Page 1
Status Status Status Status EpilepticusEpilepticusEpilepticusEpilepticus in Childrenin Childrenin Childrenin Children
Azhar Daoud
Professor of Child Neurology
Jordan Univ of science and Tech
Page 3
• Status epilepticus (SE) presents in a
multitude of forms, dependent on etiology
and patient age (myoclonic, tonic, subtle,
tonic-clonic, absence, complex partial etc.)
• Generalized, tonic-clonic SE is the most
common form of SE
• The following presentation refers to
generalized, tonic-clonic SE
Page 4
Definition
• Conventional definition:
– Single seizure > 30 minutes
– Series of seizures > 30 minutes without full
recovery
Page 5
Definition
– “If appropriate therapy is delayed, SE can cause
permanent neurologic sequelae or death …”
thus
– “ … any child who presents actively convulsing
should be assumed to have SE.”
Haafiz A. Pediatr Emerg Care 1999;15(2):119-29
Page 6
Types of Status
• Convulsive– Generalized convulsive status epilepticus (GCSE)
is the most common and the most dangerous form of SE
– If untreated, may progress to subtle status• Get an electromechanical dissociation (nonconvulsive)
• Nonconvulsive– Absence – considered benign
– Complex-partial – not benign; get cycling between levels of responsiveness and unresponsiveness
Page 7
The longer SE persists,
– the lower is the likelihood of spontaneous
cessation
– the harder is it to control
– the higher is the risk of morbidity and
mortality
Treatment for most seizures needs to be
instituted after > 5 minutes of seizure activity
Bleck TP. Epilepsia 1999;40(1):S64-6
Page 8
Climate and Geography• Jordan has a combination of Mediterranean and arid desert
climates, with Mediterranean prevailing in the North and West of
the country.
• while the majority of the country is desert. Generally, the country
has warm, dry summers and mild, wet winters
• The annual average temperatures ranges from 12 to 25 C
Petra
Page 9
Causes
• Fever
• Medication change
• Unknown
• Metabolic
• Congenital
• Anoxic
• Other (trauma, vascular,
infection, tumor, drugs)
36%
20%
9%
8%
7%
5%
15%
DeLorenzo RJ. Epilepsia 1992;33 Suppl 4:S15-25
Page 10
Drugs which can cause
seizures• Antibiotics
– Penicillins
– Isoniazid
– Metronidazole
• Anesthetics,
narcotics
– Halothane, enflurane
– Cocaine, fentanyl
– Ketamine
• Psychopharmaceuticals
– Antihistamines
– Antidepressants
– Antipsychotics
– Phencyclidine
– Tricyclic antidepressants
Page 11
Mortality
• Adults
• Children
15 to 22%
3 to 15%
Reviewed in: Fountain NB. Epilepsia 2000;41 Suppl 2:S23-30
Page 12
Prolonged seizures
Temporary
systemic
changes
Life
threatening
systemic
changes
Death
Page 13
Respiratory
• Hypoxia and hypercarbia
- ⇓⇓⇓⇓ ventilation (chest rigidity from muscle spasm)
- Hypermetabolism (⇑⇑⇑⇑ O2 consumption, ⇑⇑⇑⇑ CO2
production)
- Poor handling of secretions- Neurogenic pulmonary edema?
•• Hypoxia and Hypoxia and hypercarbiahypercarbia
-- ⇓⇓⇓⇓⇓⇓⇓⇓ ventilation (chest rigidity from muscle spasm)ventilation (chest rigidity from muscle spasm)
-- HypermetabolismHypermetabolism ((⇑⇑⇑⇑⇑⇑⇑⇑ OO22 consumption, consumption, ⇑⇑⇑⇑⇑⇑⇑⇑ COCO22
production)production)
-- Poor handling of secretionsPoor handling of secretions- Neurogenic pulmonary edema?
Page 14
Hypoxia
• Hypoxia/anoxia markedly increase
(triple?) the risk of mortality in SE
• Seizures (without hypoxia) are much
less dangerous than seizures and
hypoxia
Towne ARTowne AR. . EpilepsiaEpilepsia 1994;351994;35((11):):2727--3434
Page 15
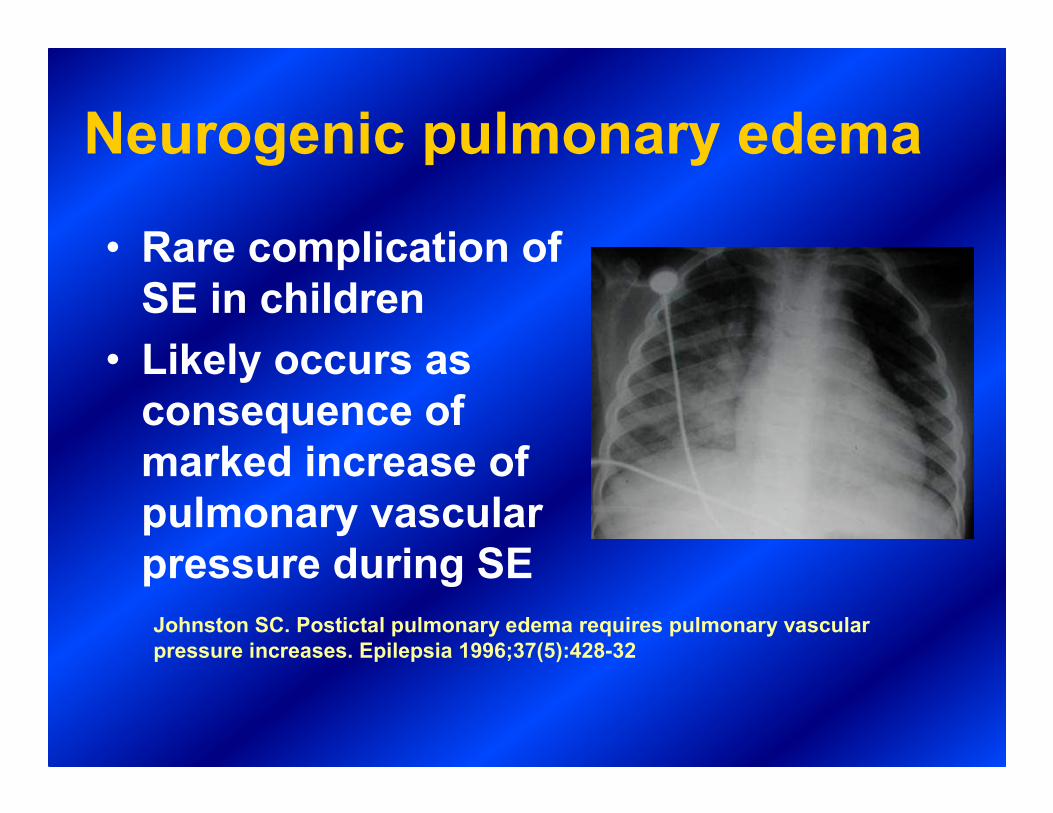
Neurogenic pulmonary edema
• Rare complication of
SE in children
• Likely occurs as
consequence of
marked increase of
pulmonary vascular
pressure during SE
Johnston SC. Postictal pulmonary edema requires pulmonary vascular
pressure increases. Epilepsia 1996;37(5):428-32
Page 16
Acidosis
• Respiratory
• Lactic
– Impaired tissue oxygenation
– Increased energy expenditure
Page 17
Hemodynamics
• Sympathetic
overdrive– Massive catecholamine /
autonomic discharge
– Hypertension
– Tachycardia
– High CVP
•Exhaustion
–Hypotension
–Hypoperfusion
0 min 60 min
Page 18
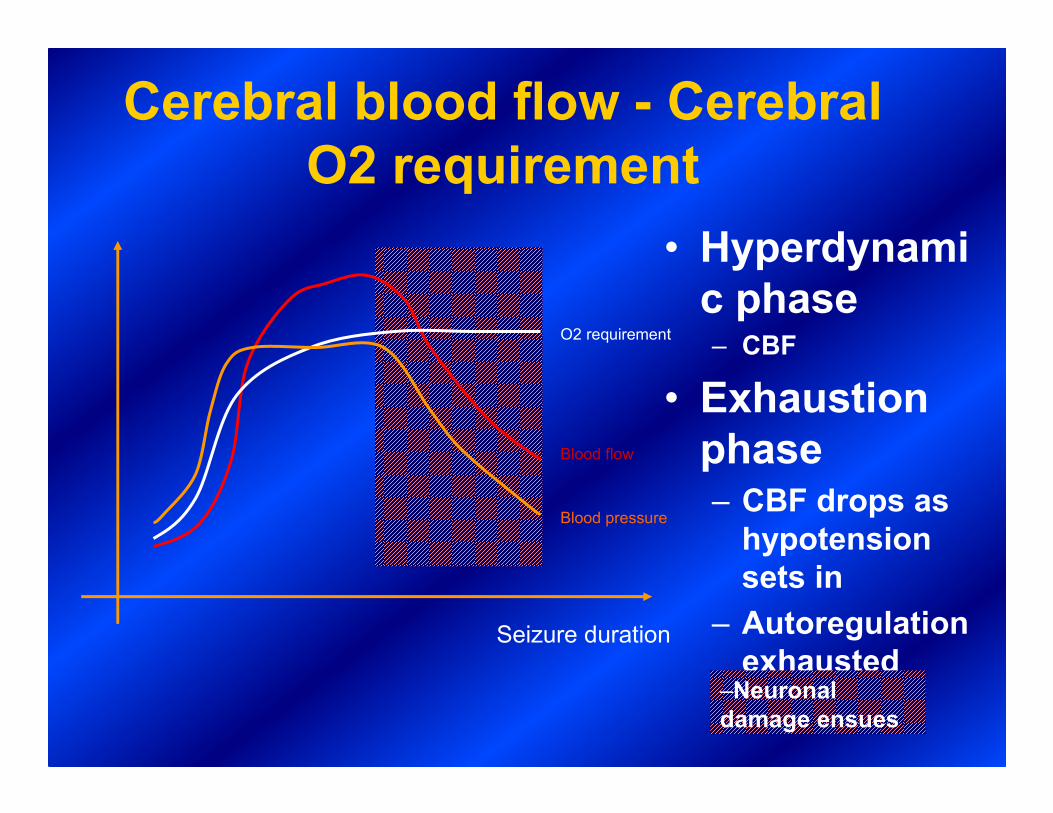
Cerebral blood flow - Cerebral
O2 requirement
• Hyperdynami
c phase – CBF
• Exhaustion
phase– CBF drops as
hypotension
sets in
– Autoregulation
exhausted
O2 requirement
Blood flow
Blood pressure
–Neuronal
damage ensues
Seizure duration
Page 19
Glucose
• Hyperdynamicphase – Hyperglycemia
• Exhaustion phase– Hypoglycemia
develops
– Hypoglycemia appears earlier in presence of hypoxia
Glucose
Seizure duration
30 min
SESE
SE + hypoxiaSE + hypoxia
Glucose
Seizure duration
30 min
SESE
SE + hypoxiaSE + hypoxia
–Neuronal damage
ensues
Page 20
Hyperpyrexia
• Hyperpyrexia may develop during
protracted SE, and aggravate possible
mismatch of cerebral metabolic
requirement and substrate delivery
• Treat hyperpyrexia aggressively
– Antipyretics, external cooling
– Consider intubation, relaxation, ventilation
Page 21
Other alterations
• Blood leukocytosis (50% of children)
• Spinal fluid leukocytosis (15% of children)
• ⇑ K+
• ⇑ creatine kinase
• Myoglobinuria
•• Blood Blood leukocytosisleukocytosis (50% of children)(50% of children)
•• Spinal fluid Spinal fluid leukocytosisleukocytosis (15% of children)(15% of children)
• ⇑ KK++
• ⇑ creatinecreatine kinasekinase
•• MyoglobinuriaMyoglobinuria
Page 22
First line
Oxygen, oral airway. Avoid
hypoxia!
Consider bag-valve mask
ventilation.
Consider intubation
IV/IO access. Treat hypotension, but
NOT hypertension
A
B
C
Page 24
Treatment
• Arterial blood gas?– All children in SE have acidosis. It often resolves
rapidly with termination of SE
• Intubate?– It may be difficult to intubate the actively seizing
child
– Stop or slow seizures first, give O2, consider BVM
ventilation
– If using paralytic agent to intubate, assume that
SE continues
Page 25
Initial investigations
• Labs
– Na, Ca, Mg, PO4 , glucose
– CBC
– Liver function tests, ammonia
– Anticonvulsant level
– Toxicology
Page 26
Initial investigations
• Lumbar puncture
– Always defer LP in unstable patient, but
never delay antibiotic/antiviral rx if
indicated
• CT scan
– Indicated for focal seizures or deficit,
history of trauma or bleeding d/o
Page 27
Treatment
• Give glucose (2-4 ml/kg D25%, infants 5
ml/kg D10%), unless normo- or
hyperglycemic
• Hyperglycemia has no negative effect in SE
(as long as significant hyperosmolality is being avoided)
Page 28
Treatment
• The longer you wait with anticonvulsant,
the more anticonvulsant you will need to
stop SE
• Most common mistake is ineffective dose
Page 29
Anticonvulsants
• Rapid acting
Plus
• Long acting
Page 30
Anticonvulsants - Rapid acting
• Benzodiazepines
– Lorazepam 0.1 mg/kg i.v. over 1-2 minutes
– Diazepam 0.2 mg/kg i.v. over 1-2 minutes
– If SE persists, repeat every 5-10 minutes
Page 31
Benzodiazepines
• Midazolam
– May be given i.m.
• Diazepam
– High lipid solubility
– Thus very rapid onset
– Redistributes rapidly
– Thus rapid loss of
anticonvulsant effect
– Adverse effects are
persistent:
• Hypotension
• Respir depression
•Lorazepam
–Low lipid solubility
–Action delayed 2 minutes
–Anticonvulsant effect 6-12 hrs
–Less respiratory depression than
diazepam
Page 32
Lorazepam Superiority
IV Treatment in Out-of-hospital SE
SE at Time of Arrival at the ER
Lorazepam Diazepam Placebo
SE terminated 39 (59.1%) 29 (42.6%) 15 (21.1%)
Ongoing SE 27 (40.9%) 39 (57.4%) 56 (78.9%)
Alldredge BK, et al. N Eng J Med. 2001.
Page 33
Anticonvulsants - Long acting
• Phenytoin– 20 mg/kg i.v. over 20
min
– pH 12
Extravasation causes severe tissue injury
– Onset 10-30 min
– May cause hypotension, dysrhythmia
– Cheap
• Fosphenytoin– 20 mg PE/kg i.v. over 5-7
min PE = phenytoin equivalent
– pH 8.6
Extravasation well tolerated
– Onset 5-10 min
– May cause hypotension
– Expensive
Page 34
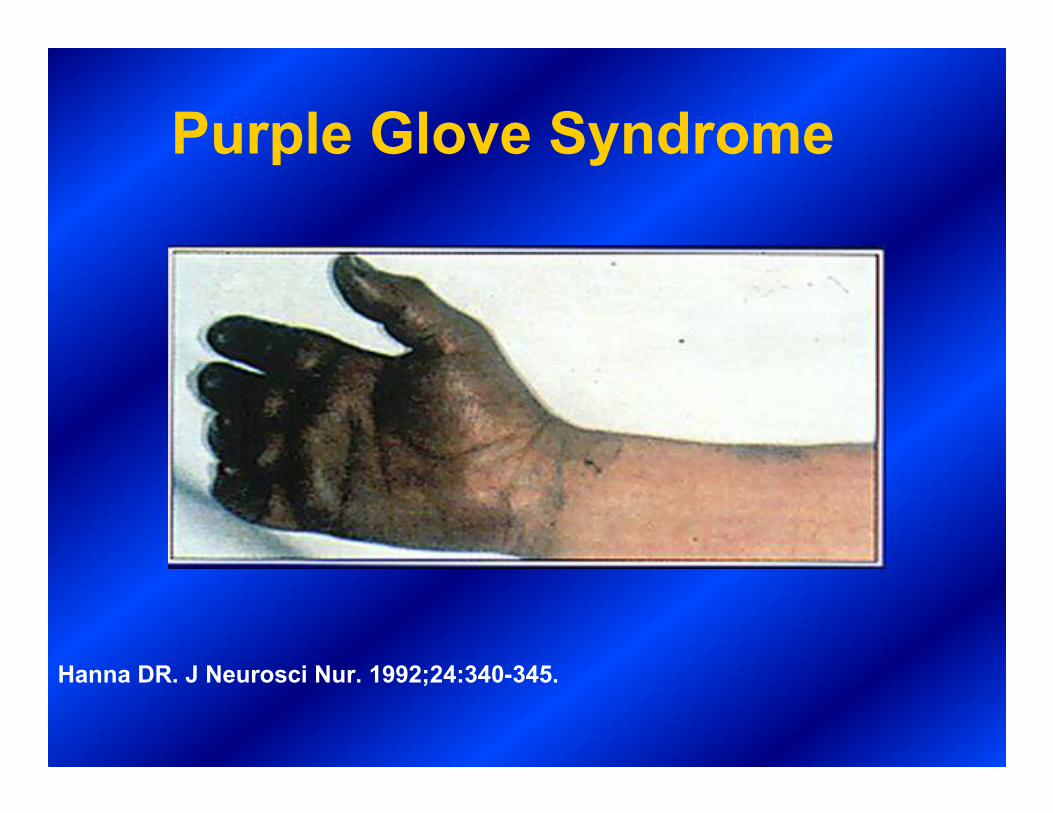
Cutaneous Reactions in Patients
Receiving IV Phenytoin: Purple Glove
Syndrome (PGS)• PGS = delayed, soft-tissue injury of the hand
and forearm following IV administration of phenytoin
• PGS is frequently, but not exclusively, associated with phenytoin extravasation
• PGS is characterized by pain, edema, and purplish discoloration
• Skin may blister or slough prior to resolution
�Retrospective study of 152 patients who received IV phenytoin over 3
months at the Mayo Clinic
–9 patients (5.9%) developed PGS
O'Brien TJ et al. Neurology. 1998;51:1034-1039.
Page 35
Purple Glove Syndrome
Hanna DR. J Neurosci Nur. 1992;24:340-345.
Page 36
Anticonvulsants - Long acting
• Phenobarbital
– 20 mg/k g i.v. over 10 - 15 min
– Onset 15-30 min
–May cause hypotension, respiratory
depression
Page 37
Third-Line Agents
Valoproat – load 20mg/kg at 3mg/kg/min
+no associations with hypotension or arrhythmias
+don’t need to place patient on monitor
+very few side effects even at high doses
-minimal data (80% effective in 2 trials)
Phenobarbital – load 15mg/kg at 100mg/min
+a lot of clinical experience with this
-prolonged sedation, hypotension, respiratory depression
Pentobarbital – like phenobarb. but faster acting, shorter t1/2
Propofol – don’t use in kids (metabolic acidosis and rhabdomyolysis)
-load 2mg/kg, then 5-10 mg/kg/hr
Page 38
65 70 75 80 85 90 95 100
Lorazepam 0.1 mg/kg by IV push (<2 mg/min)
0 5 10 15 20 25 30 35 40
Time (Minutes)
Start EEG; do not delay treatment unless EEG
necessary to verify diagnosis
Fosphenytoin 20 mg PE/kg (up to 150 mg PE/min).
If only phenytoin is available: 20 mg/kg (<50 mg/min)
Additional fosphenytoin 5-10 mg PE/kg
Phenobarbital (PB) 20 mg/kg
(<100 mg/min)
Midazolam 0.2 mg/kg bolus, then
0.05-0.5 mg/kg/hr
Seizures continue
Seizures continue
Seizures continue
OR
Induce barbiturate coma:
Pentobarbital (5-15 mg/kg) slowly as
loading dose, then 0.5-5 mg/kg/hr
Continuous infusion propofol
1 mg/kg over 5 min, then
2-4 mg/kg/hrOR
45 50 55 60
Seizures continue
Valproate 20 mg/kg
(3 mg/kg/min) is an
alternative to PBCall for help
Page 39
If SE persists
• Propofol infusion 5-10 mg/kg/hr after bolus 2 mg/kg
• Midazolam infusion 1 - 10 mcg/kg/min after bolus 0.15 mg/kg
• Pentobarbital infusion 1-3 mg/kg/hr after bolus 10 mg/kg
• Paraldehyde
• Isoflurane
• Leviteracetam? Lacosamide?
Page 40
Non - convulsive status
epilepticus
• How do you tell that patient’s seizures
have stopped?
Page 41
Non - convulsive SE ?
• Neurologic signs after termination of
SE are common:
– Pupillary changes
– Abnormal tone
– Babinski
– Posturing
– Clonus
–May be asymmetrical
Page 42
Non - convulsive SE ?
• Up to 20% of children with SE have non
- convulsive SE after tonic - clonic SE
Page 43
Non - convulsive SE ?
• If child does not begin to respond to
painful stimuli within 20 - 30 minutes
after tonic - clonic SE, suspect non -
convulsive SE
– Urgent EEG



















































![Focal hemodynamic patterns of status epilepticus detected ... · epilepticus or subtle status epilepticus [4]. Electroenceph-alogram (EEG), the diagnostic gold standard, may not be](https://static.documents.pub/doc/80x56/6074493ed430437ef144c30f/focal-hemodynamic-patterns-of-status-epilepticus-detected-epilepticus-or-subtle.jpg)



