JOURNALOF ELSEVIER Journal of Dermatological Science 11 (1996) 234-238 Dermatological Science Staphylococcus aureus infection on cut wounds in the mouse skin: experimental staphylococcal botryomycosis Hisanori Akiyama *, Hiroko Kanzaki, Joji Tada, Jir6 Arata Department of Dermatology, Okayama University Medical School, Shikata-cho 2-5-1, Okayama 700, Japan Received 25 January 1995; revision received 8 May 1995; accepted 25 May 1995 Abstract Staphylococcus aureus cells were inoculated on the cut wounds in the skin of cyclophosphamide-treated mice. Biopsy specimens were taken from three mice at 1, 3, 6, 12, 24, 36, 48 and 60 h after the inoculation and were examined by light and electron microscopies. One hour after the inoculation Staphylococcus aureus cells were seen around the cut wound and deeper into the subcutaneous tissue. By 6 h after the inoculation, Staphylococcus aureus cells formed clusters of bacterial colonies. By 36 h after the inoculation inflammatory cells, mainly polymorphonu- clear leukocytes and macrophages, were seen around the clusters. Electron microscopic examination revealed fibril-like structures around the Staphylococcus aureus cells at 1 h. The Staphylococcus aureus cells were enclosed in membrane-like structures at 3 h. The membrane-like structures and the fibril-like structures were positive for Ruthenium red. By 12 h after the inoculation, the membrane-like structures increased in thickness and in electron density. Inflammatory cells were seen around but outside of the membrane-like structures at 24, 36 and 48 h. At 60 h the tissues around the membrane-like structures were degenerated and almost necrotic. These results suggest that Staphylococcus aureus cells may form biofilm in dermal or subcutaneous tissues in a neutropenic condition. Keywords: Staphylococcus aureus; Glycocalyx; Biofilm; Experimental botryomycosis 1. Introduction Bacterial skin infections develop after the bacte- ria bind to skin tissues. Staphylococcus aureus cells bind to skin tissues through Staphylococcus aureus receptors to fibronectin [l-4] or through fibril-like structures [5,6]. The bacterial glycocalyx * Corresponding author, Tel.: 086 223 7151, ext 2510; Fax: 086 225 1640. is a polysaccharide-containing Ruthenium red- positive structure produced by bacteria bound to tissues or foreign bodies [7-lo]. Bacteria are en- veloped by glycocalyx and enclosed in membrane- like structures. These membrane-like bacterial layers are known as biofilms [11,12]. We inocu- lated Staphylococcus aureus cells suspension on the cut backs of cyclophosphamide-treated mice and observed the sequential events which occur between skin tissues, inflammatory cells and Staphylococcus aureus cells. 0923-181 l/96/$15.00 0 1996 Elsevier Science Ireland Ltd. All rights reserved SSDI 0923-1811(95)00448-Z
Transcript
JOURNALOF
ELSEVIER Journal of Dermatological Science 11 (1996) 234-238
Dermatological Science
Staphylococcus aureus infection on cut wounds in the mouse skin: experimental staphylococcal botryomycosis
Hisanori Akiyama *, Hiroko Kanzaki, Joji Tada, Jir6 Arata
Department of Dermatology, Okayama University Medical School, Shikata-cho 2-5-1, Okayama 700, Japan
Received 25 January 1995; revision received 8 May 1995; accepted 25 May 1995
Abstract
Staphylococcus aureus cells were inoculated on the cut wounds in the skin of cyclophosphamide-treated mice. Biopsy specimens were taken from three mice at 1, 3, 6, 12, 24, 36, 48 and 60 h after the inoculation and were examined by light and electron microscopies. One hour after the inoculation Staphylococcus aureus cells were seen around the cut wound and deeper into the subcutaneous tissue. By 6 h after the inoculation, Staphylococcus aureus cells formed clusters of bacterial colonies. By 36 h after the inoculation inflammatory cells, mainly polymorphonu- clear leukocytes and macrophages, were seen around the clusters. Electron microscopic examination revealed fibril-like structures around the Staphylococcus aureus cells at 1 h. The Staphylococcus aureus cells were enclosed in membrane-like structures at 3 h. The membrane-like structures and the fibril-like structures were positive for Ruthenium red. By 12 h after the inoculation, the membrane-like structures increased in thickness and in electron density. Inflammatory cells were seen around but outside of the membrane-like structures at 24, 36 and 48 h. At 60 h the tissues around the membrane-like structures were degenerated and almost necrotic. These results suggest that Staphylococcus aureus cells may form biofilm in dermal or subcutaneous tissues in a neutropenic condition.
Bacterial skin infections develop after the bacte- ria bind to skin tissues. Staphylococcus aureus cells bind to skin tissues through Staphylococcus aureus receptors to fibronectin [l-4] or through fibril-like structures [5,6]. The bacterial glycocalyx
is a polysaccharide-containing Ruthenium red- positive structure produced by bacteria bound to tissues or foreign bodies [7-lo]. Bacteria are en- veloped by glycocalyx and enclosed in membrane- like structures. These membrane-like bacterial layers are known as biofilms [11,12]. We inocu- lated Staphylococcus aureus cells suspension on the cut backs of cyclophosphamide-treated mice and observed the sequential events which occur between skin tissues, inflammatory cells and Staphylococcus aureus cells.
0923-181 l/96/$15.00 0 1996 Elsevier Science Ireland Ltd. All rights reserved SSDI 0923-1811(95)00448-Z
H. Akiyama et al. / Journal of Dermatological Science II (1996) 234-238 235
2. Materials and methods
2.1. Animals Five-week-old female mice of ddy-strain, weigh-
ing approximately 20 g, were purchased from Keari Co. (Osaka, Japan).
2.2. Bacterial strain A Staphylococcus aureus strain (labelled N strain)
isolated from a skin lesion of furunculosis was used. The N strain belonged to coagulase type IV [13] and phage type (1 x RTD) 80/77/8 1 (I.111 group), and contained a met A gene [14,15]. It was a non-producer of TSST-1 exfoliative toxin, p-toxin, b-toxin. It produced a-toxin and entero- toxin A.
2.3. Bacterial suspension for inoculation N strain was grown in 4 ml of tryptic soy broth
(Nissui Pharmaceutical Co.) at 37°C for 24 h without shaking. After the incubation, bacteria were harvested by centrifugation at 9000 x g for 10 min. The bacteria were resuspended in sterile saline solution and centrifuged as described above. Resuspension in sterile saline solution and centrifugation were repeated 3 times. Inoculum suspensions were prepared by resuspending the washed bacteria in 4 ml of sterile saline solution. The final suspension contained 3.7 x 10’ Staphy- lococcus aureus cells/ml.
2.4. Cyclophosphamide treatment Mice were made leukocytopenic by one in-
traperitoneal injection of cyclophosphamide (En- doxana, Shionogi Pharmaceutical Co., Osaka, Japan) in a dose of 3 mg/mouse 2 days before the bacterial inoculation. Mean peripheral white blood cell count (n = 3) was 1275 mm3 (control mice 6505/mm3).
2.5. Inoculation in mice The backs of cyclophosphamide-treated mice
were shaved by a razor blade and cut wounds 1 cm in length were produced by surgical blades (Feather@ No. 15). One hundred microliters of the bacterial suspension (3.7 x lo6 Staphylococcus aureus cells) were slowly applied through a mi- cropipette on the wounded area.
2.6. Studies of the skin lesions using light microscopy and electron microscopy
Biopsy specimens were obtained from the skin lesions at 1, 3, 6 12, 24, 36, 48 and 60 h after the bacterial inoculation. Three mice were tested at each point in time. Each biopsy specimen was divided into two pieces, one half for light mi- croscopy and the other half for electron mi- croscopy.
Specimens for light microscopy were fixed in 10% formalin solution and embedded in paraffin. Sections were stained with hematoxylin-eosin. Preparation of specimens for electron microscopi- cal examination was as follows. One halves of the specimens were fixed with 2% glutaraldehyde ca- codylate buffer (pH 7.4) for 3 h at 4°C and then the specimens were cut into 1 mm3 pieces. The fixed specimens were dehydrated with graduated ethanol solutions and embedded in Epon 812. Ultrathin sections were cut with a Porter Blum MT2-B (SOR VALL, CT, USA) and stained with 11.1% (w/v) uranyl acetate and 2.66% (w/v) lead citrate. The stained sections were examined by a JEM-100 SX electron microscope (JEOL, Ak- ishima. Japan). The other halves of the specimens were cut into 1 mm3 pieces and fixed with a mixture of 3.6% glutaraldehyde (0.5 ml) 0.2 M sodium cacodylate buffer (pH 7.4) (0.5 ml), and Ruthenium red (1.5 mg/ml) solution (0.5 ml) with shaking for 3 h at 4°C. The fixed specimens were washed with 0.1 M cacodylated buffer (pH 7.4) for 10 min 3 times and soaked in a mixture of 4% osmium tetroxide solution (0.5 ml), 0.2 M sodium cacodylated buffer (pH 7.4) (0.5 ml), and Ruthe- nium red (1.5 mg/ml) solution (0.5 ml) for 9 h at room temperature. The specimens were then washed with 0.1 M sodium cacodylate buffer (pH 7.4), dehydrated with graduated ethanol solution and embedded in Epon 812. The specimens were cut with a Porter Blum MT-2B and examined by a JEM- 1 OOSX electron microscope.
3. Results
3.1. Histopathological findings (Fig. 1) One hour after the inoculation, Staphylococcus
aureus cells were seen around the cut wound. By 3 h after the inoculation, Staphylococcus aureus cells
236 H. Akiyama et al. / Journal of Dermatological Science 11 (1996) 234-238
invaded the subcutaneous tissue and by 6 h after the inoculation Staphylococcus aureus cells formed clusters of bacterial colonies. By 36 h after the inoculation, inflammatory cells composed mainly of polymorphonuclear leukocytes and macro- phages were seen around the clusters formed by Staphylococcus aureus cells. By 60 h after the inoculation, inflammatory cells invaded partly the clusters of Staphylococcus aureus cells.
3.2. Electron microscopical jindings (Figs. 2-4) One hour after the inoculation, fibril-like struc-
tures were observed around the Staphylococcus aureus cells. By 3 h after the inoculation, the Staphylococcus aureus cells had formed micro- colonies. These microcolonies were enclosed in membrane-like structures. These membrane-like structures and the fibril-like structures were stained positive by Ruthenium red. By 12 h after the inoculation, the membrane-like structures in- creased in thickness and in electron density. At 24, 36 and 48 h after the inoculation, inflamma- tory cells were seen around the membrane-like structures but not invaded the membrane-like structures. As most inflammatory cells were de-
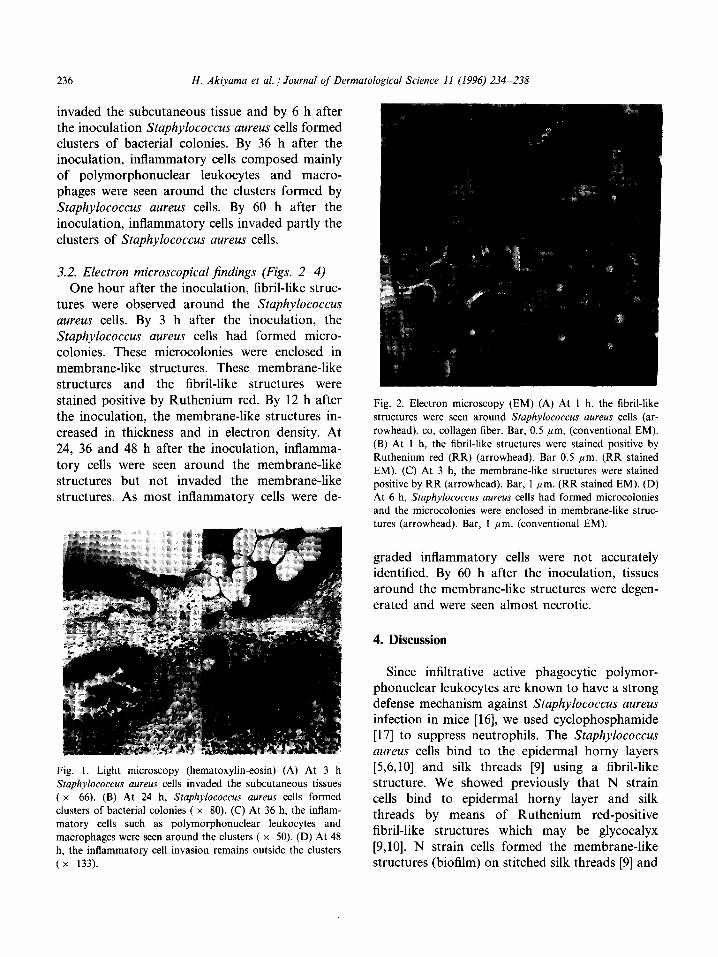
Fig. 1. Light microscopy (hematoxylin-eosin) (A) At 3 h Staphylococcus aureus cells invaded the subcutaneous tissues ( x 66). (B) At 24 h, Staphylococcus aureus cells formed clusters of bacterial colonies ( x 80). (C) At 36 h, the inflam- matory cells such as polymorphonuclear leukocytes and macrophages were seen around the clusters ( x 50). (D) At 48 h, the inflammatory cell invasion remains outside the clusters (x 133).
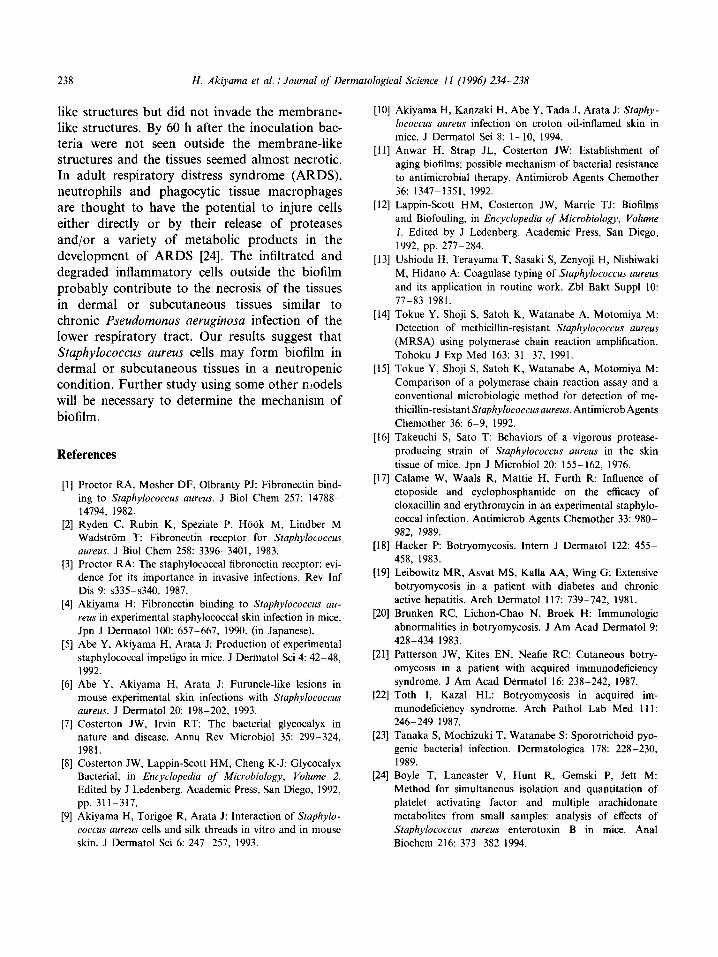
Fig. 2. Electron microscopy (EM) (A) At 1 h, the fibril-like structures were seen around Staphylococcus aureus cells (ar- rowhead). co, collagen fiber. Bar, 0.5 pm, (conventional EM). (B) At 1 h, the fibril-like structures were stained positive by Ruthenium red (RR) (arrowhead). Bar 0.5 pm. (RR stained EM). (C) At 3 h, the membrane-like structures were stained positive by RR (arrowhead). Bar, 1 pm. (RR stained EM). (D) At 6 h, Staphylococcus aureus cells had formed microcolonies and the microcolonies were enclosed in membrane-like struc- tures (arrowhead). Bar, 1 pm. (conventional EM).
graded inflammatory cells were not accurately identified. By 60 h after the inoculation, tissues around the membrane-like structures were degen- erated and were seen almost necrotic.
4. Discussion
Since infiltrative active phagocytic polymor- phonuclear leukocytes are known to have a strong defense mechanism against Staphylococcus aureus infection in mice [16], we used cyclophosphamide [ 171 to suppress neutrophils. The Staphylococcus aureus cells bind to the epidermal horny layers [5,6,10] and silk threads [9] using a fibril-like structure. We showed previously that N strain cells bind to epidermal horny layer and silk threads by means of Ruthenium red-positive fibril-like structures which may be glycocalyx [9,10]. N strain cells formed the membrane-like structures (biofilm) on stitched silk threads [9] and
H. Akiyama et al. / Journal of Dermatological Science II (1996) 234-238 237
on the basal lamina [lo]. In the present electron microscopic study the fibril-like structures and membrane-like structures in the dermal or subcu- taneous tissues were stained positive by Ruthe- nium red and inflammatory cells were seen around the membrane-like structures but not in- vaded the membrane-like structures. These find- ings indicate the possibility that these structures are a glycocalyx and a biofilm. We think that cyclophosphamide treatment is necessary for the formation of biofilms, because neutrophils phago- cytose the Staphylococcus aureus cells before the formation of biofilm in the mouse skin.
Botryomycosis is a chronic bacterial infection of the skin and the viscera, and literally means a bunch of grapes [l&23]. In the tissue reaction, the central area consists of a focus of suppuration within which bacterial granules can be found. These granules are the hallmark in the diagnosis of botryomycosis. The granules may be piled up in grape-like forms or may present club-like pro-
Fig. 3. Electron microscopy (EM) (A) At 12 h, the membrane- like structures increased in thickness and in electron density (arrowhead). co, collagen fiber. Bar, 1 pm. (conventional EM). (B),(C) At 24 h. the inflammatory cells were seen around the membrane-like structures but not invaded the membrane-like structures (arrowhead). n, nucleus. Bar, 1 pm. (RR stained EM). (D) At 36 h, outside the membrane-like structures, most inflammatory cells were degraded. n. nucleus. Bar, 1 pm. (RR stained EM).
Fig. 4. Electron microscopy (EM) (A) At 48 h Staphylococcus aureus cells were enclosed in the membrane-like structures (arrowhead). Bar, 1 pm. (RR stained EM). (B) At 48 h, outside the membrane-like structures, the degraded inflamma- tory cells were observed. n, nucleus. Bar, 1 pm. (RR stained EM). (C) At 60 h, Staphylococcus aureus cells were seen inside the thick membrane-like structures (arrowhead). co, collagen fiber. Bar, 1 pm. (conventional EM). (D) At 60 h, the tissues outside the membrane-like structures were degenerated and were seen almost necrotic. co, collagen fiber. Bar, 1 pm. (conventional EM).
jections or knobs. Around the area of the central suppuration, there is a non-specific, chronic infl- ammatory reaction that may contain a large num- ber of polymorphonuclear leukocytes and a small number of histiocytes and epitheloid cells. The most frequent causative organism is Staphylococ- cus aureus, but other agents Pseudomonas, Strep- tococcus, Escherichia coli may also be isolated. The pathogenesis is unknown, but some immuno- logical defects are probably underlying.
By 36, 48 and 60 h after the inoculation, the histological findings of central bacterial granules and inflammatory infiltrations around the gran- ules are similar to those of botryomycosis. The present model could be regarded as experimental staphylococcal botryomycosis. By 24, 36 and 48 h after the inoculation, inflammatory cells mainly composed of polymorphonuclear leukocytes infiltrated and degraded outside the membrane-
238 H. Akiyama et al. 1 Journal of Dermatological Science 1 I (1996) 234-238
like structures but did not invade the membrane- like structures. By 60 h after the inoculation bac- teria were not seen outside the membrane-like structures and the tissues seemed almost necrotic. In adult respiratory distress syndrome (ARDS), neutrophils and phagocytic tissue macrophages are thought to have the potential to injure cells either directly or by their release of proteases and/or a variety of metabolic products in the development of ARDS [24]. The infiltrated and degraded inflammatory cells outside the biofilm probably contribute to the necrosis of the tissues in dermal or subcutaneous tissues similar to chronic Pseudomonas aeruginosa infection of the lower respiratory tract. Our results suggest that Staphylococcus aweus cells may form biofilm in dermal or subcutaneous tissues in a neutropenic condition. Further study using some other models will be necessary to determine the mechanism of biofilm.
References
[I] Proctor RA, Mosher DF, Olbranty PJ: Fibronectin bind- ing to Staphylococcus aureus. J Biol Chem 257: 14788- 14794, 1982.
[2] Ryden C, Rubin K, Speziale P, Hook M, Lindber M Wadstrom T: Fibronectin receptor for Staphylococcus aureus. J Biol Chem 258: 339663401, 1983.
[3] Proctor RA: The staphylococcal fibronectin receptor: evi- dence for its importance in invasive infections. Rev Inf Dis 9: s335-~340, 1987.
[4] Akiyama H: Fibronectin binding to Staphylococcus au- reus in experimental staphylococcal skin infection in mice. Jpn J Dermatol 100: 657-667, 1990. (in Japanese).
[5] Abe Y, Akiyama H, Arata J: Production of experimental staphylococcal impetigo in mice. J Dermatol Sci 4: 42-48, 1992.
[6] Abe Y, Akiyama H, Arata J: Furuncle-like lesions in mouse experimental skin infections with Staphylococcus aureus. J Dermatol 20: 198-202, 1993.
[7] Costerton JW, Irvin RT: The bacterial glycocalyx in nature and disease. Annu Rev Microbial 35: 299-324, 1981.
[8] Costerton JW, Lappin-Scott HM, Cheng K-J: Glycocalyx Bacterial, in Encyclopedia of Microbiology, Volume 2. Edited by J Ledenberg. Academic Press, San Diego, 1992, pp. 31 l-317.
[9] Akiyama H, Torigoe R, Arata J: Interaction of Sraphylo- coccus aureus cells and silk threads in vitro and in mouse skin. J Dermatol Sci 6: 2477257, 1993.
[lo] Akiyama H, Kanzaki H, Abe Y, Tada J, Arata J: Staphy- lococcus aureus infection on croton oil-inflamed skin in mice. J Dermatol Sci 8: l-10, 1994.
[Ill Anwar H, Strap JL, Costerton JW: Establishment of aging biofilms: possible mechanism of bacterial resistance to antimicrobial therapy. Antimicrob Agents Chemother 36: 1347-1351, 1992.
[I21 Lappin-Scott HM, Costerton JW, Marrie TJ: Biofilms and Biofouling, in Encyclopedia of Microbiology, Volume I. Edited by J Ledenberg. Academic Press, San Diego, 1992, pp. 277-284.
[13] Ushioda H, Terayama T, Sasaki S, Zenyoji H, Nishiwaki M, Hidano A: Coagulase typing of Staphylococcus aureus and its application in routine work. Zbl Bakt Suppl 10: 77783 1981.
[14] Tokue Y, Shoji S, Satoh K, Watanabe A, Motomiya M: Detection of methicillin-resistant Staphylococcus aureus (MRSA) using polymerase chain reaction amplification. Tohoku J Exp Med 163: 31-37, 1991.
[15] Tokue Y, Shoji S, Satoh K, Watanabe A, Motomiya M: Comparison of a polymerase chain reaction assay and a conventional microbiologic method for detection of me- thicillin-resistant Staphylococcusaureus. Antimicrob Agents Chemother 36: 6-9, 1992.
[I61 Takeuchi S, Sato T: Behaviors of a vigorous protease- producing strain of Staphylococcus aureus in the skin tissue of mice. Jpn J Microbial 20: l55- 162, 1976.
[I71 Calame W, Waals R, Mattie H, Furth R: Influence of etoposide and cyclophosphamide on the efficacy of cloxacillin and erythromycin in an experimental staphylo- coccal infection. Antimicrob Agents Chemother 33: 980- 982, 1989.
[19] Leibowitz MR, Asvat MS, KaIla AA, Wing G: Extensive botryomycosis in a patient with diabetes and chronic active hepatitis. Arch Dermatol 117: 739-742, 1981.
[20] Brunken RC, Lichen-Chao N, Broek H: Immunologic abnormalities in botryomycosis. J Am Acad Dermatol 9: 4288434 1983.
[21] Patterson JW, Kites EN, Neafie RC: Cutaneous botry- omycosis in a patient with acquired immunodeficiency syndrome. J Am Acad Dermatol 16: 238-242, 1987.
[22] Toth I, Kazal HL: Botryomycosis in acquired im- munodeficiency syndrome. Arch Pathol Lab Med 111: 246-249 1987.
[24] Boyle T, Lancaster V, Hunt R, Gemski P, Jett M: Method for simultaneous isolation and quantitation of platelet activating factor and multiple arachidonate metabolites from small samples: analysis of effects of Staphylococcus aureus enterotoxin B in mice. Anal Biochem 216: 373-382 1994.