimately connected with the dura mater.This was carefully dissected off. There was no splinteringof the internal table of the skull, nor anything causingundue pressure on the membranes of the brain. The woundwas closed and dressed.After the operation the man seemed much brighter and
better, and volunteered the statement that he felt betterthan he had done for some time, and had entirely lost thesensation of tightness and pain in his head. His tempera-ture was normal, and remained so throughout the futureprogress of the case. On March 20th the wound wasdressed and found to be healed. He was allowed to get up.He seemed brighter, and said that he had entirely lost theold pain in the head. On April 8th he was sent to theAtkinson Morley Convalescent Hospital. He seemed tohave qaite recovered from the operation and complained ofno pain. He was still odd and irrational in his manner,inclined to be quarrelsome and to take offence. OnApril 15th after some trivial dispute, in which he had beenmuch excitfd, he had a fit, and again the next day he hada second. He was therefoie readmitted into St. George’sHospital. He remained there until April 22nd, when hewas discharged to go to his own home at Maidstone. Hepromised to return to the hospital if he had any more fits,but he has not made his appearance.
STANLEY HOSPITAL, LIVERPOOL.SEQUEL OF THE CASE OF GASTRO-ENTEROSTOMY AND
JEJUNOSTOMY; DEATH FROM INTERNAL HERNIA.
(Under the care of Mr. LARKIN.)WE give the final result of the operative measures under-
taken for the relief of this patient. The earlier notes were
published in THE LANCET of July llth and Sept. 19th ofthis year. Our readers will recollect also that much discus-sion ensued after the publication of the second part of thecase as to the reason why the symptoms had returned.Jane G-, aged forty-seven, had symptoms of pyloric
obstruction from July, 1890. On May 22nd, 1891, Mr.Larkin performed gastro-enterostomy, which completelyrelieved the symptoms for eight weeks, when they returned,and on Aug. 4th jejunostomy was performed, and the patientfed on milk, eggs, &c., through a catheter. She did well,and left the hospital much relieved on Sept. 13th. Whenat home she thought she would try to take food again bythe mouth. She took a cup of tea, and, finding this did notcome back, tried bread-and-butter, milk, rice pudding,minced meat, fish, &c. As she did not vomit, felt well, andher bowels were regular, she withdrew the catheter fromthe jejunostomy aperture, and took food only by the mouth.About the commencement of October she began to feelweaker and ill. She took to her bed, and a few days latera bedsore appeared over the coccyx and spread rapidly.On October 12th she was readmitted to the hospital in
very weak and emaciated state. There was a large bedsoreover the region of the coccyx. Temperature normal ; bowelsregular; slight yellow ooze from jejunal opening. Tookliquid food by the mouth and was not sick. She continuedin the same condition until Oct. 20th, when she was sickafter everything she took, and had slight pain in theabdomen.
Oct. 21st.-Vomiting continued. Bowels moved.22nd.-Had no food, but vomited bile-stained fluid.
Bowels moved.23rd.-Condition the same.24th.-Takes nothing. The least thing causes vomiting.
Bowels not moved since the 22nd. No pain. At 5 P.M. shewas suddenly seized with great pain in the abdomen,became collapsed, and died at 1 A.M. on the 25th.An examination of the body was made twenty-four hours
after death. The points of interest are the following :-Onopening the abdomen the peritoneal cavity was found tocontain much thin faeces. There was a firm adhesion
between the jejunum and the incision in the abdominalwall made in performing the gastro-enterostomy. Theportion of jejunum selected in the jejunostomy was
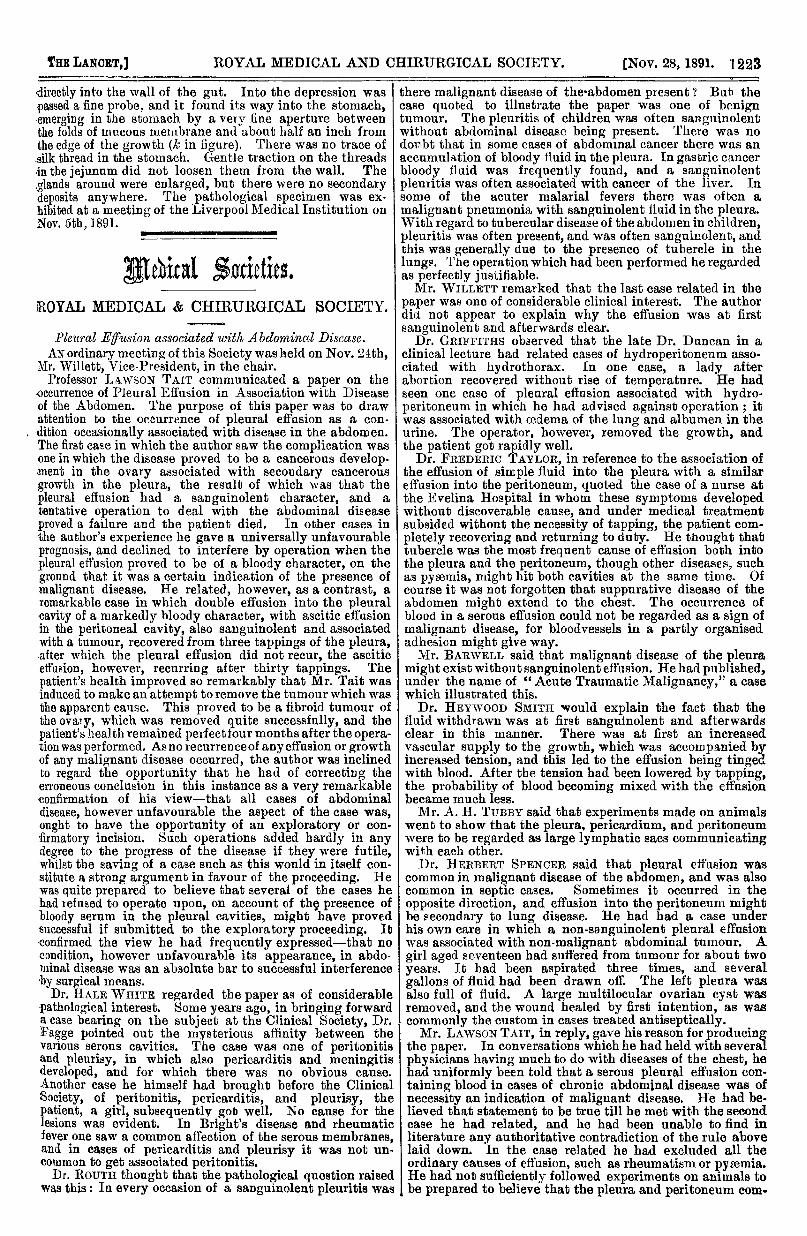
only from two to three inches above this adhesion, anda little over two feet from the part attached to the stomach.The piece of jejunum between these two attachments to theabdominal wall formed a little loop, and between this loopand the parietes the upper segment of jejunum had slipped.It was firmly nipped. The intestine above was greatlydilated, and had ruptured just above the seat of constriction.The intestine below was contracted. There was slightgeneral peritonitis. After tying the aperture and washingout the abdomen, it was at once noticed that almost all theintestines were in front of the great omentum, and suchcover as it gave to them was only on the left side, and dueto its covering round their left border. Careful examination,.in fact, showed that all the small intestine had prolapsedthrough a large hole, three inches in diameter, situated in thegreat omentum and transverse mesocolon, lying just belowthe stomach and above the transverse colon (g in figure). Thehole had smooth, round, strong edges, and through it passedsuperiorly the commencement of the jejunum, and inferiorlythe ileum, about four inches from the ileo-csecal valve.This was obviously the hole made in these structures at thefirst operation. The stomach and intestines were then
a, Cardiac margin of new growth. b, Pyloric margin of newgrowth. c, Ca3cum. d, Ascending colon. e, Dotted outlineof transverse colon. f, Omentum majus. g, Aperture in greatomentum and transverse mesocolon. h, Ileum. i, Jejunum.k, Communication with stomach. I, Mesentery, adherent tostomach.
removed en masse. The lower end of the oesophagus wathen held on to the water-tap, and the stomach distendedwith water. The water flowed easily on into the intestines,but when the duodenum was pinched none passed, showingthat the pylorus was patent, while the gastro-jejunalopening was not. The stomach was now opened along thelesser curvature; when partially opened the little fingercould be easily passed through the pylorus. The wall ofthe greater part of the stomach was much thickened, varyingfrom three-quarters to an inch and a quarter in thickness.From one-third to one-half of this thickness consisted of thegreatly hypertrophied muscularis, while inside of this wasa soft, white growth, with a rough, irregular surface. To theright it ceased abruptly at the duodenum, but to the left moregradually, ending along the lesser curvature at the cardiac-orifice, but along the growth some four to five inches fromthe oesophagus. The uninvolved cardiac end was of ordi-nary appearance. Careful search failed to detect any traceof the communication with the jejunum. The jejunal coil(fastened to the stomach at the operation) was now opened,and the silk threads used in the operation were at oncerecognised. Two of them passed into a small depressionan eighth of an inch broad, while the other two passed
1223
directly into the wall of the gut. Into the depression waspassed a fine probe, and it found its way into the stomach,emerging in the stomach by a very fine aperture betweenthe folds of mucous membrane and about half an inch fromthe edge of the growth (A in figure). There was no trace ofsilk thread in the stomach. Gentle traction on the threadsin the jejunum did not loosen them from the wall. The,glands around were enlarged, but there were no secondarydeposits anywhere. The pathological specimen was ex-hibited at a meeting of the Liverpool Medical Institution onNov. 5the,1891.
_____________
Medical Societies.ROYAL MEDICAL & CHIRURGICAL SOCIETY.
Pleural Effusion associated with Abdominal Disease. IAN ordinary meeting of this Society was held on Nov. 24th, I
Mr. Willett, Vice-President, in the chair.Professor LAWSON TAIT communicated a paper on the
occurrence of Pleural Effusion in Association with Diseaseof the Abdomen. The purpose of this paper was to drawattention to the occurrence of pleural effusion as a con-
. dition occasionally associated with disease in the abdomen.The first case in which the author saw the complication wasone in which the disease proved to be a cancerous develop-ment in the ovary associated with secondary cancerousgrowth in the pleura, the result of which was that thepleural effusion had a sanguinolent character, and a
tentative operation to deal with the abdominal diseaseproved a failure and the patient died. In other cases inthe author’s experience he gave a universally unfavourableprognosis, and declined to interfere by operation when thepleural effusion proved to be of a bloody character, on theground that it was a certain indication of the presence ofmalignant disease. He related, however, as a contrast, aremarkable case in which double effusion into the pleuralcavity of a markedly bloody character, with ascitic effusionin the peritoneal cavity, also sanguinolent and associatedwith a tumour, recovered from three tappings of the pleura,.after which the pleural effusion did not recur, the asciticeffasion, however, recurring after thirty tappings. Thepatient’s health improved so remarkably that Mr. Tait wasinduced to make an attempt to remove the tumour which wasthe apparent cause. This proved to be a fibroid tumour ofthe ovary, which was removed quite successfully, and thepatient’s health remained perfect four months after the opera-tion was performed. As no recurrence of any effusion or growthof any malignant disease occurred, the author was inclinedto regard the opportunity that he had of correcting theerroneous conclusion in this instance as a very remarkableconfirmation of his view-that all cases of abdominaldisease, however unfavourable the aspect of the case was,ought to have the opportunity of an exploratory or con-firmatory incision. Such operations added hardly in anydegree to the progress of the disease if they were futile,whilst the saving of a case such as this would in itself con-stitute a strong argument in favour of the proceeding. Hewas quite prepared to believe that several of the cases hehad refused to operate upon, on account of thg presence ofbloody serum in the pleural cavities, might have provedsuccessful if submitted to the exploratory proceeding. It-confirmed the view he had frequently expressed-that nocondition, however unfavourable its appearance, in abdo-minal disease was an absolute bar to successful interferenceby surgical means.Dr. HALE WHITE regarded the paper as of considerable
-pathological interest. Some years ago, in bringing forwarda case bearing on the subject at the Clinical Society, Dr.Fagge pointed out the mysterious affinity between thevarious serous cavities. The case was one of peritonitisand pleurisy, in which also pericarditis and meningitisdeveloped, and for which there was no obvious cause.
Another case he himself had brought before the ClinicalSociety, of peritonitis, pericarditis, and pleurisy, thepatient, a girl, subsequently gob well. No cause for thelesions was evident. In Bright’s disease and rheumaticfever one saw a common affection of the serous membranes,and in cases of pericarditis and pleurisy it was not un-common to get associated peritonitis.
Dr. RouTH thought that the pathological question raisedwas this: In every occasion of a sanguinolent pleuritis was
there malignant disease of the-abdomen present ? Bab thecase quoted to illustrate the paper was one of benigntumour. The pleuritis of children was often sanguinolentwithout abdominal disease being present. There was nodoubt that in some cases of abdominal cancer there was anaccumulation of bloody fluid in the pleura. In gastric cancerbloody fluid was frequently found, and a sanguinolentpleuiitis was often associated with cancer of the liver. Insome of the acuter malarial fevers there was often amalignant pneumonia with sanguinolent fluid in the pleura.With regard to tubercular disease of the abdomen in children,pleuritis was often present, and was often sanguinolent, andthis was generally due to the presence of tubercle in thelungs. The operation which had been performed he regardedas perfectly justifiable.Mr. WILLETT remarked that the last case related in the
paper was one of considerable clinical interest. The authordid not appear to explain why the effusion was at firstsanguinolent and afterwards clear.
Dr. GRIFFITHS observed that the late Dr. Duncan in aclinical lecture had related cases of hydroperitoneam asso-ciated with hydrothorax, In one case, a lady afterabortion recovered without rise of temperature. He hadseen one case of pleural effusion associated with hydro-peritoneum in which he had advised against operation ; itwas associated with oedema of the lung and albumen in theurine. The operator, however, removed the growth, andthe patient got rapidly well.
Dr. FREDERIC TAYLOR, in reference to the association ofthe effusion of simple fluid into the pleura with a similareffusion into the peritoneum, quoted the case of a nurse atthe Evelina Hospital in whom these symptoms developedwithout discoverable cause, and under medical treatmentsubsided without the necessity of tapping, the patient com-pletely recovering and returning to duty. He thought thattubercle was the most frequent cause of effusion both intothe pleura and the peritoneum, though other diseases, suchas pyaemia, might hit both cavities at the same time. Ofcourse it was not forgotten that suppurative disease of theabdomen might extend to the chest. The occurrence ofblood in a serous effusion could not be regarded as a sign ofmalignant disease, for bloodvessels in a partly organisedadhesion might give way.Mr. BARWELL said that malignant disease of the pleura
might exist without sanguinolent effusion. He had published,under the name of " Acute Traumatic Malignancy," a casewhich illustrated this.
Dr. HEYWOOD SMITH would explain the fact that thefluid withdrawn was at first sanguinolent and afterwardsclear in this manner. There was at first an increasedvascular supply to the growth, which was accompanied byincreased tension, and this led to the effusion being tingedwith blood. After the tension had been lowered by tapping,the probability of blood becoming mixed with the effusionbecame much less.Mr. A. H. TUBBY said that experiments made on animals
went to show that the pleura, pericardium, and peritoneumwere to be regarded as large lymphatic sacs communicatingwith each other.
Dr. HERBERT SPENCER said that pleural effusion wascommon in malignant disease of the abdomen, and was alsocommon in septic cases. Sometimes it occurred in theopposite direction, and effusion into the peritoneum mightbe secondary to lung disease. He had had a case underhis own care in which a non-sanguinolent pleural effusionwas associated with non-malignant abdominal tumour. Agirl aged seventeen had suffered from tumour for about twoyears. It had been aspirated three times, and severalgallons of fluid had been drawn off. The left pleura wasalso full of fluid. A large multilocular ovarian cyst wasremoved, and the wound healed by first intention, as wascommonly the custom in cases treated antiseptically.Mr. LAWSON TAIT, in reply, gave his reason for producing
the paper. In conversations which he had held with severalphysicians having much to do with diseases of the chest, hehad uniformly been told that a serous pleural effusion con-taining blood in cases of chronic abdominal disease was ofnecessity an indication of malignant disease. He had be-lieved that statement to be true till he met with the secondcase he had related, and he had been unable to find inliterature any authoritative contradiction of the rule abovelaid down. In the case related he had excluded all theordinary causes of effusion, such as rheumatism or pyaemia.He had not sufficiently followed experiments on animals tobe prepared to believe that the pleura and peritoneum com-