Page 1
STRATEGICINITIATIVEPANELS
FinalReportsfrom:CommonTerminologyPanel
IntegratedClinicalEducationPanelStudentReadinessPanel
June2017
TABLEOFCONTENTS
PANELSUMMARYREPORTS• GLOSSARY• DOCUMENTLISTING• ICEAPPENDIX• READINESSAPPENDIX• SUMMARYOFRECOMMENDATIONS
COMMONTERMINOLOGYPANEL–FULLREPORT• GLOSSARY• DOCUMENTLISTINGINTEGRATEDCLINICALEDUCATIONPANEL-FULLREPORT• TABLE1• TABLE2• APPENDIXASTUDENTREADINESSPANEL–FULLREPORT• APPENDIXC
Page 2
AmericanCouncilofAcademicPhysicalTherapyPost-SummitStrategicPanelReports
FinalReportsfrom:CommonTerminologyPanel
IntegratedClinicalEducationPanelStudentReadinessPanel
June2017
OVERVIEWInOctober2014theAmericanCouncilofAcademicPhysicalTherapy(ACAPT)coordinatedaClinicalEducationSummitwiththesupportoftheAmericanPhysicalTherapyAssociation(APTA),theEducationSectionoftheAPTA,theFederationofStateBoardsofPhysicalTherapy(FSBPT),andtheJournalofPhysicalTherapyEducation(JOPTE).
FollowingtheSummit,theACAPTBoardofDirectorsassembledandprioritizedtheSummitfindingsandrecommendations.ACAPTsubsequentlyappointed3strategicinitiativepanelstoaddressthehighestprioritySummitrecommendations.Thisdocumentisacompilationofthefinalreportsfromthese3panelstotheACAPTBoard.
REPORTFORMATThereare3componentstothisreport:
• Summary–thisdocumentcontainsanoverviewoftheprocessandthefinalworkproductsfromeachpanel.
• Recommendationsforconsideration–thisdocumentincludestherecommendationsfromeachpanelthatwillbeconsideredbythemembership.
• Finalreportsfrompanels–thisdocumentisacompilationofthefinalreportfromall3panelsandcontainsthedetailedmethodologyleadingtothefinalworkproducts.
SUMMARY
BACKGROUNDTheClinicalEducationSummitbroughttogetherclinicalandacademiceducatorstodiscusstheconcernsofthephysicaltherapyclinicaleducationsystemanddevelopoptionstoaddressidentifiedissueswithinthephysicaltherapist(PT)clinicaleducationsystem.TheSummitgoalwastoreachagreementonbestpracticeinPTclinicaleducation.Representativesincludedacademicandclinicalfacultyfrom202ofthe212ACAPTmemberinstitutionsaswellasotherkeystakeholders.TheresultoftheSummitwasareportcontaining11harmonizingrecommendationsand3innovativerecommendations.
(ClinicalEducationSummitReport)
Followingthereceiptofthereport,theACAPTBoardofDirectorsprioritizedtherecommendations,integratedtheworkintotheorganization’sstrategicplan,andformed3strategicinitiativepanelstoaddressthehighestprioritytopics.The3topicschosenwerecommonterminologyforphysicaltherapisteducation,integratedclinicaleducation,andassessmentofstudentreadiness.
1
Page 3
PANELSTRUCTUREANDMEMBERSHIPACAPTidentifiedachairofeachpanelandacoordinatortohelpfacilitatetheongoingworkofall3groups.Inmid-November2015acallforvolunteerstoserveonthethreepanelswasdistributedresultingin62applicants,severalofwhomappliedtomultiplepanels.Thepanelchairsandcoordinatorreviewedallapplicationsanddevelopedalistofmemberswhopossessedthenecessarystrengthsandexperiencestoaddressthepanelchargesandwererepresentativeoftheprofession’svariability.ThenomineesweresubsequentlyappointedtothepanelsbytheACAPTBoardonJanuary20,2016.ACAPTalsoappointedaliaisonfromtheBoardtofacilitatecommunicationandassistthepanelsinaccomplishingtheirwork.CommonTerminologyPanelMiaErickson,PT,EdD,CHT,ATC–MidwesternUniversity(Chair)DebbieIngram,PT,EdD,FAPTA–UniversityofTennesseeChattanoogaEmmaWheeler,PT,DPT–VirginiaCommonwealthUniversityJanetJackson-Coty,PT,DPT–ThomasJeffersonUniversityJohnBorstad,PT,PhD–TheCollegeofSt.ScholasticaJulieHartmann,PT,DSc.–GannonUniversityLauritaHack,PT,DPT,MBA,PhD,FAPTA–ArcadiaUniversityMarisaBirkmeier,PT,DPT–GeorgeWashingtonUniversityMelissaBooth,PT,DPT–UniversityofCentralArkansasVickiLaFayPT,DPT–ClarksonUniversityIntegratedClinicalEducationPanelChristineMcCallum,PT,PhD-WalshUniversity(Chair)JamieBayliss,PT,DHSc-MountSt.JosephUniversityElaineBeckerPT,DPT,MA–NewYorkUniversityYvonneColgrove,PT,PhD-UniversityofKansasMedicalCenterKimeranEvans,PT,DPT-WestVirginiaUniversityJannaKucharski-Howard,PT,DPT,MSM-MCPHSUniversityTaraLegar,PT,MPT-OhioUniversityKimNixon-Cave,PT,PhD-ThomasJeffersonUniversityByronRussell,PT,PhD-MidwesternUniversityDebraStern,PT,DPT,DBA-NovaSoutheasternUniversity,FortLauderdale,FLAValerieStrunk,PT,MS-IndianaUniversity,Indianapolis,INEllenWetherbee,PT,DPT,Med-QuinnipiacUniversity,NorthHaven,CTStudentReadinessPanelJeanFitzpatrickTimmerbergPT,PhD,MHS-ColumbiaUniversity(Chair) RobinDole,PT,DPT,EdD-WidenerUniversity StephenL.Goffar,PT,PhD-UniversityoftheIncarnateWord DivyaMathur,PT,MPA-NYUHospitalforJointDisease AmyMiller,PT,DPT,EdD-ArcadiaUniversity LeighMurray,PT,PhD,MA-WalshUniversityDeborahPelletier,PT-SpringfieldCollegeNickiSilberman,PT,DPT,PhD-HunterCollegeMichaelSimpson,PT,DPT-UniversityofSouthernCaliforniaAngelaStolfi,PT,DPT-NYULangoneMedicalCenter AnneThompson,PT,EdD-ArmstrongStateUniversity RalphUtzman,PT,MPH,PhD-WestVirginiaUniversityShawneSoper,PT,DPT,MBA,VirginiaCommonwealthUniversity(StrategicInitiativePanelCoordinator)MichaelSheldon,PT,PhD,NewEnglandUniversity(ACAPTBoardLiaison)
2
Page 4
PANELPROCESSTheworkofthepanelsisintendedtoaddressspecificrecommendationsfromtheClinicalEducationSummitreport.TheACAPTBoardofDirectorsdevelopedaspecificchargeforeachgroup,providingsomeadditionaldetailandcontexttohelpframetheirwork.TherecommendationsfromtheSummitreportandthepanelchargesaresummarizedbelow.
CommonTerminologySummitRecommendationI:Academicandclinicalfacultywilldevelop,disseminate,use,andperiodicallyreviewstandardterminologyanddefinitionsforphysicaltherapyeducation.
Charge:TheACAPTCommonTerminologyPanelwilldevelopcommonterminologyrelatedtoclinicaleducation.Thisworkmayalsoresultintemplatesandmodelstosupportclinicaleducation,suchasplacementrequestformsandstudentinformationforms.Thisrecommendationalsorelatestootherrecommendationsdefiningdifferentaspectsofclinicaleducation.Thespecificchargetothisworkingpanelis:
• InvestigateandidentifyallcurrentsourcesofterminologyrelatedtoclinicaleducationbyinvitingparticipationoftheNationalConsortiumofClinicalEducators(NCCE),APTAEducationSectionandSpecialInterestGroups,CommissiononAccreditationinPhysicalTherapyEducation(CAPTE),andothergroups
• Reviewallcurrentsupportdocuments–CAPTE,ClinicalPerformanceInstrument(CPI),theGuidetoPTPractice,andotherrelateddocuments
• Considertemplatesandmodelstosupportclinicaleducationsuchasplacementrequestformsandstudentinformationforms
• Recommendotheritemsforconsiderationrelatedtoacommonterminology • Developguidelinesforimplementationoftheproposedterminology
IntegratedClinicalEducationSummitRecommendationVII:Allprogramswilloffergoaloriented,diverseactive-learningexperiencesthataredevelopedincollaborationwithinvestedstakeholdersandembeddedwithinthedidacticcurriculum,priortoterminalexperiences.Charge:TheACAPTIntegratedClinicalEducationStrategicInitiativePanelwilldeveloparecommendationforimplementationofintegratedclinicaleducationasacomponentofphysicaltherapisteducation.Thespecificchargetothisworkingpanelis:
• Define‘integratedclinicaleducation’• Makerecommendationsforachievingconsistentuseoftheterm‘integratedclinicaleducation’
acrossACAPT,APTAandCAPTE• Discernanddescribemodelsofintegratedclinicaleducationthatcurrentlyexistwithinphysical
therapistcurricula• Definebaselineexpectationsandparametersforqualityintegratedclinicaleducationinphysical
therapisteducation• Developguidelinesforcollaborativedevelopmentandimplementationofintegratedclinical
experiences
StudentReadinessSummitRecommendationsIXandX:Developarequisitecoresetofknowledge,skills,attitudesandprofessionalbehaviorstomoveintoearly,intermediate,andfinalfull-timeclinicalexperiences.Establishaprocessforidentifyinghowandifstudentsmeetclinicalcoreperformancecompetenciesuponenteringeachleveloffull-timeclinicalexperience.
3
Page 5
(Note:RecommendationsIXandXwereinterrelated.BecausetheyweredevelopedbyseparateteamsattheSummittheywerebothreportedtopreservethefullnessoftheirproposal.Arelatedrecommendation(XI)wasalsoincludedintheSummitreport.ItwasnotaddressedbytheStudentReadinessPanel;however,itisreferencedlaterinthisreport.)Charge:TheACAPTStudentReadinessStrategicInitiativePanelwillidentifyanddefineacoresetofcompetencies(knowledge,skills,attitudesandprofessionalbehaviors)thataretobedemonstratedbystudentspriortofull-timeclinicaleducation.Theinitialfocusofthepanelwillbeonentrytotheinitialfull-timeclinicalexperience.Thespecificchargetothisworkingpanelis:
• Investigateanddescribemodelsofcompetencyassessmentusedacrossotherhealthprofessions
• Proposetwoformatoptionsforestablishingcompetenciestotheboardmembership• Collectbroad-based,representativedataonminimumcompetencyexpectationsfromthe
physicaltherapypracticecommunity• Onceapreferredmodelisselectedandminimumcompetenciesareidentified,proposebaseline
expectationsandcriteriaforminimumcompetenciesthatmustbemetwithintheacademicprogrambystudentpriortoprogressingintofull-timeclinicaleducationexperiences.
• Developguidelinesforacademicprogramstoimplementthesecompetencyrequirementswithintheircurriculum.
EachpanelheldafacetofaceinitialmeetingattheCombinedSectionsMeeting(CSM)inFebruary2016followedbybothvirtualandfacetofacemeetingsspanningthepast18months.
Thepanelshaveworkedinconcertwithoneanotherthroughoutthisprocess.Thecoordinatorandpanelchairshavemetonaregularbasis,bothvirtuallyandfacetoface.Eachmeetinghasincludedanupdatefromthepanelchairsandidentificationofareasinwhichthe3groupsmustcollaboratetoensurethattheworkproductsaresupportiveandwell-coordinated.
InOctoberof2016thecoordinatorandpanelchairspresentedaneducationalsessionattheEducationLeadershipConference.Thesession,entitledClinicalEducationSummitStrategicInitiatives:UpdatesandIdeas,servedtopresentthefindingsofeachpanelandengageparticipantsindiscussiontohelpshapethefuturerecommendationstobemadetotheACAPTBoardandmembership.Thisoutcomeoftheroundtablediscussionsthatoccurredduringthesessionprovedbothtimelyandvaluabletothefutureworkofthepanels.
Studentswerealsoinvolvedintheprocessofshapingpanelrecommendations.Thecoordinatorhostedtwostudentfocusgroups:onefacetofacesessionduringtheNationalStudentConclaveinOctober2016andavirtualsessiononNovember16,2016.Intotal17studentsrepresenting5universitiesparticipatedinthefocusgroups.Informationfromthesesessionswassummarizedandprovidedtothepanelsforconsiderationasthegroupsdevelopedtheirrecommendations.
4
Page 6
COMMONTERMINOLOGYSTRATEGICINITIATIVEPANELSUMMARYOFWORKFromFebruarytoApril2016,membersofthePanelgathereddata,whichincludedtermsandtheirdefinitionsrelatedtoanyaspectofphysicaltherapistclinicaleducation,fromallrelevantsources.SourcesincludedACAPT,APTA,CAPTE,ClinicalEducationSpecialInterestGroup(CESIG),FSBPT,clinicaleducationconsortia,residency,andfellowshipdocuments;clinicaleducationevaluationtools;ANormativeModelofPhysicalTherapistProfessionalEducation1;andmaterialsfromtheClinicalEducationSummit.Asystematicreviewoftheclinicaleducationliteraturewasalsoperformed.Theprocessdescribedaboveledtoasetoftermsforphysicaltherapistclinicaleducation.ThesetermshavebeenassembledintothePhysicalTherapistClinicalEducationGlossaryandareprovidedinAppendixA.AfterdevelopmentoftheGlossary,acomprehensivereviewofprofessionaldocumentswasconductedtoidentifythosethatwouldneedtobechangedtobeconsistentwiththeterminologybeingproposedbythePanel.MembersofthePanelreachedouttootherstakeholdergroups,collaboratingandsharingtheworkbeingdoneacrossgroups.TherehasbeenongoingandextensivecollaborationwiththeIntegratedClinicalEducationPanelandtheStudentReadinessPanel.Wealsoinvitedcollaborationwithothersthrough1)roundtablediscussionswiththeparticipantsatthe2016EducationalLeadershipConference,2)anopencommentperiodprovidedformembersofthephysicaltherapyacademicandclinicalcommunities,and3)studentfocusgroupsduringtheNationalStudentConclaveandvirtuallyinNovember2016.ThisallowedmemberstoprovidefeedbackonadraftoftheGlossary.FeedbackwasusedfromtheroundtablediscussionsandthecommentperiodtodevelopthefinalGlossary.Anadditionalitemforconsiderationisrelatedtotheuseoftheterm‘internship.’Theinformationdetailedabovehasledthepaneltotheconclusionthatinthecurrentphysicaltherapistclinicaleducationinfrastructure,thetermisbeingusedinappropriatelyandtheclinicaleducationcommunityneedstotakestepstoeliminatetheuseoftheterm.ThePanelrecognizesthatsomeoftheinnovativechangescurrentlybeingexaminedmaypresentopportunityforappropriateuseoftheterminthefuture.
5
Page 7
PHYSICALTHERAPISTCLINICALEDUCATIONGLOSSARY
Thisglossaryoftermswasdevelopedafterareviewofthephysicaltherapyliterature,extensivediscussionanddebatebytheACAPTCommonTerminologyPanel,andengagementofkeystakeholderswithinthephysicaltherapyclinicaleducationcommunity.TheGlossaryisdividedintomajorcategoriesand,asapplicable,definitionsarereferenced. CLINICALEDUCATIONINFRASTRUCTURE Clinicaleducation Aformaltypeofsupervisedexperientiallearning,focusedon
developmentandapplicationofpatient-centeredskillsandprofessionalbehaviors.Itisdesignedsothatstudentsgainsubstantial,relevantclinicalexperienceandskills,engageincontemporarypractice,anddemonstratecompetencebeforebeginningindependentpractice.1-3
Clinicaleducationagreement
Aformalandlegallybindingagreementthatisnegotiatedbetweenacademicinstitutionsandclinicaleducationsitesorindividualprovidersofclinicaleducationthatspecifieseachparty'sroles,responsibilities,andliabilitiesrelatingtostudentclinicaleducation.4
Clinicaleducationcurriculum
Theportionofaphysicaltherapyeducationprogramthatincludesallpart-timeandfull-timeclinicaleducationexperiencesaswellasthesupportivepreparatoryandadministrativecomponents.4
Clinicaleducationexperience
Experiencesthatallowstudentstoapplyandattainprofessionalknowledge,skills,andbehaviorswithinavarietyofenvironments.Experiencesincludethoseofshortandlongduration(e.g.,part-time,full-time),provideavarietyoflearningopportunities,andincludecareofpatients/clientsacrossthelifespanandpracticesettings.Whiletheemphasisisonpatient-careskills,experiencesmayalsoincludeinter-professionalexperiencesandnon-patientcaredutiessuchasresearch,teaching,supervision,andadministration.Clinicaleducationexperiencesareapartoftheprofessionalcurriculumandincludeformalstudentassessment.5-8
Collaborativeclinicaleducationmodel
Aclinicaleducationexperienceinwhichtwo(ormore)physicaltherapiststudentsareassignedtoone(ormore)preceptor/clinicalinstructor(s).Thestudentsworkcooperativelyunderthepreceptor/clinicalinstructor(s).Examplesinclude2:1,2:2,3:1,etc.studenttopreceptor/clinicalinstructorratio.Studentsmaybefromthesameordifferentprogramsandmaybeatthesameordifferentlevelsoftraining.9-11
6
Page 8
Didacticcurriculum Thecomponentofthephysicaltherapistprofessionaleducationprogramthatiscomprisedofthecontent,instruction,learningexperiences,andassessmentdirectedbytheacademicfaculty.3,12,13
Fellowship Apost-professionalfundedandplannedlearningexperienceinafocusedareaofclinicalpractice,education,orresearch(notinfrequentlypost-doctoralorforpost-residencyorboardcertifiedtherapists).14
Full-timeclinicaleducationexperience
Aclinicaleducationexperienceinwhichastudentengagesforaminimumof35hoursperweek.Anintegratedclinicaleducationexperiencemaybeafull-timeclinicaleducationexperience;however,full-timeclinicaleducationexperiencesdesignatedtoachievetheminimumnumberofweekssetforthbyCAPTEaredirectedbyaphysicaltherapistclinicalinstructor.5,7
Firstfull-timeclinicaleducationexperience
ThefirstclinicaleducationexperiencedesignatedtoachievetheminimumnumberofweekssetforthbyCAPTEinwhichastudentengagesforaminimumof35hoursperweek.
Intermediatefull-timeclinicaleducationexperience
AclinicaleducationexperiencedesignatedtoachievetheminimumnumberofweekssetforthbyCAPTEinwhichastudentengagesforaminimumof35hoursperweekandreturnstotheacademicprogramforfurthercompletionofthedidacticcurriculum.
Terminalfull-timeclinicaleducationexperience
Asingle,orsetof,full-timeclinicaleducationexperience(s)designatedtoachievetheminimumnumberofweekssetforthbyCAPTEthatoccurafterthestudenthascompletedthedidacticcurriculumofaphysicaltherapistprofessionaleducationprogram.Studentsmayreturntotheacademicprogramfordidacticinstructionthatdoesnotrequireadditionalclinicaleducationexperiences.Theexpectedoutcomeofthefinal,orlastterminalexperienceisentry-levelperformance.7
Internationalclinicaleducationexperiences
Aneducationalopportunitythatastudentparticipatesin,outsideofthecountrywherethephysicaltherapisteducationprogramissituated,forwhichhe/sheobtainsclinicaleducationcredit.TheabbreviationICEshouldnotbeusedtodescribeaninternationalclinicaleducationexperience.7,15
Internship Aterminalfull-timeclinicaleducationexperiencethatprovidesrecompensetoparticipantsinaccordancewithfederallaborlawsundertheFairLaborStandardsAct.16
Learningexperience Anyexperiencewhichallowsorfacilitatesachangeinattitudeorbehavior.Aplannedlearningexperienceincludesalearner,anobjectiveforthelearner,asituationdevisedtoproducearesponsethatcontributestotheobjective,aresponsebythestudent,andreinforcementtoencouragethedesiredresponse.3
7
Page 9
Part-timeclinicaleducationexperience
Aclinicaleducationexperienceinwhichastudentengagesinclinicaleducationforlessthan35hoursperweek.Part-timeexperiencesvaryinlength.Apart-timeclinicaleducationexperiencemaybeconsideredanintegratedclinicaleducationexperiencedependingonthedesignoftheexperienceandthelearningobjectives.7,17
Physicaltherapistprofessionaleducationprogram
Educationcomprisedofdidacticandclinicaleducationdesignedtoassurethatstudentsacquiretheprofessionalknowledge,skills,andbehaviorsrequiredforentry-levelphysicaltherapistpractice.3,18,19
Physicaltherapistpost-professionaleducationprogram
Degreeandnon-degreebasedprofessionaldevelopmentforthephysicaltherapisttoenhanceprofessionalknowledge,skills,andabilitiesbeyondentrylevel.Examplesinclude,butarenotlimitedto,continuingeducationcourses,post-professionaldoctoraleducationprograms,certificateprograms,residency,andfellowship.19
Residency Post-professionalprogramsthatoccurafterthegraduatephysicaltherapisthasobtainedalicensetopractice.Theymaybeclinicalprogramsthatadvanceaphysicaltherapist'sknowledgeandskillsinpatient/clientmanagement,ornonclinicalfocusingonadvancingaphysicaltherapist'scareeroutsideofclinicalduties.20
CLINICALEDUCATIONSITES Clinicaleducationsite
Ahealthcareagencyorothersettinginwhichclinicaleducationexperiencesareprovidedforphysicaltherapiststudents.Theclinicaleducationsitemaybe,butisnotlimitedto,ahospital,agency,clinic,office,school,orhomeandisaffiliatedwithoneormoreeducationalprogramsthroughacontractualagreement.3,4
Clinicaleducationenvironment
Thephysicalspace(s),aswellasthestructures,policies,procedures,andculturewithintheclinicaleducationsite.
CLINICALEDUCATIONSTAKEHOLDERS Academicfaculty Teachersandscholarswithintheacademicinstitutiondedicatedto
preparingstudentsintheskillsandaptitudesneededtopracticephysicaltherapy.21
Academicinstitution Universityorcollegethroughwhichanacademicdegreeisgranted.4
Clinicaleducationconsortia
Nationalandregionalgroupsthatincludeacademicandclinicaleducationfacultyforthepurposeofsharingresources,ideas,andefforts.4
8
Page 10
Clinicaleducationfaculty
Theindividualsengagedinprovidingtheclinicaleducationcomponentsofthecurriculum,generallyreferredtoaseitherSiteCoordinatorsofClinicalEducation(SCCEs),preceptors,orclinicalInstructors.Whiletheacademicinstitutiondoesnotusuallyemploytheseindividuals,theydoagreetocertainstandardsofbehaviorthroughcontractualarrangementsfortheirservices.7
Clinicalinstructor(CI)
Thephysicaltherapistresponsibleforthephysicaltherapiststudentanddirectlyinstructs,guides,supervises,andformallyassessesthestudentduringtheclinicaleducationexperience.Whenengagedinfull-timeclinicaleducationdesignatedtomeettheminimumnumberofweeksrequiredbyCAPTE,theclinicalinstructormustbealicensedphysicaltherapistwithaminimumofoneyearoffulltime(orequivalent)post-licensureclinicalexperience.4,22,23
DirectorofClinicalEducation(DCE)
Academicfacultymemberwhoisresponsibleforplanning,directingandevaluatingtheclinicaleducationprogramfortheacademicinstitution,includingfacilitatingclinicalsiteandclinicalfacultydevelopment.22,24,25
Physicaltherapiststudent
StudentenrolledinaCAPTE-accreditedorapproveddevelopingphysicaltherapistprofessionaleducationprogram.Studentsshouldnotbereferredtoasaphysicaltherapystudent.
Preceptor Anindividualwhoprovidesshort-termspecializedinstruction,guidance,andsupervisionforthephysicaltherapiststudentduringaclinicaleducationexperience.Thisindividualmayormaynotbeaphysicaltherapistaspermittedbylaw.
SiteCoordinatorofClinicalEducation(SCCE)
Professionalwhoadministers,manages,andcoordinatesclinicalassignmentsandlearningactivitiesforstudentsduringtheirclinicaleducationexperience.Inaddition,thispersondeterminesthereadinessofpersonstoserveaspreceptorsandclinicalinstructorsforstudents,supervisespreceptorsandclinicalinstructorsinthedeliveryofclinicaleducationexperiences,communicateswiththeacademicprogramregardingstudentperformance,andprovidesessentialinformationtoacademicprograms.4,22,26
CLINICALEDUCATIONASSESSMENT Clinicalperformanceassessment
Clinicalperformanceassessmentencompassesformalandinformalprocessesdesignedtoappraisephysicaltherapiststudentperformanceduringclinicaleducationexperiences.Assessmentmaybeformativeorsummativeinnatureandperformedforthepurposesofprovidingfeedback,improvinglearning,revisinglearningexperiences,anddeterminingsuccessfulattainmentofstudentperformanceexpectationsduringclinicaleducationexperiences.3,22,27,28
9
Page 11
Clinicalperformanceevaluationtool
Avalid,reliable,andmultidimensionalclinicalperformanceassessmenttoolutilizedtodetermineif,andhowwell,astudentmeetsestablishedbehavioralobjectivesduringclinicaleducationexperiences.4,29,30,31
Entry-levelphysicaltherapistclinicalperformance
Performancethatdemonstratesknowledge,skills,andbehaviorsconsistentwitheffective,efficient,andsafepatient/clientmanagementtoachieveoptimaloutcomes.22,28
Supervision Theguidanceanddirectionprovidedtoaphysicaltherapiststudentbythepreceptororclinicalinstructor.Thisvariesbasedonthecomplexityofthepatientorenvironment;jurisdictionandpayerrulesandregulations;andabilitiesofthephysicaltherapiststudent.4,22,27
References
1. DelanyC,BraggeP.Astudyofphysiotherapystudents’andclinicaleducators’perceptionsof
learningandteaching.MedicalTeacher.2009;31(9):402-411.
2. OʼBrienB,TeheraniA.UsingWorkplaceLearningtoImprovePatientCare.AcadMed.2011;86(11):e12.
3. MooreML,PerryJF.ClinicalEducationinPhysicalTherapy:PresentStatus/FutureNeeds.Final
ReportoftheProjectonClinicalEducationinPhysicalTherapy.Washington,DC:SectionforEducationAmericanPhysicalTherapyAssociation;June1976;NO1-AH.
4. AmericanPhysicalTherapyAssociation.ThePhysicalTherapyClinicalInstructorEducationandCredentialingProgramManual.Alexandria,VA:AmericanPhysicalTherapyAssociation;2009.
5. TerminologyforClinicalEducationExperiencesProposedbyAcademicCouncilBoardofDirectors[ACAPTmotionAC-2-13].http://acapt.myriadmedia.com/docs/default-source/motions/2013-motions/ac-2-13_terminology_for_clincal_education_passed.pdf?sfvrsn=2.AccessedMay16,2017.
6. PivkoSE,AbbruzzeseLD,DuttarovP,HansenRL,RyansK.Effectofphysicaltherapystudents'clinicalexperiencesonclinicianproductivity.JAlliedHealth.2016;45(1):33-40.
7. CommissiononAccreditationinPhysicalTherapyEducation.StandardsandRequiredElementsforAccreditationofPhysicalTherapistEducationPrograms,2016.http://www.capteonline.org/AccreditationHandbook/.PublishedNovember11,2015,UpdatedMarch4,2016.AccessedApril10,2017.
8. GibersonTR,BlackB,PinkertonE.Theimpactofstudent-clinicalinstructorfitandstudent-organizationfitonphysicaltherapistclinicaleducationexperienceoutcomes.JPhysTherEduc.2008;22(1):59-64.
10
Page 12
9. RindfleschAB,DunfeeHJ,CieslakKR,etal.CollaborativemodelofclinicaleducationinphysicalandoccupationaltherapyattheMayoClinic.JAlliedHealth.2009;38(3):132-142.
10. DecluteJ,LadyshewskyR.Enhancingclinicalcompetenceusingacollaborativeclinicaleducationmodel.PhysTher.1993;73(10):683-689.
11. LadyshewskyRK.Peerassistedlearninginclinicaleducation:areviewoftermsandlearningprinciples.JPhysTherEduc.2000;14(2):15-22.
12. CommissiononAccreditationinPhysicalTherapyEducation.EvaluativeCriteriaforAccreditationofEducationProgramsforthePreparationofPhysicalTherapists.CommissiononAccreditationinPhysicalTherapyEducationWebsite.http://www.capteonline.org/uploadedFiles/CAPTEorg/About_CAPTE/Resources/Accreditation_Handbook/EvaluativeCriteria_PT.pdf.UpdatedAugust2014.AccessedApril10,2017.
13. KenyonLK,DoleRL,KellySP.Perspectivesofacademicfacultyandclinicalinstructorsonentry-leveldptpreparationforpediatricphysicaltherapistpractice.PhysTher.2013;93(12):1661-1672.
14. AmericanPhysicalTherapyAssociation.Clinicalexperienceterminologyforphysicaltherapists.http://www.apta.org/uploadedFiles/APTAorg/About_Us/Policies/Terminology/ClinicalExperienceTerminology.pdf.UpdatedDecember2009.AccessedApril10,2017.
15. PechakCM.Surveyofinternationalclinicaleducationinphysicaltherapisteducation.JPhysTherEduc.2012;26(1):69-77.
16. U.S.DepartmentofLaborWageandHourDivision.FactSheet#71:InternshipprogramsundertheFairLaborStandardsAct.https://www.dol.gov/whd/regs/compliance/whdfs71.pdf.UpdatedApril2010.AccessedMay16,2017.
17. AmericanPhysicalTherapyAssociation.2007-2008Factsheet:physicaltherapisteducationprograms.AmericanPhysicalTherapyAssociationWebsite.http://www.apta.org/AM/Template.cfm?Section=Home&TEMPLATE=/CM/.AccessedApril10,2017.
18. BarrJS,GwyerJ,TalmorZ.Evaluationofclinicaleducationcentersinphysicaltherapy.PhysTher.1982;62(6):850-861.
19. AmericanPhysicalTherapyAssociation.EducationForPhysicalTherapists:TerminologyUsedToDescribe[HODP05-07-11-04].https://www.apta.org/uploadedFiles/APTAorg/About_Us/Policies/HOD/Terminology/Education.pdf.UpdatedDecember14,2009.AccessedApril10,2017.
20. AmericanBoardofPhysicalTherapyResidencyandFellowshipEducation.Aboutresidencyprograms.http://www.abptrfe.org/ResidencyPrograms/About/.AccessedApril10,2017.
11
Page 13
21. Kondela-CebulskiPM.Counselingfunctionofacademiccoordinatorsofclinicaleducationfrom
selectentry-levelphysicaltherapyeducationalprograms.PhysTher.1982;62(4):470-476.
22. AmericanPhysicalTherapyAssociation.PhysicalTherapistClinicalPerformanceInstruments:Version2006.Alexandria,VA:AmericanPhysicalTherapyAssociation;2006.
23. HalcarzPA,MarzoukDK,AvilaE,BowserMS,Hurm,L.Preparationofentrylevelstudentsforfuturerolesasclinicalinstructors.JPhysTherEduc.1991;5(2):78-80.
24. BucciereiKM,BrownR,MaltaS.Evaluatingtheperformanceoftheacademiccoordinator/directorofclinicaleducation:toolstosolicitinputfromprogramdirectors,academicfaculty,andstudents.JPhysTherEduc.2011;25(2):26-35.
25. PerryJF.Amodelfordesigningclinicaleducation.PhysTher.1981;61(10):1427-1432.
26. PhilipsBU,McphailS,RoemerS.Roleandfunctionsoftheacademiccoordinatorofclinicaleducationinphysicaltherapyeducation:asurvey.PhysTher.1986;66(6):981-985.
27. KernBP,MickelsonJM.Thedevelopmentanduseofanevaluationinstrumentforclinicaleducation.PhysTher.1971;51(5):540-546.
28. TexasConsortiumforPhysicalTherapyEducationandResearchFoundation.PhysicalTherapistManualfortheAssessmentofClinicalSkills.Austin,TX:2004.
29. BeckelC,AustinT,KettenbachG,SargeantD.Computerandinternetaccessforphysicaltherapistclinicaleducation.JPhysTherEduc.2008;22(3):19-23.
30. FitzgeraldLM,DelittoA,IrrgangJJ.Validationoftheclinicalinternshipevaluationtool.PhysTher.2007;87(7):844-860.
31. HouselN,GandyJ.Clinicalinstructorcredentialinganditseffectonstudentclinicalperformanceoutcomes.JPhysTherEduc.2008;22(3):43-51.
12
Page 14
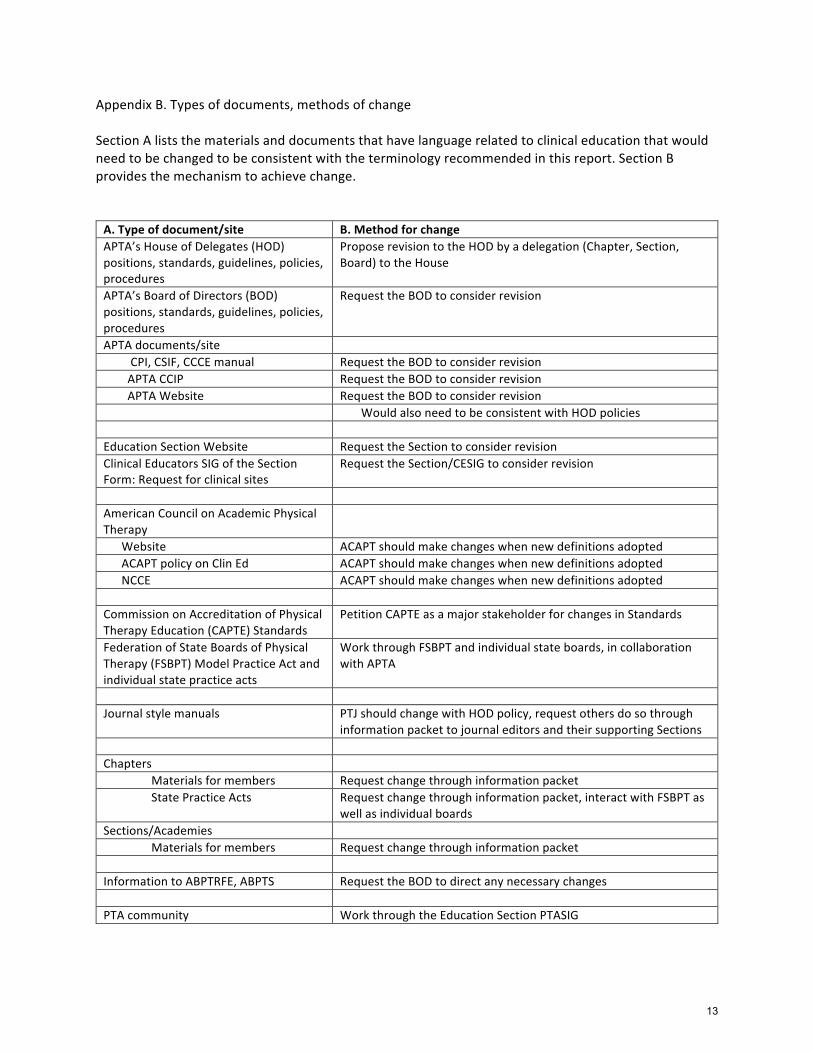
AppendixB.Typesofdocuments,methodsofchangeSectionAliststhematerialsanddocumentsthathavelanguagerelatedtoclinicaleducationthatwouldneedtobechangedtobeconsistentwiththeterminologyrecommendedinthisreport.SectionBprovidesthemechanismtoachievechange.A.Typeofdocument/site B.MethodforchangeAPTA’sHouseofDelegates(HOD)positions,standards,guidelines,policies,procedures
ProposerevisiontotheHODbyadelegation(Chapter,Section,Board)totheHouse
APTA’sBoardofDirectors(BOD)positions,standards,guidelines,policies,procedures
RequesttheBODtoconsiderrevision
APTAdocuments/site CPI,CSIF,CCCEmanual RequesttheBODtoconsiderrevisionAPTACCIP RequesttheBODtoconsiderrevisionAPTAWebsite RequesttheBODtoconsiderrevision WouldalsoneedtobeconsistentwithHODpolicies EducationSectionWebsite RequesttheSectiontoconsiderrevisionClinicalEducatorsSIGoftheSectionForm:Requestforclinicalsites
RequesttheSection/CESIGtoconsiderrevision
AmericanCouncilonAcademicPhysicalTherapy
Website ACAPTshouldmakechangeswhennewdefinitionsadoptedACAPTpolicyonClinEd ACAPTshouldmakechangeswhennewdefinitionsadoptedNCCE ACAPTshouldmakechangeswhennewdefinitionsadopted CommissiononAccreditationofPhysicalTherapyEducation(CAPTE)Standards
PetitionCAPTEasamajorstakeholderforchangesinStandards
FederationofStateBoardsofPhysicalTherapy(FSBPT)ModelPracticeActandindividualstatepracticeacts
WorkthroughFSBPTandindividualstateboards,incollaborationwithAPTA
Journalstylemanuals PTJshouldchangewithHODpolicy,requestothersdosothrough
informationpackettojournaleditorsandtheirsupportingSections Chapters Materialsformembers Requestchangethroughinformationpacket StatePracticeActs Requestchangethroughinformationpacket,interactwithFSBPTas
wellasindividualboardsSections/Academies Materialsformembers Requestchangethroughinformationpacket InformationtoABPTRFE,ABPTS RequesttheBODtodirectanynecessarychanges PTAcommunity WorkthroughtheEducationSectionPTASIG
13
Page 15
INTEGRATEDCLINICALEDUCATIONSTRATEGICINITIATIVEPANELSUMMARYOFWORKPhase1:Weembarkedon2concurrentmethodsofdatacollectiontoestablishabroadviewofcurrenteducationalpracticesinvolvingclinicaleducationdeliveredthroughthelensofanintegratedcurriculumperspective.Thedatacollectionmethodsincludedasystematicreviewoftheliteratureandthedevelopmentanddistributionofadescriptivesurvey.Reviewoftheliterature.Onesubgroupofpanelmemberscompletedthesystematicreviewoftheliteratureusingstandarddatabasesknownforpublicationofeducationalresearchofthehealthprofessions.ThePreferredReportingItemsforSystematicReviewsandMeta-Analysis(PRISMA)guidelineswereselectedtoguidetheprocess.Theinitialsearchresultedin3808articles.Searchtermswererefinedusingkeyworksandsubjectheadingsandarticleswerescreenedfortitleandabstractwhichyielded83articles.Furtherreviewresultedinatotalof22articlesincludedinthefinalreviewoftheliterature.Thesearticlesrepresentthebestavailableevidenceaboutthetopicofintegratedclinicaleducationinhealthprofessions.Surveyresearch.Asecondsubgrouputilizedsurveyresearchtogatherinformationaboutcurrentprogrampracticesthatwereperceivedasintegratedclinicaleducationexperiences.Theresultsofeachofthesedatacollectionmethodswerethematicallycategorizedindependentfromtheother,followedbyanaggregationofthecategoriesforgroupdiscussiontodetermineiftheidentifiedcategorieswereconsideredsoundeducationalpracticesintermsofclinicaleducationexperiencesofferedinanintegratedfashionwithinaprofessionaleducationprogram.Phase2:Twoseriesoffocusgroupswereconductedtogainperspectivefromstakeholdersinvolvedinclinicaleducation:onewithparticipantsatthe2016EducationalLeadershipConferenceandthesecondwithphysicaltherapiststudents.Afterreviewofbothsetsoftranscribedfocusgroupdata,itwasdeterminedapointofdatasaturationwasachieved.Nofurtherdatawassoughtfromotheracademicorclinicalfaculty,orDPTstudentstodeveloptheparameters.ThefinalresultsofPhases1and2includedidentificationofeight(8)categoricalparametersthatdescribecomponentsrequiredforintegratedclinicaleducationexperiences;developmentofthedefinitionofintegratedclinicaleducation,anddevelopmentofdescriptivemodelsofintegratedclinicaleducationbasedonselectedpeer-reviewedarticles.
14
Page 16
ICEAppendixA
INTEGRATEDCLINICALEDUCATIONFORPHYSICALTHERAPISTSTUDENTSDefinition,Parameters,andGuidelines
Educationalliteraturesuggeststhatintegratedclinicaleducationexperiences,aformofexperientiallearning,canexposestudentstoaspectsofpatientcenteredcareduringflexibleclinicaltrainingperiodsthroughoutthecurriculum.Theseexperiencesaffordstudentsanopportunitytofacilitatedevelopmentoftheircognitive,affective,andpsychomotorskillswhileconcurrentlyallowingacademicand/orclinicalfacultytofacilitatestudentdevelopmentwithrespecttothetransferofdidacticknowledgeintoclinicalapplication.(Hakimetal,2014)Thedefinition,parameters,andguidingprinciplespresentedinthisdocumentareprovidedtoassistprogramsinthedevelopmentofintegratedclinicaleducationexperiences.
DefinitionThefollowingisthedefinitionofIntegratedClinicalEducation(ICE).Integratedclinicaleducationisacurriculumdesignmodelwherebyclinicaleducationexperiencesarepurposivelyorganizedwithinacurriculum.Inphysicaltherapisteducation,theseexperiencesareobtainedthroughtheexplorationofauthenticphysicaltherapistroles,responsibilitiesandvaluesthatoccurpriortotheterminalfulltimeclinicaleducationexperience.
Integratedexperiencesarecoordinatedbytheacademicprogramandaredrivenbylearningobjectivesthataresynchronouswithdidacticcontentdeliveryacrossthecurricularcontinuum.Theseexperiencesallowstudentstoattainprofessionalbehaviors,knowledgeand/orskillswithinavarietyofenvironments.Thesupervisedexperiencesalsoallowforexposureandacquisitionacrossalldomainsoflearningandincludestudentperformanceassessment.
Forintegratedclinicaleducationexperiencestoqualifytowardstheminimumnumberoffull-timeclinicaleducationweeksrequiredbyaccreditation(CAPTE)standards,itmustbefulltimeandsupervisedbyaphysicaltherapistwithinaphysicaltherapyworkplaceenvironmentorpracticesetting.
ICE=IntegratedClinicalEducation
ParametersforIntegratedClinicalEducationThefollowingaretheparametersandbaselineexpectationsforICEinphysicaltherapisteducation.Pleaseseethefullreportfortheevidencesupportingtheseparameters.
1.Integratedclinicaleducationmayoccurinanyacademictermpriortothecompletionofthedidacticcourseworkleadingtothecompletionofaterminalfulltimeclinicaleducationexperience.
2.Integratedclinicaleducationexperienceswillhavespecificdesiredoutcomesthatcorrespondtocourseand/orprogrammaticobjectives.
3.Integratedclinicaleducationexperiencesmayberepresentedasacomponentofadidacticcourseorastandalonecoursethatoccursinasynchronousfashionwithotherdidacticcoursework.
4.Integratedclinicaleducationexperiencetimeframesaredevelopedbytheacademicprogrambaseduponthecourseand/orprogrammaticobjectives.Integratedclinicaleducationmayincludefulltimeand/orparttimeexperiences.
15
Page 17
ICEAppendixA
5.Integratedclinicaleducationexperiencesmayoccurinavarietyoflearningenvironmentsincludingcampusorcommunitybasedclinicalornon-clinicalsettings,baseduponthecourseand/orprogrammaticobjectives.Integratedfulltimeclinicaleducationexperiencesthatqualifyforaprogram’sminimumnumberofclinicaleducationweeksshallbecompletedinaphysicaltherapyworkplaceenvironmentorpracticesetting.
6.Integratedclinicaleducationexperiencesshallincludestudentassessmentsthataredesignedtolinktothecourseorprogramobjectiveswithexpectedstudentprogressioninprofessionalbehaviors,clinicalknowledge,and/orskills.
7. Integrated clinical education experiences are coordinated by a faculty member of the academicprogram,inpartnershipwithacoordinatorfromtheclinicaleducationsite.
8. Integrated clinical education experiences are typically supervised by a course instructor and apreceptor. The preceptormay be an academic course facultymember, a clinical instructor, or otherhealthcareprofessionalatthesitethestudentisengagedintheexperience,dependinguponthecourseand/orprogrammaticobjectives. Integrated full time clinical educationexperiences thatqualify for aprogram’s minimum number of clinical education weeks shall be supervised by a licensed physicaltherapist.
GuidelinesforDevelopmentofICE
The following are guidelines for collaborative development and implementation of integrated clinicaleducationexperiences.PleaserefertotheICEPanelreportfortheprovocativequestionsandevidencethataccompanytheseguidelines.
Thekeytowell-developedintegratedclinicaleducationexperiencesisintentionality.Intentionalandtargetedinstructionencompassesplanningwithapurpose,cultivatingthelearningenvironment,instructingwithintention,andassessingtheimpactthatthemodelhasonstudentlearningwhichiswhattheguidingprinciplesareattemptingtodirect(Fisher,Frey&Hite,2016).Theguidingprinciplesprovidedfocusonthekeyelementsthatprogramsshouldconsiderindevelopingorrefiningintegratedclinicalexperiences.Theseinclude:
1. Anacademicprogramidentifiestheprogrammaticoutcomesthatareexpectedwhenstudentsparticipateinintegratedclinicalexperiences.
2. Theacademicprogramconsiderstheintentionalplacementofintegratedclinicaleducation
experienceswithinitscurriculum.3. Theacademicprogramidentifiesthecourse(s)whereclinicaleducationshouldbeintegrated
withintheprogram.
4. Theacademicprogram,incollaborationwithprogramfacultydevelopsthecoursespecificobjectivesforstudentachievementwithinanintegratedclinicaleducationexperience.
5. Theacademicprogram,incollaborationwithprogramfaculty,identifiesthetimingand
timeframesofwhenclinicaleducationexperiencesshouldbeintegratedwithincourse(s).
16
Page 18
ICEAppendixA
6. Theacademicprogram,incollaborationwithprogramfaculty,identifiestheindividualorindividualswhowilloverseetheintegratedclinicaleducationexperiences.
7. Theacademicprogram,incollaborationwithprogramfaculty,identifiesthemethodsofstudent
andcourseassessmenttomeettheintendedcourseand/orprogramoutcomes.8. Theacademicprogramidentifiesresourcesandlegal/regulatoryparametersthatimpacts
deliveryofintegratedclinicaleducationexperienceswithinprogram.9. Theacademicprogram,incollaborationwithprogramfaculty,selectsthetypeofclinicalor
communitysitesrequiredforintegratedclinicaleducationexperiences.10. Theacademicprogram,incollaborationwithprogramfaculty,acceptsresponsibilityforthe
developmentofrelationshipswithrepresentativesoftheclinicaleducationsite.
Currentevidenceoutlinestheintentionalityofintegratedclinicaleducationexperienceplacement,purpose,necessaryresourceallocation,anddesiredoutcomeswithinphysicaltherapisteducationattheprogramlevel.Assuch,integratedclinicaleducationexperiencesmaybeembeddedwithinacourseoroccurconcurrentwithothercourseworkdependingonthedesiredprogrammaticand/orcourseobjectivesanddesireoutcomes.Intentionalityalsooccursinthedesign,resourcenecessities,andplacementofobjectivedrivencollaborativelearningexperiencesthatadheretopedagogicallysoundprinciplesthatareinnovativeand/orflexible(Fisheretal,2016)
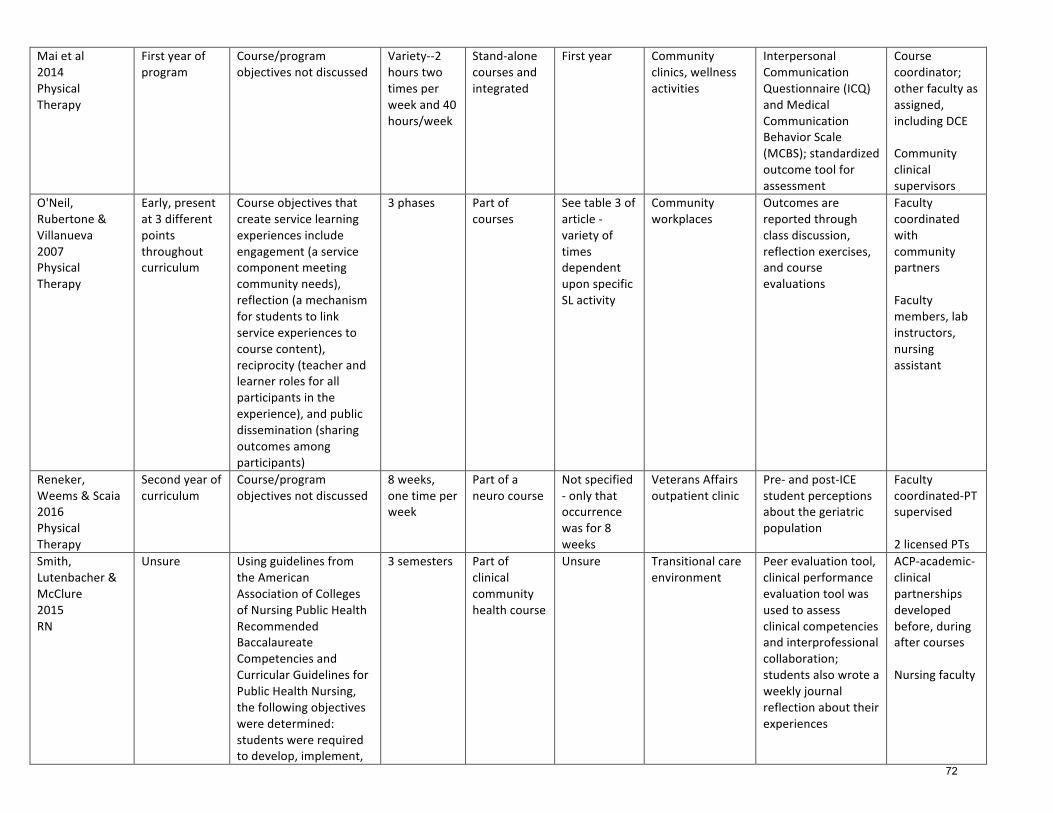
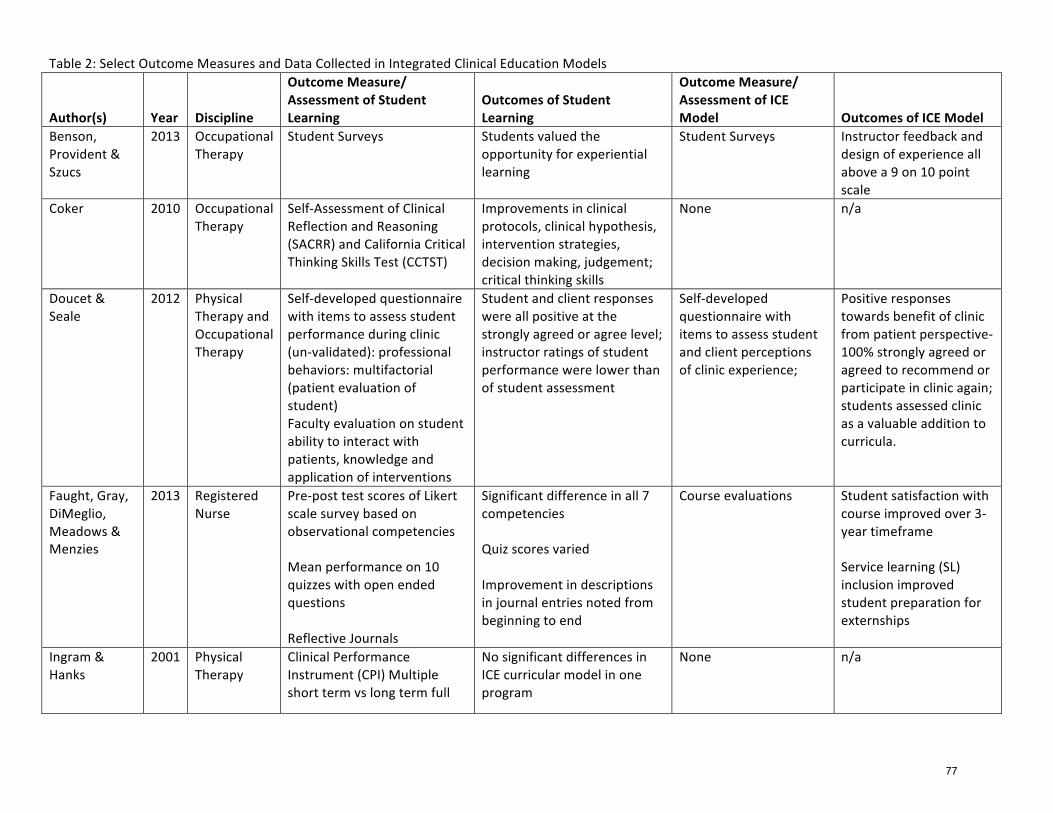
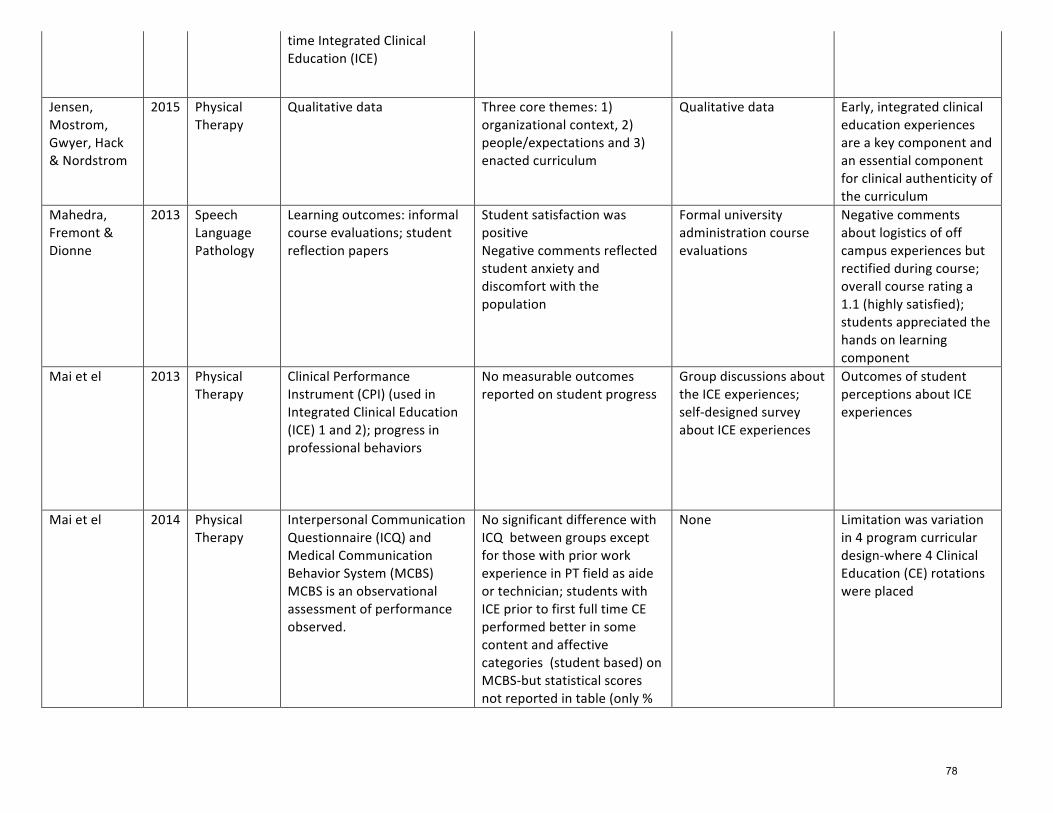
Whilemuchattentionshouldbeplacedonthedesignandimplementationofintegratedclinicaleducation,planningforandcompletingawell-roundedassessmentisalsorequired(Weddle&Sellheim,2009).Outcomeassessmentofstudentlearning,overallcoursesuccess,andtheintegratedclinicaleducationprogramdesignarethreetargetedareasforconsideration.Selectionofvalidandreliableoutcomemeasuresthatprovidefacultyandstudentssummativeandformativefeedbacktoguidelearningisimperative.Table2providesanexampleofoutcomemeasuresusedandtypeofdatacollectedthathaveguidedacademicprograms.Itisimportanttonotethatnoattemptsweremadetocomparemodelsoroutcomedata;ratherthedatageneratedprovidedathematicanalysisofimportantconceptswithintheliterature.
Despitethefactchallengesineducationalresearchexist(Jensenetal,2016),itbehoovesourprofessiontocontinueresearchingoutcomesofinnovativecurricularmodels,includingintegratedclinicaleducationexperiences,tocontinuetostriveforexcellenceinphysicaltherapisteducation.Therefore,furtherinvestigationintobestpracticeforICEexperiencesshouldcontinueinacollaborativemannerbetweeninstitutionaladministrators,academicphysicaltherapyfaculty,clinicalfaculty,patients,andstudents.Itishungerforimprovementthatpushesboundariestopromoteexcellence(Fullan,2005).
17
Page 19
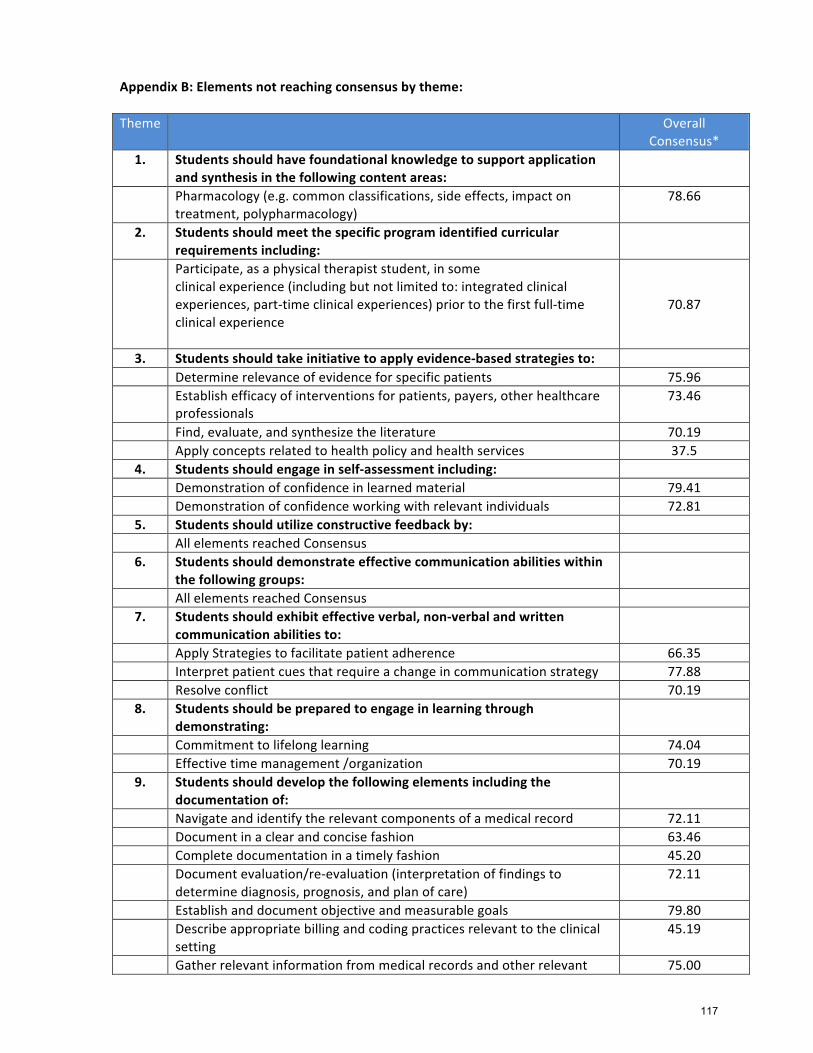
STUDENTREADINESSSTRATEGICINITIATIVEPANELSUMMARYOFWORKThepanelbeganbyreviewingliteraturefromdifferenthealthprofessionsincludingmedicine,pharmacy,nursing,speech,athletictrainingandoccupationaltherapy.Thepanelinvestigatedthevariedcompetencyexpectationsofthedifferentprofessionsaswellaswhenandhowtheyassessedstudentsatvariouspointsalongtheircontinuumoflearning.Theliteraturereviewrevealedthatcompetencybasededucationandsubsequentassessmentispresentthroughoutvarioushealthprofessions.Themedicalprofessionseemsmostevolvedandcanprovideuswithastructureandprocessthatwemightwanttoconsiderassuchsystemsaredevelopedforphysicaltherapisteducation.Beforeonecantrulydeveloptheappropriateassessmentsystem,theminimalknowledge,skills,attitudesandprofessionalbehaviors,collectivelyreferredtoasKSAs,andatwhatlevelofproficiencymustfirstbeidentified.Thepaneldiscussedvariouspossibleoptionstoestablishcompetenciesincludingobtainingconsensuswithinourpanel,focusgroups,consensusconference,surveys,andaDelphistudy.Toachievetheaimofourpanel,thegroupselectedtheDelphimethodofconsensusdevelopment.ADelphistudyallowsindividualswithexpertiseandinsighttoprovideinformationandtoreachconsensusonaparticulartopic.Thismethodengagesagroupofparticipantsorexpertsovermultipleroundsofsurveystoestablishaconsensusontheparticulartopicofinterest(Keeney,2011;Soma,2009).ThepurposeofthisDelphistudywastogainconsensus,definedas80%agreement,onthepre-requisitesforstudentsenteringafirstfull-timeclinicaleducationexperience,specificallyfocusingonwhatattributessignaledreadiness.Thisreadinessforthefirstfull-timeclinicaleducationexperiencewouldberelevantregardlessofwhereitfallswithinaprogram’scurriculumortheparticularsettinginwhichtheexperiencetakesplace.TheDelphimethodwasidentifiedasthemostpracticalmethodtogainconsensusamongthevariousmembersofthephysicaltherapypracticecommunity.Clinicians,recentgraduates,academicfaculty,andDirectorsofClinicalEducation/AcademicCoordinatorsofClinicalEducationwereidentifiedaskeystakeholders.GiventhevariabilityofcurriculuminCAPTEaccreditedphysicaltherapyprogramsaswellastheplacementofclinicalexperienceswithinthatcurriculum,thepanelthoughtitbesttobeginwithastudentsentranceintothefirstfull-timeclinicaleducationexperience.ThepanelalsofeltthattheearlyclinicalexperiencescanbeinanypracticesettingandareoftenthemostchallengingforDCEs/ACCEstofindstudentplacements,ascliniciansarereluctanttotakeonastudentwhileontheirfirstclinicalexperience.Startingwithcompetenciesforthisexperiencewouldonlybeonepointalongthecontinuumoflearningwherestudentswouldbeassessedbutwasanimportantplacetostart.AfterfourroundsoftheDelphistudywerecompleted,therewere95elementsidentifiedandagreeduponbythecombinedstakeholdersasbeingnecessaryforreadinessforafirstfull-timeclinicalexperience.These95elementsweregroupedunder14themes.Participantsalsoprovidedthelevelofproficiency(Familiar,Emerging,orProficient)deemedappropriateforeachitemidentified.Nineelementswereidentifiedasrequiringproficiencypriortothefirstfull-timeclinicalexperience(Table7).Themajorityoftheseelementsfellintheareaofprofessionalbehaviorswhileotherssurroundedsuccessfulacademicperformance.ParticipantsratedthevastmajorityofelementsasrequiringatleastanEmerginglevelofmastery(ratingsofEmergingorProficient)priortobeginningthefirstfulltimeclinicalexperience(AppendixA).Therewere,however,34elementsthatdidnotachievethelevelofconsensusrequiredtoindicatethattheybemorethanFamiliartothestudentpriortothefirstfulltimeclinicalexperience(AppendixA).
18
Page 20
AppendixC
StudentReadinessfortheFirstFull-TimeClinicalExperience
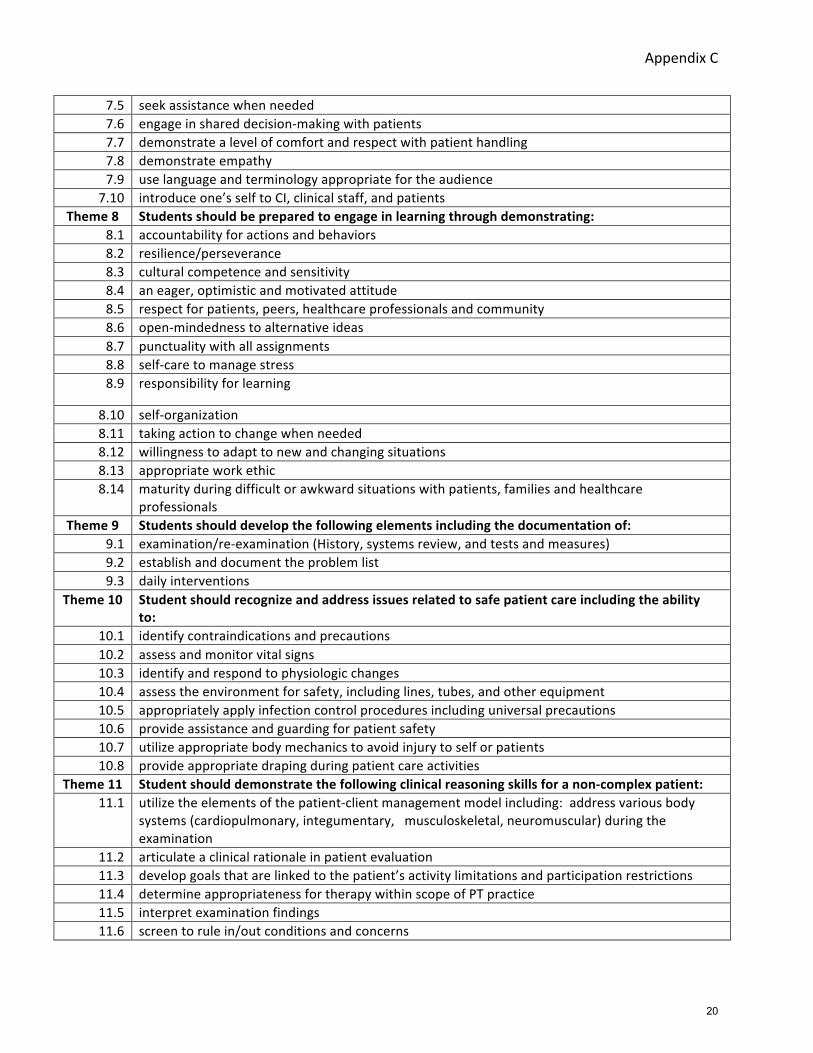
Thefollowingtablesummarizestheminimalknowledge,skillsandabilities(KSAs)inwhichphysicaltherapiststudentsmustdemonstratecompetencepriortoentryintothefirstfull-timeclinicalexperience.TheKSAsaregroupedinto14themes,numberedandindicatedinboldtextwiththecorrespondingKSAslistedbelow.Greaterthan80%ofparticipantsintheDelphistudyindicatedthattheseitemswerenecessary.
StudentReadinessThemesandKSAsTheme1 Studentsshouldhavefoundationalknowledgetosupportapplicationandsynthesisinthe
followingcontentareas:1.1 Anatomy(i.e.functionalanatomy)1.2 Commondiagnosesrelatedtosystemsreview(e.g.medical,physicaltherapy1.3 Kinesiology(i.e.biomechanics,exercisescience,movementscience)1.4 Physiology/Pathophysiology(relatedtogeneralsystemsreview)1.5 Tissuemechanics(e.g.stagesofhealing,use/disuse,load/overload)
Theme2 Studentsshouldmeetthespecificprogramidentifiedcurricularrequirementsincluding:2.1 achieveminimumGPA2.2 meetminimumexpectationsforpracticalexaminations2.3 remediationofanyandallsafetyconcerns
Theme3 Studentsshouldtakeinitiativetoapplyevidence-basedstrategiesto:3.1 generateinterventionsideas3.2 guidedecision-making3.3 measureoutcomes3.4 researchunfamiliarinformationorconditions
Theme4 Studentsshouldengageinself-assessmentincluding:4.1 self-assessmentoftheimpactofone’sbehaviorsonothers4.2 theunderstandingofone’sownthoughtprocesses(metacognition)4.3 self-reflectionandidentificationofareasofstrengthandthoseneedingimprovement,
developmentofaplantoimprove,anddiscussionofthatplanwithinstructors4.4 seekingoutresources,includingsupportfromotherswhenneeded,toassistinimplementationof
theplanTheme5 Studentsshouldutilizeconstructivefeedbackby:
5.1 beingopenandreceptive,verbally/non-verbally5.2 implementingactionstoaddressissuespromptly5.3 reflectingonfeedbackprovided
Theme6 Studentsshoulddemonstrateeffectivecommunicationabilitieswithinthefollowinggroups:
6.1 diversepatientpopulations6.2 familiesandotherindividualsimportanttothepatients6.3 healthcareprofessionals
Theme7 Studentsshouldexhibiteffectiveverbal,non-verbalandwrittencommunicationabilitiesto:7.1 listenactively7.2 demonstratepolite,personable,engagingandfriendlybehaviors7.3 independentlyseekinformationfromappropriatesources7.4 buildrapport
19
Page 21
AppendixC
7.5 seekassistancewhenneeded7.6 engageinshareddecision-makingwithpatients7.7 demonstratealevelofcomfortandrespectwithpatienthandling7.8 demonstrateempathy7.9 uselanguageandterminologyappropriatefortheaudience
7.10 introduceone’sselftoCI,clinicalstaff,andpatientsTheme8 Studentsshouldbepreparedtoengageinlearningthroughdemonstrating:
8.1 accountabilityforactionsandbehaviors8.2 resilience/perseverance8.3 culturalcompetenceandsensitivity8.4 aneager,optimisticandmotivatedattitude8.5 respectforpatients,peers,healthcareprofessionalsandcommunity8.6 open-mindednesstoalternativeideas8.7 punctualitywithallassignments8.8 self-caretomanagestress8.9 responsibilityforlearning
8.10 self-organization8.11 takingactiontochangewhenneeded8.12 willingnesstoadapttonewandchangingsituations8.13 appropriateworkethic8.14 maturityduringdifficultorawkwardsituationswithpatients,familiesandhealthcare
professionalsTheme9 Studentsshoulddevelopthefollowingelementsincludingthedocumentationof:
9.1 examination/re-examination(History,systemsreview,andtestsandmeasures)9.2 establishanddocumenttheproblemlist9.3 dailyinterventions
Theme10 Studentshouldrecognizeandaddressissuesrelatedtosafepatientcareincludingtheabilityto:
10.1 identifycontraindicationsandprecautions10.2 assessandmonitorvitalsigns10.3 identifyandrespondtophysiologicchanges10.4 assesstheenvironmentforsafety,includinglines,tubes,andotherequipment10.5 appropriatelyapplyinfectioncontrolproceduresincludinguniversalprecautions10.6 provideassistanceandguardingforpatientsafety10.7 utilizeappropriatebodymechanicstoavoidinjurytoselforpatients10.8 provideappropriatedrapingduringpatientcareactivities
Theme11 Studentshoulddemonstratethefollowingclinicalreasoningskillsforanon-complexpatient:11.1 utilizetheelementsofthepatient-clientmanagementmodelincluding:addressvariousbody
systems(cardiopulmonary,integumentary,musculoskeletal,neuromuscular)duringtheexamination
11.2 articulateaclinicalrationaleinpatientevaluation11.3 developgoalsthatarelinkedtothepatient’sactivitylimitationsandparticipationrestrictions11.4 determineappropriatenessfortherapywithinscopeofPTpractice11.5 interpretexaminationfindings11.6 screentorulein/outconditionsandconcerns
20
Page 22
AppendixC
Theme12 StudentshouldhaveBOTHtheunderstandingandskilltoperformthefollowingexaminationskills:
12.1 balanceassessment12.2 chartreviewtoextractrelevanthistory12.3 dermatomescreening12.4 functionalmobilityassessment12.5 gaitassessment12.6 goniometry12.7 interview/historytaking12.8 lowerquadrantscreening12.9 manualmuscletesting
12.10 musclelengthtesting12.11 myotomescreening12.12 reflextesting12.13 sensoryexamination12.14 medicalscreeningforredflags12.15 systemsreview12.16 upperquadrantscreening
Theme13 Studentshouldhavetheunderstandingandskilltoperformthefollowinginterventions:13.1 prescribe,fit,andinstructpatientsinproperuseofassistivedevices13.2 functionaltraining(includingbedmobility,transfers,andgait)withappropriateguardingand
assistance13.3 individualizedpatienteducation13.4 therapeuticexercise:specificallystrengthening13.5 therapeuticexercise:specificallystretching13.6 therapeuticexercise:specificallyaerobicexercise
Theme14 Studentshouldrecognizeandfollowspecificprofessionalstandards,including:14.1 appropriatedresscode14.2 corevaluesidentifiedbytheAPTAasaccountability,altruism,compassion/caring,excellence,
integrity,professionalduty,andsocialresponsibility14.3 clinicalexpectationsspecifictosetting14.4 HIPAAregulations14.5 legalaspectsrelatedtopatientcare14.6 obligationsofthepatient-providerrelationship14.7 passionfortheprofession14.8 patientrights14.9 maintainingprofessionalboundaries
14.10 understandingphysicaltherapy'sroleinthehealthcaresystem
21
Page 23
Attachment1
ACAPTStrategicInitiativePanels:SummaryofRecommendationsCommonTerminology
IntegratedClinicalEducationStudentReadiness
Eachofthe3panelsdevelopedrecommendationsbasedontheirwork.TheserecommendationshavebeenreviewedbytheACAPTBoardofDirectorsandwillbeconsideredbythememberinstitutionsattheACAPTbusinessmeetinginOctober2017.Thisdocumentisasummaryoftherecommendations.Astheserecommendationsarebeingreviewed,itisessentialtoreflectontheworkoftheClinicalEducationSummit.TheSummitgeneratedasignificantamountofenergyandenthusiasmaroundthetopicofPTclinicaleducation.AttendeeslefttheSummitanxioustotackletheideasgeneratedduringthetwo-daymeeting.
Asaresult,workonsomerecommendationshasbeenpickedupbygroupsoutsideofACAPTandsomehasbeguntooccurorganicallywithinthePTclinicaleducationcommunity.TheHouseofDelegateschargedtheAPTAtoassessissuesaroundPTclinicaleducationresultinginareporttotheAPTABoardfromtheAPTABestPracticeforClinicalEducationTaskForce.TworecentarticleshavebeenpublishedinthePhysicalTherapyJournal(PTJ)becauseoftheNationalStudyofExcellenceandInnovationinPhysicalTherapistEducation,aqualitativeresearchprojectrecentlycompleted.Thesethreeworksoutlineinnovativeresponsestotheissuesthatplagueourclinicaleducationsystem.
ThesepanelrecommendationsgrewoutoftheharmonizingrecommendationsfromtheClinicalEducationSummit.Thelistofharmonizingrecommendationssentaclearmessagethatweneedmorestandardizationinsomeareasofourclinicaleducationsystem.AchievingthisharmonizationisnecessarytomovetomoreinnovativeideasthatcanshapethefutureofPTclinicaleducation.TherecommendationsoftheACAPTpanels,ifadopted,willlayastrongfoundationwithcommonterminology,standardsforintegratedclinicaleducation,andconsistentassessmentofstudentreadinessforentryintofull-timeclinicalexperiencesonwhichinnovativeideascanbebuilt.COMMONTERMINOLOGYRECOMMENDATIONSRECOMMENDATION1(Terminology)ThatthePhysicalTherapistClinicalEducationGlossary(AppendixA)beadoptedandusedfordiscussionanddescriptionofphysicaltherapistclinicaleducation.SS:Usingacommonlanguagetodiscussphysicaltherapistclinicaleducationisessentialtoefficientandeffectivecommunication.TheparticipantsattheSummitcertainlyacknowledgedthisfactandthusdevelopedaSummitrecommendationrequestingacommonsetofterms.Inorderforthisinitiativetobesuccessful,itisessentialthatphysicaltherapisteducationprogramscommittoadoptionofthecommonterms.ItwillalsobeessentialthatprogramsrefrainfromuseofadditionaltermsnotincludedintheGlossarytodescribephysicaltherapistclinicaleducation.Thereisnodoubtthatchangeishardanditwilltakeworkforthecommontermstofilterdownintoorganizationaldocuments.However,inorderfortheinnovativechangesneededtorestructurethephysicaltherapistclinicaleducationinfrastructuretobeeffective,wemustbeginwithastrongfoundation.Commonterminologyenableseveryonetospeakthesamelanguageandhaveclear
22
Page 24
Attachment1
understandingabouttheclinicaleducationsystemwhichisanessentialbuildingblockofthesolidfoundation.RECOMMENDATION2(Terminology)That,followingadoptionofthePhysicalTherapistClinicalEducationGlossary,ACAPTworktoencourageadoptionofthenewterminologyinthedocumentsandsitesidentifiedinAppendixB.SS:AdoptionofthePhysicalTherapistClinicalEducationGlossarybyACAPTmemberinstitutionsisanessentialcomponentofdevelopingacommonlanguage.ThesecondcomponentofthisprocessistoensurethatthecommontermsareincludedindocumentsthroughoutACAPT,APTA,theEducationSection,andotherorganizationsthatimpactPTeducationsuchastheCommissionontheAccreditationofPhysicalTherapyEducation(CAPTE)andpotentiallytheFederationofStateBoardsofPhysicalTherapy(FSBPT).Speakingacommonlanguagerequiresthatallinterestedstakeholdersadoptthetermsandassociateddefinitions.ThisrecommendationsuggeststhatACAPTtakealeadershiproleinassistingwiththebroaddisseminationandrequestsforadoptionofthecommonterminology.CertainlyACAPTadoptionoftheGlossarydoesnotmakeitincumbentonsomeoftheorganizationslistedinAppendixBtoadopttheseterms.ItisthehopeofthePanelsthatACAPTleaderswillbeabletonegotiateoptionsandassistintheprocessfortheprofessiontoembracethesesuggestedtermsforcommonuse.RECOMMENDATION3(Terminology)ThatACAPTassistmemberinstitutionsindisseminatingthePhysicalTherapistClinicalEducationGlossarytotheirclinicalpartners.SS:Consideringtheimportanceoftheclinicaleducationcommunityembracingthenewcommonterminology,itisessentialtotheoverallsuccessofthisinitiativethatthedisseminationofthetermsandaneducationalprogramortoolstoassistclinicalfacultyinadaptingtothenewterms.Optionstoassistschoolsinthisprocessmayincludetrainingmaterials,linkstoonlineresources,etc.RECOMMENDATION4(Terminology)ThattheACAPTpolicyTerminologyforClinicalEducationExperiences(AC2-13)berescinded.SS:TheproposedPhysicalTherapistClinicalEducationGlossaryaddressesthetermsandsituationspreviouslydescribedbythispolicy.TheGlossaryisamorecomprehensivedocumentandthereforethecurrentpolicyshouldberescinded.Inaddition,thefinalreportfortheIntegratedClinicalEducationPanelincludesarecommendationtoaddthedefinitionforintegratedclinicaleducationtothePhysicalTherapistClinicalEducationGlossary.Onceapproved,theacronymICEwillbeassociatedwiththeterm‘integratedclinicaleducation’–not‘integratedclinicalexperience.’INTEGRATEDCLINICALEDUCATIONRECOMMENDATIONSRECOMMENDATION1(ICE)Thattheproposeddefinitionofintegratedclinicaleducation(ICE)beadoptedasthedefinitionforusewithintheprofession.
23
Page 25
Attachment1
SS:Consistentandproperuseoftheterm‘integratedclinicaleducation’isessentialtosuccessfulcommunicationwithintheacademicandclinicalenvironmentsofphysicaltherapisteducation.Thepanel,afterextensiveresearch,discussion,anddebatehasdevelopedadefinitionthatisclearandrepresentativeofthevarietyofsettingsandtypesofexperiencesthathavedevelopedwithinourprofession.ThedefinitionalsoincludesareferencetotheCAPTEcriteriaforfull-timeclinicaleducation,thusrecognizingthatICEcantakemanyforms,someofwhichmeetthecriteriasetforthinaccreditationstandards.RECOMMENDATION2(ICE)ThatthedefinitionofintegratedclinicaleducationbeaddedtotheglossarydevelopedbytheCommonTerminologypanel.SS:TheworkoftheCommonTerminologyPanelandICEPanelwascoordinatedtoensureconsistencyofterms.BecausedevelopmentofadefinitionforICEwasacomponentofthispanel’scharge,thedefinitionisprovidedinthereportandproposedforadoption.Onceadopted,itshouldbeincludedintheglossaryofterms,ensuringconsistentdisseminationofthetermandacronym.RECOMMENDATION3(ICE)ThatthecurrentlypublisheddefinitionofintegratedclinicalexperienceintheACAPTpolicyentitledTerminologyforClinicalEducationExperiences(AC2-13)berescinded.SS:AdefinitionforintegratedclinicalexperiencewasadoptedbyACAPTin2014.TheworkoftheICEpanelhasledtoarecommendationthattheappropriatetermisintegratedclinicaleducationandthattheexperiencesofICEarereferredtoasICEexperiences.Oncethisnewdefinitionforintegratedclinicaleducationisadopted,thetermanddefinitionfor‘integratedclinicalexperience’shouldberescindedtoensureconsistencyintheuseoftermsanddefinitions.RECOMMENDATION4(ICE)Thatthe8parametersaspresentedasbaselineexpectationsforintegratedclinicaleducationbeadoptedanddisseminatedforusebyphysicaltherapisteducationalprograms.SS:ParticipantsintheSummitrecognizedboththevalueofICEandthevariabilityofICEexperienceswithintheeducationalprograms.Asaresult,theparticipantsagreedthattheprofessionisbestservedbyinclusionofICEthatisbuiltonagreeduponstandardsfordesignandimplementation.The8parametersdevelopedbytheICEpanelprovidesuchguidance.Theseparametersweredevelopedafterextensivereviewoftheliterature,engagementwithstakeholders,discussion,anddebate.AdoptionoftheseparametersbyACAPTmemberinstitutionswillensurethatICEaredevelopedusingastandardizedsetofexpectationsyetcontinuetoallowandencourageeducationalprogramstoinvolvetheirstudentsinawidevarietyofICEexperiencestomeetuniqueneedsortakeadvantageofuniquesituations.ThisguidanceforICEdevelopmentwillalsoassistfacultyinensuringthattheexperiencesprovidedtostudentsarebasedonsoundeducationalpractices.RECOMMENDATION5(ICE)Thatthe10guidelinesfordevelopmentofintegratedclinicaleducationexperiencesbedisseminatedtophysicaltherapisteducationalprograms.
24
Page 26
Attachment1
SS:Distinctfromtheparametersdescribedabove,thepanelwasalsoaskedtoprovideguidancetoprogramsinterestedindevelopingICE.Thepaneldevelopedalistof10guidelinesthataddresstheintentionalstepsthatfacultyshoulduseandconsiderintheprocessofdevelopingICEexperiences.ThepanelbelievesthatthecombinationoftheparametersbeingusedasqualitystandardsalongwiththeguidelinestohelpguideICEdevelopmentwillensurethatphysicaltherapisteducationalprogramshavethetoolsnecessarytoprovidehighqualityandeffectiveICEtotheirphysicaltherapiststudents.RECOMMENDATION6(ICE)ThattheACAPTBoardofDirectorssharethisdocument,onceapproved,withthemembersoftheEducationalLeadershipPartnership(ELP)fordiscussiononhowtomoveforwardwithconsistentuseofthetermintegratedclinicaleducationwithinthephysicaltherapistclinicaleducationcommunity.SS:Ifwearetoachieveconsistentuseofthetermintegratedclinicaleducation,thetermanditsdefinitionwillneedtobedisseminatedbroadly.ThistermrepresentsachangefromthetermpreviouslyadoptedbyACAPTinthepolicy‘TerminologyforClinicalEducationExperiences’(AC2-13)andthusthechangewillrequireacoordinatedefforttoeducateeducationalprogramsandclinicalfacultyonthepropertermandproperusage.ELPiswellpositionedtoassistinthisinitiative.RECOMMENDATION7(ICE)ThatACAPTsupporteducationalresearchfocusedonprogrammaticoutcomesofdifferentmodelsofintegratedclinicaleducationusingstandardizedoutcomemeasures.SS:ThepanelwasaskedtodiscernanddescribemodelsofICEthatexistwithinphysicaltherapistcurricula.Thisportionofthechargewasaccomplishedbyathoroughreviewoftheliteratureandthemodelsweredescribedastheyrelatetothe8establishedparametersproposedbythepanel.Throughthisprocessthepaneldiscoveredthatalthoughmodelsaredescribedintheliterature,thereislittletonoassessmentoftheoutcomesofthevariousmodelsdescribed.Inresponsetothisfinding,thepanelisrecommendingthatadditionalresearchbedevelopedandsupported.FindingsfromthisresearchcanthenbeusedbythephysicaltherapyeducationalcommunitytodevelopthemosteffectiveandefficientmodelsofICE,thusenhancingtheeducationofthephysicaltherapiststudents.STUDENTREADINESSRECOMMENDATIONSRECOMMENDATION1(StudentReadiness)Thatthelistofknowledge,skills,andabilities(KSAs),groupedinto14themes,requiringstudents’demonstrationofcompetencepriortoenteringtheirfirstfull-timeclinicalexperienceasshowninAppendixC(FirstFull-timeClinicalExperienceKSAs)beadopted.SS:Academicprogramsshouldbeencouragedtoprovidestudentswiththeappropriateeducationalexperiences/modulessothatthestudentmayachievethelevelofproficiencyindicatedforthesaiditems(AppendixA).Thisinformationwouldensureconsistentpreparationpriortoastudent’sfirstfull-timeclinicalexperience.Giventhisinformation,clinicalinstructorscanbeconfidentthatstudentswouldbegintheirclinicalexperiencewithcompetencyintheseitemsandcanthereforedevelopandprovideamoreappropriatelearningenvironmentforastudenttocontinuetogrow.Theformatofthethemesandelementsmaybestartingpointsforthepotentialdevelopmentofentrustableprofessionalactivitiesandcompetencymilestonesthatwouldbeapplicabletoallstudentsinphysicaltherapisteducationpriortoentranceintotheirfirstfull-timeclinicalexperience.
25
Page 27
Attachment1
RECOMMENDATION2(StudentReadiness)ThatACAPTdevelopaplan,includinganimplementationtimeline,toguidephysicaltherapisteducationalprogramsinimplementingtheuseoftheFirstFullTimeClinicalEducationExperienceKSAs.Thisplanshallalsoincludeguidanceoncommunicationtoclinicalpartners.SS:AdoptingtheidentifiedKSAsisanimportantfirststepofthisinitiative.TheparticipantsintheSummitclearlyidentifiedaneedforconsistencyinthelevelofcompetenceofstudentsenteringtheirfirstfulltimeclinicalexperience.ThissetofKSAsprovidestheminimalexpectationsforthosestudents.InorderfortheeducationalprogramsandclinicalpartnerstoimplementtheseKSAs,additionalconsiderationstocommunication,assessment,expectations,andtimelinesneedtobeconsidered.RECOMMENDATION3(StudentReadiness)ThatACAPTencouragephysicaltherapisteducationalprogramstoevaluateandmakeappropriatechangestotheircurriculumtoenablestudentstoachievecompetencyintheFirstFull-timeClinicalExperienceKSAs.SS:Asdescribedabove,theclinicalsitesareanxiousforastandardsetofcompetenciesthatallfirstfull-timestudentshaveachievedpriortoarrivingintheirclinics.Onestepinachievingthisgoalrequireseducationalprogramstoassesstheircurriculumanddetermineifchangesareneededtoenablestudentstoachievethedescribedlevelsofcompetence.ManyprogramslikelyhavethecomponentsinplacethatenablestudentstomeettheseKSAs;otherprogramsmayneedtomakeonlysmallchangestoachievethisgoal;andstillothersmayneedtoconsidershiftintheprogramdesign.Inanycase,beingresponsivetotheSummitrecommendationsandthusthevoiceofourclinicalpartners,startswithanassessmentofcurrentstateandnecessarychanges.RECOMMENDATION4(StudentReadiness)Thatstudentreadinesspriortoentranceintoclinicalpractice(entry-level)beexaminedasthenextsteptoachievingtheSummitrecommendationsrelatedtoreadinessandcompetency.SS:Thispanelfocusedonstudentreadinessforentranceintothefirstfull-timeclinicaleducationexperience.Itrepresentsonemomentalongastudent’scontinuumoflearning.TheSummitparticipantsidentifiedtheneedforadditionalpointsofcompetenceassessment.Thevariabilityofnumber,length,andtimingofclinicalexperienceswithinphysicaltherapistcurriculamakestandardizationofcompetenceexpectationsatseveralpointsalongthestudent’seducationimpossible.ThisrealizationledtheStudentReadinesspaneltochoosethepointofentryintothefirstfull-timeclinicalexperienceasacommonpointthatwasappropriateforstandardization.Theotherpointintimethatlendsitselftostandardcompetenceassessmentisjustpriortoentryintopractice.Identifyingstandardelementsofcompetencethatshouldexistaftercompletionofalldidacticandclinicalcourseworkwillprovidevaluableinformationtoclinicalinstructorsandensureacommonlevelofpreparationforstudentsatentryintopractice.RECOMMENDATION5(StudentReadiness)ThatACAPTsupporttheneededcollaborativeeducationalresearchtodeterminethemostappropriatetypesofassessmentsofstudentreadinessandatimelineforimplementation.
26
Page 28
Attachment1
SS:ParticipantsindicatedthevariousassessmentmethodsthatcanbeutilizedforeachitemthatachievedconsensusintheDelphistudy(Table7).Thislistisnotmeanttobeprescriptivebuttoprovideoptionsforacademicprograms.TheseitemsreflectcurrentmethodsofassessmentandmaynotbethemostconnectedtowhatisusedinCBME.Nowthatconsensushasbeenachievedontheknowledge,skills,attitudesandprofessionalbehaviorsstudentsmusthaveordisplayandgiventheimportanceofassessmentandevaluationincompetency-basededucation,additionalresearchtodeterminethebestassessmentmethodsiswarranted.Bestpracticeshouldbeutilizedtodevelopacontinuedandfrequentassessmentprocesstoensurephysicaltherapiststudentsachievethemilestonesattheappropriatetimeintheircontinuumoflearning.Competency-basedphysicaltherapistclinicaleducation(CBPTCE)necessitatesarobustandmultifacetedassessmentsystem.Theleadershipwithinourprofessionmustattendtothecontextofthemultiplesettingswhereclinicaleducationoccurs.CBPTCE,likeCBME,furtherrequiresassessmentprocessesthataremorecontinuousandfrequent,criterion-based,developmental,work-basedwherepossible,useassessmentmethodsandtoolsthatmeetminimumrequirementsforquality,usebothquantitativeandqualitativemeasuresandmethods,andinvolvethewisdomofgroupprocessinmakingjudgmentsaboutstudentprogress.Inaddition,ashiftinthinkingneedstooccurfromassessmentoflearningtoassessmentforlearning.Researchintothequalityofassessmentprograms,howassessmentinfluenceslearningandteaching,newpsychometricmodelsandtheroleofhumanjudgmentismuchneeded(Schuwirth&VanderVleuten,2011)TheStudentReadinessStrategicInitiativePanel’srecommendationcomplimentswiththerecommendation#5bytheExcellenceinPhysicalTherapyEducationTaskForce(APTA,2015).Theynotetheprofessionshouldsupportthedevelopmentofastandardizedassessmentforphysicaltherapiststudentspriortoenteringtheirterminalclinicalexperience.Theassessmentwouldevaluatestudents’readinessfortheclinicaleducationandassistinimprovingrelationshipswithclinicaleducationsitesbysettingconsistentstandardsforstudentsbeforetheybegintheseexperiences.Theassessmentmayalsodecreaseunwarrantedvariationinstudentpreparation,whichwoulddecreasetheburdenonclinicalsitesduetodifferencesincurriculumacrossprograms.
27
Page 29
COMMONTERMINOLOGYSTRATEGICINITIATIVEPANELFinalReportJune2017
BACKGROUNDTheSummitrecommendationrelatedtocommonterminologywasbasedontheunderstandingandbeliefthattheabilitytouseconsistentlanguagebetweenacademicandclinicalfacilitiesisessentialforeffectiveandefficientbesteducationpractice.ThechargefortheCommonTerminologypanelwasbasedonthisSummitrecommendation.(RecommendationI)CHARGEInJanuary2016,theCommonTerminologyPanelwasconvenedtoaccomplishthefollowing:
1. Developcommonterminologyrelatedtophysicaltherapistclinicaleducation2. Developtemplatesormodelstosupportclinicaleducationsuchasrequestformsand
studentinformationforms.Inthespringof2017,thiswasmodifiedto:Suggestelementsofformstosupportclinicaleducation*
3. Investigateandidentifyallcurrentsourcesofterminologyrelatedtoclinicaleducationbyinvitingcollaborationwithvariousgroups,NCCE,EducationSection,CAPTE
4. Reviewallcurrentsupportdocuments,i.e.,CAPTE,CPI,GuidetoPTPractice5. Recommenditemsforconsiderationrelatedtocommonterminology6. Developguidelinesforimplementationoftheproposedterminology
*Therationaleforthischangeisbasedonanunderstandingthatmoreprogramsareadoptingelectronicsystemsbuiltbythird-partyvendorstomanageslotrequests,placementnotifications,andstudentinformationandthuspaperformsareusedlessfrequently.Inaddition,membersofthisPanelareawareofothergroupsattemptingtodevelopformsandhaveconcludedthattheirmostvaluablecontributionistosuggestelementstobeincludedoneitherpaperorelectronicforms.SUMMARYOFWORKFromFebruarytoApril2016,membersofthePanelgathereddata,whichincludedtermsandtheirdefinitionsrelatedtoanyaspectofphysicaltherapistclinicaleducation,fromallrelevantsources.SourcesincludedACAPT,APTA,CAPTE,ClinicalEducationSpecialInterestGroup(CESIG),FSBPT,clinicaleducationconsortia,residency,andfellowshipdocuments;clinicaleducationevaluationtools;ANormativeModelofPhysicalTherapistProfessionalEducation1;andmaterialsfromtheClinicalEducationSummit.Asystematicreviewoftheclinicaleducationliteraturewasalsoperformed.SystematicreviewThesystematicreviewincludedaMeSHandkeywordsearchinPubMedandCINAHL(1960topresent)usingtheterms“physicaltherapy”AND“clinicaleducation,”internship,“clinical
28
Page 30
instruct,*”preceptor,residency,fellowship,andterminology.HistoricaldocumentswerealsoretrievedfromtheAPTAandadditionalarticles,notalreadyidentifiedintheliteraturesearchwereretrievedfromtheAnthologyofClinicalEducation,Volumes1and2(Figure).Figure.Articlescreeningforsystematicreview.
Data,includingallrelevantdefinitionsrelatedtoclinicaleducationfromallrelevantsources,wereextractedfromallsources.Theterm,definition,andreferencewereplacedintoamasterspreadsheet.Themasterspreadsheetincluded260termsincluding6definitionsforclinicaleducation,12definitionsforacademiccoordinatorofclinicalinstruction,and15definitionsforclinicalinstructor.The260termswerecategorizedinto1of5clinicaleducationconstructsreportedintheliterature.2,3The5categorieswereinfrastructure,site,stakeholder,assessment,andother.ThePaneldividedintosubgroups(oneforeachoftheaforementionedconstructs)andunderwentthefirstroundofconsensusbuildingtoarriveatadefinition.Also,additionalliteraturefromotherprofessionsandfromnon-USpublicationswereaddedasneededwhentherewereconflictsfromtheinitialsearchinordertohelpinconsensusbuilding.Inthisinitialround,thenumberoftermswasreducedtoeliminateredundancyandadraftdefinitionforremainingtermswaspresentedbacktotheentirePanelforadditionaldiscussionandfurtherconsensusbuilding.ThetermsthatdidnotachieveconsensusbythePanelwerepresentedtotheaudienceinapresentationattheEducationLeadershipConferenceinOctoberof2016.Termswerediscussedinsmallgroupsandfeedbackfromthesmallgroupswasprovidedbackto
ScreenedTitles/Abstracts (n=452): PubMed=244 CINAHL=184 Historicaldocuments=24
PubMed=219 CINAHL=141 Historicaldocuments=24
Total=42
Excludedduplicates,non-US(n=68)
Excludedthosethatdidnotcontaindefinitions
(n=342)
29
Page 31
thePanel.Alltermsanddefinitionsweremadeavailabletoandadditionalfeedbackwassoughtfromthephysicaltherapycommunityina3-weekopencommentperiod(SurveyMonkey®,SanMateo,CA)inOctober2016.Therewere154respondentstotheopencommentperiod,62%academiciansand38%clinicians.UsingfeedbackfromtheEducationLeadershipConferenceandtheopencommentperiod,thePanelsubgroupsrevieweddefinitionsandintegratedfeedbackasappropriate.EditstothetermswerefurtherreviewedbytheentirePanelbetweenJanuaryandMarch2017whenconsensusonalltermswasachieved.ThefinalsetoftermscanbefoundinAppendixA.Useoftheterm“Internship”Followingtheinitialroundofconsensusbuilding,thePanelagreedthatthetermInternshipwouldbeusedtodescribeanyclinicaleducationexperiencethatoccurredfollowingthedidacticcurriculum.However,feedbackfromtheEducationalLeadershipConferenceandtheopencommentperiodindicatedthatsomestatesdonotallowuseoftheterminternshiptodescribeclinicaleducationexperiencesthattypicallyoccurinaphysicaltherapisteducationprogram.AdditionalresearchontheuseoftheterminternshipwasconductedbythePanelmembers.AccordingtotheUSDepartmentofLabor,WageandHourDivision,undertheFairLaborStandardsAct,therearecriteriathatmustbemettodetermineifaninternmustbepaidtheminimumwageandovertimewhenprovidingservicesinthe“for-profit”privatesector.Thefollowing6criteriamustbeappliedwhenmakingthedetermination:1.Theinternship,eventhoughitincludesactualoperationofthefacilitiesoftheemployer,issimilartotrainingwhichwouldbegiveninaneducationalenvironment;2.Theinternshipexperienceisforthebenefitoftheintern;3.Theinterndoesnotdisplaceregularemployees,butworksunderclosesupervisionofexistingstaff;4.Theemployerthatprovidesthetrainingderivesnoimmediateadvantagefromtheactivitiesoftheintern;andonoccasionitsoperationsmayactuallybeimpeded;5.Theinternisnotnecessarilyentitledtoajobattheconclusionoftheinternship;and6.Theemployerandtheinternunderstandthattheinternisnotentitledtowagesforthetimespentintheinternship.Ifallofthecriteriaaremet,anemploymentrelationshipdoesnotexistundertheFLSA,andtheAct’sminimumwageandovertimeprovisionsdonotapplytotheintern.4
30
Page 32
BaseduponreviewofthecriteriaandagreementwithinthePanelthata)studentsdoprovidepositivecontributionstotheclinicalsiteandb)theemployerdoesreceiveanadvantagefromthephysicaltherapiststudent,thereisthepossibilitythatanemploymentrelationshipcouldbeconstrued.Also,datafromthesmall-groupdiscussionsandopencommentperiodindicatedtherearestatelawsthatprecludeuseoftheterms“intern”and“internship.”Therefore,wearerecommending:a)theterminternshipshouldnotbeusedtodescribephysicaltherapistclinicaleducationexperiencesinwhichstudentsareeitherunpaidorpaidlessthanthefederalminimumwage;andb)theterminternshipcouldbeusedtodescribeaclinicaleducationexperienceinwhichparticipantsarebeingpaidinaccordancewithfederallaborlawsundertheFairLaborStandardsAct.Charge1:Developcommonterminologyrelatedtophysicaltherapistclinicaleducation.Theprocessdescribedaboveledtoasetoftermsforphysicaltherapistclinicaleducation.ThesetermshavebeenassembledintothePhysicalTherapistClinicalEducationGlossaryandareprovidedinAppendixA.Charges2,4,and6:SuggestelementsofformstosupportclinicaleducationReviewallcurrentsupportdocuments,ie,CAPTE,CPI,GuidetoPTPracticeDevelopguidelinesforimplementationoftheproposedterminologyAsdescribedabove,allsupportdocumentswereincludedintheinitialreviewofdocumentstodevelopthelistoftermsrelatedtophysicaltherapistclinicaleducation.AfterdevelopmentoftheGlossary,acomprehensivereviewofprofessionaldocumentswasconductedtoidentifythosethatwouldneedtobechangedtobeconsistentwiththeterminologybeingproposedbythePanel.Inadditiontothemanyformsinuse,policyandregulatorydocumentswereincludedinthereview.OnlyonedocumentwasidentifiedthatisinthepurviewofACAPT.TheresponsiblepartiesforthedocumentsandthegeneralmeansnecessarytomakechangesinthedocumentsarelistedinAppendixB.Charge3:Investigateandidentifyallcurrentsourcesofterminologyrelatedtoclinicaleducationbyinvitingcollaborationwithvariousgroups,NCCE,EducationSection,CAPTE.MembersofthePanelhavereachedouttootherstakeholdergroups,collaboratingandsharingtheworkbeingdoneacrossgroups.TherehasbeenongoingandextensivecollaborationwiththeIntegratedClinicalEducationPanelandtheStudentReadinessPanel.Wealsoinvitedcollaborationwithothersthrough1)roundtablediscussionswiththeparticipantsatthe2016EducationalLeadershipConference,2)anopencommentperiodprovidedformembersofthephysicaltherapyacademicandclinicalcommunities,and3)studentfocusgroupsduringthe
31
Page 33
NationalStudentConclaveandvirtuallyinNovember2016.ThisallowedmemberstoprovidefeedbackonadraftoftheGlossary.FeedbackwasusedfromtheroundtablediscussionsandthecommentperiodtodevelopthefinalGlossary.Charge5:Recommenditemsforconsiderationrelatedtocommonterminology.Primaryconsiderationsarerelatedtoadoption,inclusion,anddisseminationoftheterms.ThePanelhasdevelopedthreerecommendationstoaddresstheseitems.Anadditionalitemforconsiderationisrelatedtotheuseoftheterm‘internship.’Theinformationdetailedabovehasledthepaneltotheconclusionthatinthecurrentphysicaltherapistclinicaleducationinfrastructure,thetermisbeingusedinappropriatelyandtheclinicaleducationcommunityneedstotakestepstoeliminatetheuseoftheterm.ThePanelrecognizesthatsomeoftheinnovativechangescurrentlybeingexaminedmaypresentopportunityforappropriateuseoftheterminthefuture.ThePanelhasdevelopedonerecommendationrelatedtothisissue.RECOMMENDATION1:ThatthePhysicalTherapistClinicalEducationGlossary(AppendixA)beadoptedbytheACAPTmemberinstitutionsandusedfordiscussionanddescriptionofphysicaltherapistclinicaleducation.SS:Usingacommonlanguagetodiscussphysicaltherapistclinicaleducationisessentialtoefficientandeffectivecommunication.TheparticipantsattheSummitcertainlyacknowledgedthisfactandthusdevelopedaSummitrecommendationrequestingacommonsetofterms.Inorderforthisinitiativetobesuccessful,itisessentialthatphysicaltherapistprogramscommittoadoptionofthecommonterms.ItwillalsobeessentialthatprogramsrefrainfromuseofadditionaltermsnotincludedintheGlossarytodescribephysicaltherapistclinicaleducation.Thereisnodoubtthatchangeishard,anditwilltakeworkforthecommontermstofilterdownintoorganizationaldocuments.However,inorderfortheinnovativechangesthatareneededtorestructurethephysicaltherapistclinicaleducationinfrastructuretobeeffective,wemustbeginwithastrongfoundation.Commonterminologyenableseveryonetospeakthesamelanguageandhaveclearunderstandingabouttheclinicaleducationsystemwhichisanessentialbuildingblockofthesolidfoundation.RECOMMENDATION2:That,followingadoptionofthePhysicalTherapistClinicalEducationGlossary,ACAPTworktoencourageadoptionofthenewterminologyinthedocumentsandsitesidentifiedinAppendixB.
32
Page 34
SS:AdoptionofthePhysicalTherapistClinicalEducationGlossarybyACAPTmemberinstitutionsisanessentialcomponentofdevelopingacommonlanguage.ThesecondcomponentofthisprocessistoensurethatthecommontermsareincludedindocumentsthroughoutACAPT,APTA,theEducationSection,andotherorganizationsthatimpactPTeducationsuchasCAPTEandpotentiallyFSBPT.Speakingacommonlanguagerequiresthatallinterestedstakeholdersadoptthetermsandassociateddefinitions.ThisrecommendationsuggeststhatACAPTtakealeadershiproleinassistingwiththebroaddisseminationandrequestsforadoptionofthecommonterminology.CertainlyACAPTadoptionoftheGlossarydoesnotmakeitincumbentonsomeoftheorganizationslistedinAppendixBtoadopttheseterms.ItisthehopeofthePanelsthatACAPTleaderswillbeabletonegotiateoptionsandassistintheprocessfortheprofessiontoembracethesesuggestedtermsforcommonuse.RECOMMENDATION3:ThatACAPTassistmemberinstitutionsindisseminatingthePhysicalTherapistClinicalEducationGlossarytotheirclinicalpartners.SS:Consideringtheimportanceoftheclinicaleducationcommunityembracingthenewcommonterminology,itisessentialtotheoverallsuccessofthisinitiativethateducationalprogramsassistindisseminatingandaidclinicalfacultyinadaptingthenewterms.Optionstoassistschoolsinthisprocessmayincludetrainingmaterials,linkstoonlineresources,etc.RECOMMENDATION4:ThattheACAPTpolicyTerminologyforClinicalEducationExperiences(AC2-13)berescinded.SS:TheproposedPhysicalTherapistClinicalEducationGlossaryaddressesthetermsandsituationspreviouslydescribedbythispolicy.TheGlossaryisamorecomprehensivedocumentandthereforethecurrentpolicyshouldberescinded.Inaddition,thefinalreportfortheIntegratedClinicalEducationPanelincludesarecommendationtoaddthedefinitionforintegratedclinicaleducationtothePhysicalTherapistClinicalEducationGlossary.Onceapproved,theacronymICEwillbeassociatedwiththeterm‘integratedclinicaleducation’–not‘integratedclinicalexperience.’MEETINGHISTORYFace-to-facemeetings:February20,2016andOctober6,2016Conferencecalls:(2016)April12,May27,August12,August23,November28(2017)January24,January25,March28,May4,2017
33
Page 35
References1. AmericanPhysicalTherapyAssociation.ANormativeModelofPhysicalTherapist
ProfessionalEducation.Alexandria,VA;AmericanPhysicalTherapyAssociation;2004.
2. MooreML,PerryJF.Clinicaleducationinphysicaltherapy:presentstatus/futureneeds.Finalreportoftheprojectonclinicaleducationinphysicaltherapy.Washington,D.C.:SectionforEducationAmericanPhysicalTherapyAssociation;June1976;NO1-AH.
3. GwyerJ,OdomC,GandyJ.HistoryofclinicaleducationintheUnitedstates.JPhysTherEduc.2003:17(3):34-43.
4. U.S.DepartmentofLaborWageandHourDivision.FactSheet#71:Internship
programsundertheFairLaborStandardsAct.https://www.dol.gov/whd/regs/compliance/whdfs71.pdf.AccessedMay16,2017.
34
Page 36
PHYSICALTHERAPISTCLINICALEDUCATIONGLOSSARY
Thisglossaryoftermswasdevelopedafterareviewofthephysicaltherapyliterature,extensivediscussionanddebatebytheACAPTCommonTerminologyPanel,andengagementofkeystakeholderswithinthephysicaltherapyclinicaleducationcommunity.TheGlossaryisdividedintomajorcategoriesand,asapplicable,definitionsarereferenced. CLINICALEDUCATIONINFRASTRUCTURE Clinicaleducation Aformaltypeofsupervisedexperientiallearning,focusedon
developmentandapplicationofpatient-centeredskillsandprofessionalbehaviors.Itisdesignedsothatstudentsgainsubstantial,relevantclinicalexperienceandskills,engageincontemporarypractice,anddemonstratecompetencebeforebeginningindependentpractice.1-3
Clinicaleducationagreement
Aformalandlegallybindingagreementthatisnegotiatedbetweenacademicinstitutionsandclinicaleducationsitesorindividualprovidersofclinicaleducationthatspecifieseachparty'sroles,responsibilities,andliabilitiesrelatingtostudentclinicaleducation.4
Clinicaleducationcurriculum
Theportionofaphysicaltherapyeducationprogramthatincludesallpart-timeandfull-timeclinicaleducationexperiencesaswellasthesupportivepreparatoryandadministrativecomponents.4
Clinicaleducationexperience
Experiencesthatallowstudentstoapplyandattainprofessionalknowledge,skills,andbehaviorswithinavarietyofenvironments.Experiencesincludethoseofshortandlongduration(e.g.,part-time,full-time),provideavarietyoflearningopportunities,andincludecareofpatients/clientsacrossthelifespanandpracticesettings.Whiletheemphasisisonpatient-careskills,experiencesmayalsoincludeinter-professionalexperiencesandnon-patientcaredutiessuchasresearch,teaching,supervision,andadministration.Clinicaleducationexperiencesareapartoftheprofessionalcurriculumandincludeformalstudentassessment.5-8
Collaborativeclinicaleducationmodel
Aclinicaleducationexperienceinwhichtwo(ormore)physicaltherapiststudentsareassignedtoone(ormore)preceptor/clinicalinstructor(s).Thestudentsworkcooperativelyunderthepreceptor/clinicalinstructor(s).Examplesinclude2:1,2:2,3:1,etc.studenttopreceptor/clinicalinstructorratio.Studentsmaybefromthesameordifferentprogramsandmaybeatthesameordifferentlevelsoftraining.9-11
35
Page 37
Didacticcurriculum Thecomponentofthephysicaltherapistprofessionaleducationprogramthatiscomprisedofthecontent,instruction,learningexperiences,andassessmentdirectedbytheacademicfaculty.3,12,13
Fellowship Apost-professionalfundedandplannedlearningexperienceinafocusedareaofclinicalpractice,education,orresearch(notinfrequentlypost-doctoralorforpost-residencyorboardcertifiedtherapists).14
Full-timeclinicaleducationexperience
Aclinicaleducationexperienceinwhichastudentengagesforaminimumof35hoursperweek.Anintegratedclinicaleducationexperiencemaybeafull-timeclinicaleducationexperience;however,full-timeclinicaleducationexperiencesdesignatedtoachievetheminimumnumberofweekssetforthbyCAPTEaredirectedbyaphysicaltherapistclinicalinstructor.5,7
Firstfull-timeclinicaleducationexperience
ThefirstclinicaleducationexperiencedesignatedtoachievetheminimumnumberofweekssetforthbyCAPTEinwhichastudentengagesforaminimumof35hoursperweek.
Intermediatefull-timeclinicaleducationexperience
AclinicaleducationexperiencedesignatedtoachievetheminimumnumberofweekssetforthbyCAPTEinwhichastudentengagesforaminimumof35hoursperweekandreturnstotheacademicprogramforfurthercompletionofthedidacticcurriculum.
Terminalfull-timeclinicaleducationexperience
Asingle,orsetof,full-timeclinicaleducationexperience(s)designatedtoachievetheminimumnumberofweekssetforthbyCAPTEthatoccurafterthestudenthascompletedthedidacticcurriculumofaphysicaltherapistprofessionaleducationprogram.Studentsmayreturntotheacademicprogramfordidacticinstructionthatdoesnotrequireadditionalclinicaleducationexperiences.Theexpectedoutcomeofthefinal,orlastterminalexperienceisentry-levelperformance.7
Internationalclinicaleducationexperiences
Aneducationalopportunitythatastudentparticipatesin,outsideofthecountrywherethephysicaltherapisteducationprogramissituated,forwhichhe/sheobtainsclinicaleducationcredit.TheabbreviationICEshouldnotbeusedtodescribeaninternationalclinicaleducationexperience.7,15
Internship Aterminalfull-timeclinicaleducationexperiencethatprovidesrecompensetoparticipantsinaccordancewithfederallaborlawsundertheFairLaborStandardsAct.16
Learningexperience Anyexperiencewhichallowsorfacilitatesachangeinattitudeorbehavior.Aplannedlearningexperienceincludesalearner,anobjectiveforthelearner,asituationdevisedtoproducearesponsethatcontributestotheobjective,aresponsebythestudent,andreinforcementtoencouragethedesiredresponse.3
36
Page 38
Part-timeclinicaleducationexperience
Aclinicaleducationexperienceinwhichastudentengagesinclinicaleducationforlessthan35hoursperweek.Part-timeexperiencesvaryinlength.Apart-timeclinicaleducationexperiencemaybeconsideredanintegratedclinicaleducationexperiencedependingonthedesignoftheexperienceandthelearningobjectives.7,17
Physicaltherapistprofessionaleducationprogram
Educationcomprisedofdidacticandclinicaleducationdesignedtoassurethatstudentsacquiretheprofessionalknowledge,skills,andbehaviorsrequiredforentry-levelphysicaltherapistpractice.3,18,19
Physicaltherapistpost-professionaleducationprogram
Degreeandnon-degreebasedprofessionaldevelopmentforthephysicaltherapisttoenhanceprofessionalknowledge,skills,andabilitiesbeyondentrylevel.Examplesinclude,butarenotlimitedto,continuingeducationcourses,post-professionaldoctoraleducationprograms,certificateprograms,residency,andfellowship.19
Residency Post-professionalprogramsthatoccurafterthegraduatephysicaltherapisthasobtainedalicensetopractice.Theymaybeclinicalprogramsthatadvanceaphysicaltherapist'sknowledgeandskillsinpatient/clientmanagement,ornonclinicalfocusingonadvancingaphysicaltherapist'scareeroutsideofclinicalduties.20
CLINICALEDUCATIONSITES Clinicaleducationsite
Ahealthcareagencyorothersettinginwhichclinicaleducationexperiencesareprovidedforphysicaltherapiststudents.Theclinicaleducationsitemaybe,butisnotlimitedto,ahospital,agency,clinic,office,school,orhomeandisaffiliatedwithoneormoreeducationalprogramsthroughacontractualagreement.3,4
Clinicaleducationenvironment
Thephysicalspace(s),aswellasthestructures,policies,procedures,andculturewithintheclinicaleducationsite.
CLINICALEDUCATIONSTAKEHOLDERS Academicfaculty Teachersandscholarswithintheacademicinstitutiondedicatedto
preparingstudentsintheskillsandaptitudesneededtopracticephysicaltherapy.21
Academicinstitution Universityorcollegethroughwhichanacademicdegreeisgranted.4
Clinicaleducationconsortia
Nationalandregionalgroupsthatincludeacademicandclinicaleducationfacultyforthepurposeofsharingresources,ideas,andefforts.4
37
Page 39
Clinicaleducationfaculty
Theindividualsengagedinprovidingtheclinicaleducationcomponentsofthecurriculum,generallyreferredtoaseitherSiteCoordinatorsofClinicalEducation(SCCEs),preceptors,orclinicalInstructors.Whiletheacademicinstitutiondoesnotusuallyemploytheseindividuals,theydoagreetocertainstandardsofbehaviorthroughcontractualarrangementsfortheirservices.7
Clinicalinstructor(CI)
Thephysicaltherapistresponsibleforthephysicaltherapiststudentanddirectlyinstructs,guides,supervises,andformallyassessesthestudentduringtheclinicaleducationexperience.Whenengagedinfull-timeclinicaleducationdesignatedtomeettheminimumnumberofweeksrequiredbyCAPTE,theclinicalinstructormustbealicensedphysicaltherapistwithaminimumofoneyearoffulltime(orequivalent)post-licensureclinicalexperience.4,22,23
DirectorofClinicalEducation(DCE)
Academicfacultymemberwhoisresponsibleforplanning,directingandevaluatingtheclinicaleducationprogramfortheacademicinstitution,includingfacilitatingclinicalsiteandclinicalfacultydevelopment.22,24,25
Physicaltherapiststudent
StudentenrolledinaCAPTE-accreditedorapproveddevelopingphysicaltherapistprofessionaleducationprogram.Studentsshouldnotbereferredtoasaphysicaltherapystudent.
Preceptor Anindividualwhoprovidesshort-termspecializedinstruction,guidance,andsupervisionforthephysicaltherapiststudentduringaclinicaleducationexperience.Thisindividualmayormaynotbeaphysicaltherapistaspermittedbylaw.
SiteCoordinatorofClinicalEducation(SCCE)
Professionalwhoadministers,manages,andcoordinatesclinicalassignmentsandlearningactivitiesforstudentsduringtheirclinicaleducationexperience.Inaddition,thispersondeterminesthereadinessofpersonstoserveaspreceptorsandclinicalinstructorsforstudents,supervisespreceptorsandclinicalinstructorsinthedeliveryofclinicaleducationexperiences,communicateswiththeacademicprogramregardingstudentperformance,andprovidesessentialinformationtoacademicprograms.4,22,26
CLINICALEDUCATIONASSESSMENT Clinicalperformanceassessment
Clinicalperformanceassessmentencompassesformalandinformalprocessesdesignedtoappraisephysicaltherapiststudentperformanceduringclinicaleducationexperiences.Assessmentmaybeformativeorsummativeinnatureandperformedforthepurposesofprovidingfeedback,improvinglearning,revisinglearningexperiences,anddeterminingsuccessfulattainmentofstudentperformanceexpectationsduringclinicaleducationexperiences.3,22,27,28
38
Page 40
Clinicalperformanceevaluationtool
Avalid,reliable,andmultidimensionalclinicalperformanceassessmenttoolutilizedtodetermineif,andhowwell,astudentmeetsestablishedbehavioralobjectivesduringclinicaleducationexperiences.4,29,30,31
Entry-levelphysicaltherapistclinicalperformance
Performancethatdemonstratesknowledge,skills,andbehaviorsconsistentwitheffective,efficient,andsafepatient/clientmanagementtoachieveoptimaloutcomes.22,28
Supervision Theguidanceanddirectionprovidedtoaphysicaltherapiststudentbythepreceptororclinicalinstructor.Thisvariesbasedonthecomplexityofthepatientorenvironment;jurisdictionandpayerrulesandregulations;andabilitiesofthephysicaltherapiststudent.4,22,27
References
1. DelanyC,BraggeP.Astudyofphysiotherapystudents’andclinicaleducators’perceptionsof
learningandteaching.MedicalTeacher.2009;31(9):402-411.
2. OʼBrienB,TeheraniA.UsingWorkplaceLearningtoImprovePatientCare.AcadMed.2011;86(11):e12.
3. MooreML,PerryJF.ClinicalEducationinPhysicalTherapy:PresentStatus/FutureNeeds.Final
ReportoftheProjectonClinicalEducationinPhysicalTherapy.Washington,DC:SectionforEducationAmericanPhysicalTherapyAssociation;June1976;NO1-AH.
4. AmericanPhysicalTherapyAssociation.ThePhysicalTherapyClinicalInstructorEducationandCredentialingProgramManual.Alexandria,VA:AmericanPhysicalTherapyAssociation;2009.
5. TerminologyforClinicalEducationExperiencesProposedbyAcademicCouncilBoardofDirectors[ACAPTmotionAC-2-13].http://acapt.myriadmedia.com/docs/default-source/motions/2013-motions/ac-2-13_terminology_for_clincal_education_passed.pdf?sfvrsn=2.AccessedMay16,2017.
6. PivkoSE,AbbruzzeseLD,DuttarovP,HansenRL,RyansK.Effectofphysicaltherapystudents'clinicalexperiencesonclinicianproductivity.JAlliedHealth.2016;45(1):33-40.
7. CommissiononAccreditationinPhysicalTherapyEducation.StandardsandRequiredElementsforAccreditationofPhysicalTherapistEducationPrograms,2016.http://www.capteonline.org/AccreditationHandbook/.PublishedNovember11,2015,UpdatedMarch4,2016.AccessedApril10,2017.
8. GibersonTR,BlackB,PinkertonE.Theimpactofstudent-clinicalinstructorfitandstudent-organizationfitonphysicaltherapistclinicaleducationexperienceoutcomes.JPhysTherEduc.2008;22(1):59-64.
39
Page 41
9. RindfleschAB,DunfeeHJ,CieslakKR,etal.CollaborativemodelofclinicaleducationinphysicalandoccupationaltherapyattheMayoClinic.JAlliedHealth.2009;38(3):132-142.
10. DecluteJ,LadyshewskyR.Enhancingclinicalcompetenceusingacollaborativeclinicaleducationmodel.PhysTher.1993;73(10):683-689.
11. LadyshewskyRK.Peerassistedlearninginclinicaleducation:areviewoftermsandlearningprinciples.JPhysTherEduc.2000;14(2):15-22.
12. CommissiononAccreditationinPhysicalTherapyEducation.EvaluativeCriteriaforAccreditationofEducationProgramsforthePreparationofPhysicalTherapists.CommissiononAccreditationinPhysicalTherapyEducationWebsite.http://www.capteonline.org/uploadedFiles/CAPTEorg/About_CAPTE/Resources/Accreditation_Handbook/EvaluativeCriteria_PT.pdf.UpdatedAugust2014.AccessedApril10,2017.
13. KenyonLK,DoleRL,KellySP.Perspectivesofacademicfacultyandclinicalinstructorsonentry-leveldptpreparationforpediatricphysicaltherapistpractice.PhysTher.2013;93(12):1661-1672.
14. AmericanPhysicalTherapyAssociation.Clinicalexperienceterminologyforphysicaltherapists.http://www.apta.org/uploadedFiles/APTAorg/About_Us/Policies/Terminology/ClinicalExperienceTerminology.pdf.UpdatedDecember2009.AccessedApril10,2017.
15. PechakCM.Surveyofinternationalclinicaleducationinphysicaltherapisteducation.JPhysTherEduc.2012;26(1):69-77.
16. U.S.DepartmentofLaborWageandHourDivision.FactSheet#71:InternshipprogramsundertheFairLaborStandardsAct.https://www.dol.gov/whd/regs/compliance/whdfs71.pdf.UpdatedApril2010.AccessedMay16,2017.
17. AmericanPhysicalTherapyAssociation.2007-2008Factsheet:physicaltherapisteducationprograms.AmericanPhysicalTherapyAssociationWebsite.http://www.apta.org/AM/Template.cfm?Section=Home&TEMPLATE=/CM/.AccessedApril10,2017.
18. BarrJS,GwyerJ,TalmorZ.Evaluationofclinicaleducationcentersinphysicaltherapy.PhysTher.1982;62(6):850-861.
19. AmericanPhysicalTherapyAssociation.EducationForPhysicalTherapists:TerminologyUsedToDescribe[HODP05-07-11-04].https://www.apta.org/uploadedFiles/APTAorg/About_Us/Policies/HOD/Terminology/Education.pdf.UpdatedDecember14,2009.AccessedApril10,2017.
20. AmericanBoardofPhysicalTherapyResidencyandFellowshipEducation.Aboutresidencyprograms.http://www.abptrfe.org/ResidencyPrograms/About/.AccessedApril10,2017.
40
Page 42
21. Kondela-CebulskiPM.Counselingfunctionofacademiccoordinatorsofclinicaleducationfrom
selectentry-levelphysicaltherapyeducationalprograms.PhysTher.1982;62(4):470-476.
22. AmericanPhysicalTherapyAssociation.PhysicalTherapistClinicalPerformanceInstruments:Version2006.Alexandria,VA:AmericanPhysicalTherapyAssociation;2006.
23. HalcarzPA,MarzoukDK,AvilaE,BowserMS,Hurm,L.Preparationofentrylevelstudentsforfuturerolesasclinicalinstructors.JPhysTherEduc.1991;5(2):78-80.
24. BucciereiKM,BrownR,MaltaS.Evaluatingtheperformanceoftheacademiccoordinator/directorofclinicaleducation:toolstosolicitinputfromprogramdirectors,academicfaculty,andstudents.JPhysTherEduc.2011;25(2):26-35.
25. PerryJF.Amodelfordesigningclinicaleducation.PhysTher.1981;61(10):1427-1432.
26. PhilipsBU,McphailS,RoemerS.Roleandfunctionsoftheacademiccoordinatorofclinicaleducationinphysicaltherapyeducation:asurvey.PhysTher.1986;66(6):981-985.
27. KernBP,MickelsonJM.Thedevelopmentanduseofanevaluationinstrumentforclinicaleducation.PhysTher.1971;51(5):540-546.
28. TexasConsortiumforPhysicalTherapyEducationandResearchFoundation.PhysicalTherapistManualfortheAssessmentofClinicalSkills.Austin,TX:2004.
29. BeckelC,AustinT,KettenbachG,SargeantD.Computerandinternetaccessforphysicaltherapistclinicaleducation.JPhysTherEduc.2008;22(3):19-23.
30. FitzgeraldLM,DelittoA,IrrgangJJ.Validationoftheclinicalinternshipevaluationtool.PhysTher.2007;87(7):844-860.
31. HouselN,GandyJ.Clinicalinstructorcredentialinganditseffectonstudentclinicalperformanceoutcomes.JPhysTherEduc.2008;22(3):43-51.
41
Page 43
AppendixB.Typesofdocuments,methodsofchangeSectionAliststhematerialsanddocumentsthathavelanguagerelatedtoclinicaleducationthatwouldneedtobechangedtobeconsistentwiththeterminologyrecommendedinthisreport.SectionBprovidesthemechanismtoachievechange.A.Typeofdocument/site B.MethodforchangeAPTA’sHouseofDelegates(HOD)positions,standards,guidelines,policies,procedures
ProposerevisiontotheHODbyadelegation(Chapter,Section,Board)totheHouse
APTA’sBoardofDirectors(BOD)positions,standards,guidelines,policies,procedures
RequesttheBODtoconsiderrevision
APTAdocuments/site CPI,CSIF,CCCEmanual RequesttheBODtoconsiderrevisionAPTACCIP RequesttheBODtoconsiderrevisionAPTAWebsite RequesttheBODtoconsiderrevision WouldalsoneedtobeconsistentwithHODpolicies EducationSectionWebsite RequesttheSectiontoconsiderrevisionClinicalEducatorsSIGoftheSectionForm:Requestforclinicalsites
RequesttheSection/CESIGtoconsiderrevision
AmericanCouncilonAcademicPhysicalTherapy
Website ACAPTshouldmakechangeswhennewdefinitionsadoptedACAPTpolicyonClinEd ACAPTshouldmakechangeswhennewdefinitionsadoptedNCCE ACAPTshouldmakechangeswhennewdefinitionsadopted CommissiononAccreditationofPhysicalTherapyEducation(CAPTE)Standards
PetitionCAPTEasamajorstakeholderforchangesinStandards
FederationofStateBoardsofPhysicalTherapy(FSBPT)ModelPracticeActandindividualstatepracticeacts
WorkthroughFSBPTandindividualstateboards,incollaborationwithAPTA
Journalstylemanuals PTJshouldchangewithHODpolicy,requestothersdosothrough
informationpackettojournaleditorsandtheirsupportingSections Chapters Materialsformembers Requestchangethroughinformationpacket StatePracticeActs Requestchangethroughinformationpacket,interactwithFSBPTas
wellasindividualboardsSections/Academies Materialsformembers Requestchangethroughinformationpacket InformationtoABPTRFE,ABPTS RequesttheBODtodirectanynecessarychanges PTAcommunity WorkthroughtheEducationSectionPTASIG
42
Page 44
1
INTEGRATEDCLINICALEDUCATIONSTRATEGICINITIATIVEPANELFinalReportJune2017
BACKGROUNDTheSummitrecommendationrelatedtointegratedclinicaleducation(ICE)wasdevelopedaroundthepremisethatICE‘allowsstudentstodevelopcognitivepsychomotor,andaffectivebehaviorsforsuccessfulterminalexperiences.’(SummitReport)TheSummitparticipantsrecognizedthevariabilityinmodelsandapproachestoICEinthephysicaltherapisteducationcurriculaandthusidentifiedvalueinestablishmentofbaselineexpectationsforICE.ThechargefortheIntegratedClinicalEducationpaneladdressedthisSummitrecommendation(RecommendationVII)
CHARGEThespecificchargetothisworkpanelisto:1. Define‘integratedclinicaleducation.2. Makerecommendationsforachievingconsistentuseoftheterm‘integratedclinicaleducation’
acrossACAPT,APTAandCAPTE.3. Definebaselineexpectationsandparametersforqualityintegratedclinicaleducationinphysical
therapisteducation.4. Discernanddescribemodelsofintegratedclinicaleducationthatcurrentlyexistwithinphysical
therapistcurricula.5. Developguidelinesforcollaborativedevelopmentandimplementationofintegratedclinical
experiences.
Stakeholdersinvolved
TheWorkgroupwaspurposefullyselectedtorepresentstakeholdersfromboththeacademicandclinicalenvironments.Considerationsinselectingtheworkpanelmembersincluded:previousexperience/knowledgeofprofessionaleducationprogramswhereanintegratedmodelofclinicaleducationwasused,academicorclinicalpositionheld,geographiclocationandtypeofinstitutionrepresented(public/private).Theintentwastoselectadiversegroupthatwouldbeabletobringmultipleperspectivestotheconversation.Thepositionsheldofworkgroupmembersincluded:academicprogramdirectors,directorsofclinicaleducation,andacentercoordinatorofclinicaleducation/clinicalinstructor.
IndividualsinvolvedduringdatacollectionincludedacademicandclinicalfacultyaswellascurrentDPTstudentsfromacrossthecountry.
SUMMARYOFWORKPhase1:Weembarkedon2concurrentmethodsofdatacollectiontoestablishabroadviewofcurrenteducationalpracticesinvolvingclinicaleducationdeliveredthroughthelensofanintegratedcurriculumperspective.Thedatacollectionmethodsincludedasystematicreviewoftheliteratureandthedevelopmentanddistributionofadescriptivesurvey.Work-panelmembersvolunteeredtoworkinoneofthesetwogroupstogatherandanalyzethedata.Reviewoftheliterature.Thefirstsubgroupmemberswereinvolvedinasystematicreviewoftheliterature.Thesubgroupidentifiedthefollowinghealthprofessiondisciplinesforinclusion:medicine,nursing,physicaltherapy(PT),occupationaltherapy(OT)physicianassistant(PA)andspeechtherapy
43
Page 45
2
(SP).Theliteraturewassearchedusingstandarddatabasesknownforpublicationofeducationalresearchofthehealthprofessions.TheseincludedMEDLINEandCINAHL.Additionaldatabasesweresearchedformedicine,howevernofurtherarticleswereidentifiedthereforeMEDLINEandCINAHLweretheprimarydatabasesutilizedtocollectmedicineliterature.
ThePreferredReportingItemsforSystematicReviewsandMeta-Analysis(PRISMA)guidelineswereselectedtoguidetheprocess.Aworkgroupmemberwasassignedtooneofthesixselectedhealthprofessions.Eachindividualsearchedtheliteraturefromtheselectedhealthprofessiontonarrowtheliteraturebytitleandabstractreview.Inclusioncriteriaforthebroadinitialsearchincludedthesearchterms“integratedclinicaleducation”andthehealthprofession(i.e.medicine,nursing,physicaltherapy,physicianassistant,occupationaltherapyandspeech-languagepathology).Thisresultedin3808articles.SearchtermswererefinedusingkeyworksandsubjectheadingsineitherCINAHLorMEDLINE.Articleswerescreenedfortitleandabstractbythesubgroupmembers,whichyielded83articles.
Twogroupmemberscompletedthetaskoffull-textreviewofthe83articles.Inclusioncriteriawasrefinedtoincludearticlesthatincluded:amodeldescriptionofaclinicaleducationexperienceprovidedinanintegratedmanner,aclearpurposeofthearticle,identifiedoutcomemeasuresthatincludedatleastoneofthefollowing:studentoutcomes,courseoutcomesorprogrammaticoutcomes.ThearticlesalsowererequiredtobewritteninEnglishandaccessibleinfulltext.Thisprocessnarrowedtheselectedarticlesto19.Referencelistsofthesearticleswerereviewedwhichresultedinanadditional3articlesforinclusion.Atotalof22articleswereincludedinthefinalreviewoftheliterature.Thesearticlesrepresentthebestavailableevidenceaboutthetopicofintegratedclinicaleducationinhealthprofessions.
Surveyresearch.Thesecondsubgrouputilizedsurveyresearchtogatherinformationaboutcurrentprogrampracticesthatwereperceivedasintegratedclinicaleducationexperiences.AsurveytoolwasdevelopedanddistributedtotheICEwork-panelmembersusingSurveyMonkey(n-11).Thesurveyconsistedoftwodemographicquestions,threeglobalquestionsabouttheprogramsclinicaleducationcurriculum,and10questionsrelatedtoeachcourseconsideredasanintegratedclinicaleducationcourse-upto5courses.Thequestionsincluded1openended,and9closedquestionswithoptiontocomment,foramaximumofpotential50questionstobeanswered.
Analysis.Theresultsofeachofthesedatacollectionmethodswerethematicallycategorizedindependentfromtheother,followedbyanaggregationofthecategoriesforgroupdiscussion.Commoncategorieswereidentifiedbetweenthe2groupsofdata.Groupdiscussionensuedtodetermineiftheidentifiedcategorieswereconsideredsoundeducationalpracticesintermsofclinicaleducationexperiencesofferedinanintegratedfashionwithinaprofessionaleducationprogram.Agroupvotewastakenoneachidentifiedcategory.Thegroupagreedtousemajorityconsensusasanindicatorthecategoryshouldbeincludedasaprimaryparameterfordescribinganintegratedclinicaleducationexperience.
Phase2:Twoseriesoffocusgroupswereconductedtogainperspectivefromstakeholdersinvolvedinclinicaleducation.Thefirstfocusgroupwasanopeninvitationeducationalsessiontitled“ClinicalEducationSummitStrategicInitiatives:UpdatesandIdeas”atthe2016EducationalLeadershipConferenceinPhoenixArizona.Participantsincludedbothacademicandclinicaleducators.Duringthis90-minutesession,facilitatorsledsmallgroupdiscussionsusingpre-determinedquestionsaboutissues
44
Page 46
3
relatedtocurrentperceptionsofintegratedclinicaleducation.Theresultsweretranscribedonsite.Thetranscribeddatawasthencollatedthematicallyandanalyzedforcontent.
Thesecondseriesoffocusgroupswasheldwithphysicaltherapiststudents:thefirstatthe2016NationalStudentConclaveinMiami,FloridaandthesecondwasheldvirtuallyonNovember16,2016.Afacilitatorledapurposefuldiscussionwithstudentleadersofthenationalstudentbody.ThefacilitatortooknotesandcollatedthedatapriortosendingtotheICEwork-panel.
Afterreviewofbothsetsoftranscribedfocusgroupdata,itwasdeterminedapointofdatasaturationwasachieved.Nofurtherdatawassoughtfromotheracademicorclinicalfaculty,orDPTstudentstodeveloptheparameters.Whilecollectionofadditionaldatamayhaveprovidedthegroupwithadditionalexamplesofclinicaleducationexperiencesprovidedinanintegratedfashion,itwasdeterminedthemodeldescriptionsidentifiedintheliteraturewererichenoughforthegrouptomoveforward.
Results.ThefinalresultsofPhases1and2includedidentificationofeight(8)categoricalparametersthatachieved100%agreementbythe12work-panelmembers.Theseparametersdescribecomponentsrequiredforintegratedclinicaleducationexperiences.
Developmentofdefinition.
Oncethe8parameterswereidentifiedandapproved,asubgroupofthework-panelreviewedtheparameterdescriptionsandtheliteraturetodevelopthedefinitionofintegratedclinicaleducation.Thedevelopeddefinitionwasdistributedtothe12-memberwork-panel,followedbygroupdiscussionandaperiodofrevision.Afterrevision,agroupvotewastaken.Thegroupagreedtousemajorityconsensusasanindicatorthedefinitionshouldbeacceptedfordescribingintegratedclinicaleducation.Thedefinitionofintegratedclinicaleducationwasachievedby100%agreementbythe12work-panelmembers.
Developmentofdescriptivemodels
Themodeldescriptionsweregeneratedusingathematicanalysisprocessfromthe22selectedarticlesinthesystematicreview.Afullreviewofthemanuscriptswerecompletedbymembersofthework-panel,withdataextractedincluding:author(s),yearofpublication,discipline,placementofcourse(s)inrespecttotheentireeducationalcurriculum,courseorprogramobjectivesaddressesinmanuscript,frequencyoftheICEexperience,thetypeofcoursetheICEexperiencewasoffered(standalonecourseorembeddedwithinacourse),frequencyofICEexperience,locationofICEexperience,methodsofassessmentandoutcomesofassessments,andcoordinator/facilitatoroftheICEexperience.Datawassynthesizedbyparametertoprovideaqualitativedescriptionofeach.
TheworkpanelagreedthatthedescriptionsofmodelspresentintheliteraturewererichenoughtoprovideoutcomesforCharge4.Themembersrecognizethevarietyofeducationalcurricularmodelsanddesignspresenttodaywithinphysicaltherapyeducationprograms,anddeterminedthecollectivedescriptionofallavailablemodelswasoutsidethescopeofourcharge.Thereadersareencouragedtorefertoeachoftheselectedpeer-reviewedarticlesandtheirreferencesforacompletedescriptionofICEmodeldesigns.
45
Page 47
4
OUTCOMES
Charge1:Define‘integratedclinicaleducation.’Thefollowingdefinitionof‘integratedclinicaleducation’wasdevelopedasaresultoftheworkprocessdescribedabove.
Integratedclinicaleducationisacurriculumdesignmodelwherebyclinicaleducationexperiencesarepurposivelyorganizedwithinacurriculum.Inphysicaltherapisteducation,theseexperiencesareobtainedthroughtheexplorationofauthenticphysicaltherapistroles,responsibilitiesandvaluesthatoccurpriortotheterminalfulltimeclinicaleducationexperience.
Integratedexperiencesarecoordinatedbytheacademicprogramandaredrivenbylearningobjectivesthataresynchronouswithdidacticcontentdeliveryacrossthecurricularcontinuum.Theseexperiencesallowstudentstoattainprofessionalbehaviors,knowledgeand/orskillswithinavarietyofenvironments.Thesupervisedexperiencesalsoallowforexposureandacquisitionacrossalldomainsoflearningandincludestudentperformanceassessment.
Forintegratedclinicaleducationexperiencestoqualifytowardstheminimumnumberoffull-timeclinicaleducationweeksrequiredbyaccreditation(CAPTE)standards,itmustbefulltimeandsupervisedbyaphysicaltherapistwithinaphysicaltherapyworkplaceenvironmentorpracticesetting.
ICE=IntegratedClinicalEducation
Charge2:Makerecommendationsforachievingconsistentuseoftheterm‘integratedclinicaleducation’acrossACAPT,APTAandCAPTE
Thepanelhasprovidedrecommendationsrelatedtoachievingconsistentuseofthesetermsintherecommendationssectionofthereport.Theserecommendationsincludeadoptingthetermanddefinition,includingitinthePhysicalTherapistClinicalEducationGlossary,andengagingwiththeEducationLeadershipPartnership(ELP)tohelpdisseminateinformationandeducatestakeholders.
Inaddition,theterm“integratedclinicaleducation”willbedefinedinthesystematicreviewmanuscriptindevelopmentforpublication.Oncepublished,thedefinitionwillbeinprintforfuturereference.
Charge3:Definebaselineexpectationsandparametersforqualityintegratedclinicaleducationinphysicaltherapisteducation
Basedonthedescribedworkprocess,eight(8)parametershavebeendevelopedtodefinebaselineexpectationsforintegratedclinicaleducationexperiences.Theseinclude:
1.Integratedclinicaleducationmayoccurinanyacademictermpriortothecompletionofthedidacticcourseworkleadingtothecompletionofaterminalfulltimeclinicaleducationexperience.
46
Page 48
5
2.Integratedclinicaleducationexperienceswillhavespecificdesiredoutcomesthatcorrespondtocourseand/orprogrammaticobjectives.
3.Integratedclinicaleducationexperiencesmayberepresentedasacomponentofadidacticcourseorastandalonecoursethatoccursinasynchronousfashionwithotherdidacticcoursework.
4.Integratedclinicaleducationexperiencetimeframesaredevelopedbytheacademicprogrambaseduponthecourseand/orprogrammaticobjectives.Integratedclinicaleducationmayincludefulltimeand/orparttimeexperiences.
5.Integratedclinicaleducationexperiencesmayoccurinavarietyoflearningenvironmentsincludingcampusorcommunitybasedclinicalornon-clinicalsettings,baseduponthecourseand/orprogrammaticobjectives.Integratedfulltimeclinicaleducationexperiencesthatqualifyforaprogram’sminimumnumberofclinicaleducationweeksshallbecompletedinaphysicaltherapyworkplaceenvironmentorpracticesetting.
6.Integratedclinicaleducationexperiencesshallincludestudentassessmentsthataredesignedtolinktothecourseorprogramobjectiveswithexpectedstudentprogressioninprofessionalbehaviors,clinicalknowledge,and/orskills.
7. Integratedclinicaleducationexperiencesarecoordinatedbya facultymemberof theacademicprogram,inpartnershipwithacoordinatorfromtheclinicaleducationsite.
8. Integrated clinical education experiences are typically supervised by a course instructor and apreceptor.Thepreceptormaybeanacademiccoursefacultymember,aclinicalinstructor,orotherhealthcareprofessional at the site the student is engaged in theexperience,dependingupon thecourse and/or programmatic objectives. Integrated full time clinical education experiences thatqualifyforaprogram’sminimumnumberofclinicaleducationweeksshallbesupervisedbyalicensedphysicaltherapist.
Charge4:Discernanddescribemodelsofintegratedclinicaleducationthatcurrentlyexistwithinphysicaltherapistcurricula
Theeight(8)parametersrequiredofintegratedclinicaleducationexperiences(aslistedincharge3)areexplainedthroughmodeldescriptions.Thesedescriptionsweredevelopedfromthearticlesselectedduringthesystematicreviewoftheliterature.RefertoTable1foradescriptionofprogram/coursemodels.
1.Integratedclinicaleducationmayoccurinanyacademictermpriortothecompletionofthedidacticcourseworkleadingtothecompletionofaterminalfulltimeclinicaleducationexperience.
TheplacementandfrequencyofICEwithincurriculaisquitevariable.Integratedclinicaleducationhasbeenreportedtooccurasearlyasthefirstorsecondsemesterofyearone.WhilesomeprogramsincorporateICEaslateinaprogramasthethirdyear,themajorityofICEmodelsdescribedexperiencesthatoccurinyearsoneandtwo.Insomeprograms,ICEisnotanisolatedexperience,butratheronewherebystudentsareaffordedseveralopportunitiestoparticipateinoverthecourseofaprofessionalprogram.
47
Page 49
6
References:Coker,Doucet&Seale,2010;Doucet&Seale,2012;Faught,Gray,DiMeglio, Meadows&Menzies,2013;Goldberg,Richburg&Wood,2006;Hakim,Moffat&Beckeretal, 2014;Ingram&Hanks,2001;Mahendraetal2013;Maietal2013;Maietal,2014;O’Neil, Rubertone&Villaneuva,2007;Smith,Lutenbacher&McClure,2015;Stern&Rone-Adams, 2006;Weddle&Sellheim,2011;Wilson,2006;Wilson&Collins,2011;Yardley,Brosnan, Richardson&Hays2014.
2.Integratedclinicaleducationexperienceswillhavespecificdesiredoutcomesthatcorrespondtocourseand/orprogrammaticobjectives.
Integratedclinicaleducation(ICE)experiencesarepartofthephysicaltherapycurriculumthataredesignedtocontributetospecific,desiredoutcomesforcourseand/orprogramobjectives.Theoreticalknowledgethatstudentsgainintheclassroomcanbereinforcedwithconcrete,experienceswhenICEexperiencesareappropriatelyplacedinthecurriculumtoaugmentthecontentbeingtaughtanddesignedtomeetspecificlearningobjectives.Asthecurriculumprogresses,ICEexperiencescanbestructuredsothatstudentsdemonstrateagreaterbreadthandcomplexityofclinicalskills.PTstudentsmustapplyalldomainsoflearning(i.e.cognitive,affectiveandpsychomotor)tobesuccessfulinclinicalpractice.Theclassroomsettingdoesnotalwaysallowstudentstodemonstrateskillsinallthedomainsoflearning,astheywouldbeusedinprofessionalsettings.ICEexperiencesaffordstudentstheopportunitytodemonstratetheseskillsinsituationsthatreflectthecomplexityofthehealthcaredeliverysystem.Inthesesituations,studentsprioritizecare,demonstratecriticalthinking,andmakedecisionsinanevidence-basedmanner.ICEexperiencescanalsobedesignedtoincludeserviceactivitieswhichhavethepotentialtoinfluencestudents’futurebehaviorsrelatedtotheAPTACoreValuesandCodeofEthics.
Furthermore,ICEexperiencesmaybedesignedasinter-professionalactivitiessothatstudentscomprehendtheroleofothermembersofthehealthcareteam.ItisimportantthatacademicinstitutionspreparestudentPTstobeclinicalteachers,soICEexperiencescanbedesignedinwhichstudentsaregivenpeerteachingandassessmentopportunitiestopreparethemforfutureteachingroles.OtherexamplesofpracticeinwhichstudentscangainexperienceduringICEiswiththemanagementofpatientswhohavehighlyspecializeddiagnoseswhoareunderservedarechallengedwithcommunicationdisorders,havementalhealthdisordersandconveydivergentculturalvalues.
References:Benson,Provident&Szucs,2013;Doucet&Seale,2012;Faughtatal,2013; Goldbergetal,2006;Jensen,Mostrom,Gwyer,Hack&Nordstrom,2015;Maietal, 2013;Mehendraetal,2013;O’Neiletal,2007;Smithetal,2015;Stern&Rone-Adams, 2006;Stuhlmiller&Tolchard,2015;Weddle&Sellheim,2011;Wilson,2006.;Williams- Barnard,Sweatt,Harkness&DiNapoli,2004.
3.Integratedclinicaleducationexperiencesmayberepresentedasacomponentofadidacticcourseorastandalonecoursethatthatoccursinasynchronousfashionwithotherdidacticcoursework.
48
Page 50
7
Integratedclinicaleducationhasbeenfoundtooccurbothaspartofadidacticcontentcourseorasasingleorrepeatedstand-aloneclinicaleducationcourse(s).MostICEexperiencestendedtobeconductedparttimealthoughacoupleofexamplesincludedfulltimeexperiences.Incurrentphysicaltherapyliterature,therangeofstand-alonecourseswithinacurriculumhasrangedfromoneuptothreeseparatecourses.Withinasingledidacticcontentcourse,thesettingsaswellasthecoursesinwhichICEwasacomponentwerequitevariablewitharangefromneurological,geriatric,andbusinesscourses.Oneexamplethreadsintegratedclinicalexperiencesinavarietyofcommunitybasedsettingsthatarecomponentsofaseriesofcourseswithinthecurriculum.Literaturefromotherhealthcaredisciplines(includingmedicine,nursing,occupationaltherapy,andspeechpathologyrevealaslightlydifferentpictureinthatmostoftheintegratedexperienceswerepartofadidacticcontentcourse.Thesimilaritytothephysicaltherapyliteraturewasinthefactthatthetypeofcoursesinwhichtheseexperienceswerehousedwerequitevariableandincludedpediatrics,mentalhealth,dysphagia,aginganddementia,communityhealth,andalifespancourse.
References:Bensonetal,2013;Doucet&Seale,2012;Faughtetal,2013;Goldbergetal, 2006;Ingram&Hanks,2001;Maiatal,2013;Mahendraetal,2013;O’Neiletal,2007; Reneker,Weems,&Scaia,2016;Smithetal,2015;Stern&Rone-Adams,2006;Weddle &Sellheim,2011;Williams-Barnardetal,2004;Wilson&Collins,2011.
4.Integratedclinicaleducationexperiencetimeframesaredevelopedbytheacademicprogrambaseduponthecourseand/orprogrammaticobjectives.Integratedclinicaleducationmayincludefulltimeand/orparttimeexperiences.
Similartophysicaltherapisteducationcurricula,thetimeframesforICEexperiencesarequitevariable.ThetimeframesassociatedwithICEtendtobeselectedbasedonthecourseand/orprogrammaticobjectivesaswellaswhatismostfeasiblefortheacademicprogramandclinicalsite.SeveralacademicprogramshaveimbeddedICEintothecurriculumasearlyasthefirstsemester,whilealargemajorityofexperiencesareembeddedattheendoforfollowingthefirstyearoftheprogram.Integratedclinicaleducationexperiencesmayalsospanconsecutivesemestersandareembeddedaslateinacurriculumasyeartwooryearthree.Suchexperiencescanalsobeincorporatedafterafewweeksintoacourseorthelastfewweeksofacourse.
WhetherICEexperiencesareembeddedinacourseorareastandalonecourse,thereisalsovariabilityregardingthefrequencyandduration.Theexperiencesrangefromasmallnumberofhoursthatareprimarilyobservation(example:2hours/weekortotalof2hoursinasemester),toseveralweeksthatoccurthroughoutyear1,2andperhapsyear3,butallpriortotheterminalfulltimeterminalexperiences.Integratedclinicaleducationexperiencescanoccurasinfrequentasaquarterday/twiceweeklyone-halfday/weekoronefullday/weekandforlongerdurationsoftimesuchasparttimeforupto8weeksorfulltimefor1-4weeks.Theexperiencesdonotneedtooccuronaregularbasishowever,asstudentscanstillbenefitfromopportunitiestoparticipateinICEexperiencesthatoccurmultipletimes(6-16sessions)overthecourseofasemesterorseveralsemesters.
49
Page 51
8
References:Bensonetal,2013;Coker,2010;Goldbergetal,2006;Hakimetal,2014; Ingram&Hanks,2001;Jensenetal,2015;Mahendraetal,2013;Maietal,2013;O’Neil etal,2007;Renekeretal,2016;Stern&Rone-Adams,2006;Weddle&Sellheim,2011; Wilson,2006.
5.Integratedclinicaleducationexperiencesmayoccurinavarietyoflearningenvironmentsincludingcampusorcommunitybasedclinicalornon-clinicalsettings,baseduponthecourseand/orprogrammaticobjectives.Integratedfulltimeclinicaleducationexperiencesthatqualifyforaprogram’sminimumnumberofclinicaleducationweeksshallbecompletedinaphysicaltherapyworkplaceenvironmentorpracticesetting.
Integratedclinicaleducation(ICE)canoccurinavarietyofclinical,non-clinicalandcommunitysettings.Campusprobonoclinics,probonoprogramssuchasexercisewellnessorkids’fitness,ormoreestablishedcampusfacilitiessuchasanoutpatientclinicorprimarycareclinic)allowtheintegratedclinicalexperiencestobeconductedintheconvenienceoftheacademicinstitution.
OtheracademicprogramsusedoffcampuscommunitysettingstoconductICEwithawiderangeofclinicalsettingsincludinglongtermcare,acutecare,inpatientrehabilitationfacilities,skillednursingfacilities,outpatientorthopedicclinics,VeteransAffairsMedicalCenteroutpatientclinic,pediatricinpatientandoutpatientfacilitiesandcommunityhealthcarecenters.SeveralICEexperiencesusedacombinationofonandoffcampussettingsasresourcestomeettheirlearningobjectives.ICEisalsoconductedinwhataretypicallyconsiderednon-clinicalsettingsthatincludeseniorliving/communityretirementhomes,childdevelopmentcentersorcommunitybasedpreschools,residentialhomelessassistancecentersorshelters,communitybasedprogramssuchasfamilyfitnessandaquaticprograms,orseniorcitizenprograms/adultdaycare.Theunifyingfactorwithalloftheselocationsisthatthesettingallowsforhumaninteractions.
References:Bensonetal,2013;Coker,2010;Ingram&Hanks,2001;Maietal,2013;Mai etal,2014;Renekeretal,2016;O’Neiletal,2007;Stern&Rone-Adams,2006; Stuhlmiller&Tolchard,2015;Weddle&Sellheim,2009;Weddle&Sellheim,2011; Wilson,2006;Wilson&Collins,2011.
6.Integratedclinicaleducationexperiencesshallincludestudentassessmentsthataredesignedtolinktotheprogramorcourseobjectiveswithstudentprogressioninprofessionalbehaviors,clinicalknowledge,and/orskills.
InorderforICEexperiencestocontributetolearning,assessmentoftheexperienceandstudentlearningshouldbecompletedwithdirectandtimelyfeedback.Formativeassessmentcanbeprovidedbypeersorclinicalfaculty,butacademicfacultyshouldbeprimarilyresponsibleforsummativeassessmentandgradingofstudents’clinicalbehaviors.Assessmentsarechosentodeterminetheprogressionofthestudent’slearning;assessmentandreflectioncanalsoserveasacatalystforheightenedengagementwiththelearningprocess.
50
Page 52
9
WhentheobjectiveoftheICEistopreparestudentsforfuturefulltimeclinicaleducationexperiences,studentassessmentoftenincludeduseofoutcomemeasurementtools,suchastheClinicalPerformanceInstrument(CPI),May’sProfessionalBehavior/GenericAbilities,oraschooltracking/assessmentformorotherselectedstandardizedoutcomemeasurementtoolassessingclinicalknowledge,skillsorprofessionalbehaviors.Forexample,Maietal(2013)selectedtheInterpersonalCommunicationQuestionnaireandtheMedicalCommunicationBehaviorScaletoassessstudentlearningofcommunicationabilities,whileWeddle&Sellheim(2009)utilizedaprogramdevelopedonlinereportingformtotrackeachICEsession.
Additionalstudentassessmentmethodsincludefacultyinstructorledverbaldebriefinganddiscussionsessions,wherebycriticalquestionswereaskedandformalreflectionpapersassignedtodeterminethelevelofthestudent’scriticalthinking.Peer-assistedlearningwasalsobeneficial,wherebyfirstyearstudentsarementoredbythirdyearstudentsduringICEexperiences.Authorsrecommendthatreflectionjournalsorpapersincorporatestudentself-assessmentofcriticalfactorstodeterminelearning,anddevelopmentofreflectivepractitioners.
WhentheICEexperiencewasmorefocusedonanovelpracticeenvironment,studentassessmentswereconcentratedontheunderstandingofthehealthcaremaze,theabilitytocompareandcontrastsites,identifyclinicalandsocialbenefits,ordemonstrateinter-professionalskills.
Whentheexperiencewasanexperientiallabwithinacourseorafocusedclinicaleducationexperiencewithaspecificpatientpopulation,suchaspatientswithchildhooddisabilitiesoradultswithdementia,studentassessmentsincludedfacultyreviewofstudentdocumentationincludingpatientexaminations,evidence-basedtreatmentplansoronsiteassessmentofthetreatmentsession,andevaluationofthetherapeuticmannerofstudentperformanceinestablishingtherelationshipformedbetweenthestudentandthepatient.
Inaddition,someacademicprogramsusedstudentfeedbackandstandardizedassessmenttodetermineifthecurriculardesignedexperiencewasthebestapproachtoaccomplishthislearning.
References:Bensonetal,2013;Coker,2010;Doucet&Seale,2012;Faughtetal,2013; Goldbergetal,2006;Faughtetal,2013;Hakimetal,2014;Ingram&Hanks,2001;Mai etal,2013;Mahendraetal,2013;O'Neiletal,2007;Smithetal,2015;Stern&Rone- Adams,2006;Stuhlmiller&Tolchard,2015;Weddle&Sellheim,2009;Weddle& Sellheim,2011;Williams-Barnardetal,2004;Wilson,2006;Wilson&Collins,2011.
7. Integratedclinicaleducationexperiencesarecoordinatedbya facultymemberof theacademicprogram,inpartnershipwithacoordinatorfromtheclinicaleducationsite.
Integratedclinicaleducationexperiencesarecoordinatedbyafacultymemberoftheacademic programandanindividual(s)fromclinical/communitybasededucationsites.Ithasbeen suggestedthattheacademicprogrambetheresponsiblepartyforfacilitatingapartnership, buildingrelationships,andsharingintheeducativeelement.Severalauthorshavedescribedthe
51
Page 53
10
roleoftheacademicfacultymemberorthedirectorsofclinicaleducationindevelopingand sustainingtheclinicalpartnerships.
Theacademicprogramselectsclinicaleducationsitestopartnerbaseduponfactorssuchasgeographicalproximitytotheacademicinstitution,theavailabilityofthepatientpopulationdesired,theavailabilityofanonsiterepresentativetoorganizeonsitelogisticsandtheavailabilityofonsitestaffsupervisionbyapreceptor.RegardlessofthelocalityoftheICEexperienceortheonsitesupervisoridentity,theacademicfacultymemberisresponsibleforgrading/assessmentofstudentprogresstowardsthecourseorprogramobjectives.
References:Bensonetal,2013;Coker,2010;Doucet&Seale,2012;Faughtetal,2013; Goldbergetal,2006;Hakimetal,2014;Mahendraetal,2013;Maietal,2013;Smithet al,2015;Stuhmiller&Tolchardetal,2015;Williams-Barnardetal,2004;Wilson,2006.
8. Integrated clinical education experiences are typically supervised by a course instructor and apreceptor.Thepreceptormaybeanacademiccoursefacultymember,aclinicalinstructor,orotherhealthcareprofessional at the site the student is engaged in theexperience,dependingupon thecourse and/or programmatic objectives. Integrated full time clinical education experiences thatqualifyforaprogram’sminimumnumberofclinicaleducationweeksshallbesupervisedbyalicensedphysicaltherapist.
StudentswhoparticipateinICEmustbesupervised,atsomelevel,dependentontheobjective(s)oftheexperience.Threemodelsofsupervisionwereidentifiedintheliteraturethathighlightoversightoftheexperiences.Onsitesupervisionwasprovidedeitherby:1)anacademicfacultymember;2)anacademicfacultymemberplusacommunitybasedclinicianorotherrepresentativeor3)acommunitybasedclinicianorotherhealthcareprofessional.Manytimes,thecourseinstructoralsoservedastheclinicalpreceptorduringtheICEexperience.Regardlessofwhoservesastheonsitepreceptor,afacultycourseinstructoroverseesthecoursemanagementandgradingofstudentoutcomes.
References:Bensonetal,2013;Coker,2010;Doucet&Seale,2012;Goldbergetal, 2006; Ingram&Hanks,2001;Jensenetal,2015;Maietal,2013;O’Neiletal,2007; Renekeretal,2016;Stern&Rone-Adams,2006;Stuhlmiller&Tolchard,2015;Weddle &Sellehim,2009;Williams-Barnardetal,2004.
52
Page 54
11
Charge5.Developguidelinesforcollaborativedevelopmentandimplementationofintegratedclinicaleducationexperiences.
TheACAPTintegratedclinicaleducationwork-panelwaschargedwithdevelopingguidelinestoassistacademicprogramsinthedevelopmentandimplementationofintegratedclinicaleducationlearningexperiencesforstudents.Toaddressthischarge,thepanelcreatedguidingrecommendationsthatareofferedbelowinboldtext.Provocativequestionsfollowtheguidelineinitalicsforprogramstoconsiderandreflectonduringacurricularreviewprocess.Finally,eachguidingprincipleissummarizedusingtheevidencebehindtherecommendation(bullets).Thesummaryisinclusiveoftheliteraturereviewed,howevershouldnotbeconsideredanexhaustivereviewofeverypotentialpieceofevidencethatmaylendsupporttotheguidingprinciple.Figure1providesaframeworkforconsiderationinthedevelopmentandimplementationofintegratedclinicaleducationexperiences.
Figure1:GuidingPrinciplesforDevelopingandImplementingIntegratedClinicalEducation
OverallAcademicProgramDesign
Physicaltherapisteducationhashistoricallyincludedbothadidacticcomponentaswellasaclinicaleducationcomponentinitscurriculumdesign.Curricularmodelsvaryineducationalpatterns,includingtheoverallcurriculumdesign,aswellasthetimeandlengthofclinicaleducationpriortograduation(Jensenetal,2016).WhiletheclinicaldoctorateinphysicaltherapyistheexpecteddegreeearnedtoentertheprofessionofphysicaltherapytodayintheUnitedStates,nostandarddesignmodelsguidethedevelopmentofcurriculumtoincludeboththedidacticandclinicaleducationcomponents(Engelhard&McCallum,2015;Jensenetal,2016).
Whiledesignmodelsvary,thereisabodyofknowledgethatsupportsstudentlearninginauthenticworkplaceenvironments.Scholarsofeducationalphilosophyhavefoundthatearly,authentic
53
Page 55
12
experiencesenhancelearning(Dewey,1944;Shulman,2004;Jensenetal,2015;Weddle&Sellheim,2009).Theselearningexperiencesprovidestudentswithamechanismtoattachalifeexperiencewiththeoreticalknowledge,resultinginmorecomplexinsighttobasicconcepts(Hakimetal,2014).Theinclusionofclinicaleducationexperiencesthroughoutastudent’sacademicprogramappearstoprovideanenvironmentfortransformativepractice,wherestudentscanfocusonliveexperiencesduringimmersionactivities(Bensonetal,2013).Reallifeexperiencessupportthedevelopmentofskills,reinforcesacademicknowledge,facilitatestheclinicalreasoningprocessanddevelopsself-confidencewithservicedelivery(Bensonetal,2013).
Designingaprofessionaleducationcurriculumischallengingtoensurestudentsmastertheexpectedknowledge,skillsandbehaviorsoftheprofession.Itisan“educator’sresponsibilitytoprovidestudentswithlearningopportunitiesthatdeveloptheabilitytoengageincomplexitiesofclient-centeredpractice”(Knetch-SabresinBensonetal,2013).Itisevenmorechallengingtodesignclinicaleducationexperiencesthatareintegratedinapurposefulmannerthroughoutanacademicprogrambecauseoftheneedforaflexiblecurriculardesign,theneedforadministrativesupportandtheneedtostayabreastofthedynamicsofthehealthcareenvironment(Jensenetal,2015).Educatorsmustattendtocriticalcomponentsofcurriculumdesigntoensureeffectivelearningopportunitiesforstudents.Thesecriticalcomponentsinclude:timespentdesigningtheexperience,conductingtheapplication,evaluatingtheoutcomesandprovidingfeedbacktostudents(WolfeandByrneinBensonetal,2013).Asaresult,10keyguidelinesareofferedforacademicprogramconsiderationduringthedesign,implementationandreviewofintegratedclinicaleducationexperiences.
Guidelines
1. Anacademicprogramshouldidentifytheprogrammaticoutcomesthatareexpectedwhenstudentsparticipateinintegratedclinicalexperiences.
Questiontoconsider:Doesmyprogramhaveexpectedprogrammaticoutcomesthatcouldbeorshouldbemetbyprovidingstudentsintegratedclinicaleducationexperiences?
• Experientiallearningshouldbeintentionalfromaprogramlevelandnotjustacourselevel(Hakimetal,2014).Itisimportant,therefore,foreducatorstodeterminetherationalefor,andidentificationof,theexpectedprogramoutcomesexpectedtobeachievedbyparticipationinintegrationofclinicaleducationexperiencesinone’sacademiccurriculum.
• Opportunitiesshouldbeprovidedforstudentstodemonstrateknowledge,psychomotorand/orbehavioralskillsinactualclinicalsettingswithpatientswhomaypresentwithphysical,emotionalandcognitiveimpairments,inanunpredictableenvironment.Someexperiencescouldinclude:o 1)thecommunicationandprofessionalbehavioralskillsnecessaryforclinicalpractice;o 2)effectivepsychomotorskillsonindividualsotherthanhealthy,unimpairedclassmates;
ando 3)anappreciationoftheroleinter-professionalcollaborationinthedeliveryofhealthcare
(Bensonetal,2013;Jensonetal,2015;Maietal,2014).• Programmaticconsiderationofintegratedclinicaleducationexperiencescouldinclude:
o Physicaltherapiststudent’sdemonstrationofskillsinvolvingthedomainsoflearning-i.e.cognitive,affectiveandpsychomotor,aswellasdemonstrationofclinicalreasoningand
54
Page 56
13
problemsolvingskillstosuccessfullyentertheprofession.Students’expectationstodevelopanappreciationforethicalpracticeandthecorevaluesadoptedbytheprofession.
o Physicaltherapypracticeisexpandingintoareasofwellnessandotherareasofhealthcarewherepatientshavebeenunderserved.Studentexposuretotheseactivitiesinuniquesettingsallowstudentstodevelopanexpandedviewofprofessionalpossibilitiesforpracticeandtheneedsofcommunities.
• Physicaltherapiststudentsareeducatedtouseevidencetosupporttheirpractice.Applicationofevidencebasedpracticeinauthenticsettingsallowstudentstoapplyallaspectsofevidencebasedpracticethatisbasedonacombinationof“patientvalues,clinicalexpertiseandbestresearchevidence(Sackettetal,2000).
2. Theacademicprogramconsiderstheintentionalplacementofintegratedclinicaleducationexperienceswithinitscurriculum.
Questionstoconsider:Doesmyprogramconsidertheintentionalplacementofintegratedclinicaleducationexperiencesthroughouttheentiretyoftheprogram?Isthereasoundrationalewhereintegratedclinicaleducationexperiencesareplacedwithinthecurriculum?
• Avarietyofmodelscouldbeconsideredforintegratedclinicaleducationwithinaprogram,addressingplacementandtype(Hakimetal,2014;Jensenetal,2015).Threetimeframescouldbeconsidered:o Year1:EarlyICE,ineitherSemester1,2or3;o Year2:MidCurricularICE;ineitherSemester1,2or3;o Year3:LateICE;priortothecompletionofaterminalfulltimeclinicaleducationexperience.
• Typesofexperiences:o Full-timeorparttimemodelso Overaweeks’timeorspanmultipleweekso Offeredonetimeonlyordispersedthroughoutthecurriculumplano Decisionsaboutplacementandtimeframesshouldbebaseduponprogramandcourse
objectivesandthedecisionofthefaculty.• Considerationshouldbegiventothecomplexityoftheexperiencewithincreasinglevelsof
studentperformancewithsuccessiveexposuretoclinicalenvironmentsthroughoutthedidacticportionofthecurriculum(Hakimetal,2014).
• Considerationforpeerlearningmayalsobeacomponentofintentionalplacementofintegratedclinicaleducationexperienceswithinanacademicprogram.Integratedclinicaleducationexperiencesmaybedesignedsuchthatupperlevelstudentsmentorlowerlevelstudentstopreparethemforrolesasclinicalinstructors,orprovideastructuredenvironmentforbothsetsofstudentstolearnessentialskills(Wilson,2006).
3. Theacademicprogramidentifiesthecourse(s)whereclinicaleducationshouldbeintegratedwithintheprogram.
Questiontoconsider:Doesmyprogramhaveidentifiedcourseswhereintegratedclinicaleducationexperiencesareprovidedorcouldbeofferedinthefuture?
55
Page 57
14
• Integratedclinicaleducationexperiencesmaybeofferedasdistinct,stand-alonecoursesthatarecreditbearingwithinthecurriculumand/orexperiencesthatareembeddedwithinexistingcoursesinthedidacticcurriculum.
o Considerationstodetermineifintegratedclinicaleducationexperiencesshouldbeembeddedwithinacourseorastand-alonecourseshouldbegiventothegoalsandobjectivesofthecourseandexpectedstudentoutcomes.Thismaybeparticularlyusefulwhencoursecontentisabstractanddifficultforstudentstounderstand(e.g.BensonOT,1of-3interventionscoursesforNeurologicalandSensorimotorFunction)
o Itmaybebeneficialtodesignstand-aloneintegratedclinicaleducationcoursesiftheintendedgoaloftheexperienceistodemonstrateskillsandbehaviorswhichspanmultiplecontentareas.Thismayactuallypromotestudents’clinicalreasoningandintegrationofcoursematerialacrossthecurriculumbecausestudentslearnbycreatingtheirownunderstandingofinformation(Benson,2013).
4. Theacademicprogram,incollaborationwithprogramfaculty,developsthecoursespecificobjectivesforstudentachievementwithinanintegratedclinicaleducationexperience.
Questionstoconsider:Doeachoftheidentifiedcoursesthatofferanintegratedclinicaleducationexperiencehavespecificcourseobjectivesthataretobemetthroughtheexperientiallearningexperience?Dothecourseobjectivesrelatetotheoverallprogrammaticoutcomes?
• Courseobjectivesorprogrammaticobjectivesshouldguidestudentlearninginintegratedclinicaleducationexperiencesbyclearlyidentifyingthecognitive,psychomotorand/oraffectivedomainsoflearningexpectedofstudentsinordertomaximizeprofessionalgrowth(Hakimetal,2014;Jensenetal,2015;Maietal,2013).
• Objectivesforintegratedclinicaleducationexperiencescanguide:o thetransfer,applicationandreinforcementofclassroomlearningtoauthentic
patient/clientsituations(Hakimetal,2014);o thedevelopmentofcommunicationskills,interpersonalcommunicationskills
collaborationandconflictmanagement(Hakimetal,2014;Jensenetal,2015);o theapplicationofevidencebasedpracticeskills(Maietal,2013);o thedevelopmentoftherapeuticrelationshipsratherthansolelyanopportunityfor
learninginterventions(Bensonetal,2013); o theexposuretoemotional,psychologicalandsocialelementsofpatient/client
management(Hakimetal,2014);o theattainmentofaprofessionalidentityamongstudentphysicaltherapists.
5. Theacademicprogram,incollaborationwithprogramfaculty,identifiesthetimingandtimeframesofwhenclinicaleducationexperiencesshouldbeintegratedwithincourse(s).
Questionstoconsider:Whereshouldtheintegratedclinicaleducationexperiencesbeplacedwithinacurriculum?Withinacourse?Howmuchtimeshouldbeallocatedtointegratedclinicaleducationexperiencestomeetthedesiredoutcomes?
56
Page 58
15
• Thetimingandtimeframesoftheintegratedclinicaleducationexperiencesaredeterminedbytheprogramfacultyandtheintendedcoursegoalsandobjectivesaswellasprogrammaticoutcomes(Hakimetal,2014).
o Curricularflexibilityisneededwhendesigningintegratedclinicaleducationexperienceswithinacurriculumtoallowformodificationoftimingandstructuretoensurestudentlearningandcourse/programoutcomesarebeingachieved.(Hakimetal,2014;Jensenetal,2015;Wilson,2006)
• Theacademicprogramshoulddetermineareasonableamountoftimeinwhichskillsshouldbepracticedcreatingafavorablelearningenvironment.(Bensonetal,2013)Studentsmaybeinvolvedinintegratedclinicaleducationexperiencesfortimeperiodsthatrange:
o from1-2hours,o tohalfdays,o tofulldays.o Thefrequencyoftheseexperiencesmayrangefromisolateddaysthroughouta
curriculumtoregularlyscheduled,frequentdaysthroughoutsemesters.• Theexacttimingandconstructionofthesetimeframesarehighlyvariablebutshouldbe
offeredinasynchronousmannerwithotherdidacticprogramming(Bensonetal,2013).
6. Theacademicprogram,incollaborationwithprogramfaculty,identifiestheindividualorindividualswhowilloverseetheintegratedclinicaleducationexperiences.
Questionstoconsider:Whoshouldoverseetheorganizationanddeliveryofintegratedclinicaleducationexperiences?Shouldoneormoreindividualsmanagethecourse?Whoisresponsiblefortheonsitesupervisionofstudentsduringintegratedclinicaleducationexperiences?Whatisafeasiblepreceptortostudentratioduringanintegratedclinicaleducationexperiencetomeetthedesiredoutcomes?
• Academicleadershipisrequiredtoidentifyacoursecoordinatortooverseetheintegratedclinicaleducationexperiencetoensurethecriticalcomponentsofdesign,applicationandevaluationofbothstudentandcourse/programoutcomesisachieved.
o Afacultymember,eitheracademicorclinical,isneededtoguidestudentlearningtomeetintendedoutcomes.Itshouldbeconsideredthatexperiences“thatoccurwithouteitherinstructorguidanceoradequateacademicpreparationonthepartofthestudentmayyieldtolittleinsightintothegeneralprocessestakingplace.”(Bensonetal,2013).
o Thefacultymembermayormaynotbethedirectorofclinicaleducation,asitdependsontheorganizationalstructureandneedsoftheacademicprogram.
• Theonsitesupervisionofphysicaltherapiststudentsmaybeprovidedbyoneormoreofthefollowing:
o anacademicfacultymember;o anacademicfacultymemberplusacommunitybasedclinicianorotherrepresentative;oro acommunitybasedclinicianorotherhealthcareprofessional(Bensonetal,2013;Coker,2010;Doucet&Seale,2012;Goldbergetal,2006;Ingram&Hanks,2001;Jensenetal,2015;O’Neilletal,2007;Renekeretal,2016;Weddle&Sellheim,2011;Williams-Barnardetal,2004).
• Integratedfulltimeclinicaleducationexperiencesthatqualifyforaprogram’sminimumnumberofclinicaleducationweeksshallbesupervisedbyalicensedphysicaltherapist.
57
Page 59
16
• Preceptortostudentratioscanbeconfiguredbasedoncourseorprogramobjectiveswithconsiderationforstateandsupervisoryregulation(Wilson2006).
7. Theacademicprogram,incollaborationwithprogramfaculty,identifiesthemethodsofstudentandcourseassessmenttomeettheintendedcourseand/orprogramoutcomes.
Questionstoconsider:Howshouldstudentlearningbeassessed?Whatassessmentmethodswouldbebesttoevaluatetheknowledge,psychomotorskills,orbehaviorsofstudentprogress?Whatassessmentsmethodsshouldbeconsideredtoassesstheoveralldesignandtheshort/longtermprogrammaticoutcomesofintegratedclinicaleducationexperiences?
• Integratedclinicaleducationexperiencesshouldhavemethodsofassessmentforbothstudentachievementoflearningasitrelatestothedesiredcourseobjectives,aswellascourseand/orprogramassessmenttodetermineiftheintegratedclinicaleducationcomponentofthecurriculumhasachievedtheacademicprogram’sdesiredoutcomes.
• Studentlearningcanbeassessedatvariestimesthroughoutthestudent’sclinicaleducationexperiences:
o eitherduringorafteranexperienceembeddedwithinacourse,o duringorattheendofastand–alonecourse,oro attheendofablockofcourses(Jensenetal,2015).
• Avarietyofassessmentmethodscouldbeusedtomeettheintendedstudentlearningoutcome.Theseinclude:
o reflectivejournals,papers,orportfolios;o standardizedtests;o surveys;o debriefingsessions;discussionsessions;o check-offlists;o useofaclinicalperformancetool/formforclinicalskillacquisitionandgenericabilities.
• Reflectiononaction,inactionandforactionareessentialcomponentsoflearninginintegratedclinicaleducationexperiences(Schon,1983;Wainwrightetal,2010).
• Thestakeholdersshouldincludestudents,academicfaculty,clinicians,andthosereceivingphysicaltherapyserviceswhocanprovidefeedbackandreflectiontodetermineastudent’sachievementandsuccessduringtheintegratedclinicaleducationcomponentoftheacademiccurriculum(Hakimetal,2014;Maietal,2013;O’Neiletal,2007;Wilson,2006).
o Assessmentscanbecompletedbythestudent,peers,peermentors,clinicians/preceptors,andfaculty.Facultymembersareresponsibleforthefinaldeterminationofthestudent’slearning(Maietal,2013;Weddle&Sellheim,2011;Smithetal,2015;Stern&Rone-Adams,2006;Wilson,2006).
• Programmatic,longitudinaloutcomesofintegratedclinicaleducationexperiencesshouldbeassessedbystudentperformanceduringsubsequentaffiliationsorinternships,bysuccessfulcompletionoflicensing\examinations,employers,andbyfutureclinicalperformanceandattitudes(IngramandHanks,2001;Weddle&Sellheim,2009;Weddle&Sellheim,2011;Wilson,2006).
58
Page 60
17
8.Theacademicprogramidentifiesresourcesandlegal/regulatoryparametersthatimpactsdeliveryofintegratedclinicaleducationexperienceswithintheprogram.Questiontoconsider:Whatresourceareneededtoensuresuccessfuldesignandimplementationofintegratedclinicaleducationexperiences?Whatarethelegalorregulatoryparametersthatmustbeconsideredbeforeimplementationofintegratedclinicaleducationexperiences?
• Identificationofresourcesisacriticalrequirementinthedevelopment,deliveryandassessmentofintegratedclinicaleducation.Resourcesmustinclude,butarenotlimitedto:
o Dedicatedprogramleadershipwithadministrationsupport(Jensenetal,2015;Weddle&Sellheim,2009).
o Soundfiscalmanagement(Jensenetal,2015)withadequatefinancialresourcesavailableforfacultyworkload,whichincludescoreandadjunctclinicalfaculty(Weddle&Sellheim,2009).
o Personnelanddedicatedtimenecessarytodevelopandnurturerelationshipswithclinicians,andcommunityeducatorstoadministerandcoordinateallactivitiesinvolvedwithintegratedclinicaleducationexperiences;(Hakimetal,2014;Jensenetal,2016;Stern&Rone-Adams,2006)
o Spaceandequipment,eitheron-campusorwithlocalfacilities,needtobesecured.• Negotiatedaffiliation-typeagreementswithliabilityinsurancemayberequiredforproviding
integratedclinicaleducationexperiencesatsitesexternallocationswhichmaybeusedforeducationalpurposes.Theseagreementsofteninclude,butarenotlimitedto,requirementsofhealthclearancesandcriminalbackgroundchecks(Maietal,2013).
• Determinationofgeneralliabilityrequirementsshouldbereviewedbytheprogramdirectorandappropriateinstitutionaladministrativeofficials,fordeliveryofclinicaleducationservicesoncampus(Maietal,2013;Wilson,2006).
• Considerationforgovernmentandstateregulationsshouldbeinvestigatedbytheinstitutiontoensureregulatorystatutesarefollowed(Romigetal,2017).
• Reviewofaccreditationstandardsattheinstitutionalandprogramlevelshouldoccurtoensurecompliance.ProgramsareaffordedleewayindesigningintegratedclinicaleducationinwhichtheexperiencesshouldtakeplaceasoutlinedintheCommissiononAccreditationofPhysicalTherapyEducationevaluativecriteria,howeverknowledgeofstandardsareneeded(Wilson,2006).
9.Theacademicprogram,incollaborationwithprogramfaculty,selectsthetypeofclinicalorcommunitysitesrequiredforintegratedclinicaleducationexperiences.Questiontoconsider:Wherearethemostappropriatesettings/placesconsideringthepatientpopulationmostappropriateforstudentstoachievetheintendedcourseand/orprogrammaticobjectives?
• Clinicaleducationsitesthathavetheresourcesavailabletomatchtheacademicprogramsdesiredintegratedclinicaleducationcourseandprogramobjectivesoutcomesshouldbeselectedinanefforttoachievedesiredoutcomes.
o Afacultyclinicalpracticehastheadvantageofhavingthecorefacultyfunctionasinstructorsintheclassroomandmentorsintheon-campusclinic,withsomeprogramschoosingtoaugmenttheexperiencebyincludingphysicaltherapistsfromthelocal
59
Page 61
18
community.Anotherapproachistohavetheacademicclinicalfacultyserveasmentorsinavarietyofcommunityenvironments(Jensenetal,2015;Stern&Rone-Adams,2006;Wilson,2006).
o Anotherapproachistouseclinicalsiteswithmentorsexternaltotheuniversity(Hakimetal,2014;Jensenetal,2015).
• Thefollowingshouldbeconsideredwhenselectingclinicalandcommunitysitestoassureaseamlesscollaborationbetweentheacademicandintegratedclinicaleducationsetting:
o Apopulationofpatients/clientsappropriatefortheparticularintegratedclinicaleducation(musculoskeletal,neuromuscular,integumentary,othersystems.)(Hakimetal,2014;Weddle&Sellheim,2011;Wilson,2006)
o Proximitytothecampusorreasonablecommuteforthestudent(s)(Bensonetal,2013;Weddle&Sellheim,2011).
o Physicaltherapistsandotherprofessionals,asappropriate,withexperiencefortheparticularintegratedclinicaleducationexperience.Considerationcanbegivento:
• Yearsofexperience,boardcertificationsrequiredorrecommendedandmembershiptoprofessionalorganizations(Hakimetal,2014;Weddle&Sellheim,2011;Wilson,2006);
• Professionalswithmentorship/teachingabilities(CIcredentialingrequiredorrecommended)(Hakimetal,2014;Weddle&Sellheim,2011;Wilson,2006);
• Professionalswithvaluesthatarecongruentwithuniversitystandardsforbestpracticeandphilosophiesofservicedelivery(Hakimetal,2014;Jensenetal,2015;Weddle&Sellheim,2011).
o Facultyclinicalpractices,probonoclinics,servicelearningenvironments,healthandwellnessprograms,andnovelcommunitycentershavebeenusedsuccessfullyforintegratedclinicaleducationexperiences.
• Integratedfulltimeclinicaleducationexperiencesthatqualifyforaprogram’sminimumnumberoffulltimeclinicaleducationweeksshallbecompletedinaphysicaltherapyworkplaceenvironmentorpracticesetting.
10.Theacademicprogram,incollaborationwithprogramfaculty,acceptresponsibilityforthedevelopmentofrelationshipswithrepresentativesoftheclinicaleducationsite.
Questiontoconsider:Whataretherelationshipsrequiredtodevelopandsustainintegratedclinicaleducationexperienceswithinthecommunity?
• Academicprogramsthatwishtodevelopandimplementintegratedclinicaleducationexperiencesshouldfacilitateastructurethatsupportsacollaborativeworkingrelationshipbetweentheacademicenvironmentandtheclinicaleducationsite.(Hakimetal,2014;Jensenetal,2015)
• Ifclinicalsitesandinstructorsareexternaltotheacademicinstitution,abi-directionalpartnershipshouldbedevelopedtopromotetranslationofdidacticcontentintopracticeandtherebyinformcurricularstrengthsandweaknesses(Hakimetal,2014).
60
Page 62
19
RECOMMENDATION1:
Thattheproposeddefinitionofintegratedclinicaleducation(ICE)beadoptedasthedefinitionforusewithintheprofession.
SS:Consistentandproperuseoftheterm‘integratedclinicaleducation’isessentialtosuccessfulcommunicationwithintheacademicandclinicalenvironmentsofphysicaltherapisteducation.Thepanel,afterextensiveresearch,discussion,anddebatehasdevelopedadefinitionthatisclearandrepresentativeofthevarietyofsettingsandtypesofexperiencesthathavedevelopedwithinourprofession.ThedefinitionalsoincludesareferencetotheCAPTEcriteriaforfull-timeclinicaleducation,thusrecognizingthatICEcantakemanyforms,someofwhichmeetthecriteriasetforthinaccreditationstandards.
RECOMMENDATION2:
ThatthedefinitionofintegratedclinicaleducationbeaddedtotheglossarydevelopedbytheCommonTerminologypanel.
SS:TheworkoftheCommonTerminologyPanelandICEPanelwascoordinatedtoensureconsistencyofterms.BecausedevelopmentofadefinitionforICEwasacomponentofthispanel’scharge,thedefinitionisprovidedinthereportandproposedforadoption.Onceadopted,itshouldbeincludedintheglossaryofterms,ensuringconsistentdisseminationofthetermandacronym.
RECOMMENDATION3:
ThatthecurrentlypublisheddefinitionofintegratedclinicalexperienceintheACAPTpolicyentitledTerminologyforClinicalEducationExperiences(AC2-13)berescinded.
SS:AdefinitionforintegratedclinicalexperiencewasadoptedbyACAPTin2014.TheworkoftheICEpanelhasledtoarecommendationthattheappropriatetermisintegratedclinicaleducationandthattheexperiencesofICEarereferredtoasICEexperiences.Oncethisnewdefinitionforintegratedclinicaleducationisadopted,thetermanddefinitionfor‘integratedclinicalexperience’shouldberescindedtoensureconsistencyintheuseoftermsanddefinitions.
RECOMMENDATION4:
Thatthe8parametersaspresentedasbaselineexpectationsforintegratedclinicaleducationbeadoptedanddisseminatedforusebyphysicaltherapisteducationalprograms.
SS:ParticipantsintheSummitrecognizedboththevalueofICEandthevariabilityofICEexperienceswithintheeducationalprograms.Asaresult,theparticipantsagreedthattheprofessionisbestservedbyinclusionofICEthatisbuiltonagreeduponstandardsfordesignandimplementation.The8parametersdevelopedbytheICEpanelprovidesuchguidance.
61
Page 63
20
Theseparametersweredevelopedafterextensivereviewoftheliterature,engagementwithstakeholders,discussion,anddebate.AdoptionoftheseparametersbyACAPTmemberinstitutionswillensurethatICEaredevelopedusingastandardizedsetofexpectationsyetcontinuetoallowandencourageeducationalprogramstoinvolvetheirstudentsinawidevarietyofICEexperiencestomeetuniqueneedsortakeadvantageofuniquesituations.ThisguidanceforICEdevelopmentwillalsoassistfacultyinensuringthattheexperiencesprovidedtostudentsarebasedonsoundeducationalpractices.
RECOMMENDATION5:
Thatthe10guidelinesfordevelopmentofintegratedclinicaleducationexperiencesbedisseminatedtophysicaltherapisteducationalprograms.
SS:Distinctfromtheparametersdescribedabove,thepanelwasalsoaskedtoprovideguidancetoprogramsinterestedindevelopingICE.Thepaneldevelopedalistof10guidelinesthataddresstheintentionalstepsthatfacultyshoulduseandconsiderintheprocessofdevelopingICEexperiences.ThepanelbelievesthatthecombinationoftheparametersbeingusedasqualitystandardsalongwiththeguidelinestohelpguideICEdevelopmentwillensurethatphysicaltherapisteducationalprogramshavethetoolsnecessarytoprovidehighqualityandeffectiveICEtotheirphysicaltherapiststudents.
RECOMMENDATION6:
ThattheACAPTBoardofDirectorssharethisdocument,onceapproved,withthemembersoftheEducationalLeadershipPartnership(ELP)fordiscussiononhowtomoveforwardwithconsistentuseofthetermintegratedclinicaleducationwithinthephysicaltherapistclinicaleducationcommunity.
SS:Ifwearetoachieveconsistentuseofthetermintegratedclinicaleducation,thetermanditsdefinitionwillneedtobedisseminatedbroadly.ThistermrepresentsachangefromthetermpreviouslyadoptedbyACAPTinthepolicy‘TerminologyforClinicalEducationExperiences’(AC2-13)andthusthechangewillrequireacoordinatedefforttoeducateeducationalprogramsandclinicalfacultyonthepropertermandproperusage.ELPiswellpositionedtoassistinthisinitiative.
RECOMMENDATION7:
ThatACAPTsupporteducationalresearchfocusedonprogrammaticoutcomesofdifferentmodelsofintegratedclinicaleducationusingstandardizedoutcomemeasures.
SS:ThepanelwasaskedtodiscernanddescribemodelsofICEthatexistwithinphysicaltherapistcurricula.Thisportionofthechargewasaccomplishedbyathoroughreviewoftheliteratureandthemodelsweredescribedastheyrelatetothe8establishedparametersproposedbythepanel.
Throughthisprocessthepaneldiscoveredthatalthoughmodelsaredescribedintheliterature,thereislittletonoassessmentoftheoutcomesofthevariousmodelsdescribed.Inresponsetothisfinding,thepanelisrecommendingthatadditionalresearchbedevelopedandsupported.Findingsfromthis
62
Page 64
21
researchcanthenbeusedbythephysicaltherapyeducationalcommunitytodevelopthemosteffectiveandefficientmodelsofICE,thusenhancingtheeducationofthephysicaltherapiststudents.
MEETINGHISTORY
TheIntegratedClinicalEducation(ICE)WorkGroupmet14times,including11webconferencecallsand3onsitemeetings(CSM2016and2017andELC2016)fromFebruary2016-May2017.Manyadditionalsubgroupmeetingswereheldbetweenthemeetingsofthewhole.
63
Page 65
22
References
BensonJD,ProvidentI,SzucsKA.Anexperientiallearninglabembeddedinadidacticcourse:outcomesfromadidacticinterventioncourse.OTHC.2013;27(1):46-57.
BrusconiM,DamianR,SauriJG,et.al.TheConceptofExcellenceinHigherEducation.Brussels,Belguim.:EuropeanAssociationforQualityAssuranceinHigherEducation;2014.http://www.enqa.eu/indirme/papers-and-reports/occasional-papers/ENQA%20Excellence%20WG%20Report_The%20Concept%20of%20Excellence%20in%20Higher%20Education.pdf
CokerP.Effectsofanexperientiallearningprogramontheclinicalreasoningandcriticalthinkingskillsofoccupationaltherapystudents.JAlliedHealth.Winter2010;39(4):280-286.
DeweyJ.DemocracyandEducation.NewYork,NY:Simon&SchusterInc;1916,1944.
DoucetB,SealeJ.Thefreepost-strokeclinic:asuccessfulteachingandlearningmodel.JAlliedHealth.2012;41(4):162-169.
EngelhardC,McCallumCA.AdescriptionofcurrentcurriculardesignmodelsusedinphysicaltherapyclinicaleducationandtheirrelationshiptopassratesontheNationalPhysicalTherapyExamination.TheInternetJournalofAlliedHealthSciencesandPractice.Vol.13No.3ISSN1540-580X.October2015.
FaughtDD,Gray,DP,DiMeglioC,MeadowsS,MenziesV.Creatinganintegratedpsychiatric-mentalhealthnursingclinicalexperience.NurseEduc.May/June2013;38(3):122-125.
FisherD,FreyN,HiteSA.IntentionalandTargetedTeaching:AFrameworkforTeacherGrowthandLeadership.Alexandria,VA:AssociationforSupervisionandCurriculumDevelopment;2016.
FullanM.LeadershipandSustainability.SystemThinkersinAction.Ontario,Canada:CorwinPress;2005,57-58.
GoldbergLR,RichburgCM,WoodLA.Activelearningthroughservicelearning.CommunDisordQ.Spring2006;27(3):131-145.
HakimWE,MoffatM,BeckerEetal.Applicationofeducationaltheoryandevidenceinsupportofanintegratedmodelofclinicaleducation.JOPTE.2014;28(1):13-21.
IngramD,HanksJ.Acomparisonofclinicalperformanceoutcomesinshortintegratedversussinglelong-termclinicalexperiencesofphysicaltherapiststudents.JOPTE.2001;15(1):32-35.
JensenG,MostromE,GwyerJ,HackL,NordstromT.Learningforpractice:Early,integratedworkplaceexperiencesmatter.AERAOnlinePaperRepository.2015.Availableat:http://www.aera.net/repository
64
Page 66
23
JensenGM,NordstromT,SegalRL,McCallumC,GrahamC,GreenfieldB.EducationResearchinPhysicalTherapy:VisionsofthePossible.PhysTher.2016;96(12):1874-1884.AccessedJanuary16,2016.
Knetch-SabresLJ.Theuseofexperientiallearninginanoccupationaltherapyprogram.Canitfosterskillsforclinicalpractice?OccupationalTherapyinHealthCare.2010;24:320-334.InBensonJD,ProvidentI,SzucsKA.Anexperientiallearninglabembeddedinadidacticcourse:outcomesfromadidacticinterventioncourse.OTHC.2013;27(1):46-57.
MahendraN,FremontK,DionneE.Teachingfutureprovidersaboutdementia:Theimpactofservicelearning.SeminSpeechandLang.2013;34(1):5-17.
MaiJ,ThieleA,O'DellB,KruseB,VaassenM,PriestA.Utilizationofanintegratedclinicalexperienceinaphysicaltherapisteducationprogram.JOPTE.2013;27(2):25-32.
MaiJ,SternD,HollmanJ,MelzerB,ThieleA,RosenthalR.Examiningtheimpactofanintegratedclinicalexperience(ICE)oninterpersonalskillspriortothefirst,full-timeclinicalinternship:coolasICE.JPhysTherEduc.2014;28(2):81-97.
O'NeilM,RubertoneP,VillaneuvaA.CommunityexperientiallearningopportunitiesintheDrexelUniversityprofessionalDoctorofPhysicalTherapyProgram.JOPTE.2007;21(2):66-72.
RenekerJ,WeemsK,ScaiaV.Effectsofanintegratedgeriatricgroupbalanceclasswithinanentry-levelDoctorateofPhysicalTherapyprogramonstudents'perceptionsofgeriatricsandgeriatriceducationintheUnitedStates.JEducEvalHealthProf.2016;13(35).doi:10.3352/jeehp.2016.13.35
RomigBD,HewittAM,MailletJO.Thefutureofclinicaleducation:opportunitiesandchallengesfromalliedhealthdeans’perspective.JAlliedHealth.2017;46(1):43-55.
SackettDL,StraussS,RichardsonS,RosenbergW,HaynesRB.Evidence-BasedMedicine:HowtoPracticeandTeachEBM.Edinburgh,Scotland.ChurchillLivingstone;2000.
Scho¨nD.TheReflectivePractitioner:HowProfessionalsThinkinAction.SanFrancisco,CA:Jossey-BassIncPublishers;1983.
ShulmanLS.TeachingasCommunityProperty:EssaysonHigherEducation.SanFrancisco,CA:Jossey-Bass;2004.
SmithKM,LutenbacherM,McClureN.Leveragingresourcestoimproveclinicaloutcomesandteachtransitionalcarethroughdevelopmentofacademic-clinicalpartnerships.NurseEduc.2015;40(6):303-307.
SternD,Rone-AdamsS.Analternativemodelforfirstlevelclinicaleducationexperiencesinphysicaltherapy.IJAHSP.2006;4(3).Availableat:http://ijahsp.nova.edu.AccessedJune23,2016.
StuhlmillerCMandTolchardB.Developingastudent-ledhealthandwellbeingclinicinanunderservedcommunity:collaborativelearning,healthoutcomesandcostsavings.BMCNurs.2015;14(32).
65
Page 67
24
SzucsKA.Anexperientiallearninglabembeddedinadidacticcourse:outcomesfromadidacticinterventioncourse.OTHC.2013;27(1):46-57.
WainwrightSF,ShepartKF,HarmanLB,StephensJ.Noviceandexperiencedphysicaltherapistclinicians:Acomparisonofhowreflectionisusedtoinformtheclinicaldecision-makingprocess.PTJ.2010;90(1):75-88.
WeddleM.SellheimD.Anintegrativecurriculummodelpreparingphysicaltherapistsforvision2020practice.JOPTE.2009;23(1):12-21.
WeddleM.SellheimD.Linkingtheclassroomandtheclinic:amodelofintegratedclinicaleducationforfirst-yearphysicaltherapiststudents.JOPTE.2011;25(3):68-79.
Williams-BarnardCL,SweattAH,HarknessGA,DiNapoliP.Theclinicalhomecommunity:amodelforcommunity-basededucation.IntNursRev.2004;51:104-112.
WilsonA.Integratedclinicalexperiencesinacampusonsiteclinic:aself-containedmodelofphysicaltherapyeducation.IJAHSP.2014;12(3):1-17.Availableat:http://ijahsp.nova.edu
WilsonJ,CollinsJ.Physicaltherapiststudentlearningthroughauthenticexperiencesinmanagement:oneprogram’sinterpretationofservicelearning.JOPTE.2006;20(3):25-32.
Wolfe,D.E.,&Byrne,E.T.Researchonexperientiallearning:Enhancingtheprocess.ScandinavianJournalofOccupationalTherapy,1975.8,163–173.InBensonJD,ProvidentI,SzucsKA.Anexperientiallearninglabembeddedinadidacticcourse:outcomesfromadidacticinterventioncourse.OTHC.2013;27(1):46-57.
YardleyS,BrosnanC,RichardsonJ,HaysR.Authenticearlyexperienceinmedicaleducation:asocio-culturalanalysisidentifyingimportantvariablesinlearninginteractionswithinworkplaces.AdvHealthSciEduc.2013;18:873-891.
66
Page 68
Table1:ModeldescriptionsofIntegratedClinicalEducationthatcurrentlyexistintheliterature:Organizedbythe8parametersAuthor(s)YearDiscipline
Placement Course/ProgramObjectives
Frequency Typeofcourse
Occurrencew/incourse
Locality AssessmentandOutcomes
CoordinationSupervision
Benson,Provident&Szucs2013OccupationalTherapy
4interventioncourses,experientiallabinall,ICEinfirstNeurologicalcourse
Courselabobjectives:1)selecting,administeringandinterpretingresultsofassessmentinstrumentsandtechniques,forusewithclientswithperformance,deficitsrelatedtoneurological,sensory,motor,cognitiveandperceptualdysfunction;2)designingandimplementinginterventionplanstoremediateand/orrehabilitateoccupationalperformancedeficitsinthebirthtoadolescentpopulation;3)evaluatingandutilizingcurrentresearchinthedesignandimplementationofintervention;and4)producingappropriatedocumentationsupportingevaluationfindingsanddelineatinginterventionactivitiesandplansandprogressnotes
Notclearlypresented,first4weeksinclassroom-thenincommunity
Experientiallearninglabwithinacoursewithpediatriccontent
Firstexperientiallaboccurredafterweek4ofthecourse
Communitysite-Privateschooldeliveringservicestochildrenandadolescents;neededservicesnotavailableinpublicschoolsystem
Observationofstudentperformance,writtenandoralfeedbackofperformance,review/assessmentof/feedbackaboutinterventionplans,studentchoiceofevidenceandabilitytoapplytointerventionplan,andpatientevaluationreport;finalcourseassessment-masterytestingofclinicalskillstoensurereadinessforfieldwork
Courseinstructor;partneredwith5OTsfromschoolInstructorofcourseand/orcommunityclinician
67
Page 69
Coker2010OccupationalTherapy
Afterfirstyearinprogram-partof2yearprogram
Course/programobjectivesnotdiscussed
1week(5days,6hoursday)
Stand-alonecourse
Afterfirstyearintheprogram
1weekday-campforchildrenwithCP
UsestudentfeedbackandstandardizedassessmentusingSelf-AssessmentofClinicalReflectionandReasoning(SACRR)andCaliforniaCriticalThinkingSkillsTest(CCTST)todetermineiftheirdesignedexperienceisthebestapproachtoaccomplishthislearning
OTfacultymember;OTclinicianatcampLicensedOTincludingthefacultywhocoordinatedtheexperience
Doucet&Seale2012PhysicalTherapyandOccupationalTherapy
SecondorthirdyearofPT/OTprograms
Course/programobjectivesnotdiscussed
1weekinlengthforclinic
Stand-alonecourse
Embeddedineducationalcourse
Oncampusclinic Writtenquestionnaireconsistingofmultiplequestionswithresponsesbasedona5-pointLikertscale;Patientsratedtheirperceptionofthestudentintern(s)assigned,thetreatmentgiven,andtheorganizationoftheclinic.Studentsratedtheirperceptionoftheclinicexperience,whetherclinicpreparedthemforfieldwork/clinicalrotations,connectiontodidacticknowledge,andoverallbenefit.Supervisorsratedstudentinternsontheirabilitytointeractwithpatients,
2facultymembers(oneOT,onePT)Facultyandcommunityclinicians(clinicalinstructors)
68
Page 70
demonstrationofknowledge,andapplicationofappropriateinterventions,alongwiththeiroverallperceptionoftheeffectivenessandorganizationoftheclinic
Faught,Gray,DiMeglio,Meadows&Menzies2013RN
Unsure Goalthatstudentscould(1)gainskillinprovidingintegratedphysicalandmentalhealthcaretotheirpatients,(2)becomeawareofandpossiblyimproveperceptionsregardingmentalhealth/mentalillness,and(3)expandtheirunderstandingofthecriticalimportanceofthetherapeuticnurse-patientrelationshipincaringforallpatients
24hours Partofmentalhealthcourse
Unsure Inpatienthealthcareunit
Quantitativeend-of-semesterevaluationsoftheclinicalrotations,qualitativeevaluationsofthemodifiedclinicalexperience(nothingspecificidentified)
Facultymembers2clinicianswitheducatorexperiencewhowereemployedoninpatientmedicalunits,hadpsychiatricnursingclinicalexpertise
69
Page 71
Goldberg,Richburg&Wood2006SLP
Secondyearcourse
Tofacilitatereflectiveproblem-basedlearninganddecision-making,integrationoftheoreticalandclinicalknowledge,andstudentawarenessoftheimportanceofevidence-basedpracticeintheareaofdysphagia.
15hours Partofadysphagiacourse
Secondyearcourseinspringsemester(15hours)
Communitypartnerswithdysphasiamanagementprogram
Competenciesonthestudents’analysis,synthesis,andevaluationofthefollowing:ethicalbehavior;ASHApoliciesandguidelinesandlocal,state,andnationallegislation;normalanddisorderedswallowing;effectivepreventionandassessment;researchprinciplesandevidence-basedtreatment;effectivespeakingandlistening;andwrittenreports,treatmentplans,andprofessionalcorrespondence,reflectivejournals
Facultymemberplacesstudentwithcommunitysupervisor(goaltobeplacedwithexternshippartner)Communitysupervisor
Hakim,Moffat,Beckeretal2014PhysicalTherapy
Earlyincurriculum(authenticearlyexperiences)-year1
Course/programobjectivesnotdiscussed
Variety Variety Variety Academic-communitypartnerships
Notdescribed Facultyled-placementproviders(DCE)Clinicalfaculty;masterclinicians
Ingram&Hanks2001PhysicalTherapy
Firstyearoftheprogram
Course/programobjectivesnotdiscussed
Fulltimeweeks;varyingpointsintimeduringthefirstyear
MPTstudents-stand-alonecourse;BSstudents-partofcourse
MPTstudents-7weekcourseendoffirstyear;BSstudents-integrated7weeks(1weekendoffallsemester,2weeksendofspringsemester,and4weeks
VarietyoftraditionalPTclinics
ClinicalPerformanceInstrument
FacultycoordinatedClinicalfaculty
70
Page 72
endofsummersemester)
Jensen,Mostrom,Gwyer,Hack&Nordstrom2015PhysicalTherapy
Variety-highlightsearlyintegrated
Course/programobjectivesnotdiscussed
Variety Variety(bothstandaloneandpartsofcourses)
Variety Academic-communitypartners(facultypractice)
Variety-writtenpre-work,postdebriefing
FacultycoordinatedandsupervisedVariety(clinicalfacultyandacademicfaculty)
Mahendra,Fremont&Dionne2013SLP
Electivecourseover2years(SLP)
Learningoutcomesforthecoursewerederivedfromstudentself-reflectionsbuttheactualobjectiveswerenotdescribed
Last4weeksofcourse
Partofacourse
Last4weeksofcourse
Localdementiaunit
Quizondementia,personalreflectionpriortoandaftertheservicelearning(SL),ethnographicinterview,screeningofindividuals(forcognition,affect,hearingandvision),collaborativeinterpretationofresults,researchanddevelopmentofadiagnosisplan,andactualparticipationinSL
Notexplicitlystated--facultyandsitepersonnelNotspecified
Maietal2013PhysicalTherapy
3courses-successivesemesters,startsfirstyear
Specificcourse/programobjectivesnotmentioned
Semester-longcourses
Stand-alonecourses
BegininfirstyearofDPTprogram-2hourstwiceweekly(ClarkeUniversity);wintersemesterofyear1(NovaSoutheasternU)
Oncampuswellnessclinic:patientsreferredfromcommunityhealthclinicsandlocaldialysiscenter;andseniorlivingcenters,communitywellnesscentersorlongtermcarecenters
GenericabilitiesandCPI;groupdebriefings,servicelearningpapers
FacultycoordinatedandsupervisedLicensedPTfaculty
71
Page 73
Maietal2014PhysicalTherapy
Firstyearofprogram
Course/programobjectivesnotdiscussed
Variety--2hourstwotimesperweekand40hours/week
Stand-alonecoursesandintegrated
Firstyear Communityclinics,wellnessactivities
InterpersonalCommunicationQuestionnaire(ICQ)andMedicalCommunicationBehaviorScale(MCBS);standardizedoutcometoolforassessment
Coursecoordinator;otherfacultyasassigned,includingDCECommunityclinicalsupervisors
O'Neil,Rubertone&Villanueva2007PhysicalTherapy
Early,presentat3differentpointsthroughoutcurriculum
Courseobjectivesthatcreateservicelearningexperiencesincludeengagement(aservicecomponentmeetingcommunityneeds),reflection(amechanismforstudentstolinkserviceexperiencestocoursecontent),reciprocity(teacherandlearnerrolesforallparticipantsintheexperience),andpublicdissemination(sharingoutcomesamongparticipants)
3phases Partofcourses
Seetable3ofarticle-varietyoftimesdependentuponspecificSLactivity
Communityworkplaces
Outcomesarereportedthroughclassdiscussion,reflectionexercises,andcourseevaluations
FacultycoordinatedwithcommunitypartnersFacultymembers,labinstructors,nursingassistant
Reneker,Weems&Scaia2016PhysicalTherapy
Secondyearofcurriculum
Course/programobjectivesnotdiscussed
8weeks,onetimeperweek
Partofaneurocourse
Notspecified-onlythatoccurrencewasfor8weeks
VeteransAffairsoutpatientclinic
Pre-andpost-ICEstudentperceptionsaboutthegeriatricpopulation
Facultycoordinated-PTsupervised2licensedPTs
Smith,Lutenbacher&McClure2015RN
Unsure UsingguidelinesfromtheAmericanAssociationofCollegesofNursingPublicHealthRecommendedBaccalaureateCompetenciesandCurricularGuidelinesforPublicHealthNursing,thefollowingobjectivesweredetermined:studentswererequiredtodevelop,implement,
3semesters Partofclinicalcommunityhealthcourse
Unsure Transitionalcareenvironment
Peerevaluationtool,clinicalperformanceevaluationtoolwasusedtoassessclinicalcompetenciesandinterprofessionalcollaboration;studentsalsowroteaweeklyjournalreflectionabouttheirexperiences
ACP-academic-clinicalpartnershipsdevelopedbefore,duringaftercoursesNursingfaculty
72
Page 74
andevaluateanindividualizedplanbasedontheirassessmentofthepatientandtheircommunity
Stern&Rone-Adams2006PhysicalTherapy
Firstandsecondyearoftheprogram
Primarylearningobjectivesforthefirstyearstudentsincludedevaluation,examination,assessmentskills,anddevelopmentofprofessionalbehaviorsasdefinedbytheGenericAbilitiesbehaviors;learningobjectivesforsecondyearstudentsincludedcognitive,psychomotor,andaffectiveskillspracticedthefirstyearoftheprogram
Onedayperweekeveryotherweek
Stand-alonecourse
Notspecified-didbeginduringthesecondmonthofthecurriculumandcontinuedfor3consecutivesemesters
Clinicalpractices(SNF,Adultdaycare,homelessshelter,outpatientclinics)
GenericAbilitiesself-assessment,student-facultyclinicalinstructorself-assessmentdiscussionwithfeedback,studentreflectivejournalthatwasdiscussedattheendofeachrotation
Clinicaleducationteamcoordinated;facultyoversightinareaswithpriorexperienceFacultyclinicalinstructors
Stuhlmiller&Tolchard2015RN
Unsure Courseobjective:effectivelyengagewiththecommunity,itsleadersandotherstakeholdersinassessingandrespondingtohealthandsocialwell-beingneeds,2.increaseprovisionofevidence-basedintegratedhealthhelpthatpromotescollaborativelearning,self-determinationandresponsibility,and3.demonstratepositivehealthoutcomesasdeterminedbystandardizedmeasures
Ongoingclinic-rangeof80-120hoursattachedtoaunitofstudy
Notexplicitlystated
Unsure Student-ledclinic(Australia)-partneredwithanexistingcommunityclinic
Nonereported Principalinvestigatorfromacademicsidepartneredwithcommunitysupervisors;supervisorsonsiteprovideddaytodaysupervisionNoreferencetowhoprovidedspecificsupervision
73
Page 75
Weddle&Sellheim2009PhysicalTherapy
Beginsfirstsemester,extendsintothesecondsemesterofsecondyear
Course/programobjectivesnotdiscussed
1/2day Partofcourses
Notspecific,butsecondweekofthecurriculumuntilthesecondsemesterofyear2
PhysicalTherapistpracticesettings
DirectoutcomesandmeasuresrelatedtoICEnotreported,NPTEpassratesofstudentswhoparticipatedinthenewmodelwere94%and100%overthetwoyearsdiscussed,oneyeargraduatesurveyandalumnisurveybothindicatedstudentsandemployersfeltthenewgradwaswell-preparedforpractice
FacultyandclinicalfacultycoordinatedClinicalfaculty
Weddle&Sellheim2011PhysicalTherapy
Firstsemester ObjectivesofICEaretohavestudentspracticecomponentsofpatient/clientmanagement;begintoapplybasic,medical,andbehavioralsciencestoclinicalscience;andtodeepentheirunderstandingofthebreadthandcomplexitiesofphysicaltherapistpractice
75hourspriortofirstFTexperience
Partofcourses
Notspecific,but2experiencesoccurduringfirstsemesteryearone,and6experiencesoccursecondsemesteryearone
PhysicalTherapistpracticesettings
Learningactivitycheckoffform,skillscompetency-patientmanagement-anddocumentationchecksthroughoutmodellearningunits,onlinereportingforms,onceasemesterprofessionalbehaviorsmeetingbetweenstudentandfacultyadvisortogooverstudentself-assessmentandperformance,10itemprofessionalbehaviorsassessmentofstudentbytheclinicalfaculty
Facultycoordinated-clinicalfacultysupervisedClinicalfaculty
74
Page 76
Williams-Barnard,Sweatt,Harkness&DiNapoli2004RN
Unsure Vagueobjective:engageinhealthpromotionanddiseasepreventionstrategies;2providenewavenuesforsecondaryandtertiarycare;and3offerinnovativetreatmentapproachesinthecommunitysettingtocareforpeoplethroughouttheirlives
Partofacourse
Partofparentchildhealthandmentalhealthcourse
Unsure Community-basedpartners
Unsure,possiblyfocusgroupstoassessstudentperceptionoftheexperience
Facultyled-communitysupervisorsFacultyandcommunitysupervisors
Wilson2006PhysicalTherapy
3consecutivesemestersinsecond/thirdyearofcurriculum
ICEI:Becomefamiliarwithclinicenvironment,Observeandassistwithpatientcare,Practicedocumentationandinterviewingskills,Prescribeexerciseforahealthypopulation;ICEII:Developpatient-professionalinteractionskills,Developdocumentationskills,Developskillinpatienthandlingandtreatmentinterventions,Developcriticalclinicalreasoningandclinicaldecision-makingskills;ICEIII:Refinepatient-professionalinteractionskills,Assumeresponsibilityforallaspectsofpatient,management,Refinedocumentationskills,Refineclinicalreasoningandclinicaldecision-makingskills,Begintodeveloppeermentoringandsupervisoryskills
Onedayperweek
Stand-alonecourse
N/Aasitisastand-alonecourse;beginsinthefallsemesterofyeartwofor3consecutivesemesters
Campusonsiteclinic
ICEI:writtenevaluationsofstudentperformancefrombothpeermentorsintheonsiteclinicandfromCIsintheexercise/wellnessgroup;ICEII:writtenmidtermandevaluationsoftheCI’sassessmentofthestudent’sperformanceintheareasofsafety,professionalbehavior,communication,examinationandinterventionskills,andclinicalreasoning;ICEIII:writtenmidtermandfinalevaluationsoftheCIsassessmentofthestudent’sperformanceintheareasofsafety,professionalbehavior,communication,
FacultycoordinatedandsupervisedCorefacultyandPTcliniciansfromthelocalcommunity
75
Page 77
examinationandinterventionskills,andclinicalreasoning
Yardley,Brosnan,Richardson&Hays2014Medicine
Earlyincurriculum(authenticearlyexperiences)-year1
Learningoutcomesforindividualepisodesweregenericratherthancontextspecificandrelatedtothetitleofeachexperience
Partofacourse
Incorporatedintomedicalschoolactivities
Incorporatedintomedicalschoolactivities
Workplaces(health,social,voluntarycommunityservices)
Reflectivesummarieswithinaportfoliowhichwasgradedforpresentationofwork,depthofreflectionandself-awareness
Facultyled-placementprovidersObservationalexperienceswith"somesupervision"
Wilson&Collins2011PhysicalTherapy
Firstyearofprogram
Leadershipandmanagementprincipleswereprimaryfocus
Partofacourse-4to8hours/week)
Clinicalcoursecoordinatedwithmanagementcourse
Clinicalcoursecoordinatedwithmanagementcourse
Oncampusandoffcampus
Studentsatisfaction,surveys,courseevaluations,reflectiondiscussions,graduatesurveys1yearpost-graduation;Keythemes:delegation,communication,givingandreceivingfeedback;roleasmanager;developmentoffundamentalbusinessskills
Coursecoordinator;otherfacultyasassigned,includingDCECoursecoordinator
76
Page 78
Table2:SelectOutcomeMeasuresandDataCollectedinIntegratedClinicalEducationModels
Author(s) Year Discipline
OutcomeMeasure/AssessmentofStudentLearning
OutcomesofStudentLearning
OutcomeMeasure/AssessmentofICEModel OutcomesofICEModel
Benson,Provident&Szucs
2013 OccupationalTherapy
StudentSurveys Studentsvaluedtheopportunityforexperientiallearning
StudentSurveys Instructorfeedbackanddesignofexperienceallabovea9on10pointscale
Coker 2010 OccupationalTherapy
Self-AssessmentofClinicalReflectionandReasoning(SACRR)andCaliforniaCriticalThinkingSkillsTest(CCTST)
Improvementsinclinicalprotocols,clinicalhypothesis,interventionstrategies,decisionmaking,judgement;criticalthinkingskills
None n/a
Doucet&Seale
2012 PhysicalTherapyandOccupationalTherapy
Self-developedquestionnairewithitemstoassessstudentperformanceduringclinic(un-validated):professionalbehaviors:multifactorial(patientevaluationofstudent)Facultyevaluationonstudentabilitytointeractwithpatients,knowledgeandapplicationofinterventions
Studentandclientresponseswereallpositiveatthestronglyagreedoragreelevel;instructorratingsofstudentperformancewerelowerthanofstudentassessment
Self-developedquestionnairewithitemstoassessstudentandclientperceptionsofclinicexperience;
Positiveresponsestowardsbenefitofclinicfrompatientperspective-100%stronglyagreedoragreedtorecommendorparticipateinclinicagain;studentsassessedclinicasavaluableadditiontocurricula.
Faught,Gray,DiMeglio,Meadows&Menzies
2013 RegisteredNurse
Pre-posttestscoresofLikertscalesurveybasedonobservationalcompetenciesMeanperformanceon10quizzeswithopenendedquestionsReflectiveJournals
Significantdifferenceinall7competenciesQuizscoresvariedImprovementindescriptionsinjournalentriesnotedfrombeginningtoend
Courseevaluations Studentsatisfactionwithcourseimprovedover3-yeartimeframeServicelearning(SL)inclusionimprovedstudentpreparationforexternships
Ingram&Hanks
2001 PhysicalTherapy
ClinicalPerformanceInstrument(CPI)Multipleshorttermvslongtermfull
NosignificantdifferencesinICEcurricularmodelinoneprogram
None n/a
77
Page 79
timeIntegratedClinicalEducation(ICE)
Jensen,Mostrom,Gwyer,Hack&Nordstrom
2015 PhysicalTherapy
Qualitativedata Threecorethemes:1)organizationalcontext,2)people/expectationsand3)enactedcurriculum
Qualitativedata Early,integratedclinicaleducationexperiencesareakeycomponentandanessentialcomponentforclinicalauthenticityofthecurriculum
Mahedra,Fremont&Dionne
2013 SpeechLanguagePathology
Learningoutcomes:informalcourseevaluations;studentreflectionpapers
StudentsatisfactionwaspositiveNegativecommentsreflectedstudentanxietyanddiscomfortwiththepopulation
Formaluniversityadministrationcourseevaluations
Negativecommentsaboutlogisticsofoffcampusexperiencesbutrectifiedduringcourse;overallcourseratinga1.1(highlysatisfied);studentsappreciatedthehandsonlearningcomponent
Maietel 2013 PhysicalTherapy
ClinicalPerformanceInstrument(CPI)(usedinIntegratedClinicalEducation(ICE)1and2);progressinprofessionalbehaviors
Nomeasurableoutcomesreportedonstudentprogress
GroupdiscussionsabouttheICEexperiences;self-designedsurveyaboutICEexperiences
OutcomesofstudentperceptionsaboutICEexperiences
Maietel 2014 PhysicalTherapy
InterpersonalCommunicationQuestionnaire(ICQ)andMedicalCommunicationBehaviorSystem(MCBS)MCBSisanobservationalassessmentofperformanceobserved.
NosignificantdifferencewithICQbetweengroupsexceptforthosewithpriorworkexperienceinPTfieldasaideortechnician;studentswithICEpriortofirstfulltimeCEperformedbetterinsomecontentandaffectivecategories(studentbased)onMCBS-butstatisticalscoresnotreportedintable(only%
None Limitationwasvariationin4programcurriculardesign-where4ClinicalEducation(CE)rotationswereplaced
78
Page 80
observed);othercategoriesnotsignificantOverallassessment:ICEpreparedstudentsself-perceivedreadinessincommunicationrealmwashigherthannon-ICEtrainedgroup
O'Neil,Rubertone&Villanueva
2007 PhysicalTherapy
Classdiscussions;reflectionexercises
Themes:newlevelofknowledgeandempathywhenworkingwithunderservedpopulations;betterunderstandingofphysicalandsocialenvironmentalfactorsthatarefacilitatorsorbarrierstoadoptinghealthylifestyles
CourseevaluationsParticipantandcommunityagencyoutcomesviaself-designedquestionnaires
Positiveresponses
Reneker,Weems&Scaia
2016 PhysicalTherapy
Surveyinstrumentmeasuringstudentperceptionofgeriatricphysicaltherapy(adaptedfrommedicine)
Studentsmorelikelytoseekoutemploymentwithgeriatricpopulationasaresultoftheexperience
Perceptionsofgeriatriceducationincourse-baseduponenjoyment
Studentsindicatemoregeriatriccontentneeded
Smith,Lutenbacher&McClure
2015 RegisteredNurse
Peerevaluationtool,ClinicalPerformanceEvaluationtool,Weeklyreflectionjournals
Positivefeedbackabouttheexperience;Studentprojectscompletedreported
Lessonslearned Studentparticipationvoluntarybecauseoftimecommitmentexceededcourserequirements;Studenttoolkitvaluableadditiontostructureofexperience
SternandRone-Adams
2006 PhysicalTherapy
None n/a Programoutcomespresented
Curriculardesign;Benefitsandchallenges
Stuhlmiller&Tolchard
2015 Unsure None n/a Programoutcomesreported
Numberofpatientsserved,servicesprovided;Inter-professionalClinicalEducation(IPE)exposure;costsavingstocommunity
79
Page 81
WeddleandSelheim
2009 PhysicalTherapy
None n/a Programoutcomes CurriculumdesignDescriptionofclinicalpartnershipsandclinicalfacultyresponsibilities
WeddleandSelheim
2011 PhysicalTherapy
None n/a Programevaluationplan Descriptivestats7cohortsofstudentsinstudyoutcomesQualitativedataandsurveyresponsesStudentdata:benefitsofworkingwithpatientsratherthanwithclassmatesGraduatedata(priortograduation)Clinicalfacultydata(positiveandnegative)Corefacultydata
Williams-Barnard,Sweatt,Harkness&DiNapoli
2004 RegisteredNurse
CaliforniaCriticalThinkingSkillsTest(CCTST)
LooselypresenteddataPostscoreshavebeenabovestandardizedmeanwithwiderrangeofscoresbetweenpreandposttestsPostscoreshavebeenabovestandardizedmeanwithwiderrangeofscoresbetweenpreandposttests
IntegratedClinicalEducation(ICE)programassessment
ArnettStimulationTest(AST)andNationalLeagueforNursing(NLN)BaccalaureateAchievementTest(CNAT):variableresultsNationalCouncilLicensureExamination-RegisteredNurse(NCLEX-RN)outcomesrelatedtoclinicalcare:upwardtrendduringpilotwithICE
80
Page 82
Wilson 2006 PhysicalTherapy
StudentandClinicalInstructor(CI)(oral)debriefingandquestionnaires
Positivefeedbackandenhancedstudentprofessionalandclinicaldevelopment
StudentandCI(oral)debriefingCIadvisorypanel
FeedbackresultsinchangestoIntegratedClinicalEducation(ICE)experiencesFeedbackduringfulltimeClinicalEducation(CE)(afterICE)-anecdotalevidenceGraduatesurveys=openendedqualitativedata-providesasolidfoundationtobuildconfidenceandprofessionaldevelopmentNumberofpatientvisits
Wilson&Collins
2011 PhysicalTherapy
Studentsatisfactionsurveys,reflectivejournaling,graduatesurveys1yearpostgraduation
StudentlearningobjectivesweremetandoftenexceededStudentsidentifiedandmanagedchallengesDevelopmentofsuccessandprofessionalism
CourseevaluationsRoleofPhysicalTherapistsasmanagerEndofsemesterfeedbacksessionsGraduatesurveys1yearpost
Programevaluationdatapresented:descriptivebothquantitativeandqualitative
Yardley,Bronan,Richardson&Hays
2014 Medicine LearningoutcomesforindividualepisodesofAuthenticEarlyExperience(AEE)
UnlessAEEisappropriatelyplacedoneachoftheworkplacespectra,thensocio-culturaltheoriessuggestthatstudentswillnotbeabletoadequatelyengageintheprocessesoftheeducationalspectra
Programevaluation Qualitativedataonexpectations,processesandconsequencesofAEE
81
Page 83
ICEAppendixA
INTEGRATEDCLINICALEDUCATIONFORPHYSICALTHERAPISTSTUDENTSDefinition,Parameters,andGuidelines
Educationalliteraturesuggeststhatintegratedclinicaleducationexperiences,aformofexperientiallearning,canexposestudentstoaspectsofpatientcenteredcareduringflexibleclinicaltrainingperiodsthroughoutthecurriculum.Theseexperiencesaffordstudentsanopportunitytofacilitatedevelopmentoftheircognitive,affective,andpsychomotorskillswhileconcurrentlyallowingacademicand/orclinicalfacultytofacilitatestudentdevelopmentwithrespecttothetransferofdidacticknowledgeintoclinicalapplication.(Hakimetal,2014)Thedefinition,parameters,andguidingprinciplespresentedinthisdocumentareprovidedtoassistprogramsinthedevelopmentofintegratedclinicaleducationexperiences.
DefinitionThefollowingisthedefinitionofIntegratedClinicalEducation(ICE).Integratedclinicaleducationisacurriculumdesignmodelwherebyclinicaleducationexperiencesarepurposivelyorganizedwithinacurriculum.Inphysicaltherapisteducation,theseexperiencesareobtainedthroughtheexplorationofauthenticphysicaltherapistroles,responsibilitiesandvaluesthatoccurpriortotheterminalfulltimeclinicaleducationexperience.
Integratedexperiencesarecoordinatedbytheacademicprogramandaredrivenbylearningobjectivesthataresynchronouswithdidacticcontentdeliveryacrossthecurricularcontinuum.Theseexperiencesallowstudentstoattainprofessionalbehaviors,knowledgeand/orskillswithinavarietyofenvironments.Thesupervisedexperiencesalsoallowforexposureandacquisitionacrossalldomainsoflearningandincludestudentperformanceassessment.
Forintegratedclinicaleducationexperiencestoqualifytowardstheminimumnumberoffull-timeclinicaleducationweeksrequiredbyaccreditation(CAPTE)standards,itmustbefulltimeandsupervisedbyaphysicaltherapistwithinaphysicaltherapyworkplaceenvironmentorpracticesetting.
ICE=IntegratedClinicalEducation
ParametersforIntegratedClinicalEducationThefollowingaretheparametersandbaselineexpectationsforICEinphysicaltherapisteducation.Pleaseseethefullreportfortheevidencesupportingtheseparameters.
1.Integratedclinicaleducationmayoccurinanyacademictermpriortothecompletionofthedidacticcourseworkleadingtothecompletionofaterminalfulltimeclinicaleducationexperience.
2.Integratedclinicaleducationexperienceswillhavespecificdesiredoutcomesthatcorrespondtocourseand/orprogrammaticobjectives.
3.Integratedclinicaleducationexperiencesmayberepresentedasacomponentofadidacticcourseorastandalonecoursethatoccursinasynchronousfashionwithotherdidacticcoursework.
4.Integratedclinicaleducationexperiencetimeframesaredevelopedbytheacademicprogrambaseduponthecourseand/orprogrammaticobjectives.Integratedclinicaleducationmayincludefulltimeand/orparttimeexperiences.
82
Page 84
ICEAppendixA
5.Integratedclinicaleducationexperiencesmayoccurinavarietyoflearningenvironmentsincludingcampusorcommunitybasedclinicalornon-clinicalsettings,baseduponthecourseand/orprogrammaticobjectives.Integratedfulltimeclinicaleducationexperiencesthatqualifyforaprogram’sminimumnumberofclinicaleducationweeksshallbecompletedinaphysicaltherapyworkplaceenvironmentorpracticesetting.
6.Integratedclinicaleducationexperiencesshallincludestudentassessmentsthataredesignedtolinktothecourseorprogramobjectiveswithexpectedstudentprogressioninprofessionalbehaviors,clinicalknowledge,and/orskills.
7. Integrated clinical education experiences are coordinated by a faculty member of the academicprogram,inpartnershipwithacoordinatorfromtheclinicaleducationsite.
8. Integrated clinical education experiences are typically supervised by a course instructor and apreceptor. The preceptormay be an academic course facultymember, a clinical instructor, or otherhealthcareprofessionalatthesitethestudentisengagedintheexperience,dependinguponthecourseand/orprogrammaticobjectives. Integrated full time clinical educationexperiences thatqualify for aprogram’s minimum number of clinical education weeks shall be supervised by a licensed physicaltherapist.
GuidelinesforDevelopmentofICE
The following are guidelines for collaborative development and implementation of integrated clinicaleducationexperiences.PleaserefertotheICEPanelreportfortheprovocativequestionsandevidencethataccompanytheseguidelines.
Thekeytowell-developedintegratedclinicaleducationexperiencesisintentionality.Intentionalandtargetedinstructionencompassesplanningwithapurpose,cultivatingthelearningenvironment,instructingwithintention,andassessingtheimpactthatthemodelhasonstudentlearningwhichiswhattheguidingprinciplesareattemptingtodirect(Fisher,Frey&Hite,2016).Theguidingprinciplesprovidedfocusonthekeyelementsthatprogramsshouldconsiderindevelopingorrefiningintegratedclinicalexperiences.Theseinclude:
1. Anacademicprogramidentifiestheprogrammaticoutcomesthatareexpectedwhenstudentsparticipateinintegratedclinicalexperiences.
2. Theacademicprogramconsiderstheintentionalplacementofintegratedclinicaleducation
experienceswithinitscurriculum.3. Theacademicprogramidentifiesthecourse(s)whereclinicaleducationshouldbeintegrated
withintheprogram.
4. Theacademicprogram,incollaborationwithprogramfacultydevelopsthecoursespecificobjectivesforstudentachievementwithinanintegratedclinicaleducationexperience.
5. Theacademicprogram,incollaborationwithprogramfaculty,identifiesthetimingand
timeframesofwhenclinicaleducationexperiencesshouldbeintegratedwithincourse(s).
83
Page 85
ICEAppendixA
6. Theacademicprogram,incollaborationwithprogramfaculty,identifiestheindividualorindividualswhowilloverseetheintegratedclinicaleducationexperiences.
7. Theacademicprogram,incollaborationwithprogramfaculty,identifiesthemethodsofstudent
andcourseassessmenttomeettheintendedcourseand/orprogramoutcomes.8. Theacademicprogramidentifiesresourcesandlegal/regulatoryparametersthatimpacts
deliveryofintegratedclinicaleducationexperienceswithinprogram.9. Theacademicprogram,incollaborationwithprogramfaculty,selectsthetypeofclinicalor
communitysitesrequiredforintegratedclinicaleducationexperiences.10. Theacademicprogram,incollaborationwithprogramfaculty,acceptsresponsibilityforthe
developmentofrelationshipswithrepresentativesoftheclinicaleducationsite.
Currentevidenceoutlinestheintentionalityofintegratedclinicaleducationexperienceplacement,purpose,necessaryresourceallocation,anddesiredoutcomeswithinphysicaltherapisteducationattheprogramlevel.Assuch,integratedclinicaleducationexperiencesmaybeembeddedwithinacourseoroccurconcurrentwithothercourseworkdependingonthedesiredprogrammaticand/orcourseobjectivesanddesireoutcomes.Intentionalityalsooccursinthedesign,resourcenecessities,andplacementofobjectivedrivencollaborativelearningexperiencesthatadheretopedagogicallysoundprinciplesthatareinnovativeand/orflexible(Fisheretal,2016)
Whilemuchattentionshouldbeplacedonthedesignandimplementationofintegratedclinicaleducation,planningforandcompletingawell-roundedassessmentisalsorequired(Weddle&Sellheim,2009).Outcomeassessmentofstudentlearning,overallcoursesuccess,andtheintegratedclinicaleducationprogramdesignarethreetargetedareasforconsideration.Selectionofvalidandreliableoutcomemeasuresthatprovidefacultyandstudentssummativeandformativefeedbacktoguidelearningisimperative.Table2providesanexampleofoutcomemeasuresusedandtypeofdatacollectedthathaveguidedacademicprograms.Itisimportanttonotethatnoattemptsweremadetocomparemodelsoroutcomedata;ratherthedatageneratedprovidedathematicanalysisofimportantconceptswithintheliterature.
Despitethefactchallengesineducationalresearchexist(Jensenetal,2016),itbehoovesourprofessiontocontinueresearchingoutcomesofinnovativecurricularmodels,includingintegratedclinicaleducationexperiences,tocontinuetostriveforexcellenceinphysicaltherapisteducation.Therefore,furtherinvestigationintobestpracticeforICEexperiencesshouldcontinueinacollaborativemannerbetweeninstitutionaladministrators,academicphysicaltherapyfaculty,clinicalfaculty,patients,andstudents.Itishungerforimprovementthatpushesboundariestopromoteexcellence(Fullan,2005).
84
Page 86
STUDENTREADINESSSTRATEGICINITIATIVEPANELFinalReportJune2017
BACKGROUNDTwooftheSummitrecommendationsincludedaspectsofensuringconsistentpreparationofstudentsforvaryinglevelsofclinicaleducation.Thisconsistencywasdescribedas‘arequisitecoresetofknowledge,skills,attitudesandprofessionalbehaviors’(RecommendationIX)and‘clinicalcoreperformancecompetencies’(RecommendationX)foreachlevelofclinicalexperience,includingearlyclinicalexperiences.Athirdrelatedrecommendationsuggeststheneedfordefiningentry-levelgraduatecompetencewhichiscontemporaryandadaptabletoachanginghealthcareenvironment(RecommendationXI).ThechargefortheStudentReadinesspanelconsideredaddressedrecommendationsIXandX.CHARGETheACAPTStudentReadinessStrategicInitiativePanelwillidentifyanddefineacoresetofcompetencies(knowledge,skills,attitudesandprofessionalbehaviors)thataretobedemonstratedbystudentspriortoentryintofull-timeclinicaleducation.FortheperiodofOctober2015throughOctober2017theACAPTBoardofDirectors’determinedthechargefortheACAPTStudentReadinessTaskForceas:
1. Investigateanddescribemodelsofcompetencyassessmentusedacrossotherhealthprofessions
2. Proposetwoformatoptionsforestablishingcompetenciestotheboardmembership3. Collectbroad-based,representativedataonminimumcompetencysfromthephysicaltherapy
practicecommunity4. Onceapreferredmodelisselectedandminimumcompetenciesareidentified,proposebaseline
expectationsandcriteriaforminimumcompetencies(knowledge,skills,attitudesandprofessionalbehaviors)thatmustbemetwithintheacademicprogrambystudentpriortoprogressingintofull-timeclinicaleducationexperiences.
5. Developguidelinesforacademicprogramstoimplementthesecompetencyrequirementswithintheircurriculum.
AcallforvolunteersforthisStudentReadinessStrategicInitiativePanelwasmadeinthefallof2015withmembersappointedinDecemberof2015.TheStudentReadinessStrategicInitiativePanelconsistsofa12-memberteamwithawealthofinformationandexperience.Thereare4DirectorsofClinicalEducation,2CenterCoordinatorsofClinicalEducation,2AcademicFaculty,3ProgramDirectors,and2AssociateDeans.TheACAPTLiaisontothegroupisShawneSoper,PT,DPT,MBA.
SUMMARYOFWORKThepanelmetatCSM2016andbeganreviewingliteraturefromdifferenthealthprofessionsincludingmedicine,pharmacy,nursing,speech,athletictrainingandoccupationaltherapy.Thepanelinvestigatedthevariedcompetencyexpectationsofthedifferentprofessionsaswellaswhenandhowtheyassessedstudentsatvariouspointsalongtheircontinuumoflearning.Thisinformationwascollectedandsummarizedtomeetthefollowingcharge:Charge1:Investigateanddescribemodelsofcompetencyassessmentusedacrossotherhealthprofessions.
85
Page 87
Competencybasededucationtraining(CBET),whichisdefinedastheabilitytoperformataskoractivitysuccessfullyandefficiently,islearner-centeredandbeganintheteachereducationreformmovementofthe1960s(Sullivan,1995).AccordingtoShah(2016),competencyis“theabilityofahealthprofessionalwhichcanbeobserved.Itencompassesvariouscomponentssuchasknowledge,skills,values,andattitudes.”Astudentappliesthesecompetenciesinanactualsettingandoncetheycantheyareconsideredcompetent.Competency-basededucationinthehealthcareprofessionshasbecomeaprominentapproachtopostgraduatemedicaltraininginCanada,theNetherlands,theUnitedKingdom,theUnitedStates,andmanyothercountries.Otherhealthprofessions,suchasnursing,haveusedcompetencyframeworksfordecades,whileothers,suchasdentistry,havedescribedtherequiredcompetenciesoftheirprofessionsmorerecently.Thenursingprofessionembracesavarietyofeducationalprogramsandtrackstheirlearnersthroughoutacontinuumincludingcompetencyattheassociate,bachelors(AACN,2008),masters(AACN,1996;AACN,2011),andatthedoctorofnursingpractice(DNP)level(AACN,2006).Formedicaleducation,theAssociationofAmericanMedicalColleges(AAMC)haspublishedguidelinesformedicalschoolstofollowindesigningtheirpre-clinicalcurriculum(AAMC,2008).Thisdocumentoutlines12competencyareasformedicalstudentstoachievebeforeembarkingonclinicalclerkships:professionalism,patientengagementandcommunicationskills,applicationofbiomedicalknowledge,history-taking,patientexamination,clinicaltesting,clinicalprocedures,informationmanagement,diagnosis,clinicalintervention,prognosis,andpersonalizingpatientcare.Thedocumentprovidesaseriesofrecommendationstoguidemedicalschoolsindesigningcurriculathatenablestudentstoachievethesecompetencies.Oncemedicalstudentscompletetheirclerkshipsandgraduatefrommedicalschool,mostprogresstospecialtyresidencyprograms.AsaresultoftheOutcomesprojectinthelate1900s,theAAMCestablished8competencydomainsaswellasCoreEntrustableProfessionalActivities(EPAs)thatmedicalschoolgraduatesshouldachievepriortobeginningaresidency(AAMC,2014).TheseEPAsfocuson“activities”thatencompasstheday-to-dayworkoftheresidentphysicianratherthantraditionalcompetencies.TheEPAsaregenericinthattheyarenotspecifictoanyonemedicalspecialty.Foreachofthe10EPAs,thedocumentincludesdescriptionsandvignettesoflearnerswhohaveeithermetornotmettheexpectedlevelofperformance.“EPAsareobservableandmeasurableandthereforecanfunctionasaquantifiableoutcomethatcanaidintheassessmentofastudent(TenCate,2013).”
PhysicalTherapyLiterature:
Therearemanyestablishedrequirementsandcompetenciesforphysicaltherapystudentsatvariouspointsalongtheircontinuumoflearning.Therearepre-requisitesforstudentstoentertheDPTprogram(AC-4-12STANDARDPREREQUISITECOURSESFORADMISSIONINENTRY-LEVELPHYSICALTHERAPISTEDUCATIONPROGRAMS).Setting-specificcorecompetencieshavealsobeenestablished.Forexample,inpediatrics,aqualitativestudyusingtheDelphimethodbyKenyon,DoleandKelly(2013),lookedattheperspectivesofAcademicfacultyandClinicalInstructorsonEntry-LevelDPTPreparationforpediatricphysicaltherapistpractice.Theyfoundconsensusontheknowledge,skills,andabilitiesrequiredforpediatricPTpracticeatvariouspointsinthecurriculum;beforeapediatricclinicalexperience,followingapediatricclinicalexperienceandpriortoentranceintoclinicalpractice.Theauthorsalsodefinedlevelsofproficiencypertainingtoknowledgeaswellasskillsandabilitiesateachofthosepoints.Thisstudybringsforththeconceptofvariousskillsandabilitiesexpectedatvariouspointsofapediatricspecificcurriculum.AtaskforcefromtheSectiononWomen’sHealthdevelopedguidelinestoassistphysicaltherapisteducationprogramswithidentifyingspecificwomen’shealthcontentthatshouldbeincludedinentrylevelphysicaltherapyprograms(APTA:Women’sHealthSection,2014).Thestudyidentifiedcontent
86
Page 88
alongwithalevelofcompetencetheentry-levelstudentisexpectedtoachieverangingfromfamiliaritytomastery.Thisstudyprovidesacomprehensiveframeworkfordeterminingproficiencyofvariousskillsets.Gazsi(2011)exploredexpectationsofphysicaltherapyemployers,andacademicandclinicalfacultyregardingentry-levelknowledge,skills,andbehaviorofphysicaltherapistgraduatesinacuterehabilitationpractice.Theauthorfoundconsensusonselectentry-levelcharacteristicsandmostoftheparticipantsreportedthatnewDPTgraduatesaremeetingexpectationsintheacuterehabpracticesetting.Otherpopulationandsetting-specificcorecompetenciesforentranceintoclinicalpracticeexist,includingintegumentary,handtherapy,musculoskeletal,acutecare,andresearchtonameafew(Gazes,2011;Gorman,2010;APTA:NeurologySection,2011;Rapport,2014)
Entry-levelexpectationshavebeenreportedintheliteraturefromavarietyofviewpoints(Jette,2007;Lopopolo,2004;Mathwig,2001;Schafer,2007).AstudybyJetteetal(2007)surveyedphysicaltherapyclinicalinstructorsonwhataspectsofastudent’sperformancedemonstratethattheymeetentry-levelexpectationsforthephysicaltherapypractice.Participantsidentifiedsevenattributesincluding:knowledge,clinicalskills,safety,clinicaldecision-making,self-directedlearning,interpersonalcommunication,andprofessionaldemeanor.Thestudydescribedbehaviorsandcharacteristicsthatclinicalinstructorsbelievecompriseentry-levelperformancealongwithadecision-makingprocessbyinstructorsthatintegratescharacteristicsintosubjectiveperceptionofanentry-levelclinician.Thestudydidnotidentifythespecificclinicalskillsneededforentry-levelphysicaltherapyperformance.
Chipchaseetal(2012)examinedthecharacteristicsofstudentpreparednessforclinicallearningfromtheperspectiveofclinicaleducators.Thestudyidentifiescertainbehaviorssuchaswillingness,professionalism,andcommunicationasbeingmostimportantwhenenteringaclinicalexperience.Thisstudyfocusesonthestudentphysicaltherapistastheyenterclinicalexperiences,notonthebehaviorsrequiredforentry-levelpractice.Itidentifieskeybehaviorsandcharacteristicsfromtheclinicaleducator’sperspectiveonreadiness.However,itdoesnotprovideaconsensusamongstotherstakeholdersincludingacademicfacultyanddirectorsofclinicaleducation,whoareallintegrallyinvolvedinclinicaleducation.Nordoesitprovidelevelsofcompetenceneededintheknowledge,skillsandattitudesidentified.TheAmericanPhysicalTherapyAssociationhasdevelopedaframeworkidentifyingminimumrequiredskillsofphysicaltherapistgraduatesatentry-level(APTA,2005),howeverresearchstilldemonstratesthatdisparityexistsinperceptionsofwhatconstitutesentrylevelperformance.Withtheinceptionofthefirstresidencyandfellowshipeducationprogramsin2000,researchhasbegantoexaminecompetenceatthepost-professionallevel.ArecentpublicationbyFurzeetal(2016)lookedatPTResidencyandFellowshipEducation:ReflectionsonthePast,Present,andFuture.Theauthorsproposed7domainsofcompetence,similartothe8frommedicine,whichinclude:knowledgeofpractice,inquiryskills,clinicalskills,clinicalreasoning,systems-basedapproach,communication,andprofessionalism.Thesedomainsarethoughttotheoreticallygroundresidencyandfellowshipprogramsandfacilitateamoreconsistentapproachtocurriculardevelopmentandassessment.
Studiesfromvarioushealthprofessionsthathaveexaminedstudentreadinesshaveincludedsimilartermssuchasknowledge,skillsorabilities,aswellasthoserelatedtotheaffectivedomainincluding:attitudes,andprofessionalbehaviors.Whilethetermsbetweenthedifferentstudiesaresimilar,tobeclearmovingforwardwewillcallthetotalityofanythingthatisimportantforastudenttodemonstratepriortoaclinicalexperienceastheKSAs.AshealthcareprofessionsbegintoidentifytheessentialKSAsthatarerequiredatvariouspointsintheeducationalprocess,thequestionofhowtoassessthesecomponentsarise.Thehealthprofessionsliteraturedemonstratesavarietyoftoolsorassessmentstrategiesthatcanbeutilizedforpsychomotorandcommunicationskillsaswellasknowledgeand
87
Page 89
professionalbehaviorassessment(Peterson,Calhoun,andRider,2014;Zhuetal.,2017;Zarifsanaiey,Amini,andSaadat,2016;May,1995).Inmedicine,Competency-basedmedicaleducation(CBME)servesasthefoundationfortheNextAccreditationSystem(NAS)(ACGME,2016).ThissystemincludestheMilestonesandClinicalCompetencyCommittees(CCC),bothofwhicharedesignedtomonitorandcontinuallyimproveeducationaloutcomes,andthereforeclinicaloutcomes,attheleveloftheindividuallearnerandtheprogram(ACGME,2016).
Acompetencyisachievedgradually,step–by-step.Thesestepsaredesignatedasmilestones(Shah,2016).Milestonesdescribeperformancelevelsresidentsandfellowsareexpectedtodemonstrateforskills,knowledge,andbehaviorsintheclinicalcompetencydomains(ACGME,2016).Theylayoutaframeworkofobservablebehaviorsandotherattributesassociatedwitharesident’sorfellow’sdevelopmentasaphysician.Theyarecompetency-baseddevelopmentaloutcomesthatcanbedemonstratedprogressivelybyresidentsandfellowsfromthebeginningoftheireducationthroughgraduationtotheunsupervisedpracticeoftheirspecialties.AccordingtotheMilestoneGuidebook(2016),“Residents/fellowsareassessedroutinelythroughacombinationofassessmenttools.Theseinclude:directobservations;globalevaluation;auditsandreviewofclinicalperformancedata;CaseLogs;multisourcefeedbackfromteammembers,includingpeers,nurses,patients,andfamilies;simulation;in-servicetrainingexaminations(ITEs);self-assessment;andothers.”AnoverviewofthissystemisdepictedbelowinFigure1.
Figure1:OverviewofProfessionalSelf-RegulatoryAssessmentSystemintheU.S.
Physicaltherapyeducationliteraturehasbeguntoidentifyevaluationtechniquesaswellasspecificrubricsthatcanbeutilizedforvariousknowledge,skillsandbehaviors(Kanadaetal.,2016;Christensenetal.,2017;AndersonandIrwin,2013;Furzeetal.,2015).However,thereliabilityandvalidityofthesetoolsmustbeconsideredwhendecidingontheirusewithinindividualPTprograms.Beforeonecantrulydeveloptheappropriateassessmentsystem,theminimalknowledge,skills,andabilitiesandatwhatlevelofproficiencymustfirstbeidentified.
88
Page 90
Competencybasededucationandsubsequentassessmentispresentthroughoutvarioushealthprofessions.Themedicalprofessionseemsmostevolvedandcanprovideuswithastructureandprocessthatwemightwanttoconsiderassuchsystemsaredevelopedforphysicaltherapisteducation.Charge2:Proposetwoformatoptionsforestablishingcompetenciestotheboardmembership.
Thepaneldiscussedvariouspossibleoptionstoestablishcompetenciesincludingobtainingconsensuswithinourpanel,focusgroups,consensusconference,surveys,andaDelphistudy.Toachievetheaimofourpanel,thegroupselectedtheDelphimethodofconsensusdevelopment.ADelphistudyallowsindividualswithexpertiseandinsighttoprovideinformationandtoreachconsensusonaparticulartopic.Thismethodengagesagroupofparticipantsorexpertsovermultipleroundsofsurveystoestablishaconsensusontheparticulartopicofinterest(Keeney,2011;Soma,2009).ThepurposeofthisDelphistudywastogainconsensusonthepre-requisitesforstudentsenteringafirstfull-timeclinicaleducationexperience,specificallyfocusingonwhatattributessignaledreadiness.Thisreadinessforthefirstfull-timeclinicaleducationexperiencewouldberelevantregardlessofwhereitfallswithinaprogram’scurriculumortheparticularsettinginwhichtheexperiencetakesplace.
GiventhevariabilityofcurriculuminCAPTEaccreditedphysicaltherapyprogramsaswellastheplacementofclinicalexperienceswithinthatcurriculum,thepanelthoughtitbesttobeginwithastudentsentranceintothefirstfull-timeclinicaleducationexperience.ThepanelalsofeltthattheearlyclinicalexperiencescanbeinanypracticesettingandareoftenthemostchallengingforDCEs/ACCEstofindstudentplacements,ascliniciansarereluctanttotakeonastudentwhileontheirfirstclinicalexperience.Startingwithcompetenciesforthisexperiencewouldonlybeonepointalongthecontinuumoflearningwherestudentswouldbeassessedbutwasanimportantplacetostart.Akeyfeaturetocompetency-basededucationalprinciplesistheincreasedemphasisonassessment,especiallyongoing,longitudinalassessmentthatenablesthefacultytomoreaccuratelydeterminethedevelopmentalprogressofthelearner,aswellastohelpthelearnerthroughfrequentfeedback,coaching,andadjustmentstolearningplans(Holmboe,2010;Kogan,2013).TheDelphimethodwasidentifiedasthemostpracticalmethodtogainconsensusamongthevariousmembersofthephysicaltherapypracticecommunity.
Aspreviouslymentioned,thepanelchosetheDelphimethodasameanstoobtainconsensusontheknowledgeskills,attitudesandprofessionalbehaviorsforentranceintothefirstfulltimeclinicaleducationexperienceandtoalsoaddresscharges3and4:
Charges3and4:Collectbroad-based,representativedataonminimumcompetencyexpectationsfromthephysicaltherapypracticecommunity
Onceapreferredmodelisselectedandminimumcompetenciesareidentified,proposebaselineexpectationsandcriteriaforminimumcompetencies(knowledge,skills,attitudesandprofessionalbehaviors)thatmustbemetwithintheacademicprogrambystudentpriortoprogressingintofull-timeclinicaleducationexperiences.
Toobtainagroupofexpertparticipants,inNovember2016allACAPTmemberinstitutionswerecontactedandaskedtonominate4individualswho,basedontheirexposureandexperience(definedbelow),wouldbeabletoreflectandprovidetheirexpertopinionsandinsightsonstudentreadiness.TheprogramdirectorsofACAPTmemberinstitutionswereaskedtonominate:
• OneAcademicfacultymember(5yearsofexperienceasaCoreFacultymember)• OneDirectorofClinicalEducationorAcademicCoordinatorofClinicalEducation(5yearsof
experienceasaDCE/ACCE)• OneRecentGraduate(withinthepast8months,withsuccessfulpassageofthelicensureexam)
89
Page 91
• OneClinicianwhoserves(orwhohasserved)asclinicalinstructorforDPTstudents(atleast5firstfull-timeexperiencestudents);thisparticipantwasnominatedspecificallybytheprogram’sDCE/ACCE.
Programdirectorswereaskedtoforwardaninvitationemailtotheseindividualsandparticipantsindicatedtheirwillingnesstoparticipatebyrespondingtooneoftheresearchers.Specificquestionsinthefirstroundsurveyweredesignedtoconfirmthatparticipantsmettherelevantinclusioncriteria.Thesurveyfirstroundsurveywasdevelopedbasedontheinputofanexpertreviewpanelthatprovidedfeedbackandassistanceonindividualsurveyquestionsandinstructions.Thisfirstroundsurveyconsistedofaseriesofdemographicquestions(basedontheparticipantsgroup)aswellasopen-endedquestionswhichaskedparticipantstothinkabouttheirexperienceswithstudentsastheybegantheirfirstfull-timeclinicalexperience.Participantswereaskedtodescribethestudentthattheywouldconsiderreadyforthisclinicalexperienceandlisttheitemstheyconsideredrequisiteforastudentontheirfirstfulltimeclinicalexperience.Participantswereinstructedtoconsiderthisreadinessregardlessofwhenthefirstfull-timeexperienceoccurredwithinthestudent’sacademiccurriculumorthesettinginwhichthatfirstexperiencetookplace.Participantswerealsoaskedhowtheycouldknowormakethedeterminationthatthestudenttheydescribedwasreadyfortheclinicalexperience.InaccordancewiththeDelphimethod,surveysinsubsequentroundsthenbuiltontheresponsescollectedinpreviousrounds.ThesecondroundsurveyprovidedalloftheuniqueresponsestothequestionsfromRound1withregardtoreadinessandgatheredinformationaboutclarityandredundancyintheitemsprovided.Inordertocreatethesecondroundsurvey,theresearchersconductedcontentanalysisofthefirstroundresponsesandplacedtheresultsinbroadcategoriestoprovideorganizationtothedatainthemes.Researchersworkedinteamstoanalyzeinformationfromindividualstakeholdergroupsfirstandthencametogethertocompletethecontentanalysisoftheentiresetofdatafromthefirstround.Responsestothesecondroundsurveywerealsoanalyzedbyresearchersinsmallteamsinordertoconsolidateareasofredundancyandtoimproveonclaritybasedonparticipantfeedback.Wheneverthereweredisagreements,thegroupengagedindiscussionandconsensusonthefinalwordingormethodofconsolidationofitems.Thethirdroundaskedparticipantstoranktheiragreementwiththeremainingitems(within14identifiedthemes)usinga5-pointLikertscale(stronglyagree–stronglydisagree).Thisprocessidentifiesareasofconsensusonthoseitemsthatareessentialtostudentreadinessforafirstfulltimeclinicalexperience.Inthefourthroundparticipantsprovidedthelevelofproficiency,asdefinedinTable5,theyconsideredastudentshouldbeexpectedtoachievetodemonstratereadinessoneachitemthatachievedconsensusinRound3(>80%agreement).Ineachround,participantswereinvitedtoprovidecommentsandfeedbackonitemsandthemes.Afinalstepinthefourthandfinalroundwastoindicatethetypesofassessmentsthatwouldbeappropriatefordeterminingreadinessforeachthemeidentified.Thelistofavailableassessmentsprovidedforselectionwasgeneratedfromparticipantresponsestoquestionsfromthefirstroundsurveyonhowtodetermineorassessforreadiness.Results:
Surveysweredistributedtothe147individualswhoacceptedthenomination(39Academicfaculty,34DirectorsofClinicalEducation,37ClinicalInstructorsand38recentgraduates).ThetotalresponserateforRound1was88.4%,with130round-onesurveysreturned(Table1).Respondentstothesurveyrepresentedabroadgroupofstakeholdersdeeplyinterestedinclinicaleducation.TheywereaffiliatedwithDPTprogramsacrossallregionsoftheUnitedStates(Table2).
90
Page 92
RespondentsfromallcohortsrepresentedaffiliationswithDPTprogramsfromacrossthecountrybutfocusedprimarilyinurbanandsuburbanareas.Thetypicalprogramhadfourclinicaleducationexperiences,rangingfromatotalof30to54weeksoffulltimeclinicalexperiences(average=36weeks).Themajorityofprogramaffiliatesreportedtheirfirstfulltimeclinicalexperienceoccurredattheendofthefirstyearofthecurriculumand10respondentsindicatedthattheirfirstfulltimeclinicalexperiencebeganfollowingconclusionofalldidacticeducation.Somequestionswerespecifictoastakeholdergroupandthereforenotallgroupswerequeried.Forexample,thenumberofweeksonthe1stclinicalexperiencewasaskedofrecentgraduatesonly.Thoseindividualswithapreferenceofsettingforthefirstfulltimeclinicalexperiencepreferredoutpatientorthopedicoracutecare(Table3).Responsesregardingelementsofcompetencyfromeachcohortwereconsolidated,duplicateseliminated,andgroupedintotwentythemes.Eachthemehadbetweenoneand27supportingelements(total=193).Allthemesandelementswerereturnedto132participantsforconsiderationinRound2.Recommendedmethodsofassessingtheelementswerealsoconsolidatedacrossallgroupsanddistilleddowntoeight,whichrepresentabreadthofassessmentintheDPTcurriculum.Onehundredandfivesurveyswerecompletedandreturnedduringroundtwo(79.55%).Responseswerereviewedandclarificationsandeliminationswereexecutedbyconsensusoftheresearchteam.Roundtworesultedinconsolidationofsixthemesandtheconsolidationoreliminationof54elementsduetosimilarityorredundancy.ThemesandelementsderivedfromeachroundofdataanalysisarereportedinTable4.Thefinalremaining14themesandtheir139elementswerereturnedtoparticipantsinthethirdround.Onehundredthirty-twosurveysweredistributedinroundthreeand104(78.79%)werereturned.All14themesachievedgreaterthan80%agreementalongwith95specificelements.The44elementsthatdidnotachieve80%consensusweredeemedlessimportantornotessentialbyparticipantsandwereeliminatedfromthefinallistforroundfour.AppendixAcontainsthelistofthemesalongwiththelevelsofconsensusachievedforthe95survivingelements.AppendixBcontainsthe44elementseliminatedbythemeandthepercentconsensusachieved.
InthefinalroundofthisDelphisurvey,surveysweresenttothesame132ongoingparticipantsand104(78.79%)responseswerereceived.TotalresponsesbyroundarereportedinTable4.Basedongroupconsensusasestablishedbythe80%threshold,only9elementswereidentifiedasrequiringproficiencypriortothefirstfull-timeclinicalexperience(Table6).Themajorityoftheseelementsfellintheareaofprofessionalbehaviorswhileotherssurroundedsuccessfulacademicperformance.Therewasgeneralagreementbetweenstakeholdersforelementsdeterminedtorequireproficiencypriortothefirstclinicalexperience(AppendixA).Onlyfourelementsthatoneofthestakeholdergroupsreportedasrequiringproficiencydidnotreachthelevelneededtoreachachieveoverallconsensus.TwooftheseelementsbelievedbyexperiencedclinicalinstructorstobecriticalpriortothefirstclinicalexperiencewererelatedtoworkethicandthefamiliarityandadherencetothecorevaluesoftheAPTA.Recentgraduatesvaluedtwoelementshighlythatdidn’treachthelevelofoverallconsensus.Thesewererelatedtothewillingnesstoseek,andbereceptiveto,feedback.
ParticipantsratedthevastmajorityofelementsasrequiringatleastanEmerginglevelofmastery(ratingsofEmergingorProficient)priortobeginningthefirstfulltimeclinicalexperience(AppendixA).Therewere,however,34elementsthatdidnotachievethelevelofconsensusrequiredtoindicatethattheybemorethanFamiliartothestudentpriortothefirstfulltimeclinicalexperience(AppendixA).
Assessment:Respondentsidentifiedtheirpreferredmethodofassessingcompetenceineachofthefourteenthemesduringroundfour(Table7).Usingthepredeterminedlevelofconsensusof80%there
91
Page 93
were1to3methodsofassessmentthatreachedconsensusforeachtheme.Themesrepresentativeofthecognitivedomainwereidentifiedasbestassessedthroughwrittenexamsorskillschecks,whilethoseintheaffectivedomainwereidentifiedasbestassessedthroughfacultyandstudentassessment.Participantsreachedconsensusonassessingpsychomotorskillsthroughpracticalexaminationperformance.Discussion:
Asaresultofthisprocessthefindingshaveconfirmedthoseofpreviousstudies(Roach,2012;Kenyon,2013;May,1995)thathighlighttheimportanceearlyon,ofskillswithintheaffectivedomain.Inparticular,communicationandprofessionalism.
Theresultswereanalyzedbyeachstakeholdergroup,aswellasthenumericalaverageacrossgroups(combinedstakeholders).Therewere95elementsthatthecombinedstakeholdersagreedwereappropriateforreadinessforafirstclinicalexperience.Nineelementswereidentifiedasrequiringproficiencypriortothefirstfull-timeclinicalexperience(Table7).Threeofthenineweredichotomouschoices(accomplished/presentornot)whichthecombinedstakeholdersagreedshouldbepresent:studentsshouldhavetheminimumacademicGPA,meetminimumexpectationsforacademicpracticalexaminations,andhaveresolvedanyandallsafetyconcerns.The6additionalelementsfellintheareaofprofessionalbehaviorsalsoshowninTable7:demonstrationofpolite,personable,engagingandfriendlybehaviors;introductionofone’sselftoCI,clinicalstaff,andpatients;respectforpatients,peers,healthcareprofessionals,andcommunity;punctualitywithallassignments;understandingofHIPAAregulations;andappropriatedresscode.Thus,wehadconsensuson9elementsasessentialforreadiness,withaneedtobeproficientpriortothefirstfulltimeclinicalexperience.Whenlookingattheremaining86elementstherewere4elementsthatdidnotreceiveanoverallconsensusof80%foraparticularlevelofproficiency,butdidachieve80%proficiencyinatleastonestakeholdergroup.Theseincludeappropriateworkethic,whichachievedthresholdconsensusintheclinicalinstructorandrecentgraduategroups;corevaluesidentifiedbytheAPTA,whichachievedconsensusintheclinicalinstructorgroup;beingopenandreceptive,verballyandnon-verbally,whichachievedconsensusintherecentgraduategroup;andseekingassistancewhenneeded,alsointherecentgraduategroup.AsseeninAppendixA,theresultsfromemergingandproficientlevelsofproficiencywerecombined.Bydoingsowefoundthatthereare58itemsthatparticipantsfeltthatstudents,ataminimum,hadtodemonstrateatleastanemerginglevelofproficiency.Thisinformationcanbequitehelpfulforacademicprogramsinthattheymayneedtoincreasetheamountofcontentcoverageinthisareasothatstudentshaveabitmoredepth.Justbeingfamiliarwouldnotbesufficient.Findingsfromthisstudycanassistprogramsintheircurriculardevelopmenttostrategicallyplacecoursesthatcovercontentthatstudentswillneedtoknowpriortothefirstclinicalexperience.
RECOMMENDATION1:
Thatthelistofknowledge,skills,andabilities(KSAs),groupedinto14themes,requiringstudents’demonstrationofcompetencepriortoenteringtheirfirstfull-timeclinicalexperienceasshowninAppendixC(FirstFull-timeClinicalExperienceKSAs)beadopted.
SS:Academicprogramsshouldbeencouragedtoprovidestudentswiththeappropriateeducationalexperiences/modulessothatthestudentmayachievethelevelofproficiencyindicatedforthesaiditems(AppendixA).Thisinformationwouldensureconsistentpreparationpriortoastudent’sfirstfull-
92
Page 94
timeclinicalexperience.Giventhisinformation,clinicalinstructorscanbeconfidentthatstudentswouldbegintheirclinicalexperiencewithcompetencyintheseitemsandcanthereforedevelopandprovideamoreappropriatelearningenvironmentforastudenttocontinuetogrow.Theformatofthethemesandelementsmaybestartingpointsforthepotentialdevelopmentofentrustableprofessionalactivitiesandcompetencymilestonesthatwouldbeapplicabletoallstudentsinphysicaltherapisteducationpriortoentranceintotheirfirstfull-timeclinicalexperience.
RECOMMENDATION2:
ThatACAPTdevelopaplan,includinganimplementationtimeline,toguidephysicaltherapisteducationalprogramsinimplementingtheuseoftheFirstFullTimeClinicalEducationExperienceKSAs.Thisplanshallalsoincludeguidanceoncommunicationtoclinicalpartners.
SS:AdoptingtheidentifiedKSAsisanimportantfirststepofthisinitiative.TheparticipantsintheSummitclearlyidentifiedaneedforconsistencyinthelevelofcompetenceofstudentsenteringtheirfirstfulltimeclinicalexperience.ThissetofKSAsprovidestheminimalexpectationsforthosestudents.InorderfortheeducationalprogramsandclinicalpartnerstoimplementtheseKSAs,additionalconsiderationstocommunication,assessment,expectations,andtimelinesneedtobeconsidered.
RECOMMENDATION3:
ThatACAPTencouragephysicaltherapisteducationalprogramstoevaluateandmakeappropriatechangestotheircurriculumtoenablestudentstoachievecompetencyintheFirstFull-timeClinicalExperienceKSAs.
SS:Asdescribedabove,theclinicalsitesareanxiousforastandardsetofcompetenciesthatallfirstfull-timestudentshaveachievedpriortoarrivingintheirclinics.Onestepinachievingthisgoalrequireseducationalprogramstoassesstheircurriculumanddetermineifchangesareneededtoenablestudentstoachievethedescribedlevelsofcompetence.ManyprogramslikelyhavethecomponentsinplacethatenablestudentstomeettheseKSAs;otherprogramsmayneedtomakeonlysmallchangestoachievethisgoal;andstillothersmayneedtoconsidershiftintheprogramdesign.Inanycase,beingresponsivetotheSummitrecommendationsandthusthevoiceofourclinicalpartners,startswithanassessmentofcurrentstateandnecessarychanges.
RECOMMENDATION4:
Thatstudentreadinesspriortoentranceintotheclinicalpractice(entry-level)beexaminedasthenextsteptoachievingtheSummitrecommendationsrelatedtoreadinessandcompetency.
SS:Thispanelfocusedonstudentreadinessforentranceintothefirstfull-timeclinicaleducationexperience.Itrepresentsonemomentalongastudent’scontinuumoflearning.TheSummitparticipantsidentifiedtheneedforadditionalpointsofcompetenceassessment.
Thevariabilityofnumber,length,andtimingofclinicalexperienceswithinphysicaltherapistcurriculamakestandardizationofcompetenceexpectationsatseveralpointsalongthestudent’seducationimpossible.ThisrealizationledtheStudentReadinesspaneltochoosethepointofentryintothefirstfull-timeclinicalexperienceasacommonpointthatwasappropriateforstandardization.
Theothertwopointsintimethatlendthemselvestostandardcompetenceassessmentarepriortoentryintothefinalfulltimeclinicalexperienceandjustpriortoentryintopractice.Identifyingstandardelementsofcompetencethatshouldexistaftercompletionofalldidacticandclinicalcourseworkwillprovidevaluableinformationtoclinicalinstructorsandensureacommonlevelofpreparationforstudentsatthatphaseoftheireducation.
93
Page 95
RECOMMENDATION5:
ThatACAPTsupporttheneededcollaborativeeducationalresearchtodeterminethemostappropriatetypesofassessmentsofstudentreadinessandatimelineforimplementation.
SS:ParticipantsindicatedthevariousassessmentmethodsthatcanbeutilizedforeachitemthatachievedconsensusintheDelphistudy(Table7).Thislistisnotmeanttobeprescriptivebuttoprovideoptionsforacademicprograms.TheseitemsreflectcurrentmethodsofassessmentandmaynotbethemostconnectedtowhatisusedinCBME.NowthatconsensushasbeenachievedontheKSAsstudentsmusthaveordisplayandgiventheimportanceofassessmentandevaluationincompetency-basededucation,additionalresearchtodeterminethebestassessmentmethodsiswarranted.Bestpracticeshouldbeutilizedtodevelopacontinuedandfrequentassessmentprocesstoensurephysicaltherapiststudentsachievethemilestonesattheappropriatetimeintheircontinuumoflearning.
Competency-basedphysicaltherapistclinicaleducation(CBPTCE)necessitatesarobustandmultifacetedassessmentsystem.Theleadershipwithinourprofessionmustattendtothecontextofthemultiplesettingswhereclinicaleducationoccurs.CBPTCE,likeCBME,furtherrequiresassessmentprocessesthataremorecontinuousandfrequent,criterion-based,developmental,work-basedwherepossible,useassessmentmethodsandtoolsthatmeetminimumrequirementsforquality,usebothquantitativeandqualitativemeasuresandmethods,andinvolvethewisdomofgroupprocessinmakingjudgmentsaboutstudentprogress.Inaddition,ashiftinthinkingneedstooccurfromassessmentoflearningtoassessmentforlearning.Researchintothequalityofassessmentprograms,howassessmentinfluenceslearningandteaching,newpsychometricmodelsandtheroleofhumanjudgmentismuchneeded(Schuwirth&VanderVleuten,2011)
TheStudentReadinessStrategicInitiativePanel’srecommendationcomplimentswiththerecommendation#5bytheExcellenceinPhysicalTherapyEducationTaskForce(APTA,2015).Theynotetheprofessionshouldsupportthedevelopmentofastandardizedassessmentforphysicaltherapiststudentspriortoenteringtheirterminalclinicalexperience.Theassessmentwouldevaluatestudents’readinessfortheclinicaleducationandassistinimprovingrelationshipswithclinicaleducationsitesbysettingconsistentstandardsforstudentsbeforetheybegintheseexperiences.Theassessmentmayalsodecreaseunwarrantedvariationinstudentpreparation,whichwoulddecreasetheburdenonclinicalsitesduetodifferencesincurriculumacrossprograms.
MEETINGHISTORYFacetofacemeetingswereheldatCombinedSectionsMeeting(2016and2017),aswellastheEducationalLeadershipConference.
TheentirePanelheldthree-conferencecalls/monthfromFebruary2016–June2017.Inaddition,sub-groupsmetasneededduringthistimeframe.
94
Page 96
REFERENCES:
AccreditationCouncilforGraduateMedicalEducation(ACGME)OutcomeProject.Accessedhttp://www.acgme.org/outcomeAccreditationCouncilforGraduateMedicalEducation(ACGME)TheMilestoneBook,Version2016.http://www.acgme.org/Portals/0/MilestonesGuidebook.pdf?ver=2016-05-31-113245-103AccessedMay1st,2016.AccreditationCouncilforGraduateMedicalEducation(ACGME)ClinicalCompetencyCommittees;AGuidebookforPrograms.http://www.acgme.org/Portals/0/ACGMEClinicalCompetencyCommitteeGuidebook.pdf?ver=2015-11-06-115643-130AccessedMay1st,2017.AmericanAssociationofCollegesofNursing.TheEssentialsofMaster’sEducationforAdvancedNursingPractice.1996.http://www.aacn.nche.edu/education-resources/MasEssentials96.pdfAccessedMay1st,2016.AmericanAssociationofCollegesofNursing.TheEssentialsofDoctoralEducationforAdvancedNursingPractice.2006.http://www.aacn.nche.edu/publications/position/DNPEssentials.pdfAccessedMay1st,2016.AmericanAssociationofCollegesofNursing.TheEssentialsofBaccalaureateEducationforProfessionalNursingPractice.2008.http://www.aacn.nche.edu/education-resources/BaccEssentials08.pdfAccessedMay1st,2016.AmericanAssociationofCollegesofNursing.TheEssentialsofMaster’sEducationinNursing.2011.http://www.aacn.nche.edu/education-resources/MastersEssentials11.pdfAmericanAssociationofCollegesofNursing.EssentialsofCollegeandUniversityEducationforProfessionalNursing:FinalReport.Washington,DC:AmericanAssociationofCollegesofNursing;1986.AmericanPhysicalTherapyAssociationBoardofDirectors.ExcellenceinPhysicalTherapyEducationTaskForceReport.Alexandria,VA:AmericanPhysicalTherapyAssociation;2015.AmericanPhysicalTherapyAssociation.NormativeModelofPhysicalTherapistEducation.Alexandria,VA:AmericanPhysicalTherapyAssociation;2004.AmericanPhysicalTherapyAssociation.Minimumrequiredskillsofphysicaltherapistgraduatesatentry-level:BODG11-05-20-49[Guideline].AmericanPhysicalTherapyAssociationWebsite.http://www.apta.org/uploadedFiles/APTAorg/About_Us/Policies/BOD/Education/MinReqSkillsPTGrad.pdf.UpdatedOctober1,2013.AccessedApril,2016AmericanPhysicalTherapyAssociation:Women’sHealthSection.GuidelinesforWomen’sHealthcontentinprofessionalphysicaltherapisteducation:2014Update.http://www.womenshealthapta.org/wp-content/uploads/2014/05/SoWH-DPT-Curricular-Content-Guide-2014-1.pdfAccessedApril,2016.
95
Page 97
AmericanPhysicalTherapyAssociation:NeurologySection.Neurologicentry-levelcurricularcontentintegratedwithanormativemodelofphysicaltherapistprofessionaleducation.2011.http://www.neuropt.org/docs/default-document-library/2011_neurologic_entry-level_curriculum_guidelines7E676FEAFF3D.pdfAccessedDec.2016.AndersonDKandIrwinKE.Self-assessmentofprofessionalisminphysicaltherapyeducation.Work.2013;275-281.AssociationofAmericanMedicalColleges(AAMC).RecommendationsforPreclerkshipClinicalSkillsEducationforUndergraduateMedicalEducation;TaskForceontheClinicalSkillsEducationofMedicalStudents.2010https://www.aamc.org/download/130608/data/clinicalskills_oct09.qxd.pdf.pdfAccessedMay1st,2017.
AssociationofAmericanMedicalColleges(AAMC).CoreEntrustableProfessionalActivitiesforEnteringResidency.2014.https://www.aamc.org/download/379308/data/coreentrustableprofessionalactivities.pdfAccessedMay1st,2017.
CanMEDS2000Project.SkillsfortheNewMillennium.ReportoftheSocietalNeedsWorkingGroup,Ottawa,September1996.ChipchaseLS,ButtrumPJ,DunwoodieR,HillAE,MandrusiakA,MoranM.Characteristicsofstudentpreparednessforclinicallearning:clinicaleducatorperspectivesusingtheDelphiapproach.BMCMedicalEducation.2012;12:112.https://bmcmededuc.biomedcentral.com/articles/10.1186/1472-6920-12-112ChristensenN,BlackL,FurzeJ,etal.Clinicalreasoning:Surveyofteachingmethods,integration,andassessmentinentry-levelphysicaltherapistacademiceducation.PTJ.2017;97(2):175-186.FurzeJA,TichenorCJ,FisherBE,JensenGM,RapportMJ.PhysicalTherapyResidencyandFellowshipEducation:Reflectionsonthepast,present,andfuture.PhysTher.2016;96(7):949-960.GazesCC.2011ExpectationsofPhysicalTherapistEmployers,andAcademicandClinicalFacultyRegardingEntry-levelKnowledge,Skills,andBehaviorofPhysicalTherapistGraduatesinAcuteRehabilitationPractice.Doctoraldissertation.NovaSoutheasternUniversity.RetrievedfromNSUWorks,CollegeofHealthCareSciences-PhysicalTherapyDepartment.http://nsuworks.nova.edu/hpd_pt_stuetd/19GormanSL,WrubleHakimE,JohnsonW,etal.Nationwideacutecarephysicaltherapistpracticeanalysisidentifiesknowledge,skills,andbehaviorsthatreflectacutecarepractice.PhysTher.2010;90(10):1453-1467.doi:10.2522/ptj.20090385Guidelinesforwomen’shealthcontentinprofessionalphysicaltherapisteducation:2014update.SectiononWomen’sHealthWebsite.http://www.womenshealthapta.org/wp-content/uploads/2014/05/SoWH-DPT-Curricular-Content-Guide-2014-1.pdf.UpdatedApril2014.AccessedDecember2016.HolmboeES,SherbinoJ,LongDM,SwingSR,&FrankJR.Theroleofassessmentincompetency-basedmedicaleducation.MedTeach.2010;32(8):676-682.
96
Page 98
InterprofessionalEducationCollaborativeExpertPanel.Corecompetenciesforinterprofessionalcollaborativepractice:Reportofanexpertpanel.AmericanAssociationofCollegesofNursingWebsite.http://www.aacn.nche.edu/education-resources/ipecreport.pdf.PublishedMay2011.AccessedDecember,2016.JetteDU,BertoniA,CootsR,JohnsonH,McLaughlinC,WeisbachC.ClinicalInstructor’sperceptionsofbehaviorsthatcompromiseentry-levelclinicalperformanceinphysicaltherapiststudents:aqualitativestudy.PhysicalTherapy.July2007:87(7):833-843.KanadaY,SakuraiH,SugiuraY,etal.Developmentofaclinicalcompetenceassessmenttoolfornovicephysicalandoccupationaltherapists-amixedDelphistudy.JPhysTherSci.2016;28:971-975.KeeneyS,HassonF,MeKennaH.TlwDelphiTechniqueinNursingandHealthResearch.Oxford,UnitedKingdom;Wiley-Blaekwell;2011.KenyonLK,DoleRL,KellySP.Perspectivesofacademicfacultyandclinicalinstructorsonentry-levelPTpreparationforpediatricphysicaltherapypractice.2013;93(12):1661-1672.KoganJRandHolmboeES.RealizingthePromiseandImportanceofPerformance-basedAssessment.TeachLearnMed2013;25Suppl1:S68-74.LopopoloRB,SchaferDS,NosseLJ.Leadership,administration,management,andprofessionalism(LAMP)inphysicaltherapy:aDelphistudy.PhysicalTherapy.February2004;84(2):137-150.MathwigK,ClarkeF,OwensT,GrametP.Selectioncriteriaforemploymentofentry-levelphysicaltherapists:asurveyofNewYorkStateemployers.JournalofPhysicalTherapyEducation.2001;15(1):65-74.MayW,etal.Studentgenericabilitiesself-assessment.JournalofPhysicalTherapyEducation.1995;Neal,Ed."DukeAHEAD."Assessment.DukeUniversityHealthSystems,n.d.Web.20Sep.2015.https://dukeahead.duke.edu/educator-competencies/assessmentPetersonEB,CalhounAW,RiderEA.ThereliabilityofamodifiedKalamazooConsensusStatementChecklistforassessingthecommunicationskillsofmultidisciplinarycliniciansinthesimulatedenvironment.PatientEducationandCounseling.2014;96:411–418.RapportMJ,FurzeJ,MartinK,SchreiberJ,DannemillerLA,DibiasioPA,MoerchenVA.Essentialcompetenciesinentry-levelpediatricphysicaltherapyeducation.PediatrPhysTher.2014;26:7-18.Roach,KE,FrostJS,FrancisNJ,GilesS,NordrumJTetal.Validationoftherevisedphysicaltherapistclinicalperformanceinstrument(PTCPI):Version2006.PhysTher.2012;416-428.RouseLE.Introductiontothe2011–12ADEAAnnualProceedings.JDentEduc.2012;76:821–955.SchuwirthLWT,VanderVleutenCPM.Programmaticassessment:Fromassessmentoflearningtoassessmentforlearning.MedTeach.2011;33:478-85.
ShahN,DesaiC,JorwekarG,BadyalD,andSinghT.Competency-basedmedicaleducation:Anoverviewandapplicationinpharmacology.IndianJPharmacol.2016Oct;48(Suppl1):S5–S9.
97
Page 99
SomaM,HosoiT,YaedaJ.ExploringhighpriorityresearchquestionsinphysicaltherapyusingtheDelphistudy.JPhysTherSei.2009:21:367-371.SullivanRL.1995.TheCompetency-BasedApproachtoTraining.StrategyPaperNo1.JHPIEGOCorporation:Baltimore,Maryland.TenCateO.ScheeleF.Competency-basedpostgraduatetraining:Canwebridgethegapbetweentheoryandclinicalpractice?AcadMed.2007June;82(6):542–547.TenCateO.Nutsandboltsofentrustableprofessionalactivities.JGradMedEduc.2013;5:157-158.BarrJS,GwyerJ,TalmorZ.Standardsforclinicaleducationinphysicaltherapy:amanualforevaluationandselectionofclinicaleducationcenters.Washington,DC:AmericanPhysicalTherapyAssociation;1981.WongR,AversD,BarrJ,CiolekC,KlimaD,ThompsonM.Essentialcompetenciesinthecareofolderadultsatthecompletionoftheentry-levelphysicaltherapistprofessionalprogramofstudy.AcademyofGeriatricPhysicalTherapyWebsite.https://www.geriatricspt.org/about-academy-geriatrics-physical-therapy/essential-competencies.cfm.Pub.2011.AccessedDec.2016.ZarifsanaieyN,AminiM,SaadatF.Acomparisonofeducationalstrategiesfortheacquisitionofnursingstudent’sperformanceandcriticalthinking:simulation-basedtrainingvs.integratedtraining(simulationandcriticalthinkingstrategies).BMCMedicalEducation.2016;16:294.ZhuX,YangL,LinP,etal.AssessingNursingstudents’clinicalcompetenciesusingaproblem-focusedobjectivestructuredclinicalexamination.WesternJournalofNursingResearch.2017;39(3):388-399.
98
Page 100
TABLES
Table1.TotalResponsesbyRound
Round1 Round2 Round3 Round4SurveysDelivered 147 132 132 132
ReturnRate 88.4% 79.55% 78.79% 78.79%ClinicalInstructor 20 20 23 24AcademicFaculty 34 32 30 32
DCE/ACCE 27 27 25 25RecentGraduates 31 26 26 23
99
Page 101
Table2.RespondentDemographics
ClinicalInstructors AcademicFaculty DCEs RecentGraduatesTotalRespondents: 20
6male34
10male27
2male31
9maleAverageAge: 38 54 52 26
AverageYearsofExperience:
11-15(asaclinician)
16(asafaculty)
11(asaDCE/ACCE)
<1year(asaclinician)
Entry-LevelPTDegree:Certificate
BSMPTDPT
03143
319100
01881
00031
PracticeSetting:Acutecare
HealthSystemPrivatePracticeSNF/ECF/ICF
AcademicInstitutionHomeHealth
648110
0000340
1000260
**7017301
Practice/ProgramLocation:Urban
SuburbanRural
875
2283
15102
18112
Practice/ProgramRegion:SAtlantic
MidAtlanticE.N.CentralW.N.CentralW.S.CentralNewEngland
PacificE.S.CentralMountain
213611033
546305433
534522312
343815322
ABPTSSpecialization:GCSOCSSCSNCSCVSPCS
221000
180600
440313
NA
CICertified:APTAOther
182
149
2412
NA
DCE,DirectorofClinicalEducation;ACCE.AcademicCoordinatorofClinicalEducation;ABPTS,AmericanBoardofPhysicalTherapySpecialties*Presentedasrangeofyears**Practicesettingwhererecentgraduatescompletedtheirfirstfull-timeclinicalexperience
100
Page 102
Table3.DPTProgramClinicalExperience(CE)Information
AcademicFaculty DCE/ACCEs RecentGraduatesAverageNumberofCEs 4 4 4AveragetotalweeksofCE 37(24-54) 36(34-43) 36(28-54)Numberofweeksin1stCE - - 71stCEfollowscompletionofalldidacticcoursework
9 1 Notasked
Timingof1stCE: Middleofthe1styear 0 1
Endofthe1styear 19 13 Beginningofthe2ndyear 5 5
Middleofthe2ndyear 4 2 NotAskedEndofthe2ndyear 3 4
Beginningofthe3rdyear 1 0 Middleofthe3rdyear 1 0
Endofthe3rdyear 0 1 PreferredSettingfor1stCE
AcuteCare 4 7*Outpatient Notasked 8 17*
Rehabilitation 3 0*Pediatrics 1 3*
HomeCare 2 1*
*Newgraduatesreportedonthesettingwheretheir1stCEwascompleted.
101
Page 103
Table4.ThemesandElementsDerivedfromEachRoundofDataAnalysis
*Themesaretitledfromthefirstround.Somethemesmayhavebeenreworded,oritemscondensedorredistributedinfuturerounds.
**Aselementsarenotlisted,severalthemesmayappearincomplete,asthelistedelementsarenotprovidedhere.
RetainedElementsbyRoundTheme* Round
1Round
2Round3 Round4
1.Studentsshouldhavefoundationalknowledgetosupportapplicationandsynthesisinthefollowingcontentareas:** 17 9 5 5
2.Studentsshouldmeetthespecificprogramidentifiedandcurricularrequirements 6 6 4 3
3.Studentsshouldtakeinitiativetoapplyevidence-basedpracticestrategies 8 8 4 4
4.Studentsshouldengageinself-assessment 10 6 4 45.Studentsshouldutilizeconstructivefeedback 3 3 3 36.Studentsshoulddemonstrateeffectivecommunicationabilities 4 3 3 3
7.Studentsshouldexhibiteffectiveverbal,non-verbalandwrittencommunicationabilities 15 14 10 10
8.Studentsshouldbepreparedtoengageinthelearningprocess 17 17 14 14
9.Studentsshouldbefamiliarwithelectronicmedicalrecords 1 0 0 010.Studentsshouldcompletedocumentationinaconcisefashion 1 0 0 0
11.Studentsshouldcompletedocumentationinatimelyfashion 1 0 0 0
12.Studentsshoulddevelopthefollowingelementsincludingthedocumentationof 8 10 3 3
13.Studentsshouldgatherrelevantinformationfromachartreview 1 0 0 0
14.Studentsshouldunderstandconceptsrelatedtobilling 1 0 0 015.Studentsshouldrecognizeandaddressissuesrelatedtosafepractice 19 8 8 8
16.Studentsshouldapplyclinicalreasoningandproblemsolving 6 0 0 0
17.Studentsshoulddesignexamination,evaluation,intervention,planofcareandoutcomeassessmentprocesses 10 10 6 6
18.Studentsshouldhavetheunderstandingandskilltoperformthefollowingexaminationskills:** 27 24 16 16
19.Studentsshouldhavetheunderstandingandskilltoperformthefollowinginterventions:** 18 9 6 6
20.Studentsshouldrecognizeandfollowspecificprofessionalstandards 20 12 10 10
TotalRetainedElements 193 139 95 95
102
Page 104
Table5.DefinitionsoflevelsofproficiencyLevel Definition
Familiarity Thestudenthasbasicknowledgeofthematerial/skill/behaviorandwillrequireguidancetoapplyitappropriatelyintheclinicalsetting.
EmergingThestudentunderstandshowtoapplythematerial/skill/behaviorsafelyandconsistentlyinsimplesituationsandwillrequireguidancetoapplytheconceptorperformthetaskinmorecomplexsituations.
ProficientThestudentcanintegratetheknowledge/skill/behaviorsafelyandindependentlyinall(simpleandcomplex)clinicalsituations.Thestudentisabletoidentifytheneedforguidanceappropriately.
Table6.Elementsachieving>80%consensusrequiringproficiencypriortothefirstfull-timeclinicalexperience
Element ClinicalInstructors
AcademicFaculty
DCEs/ACCEs
RecentGraduates
OverallPercent
ConsensusAchieveminimumGPA
MeetMinimumexpectationsforpracticalexaminations
N/A*
Remediationofanyandallsafetyconcerns
Demonstratepolite,personable,engagingandfriendlybehaviors
81.82 82.76 68.18 90.48 80.85
Introduceone’sselftoCI,clinicalstaff,andpatients
73.73 93.10 90.91 76.19 84.04
Respectforpatients,peers,healthcareprofessionalsand
community
80.95 75.86 77.27 90.00 80.43
Punctualitywithallassignments 80.95 100.00 95.45 95.24 93.55UnderstandingofHIPAA
regulations78.95 89.66 77.27 90.00 84.44
Appropriatedresscode 84.21 93.10 100.00 95.00 93.33*ThefirstthreeitemsaremarkedN/Aastheyachieved>80%consensusthattheyarerequiredpriortothefirstfull-timeclinicalexperience,butthedichotomousnatureoftheseelementsdoesnotrelatetoaratingoflevelofproficiency.
103
Page 105
Table7.Consensusregardingassessmentmethodsforthemes*,**Themes
Thestudentshould:
Satisfactoryacademicperforman
ce
WrittenExaminatio
n
PracticalExamination(skillscheck)
Simulated
practiceexam(OSCE)
OralExam
SuccessfulICE
Facultyassessme
nt
Self-assessme
nt
1.Havefoundationalknowledgetosupportapplicationandsynthesisinthefollowingcontentareas…
89.58
87.50
88.54
62.50
28.13
45.83
53.13
40.63
2.Meetthespecificprogramidentifiedcurricularrequirementsincluding:GPA,remediationofsafetyconcerns,passallpracticalexams
3.Takeinitiativetoapplyevidence-basedstrategies…
88.42 77.89 70.53 58.95 33.68 53.68 47.37 40.00
4.Engageinself-assessment 67.37 22.11 26.32 38.95 20.00 49.47 91.58 90.53
5.Utilizeconstructivefeedback 50.00 10.64 36.17 41.49 20.21 55.32 91.49 88.30
6.Demonstrateeffectivecommunicationabilitieswithinthefollowinggroups…
44.68 17.02 38.30 54.26 34.04 63.83 79.79 69.15
7.Exhibiteffectiveverbal,non-verbalandwrittencommunicationabilitiesto…
42.55 19.15 56.38 68.09 34.04 70.21 90.43 80.85
8.Bepreparedtoengageinlearningthroughdemonstrating…
47.78 18.89 42.22 52.22 22.22 65.56 96.67 88.89
9.Beabletodocumentexamination/re-examination(History,systemsreview,testsandmeasures,problemlist,anddailyinterventions)
71.74 80.43 50.00 59.78 10.87 58.70 29.35 23.91
10.Recognizeandaddressissuesrelatedtosafepatientcareincludingtheabilityto…
69.57 54.35 93.48 72.83 22.83 65.22 43.48 35.87
11.Demonstratethefollowingclinicalreasoningskillsforanon-complexpatient
75.56 84.44 84.44 74.44 27.78 64.44 35.56 25.56
NotQueriedforrecommendationassessmentasmethodologyisintrinsictothetheme/items
104
Page 106
12.HaveBOTHtheunderstandingandskilltoperformthefollowingexaminationskills
75.56 83.33 98.89 76.67 23.33 57.78 30.00 23.33
13.Havetheunderstandingandskilltoperformthefollowinginterventions
71.91 74.16 93.26 74.16 23.60 61.80 33.71 24.72
14.Recognizeandfollowspecificprofessionalstandards…
71.59 71.59 37.50 39.77 20.45 55.68 82.95 75.00
*Datapresentedattheoverallpercentageofrespondentsinagreementwiththemethodofassessmentforeachtheme.
**Datainboldindicated≥80%agreementwiththemethodofassessmentforthegiventheme.OSCE:Objectivestructuredclinicalexamination;ICE:Integratedclinicalexperience
105
Page 107
AppendixA:Elementsreachingconsensusbytheme
Overall
Consensus*
Familiarity**
Emerging**
Proficientgreenfillisover80
Emerging&Proficientboxesareinpinkareover80%
1.Studentsshouldhavefoundationalknowledgetosupportapplicationandsynthesisinthefollowingcontentareas:
Anatomy(i.e.functionalanatomy)
100
OverallFaculty
DCEClinicians
NewGrads
3.130
13.6400
33.3332.2636.3636.3628.57
63.5467.74
5063.6471.43
96.87100
86.36100100
Commondiagnosesrelatedtosystemsreview(e.g.medical,physicaltherapy
95.1
OverallFaculty
DCEClinicians
NewGrads
18.756.45
36.3622.7314.29
58.3364.5245.4559.0961.9
22.9229.0318.1818.1823.81
81.2593.5563.6377.2785.71
Kinesiology(i.e.biomechanics,exercisescience,movementscience)
99.02
OverallFaculty
DCEClinicians
NewGrads
9.380
22.7318.18
0
54.1754.8445.4554.5561.9
36.4645.1631.8227.2738.1
90.63100
77.2781.82100
Physiology/Pathophysiology(relatedtogeneralsystemsreview)
92.16
OverallFaculty
DCEClinicians
NewGrads
16.6727.279.68
13.6419.05
52.0850
48.3963.6447.62
31.2522.7341.9422.7333.33
83.3372.7390.3386.3780.95
Tissuemechanics(e.g.stagesofhealing,use/disuse,load/overload)
92
OverallFaculty
DCEClinicians
NewGrads
15.633.23
27.2731.829.52
41.6738.71
5040.9147.62
42.7158.0622.7327.2742.86
84.3896.7772.7368.1890.48
2.Studentsshouldmeetthespecificprogramidentifiedcurricularrequirementsincluding:
achieveminimumGPA
85.29
OverallFaculty
DCEClinicians
NewGrads
NA NA NA
meetminimumexpectationsforpracticalexaminations
98.04
OverallFaculty
DCEClinicians
NewGrads
NA NA NA
remediationofanyandallsafetyconcerns
OverallFaculty
NA NA NA
106
Page 108
98.04 DCEClinicians
NewGrads3.Studentsshouldtakeinitiativetoapplyevidence-basedstrategiesto:
generateinterventionsideas
88.35
OverallFaculty
DCEClinicians
NewGrads
25.266.67
36.3640.9123.81
70.5386.6759.0959.0971.43
4.216.674.55
04.76
74.7493.3463.6459.0976.19
guidedecision-making
86.45
OverallFaculty
DCEClinicians
NewGrads
26.326.67
45.4531.8228.57
67.3783.33
5063.6466.67
6.3210
4.554.554.76
73.6993.3354.5568.1971.43
measureoutcomes
88.35
OverallFaculty
DCEClinicians
NewGrads
28.4213.3340.9140.9123.81
58.9573.3354.5545.4557.14
12.6313.334.55
13.6419.05
71.5886.6659.1
59.0976.19
researchunfamiliarinformationorconditions
95.14
OverallFaculty
DCEClinicians
NewGrads
16.8410
27.2718.1814.29
49.976045.45
54.5533.33
33.6830
27.2727.2752.38
83.1590
72.7281.8285.71
4.Studentsshouldengageinself-assessmentincluding:
self-assessmentoftheimpactofone’sbehaviorsonothers
95.1
OverallFaculty
DCEClinicians
NewGrads
7.376.679.094.559.52
53.6850
72.7345.4547.62
38.9543.339.0950
42.86
92.6393.3381.8295.4590.48
theunderstandingofone’sownthoughtprocesses(metacognition)
88.11
OverallFaculty
DCEClinicians
NewGrads
12.6316.6718.189.094.76
70.5373.3372.7359.0976.19
16.8410
9.0931.8219.05
87.3783.3381.8290.9195.24
self-reflectionandidentificationofareasofstrengthandthoseneedingimprovement,developmentofaplantoimprove,anddiscussionofthat
planwithinstructors
93.13
OverallFaculty
DCEClinicians
NewGrads
9.476.67
18.184.559.52
62.1163.3363.6472.7347.62
28.4230
18.1822.7342.86
90.5393.3381.8295.4690.48
seekingoutresources,includingsupportfromotherswhenneeded,toassistinimplementationoftheplan
96.08
OverallFaculty
DCEClinicians
NewGrads
7.376.67
13.644.559.52
55.7950
68.1863.6442.86
36.8443.3318.1831.8252.38
92.6393.3386.3695.4695.24
5.Studentsshouldutilizeconstructivefeedbackby:
beingopenandreceptive, Overall 0 31.91 68.09 100
107
Page 109
verbally/non-verbally 99.03
FacultyDCE
CliniciansNewGrads
0000
31.0345.4531.8219.05
68.9754.5568.1880.95
100100100100
implementingactionstoaddressissuespromptly
99.03
OverallFaculty
DCEClinicians
NewGrads
2.150
4.5505
52.6958.62
505050
45.1641.3845.45
5045
97.85100
95.4510095
reflectingonfeedbackprovided
98.04
OverallFaculty
DCEClinicians
NewGrads
1.080
4.5500
48.3944.8368.1831.82
50
50.5455.1727.2768.18
50
98.93100
95.45100100
6.Studentsshoulddemonstrateeffectivecommunicationabilitieswithinthefollowinggroups:
diversepatientpopulations
80.39
OverallFaculty
DCEClinicians
NewGrads
31.9124.2445.4531.8228.57
58.5168.9745.4554.5561.9
9.576.9
9.0913.649.52
68.0875.8754.5468.1971.42
familiesandotherindividualsimportanttothepatients
82.35
OverallFaculty
DCEClinicians
NewGrads
29.7917.2445.4540.9119.05
57.4575.8645.4545.4557.14
12.776.9
9.0913.6423.81
70.2282.7654.5459.0980.95
healthcareprofessionals
83.34
OverallFaculty
DCEClinicians
NewGrads
29.7917.2445.4531.8228.57
62.7779.31
5059.0957.14
7.453.454.559.09
23.81
70.2282.7654.5568.1880.95
7.Studentsshouldexhibiteffectiveverbal,non-verbalandwrittencommunicationabilitiesto:
listenactively
99.03
OverallFaculty
DCEClinicians
NewGrads
00000
42.5555.1740.9140.9128.57
57.4544.8359.0959.0971.43
100100100100100
demonstratepolite,personable,engagingandfriendlybehaviors
97.09
OverallFaculty
DCEClinicians
NewGrads
00000
19.1517.2431.8218.189.52
80.8582.7668.1881.8290.48
100100100100100
independentlyseekinformationfromappropriatesources
83.49
OverallFaculty
DCEClinicians
NewGrads
7.453.454.55
13.649.52
60.6451.7272.7359.0961.9
31.9144.8322.7327.2728.57
92.5596.5595.4686.3690.47
108
Page 110
buildrapport
94.18
OverallFaculty
DCEClinicians
NewGrads
5.320
9.099.094.76
69.1589.6654.5563.6461.9
25.5310.3436.3627.2733.33
94.68100
90.9190.9195.23
seekassistancewhenneeded
100
OverallFaculty
DCEClinicians
NewGrads
1.063.45
000
26.624.1445.4522.7314.29
72.3472,4154.5577.2785.71
98.9496.55100100100
engageinshareddecision-makingwithpatients
82.35
OverallFaculty
DCEClinicians
NewGrads
25.8114.29
5022.7319.05
66.6782.1440.9168.1871.43
7.533.579.099.099.52
74.285.71
5077.2780.95
demonstratealevelofcomfortandrespectwithpatienthandling
82.52
OverallFaculty
DCEClinicians
NewGrads
20.2113.7918.1827.2723.81
59.5772.4154.5554.5552.38
20.2113.7927.2718.1823.81
79.7886.2
81.8272.7376.19
demonstrateempathy
95.14
OverallFaculty
DCEClinicians
NewGrads
1.06000
4.76
48.9465.5254.55
5019.05
5034.4845.45
5076.19
98.94100100100
95.24uselanguageandterminologyappropriatefortheaudience
90.29
OverallFaculty
DCEClinicians
NewGrads
11.830
19.0513.6419.05
69.8968.9761.9
72.7376.19
18.2831.0319.0513.644.76
88.17100
80.9586.3780.95
introduceone’sselftoCI,clinicalstaff,andpatients
97.09
OverallFaculty
DCEClinicians
NewGrads
1.0600
4.550
14.896.9
9.0922.7323.81
84.0493.1
90.9172.7376.19
98.93100100
95.46100
8.Studentsshouldbepreparedtoengageinlearningthroughdemonstrating:
accountabilityforactionsandbehaviors
98.05
OverallFaculty
DCEClinicians
NewGrads
3.2600
14.290
35.8739.29
5014.2938.1
60.8760.71
5071.4361.9
96.74100100
85.72100
resilience/perseverance
82.52
OverallFaculty
DCEClinicians
NewGrads
11.836.9
18.1819.054.76
46.2448.2845.4542.8647.62
41.9444.8336.3638.1
47.62
88.1893.1181.8180.9695.24
culturalcompetenceandsensitivity
OverallFaculty
16.310.34
54.3572.41
29.3517.24
83.789.65
109
Page 111
90.29 DCEClinicians
NewGrads
18.1825
14.29
45.4545
47.62
36.3630
38.1
81.8175
85.72aneager,optimisticandmotivatedattitude
94.18
OverallFaculty
DCEClinicians
NewGrads
3.2300
4.769.52
21.5120.6936.3619.059.52
75.2779.3163.6476.1980.95
96.78100100
95.2490.47
respectforpatients,peers,healthcareprofessionalsandcommunity
98.05
OverallFaculty
DCEClinicians
NewGrads
1.0900
4.760
18.4824.1422.7314.29
10
80.4375.8677.2780.95
90
98.91100100
95.24100
open-mindednesstoalternativeideas
94.17
OverallFaculty
DCEClinicians
NewGrads
3.230
9.094.76
0
45.1644.8340.9142.8652.38
51.6155.17
5052.3847.62
96.77100
90.9195.24100
punctualitywithallassignments
98.06
OverallFaculty
DCEClinicians
NewGrads
1.0800
4.760
5.380
4.5514.294.76
93.55100
95.4580.9595.24
98.93100100
95.24100
self-caretomanagestress
80.58
OverallFaculty
DCEClinicians
NewGrads
9.680
13.6414.2914.29
58.0668.9740.9157.1461.9
32.2631.0345.4528.5723.81
90.32100
86.3685.7185.71
responsibilityforlearning
97.09
OverallFaculty
DCEClinicians
NewGrads
2.150
4.554.76
0
27.9624.1427.2723.8138.1
69.8975.8668.1871.4361.9
97.85100
95.4595.24100
self-organization
89.32
OverallFaculty
DCEClinicians
NewGrads
4.30
4.559.524.76
56.9951.7254.5561.961.9
38.7148.2840.9128.5733.33
95.7100
95.4690.4795.23
takingactiontochangewhenneeded
91.26
OverallFaculty
DCEClinicians
NewGrads
9.780
22.739.529.52
45.6557.1440.9133.3347.62
44.5742.8636.3657.1442.86
90.22100
77.2790.4790.48
willingnesstoadapttonewandchangingsituations
93.14
OverallFaculty
DCEClinicians
NewGrads
8.63.45
13.649.529.52
43.0144.8340.9142.8642.68
48.3951.7245.4547.6247.62
91.496.5586.3690.4890.48
appropriateworkethic
OverallFaculty
1.080
21.5127.59
77.4272.41
98.93100
110
Page 112
97.08 DCEClinicians
NewGrads
04.76
0
31.829.52
14.29
68.1885.7185.71
10095.23100
maturityduringdifficultorawkwardsituationswithpatients,familiesandhealthcareprofessionals
84.47
OverallFaculty
DCEClinicians
NewGrads
11.8310.3413.6414.299.52
53.7665.5259.0928.5757.14
34.4124.1427.0757.1433.33
88.1789.6686.1685.7190.47
9.Studentsshoulddevelopthefollowingelementsincludingthedocumentationof:
examination/re-examination(History,systemsreview,andtestsandmeasures)
89.32
OverallFaculty
DCEClinicians
NewGrads
28.2620.6931.82
4519.05
63.0468.9754.55
4580.95
8.710.3413.64
100
71.7479.3168.19
5580.95
establishanddocumenttheproblemlist
84.46
OverallFaculty
DCEClinicians
NewGrads
30.4320.6931.82
4528.57
59.7868.97
5050
66.67
9.7810.3418.18
54.76
69.5679.3168.18
5571.43
dailyinterventions
93.13
OverallFaculty
DCEClinicians
NewGrads
26.0917.2427.27
4519.05
57.6165.52
5040
71.43
16.317.2422.73
159.52
73.9182.7672.73
5580.95
10.Studentshouldrecognizeandaddressissuesrelatedtosafepatientcareincludingtheabilityto:
identifycontraindicationsandprecautions
98.06
OverallFaculty
DCEClinicians
NewGrads
13.040
18.18309.52
45.6562.0740.91
3042.86
41.337.9340.9147.62
86.95100
81.8270
90.48assessandmonitorvitalsigns
99.03
OverallFaculty
DCEClinicians
NewGrads
7.613.454.5515
9.52
32.6127.5936.36
3533.33
59.7868.9759.09
5057.14
92.3996.5695.45
8590.47
identifyandrespondtophysiologicchanges
95.14
OverallFaculty
DCEClinicians
NewGrads
20.656.9
27.2735
19.05
60.8775.86
5060
52.38
18.4817.2422.73
528.57
79.3593.1
72.7365
80.95assesstheenvironmentforsafety,includinglines,tubes,andotherequipment
91.26
OverallFaculty
DCEClinicians
NewGrads
21.7413.7922.73
3023.81
51.0951.7259.09
5042.86
27.1734.4818.18
2033.33
78.2686.2
77.2770
76.19appropriatelyapplyinfectioncontrol Overall 11.96 33.7 54.35 88.05
111
Page 113
proceduresincludinguniversalprecautions
97.09
FacultyDCE
CliniciansNewGrads
6.913.64
1019.05
27.5922.73
4542.86
65.5263.64
4538.1
93.1186.37
9080.96
provideassistanceandguardingforpatientsafety
99.03
OverallFaculty
DCEClinicians
NewGrads
10.876.9
13.6415
9.52
43.4837.9336.36
5547.62
45.6555.17
5030
42.86
89.1393.1
86.3685
90.48utilizeappropriatebodymechanicstoavoidinjurytoselforpatients
98.06
OverallFaculty
DCEClinicians
NewGrads
10.873.45
13.6415
14.29
47.8341.3845.45
6047.62
41.355.1740.91
2538.1
89.1396.5586.36
8585.72
provideappropriatedrapingduringpatientcareactivities
99.03
OverallFaculty
DCEClinicians
NewGrads
8.76.9
4.5515
9.52
29.3520.6931.82
3038.1
61.9672.4163.64
5552.38
91.3193.1
95.4685
90.4811.Studentshoulddemonstratethefollowingclinicalreasoningskillsforanon-complexpatient:
utilizetheelementsofthepatient-clientmanagementmodelincluding:addressvariousbodysystems(cardiopulmonary,integumentary,musculoskeletal,neuromuscular)duringtheexamination
88.35
OverallFaculty
DCEClinicians
NewGrads
27.4724.1436.36
3515
63.7465.5254.55
6570
8.7910.349.09
015
72.5375.8663.64
6585
articulateaclinicalrationaleinpatientevaluation
84.46
OverallFaculty
DCEClinicians
NewGrads
35.1620.6945.45
5030
59.3472.4145.45
5065
5.496.9
9.0905
64.8379.3154.545070
developgoalsthatarelinkedtothepatient’sactivitylimitationsandparticipationrestrictions
82.53
OverallFaculty
DCEClinicians
NewGrads
32.2224.1438.15020
62.2268.9752.38
5075
5.566.9
9.5205
67.7875.8761.95080
determineappropriatenessfortherapywithinscopeofPTpractice
82.36
OverallFaculty
DCEClinicians
NewGrads
27.4717.2440.91
4015
59.3465.52
505070
13.9117.249.091015
72.5382.7659.09
6085
interpretexaminationfindings
82.52
OverallFaculty
DCEClinicians
NewGrads
29.6720.6940.91
4020
65.9375.86
506075
4.43.459.09
05
70.3379.3159.09
6080
screentorulein/outconditionsand Overall 32.97 58.24 8.79 67.03
112
Page 114
concerns 89.21
FacultyDCE
CliniciansNewGrads
24.1436.36
5025
65.52504570
10.3413.64
55
75.8663.64
5075
12.StudentshouldhaveBOTHtheunderstandingandskilltoperformthefollowingexaminationskills:
balanceassessment
87.25
OverallFaculty
DCEClinicians
NewGrads
38.4641.3845.45
4025
50.5541.3845.45
5565
10.9917.249.09
510
61.5458.6254.54
6075
chartreviewtoextractrelevanthistory
93.2
OverallFaculty
DCEClinicians
NewGrads
26.3713.7927.27
3040
52.7558.6245.45
5550
20.8827.5927.27
1510
73.6386.2172.72
7060
dermatomescreening
94.18
OverallFaculty
DCEClinicians
NewGrads
21.9813.7922.73
3025
35.1634.4836.36
3040
42.8651.7240.91
4035
78.0286.2
77.277075
functionalmobilityassessment
100
OverallFaculty
DCEClinicians
NewGrads
27.4727.5922.73
3525
52.7544.8359.09
5060
19.7827.5918.18
1515
72.5372.4277.27
6575
gaitassessment
92.23
OverallFaculty
DCEClinicians
NewGrads
29.6724.1427.27
4030
54.9551.7254.55
5065
15.3824.2418.18
105
70.3375.8672.73
6070
goniometry
99.03
OverallFaculty
DCEClinicians
NewGrads
8.793.45
18.18105
32.9727.5931.82
3540
58.2468.97
505555
91.2196.5681.82
9095
interview/historytaking
98.06
OverallFaculty
DCEClinicians
NewGrads
15.386.9
22.732015
60.4465.5245.457060
24.1827.5931.82
1025
84.6293.1177.27
8085
lowerquadrantscreening
87.38
OverallFaculty
DCEClinicians
NewGrads
21.9820.6922.73
2025
46.1537.9354.55
4550
31.8741.3822.73
3525
78.0279.3177.28
8075
manualmuscletesting
98.06
OverallFaculty
DCE
8.793.45
18.18
39.5641.3836.36
51.6555.1745.45
91.2196.5581.81
113
Page 115
CliniciansNewGrads
105
4040
5055
9095
musclelengthtesting
88.24
OverallFaculty
DCEClinicians
NewGrads
15.383.45
18.182025
42.8637.9340.91
4550
41.7658.6240.91
3525
84.6296.5581.82
8075
myotomescreening
92.23
OverallFaculty
DCEClinicians
NewGrads
18.6813.7918.18
3015
39.5634.4840.91
3055
41.7651.7240.91
4030
81.3286.2
81.827085
reflextesting
84.47
OverallFaculty
DCEClinicians
NewGrads
16.4813.7918.18
2015
38.4637.9345.45
2545
45.0551.7236.36
4545
83.5189.6581.81
7090
sensoryexamination
97.06
OverallFaculty
DCEClinicians
NewGrads
16.4810.3418.18
3010
41.7641.3845.45
3545
41.7644.8336.36
4540
83.5286.2181.81
8085
medicalscreeningforredflags
90.29
OverallFaculty
DCEClinicians
NewGrads
20.8820.6918.18
2025
47.2551.7245.45
4545
31.8727.5936.36
3530
79.1279.3181.81
8075
systemsreview
92.23
OverallFaculty
DCEClinicians
NewGrads
24.1820.6918.18
3030
47.2551.7245.45
4050
28.5727.5936.36
3020
75.8279.3181.81
7070
upperquadrantscreening
85.44
OverallFaculty
DCEClinicians
NewGrads
25.5624.1423.81
2530
42.2234.4852.38
4045
32.2241.3823.81
3525
74.4475.8676.19
7570
13.Studentshouldhavetheunderstandingandskilltoperformthefollowinginterventions:
prescribe,fit,andinstructpatientsinproperuseofassistivedevices
87.38
OverallFaculty
93.21DCEClinicians
NewGrads
27.7820.6927.2736.84
30
48.8955.1731.8252.63
55
23.3324.1440.9110.53
15
72.2279.3172.7363.16
70functionaltraining(includingbedmobility,transfers,andgait)withappropriateguardingandassistance
93.21
OverallFaculty
DCEClinicians
NewGrads
22.2213.7931.8226.32
20
55.5658.6236.3652.63
75
22.2227.5931.8221.05
5
77.7886.2168.1873.68
80
114
Page 116
individualizedpatienteducation
86.41
OverallFaculty
DCEClinicians
NewGrads
3013.7940.9147.37
25
57.7862.07
5047.37
70
12.2224.149.095.26
5
7086.2159.0952.63
75therapeuticexercise:specificallystrengthening
95.14
OverallFaculty
DCEClinicians
NewGrads
23.3310.3431.8247.37
10
54.4455.1745.4542.11
75
22.2234.4822.7310.53
15
76.6689.6568.1852.64
90therapeuticexercise:specificallystretching
94.18
OverallFaculty
DCEClinicians
NewGrads
23.3310.3431.8247.37
10
53.3355.1745.4536.84
75
23.3334.4822.7315.79
15
76.6689.6528.1852.63
90therapeuticexercise:specificallyaerobicexercise
89.32
OverallFaculty
DCEClinicians
NewGrads
24.4410.3431.8252.63
10
54.4455.1745.4536.84
80
21.1134.4822.7310.53
10
75.5589.6568.1852.63
9014.Studentshouldrecognizeandfollowspecificprofessionalstandards,including:
appropriatedresscode
100
OverallFaculty
DCEClinicians
NewGrads
1.1100
5.260
5.566.90
10.535
93.3393.1100
84.2195
98.89100100
94.74100
corevaluesidentifiedbytheAPTAasaccountability,altruism,compassion/caring,excellence,integrity,professionalduty,andsocialresponsibility
92.08
OverallFaculty
DCEClinicians
NewGrads
4.493.454.555.56
5
32.5841.3845.4511.11
25
62.9255.17
5083.33
70
95.596.5595.4594.44
95clinicalexpectationsspecifictosetting
90.3
OverallFaculty
DCEClinicians
NewGrads
8.896.9
9.0915.79
5
37.7837.9336.3615.79
60
53.3355.1754.5568.42
35
91.1193.1
90.9184.21
95HIPAAregulations
98.06
OverallFaculty
DCEClinicians
NewGrads
4.446.90
10.530
11.113.45
22.7310.53
10
84.4489.6677.2778.95
90
95.5593.11100
89.48100
legalaspectsrelatedtopatientcare
86.41
OverallFaculty
DCEClinicians
NewGrads
13.3310.349.09
15.7920
45.5655.17
5026.32
45
41.1134.4840.9157.89
35
86.6789.6590.9184.21
80obligationsofthepatient-providerrelationship
OverallFaculty
14.4410.34
4055.17
45.5634.48
85.5689.65
115
Page 117
91.17 DCEClinicians
NewGrads
4.5521.05
20
31.8215.79
30
63.6463.16
50
95.4678.95
80passionfortheprofession
87.38
OverallFaculty
DCEClinicians
NewGrads
5.563.454.55
10.535
23.3327.5931.8215.79
30
71.1168.9763.6473.68
80
94.4496.5695.4689.47
95patientrights
98.05
OverallFaculty
DCEClinicians
NewGrads
6.673.459.09
00
41.1155.1736.3610.53
55
52.2241.3854.5573.68
45
93.3396.5590.9184.21100
maintainingprofessionalboundaries
93.2
OverallFaculty
DCEClinicians
NewGrads
3.333.459.09
00
33.3351.7231.8221.05
20
63.3344.8359.0978.95
80
96.6696.5590.91100100
understandingphysicaltherapy'sroleinthehealthcaresystem
92.23
OverallFaculty
DCEClinicians
NewGrads
8.896.9
9.0910.53
10
6075.8663.6436.84
55
31.1117.2427.2752.63
35
91.1193.1
90.9189.47
90
116
Page 118
AppendixB:Elementsnotreachingconsensusbytheme:Theme Overall
Consensus*1. Studentsshouldhavefoundationalknowledgetosupportapplication
andsynthesisinthefollowingcontentareas:
Pharmacology(e.g.commonclassifications,sideeffects,impactontreatment,polypharmacology)
78.66
2. Studentsshouldmeetthespecificprogramidentifiedcurricularrequirementsincluding:
Participate,asaphysicaltherapiststudent,insomeclinicalexperience(includingbutnotlimitedto:integratedclinicalexperiences,part-timeclinicalexperiences)priortothefirstfull-timeclinicalexperience
70.87
3. Studentsshouldtakeinitiativetoapplyevidence-basedstrategiesto: Determinerelevanceofevidenceforspecificpatients 75.96 Establishefficacyofinterventionsforpatients,payers,otherhealthcare
professionals73.46
Find,evaluate,andsynthesizetheliterature 70.19 Applyconceptsrelatedtohealthpolicyandhealthservices 37.54. Studentsshouldengageinself-assessmentincluding: Demonstrationofconfidenceinlearnedmaterial 79.41 Demonstrationofconfidenceworkingwithrelevantindividuals 72.815. Studentsshouldutilizeconstructivefeedbackby: AllelementsreachedConsensus 6. Studentsshoulddemonstrateeffectivecommunicationabilitieswithin
thefollowinggroups:
AllelementsreachedConsensus 7. Studentsshouldexhibiteffectiveverbal,non-verbalandwritten
communicationabilitiesto:
ApplyStrategiestofacilitatepatientadherence 66.35 Interpretpatientcuesthatrequireachangeincommunicationstrategy 77.88 Resolveconflict 70.198. Studentsshouldbepreparedtoengageinlearningthrough
demonstrating:
Commitmenttolifelonglearning 74.04 Effectivetimemanagement/organization 70.199. Studentsshoulddevelopthefollowingelementsincludingthe
documentationof:
Navigateandidentifytherelevantcomponentsofamedicalrecord 72.11 Documentinaclearandconcisefashion 63.46 Completedocumentationinatimelyfashion 45.20 Documentevaluation/re-evaluation(interpretationoffindingsto
determinediagnosis,prognosis,andplanofcare)72.11
Establishanddocumentobjectiveandmeasurablegoals 79.80 Describeappropriatebillingandcodingpracticesrelevanttotheclinical
setting45.19
Gatherrelevantinformationfrommedicalrecordsandotherrelevant 75.00
117
Page 119
sources10. Studentshouldrecognizeandaddressissuesrelatedtosafepatient
careincludingtheabilityto:
AllelementsreachedConsensus 11. Studentshoulddemonstratethefollowingclinicalreasoningskillsfora
non-complexpatient:
Individualizetheexaminationtothepatientandpracticesetting 69.24 Followalogicalsequenceduringtheexaminationandintervention 65.38 Developaplanofcarethatislinkedtothepatientsactivitylimitations
andparticipationrestrictions76.93
Connectassessmentofoutcomestofunctionalanalysis 71.16 Recognizetheinfluenceofpersonalandcontextualfactors 76.70 Addresstheneedtoprogressorchangeacurrentplanofcare 65.05
12. StudentshouldhaveBOTHtheunderstandingandskilltoperformthefollowingexaminationskills:
Anthropometricmeasurements 76.93 Cranialnerves 67.31 Functionalperformancetests 73.03 Integumentassessment 75.96 Movementanalysis 77.88 Orthopedicspecialtests 66.34
13. Studentshouldhavetheunderstandingandskilltoperformthefollowinginterventions:
Prescribe,fit,andinstructpatientsinproperuseofadaptiveequipment 49.04 Manualtherapy:specificallysofttissuemassage 66.32 Manualtherapy:specificallyjointmobilizations(I-IV) 53.85 Manualtherapy:specificallyjointmanipulations/thrust(V) 23.08 Biophysicalagents:specificallythermal 65.38 Biophysicalagents:specificallymechanical 59.61 Biophysicalagents:specificallyelectrical 57.69 Progressionofplanofcare 77.86 Therapeuticexercise:specificallyneuromuscularre-education 77.89
14. Studentshouldrecognizeandfollowspecificprofessionalstandards,including:
Engageinprofessionalserviceandcommunityactivities 46.16 Interprofessionalpracticecompetencies-identifiedbythe
InterprofessionalEducationCollaborative(IPEC)asvalues/ethicsforInterprofessionalPractice,roles/responsibilities,interprofessionalcommunication,teamsandteamwork
65.39
118
Page 120
AppendixC
StudentReadinessfortheFirstFull-TimeClinicalExperience
Thefollowingtablesummarizestheminimalknowledge,skillsandabilities(KSAs)inwhichphysicaltherapiststudentsmustdemonstratecompetencepriortoentryintothefirstfull-timeclinicalexperience.TheKSAsaregroupedinto14themes,numberedandindicatedinboldtextwiththecorrespondingKSAslistedbelow.Greaterthan80%ofparticipantsintheDelphistudyindicatedthattheseitemswerenecessary.
StudentReadinessThemesandKSAsTheme1 Studentsshouldhavefoundationalknowledgetosupportapplicationandsynthesisinthe
followingcontentareas:1.1 Anatomy(i.e.functionalanatomy)1.2 Commondiagnosesrelatedtosystemsreview(e.g.medical,physicaltherapy1.3 Kinesiology(i.e.biomechanics,exercisescience,movementscience)1.4 Physiology/Pathophysiology(relatedtogeneralsystemsreview)1.5 Tissuemechanics(e.g.stagesofhealing,use/disuse,load/overload)
Theme2 Studentsshouldmeetthespecificprogramidentifiedcurricularrequirementsincluding:2.1 achieveminimumGPA2.2 meetminimumexpectationsforpracticalexaminations2.3 remediationofanyandallsafetyconcerns
Theme3 Studentsshouldtakeinitiativetoapplyevidence-basedstrategiesto:3.1 generateinterventionsideas3.2 guidedecision-making3.3 measureoutcomes3.4 researchunfamiliarinformationorconditions
Theme4 Studentsshouldengageinself-assessmentincluding:4.1 self-assessmentoftheimpactofone’sbehaviorsonothers4.2 theunderstandingofone’sownthoughtprocesses(metacognition)4.3 self-reflectionandidentificationofareasofstrengthandthoseneedingimprovement,
developmentofaplantoimprove,anddiscussionofthatplanwithinstructors4.4 seekingoutresources,includingsupportfromotherswhenneeded,toassistinimplementationof
theplanTheme5 Studentsshouldutilizeconstructivefeedbackby:
5.1 beingopenandreceptive,verbally/non-verbally5.2 implementingactionstoaddressissuespromptly5.3 reflectingonfeedbackprovided
Theme6 Studentsshoulddemonstrateeffectivecommunicationabilitieswithinthefollowinggroups:
6.1 diversepatientpopulations6.2 familiesandotherindividualsimportanttothepatients6.3 healthcareprofessionals
Theme7 Studentsshouldexhibiteffectiveverbal,non-verbalandwrittencommunicationabilitiesto:7.1 listenactively7.2 demonstratepolite,personable,engagingandfriendlybehaviors7.3 independentlyseekinformationfromappropriatesources7.4 buildrapport
119
Page 121
AppendixC
7.5 seekassistancewhenneeded7.6 engageinshareddecision-makingwithpatients7.7 demonstratealevelofcomfortandrespectwithpatienthandling7.8 demonstrateempathy7.9 uselanguageandterminologyappropriatefortheaudience
7.10 introduceone’sselftoCI,clinicalstaff,andpatientsTheme8 Studentsshouldbepreparedtoengageinlearningthroughdemonstrating:
8.1 accountabilityforactionsandbehaviors8.2 resilience/perseverance8.3 culturalcompetenceandsensitivity8.4 aneager,optimisticandmotivatedattitude8.5 respectforpatients,peers,healthcareprofessionalsandcommunity8.6 open-mindednesstoalternativeideas8.7 punctualitywithallassignments8.8 self-caretomanagestress8.9 responsibilityforlearning
8.10 self-organization8.11 takingactiontochangewhenneeded8.12 willingnesstoadapttonewandchangingsituations8.13 appropriateworkethic8.14 maturityduringdifficultorawkwardsituationswithpatients,familiesandhealthcare
professionalsTheme9 Studentsshoulddevelopthefollowingelementsincludingthedocumentationof:
9.1 examination/re-examination(History,systemsreview,andtestsandmeasures)9.2 establishanddocumenttheproblemlist9.3 dailyinterventions
Theme10 Studentshouldrecognizeandaddressissuesrelatedtosafepatientcareincludingtheabilityto:
10.1 identifycontraindicationsandprecautions10.2 assessandmonitorvitalsigns10.3 identifyandrespondtophysiologicchanges10.4 assesstheenvironmentforsafety,includinglines,tubes,andotherequipment10.5 appropriatelyapplyinfectioncontrolproceduresincludinguniversalprecautions10.6 provideassistanceandguardingforpatientsafety10.7 utilizeappropriatebodymechanicstoavoidinjurytoselforpatients10.8 provideappropriatedrapingduringpatientcareactivities
Theme11 Studentshoulddemonstratethefollowingclinicalreasoningskillsforanon-complexpatient:11.1 utilizetheelementsofthepatient-clientmanagementmodelincluding:addressvariousbody
systems(cardiopulmonary,integumentary,musculoskeletal,neuromuscular)duringtheexamination
11.2 articulateaclinicalrationaleinpatientevaluation11.3 developgoalsthatarelinkedtothepatient’sactivitylimitationsandparticipationrestrictions11.4 determineappropriatenessfortherapywithinscopeofPTpractice11.5 interpretexaminationfindings11.6 screentorulein/outconditionsandconcerns
120
Page 122
AppendixC
Theme12 StudentshouldhaveBOTHtheunderstandingandskilltoperformthefollowingexaminationskills:
12.1 balanceassessment12.2 chartreviewtoextractrelevanthistory12.3 dermatomescreening12.4 functionalmobilityassessment12.5 gaitassessment12.6 goniometry12.7 interview/historytaking12.8 lowerquadrantscreening12.9 manualmuscletesting
12.10 musclelengthtesting12.11 myotomescreening12.12 reflextesting12.13 sensoryexamination12.14 medicalscreeningforredflags12.15 systemsreview12.16 upperquadrantscreening
Theme13 Studentshouldhavetheunderstandingandskilltoperformthefollowinginterventions:13.1 prescribe,fit,andinstructpatientsinproperuseofassistivedevices13.2 functionaltraining(includingbedmobility,transfers,andgait)withappropriateguardingand
assistance13.3 individualizedpatienteducation13.4 therapeuticexercise:specificallystrengthening13.5 therapeuticexercise:specificallystretching13.6 therapeuticexercise:specificallyaerobicexercise
Theme14 Studentshouldrecognizeandfollowspecificprofessionalstandards,including:14.1 appropriatedresscode14.2 corevaluesidentifiedbytheAPTAasaccountability,altruism,compassion/caring,excellence,
integrity,professionalduty,andsocialresponsibility14.3 clinicalexpectationsspecifictosetting14.4 HIPAAregulations14.5 legalaspectsrelatedtopatientcare14.6 obligationsofthepatient-providerrelationship14.7 passionfortheprofession14.8 patientrights14.9 maintainingprofessionalboundaries
14.10 understandingphysicaltherapy'sroleinthehealthcaresystem
121