69
Strategic Planning Boot Camp – Building a Strategic Plan for the Value Transformation Drs. Angood and Cacchione; and Ms. Jaskie Moderators: Dr. Chazal and Mr. Jacobovitz

Strategic Planning Boot Camp –
Building a Strategic Plan for the
Value Transformation
Drs. Angood and Cacchione; and Ms. Jaskie
Moderators: Dr. Chazal and Mr. Jacobovitz

Disclosures
Peter Angood, MD Nothing to disclose
Joseph G. Cacchione, MD, FACC Consultant Fees/Honoraria: Aim Speciality Health; United
Healthcare Scientific Advisory Board
Richard A. Chazal, MD, FACC Nothing to disclose

Disclosures
Shalom Jacobovitz Officer, Director, Trustee or Other Fiduciary Role: Clene
Nano Medicine
Suzette Jaskie, MBA
Consultant Fees/Honoraria: Boston Scientific Corporation

Disclosures
Howard T. Walpole Jr., MD, MBA, FACC
Salary: Zoll Medical (Spouse)

Agenda
1
2
3
4
5
6
Strategy and the healthcare environment
What does an effective strategy process look like
Physician compensation is a strategic issue
Break
Programs must address these strategic issues
Discussion – Q&A

Strategy and the Healthcare
Environment - Trends
Peter Angood, M.D.
February 18, 2016

8 8

9
A Brave New
World!

1
0
Changing Definition of “Hospital”
More Integration Opportunities
M&A Activity
Physician Integration
Community Coordination
More Risk Management
Increased Accountability
R. Umbdenstock-Healthcare Executive Mar/Apr 2014 (pp.78-79)

1
1
53 Global Health Care CEO’s
Challenges for Future:
Managing Change
Funding Care
Define/Measure Quality
Managing Regulation
Leadership Characteristics:
Innovative
Insightful on Patients
Insightful on Providers
Collaborative
Data Analytics
Humility R. Herzlinger & GENIE

1
2
FSMB Updated Stats Nearly 900,000 licensed physicians in the US (280 physicians/100,000 population)
Avg. age = 51yrs and ~79% are certified by an American Board
2/3 of physicians are Male but…Female physicians increased by 8% in past 2 years
compared with only 2% of male physicians
34% of female physicians are < 39 years
compared with only 18% of male physicians.
Actively licensed physician population grew faster in older population
11% increase those > 60 years vs. 1% increase those < 49 years
26% of physicians are now over age 60 years,
a demonstrable actuarial need for an increased supply of physicians
JMR 2013;99(2):11-24.

1
3
Surge With Physician Employment ~75% increase in number of active physicians employed by hospitals since 2000
~75% of hospital leaders plan to increase physician employment within next 12
to 36 months.
(MGMA Survey)
Share of physician searches for positions with hospitals hit ~75% in 2014
(Merritt Hawkins)
Trend is accelerating => 3 in 10 physicians are now hospital employees
2001 to 2011, # physicians & dentists employed by US hospitals grew by >40%
60% FP & Peds; 50% Surgeons; 25% Surg Spec are employed – not independent
(AHA & AMA)

1
4
Medscape: Employed Doctors Report (~4600 Physicians in 2014)

1
5
Employed or Considering It
1
6
The oldest and largest educational organization solely dedicated to physician leadership
250K educated & currently with 11,000 physician members representing 45 countries
75 expert faculty across dozens of disciplines
Approximately 100 physician leadership courses and several certificate programs
4 Master’s degree programs with more than 1,200 graduates (PhD in development)
More than 21,000 physicians have completed the popular Physician in Management series
More than 2,200 physicians with board certification (Certified Physician Executive)
>220 in-house leadership courses taught each year at hospitals and health systems
More than 3,200 online courses delivered annually
4 major live educational conferences per year
American Association for Physician Leadership
By the Numbers:

1
7
So What Are We Hearing Out There??

1
8

1
9
DiSC Preference Instrument
Total respondents: 2,663 physicians
Forced choice instrument – 28 sets of 4 words:
“most like me”
“least like me”
Statistically validated; some similarity to Myers Briggs

2
0
Conscientious Dominators
Steadiness •Performs
consistently
•Ponders all angles
of any problem
•Likes stability
Dominance •Quick to act
•Likes challenges
•Forceful
Influence •Considers
people first
•Is talkative
•Likes to meet
new people
Conscientiousness •Gathers data
before acting
•Is precise
•Likes to be perfect
14%
29%
50%
7%

2
1
BMC Health Serv Res. 2014; 14: 616.
How physicians identify with predetermined
personalities and links to perceived performance
and wellness outcomes: a cross-sectional study JB Lemaire, JE Wallace

2
2

2
3
MDs vs. Non-MDs as Leaders

2
4
Transformational Leaders: Measurement of Personality Attributes and Work Group Performance High scores on transformational leadership were associated with a distinct personality pattern characterized by higher levels of pragmatism, nurturance, and feminine attributes and lower levels of criticalness and aggression. This enabling pattern formed the core of transformational leadership.
SM Ross, LR Offermann
Personality and Social Psychology Bulletin
10/1997; 23(10):1078-1086.

2
5

2
6
Physicians as Hospital Leaders How are hospitals and health systems different when run by physicians?
Better understanding on nature of challenges & common knowledge base
Improved understanding of patient care operational issues
Unwilling to compromise quality/safety/labor for profit
Finance as a means not an end
Aligning differing values (RNs, PHAs, DOCs, etc.) & improved interactions
Greater value on physician leadership, compensate appropriately
Anticipate change within health care industry and selectively embrace new technologies/methods, e.g., new trends, governmental regulation
Better coordination with referral sources (private offices/clinics)
Less duplication of similar services within region, more collaboration among local hospitals
Greater insight into clinical/patient care activity on local and regional level
(Kearns et al - Physician Executive Journal, Jan/Feb 2009)

2
7
Physicians as Hospital Leaders Rank Organization State Name of CEO/Presdient Physician?
1 Johns Hopkins Hospital MD Paul B. Rothman Yes
2 Massachusetts General Hospital MA Peter Slavin Yes
3 Mayo Clinic MN John H. Noseworthy Yes
4 Cleveland Clinic OH Delos M. Cosgrove Yes
5 UCLA Medical Center CA David T. Feinberg Yes
6 Northwestern Memorial Hospital IL Dean M. Harrison No
7 New York-Presbyterian University Hospital of Columbia and Cornell NY Steven J. Corwin Yes
8 UCSF Medical Center CA Mark R. Laret No
9 Brigham and Women's Hospital MA Elizabeth G. Nabel Yes
10 UPMC-University of Pittsburgh Medical Center PA Jeffrey A. Romoff No
11 Hospital of the University of Pennsylvania PA Ralph W. Muller No
12 Duke University Medical Center NC Victor J. Dzau Yes
13 Cedars-Sinai Medical Center CA Thomas M. Priselac No
14 NYU Langone Medical Center NY Robert I. Grossman Yes
15 Barnes-Jewish Hospital/Washington University MI Richard Liekweg No
16 IU Health Academic Center IN Dan Evans No
17 Thomas Jefferson University Hospital PA Stephen K. Klasko Yes
18 University Hospitals Case Medical Center OH Thomas F. Zenty III No
U.S. News Best Hospitals 2013-14: the Honor Roll

2
8
Physicians as Hospital Leaders
Among the nearly 6,500 hospitals in the United States, only 235 are run by physicians
(2009 - Academic Medicine)
Overall hospital quality scores 25% higher when doctors ran the hospital, compared with other hospitals.
For cancer care, doctor-run hospitals posted scores 33% higher scores
Physician-Leaders and Hospital Performance: Is There an Association?
(Goodall July 2011 - Social Science and Medicine)

2
9
ACOs – MSSP (CMS: 1/30/14)
367 groups of providers formed ACOs
5.3 million Medicare patients serviced (1 in 8)
115,000 US doctors involved in some way (LEAVITT PARTNERS)
First class of ACOs saved $380 million
Of 114 ACOs in the program, 54 ACOs saved money and 29 saved enough to receive bonus.
21 of 29 successful ACOs with received bonuses were physician-led.

3
0
(Dreyfus Model)
3
1
Where is Cards…Where are YOU

What Does an Effective
Process Look Like?
Joseph Cacchione, M.D. FACC
Chairman, Strategic Operations HVI
February 18, 2016

1) Does your Organization have a plan?
A. Yes
B. No
2) Are you part of the planning process?
A. Yes
B. No
3) Are you seen as an owner or customer?
• A. Owner
• B. Customer
Question- 1

Important Concepts
• Mission – Who we are?
• Vision – Where are we going?
• Strategy – How are we going to do it?
• Tactics – What are we going to do?

Question - 2
1) Are you aware of these concepts for your
organization?
A. Yes
B. No
C. Don’t care

Strategy
A Working Definition:
Strategy is the process of profitably matching
internal resources with constantly changing
external demands

Five Iron Laws of Strategy
1. History Drives Strategy
2. Focus
3. Innovation
4. Diversification
5. All Growth Will End

Strategy – Nuts & Bolts
• Industry Analysis
• What is our position?
• How do I appeal to my customers?
• How do we organize?

Industry Analysis
• Suppliers
• Buyers
• Rivals (competition)
• Complimentors
• Substitutes(competitors)

Question 3 -Competition
1) Are we different? A. Yes
B. No
2) Is There Excess Capacity in your market, driving
competition?
A. Yes
B. No
3) Switching costs / inertia (are your customers loyal?)
A. Yes
B. No

Tacit Coordination
• Public data
• Concentration in Markets
• Capacity
• Exit Barriers

Elements of Strategic Investment Decision
• Financial Planning – IE ROI
• What are the uncertainties? (sensitivity
analysis)
• Contingency
• Technology Forces
• Market forces

Strategic Investment Decision Tree
• New Product – IE TAVR
• Capacity Expansion – New “OR”
• Shut Down – Close programs within the system
• Sequential Investment

Two Growth Paths
• Incremental, year-to-year sustaining innovations (exploiting
what we know)
– Bringing a better product or service to current customers
• Breakthrough, disruptive innovations (exploring the known
and unknown)
– Finding new customers with product or service offerings that are not
interesting to current customers
Strategic Business Leadership, March 2007

“Scenario Planning”
• A disciplined method for Imagining
• Driving Forces
• Ranges
• Create Scenarios using the portfolio of driving forces
Paul Shoemaker, Scenario Planning: A Tool for Strategic Thinking, 1995

Creativity is an idea (tangible and /or
intangible) that changes a social system
“Creativity is any act, idea or product that changes an
existing domain, or that transforms an existing
domain into a new one. And, the definition of a
creative person is: someone whose thoughts or
actions change a domain, or establish a new domain.
M. Csikszentmihalyi, Creativity, 1996

Combine Facts and Imagination
Facts Narratives
• Observe Reality “Make Believe”
• New Facts “Invent Realities”
• Logic & Deduction “Create Illusion”
Intuition

Strategy Summary
• Does your organization have a plan?
• Are you aware of that plan?
• Are you an owner, constituent, customer or
barrier?
• Does your strategy have an execution plan
and how are you measuring success?

BREAK
Tick-
Tock…

Compensation is a
Strategic Issue
Suzette Jaskie, President
MedAxiom Consulting
February 18, 2016

1) I am employed by a health system?
A. Yes
B. No
2) My compensation plan is based 90% or more on physician
productivity.
A. Yes
B. No
3) My performance is reviewed annually
A. Yes
B. No
Question- 1

ED
Admit Hospitalist
Discharge Primary
Care
PCP
Refer to EP
AF Ablation
PCP
Retain
patient
medical management
Cardiologist
Retain patient
medical
management
Cardiologist
Consult, no procedure
– no follow up
Cardiologist
Refer to EP
No AF Ablation
ANTI-VISION or Blind Operations
CORP-329802-AA July 2015
Is Fee for Service the Culprit or Notion of Clinical Strategy?

Compensation is a strategic issue
Value incentivized healthcare
system creates integrated health
systems.

1) I am involved in either an ACO or a bundled payment
initiative.
A. Yes
B. No
2) My compensation plan has changed since the introduction
of healthcare reform.
A. Yes
B. No
Question- 2

Medical
Management
Primary Care
Medical
Management
Cardiology
Procedure
PROGRAM VISION Based on Clinical
Standards and a Systematic Approach
Diagnosis
Based
Treatment
Requires new skills: Clinical Standardization,
Team based care, Care and transition
management and I.T. integration
And new strategies:
Programmatic approach, Clinical integration, Dyadic
leadership, Ambulatory V.2.0 and Value performance
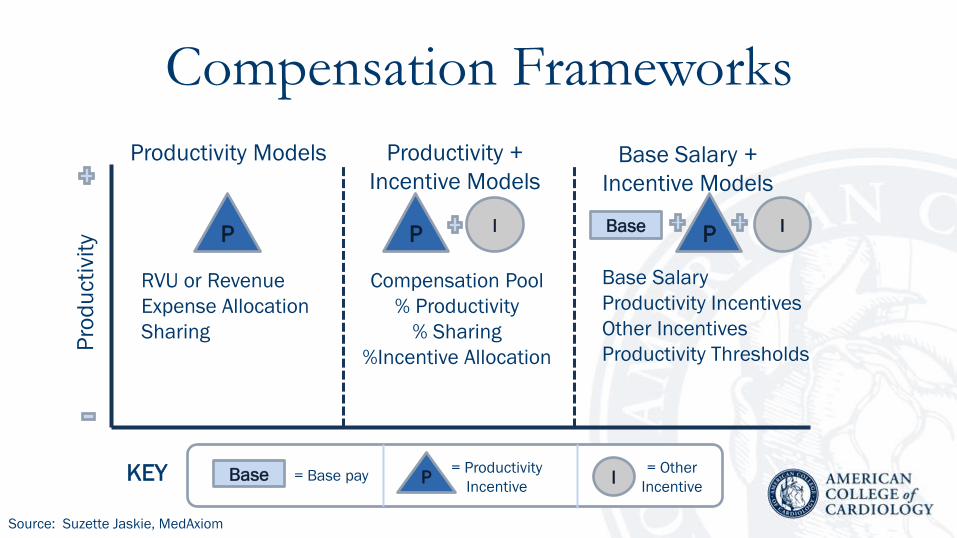
Compensation Frameworks
Base
Productivity Models Productivity +
Incentive Models
Base Salary +
Incentive Models
Pro
du
cti
vit
y
I P = Base pay = Other
Incentive
= Productivity
Incentive
P P I Base P I
KEY
RVU or Revenue
Expense Allocation
Sharing
Compensation Pool
% Productivity
% Sharing
%Incentive Allocation
Base Salary
Productivity Incentives
Other Incentives
Productivity Thresholds
Source: Suzette Jaskie, MedAxiom

Will historical models support transitioning to value based care?
Transforming to
value based care will
require
organizations to
redesign their
delivery models
Traditional models
only value direct
clinical activity
Models based on
productivity have no
connection to
outcomes

Comp and Salary Alignment
Base
Fee-for-Service Transitioning Value
Pro
du
cti
vit
y
I P = Base pay = Other
Incentive
= Productivity
Incentive
P P I Base P I
KEY
RVU Models RVU + Incentive
Models
Base + Incentives
Models
Source: Suzette Jaskie, MedAxiom

DOMAINS Deliverable examples Compensation
Physician participation Leadership participation
Medical director
Program development
Hourly or job
description based fee
Quality based incentives Quality metric improvement
Clinical process improvement
Patient satisfaction
Incentive pool
Operation Bundle coordination
EMR/CPOE functionality
On-start times
Incentive pool
Financial Purchasing
Budget variance
Cost per unit
Multiple
Program Outreach development
Program expansion
Expense support
and/or physician time Po
ten
tia
l C
om
pe
nsa
tio
n I
nce
nti
ves

Other Metric Examples
• Clinical Outcomes
• Readmission rates
• Patient safety
• National quality indicators
• Efficiency/Process
• Standardization
• Length of stay
• Cost per case
• Supply cost
• Documentation
• Patient satisfaction
• Surg/Card coordination
• Program development
• Outreach development
• AUC
• Quality assurance programs

Improvement Goal Incentive
Weighting
Operative Mortality for CABG (Estimated Odds Ratio) 15%
Surgical Re-Exploration (Estimated Odds Ratio) 15%
Prolonged Intubation 10%
Surgical pts Pts given Pre-Operative Beta Blockade 5%
Develop CABG bundle task force and base-line assessment and plan 15%
Reduce OR supply cost 15% 5%
90% adherence to CABG order sets 10%
80% appropriate discharge by 9:00 am daily 10%
Post surgical discharge follow up visit within 7 days 5%
90% of patients enrolled in clinical research protocol 10%
Improvement
incentives are
worth 20% of
physician
compensation
Qu
ality
F
ina
nce
O
PS
S
ts
Rsrc

Summary: • Health systems strategies are generally in pursuit of some aspect of the
Triple Aim
• Achieving the triple aim, or value based healthcare will require a whole-sale
change to care delivery
• Hospitals want & need active physician participation at every level
• Physicians want & need active participation at every level
– Long-term success depends on it
– Creates the best environment for improving quality, cost & service
• Compensation frameworks must be reframed in order to align strategy and
incentives

Key Strategic Issues
Peter Angood, M.D. Joseph Cacchione, M.D. FACC
Suzette Jaskie, President February 18, 2016

CV Delivery Model
1. Will the current delivery model result in high value care?
2. Do I offer my patients programs or services?
3. Have I organized CV delivery that results in the best
possible patient experience?
4. How will MACRA and Value Based Modifier impact the
organization’s revenue stream?

Physician Strategy
1. Is the delivery model organized to maintain physicians in
diagnosis and treatment mode MOST of the time?
2. Do I have the right people on the bus?
3. What is my recruiting and succession strategy?
4. Will the way we evaluate quality and physician
performance be relevant in the future?
5. Is the physician compensation plan aligned with the
organization’s strategy?

Ambulatory Strategy
1. Can I afford my outreach strategy?
2. Do patients and referring physicians have adequate access
to my program?
3. What e-health strategies make sense for my program?
4. Does my ambulatory strategy support growth?
5. Is the program offering the right services in the right
locations?





















