56
Strategic Partnership Guide: Good Practice in Working with People with Experience of Mental Health Difficulties
Strategic Partnership Guide: Good Practice in Working with People with Experience of Mental Health Difficulties

Strategic Partnership Guide: Good Practice in Working with People with Experience of Mental Health Difficulties
National Disability Authority
25 Clyde Road
Dublin 4
Tel: 01 608 0400
Fax: 01 660 9935
Email: [email protected]
2005
Acknowledgements
The Strategic Partnership Guide: Good Practice in Working with People with Experience
of Mental Health Difficulties was commissioned by the National Disability Authority (NDA)
in response to the recommendation of a NDA statutory committee, the Mental Health
Advisory Committee (MHAC). The Guide is based on research and review of good
practice undertaken by Chris Stevenson, Sue Jackson and Jean Davison (Teesside
Centre for Rehabilitation Sciences, England) and Kieran Crowe and Paddy McGowan
(Institute for Mental Health Recovery, Ireland).
The team, with the NDA, would like to thank the following representatives from a number
of voluntary, community and statutory organisations who provided input and feedback
during the research and consultation stages of developing the Guide:
Frank Flannery Chair, Mental Health Advisory Committee
Mary Clarke-Finnegan Mental Health Advisory Committee
Phil Cotter Mental Health Advisory Committee
Patsy Doolin Mental Health Advisory Committee
Frances Harvey Mental Health Advisory Committee
Paul Howard Mental Health Advisory Committee
Seamus Hoye Mental Health Advisory Committee
Mark Logan Mental Health Advisory Committee
Verena Keane Mental Health Advisory Committee
Brendan Kenny Mental Health Advisory Committee
Mary Keys Mental Health Advisory Committee
Andrew Logue Mental Health Advisory Committee
Hugo Magee Mental Health Advisory Committee
Louis McGuire Mental Health Advisory Committee
2
National Disability Authority
Tom Moran Mental Health Advisory Committee
Tom Noonen Mental Health Advisory Committee
Dan O’Connor Mental Health Advisory Committee
Winifred O’Hanrahan Mental Health Advisory Committee
Laura Thompson Mental Health Advisory Committee
Margaret Webb Mental Health Advisory Committee
Laurie Ahern Mental Disability Rights International, US
Liz Brosnan Western Mental Health Alliance
Deirdre de Burca Green Party
Will Hall Freedom Centre, US
Professor Alec Jenner Asylum, UK
Paul Johnson National Institute for Mental Health England
Limerick focus group members
Terry Lynch Private psychotherapy practice
Donal McAnaney Rehab Group
Anne O’Donnell Edinburgh Users Forum
Mary O’Hagan Mental Health Commission, New Zealand
John Redican Irish Advocacy Network
Dr Alex Reed University of Northumbria, UK
Jan Wallcroft EbyE, National Institute for Mental Health England
Aisling White North Dublin Psychology Service
3
Strategic Partnership Guide
ForewordThe National Disability Authority’s Strategic Plan 2004-2006 states that working in
partnership is one of our core values and that, in particular, the Authority will work to
‘maintain and strengthen existing partnerships, and initiate and contribute to the
development of strong partnerships and constructive working relationships… as a basis
for effecting change’.
This Strategic Partnership Guide builds on earlier guidance in the NDA’s Ask Me:
Guidelines for Effective Consultation with People with Disabilities and on our investment
in promoting the rights of people with experience of mental health difficulties, for example
through the establishment of the statutory Mental Health Advisory Committee and
publication of an issue in the Disability Agenda series, entitled Promoting Positive
Attitudes to Mental Health. Through the publication of this Guide, the NDA signals the
importance of including people with disabilities in strategic partnership, i.e. moving
beyond consultation.
This Guide represents an authoritative international and national consensus on forming
and maintaining such successful strategic partnerships. The University of Teeside,
England and the Institute for Mental Health Recovery, Ireland have been commissioned
by the Authority to develop the Guide and have done so using evidence from a number of
sources including an international Delphi exercise with a wide range of stakeholders, a
digest of selected national and international research and policy literature, focus groups
of people with experience of mental health difficulties in Ireland and an Irish focus group
with multi-stakeholder membership.
The NDA considers that disabled people’s participation in strategic decision-making is a
vital component of promoting their inclusion in Irish society. Such participation is strongly
supported by international bodies such as the World Health Organisation. It is an
increasing feature of Irish Government and public administration, where structures and
projects to promote participation are occurring at all levels. These activities are welcome.
However, it is important that good practice is established in order to ensure effective and
equal involvement.
4
National Disability Authority
This Guide is designed to be a valuable, practical tool across all sectors. The NDA looks
forward to working with all stakeholders to develop good practice in this area.
I would like to thank all those who contributed their time and expertise in providing
feedback and input into the consultation, and to particularly thank the NDA’s statutory
Advisory Committee on Mental Health members for their input and insight into delivering
this important project.
Angela Kerins
Chairperson
5
Strategic Partnership Guide
12 Essential Principles for Effective StrategicPartnership with People with Experience ofMental Health Difficulties
1 Gain support from the organisation�s management
2 Identify appropriate partners � who, why, what can theycontribute, how can they represent others?
3 Build the foundations for the partnership � ensure equalentitlements and access to resources
4 Establish shared vision, purpose and ownership
5 Recognise diversity and equality of partners
6 Define the ground conditions for working together
7 Acknowledge the human and humanitarian elements ofthe partnership
8 Avoid undue pressure through flexibility in time scale and organisation
9 Consider overlapping and differing agendas of partners
10 Be realistic and be explicit about working in partnership
11 Attend to partners� needs non-judgementally, includingneeds for training and external support
12 Continually review and revise expectations through acycle of reflection-action-reflection
6
National Disability Authority

Contents
Acknowledgements 2
Foreword 4
Twelve essential principles for effective strategic partnership with people with experience of mental health difficulties 6
1 How the Strategic Partnership Guide can help you 9
1.1 Defining partnership, strategic partnership, strategic partnership with people
with experience of mental health difficulties and advocacy 11
1.1.1 Partnership 11
1.1.2 Strategic partnership 11
1.1.3 Strategic partnership with people with experience of mental
health difficulties 11
1.1.4 Strategic partnerships and advocacy 12
2 Getting started 15
2.1 Winning hearts and minds 16
2.2 Identifying appropriate partners 17
2.3 Building the foundations for the partnership 18
2.4 Establishing shared vision, purpose and ownership 19
2.5 Recognising diversity and equality 21
2.6 Defining the ground conditions 22
2.7 Acknowledging the human and humanitarian characteristics of partners 23
7
Strategic Partnership Guide
3 Keeping going by attending to process 25
3.1 Avoiding undue pressure 26
3.2 Assessing for overlapping and differing agendas 27
3.3 Being realistic and being explicit 28
3.4 Attending to partners’ needs 29
3.5 Continually reviewing and revising expectations 30
3.6 References 31
4 Training materials 33
4.1 Training exercises 34
4.1.1 Understanding strategic partnerships 34
4.1.2 Making a case 35
4.1.3 Partners 1 35
4.1.4 Partners 2 35
4.1.5 The initial strategic partnership meeting 36
4.1.6 Building blocks 36
4.1.7 Sharing 36
4.1.8 Different and equal 37
4.1.9 The process of partnerships 38
4.1.10 How strategic partnerships have worked for others 38
4.2 Training exercise pointers 38
4.2.1 Defining strategic partnerships 38
4.2.2 Evidence to help win hearts and minds 39
4.2.3 Engaging appropriate partners 1 40
4.2.4 Engaging appropriate partners 2 42
4.2.5 Organising the initial strategic partnership meeting 43
4.2.6 Strengthen the foundations for the partnership 43
4.2.7 Working out shared vision, purpose and ownership 44
4.2.8 Diversity and equality of points of view 44
4.2.9 Partnership process 44
4.2.10 First hand testimonials 45
References and further reading 48
Feedback 49
8
National Disability Authority
1. How the StrategicPartnership Guide can help you
9
1. How the StrategicPartnership Guide can help you
The Guide is a practical tool to help people understand the processes of forming and
maintaining strategic partnerships with people with experience of mental health difficulties.
It is divided into 4 parts:
• Part One looks at definitions of partnerships
• Parts Two and Three cover the process of starting off and maintaining partnerships
• Part Four is a resource for training, either to support ongoing partnership working or
more generally as a resource for training agencies, education providers or health
provider organisations
The first three parts of the Guide give information (in black text) and instructions that
point to action (in purple text). The actions can be treated as a check list for strategic
partnerships to refer to and work through. The fourth part of the Guide provides
experiential learning tasks to support in-service or other training.
Strategic partnerships are new and are breaking new ground. Partners may find new
issues that need to be addressed. With this in mind, the Guide has an evaluation
component that users are invited to complete in order that the Guide continues to grow
and remain useful.
10
National Disability Authority
1.1 Defining partnership, strategic partnership,strategic partnership with people withexperience of mental health difficulties and advocacy
It is important to be clear about what is meant when we use the word partnership alone
and in combination as in ‘strategic partnership’ and ‘strategic partnership with people with
experience of mental health difficulties’.
1.1.1 Partnership
According to the Oxford English Dictionary, a partner is a person who takes part in an
undertaking with another or others, especially in a business with shared risks and profits.
A partnership is an association of two or more people as partners.
1.1.2 Strategic partnership
A strategic partnership involves forming part of a long-term plan or aim to achieve a
specific purpose. Strategic partnerships involve a shared sense of the need for change.
The change may be needed in organisational structure and function, in policy, or in
philosophy. The focus in strategic partnerships is action. There is a balance between
talking and doing. They are not ‘talking shops’.
1.1.3 Strategic partnership with people with experience ofmental health difficulties
When we talk about strategic partnership with people with experience of mental health
difficulties, there is a further dimension to the partnership. Mental health difficulties
involve a continuum along which all of us move. People find themselves at different points
on this continuum at different times in their lives. Human distress is universal, and we are
all recovering ourselves all of the time. However, some people find themselves at the
‘sharp end’ of the continuum for prolonged periods of time. Deegan pointed out in 1992
that severe mental health difficulties do not diminish an individual’s worth; everyone still
deserves respect and recognition of personal strengths, no matter what the mental health
issues are [1].
11
Strategic Partnership Guide
It is important to recognise that strategic partnerships are not therapeutic partnerships.
Sometimes the two merge and a means of managing the merger is needed, as the
following example shows:
In a 1998 study, Smith describes a partnership in which evaluation instruments were
developed with mental health service-users [2]. Smith points out that the most difficult
task for the group was keeping on track with the task in hand and not going off on a
tangent and becoming a ‘support group’. However, the process demonstrated a need for
such a group within the service and as a compromise they set aside 15 minutes at the
commencement of each session for the mutual support before tackling the task in hand.
In a strategic partnership the partners are considered as seeking change external to
them. Inevitably all partners will grow in the context of a successful strategic
partnership, but this is not the main function of the partnership.
One factor that can limit a strategic partnership is a strong belief that mental health
difficulties are due to a disturbance in biological functioning as in physical illnesses like
diabetes. With this belief, treatment relies heavily on medication and is controlled by
professionals. The person is not seen as having a strong degree of independence, or
the capability for self-determination. When professionals enter into partnership with this
explanation, they tend to assume greater responsibility. This is inappropriate for a
strategic partnership where the partners are equal. One way to guard against hierarchy
is to set strategic partnerships within an advocacy framework.
1.1.4 Strategic partnerships and advocacy
Advocacy has many voices: personal, political, assisted self, self, collective, and group.
The strategic partnership must explicitly acknowledge and actively support the advocacy
needs of partners. To meet advocacy needs within your strategic partnership you must:
• Look inwards and look outwards. Monitor and reflect on the process of the
partnership to ensure that it is remaining strategic and not lapsing into a hierarchical
and/or therapeutic mode. Monitor and reflect on the context of the partnership in order
to assess whether change is occurring and where change still needs to occur and
what might be affecting the change process externally.
12
National Disability Authority
• Develop and sustain self determination. Accept that people have the desire and ability
to represent their own views. Do not try to colonise others by trying to impose your
particular view of the world on them. Enable and support individual expression where
needed, even if this is sometimes at the expense of your own agenda and ego.
• Represent the group agenda. Express a belief in and commitment to the larger group
agenda, even though this may differ from your own ideas.
• Promote a culture of human rights. Ensure that the strategic partnership is non-
coercive and non-violent. Do not use force, either emotional or verbal, in order to push
one agenda over another, or block views that are culturally different.
• Facilitate people in their own empowerment process. Empowerment is defined as a
psychological sense of personal control, involvement, influence and awareness of
options in one’s life. Make explicit the importance and value of partners’ contributions.
• Redress power. In 2002, El Ansari and colleagues stated that the way decisions are
made is determined by how power is structured and make the point that power can
take many forms:
‘ …accessing and utilising data and information (information power), resources and
funds (economic power) as well as the competencies, capacities and proficiencies of
the stakeholders (technical power)’. [3]
The (re)sources of power tend to cluster around professionals who can then dictate the
nature of the partnership. In 2004, an article in Mental Health Today pointed out that for
professionals to view service-users working in a strategic fashion can be daunting [4]:
‘They were working with service users in a planning and strategic arena who knew
more about it than they did. It really flagged up how good the service user
involvement project is, how well trained the people are and how well up they are on
policy and operational issues. You might expect people to be experts on their own
health but when people say, it would help my recovery more if there was a service like
this – it’s a whole new arena for some staff.’
13
Strategic Partnership Guide
• Give equal value to professional knowledge and experiential knowledge.
• Adopt flexible practices in relation to how meetings take place, and how meetings
are recorded.
• Negotiate the roles within the strategic partnership. Encourage people to try
out roles outside their existing experience in order to maximise alternative and
creative contributions.
It is not possible to define the aims and objectives of individual strategic partnerships
involving people with experience of mental health difficulties. However, the partnership
must seek change that promotes rather than compromises the rights and dignity of
individuals within organisations and especially in the context of care provision. In this
respect, partnerships with people who experience mental health difficulties are different
from other strategic partnerships where profit may be prioritised over human rights. The
strategic partnership with people who experience mental health difficulties has a
collective advocacy function. For example, a partnership established with the aim of
introducing social employment would consider the rights of workers to an equitable wage.
14
National Disability Authority
2. Getting started
15
2. Getting startedEstablishing a responsive organisational ethos and culture helps to prevent superficial
organisational commitment, for example in relation to resources. It prevents tokenism as
the input of people who have experience of mental health difficulties will have been
appropriately justified.
2.1 Winning hearts and minds
• Seek commitment from ‘the top’, for example the management of the hospital, health
service, or team leader.
• Consider the socio-political, cultural and economic context in which the partnership
will operate.
• Beware of compromising the autonomy of the partnership by accepting sponsorship,
for example support from the pharmaceutical industry.
• Engage with cynical and obstructive individuals in positions of power for whom the
prospect of change is more threatening than keeping things the same. Try to
understand the reasons for their negativity, for example vested interests, or previous,
poor experiences of strategic partnerships.
• Make a general case for why partnership is a good way forward. Use the evidence
presented in Section 4.2.2 that supports the philosophy, principles and practice of
strategic partnerships with people who have experience of mental health difficulties.
• Make a specific argument as to why the partnership is needed now, for example,
because of a current issue, and how the partnership might be enacted, and to what
end. Identify how the change will improve the situation for individuals who resist the
idea of change.
16
National Disability Authority
2.2 Identifying appropriate partners
The first stage in establishing a strategic partnership is to identify appropriate partners,
to arrive at the right constituency. Remember that some individuals would not wish to
participate and, as Cahill suggested, professionals need to ensure that people are not
coerced as reluctant collaborators [5].
Sometimes the idea of the partnership will have emerged from existing groups. Despite
this, you must ask yourself four questions and be able to give yourself clear answers:
• Who is to be a partner?
• Why they are to be included?
• What is the potential contribution that they will make?
• How can they communicate with others to ensure they represent the broader
reference group?
This gives the partnership a solid basis for beginning to work.
There are no hard and fast rules about who should be invited, for example, how many
people with experience of mental health difficulties to how many professionals or what
disciplinary mix. However,
• The partnership must include people who have experienced mental health difficulties
at the pre-planning stage to ensure that they have parity of esteem and real, equal
status within the partnership.
• Consider all partners, and not just professionals, as stakeholders, or key players, that
is people who have special interest in the area and concern to create change.
Invitations to participate should be carefully worded, and be non-threatening or
demanding. An example of a letter that can be adapted for your own situation is given
in the training section of the Guide (4.2.4).
17
Strategic Partnership Guide
Good preparation will ease the initial coming together process. Attention to detail and
building up momentum works best. You must consider what an appropriate venue is,
by asking:
• What are the travel implications for the partners?
• What facilities are available, including provision of refreshments?
• Is the physical environment accessible for all?
• Does the venue have any drawbacks?
For example, a meeting room on a hospital ward might be unattractive to
someone who has undergone treatment there; a venue may be unsafe in relation
to evening attendance.
• Are there other venues that might be more inspirational?
For example, it may be appropriate to draw on alternative settings that are closer to
the natural environment and which can inspire different kinds of thinking in relation to
growth, learning and insight.
• What degree of formality do we want when meeting together?
Remember, a formal meeting room will lead to a more formal meeting and may inhibit
more creative discussion; equally, an informal meeting room may not help to keep
people focused on the business at hand.
2.3 Building the foundations for the partnershipThe partnership must be built on strong foundations, and with a commitment to ‘give and
take’. If it is not, then small irritations will end up becoming big enough to discourage
attendance or effective working together. The partnership is, by definition, equal and so
each partner must have equal entitlements. Resources must be made available to
support the partnership.
18
National Disability Authority

• Where possible non-wage earners must be paid appropriately for their participation.
The level and kind of payment is decided on an individual basis to allow for
differences in income sources, and preferences. For example, Pivik and colleagues
found that an honorarium was of more value to the service-user as a sign of respect
and of service-user expertise because payment could call into question the dedication
of a volunteer [6]. It should be bourne in mind that payment can also negatively
impact on benefits such as social welfare. Some statutory bodies may be precluded
from making such payments under current legislation.
• Where expenses are being paid, they should be paid promptly.
• Regular meetings must be set up in order to help to build a sense of rhythm and keep
up the partnership’s momentum.
• Sufficient time has to be allowed to get to grips with the realities of working together,
to do the groundwork.
This may be time set aside and used formally, for example in setting ground
conditions. Some time may be used more informally, for example in conversation over
lunch, so that the partners begin to know each other in a more human to human way.
They can establish trust and connectedness. A trusting relationship is critical
according to Linhorst and Eckert’s study in 2002 [7]. People who have experience of
mental health difficulties may worry that they are not heard by the professional
partners and that no change will occur, or that there will be repercussions for them as
a result of their involvement. Staff may fear victimisation from managers and other
senior professionals if they were critical of service delivery. Trust also helps to prevent
defensiveness when a challenge to a partner’s view is made.
2.4 Establishing shared vision, purpose andownership
In his 1996 study, Bowl pointed out that there was confusion about the purpose and
meaning of user involvement at all levels of the organisation [8]. The idea of creating a
strategic partnership may have come from one person or one organisation, with a
particular issue in mind. On the other hand, a strategic partnership might have been
suggested with more vague motives, for example, because of the current culture of
service user involvement. In either case, you must establish shared vision and ownership
in relation to the partnership and the hoped for outcomes. Such clarity and commonality
is found when the partnership:
19
Strategic Partnership Guide
• Establishes shared interests or aims or goals or purposes of strategic significance.
It is inevitable that people coming from different positions will have different
perspectives. The function of the partnership is to meld these into an agreed vision
and purpose. This will underpin the partnership’s Terms of Reference. The Terms of
Reference provide the reason and/or the purpose for which the partnership is being
developed. They help people to understand the perspectives and motivations of the
partnership and support a plan of action.
• Clarifies the core values.
• Shares risks.
The fear of taking risks can close down the productivity of a partnership. There is no
dignity without risk and the partners can sustain one another in this respect.
• Shares benefits.
• Shares strategising.
• Encourages joint effort and active participation.
• Clarifies the roles and responsibilities of each of the partners.
This is particularly important (within the bounds of confidentiality) when people
cross boundaries from service-user to service employee, or from professional to
service-user.
• Rotates responsibility for key tasks, especially those that can increase professional
control, for example, chairing meetings or minute and note taking.
• Clarifies the desired outcomes.
• Clearly defines the decision-making process.
• Embodies respect and trust in relation to different interests.
20
National Disability Authority
2.5 Recognising diversity and equalityStrategic partnerships benefit from the bringing together of diversely experienced people
in forums that encourage dialogue. They function best when there is shared ownership,
interests, goals and purposes but different experiences and perspectives all equally
valuable and valued. The partnership must:
• Actively bring out different experiences and perspectives by asking questions of one
another that help to energise creative dialogue. For example, ask, ‘What was your
best experience of a therapeutic activity?’
• Treat different experiences and perspectives respectfully and equally with open-
mindedness, rather than questioning which is the most accurate.
• Consider different experiences and perspectives as a pool of knowledge.
• Accept that the process of the dialogue involves unpredictability and uncertainty.
Unpredictability, uncertainty and not trying to force a solution can lead to novel
representations of an issue or a new solution to a problem.
• Check regularly with partners that the new representation is helpful.
Diversity may also mean that the needs of the partners in relation to the partnership
differ. The needs may be obvious or emerge as the partnership progresses (see Section
3.4). In the initial stages, the partnership must:
• Allow time and space to explore what initial needs different people have.
• Actively respond to those needs, with resources both within and without the group.
• Make information available about best practice in partnership working.
Some partners will be experienced in working constructively together, others less so.
Knowing that strategic partnerships can and do work inspires confidence at the start
of the enterprise.
21
Strategic Partnership Guide
2.6 Defining the ground conditionsGround conditions are not just risk limiters. They can be important in ensuring that all
participants have fair and transparent access to involvement in the partnership. The
ground conditions will vary according to the membership. However, there are some key
guiding principles that form the bedrock for the partnership:
• Treat every partner as equal with the same entitlements as a citizen.
A citizen is entitled to the protection and benefits of being part of the society and is
entitled to be included and to contribute.
• Promote dialogue between partners by asking each other questions that encourage
debate. For example, ask, ‘What are your hopes and dreams for the organisation?’
• Listen to others and hear what they say.
Sometimes people ‘listen in order to talk’ rather than ‘talk in order to listen’.
• Show mutual respect for other people’s opinions, by valuing each contribution and
trying to understand why it matters.
• Make a commitment to honesty and openness.
It is not always easy to express one’s honest opinion without the safety of statements
about confidentiality and non-judgemental philosophy.
• Build and maintain trust through being together in a respectful, honest and open way.
• Pay attention to language; make sure that language is used unambiguously.
Unambiguous communication leads to unambiguous communicating and
unambiguous communicating leads to unambiguous communication.
• Maintain accessible communication; use words that are not jargon-laden, prejudiced,
or that do not encourage stereotyping or stigmatising.
• Create freedom for partners to use the language appropriate for them (collectively
or individually).
Language that is unfamiliar to the partners will not help the relationships built up in
the group to progress.
22
National Disability Authority
• Use language to both create and reflect a culture of mutual respect and interests
shared by the partnership.
• Be aware that not everyone has access to the same communication media, for
example e-mail.
• Be creative in using communication tools, for example, verbal (audio taped) and
written submissions, questionnaires etc.
• Give space to creativity in thought, and in the use of resources. For example,
encourage partners to visualise an ‘ideal world’ or use meeting spaces to role play
different problem-solving strategies.
• Commit to a balance of rights and responsibilities.
2.7 Acknowledging the human and humanitariancharacteristics of partners
In successful partnerships, the abilities of humans are celebrated. Human capabilities are
often taken as ordinary but can have an extraordinary potential when used in partnership.
The following list serves as a reminder:
• Self-determination
• Wisdom
• Integrity
• Honesty
• Emotionality – emotions can act as a barometer for what is happening within
and outside the partnership, and can provide the passion for seeking change,
if they are contained and harnessed by the partnership
23
Strategic Partnership Guide
• Capacity for understanding, for example, understanding staff resistance – ‘These
aren’t proper users’, ‘It’s tokenism’
• Capacity for self-reflection on emotional states and communication impacts
• Accessibility or openness to the needs and views of the other
• Consistency
• Friendliness.
24
National Disability Authority
3. Keeping going by attending to process
25
3. Keeping going by attendingto process
It is very easy once a partnership is established to think that it will continue automatically
until it achieves its goals. However, without attention to the process (what is happening
within the partnership) it is possible to end up with individuals travelling in different
directions at different paces towards different ends. In maintaining strategic partnerships
you must:
• Ensure that there is a clear and open reflexive process, so that the partnership puts
itself under the spot light.
• Detect problems early through regularly seeking views.
• Engage in constructive problem solving.
3.1 Avoiding undue pressureAccording to Linhorst and Eckert’s 2002 study, people who experience mental health
difficulties reported some problems in being consistently involved in partnerships,
especially in the long term, if symptoms and treatments get in the way [7]. Professionals
have competing demands to balance. Pressure is avoided when flexible and adaptable
processes and agendas are in place.
• Do not place outcomes over process and expect too much too soon.
• Be explicit about the demands of the partnership and you will help people to decide
whether and how much they can commit.
• Ensure organisational support, and the finance and other resources that go with it.
• Be tolerant towards both the quantity and quality of the partners’ contributions.
26
National Disability Authority
3.2 Assessing for overlapping and differingagendas
The idea of forming a strategic partnership might come from different people. For
example, a person with experience of mental health difficulties, a carer, a mental health
service user organisation, a hospital manager, a professional.
• Have an open conversation about how the idea of a partnership arose, and what
the individual’s or organisation’s hopes and expectations are in relation to the
strategic partnership. Ask the questions of each other, ‘What brought you to think
about a strategic partnership?’ and ‘What do you think is to be gained by the
partnership working?’
This transparency promotes honesty and clarity in relation to the partnership’s
objectives and prevents ‘hidden agendas’ and concerns about the motives for
joint working.
• Remember that people have different hopes and expectations for the partnership
depending on the position they hold.
• Both strive for commonality and…
• take the other’s position.
When people have been trained in and/or have deeply meaningful experiences of
mental health care, it is sometimes difficult for them to see the other person’s point of
view or position as justified. Shared training sessions for staff, service users and
carers (for example, in strategic partnership working, advocacy, communication skills,
and non-violence techniques) can help develop a sense of the other’s experience.
• Pay attention to potential conflicts of interest. For example, a professional’s loyalty to
the employer may get in the way of changing how care is provided.
27
Strategic Partnership Guide
3.3 Being realistic and being explicitA partnership cannot achieve solutions for every problem or create every change needed
in an organisation.
• Identify the scope the partnership has with careful consideration of factors external to
the partnership; not everything is possible in all circumstances.
• Focus on what the partnership can achieve rather than what it cannot; that is, set
realistic goals.
• Appreciate what each other can achieve in the context of the partnership.
• Set a realistic time frame and be flexible about it to allow space for time out, or panic,
or second chances.
• Identify the steps towards goals so that progress can be monitored and achievements
acknowledged.
• Establish exit strategies for partners at early stages.
It is important that people know they can leave the partnership at any time without
any sense of resentment. When there are decisions made about what the partnership
aims to achieve it is easier to know when it has reached its natural end. Having a
meeting to ‘round off’ by celebrating the partnership’s achievements, or a social
gathering, can help with the disbanding process.
28
National Disability Authority

3.4 Attending to partners� needsDifferent partners have different support needs in relation to their functioning. The needs
may be emotional, physical, or practical. People who have experience of mental health
difficulties may have had lack of opportunities in terms of education and employment,
less chance to be self-determining and have had to deal with the reality of shattered
dreams. As Turner-Crowson and Wallcraft pointed out, this has an impact on the success
or otherwise of partnership working [9]. But it is important to remember that people who
have experience of mental health difficulties are as different as they are similar as Minett
noted recently [10]. The same applies to professionals. Partnerships must:
• Acknowledge that sometimes needs are not obvious, but nevertheless should be
actively assessed.
• Use the ability to imagine oneself in another's place and understand the other's
feelings in order to discover needs where they are not obvious.
• Accept that needs shift according to time and context. For example, as Cahill reports,
if professionals extend their roles to become involved in promoting service-user
involvement, they will have to adjust their own position with regard to the duties and
functions they perform [5]; or someone with literacy needs may develop within the
partnership and not need the same support as the partnership progresses.
• Accommodate partners’ needs non-judgementally.
• Ensure that professional partners offer support that is non-patronising, for example,
support that focuses on the person as self-determining and which tries to engineer
scope for the person to perform.
• Assess for participation.
Some people are quiet, or silent, partners. However, silence may indicate that the
person finds some obstacle to taking part and needs support to become included.
• Allow space to grow self-confidence.
29
Strategic Partnership Guide
• Accept that emotional distress for any partner is meaningful; safety to be emotional
and non-pathologising of emotions is required.
• Be vigilant in relation to professional attempts to covertly control partnership process.
• Build in adaptability in response to changing needs or agendas.
• Organise relevant training.
By not just learning ‘on the job’ individuals/groups can be more effective more quickly.
• Be willing to help each other to identify or build networks, or take consultancy, internal
and external to the organisation and to seek resources to this end.
• Ensure sharing of the resources that professional partners have in relation to meeting
needs, for example desk or office space or meeting facilities.
3.5 Continually reviewing and revisingexpectations
The initial expectations for the partnership in terms of outcomes may need to be re-
visited because of how the partnership is working internally or because of the changing
external context. For example, if there is difficulty in attending, the original expectations of
the group might not be met; if new policy is introduced in the organisation, the
partnership will have to re-think their contribution.
• Establish a review mechanism, for example, after every second meeting, or after
certain milestones are achieved.
• Rotate responsibility for review amongst partners.
• Consider review and revision of expectations as a strength and not a weakness as it
will contribute to a relevant and meaningful set of outcomes in the longer term.
• Take stock regularly as a means to recognising the achievements to date and to
ensuring early identification of obstacles that need to be overcome.
This prevents raising hopes of change that are not followed through.
30
National Disability Authority
• Engage in an action-reflection-action cycle to keep forward movement.
The partnership is subjecting itself to audit or is self governing when it is monitoring
its own performance against initial targets for performance.
• Actively seek input from all partners.
This may be achieved in regular meetings and by convening extra meetings.
3.6 References1. Pat Deegan, “The independent living movement and people with psychiatric
disabilities: taking back control over our own lives”, British Journal of Therapy and
Rehabilitation, 9/2 (1992): 52-55.
2. M.K. Smith, “Empowerment evaluation: theoretical and methodological
considerations”, Evaluation and programme Planning, 21(1998): 255-261.
3. W. El Ansari and colleagues, “Narrowing the gap between academic professional
wisdom and community lay knowledge: perceptions from partnerships”, Public Health,
116 (2002): 151-159.
4. “Shared Vision”, Mental Health Today, November (2004): 18-19.
5. J. Cahill, “Patient participation: a concept analysis”, Journal of Advanced Nursing,
24/3 (1996): 561-571.
6. J. Pivik and colleagues, “A consumer involvement model for health technology
assessment in Canada”, Health Policy, 69/2 (2004): 253-268.
7. D.M. Lindhorst and A. Eckert, “Involving people with severe mental illness in
evaluation and performance improvement”, Evaluation and the Health Professions,
25/3 (2002): 284-301.
8. R. Bowl, “Involving service users in mental health services: social services
departments and the national health service and community care act 1990”,
Journal of Mental Health, 5/3 (1996): 287-303.
31
Strategic Partnership Guide
9. J. Turner-Crowson and J. Wallcraft, “The recovery vision for mental health services
and research: A British perspective”, Psychiatric Rehabilitation Journal, 25/3
(2002): 245.
10. R.J. Minett, (2002) “User participation in mental health care: a literature review”,
British Journal of Therapy and Rehabilitation, 9/2 (2002): 52-55.
32
National Disability Authority

4. Training Materials
33
4. Training MaterialsThe purpose of this section of the Guide is to enable people who are thinking about
working within a strategic partnership with people with experience of mental health
difficulties to get started. This self-directed learning will provide you with some of the
foundations required to build successful and longstanding partnerships. The exercises
are tailored to both individual and group learning and can be undertaken by people from
different backgrounds and learning abilities. Each of the exercises relates to a part of the
Guide and we recommend that you have a look at each section before starting the
associated exercise. Additional pointers and some answers can be found in Section 4.2.
However, for some exercises there are no right or wrong answers as the exercises are
designed to encourage the individual or group to think about what partnerships mean to
their particular situation. We hope that you enjoy working through the ten exercises
shown below.
4.1 Training exercises
4.1.1 Understanding strategic partnerships
(For this exercise we suggest you read the ‘Defining partnership, strategic partnership,
strategic partnership with people who experience mental health difficulties and advocacy’
section of the Guide pages 11-12).
Task: Think of a partnership that, in your experience, works well. It might be a
relationship in an organisation that you are connected with or a relationship in your family
or social network.
Write down what you think are the important features of the partnership. Compare your
ideas to those set out in the Guide and the descriptions of partnerships in Section 4.2.1.
34
National Disability Authority
4.1.2 Making a case
(For this exercise we suggest you look at the ‘Win hearts and minds’ section of the Guide
page 16)
Task: Put together an argument for introducing Strategic Partnerships within your
organisation. If you are working in a group you each might like to present your
ideas to the group. Then turn to Section 4.2.2 to find more reasons for strategic
partnership working.
4.1.3 Partners 1
(For exercises 4.1.3 and 4.1.4 we suggest you look at the ‘Identifying partners’ section of
the Guide page 17)
Task: Ask yourself or ask within the group the following 4 questions:
• Who is to be a partner?
• Why they are to be included?
• What is the potential contribution that they will make?
• How can they communicate with others to ensure they represent the broader
reference group?
It is important to have positive attitudes in relation to involving people with experience of
mental health difficulties as partners. Section 4.2.3 gives a report of some relevant research.
4.1.4 Partners 2
Task: Design a letter to invite people to take part in the first Strategic Partnership meeting.
Have a go at writing your own letter before looking at the example in Section 4.2.4.
35
Strategic Partnership Guide
4.1.5 The initial strategic partnership meeting
(It is important here that you read the section in the Guide on Building the foundations of
the partnership, page 18, before you undertake this exercise).
Task: Imagine you are preparing for the first strategic partnership meeting. Write a list of
items that you think should appear on the agenda.
Look at Section 4.2.5 once you have done this to see if there is anything else you might
have included.
4.1.6 Building blocks
(To enable you to think about the task below first read the ‘Building foundations for the
partnership’ section of the Guide on page 18)
Task: Think about or share imaginative ways that individuals in a new Strategic
Partnership Group might get to know one another? Draw on your experiences of training,
social events or meetings.
You will find some ideas in Section 4.2.6.
4.1.7 Sharing
(You will need to read the section entitled ‘Establishing shared vision, purpose and
ownership’ on page 19 before you try this task).
Task: Make a list of the processes through which a partnership might arrive at shared
vision, purpose and ownership.
Some additional ideas on how you might do this will be found in Section 4.2.7.
36
National Disability Authority
4.1.8 Different and equal
(It is important here that you read the section in the Guide on Recognising diversity and
equality, page 21, before you undertake this exercise).
Question: Strategic partnerships benefit from bringing together people who have
had different life experiences. Different views allow others to see different aspects of
the whole picture. How can you make sure that all views have equal value and are
equally valuable?
Try this exercise:
Take ‘medication’ as your topic.
There are some ground rules. You must listen carefully to each person’s point. You may
not interrupt or disagree. Each person may only make one point.
• If you are working within a group to do this exercise
Each person in turn is to offer one thing they know about medication. It can be
anything at all.
Someone needs to write down all the ‘snippets’ of knowledge to form a pool of
information known about medication held by the whole group collectively.
• If you are working independently on these exercises
Try to generate pieces of information about medication as if they came from
the perspective of another. For example, what would a nurse, doctor, member
of the public or a person who has experienced mental health problems say
about medication?
Turn to Section 4.2.8 for a further exercise.
37
Strategic Partnership Guide
4.1.9 The process of partnerships
(We suggest you read ‘Keeping going: attend to process’ in the Guide pages 25-31 now).
Task: Think about what particular needs you might have in order to engage in a strategic
partnership. What might help meet your needs? If you are working in a group, explore
expertise within the group that might be helpful.
Refer to Section 4.2.9 for an example of how needs were attended to in a real strategic
partnership.
4.1.10 How strategic partnerships have worked for others
Task: Take time to read and discuss the first hand accounts of setting up and being
involved in strategic partnerships in Section 4.2.10. Look for similarities and differences
between the testimonial accounts and your experiences of partnerships to date.
4.2 Training exercise pointers
This section of the Guide will provide you with extra information and answers to the
training exercises in Section 4.1.
4.2.1 Defining strategic partnerships
Definitions of partnerships:
Partnership is a voluntary collaborative agreement between two or more parties in which
all participants agree to work together to achieve a common purpose or undertake a
specific task and to share risks, responsibilities, resources, competencies and benefits.
Marriage is not a ritual or an end. It is a long, intricate, intimate dance together and
nothing matters more than your own sense of balance and your choice of partner.
Amy Bloom, author.
38
National Disability Authority
4.2.2 Evidence to help win hearts and minds
Below are some arguments for working within Strategic Partnerships.
1. “It is increasingly important that consumers be involved both in the planning and
delivery of services.” Dr Dermot Walsh, Inspector of Mental Hospitals, Ireland.
2. A paper published by the Office for Health Management, Ireland in 2002 describes
different levels and qualities of partnerships in relation to patients and the public.
3. The lay public are ‘knowledgeable partners in health-care’ (Allen 2000).
4. The UK NHS and Community Care Act of 1990 emphasised the involvement of the
service-user as an essential component of healthcare philosophy (Anthony and
Crawford 2000).
5. Citizen involvement allows governments to share the blame and pain in the rationing
debate (Pivik and colleagues 2004).
6. Individuals have the right to participate in services that impact upon them and in turn
this involvement impacts on communities by promoting healthier behaviours,
increased education and support (Pivik and colleagues 2004).
7. With the increasing importance attributed to evidence based practice service-user
involvement is an essential element in any service (Anthony and Crawford 2000).
8. Partnerships or collaborations with communities have emerged as a form of
resistance to various forms of oppression including economic, cultural, gender and
sexual (El Ansari and Phillips 2001).
9. The views and decisions of service-users are powerful and add credit and worth to
any service, influencing both professional staff and management and can be an
invaluable asset in enabling change (Ainsworth 2003).
39
Strategic Partnership Guide
10. (Linhorst and Eckert (2002) and O’Donnell and Entwistle (2004) suggest:
It should be a matter of principal and an ethical requirement in the philosophy of
partnership working that the service user, as a major stakeholder in the success of
any intervention, should be evaluating it from an experiential view point as only they
know what it is like to live with a particular health condition.
Service-users might highlight areas of importance to them thus influencing policy
development which professionals and others have not considered at all or thought to
be of low priority.
Understanding between stakeholders can be greatly improved as each acknowledges
the role of the other thus increasing quality in the service delivery. Professionals in
particular will be made more aware of how their work might improve the lives of
people with a particular health condition.
11. The very act of being involved is of huge benefit to the individual service-users in
terms of increased self-esteem, development of new skills, increasing motivation,
possible financial gain if they are to be paid as equal members of the team.
Involvement may break down barriers and reduce the fear of contacting and using
mental health services (Pathways Report 2002).
12. Services are delivered to the public and are paid for by the public and therefore it is
only proper that the public influence the agenda and have a say in the processes.
Partnership working gives greater transparency to service delivery and makes them
more accountable to the community they are being provided for (O’Donnell and
Entwistle 2004).
4.2.3 Engaging appropriate partners 1
In a study conducted by Alison Summers in 2003 in the UK, psychiatrists were found to
cluster in 3 groups in relation to their attitudes to people with mental health difficulties
as partners:
• Optimists thought that users and professionals have different but equally important
perspectives, neither of which should take precedence,
40
National Disability Authority
“I think that in practice professionals do often prevail but that is not necessarily always
how it should be.”
They stated that success requires that users’ views are properly attended to through
flexible systems and that service user involvement is useful in and of itself, irrespective of
the outcome.
• Rationalists though service user involvement was helpful if it provided a specific and
limited contribution, in particular as a source of information to improve services. They
wanted to retain the last word on decisions because of their greater accountability
and greater knowledge and expertise:
“I think that it is good to hear users’ voices but that shouldn’t absolve health authorities
however from making the right decisions rather than the most popular decisions.”
Some suggested that user input be limited to specific topics like ward environment,
to general tasks rather than detailed planning. Most worryingly, the rationalists
thought that service users should not be involved in formulating ideas from scratch or
strategic planning.
“…it was suggested that users could interview staff, that was going too far. I have always
resisted user involvement at directorate level. I don’t suppose that users have to be at
every level.”
“…I think sometimes that people think that the psychiatric services should be entirely led
by what users want and anybody who says anything against that is anti-user.”
• Sceptics thought that service user involvement is unnecessary, even irrelevant to the
process of service development. They had even more extreme and cynical attitudes
than the rationalists in relation to user involvement:
“I don’t think it will be of any benefit to anybody. I really don’t think it will make much of
a difference.”
“…you see most of us are cynical, it’s just another game by the politicians.”
41
Strategic Partnership Guide
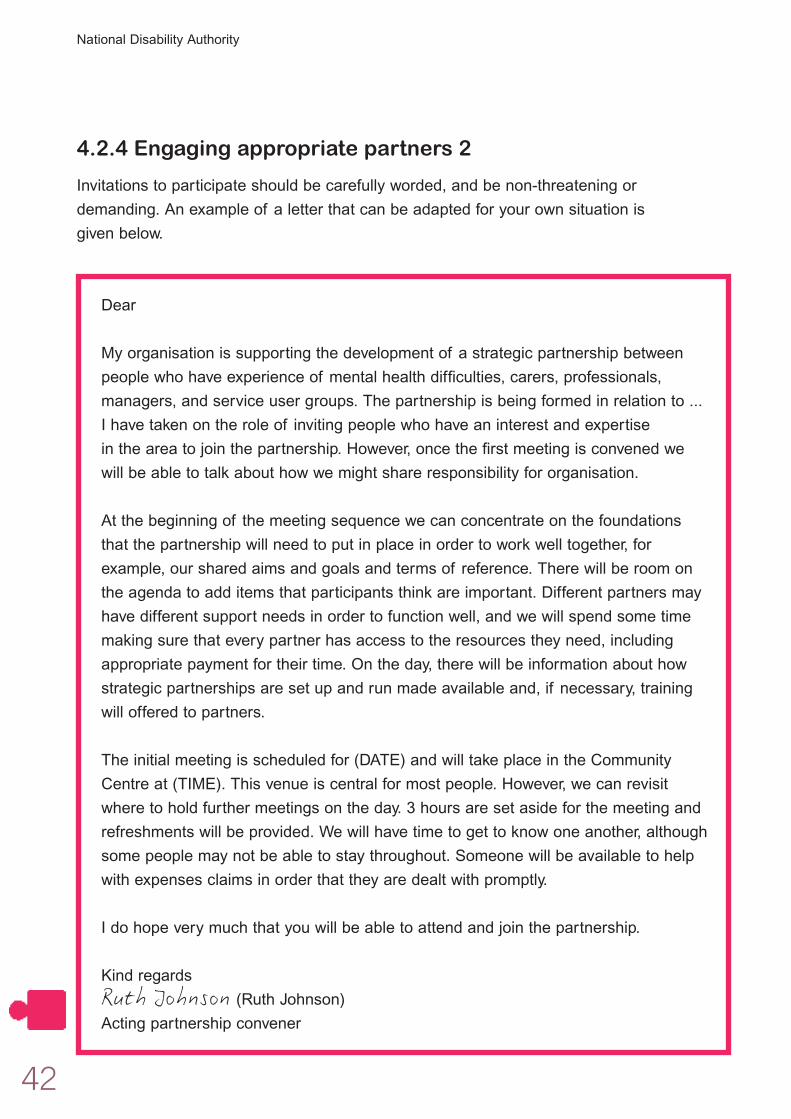
4.2.4 Engaging appropriate partners 2
Invitations to participate should be carefully worded, and be non-threatening or
demanding. An example of a letter that can be adapted for your own situation is
given below.
Dear
My organisation is supporting the development of a strategic partnership between
people who have experience of mental health difficulties, carers, professionals,
managers, and service user groups. The partnership is being formed in relation to ...
I have taken on the role of inviting people who have an interest and expertise
in the area to join the partnership. However, once the first meeting is convened we
will be able to talk about how we might share responsibility for organisation.
At the beginning of the meeting sequence we can concentrate on the foundations
that the partnership will need to put in place in order to work well together, for
example, our shared aims and goals and terms of reference. There will be room on
the agenda to add items that participants think are important. Different partners may
have different support needs in order to function well, and we will spend some time
making sure that every partner has access to the resources they need, including
appropriate payment for their time. On the day, there will be information about how
strategic partnerships are set up and run made available and, if necessary, training
will offered to partners.
The initial meeting is scheduled for (DATE) and will take place in the Community
Centre at (TIME). This venue is central for most people. However, we can revisit
where to hold further meetings on the day. 3 hours are set aside for the meeting and
refreshments will be provided. We will have time to get to know one another, although
some people may not be able to stay throughout. Someone will be available to help
with expenses claims in order that they are dealt with promptly.
I do hope very much that you will be able to attend and join the partnership.
Kind regards
Ruth Johnson (Ruth Johnson)
Acting partnership convener
42
National Disability Authority
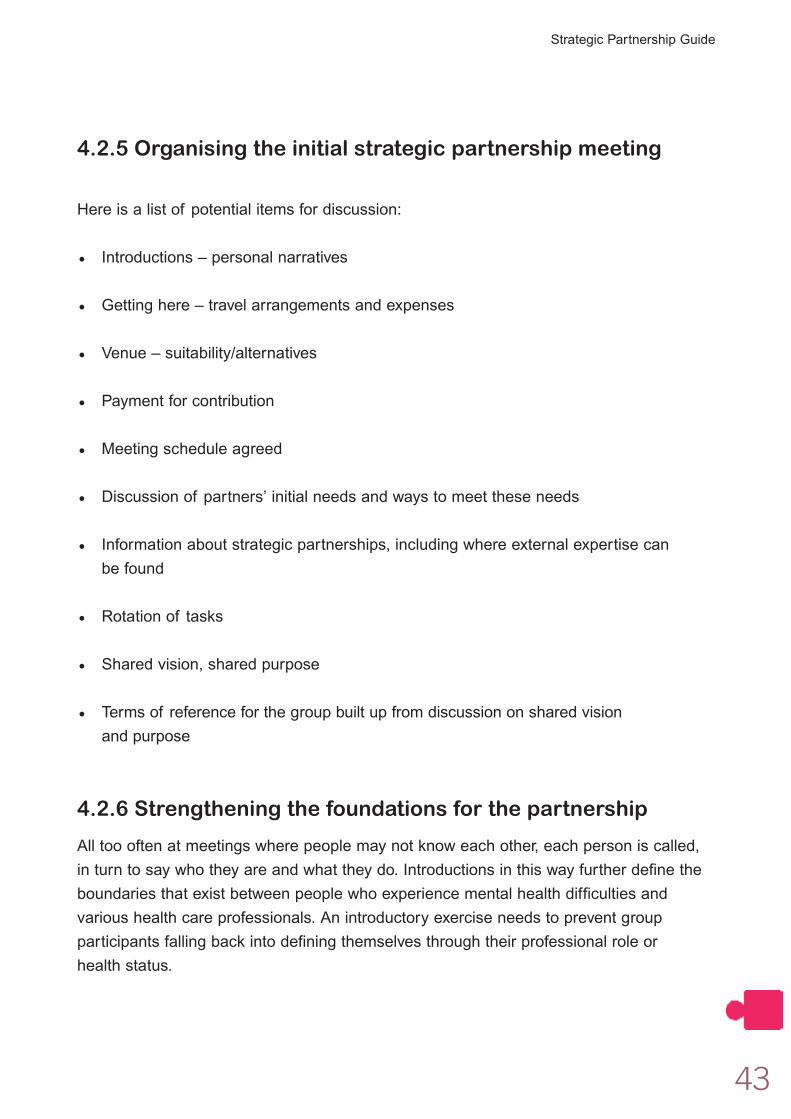
4.2.5 Organising the initial strategic partnership meeting
Here is a list of potential items for discussion:
• Introductions – personal narratives
• Getting here – travel arrangements and expenses
• Venue – suitability/alternatives
• Payment for contribution
• Meeting schedule agreed
• Discussion of partners’ initial needs and ways to meet these needs
• Information about strategic partnerships, including where external expertise can
be found
• Rotation of tasks
• Shared vision, shared purpose
• Terms of reference for the group built up from discussion on shared vision
and purpose
4.2.6 Strengthening the foundations for the partnership
All too often at meetings where people may not know each other, each person is called,
in turn to say who they are and what they do. Introductions in this way further define the
boundaries that exist between people who experience mental health difficulties and
various health care professionals. An introductory exercise needs to prevent group
participants falling back into defining themselves through their professional role or
health status.
43
Strategic Partnership Guide
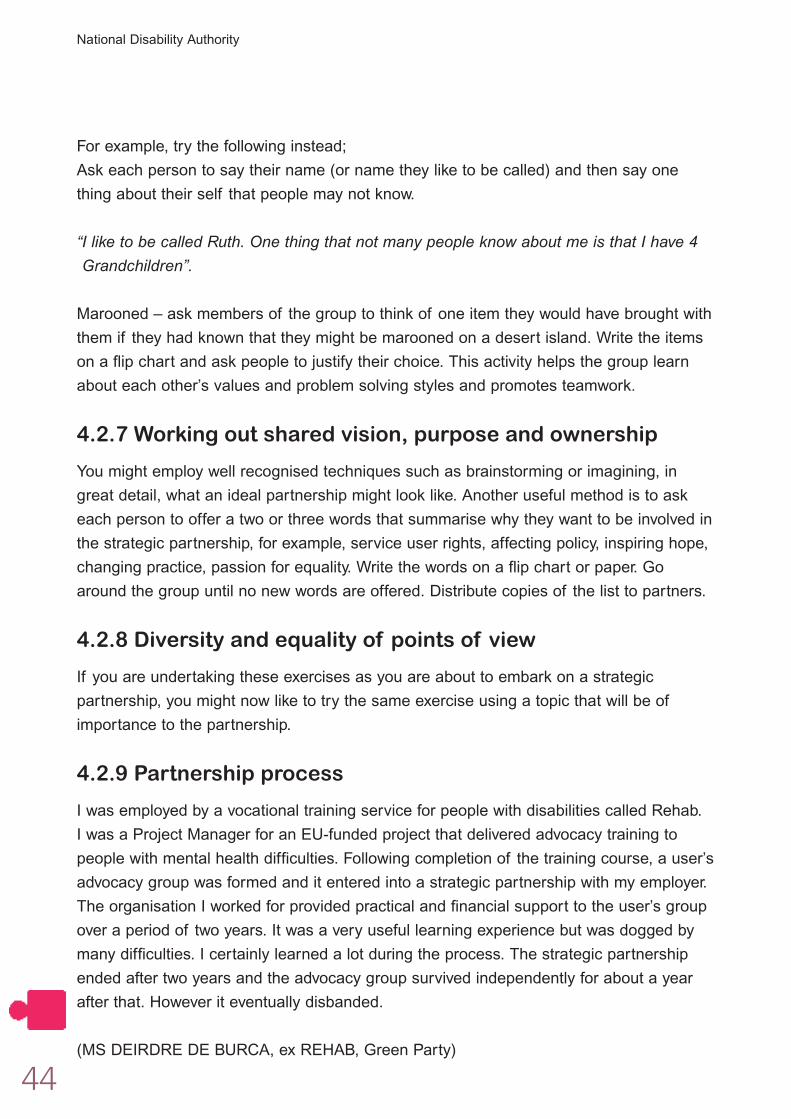
For example, try the following instead;
Ask each person to say their name (or name they like to be called) and then say one
thing about their self that people may not know.
“I like to be called Ruth. One thing that not many people know about me is that I have 4
Grandchildren”.
Marooned – ask members of the group to think of one item they would have brought with
them if they had known that they might be marooned on a desert island. Write the items
on a flip chart and ask people to justify their choice. This activity helps the group learn
about each other’s values and problem solving styles and promotes teamwork.
4.2.7 Working out shared vision, purpose and ownership
You might employ well recognised techniques such as brainstorming or imagining, in
great detail, what an ideal partnership might look like. Another useful method is to ask
each person to offer a two or three words that summarise why they want to be involved in
the strategic partnership, for example, service user rights, affecting policy, inspiring hope,
changing practice, passion for equality. Write the words on a flip chart or paper. Go
around the group until no new words are offered. Distribute copies of the list to partners.
4.2.8 Diversity and equality of points of view
If you are undertaking these exercises as you are about to embark on a strategic
partnership, you might now like to try the same exercise using a topic that will be of
importance to the partnership.
4.2.9 Partnership process
I was employed by a vocational training service for people with disabilities called Rehab.
I was a Project Manager for an EU-funded project that delivered advocacy training to
people with mental health difficulties. Following completion of the training course, a user’s
advocacy group was formed and it entered into a strategic partnership with my employer.
The organisation I worked for provided practical and financial support to the user’s group
over a period of two years. It was a very useful learning experience but was dogged by
many difficulties. I certainly learned a lot during the process. The strategic partnership
ended after two years and the advocacy group survived independently for about a year
after that. However it eventually disbanded.
(MS DEIRDRE DE BURCA, ex REHAB, Green Party)
44
National Disability Authority
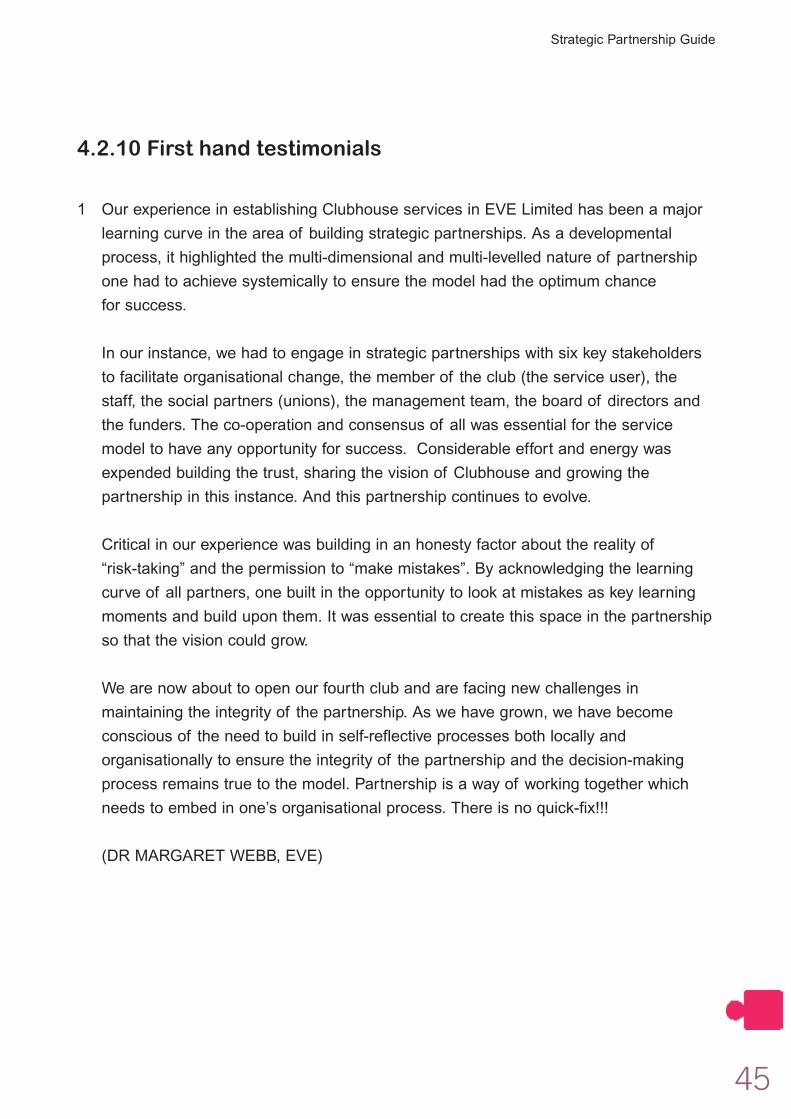
4.2.10 First hand testimonials
1 Our experience in establishing Clubhouse services in EVE Limited has been a major
learning curve in the area of building strategic partnerships. As a developmental
process, it highlighted the multi-dimensional and multi-levelled nature of partnership
one had to achieve systemically to ensure the model had the optimum chance
for success.
In our instance, we had to engage in strategic partnerships with six key stakeholders
to facilitate organisational change, the member of the club (the service user), the
staff, the social partners (unions), the management team, the board of directors and
the funders. The co-operation and consensus of all was essential for the service
model to have any opportunity for success. Considerable effort and energy was
expended building the trust, sharing the vision of Clubhouse and growing the
partnership in this instance. And this partnership continues to evolve.
Critical in our experience was building in an honesty factor about the reality of
“risk-taking” and the permission to “make mistakes”. By acknowledging the learning
curve of all partners, one built in the opportunity to look at mistakes as key learning
moments and build upon them. It was essential to create this space in the partnership
so that the vision could grow.
We are now about to open our fourth club and are facing new challenges in
maintaining the integrity of the partnership. As we have grown, we have become
conscious of the need to build in self-reflective processes both locally and
organisationally to ensure the integrity of the partnership and the decision-making
process remains true to the model. Partnership is a way of working together which
needs to embed in one’s organisational process. There is no quick-fix!!!
(DR MARGARET WEBB, EVE)
45
Strategic Partnership Guide
2 I was involved with a project which became known as the Pathways project. This was
a service user-led piece of research which explored the experiences of users of
Mental Health Services in Galway city. When I became involved in this project I’d been
using the mental health services for over 10 years and had lost faith in myself and
hope in my ability to find meaningful employment again. But this project involving
working with professionals who listened, respected and believed in me and the other
team members, and this support, as well as the affirmation of the other team
members, allowed me rediscover skills and abilities that I’d lost touch with over the
demoralising years of contact with the mental health services. The experience of
working with this project gave me the confidence to apply for and secure meaningful
work at a professional level again.
This project came about because a professional working within West Galway MHS
believed it was important to consult service users about the kind of service they
needed. She secured funding from the service administrator, sought support from the
area development officer working at that time with Schizophrenia Ireland, and another
Occupational Therapy colleague, and got a team of service users involved too. This
project involved strategic partnerships between the statutory mental health service, a
voluntary group, and service users. It was a liberating and empowering, indeed
ultimately life changing, process for me.
(MS LIZ BROSNAN, PATHWAYS PROJECT)
46
National Disability Authority
3 Rehab Group was involved in a Horizon funded project designed to establish an
organisation that represented the views of mental health service users. The project
titled NEART (meaning strength in Irish) was focused upon developing a partnership
with people with mental health difficulties rather than an established representative
organisation.
Interested people with mental health difficulties were invited to a public meeting to
discuss the issue of mental health and service user representation. After the meeting
people were invited to volunteer to join the project. Over 30 people agreed to
participate in an initial phase of capacity building and awareness raising. After a three
month phase of development, twelve individuals opted into a more intense process of
development that included awareness raising, the building of administrative and
organisational skills, advertising and marketing, the development of a formal
organisational structure and charter and an organisational development plan. The
participants chose a name ‘Making Minds Matter’, and an image for the organisation.
Two facilitators were allocated to the project on a part-time basis, both of whom came
from a psychological background.
The organisation operated for a number of years and held several public seminars
with invited speakers. They also carried out a Participant Action Research project into
‘the revolving door’. The organisation attempted to gain mainstreaming resources from
a number of agencies including the Eastern Regional Health Authority and some
charitable donors. Several submissions were made but were unsuccessful. The
Rehab Group continued to provide logistical and practical support to the organisation
until they decided to voluntarily cease operations. At this point the files and research
information generated by the organisation were handed over to the Irish Advocacy
Network, which had developed and grown substantially since the initiation of the
NEART project.
(DR DONAL McANANEY, REHAB GROUP)
47
Strategic Partnership Guide
References and furtherreading
Ainsworth, D. (2003) Patient Involvement – The Derby Theatre Project Experience.
British Journal of Perioperative Nursing, 13 (12): 519-521.
Allen, D. (2000) ‘I’ll tell you what suits me best if you don’t mind me saying’: ‘lay
participation’ in health care. Nursing Inquiry, 7: 182-190.
Anthony, P. and Crawford, P. (2000) Service user involvement in care planning: the mental
health nurse’s perspective. Journal of Psychiatric and Mental Health Nursing, 7: 425-434.
Deegan, P.E. (1992) The independent living movement and people with psychiatric
disabilities: taking back control over our own lives. British Journal of Therapy and
Rehabilitation, 9(2): 52-55.
El Ansari, W. and Phillips, C.J. (2001) Interprofessional collaboration: a stakeholder
approach to evaluation of voluntary participation in community partnerships. Journal of
Interprofessional Care, 15(4): 351-368.
Linhorst, D.M. and Eckert, A. (2002) Involving people with severe mental illness in
evaluation and performance improvement. Evaluation and the Health Professions,
25(3): 284-301.
O’Donnell, M. and Entwistle, V. (2004) Consumer involvement in research projects: the
activities of research funders. Health Policy, 69(2): 229-238.
Pathways Report (2002) Experiences of the East Galway Mental Health Services from
Service Users’ perspectives. The Western Health Board, Schizophrenia Ireland.
Pivik, J., Rode, E. and Ward, C. (2004) A consumer involvement model for health
technology assessment in Canada. Health Policy, 69(2): 253-268.
Summers, A. (2003) Involving users in the development of mental health services:
A study of psychiatrists’ views. Journal of Mental Health, 12(2): 161-174.
Office for Health Management (2002) Public and patient participation in healthcare:
A discussion paper for the Irish health services.
www.officeforhealthmanagement.ie
48
National Disability Authority
FeedbackThe National Disability Authority seeks to promote best practice in all its activities. The
Good Practice Guide will benefit from ongoing evaluation and refinement so that it meets
tomorrow’s needs as well as current ones. Thus, people already engaged in strategic
partnerships might reflect on the contents in relation to their ideas about the future
development of partnership working and suggest different or additional content for the
Guide. We would appreciate it if you, irrespective of how you are using the Guide,
would take some time to tell us of your experience of the Guide by answering the
questions below.
1. How often have you used the Guide in the last year?
2. Which sections of the Guide have you used?
3. Please could you briefly describe the situation in which the Guide was used?
4. What did you find most helpful about the Guide and its contents?
5. Please could you give us any suggestions you may have for improving future
editions of the Guide?
49
Strategic Partnership Guide
6. What other resources would be useful to include in this document?
7. Please could you also give the following information?
Name
Organisation
Position
Date
THANK YOU
Please copy and return these pages to:
National Disability Authority
25 Clyde Road, Ballsbridge, Dublin 4
Tel/Minicom: 01 608 0400
Fax: 01 660 9935
Web: www.nda.ie
email: [email protected]
50
National Disability Authority

51
Strategic Partnership Guide

52
National Disability Authority