Page 1
M. Böhm Innere Medizin III (Kardiologie / Angiologie / Internistische Intensivmedizin)
Universitätsklinikum des Saarlandes
Homburg/Saar
[email protected]
State of the Art of Drug Therapy in Heart Failure
-What is still missing?
Page 2
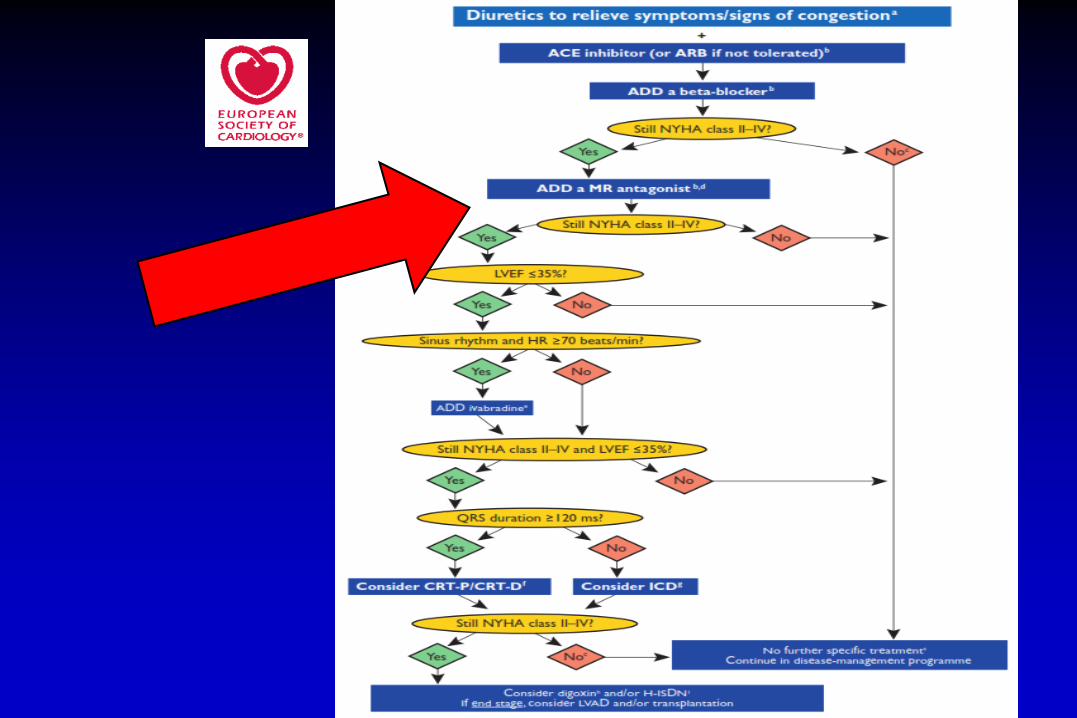
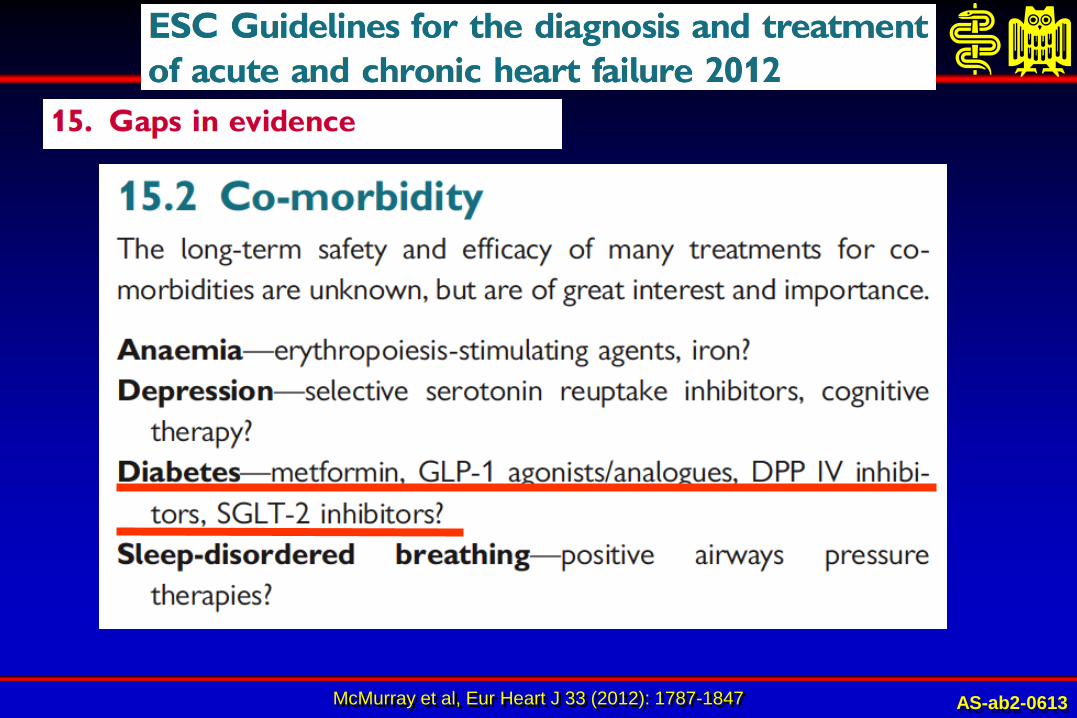
EHJ (2012) 33, 1787-1847
Page 5
23 trials in 19 209 HF patients with beta-blocker (mean EF=17%-36%)
McAlister et al. Ann Intern Med. 2009;150:784-794.
Beta-blocker dose and heart rate reduction in chronic HF patients
Results of 13 univariable meta-regressions evaluating the effect of individual covariates on mortality benefits
of beta-blockers in heart failure
Page 6
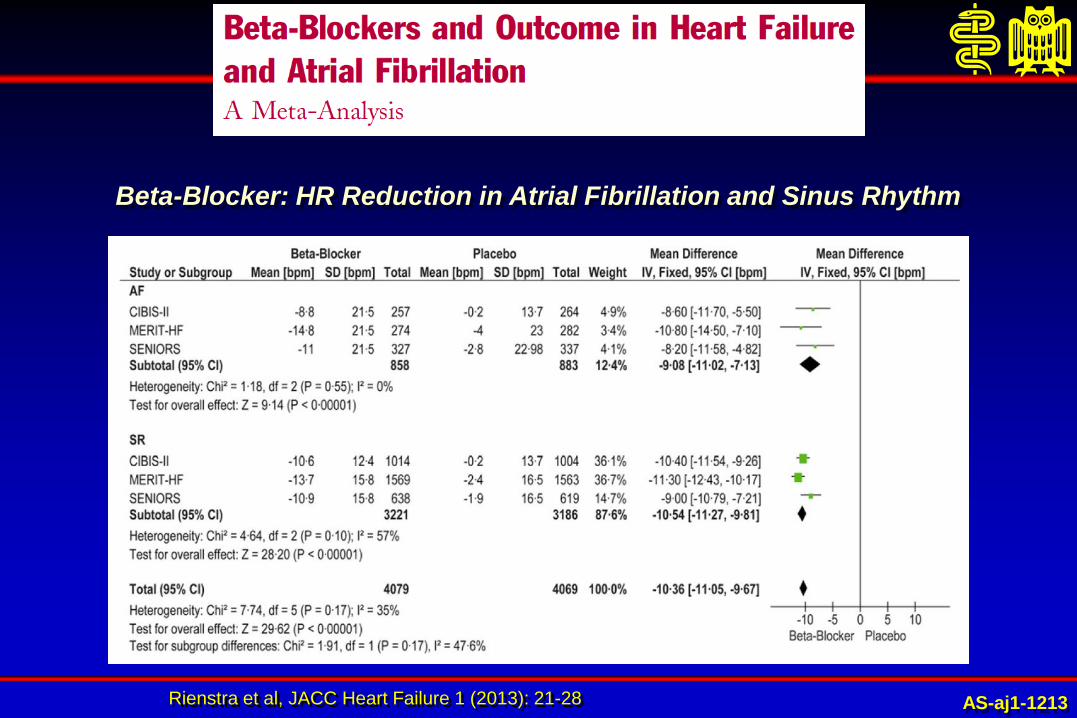
Rienstra et al, JACC Heart Failure 1 (2013): 21-28
Beta-Blocker: HR Reduction in Atrial Fibrillation and Sinus Rhythm
AS-aj1-1213
Page 7
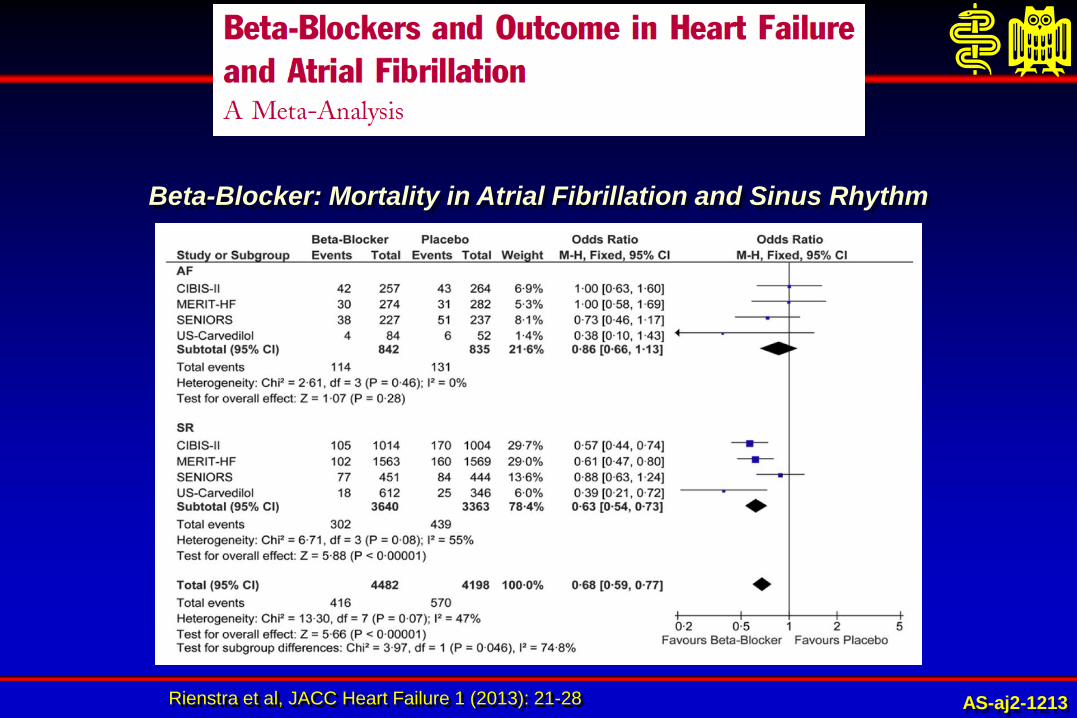
Rienstra et al, JACC Heart Failure 1 (2013): 21-28
Beta-Blocker: Mortality in Atrial Fibrillation and Sinus Rhythm
AS-aj2-1213
Page 8
Katecha et al, Lancet (2014): 10.1016/S0140-6736(14)61373-8
Survival
Page 9
Katecha et al, Lancet (2014): 10.1016/S0140-6736(14)61373-8
Survival
Page 10
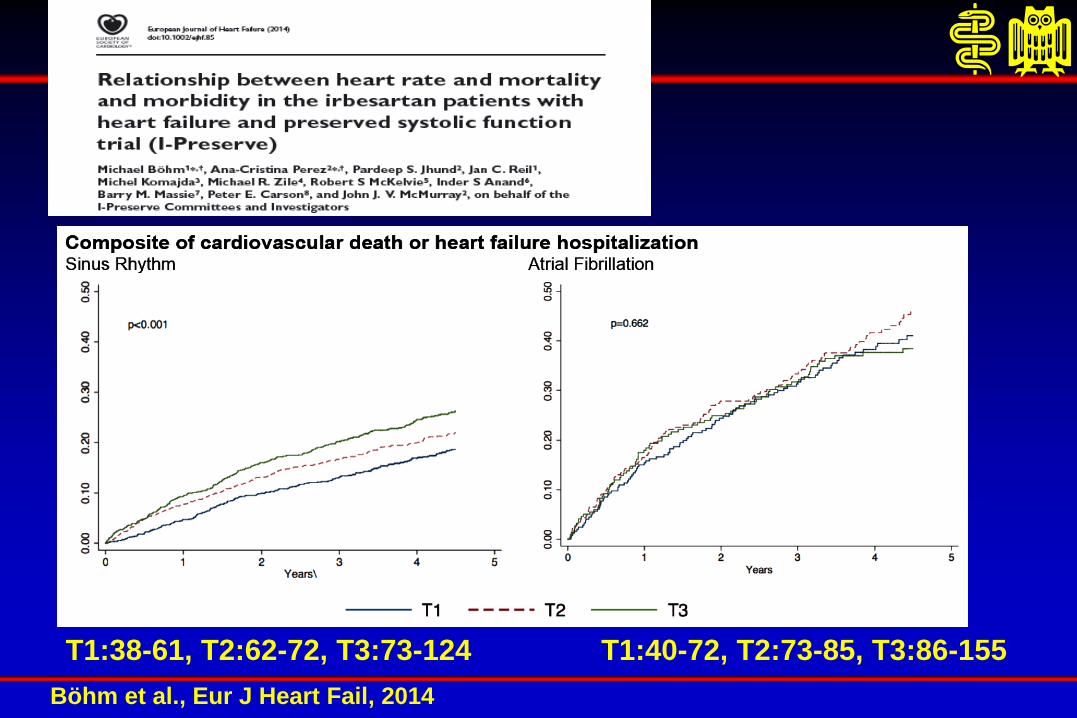
Böhm et al., Eur J Heart Fail, 2014
T1:38-61, T2:62-72, T3:73-124 T1:40-72, T2:73-85, T3:86-155
Page 11
Chronic Heart Failure
- What is missing?
- Prospective Study in AFib
- Most likely not applicable!
Page 13
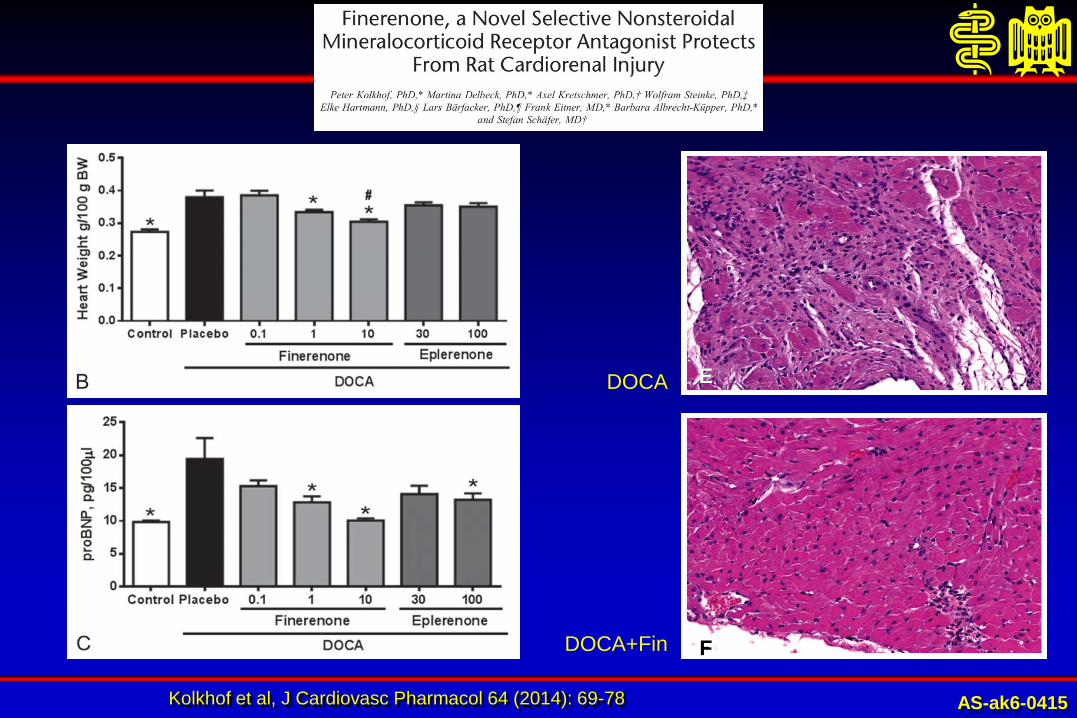
Kolkhof et al, J Cardiovasc Pharmacol 64 (2014): 69-78
DOCA E
DOCA+Fin F
AS-ak6-0415
Page 14
Results of ARTS-HF:
finerenone versus eplerenone in patients with worsening chronic heart failure
and diabetes and/or chronic kidney disease Gerasimos Filippatos, Stefan D Anker, Michael Böhm, Mihai Gheorghiade, Lars Køber, Henry Krum, Aldo P Maggioni, Piotr Ponikowski,
Adriaan A Voors, Faiez Zannad, So-Young Kim, Christina Nowack, Giovanni Palombo, Peter Kolkhof, Nina Kimmeskamp-Kirschbaum,
Alexander Pieper and Bertram Pitt,
for the MinerAlocorticoid Receptor AnTagonist Study In Heart Failure (ARTS-HF) Committees and Investigators
European Society of Cardiology Congress, 31 August 2015, London, UK AS-ag1-0815 AS-ag11-0815
Pro
ba
bilit
y o
f s
urv
iva
l (%
)
100
90
80
50
0 0
Finerenone 7.5–15 mg (n = 158)
Time (days)
Finerenone 10–20 mg (n = 160)
Finerenone 15–20 mg (n = 158)
Eplerenone (n = 207)
Finerenone 2.5–5 mg (n = 162)
Finerenone 5–10 mg (n = 157)
70
60
10 20 30 40 50 60 70 80 90 100 110 120
207
162
157
158
160
158
192
149
147
151
154
148
176
133
137
145
143
137
161
122
130
138
139
129
152
115
122
127
134
124
139
109
117
123
132
121
134
103
113
117
126
118
130
101
111
112
123
111
126
97
109
107
120
108
121
90
105
96
107
95
2
0
1
0
2
2
0
0
0
0
0
1
0
0
0
0
0
0
Study period Follow-up
Number at risk:
Eplerenone
Finerenone 2.5–5 mg
Finerenone 5–10 mg
Finerenone 7.5–15 mg
Finerenone 10–20 mg
Finerenone 15–20 mg
Page 15
Vardeny et al, Circ Heart Fail 7 (2014): 573-579
Page 16
Weir et al, N Engl J Med 372 (2015): 211-221
Time to First Recurrence of Hyperkalemia during the Randomized Withdrawal Phase
AS-aw3-0415
Page 17
Chronic Heart Failure
- What is missing?
Prospective Randomized Studies!
- GFR 15-45 ml/min below 30 ml/min!)
- Planned with Patiromir (SAPPHIRE; DIAMOND)
- Spiro plus Patiromir vs. Standard treatment
Page 19
Baseline heart rate is a predictor of endpoints on placebo
Primary composite endpoint: risk increases by 2.9% per 1-bpm increase, and by 15.6% per 5-bpm increase
50
40
30
20
10
0
0 6 12 18 24 30 Months
≥87 bpm
80 to <87 bpm
75 to <80 bpm
72 to <75 bpm
70 to <72 bpm
P<0.001
Patients with primary composite endpoint (%)
Böhm et al, Lancet 2010; 376: 886-894.
Stable CHF, SR > 70 bpm
Page 20
Prediction of Outcome by Discharge Heart Rate
- One Year Mortality -
Patients at high HR at Discharge had 41%
Increase in Mortality
Logeart D et al. Eur J Heart Failure 2012
Page 21
Ivabradine n=793 (14.5%PY) Placebo n=937 (17.7%PY)
HR = 0.82 p<0.0001
0 6 12 18 24 30
Months
40
30
20
10
0
Ivabradine
Placebo
- 18%
Cumulative frequency (%)
Primary composite endpoint
Swedberg et al, Lancet 376 (2010): 875-885
NNT=26 (annualized)
NYHA II-IV, SR > 70 bpm
Page 22
Pre-Discharge Management:
Targeting the Vulnerable Patient
Page 23
Estimated Treatment Effects of Ivabradine and Associated Numbers Needed to Treat (NNT) for SHIFT Outcomes
Rogers et al, (2015): submitted AS-al2-0715
Page 24
Rogers et al, (2015): submitted
1.0
HR (95% CI)
0.9 0.8 0.7 0.6
Primary Endpoint
1st HF Hospitalization
Recurrent HF Hospitalization
1st All-cause Hospitalization
Recurrent All-Cause Hospitalization
<0.0001
<0.0001
<0.0001
0.0036
<0.0001
26
27
14
37
10
P-Value NNT
Estimated Treatment Effects of Ivabradine and Associated Numbers Needed to Treat (NNT) for SHIFT Outcomes
AS-al1-0715
Page 25
Chronic Heart Failure
- What is missing?
- Once a day compound!
- EDIfY – Proof of concept in HFPEF
- Trial in Post Discharge Patients
Page 27
Regulation of Natriuretic Peptides, Bradykinin and Angiotensin II
Kidney
Blood vessels
Heart
Angiotensin II
Inactive products
Inactive products
Angiotensin I
Bradykinin
Natriuretic peptides
(ANP, BNP, CNP)
ACE
NEP
Cardioprotection
Vasodilation
Sodium
excretion
Hypertrophy
Vasoconstriction
Sodium Retention
{
Page 28
Concept of ARNIs : Pharmacologic Actions
Kidney
Blood vessels
Heart
Angiotensin II
Inactive products
Inactive products
Angiotensin I
Bradykinin
Natriuretic peptides
(ANP, BNP, CNP)
ACE Inhibition
NEP Inhibition
Cardioprotection
Vasodilation
Sodium
excretion
Hypertrophy
Vasoconstriction
Sodium Retention
{
Page 29
• The LCZ696 molecular structure comprises molecular moieties of the NEP
inhibitor pro-drug AHU377 and the AT-1 receptor blocker valsartan
• LCZ696 belongs to the novel ARNI class of compounds (Angiotensin
Receptor Neprilysin Inhibitors)
What is new? Molecular structure of LCZ696
Angiotensin Receptor Neprilysin Inhibitor (ARNI )
Page 30
Concentration time profiles for valsartan
Me
an
pla
sm
a c
on
ce
ntr
ati
on
(n
g/m
L)
0 6 12 18 24 30 36 42 48 54 60 66 72
0.3
1
10
30
100
300
1000
3000
10000
Time (h)
3 Valsartan 320 mg
LCZ696 400 mg
Parameter Geometric mean
ratio (90% CI)
Cmax (ng/mL)
0.98 (0.87–1.10)
AUC0–∞ (ng∙h/mL)
0.90 (0.82–0.99)
Gu et al. J Clin Pharm 2009
Similar valsartan exposures follow dosing of LCZ696
and corresponding doses of Diovan®
Page 31
At risk
Enalapril: 4212 3883 3579 2922 2123 1488 853 236
LCZ696: 4187 3922 3663 3018 2257 1544 896 249
Cu
mu
lati
ve P
rop
ort
ion
of
Pati
en
ts
wit
h P
rim
ary
En
d P
oin
t (%
)
Days after Randomization
0
10
20
30
40
0 180 360 540 720 900 1080 1260
HR: 0.80 (0.73, 0.87)
p = 0.0000002 1117 Enalapril
(n=4212)
LCZ696
(n=4187)
914
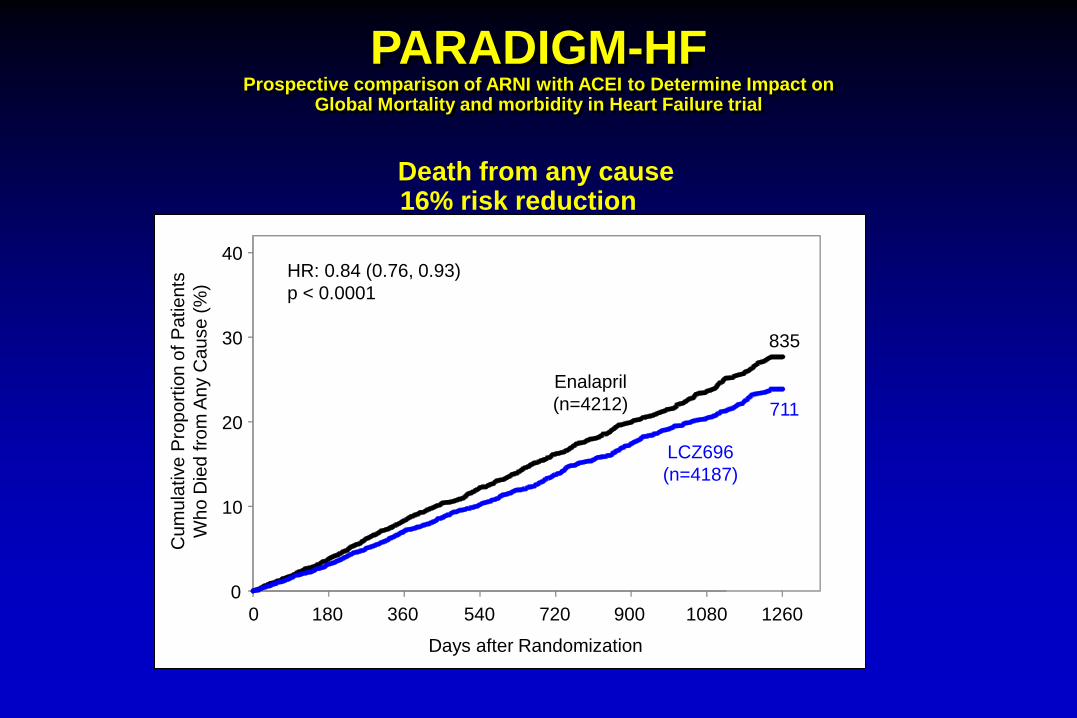
PARADIGM-HF: Primary outcome
Prospective comparison of ARNI with ACEI to Determine Impact on Global Mortality and morbidity in Heart Failure trial
Page 32
Death from CV causes 20% risk reduction
HF hospitalization 21% risk reduction
693
558
658
537
McMurray, Packer et al NEJM 2014
P = 0.00004 P = 0.00004
PARADIGM-HF
Prospective comparison of ARNI with ACEI to Determine Impact on Global Mortality and morbidity in Heart Failure trial
Page 33
Death from any cause 16% risk reduction
0
10
20
30
40
0 180 360 540 720 900 1080 1260
Enalapril
(n=4212)
835
LCZ696
(n=4187)
711
Days after Randomization
Cu
mu
lative
Pro
po
rtio
n o
f P
atie
nts
Wh
o D
ied
fro
m A
ny C
au
se
(%
)
HR: 0.84 (0.76, 0.93)
p < 0.0001
PARADIGM-HF
Prospective comparison of ARNI with ACEI to Determine Impact on Global Mortality and morbidity in Heart Failure trial
Page 34
LCZ696
(n=4187)
Enalapril
(n=4212)
p value
Hypotension (%)
symptoms
symptoms and SBP < 90 mmHg
14.0
2.7
9.2
1.4
< 0.001
<0.001
Renal impairment (%)
Cr ≥ 2.5 mg/dl
Cr ≥ 3.0 mg/dl
3.3
1.5
4.5
2.0
0.007
0.10
Hyperkalaemia (%)
K+ > 5.5 mmol/l
K+ > 6.0 mmol/l
16.2
4.3
17.4
5.6
0.15
0.007
Cough (%) 11.3 14.3 < 0.001
PARADIGM-HF: Safety
Page 35
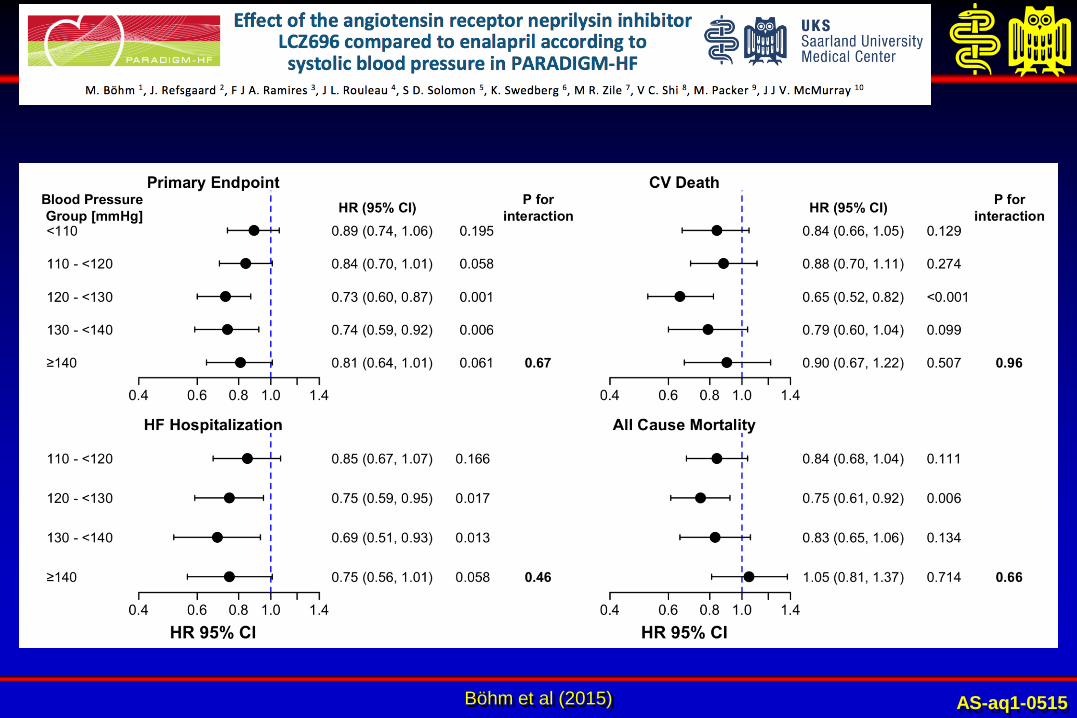
Böhm et al (2015) AS-aq1-0515
Page 36
McMurray et al (2015) AS-ap5-0515
Page 37
Simpson et al., JACC 66: 2059-71, 2015
Page 38
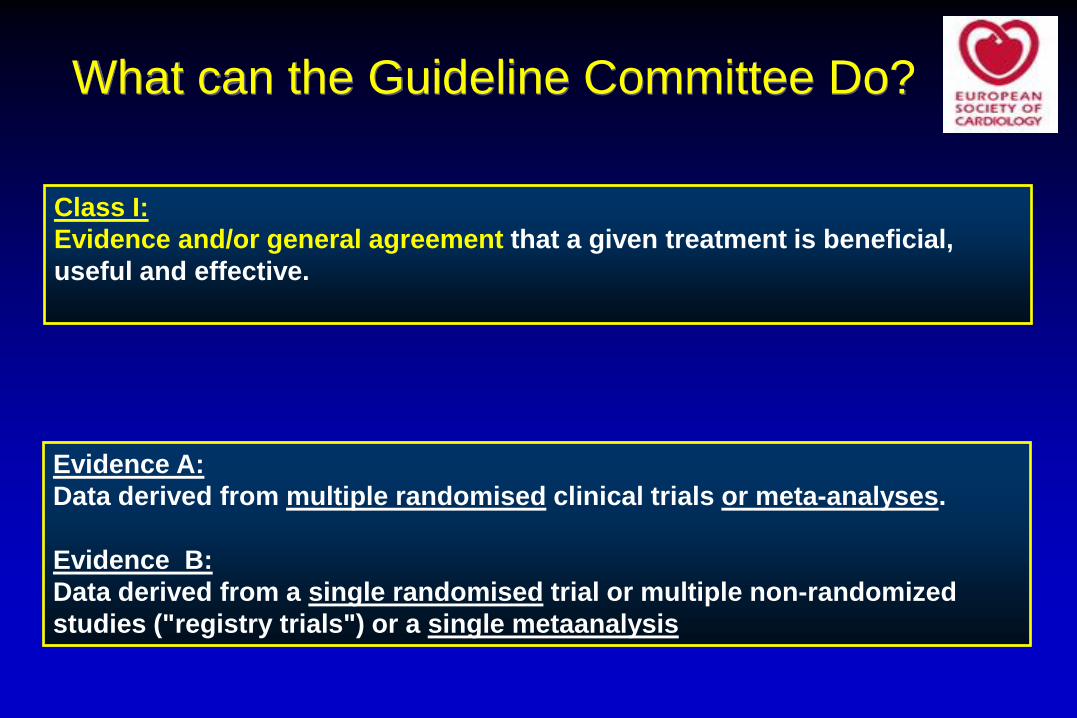
Class I:
Evidence and/or general agreement that a given treatment is beneficial,
useful and effective.
What can the Guideline Committee Do?
Evidence A:
Data derived from multiple randomised clinical trials or meta-analyses.
Evidence B:
Data derived from a single randomised trial or multiple non-randomized
studies ("registry trials") or a single metaanalysis
Page 39
Number of trials
with P < 0.05
showing efficacy
1
2
3
4
5
P value required
in a single trial to
provide same strength
of evidence
0.05
0.00125
0.00003125
0.00000078
0.0000000195
PARADIGM-HF
Effect on
primary endpoint
0.0000004
PARADIGM-HF
Effect on
cardiovascular death
Based on formula (0.025)n x 2 (personal communication Stuart Pocock)
0.00008
Levels of significance to obtain regulatory approval/change clinical practice
AS-at1-0515 McMurray et al., EHFA 2015
Page 40
Chronic Heart Failure
- What is missing?
- PARAGON in HFPEF Patients!
- New indications like resistant hypertension, CKD
- Once daily drug
Page 41
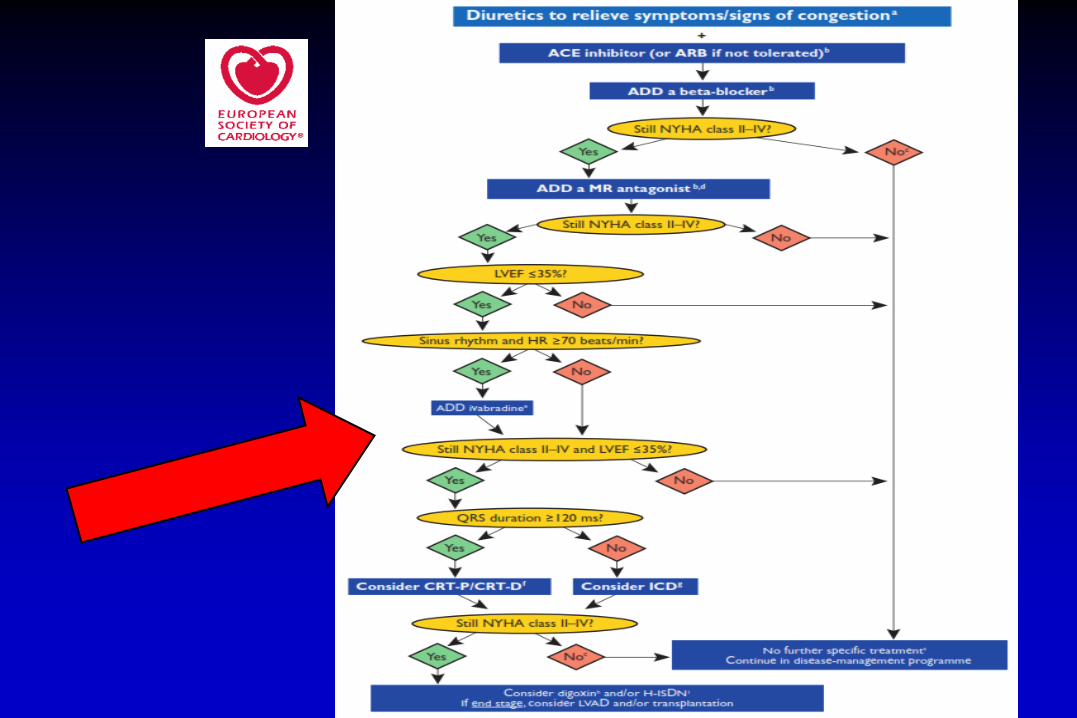
McMurray et al, Eur Heart J 33 (2012): 1787-1847 AS-ab2-0613
Page 42
AS-br-0608 Tenenbaum et al, Am J Med 114 (2003): 271-275
Risk of Diabetes Development in CHF
Page 43
AS-bp-0608 Smooke et al, Am Heart J 149 (2005): 168-174
Outcome:
Advanced
CHF
Page 44
Silverman M, Turner RJ. In: Windhager EE, ed. Handbook of Physiology, Vol. II. New York, NY: Oxford University Press; 1992:2017-2038.
0
200
400
600
0 200 400 600 800
Plasma glucose (mg/dL)
Glu
co
se
(m
g/m
in)
110 70
Normal
plasma
glucose
AS-aj12-0512
Glucose Filtration in Health and Disease
Page 45
Silverman M, Turner RJ. In: Windhager EE, ed. Handbook of Physiology, Vol. II. New York, NY: Oxford University Press; 1992:2017-2038.
0
200
400
600
0 200 400 600 800
Plasma glucose (mg/dL)
Tubular
reabsorption
TmG Transport Maximum Glu
co
se
(m
g/m
in)
110 70
Normal
plasma
glucose
Threshold
AS-aj12-0512
Glucose Filtration in Health and Disease
Page 46
Silverman M, Turner RJ. In: Windhager EE, ed. Handbook of Physiology, Vol. II. New York, NY: Oxford University Press; 1992:2017-2038.
0
200
400
600
0 200 400 600 800
Plasma glucose (mg/dL)
Tubular
reabsorption
TmG Glu
co
se
(m
g/m
in)
110 70
Normal
plasma
glucose Urine
Glucose
Threshold
Glucose in
urine
AS-aj12-0512
Glucose Filtration in Health and Disease
Page 47
Silverman M, Turner RJ. In: Windhager EE, ed. Handbook of Physiology, Vol. II. New York, NY: Oxford University Press; 1992:2017-2038.
0
200
400
600
0 200 400 600 800
Plasma glucose (mg/dL)
Tubular
reabsorption
TmG Glu
co
se
(m
g/m
in)
110 70
Normal
plasma
glucose Urine
Glucose
Threshold
negligible
glucose in
urine
Glucose in
urine
Elevated Plasma glucose
AS-aj12-0512
Glucose Filtration in Health and Disease
Page 48
Distal S3 Segment of the
proximal tubule
~10% glucose reabsorbed
transport by SGLT1
S1 Segment of the proximal
tubule
~90% Glucose reabsorbed
transport by SGLT2
No Glucose in Filtrate
Collecting
duct
Glomerular filtration
Proximal tubular reabsorbtion
Silverman M, Turner RJ. In: Windhager EE, ed. Handbook of Physiology, Vol. II. New York, NY: Oxford University Press; 1992:2017-2038.
Bakris GL, et al. Kidney Int. 2009;75:1272-1277.
Glucose
Glucose- Reabsorption Takes Place in the
Proximal Tubule
SGLT: sodium glucose transporter
Page 49
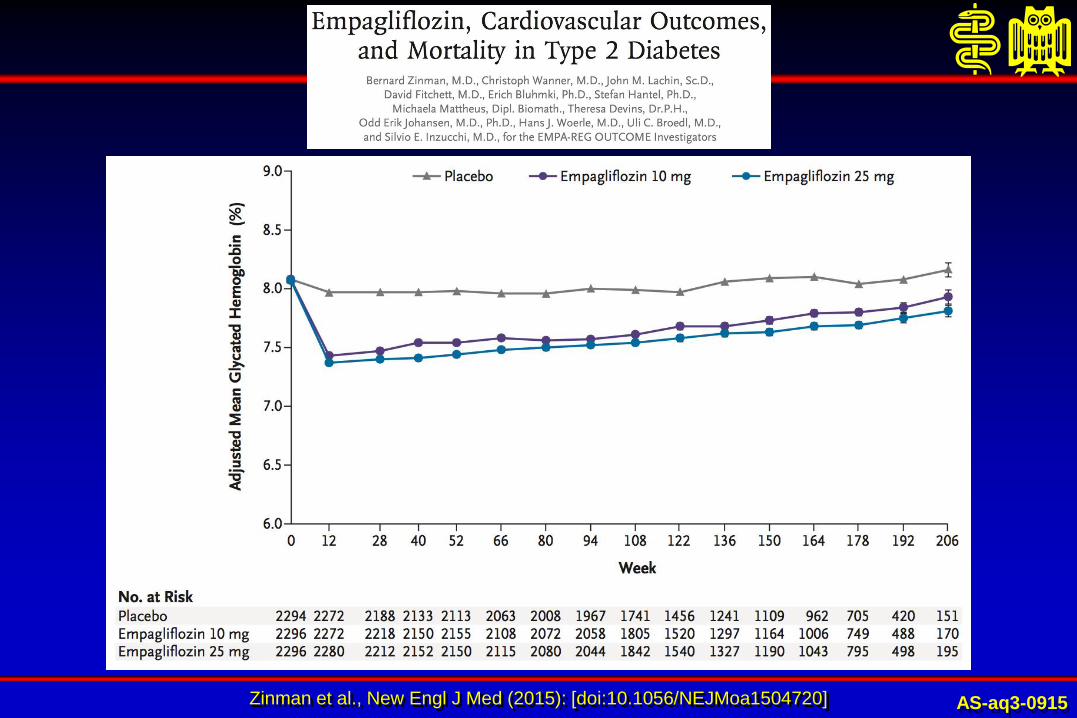
Zinman et al., New Engl J Med (2015): [doi:10.1056/NEJMoa1504720] AS-aq3-0915
Page 50
Zinman et al., New Engl J Med (2015): [doi:10.1056/NEJMoa1504720] AS-aq1-0915
Page 51
Zinman et al, N Engl J Med (Suppl.) [doi: 10.1056/NEJMoa1504720] AS-ac4-1115
Page 52
Zinman et al, N Engl J Med (Suppl.) [doi: 10.1056/NEJMoa1504720] AS-ac5-1115
Page 53
Zinman et al, N Engl J Med (Suppl.) [doi: 10.1056/NEJMoa1504720] AS-ac7-1115
Page 54
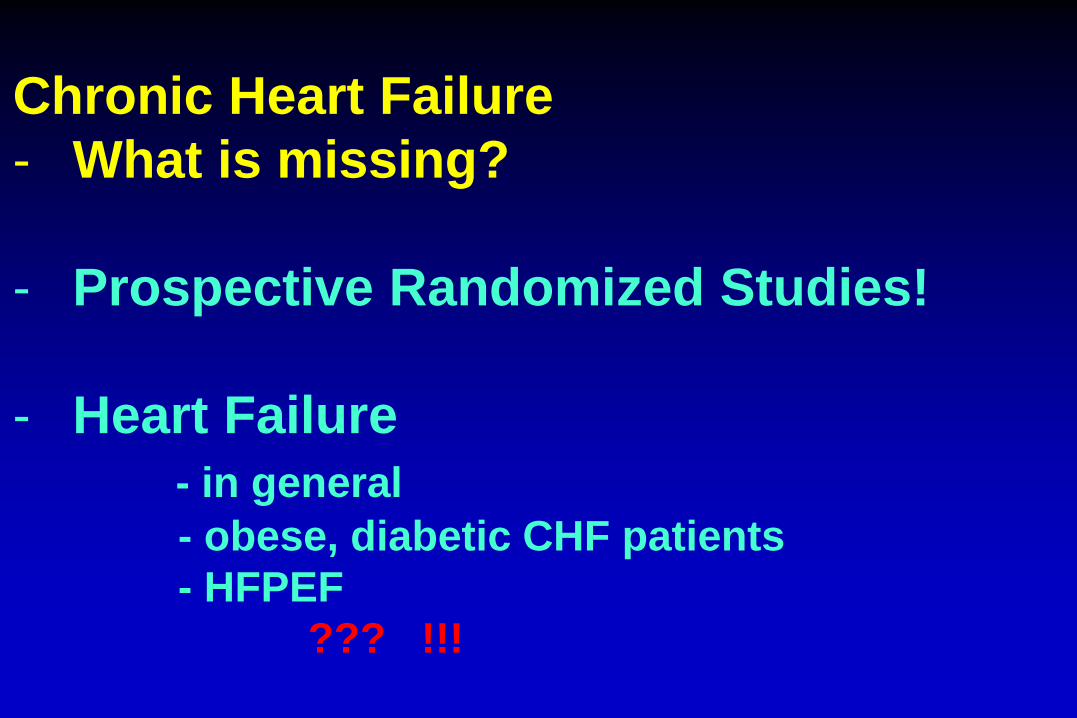
Chronic Heart Failure
- What is missing?
- Prospective Randomized Studies!
- Heart Failure
- in general
- obese, diabetic CHF patients
- HFPEF
??? !!!
Page 55
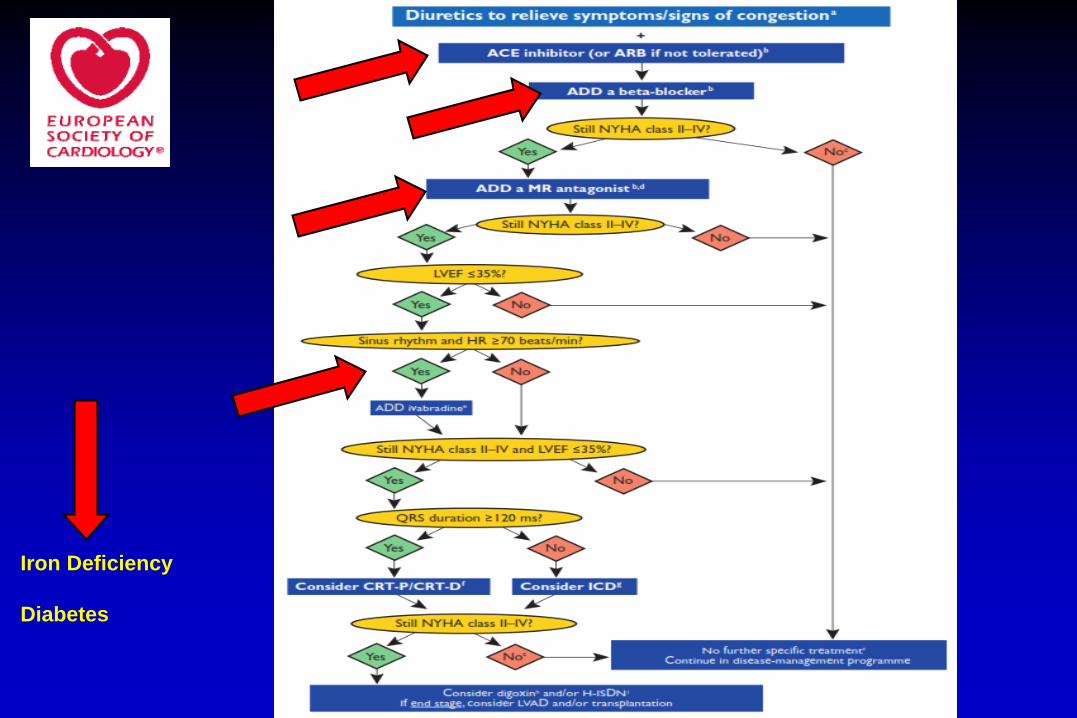
Iron Deficiency
Diabetes
Page 56
M. Böhm
Klinik für Innere Medizin III
Universitätsklinikum des Saarlandes
Homburg/Saar, Germany
Tel. 06841-16-23372
Fax. 06841-16-23369
[email protected]
Thank you!