54
STEM CELLS & AMNIOTIC MEMBRANE TO PROMOTE A RAPID HEALING OF ULCERS: RCT Hesham Al-Inany , Mirvat Ansary, Amr Gad Cairo University
| Date post: | 21-Aug-2015 |
| Category: |
Health & Medicine |
| Upload: | hesham-al-inany |
| View: | 610 times |
| Download: | 0 times |

STEM CELLS & AMNIOTIC MEMBRANE TO PROMOTE A RAPID HEALING OF ULCERS:RCT
Hesham Al-Inany, Mirvat Ansary, Amr Gad
Cairo University

WHAT IS THE PROBLEM?
Chronic leg ulcers are difficult to treat with long term sequelae

WHAT IS KNOWN ALREADY
closure of the chronic leg ulcer can be achieved but with limited functional repair due to scarring, long-standing co-morbidities.
OUTLINE
Why this research project? Point of research Methodology Results Extension of the study Implications
WHY THIS RESEARCH PROJECT?
Research strategic plan for 2012-2017 Focused on community based research targeting Multidisciplinary research

الطب لكلية البحثية للخطة الزمني الجدولالقاهرة 2017 / 2013جامعة

OUTLINE
Why this research project? Point of research Methodology Results Extension of the study Implications

MULTIDISCIPLINARY PROJECT
Surgery department Obstetrics & Gynecology department Clinical Pathology

IS THERE A RECENT TREND ?
Chronic leg ulcers often heal poorly if there is no re-vascularization.
Recent treatment modalities are based on development of angiogenesis and the use of growth factors to promote healing

WHY STEM CELLS?
Constant regeneration of the skin is achieved due to stem cell differentiation within the epidermis and the hair follicle. (Folia Histochemica et Cytobiologica 2011).

Tendogenesis/ Ligamentogenesis
Marrow Stroma
Transitory Fibroblast
Transitory Stromal Cell
Osteogenesis Chondrogenesis Myogenesis
MSC Proliferation
Transitory Osteoblast
Transitory Chondrocyte Myoblast
Myoblast Fusion
Unique Micro-niche
ChondrocyteOsteoblast
Other
Bo
ne
Mar
row
/Per
iost
eum
Mes
ench
ymal
Tis
sue
Proliferation
Commitment
Lineage Progression
Differentiation
Maturation
OsteocyteHypertrophic Chondrocyte
MyotubeStromal
CellsT/L
Fibroblast
Adipocytes, Dermal and Other Cells
BONE CARTILAGE MUSCLE MARROWTENDON/
LIGAMENTCONNECTIVE
TISSUE

MSC
S S Iyer & M Rojas: Expert Opin. Biol. Ther. (2008) 8:569-581.
IMMUNO-MODULATORY

EVIDENCE
Reports of autologous MSCs for the treatment of wounds in patients illustrate the efficacy of these cells for non-healing and/or difficult to heal wounds (Garcia-Olmo et al., 2010; Bey et al., 2010; Dash et al., 2009; Falanga et al., 2007; Lataillade et al., 2007; Yoshikawa et al., 2008)

WHY AMNIOTIC MEMBRANE ?
Amniotic membrane contain large quantity of growth factors.
AM down-regulates TGF-β and its receptor expression by fibroblasts and in doing so, reduce the risk of fibrosis. (Tseng et al., 1999; Lee et al., 2000).

POTENTIAL VALUES
no rejections; Simple and safe Minimal additional cost ??? rapid healing of ulcers

BASIC PROPERTIES OF AMNIOTIC MEMBRANE
1. Antiinflammatory effect - modulation of the production of activin, presence of lactoferrin and interleukin-1 receptor antagonist
2. Antiscarring effect and neurotrophic factors - suppression of transforming growth factor- β signaling
3. Antiangiogenic effect - expression of vascular endothelial growth factor and basic fibroblast growth factor

IT IS CURRENTLY USED IN OTHER FIELDS

OBJECTIVE
to test a new technique for treatment of
chronic non-healing wound using amniotic membrane in combination with bone marrow derived autologous MSCs

OUTLINE
Why this research project? Point of research Methodology Results Extension of the study Implications

DESIGN
randomised controlled trial Thirty seven chronic leg ulcers from February 2012 till June, 2013

21
HOW RCT?Participants
R a
n d
o m
l
y A
s s
i g
n e d
Intervention Group
Control Group
Follow-up
Follow-up
Intervention Group
Control Group

RANDOMISATION
Group I: Bone marrow aspiration was done to obtain autologous bone marrow stem cells, which were then cultured, identified, and finally, MSCs were injected into ulcer bed and ulcer edges.

Group II: Autologous MSCs were injected into ulcer bed and ulcer edges, then freshly prepared amniotic membrane was placed in contact with ulcer and held in place with secondary dressing.
Follow up for three month was done for both groups

Obtaining Amniotic Membrane and its preparation

Steps

SEVERAL WASHES OF AM THEN EMERSION IN CONTAINER CONTAINS ANTIBIOTICS AND ANTIFUNGAL.
One placenta can provide 40 to 50 AM tissue fragments 5 cm in diameter
This container contains antibiotics and antifungal.

INFECTION CONTROL
containing blood from the mother are collected for the following serology tests: HIV , HCV, HBV
Final validation of the AM is performed after a
repeat serology test after 120 days.

CRYOPRESERVATION OF AM
a cryoprotective agent was added (RPMI and glycerol),then was stored in the freezer at a temperature of -80°C
N.B: AM can be stored on dry ice for 24 hours

AM APPLICATION STEP BY STEP
Amniotic Membrane application step by step:
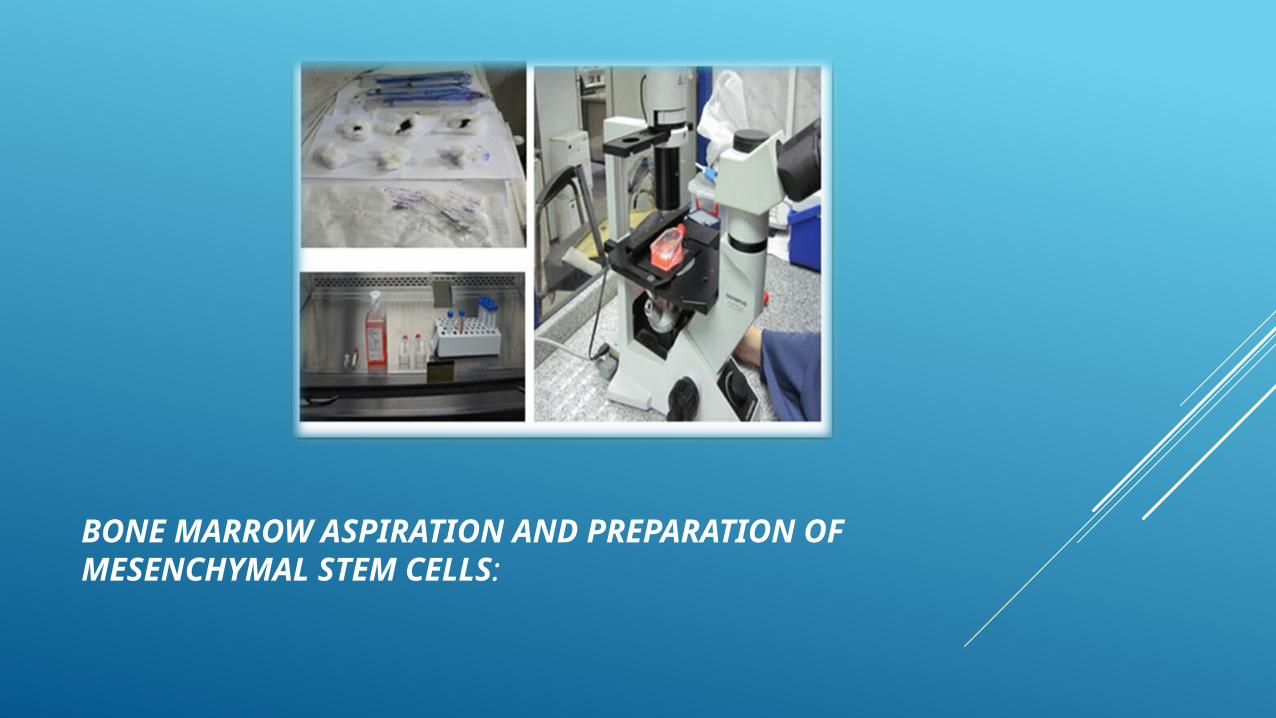
BONE MARROW ASPIRATION AND PREPARATION OF MESENCHYMAL STEM CELLS:

BM ASPIRATION
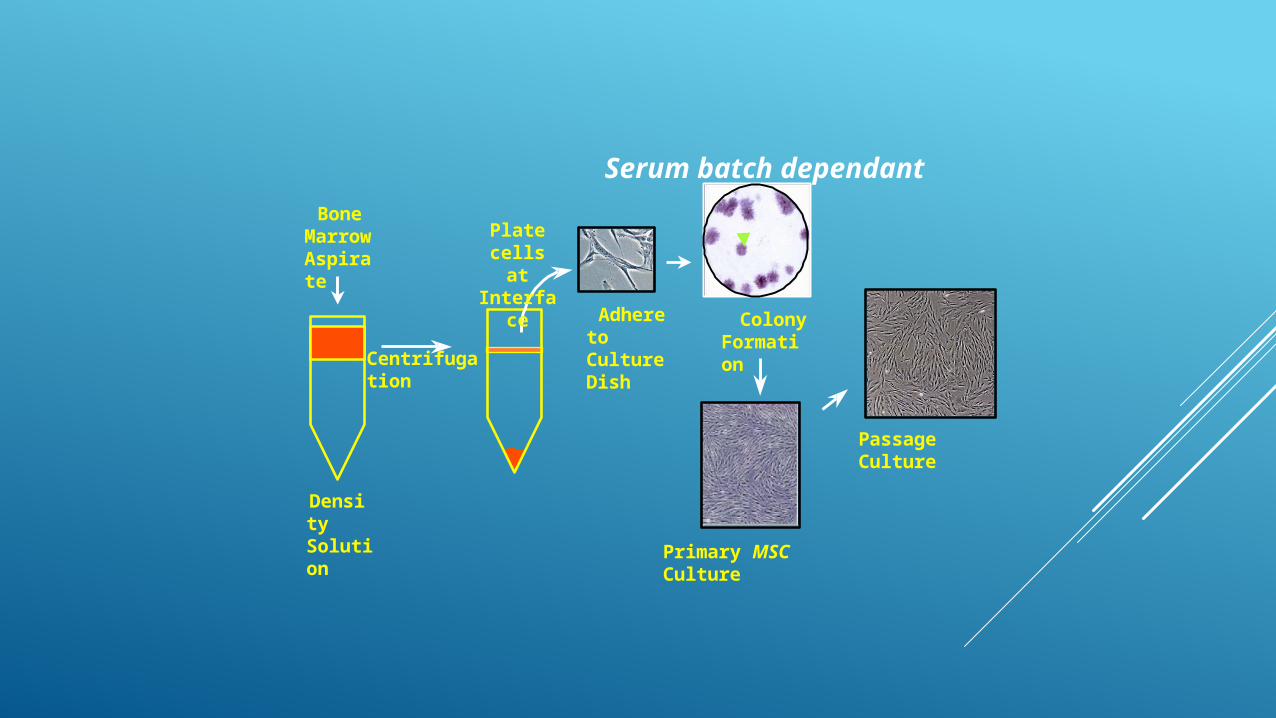
Centrifugation
Passage Culture
Bone Marrow Aspirate
Adhere to Culture Dish
Primary MSC Culture
Colony Formation
Plate cells at
Interface
Density Solution
Serum batch dependant

PREPARATION OF STEM CELLS
Bone Marrow was aspirated from iliac bone and placed in sterile tubes contained heparin sulphate to avoid platelets clumping.
The bone marrow aspirates were diluted with PBS containing EDTA then mononuclear cells were separated by density gradient centrifugation using Ficoll-Hypaque solution.

TECHNIQUE
The cells were plated in Dulbecco's modified Eagle's Medium (DMEM) and then cultured at 37º C in 5% CO2. After one day, non –adherent cells were removed and adherent cells were cultured in presence of mesenchymal media for 21 days.
the cells were harvested by incubation with trypsin /EDTA. In order to determine their immune phenotype, surface expression of CD90, CD29, and CD34 were analyzed twice before and after culture of cells by flowcytometry.
Finally 10 million MSCs in 3 ml saline were implanted in ulcer bed and ulcer edges.

Application of Amniotic membrane used together with autologous mesenchymal stem cells

FOLLOW UP OF PATIENTS:
-Healing Rate and detection of ulcer size - Assessment of pain - Graft taken or not (Day 2). - Ulcer images follow up (Day 0, Day7, Day 14, Day
21, Day 30, Day45, and Day 60).
OUTLINE
Why this research project? Point of research Methodology Results Extension of the study Implications

RESULTS
the main manifestations, including lower limb pain and ulcers, were significantly improved in patients of both groups but there was more significant difference in healing rate and reduction in ulcer size in group II (P<0.001).

The wound showed a steady overall decrease in wound size and improvement in wound bed with healthy granulation tissues.
Reduction in ulcer size and rate of healing increased with presence of healthy granulations (P=0.001).

Follow up

Groups ChronicityReduction size
(%)
rate of healing
(%)
Group I Range 4 - 156 50.4 – 100 8.4 – 78.7
Mean + SD 52.17+56.05 83.9 + 24.9 30.3+25.4
Group IIRange 5 – 120 46.5 – 100.0 35.9 – 123.1
Mean + SD 53.67+46.89 79 +24.2 75.9+36.1
Total (n=37)Range 4 – 156 0.0 – 100.0 0 – 222.1
Mean + SD 51.49+29.09 64.25+45.01 51.1+57.7

ARE THERE OTHER FACTORS ?
A negative correlation was found between age and both reduction in ulcer size and rate of healing (-0.36), (-0.173) respectively.

LIMITATIONS, REASON FOR CAUTION
Larger sample size is needed to confirm our results. The technique is costly and needs financial support
for wide application.

IS AMNIOTIC MEMBRANE ALONE ENOUGH?
How to avoid such high cost?

OUTLINE
Why this research project? Point of research Methodology Results Extension of the study Implications

EXTENSION OF THE STUDY
Group III: (14 leg ulcers) Amniotic membrane was placed in contact with ulcer and held in place with secondary dressing; which was changed day by day.

Twelve ulcers (85.7%) were venous ulcers, while two ulcers (14.3%) were traumatic ulcers. All patients of group II show no history of diabetes, hypertension, smoking or any other clinical condition.

RESULTS
complete healing of 14 ulcers in 14-60 days with mean of 33.3 ± 14.7,
healing rate range was 0.064 – 2.22 and mean of 0.896 ± 0.646 cm2/ day with 100% reduction in ulcer size.
Eleven cases (78.6%) showed improvement in their pain level at a scale from 1 to 10.

IMPORTANT NOTICE
we found that AM graft was taken by 28.6% ulcers of group III where AM alone was used alone in treatment,
while AM graft was taken by 66.7% by ulcers of group II where AM was used together with MSCs.

WHAT DOES THIS MEANS?
These results are highly suggesting that using AM in treatment may be the best choice in treating ulcers of mild severity,
while ulcers of moderate severity may be better if treated with both AM and MSCs together followed by AM alone as a best second choice

CONCLUSION
AM may be considered as a bio-therapeutic product.

OUTLINE
Why this research project? Point of research Methodology Results Extension of the study Implications
WIDER IMPLICATIONS OF THE FINDINGS
The fact of the wide availability, the no cost of AM, and being a discarded tissues after delivery, AM can be a corner stone in tissue repair programs and implementation of biotherapy

THANK YOU

















