STRESS AND STAFF IN RESIDENTAL SETTINGS: THE MOVE FROM HOSPITAL TO THE COMMUNITY John Rose Slade Hospital Resource Centre, Horspath Driftway, Headington, Oxford Abstract This paper describes a survey of direct care staff in three types of residential accommodation for people with learning disabilities. These were a hospital, community units and group homes. The questionnaire was based on a model of occupational stress developed by Payne (1979). Data was collected upon each individual’s background characteristics, the types of demands, supports and constraints they perceived themselves to be under, and the amount of strain (stress) felt by each person. Replies were received from 34 hospital staff (72% response rate), 47 community unit staff (64%) and 31 group home staff (79%). The results indicate that the hospital and group home staff reported similar, relatively high levels of strain. However, the community unit group reported significantly lower levels. The complex relationship between perceived demands, supports and constraints with strain is discussed. Care needs to be taken in interpreting the data when relating it to the quality of service the resident receives, as no link has yet been shown between this and staff wellbeing. The problems of generalisation are also considered. However, some recommendations are made for further investigations and possible action. Introduction In recent years occupational stress has received a considerable amount of interest in many work settings. There is growing evidence that working in the ‘caring professions’ can be extremely stressful (e.g. Bailey, 1985; Chernis, 1980; Claus & Bailey, 1980; Fletcher & Payne, 1982; Gibson et al., 1989; Hingley & Cooper, 1986; Jones et al., 1991; Marshall, 1980; Payne & Firth- Cozens, 1987). However, there have been relatively few studies of stress and its effects on staff who care for people with learning disabilities. When examining the few studies that have been conducted there are often 0952-9608/93/04 0312-21 $1.80/0 MENTAL HANDICAP RESEARCH 0 1993 J. Rose Vol. 6, No. 4, 1993 312
Transcript
STRESS AND STAFF IN RESIDENTAL SETTINGS: THE MOVE FROM HOSPITAL TO
THE COMMUNITY
John Rose Slade Hospital Resource Centre, Horspath Driftway, Headington, Oxford
Abstract This paper describes a survey of direct care staff in three types of residential accommodation for people with learning disabilities. These were a hospital, community units and group homes. The questionnaire was based on a model of occupational stress developed by Payne (1979). Data was collected upon each individual’s background characteristics, the types of demands, supports and constraints they perceived themselves to be under, and the amount of strain (stress) felt by each person. Replies were received from 34 hospital staff (72% response rate), 47 community unit staff (64%) and 31 group home staff (79%). The results indicate that the hospital and group home staff reported similar, relatively high levels of strain. However, the community unit group reported significantly lower levels. The complex relationship between perceived demands, supports and constraints with strain is discussed. Care needs to be taken in interpreting the data when relating it to the quality of service the resident receives, as no link has yet been shown between this and staff wellbeing. The problems of generalisation are also considered. However, some recommendations are made for further investigations and possible action.
Introduction
In recent years occupational stress has received a considerable amount of interest in many work settings. There is growing evidence that working in the ‘caring professions’ can be extremely stressful (e.g. Bailey, 1985; Chernis, 1980; Claus & Bailey, 1980; Fletcher & Payne, 1982; Gibson et al., 1989; Hingley & Cooper, 1986; Jones et al., 1991; Marshall, 1980; Payne & Firth- Cozens, 1987). However, there have been relatively few studies of stress and its effects on staff who care for people with learning disabilities.
When examining the few studies that have been conducted there are often
0952-9608/93/04 0312-21 $1.80/0 MENTAL HANDICAP RESEARCH
0 1993 J . Rose Vol. 6, No. 4, 1993
312
STRESS AND STAFF 313
difficulties in interpreting them. For example, Thomson (1987) surveyed a range of professional groups working in a variety of settings. This variety can make interpretation of results difficult. She also simply asked respondents to rate how stressful they found their work. Fletcher (1991) argues that people do not generally have reliable insights into their strain (stress) levels or the causes of stress.
There are a few studies that give some insight into occupational stress in this group. Power & Sharpe (1988) showed that nurses working in a hospital for people with learning disabilities were subject to very different stressors from hospice nurses. These included workload, conflict with other nurses and the nursing environment.
Most studies of stress have been conducted in the United States and have concentrated on staff who work in hospitals (Canton et al., 1988; Browner et af., 1987). Both of these studies found a range of factors to be important, organisational factors particularly those related to the design of jobs (underutilisation, lack of control, role conflict) were the most important in these settings.
Fewer studies have examined workers in community settings. One study (Bersani & Heifetz, 1985) found resident related factors to be generally more stressful in community settings than organisational factors. With the continued development of community based services (Malin, 1987) a direct comparison of hospital and community services in important. Allen et al. (1990) attempted to address some of these issues in a comparative study. They concluded that working with people who have learning disabilities was moderately stressful with no significant difference in the degree of stress between hospital and small group homes in the community. However, in this study no clear differentiation was made between various groups of staff with regard to stress. This is important as some roles are very different, for example there are likely to be important differences between direct care workers and managers.
Models of occupational stress
There are many models of occupational stress (e.g. Karasek, 1979; Maslach & Jackson, 1981; Meier, 1983; Motowidlow et al., 1986; Payne, 1979; Van Harrison, 1988; Warr, 1987). Payne (1979) developed the ‘Demands, Supports, Constraints Model’. This model suggests that stress (or more precisely the strain experienced by an individual) will increase as the demands placed on an individual increase. However, if an individual is receiving support to help them cope with the demands this can offset any increase in strain. Both demands and supports can be modified by
314 MENTAL HANDICAP RESEARCH
constraints, negative factors which make coping with demands difficult. This model was chosen for use in this study because it has been used with a large variety of occupational groups (Fletcher & Payne, 1982; Fletcher & Morris, 1987; Jones et al., 1991) including health professionals (Janman et al., 1988; Payne & Firth-Cozens, 1987) and because of the range of factors it considers.
Job design
There have been major changes in the content and nature of jobs in the move from hospital to community settings. The jobs of frontline staff have changed dramatically. As community facilities do not employ cooks, porters, cleaners etc. or have central ordering of supplies, direct care workers in the community are expected to fulfil all of these roles. Their jobs are very different from concentrating on the basic care and teaching performed by staff in the hospital environment. Greater dispersal of residences in the community may increase the autonomy and responsibilities of workers. It could establish a greater group identity and promote teamwork. However, it could also increase isolation and reduce opportunities for support. Job design variables such as these have been shown to have major implications in a variety of settings in terms of health (and consequently levels of strain), turnover rates, job satisfaction etc. (Kemp et al., 1983; Sarata & Jeppesen, 1977; Wall, 1978; Wall & Clegg, 1981). In general, jobs with more autonomy and greater variety promote psychological wellbeing and lower levels of strain. It is possible that this effect may have been achieved on the move to the community. This project sets out to investigate some of these issues.
Method
The sample
It was decided to compare levels of strain and the demands, supports and constraints which influence staff who work directly with residents in a number of environments. Qualified staff (enrolled and registered nurses) were excluded from the survey, as it was felt that their additional management responsibilities may complicate interpretation of the results.
Three work environments were chosen as being representative of current National Health Service provision for people with mental handicaps in the Oxford region. These were a hospital with 150 beds, three community units and eight small group homes. The community units consisted of three
STRESS AND STAFF 315
purpose built, eight bedded bungalows with offices on the same site. The group homes were ordinary houses in ordinary streets, with no more than five residents, operating essentially independently of each other but within two management groups.
There were many similarities between these environments. They were all part of the NHS and managed by qualified nursing staff. Resident characteristics were not assessed but the residents of the community units had moved from a hospital that had recently closed. The majority of the last 150 residents of the hospital had moved into the community units except for children and adults who demonstrated the most severe challenging behaviour. As a consequence of this, specialist facilities on the hospital site for people with challenging behaviour and children were excluded from the study to try to enhance comparability. The majority of residents in the group homes had lived in a small (30 bed) hospital prior to moving.
There were also some important differences. Staff ratios were better in the community but they were not supported by ancilIary staff. As a result staff were expected to perform more tasks with residents e.g. cooking and cleaning. In the hospital there were also permanent night staff, whereas community staff were generally expected to work rotating shifts including some nights. Permanent night staff were excluded from the survey as it was felt their jobs would be significantly different to staff working days. For their extra responsibilities staff in the community were generally paid more (nursing scale B or in some cases C, rather than A in the hospital). Day services in the community were provided by occupational therapists (OTs) working in the houses or taking people directly from the house to community facilities, with a more traditional OT department in the hospital.
Questionnaire
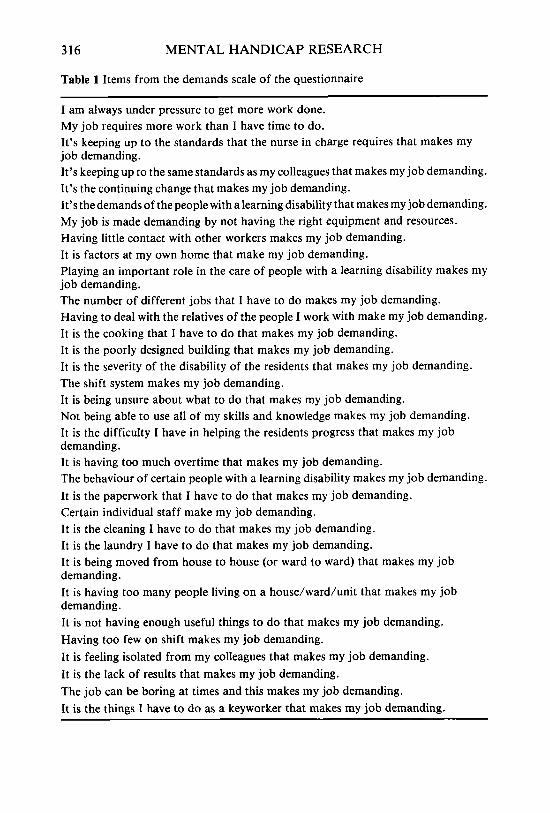
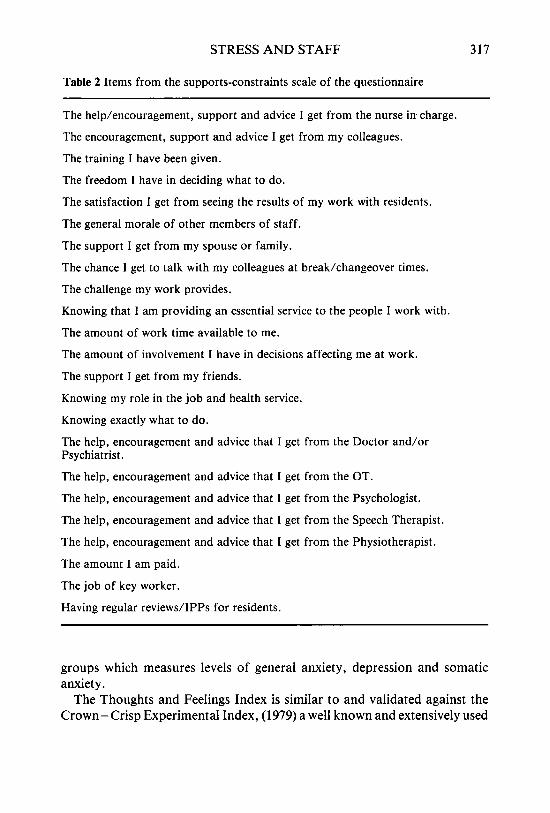
Potential demands, supports and constraints were identified from previous research, informal discussions between the author and staff and the use of a semi-structured interview schedule. Thirty-three demand items and twenty-three support-constraint items were identified. These are listed in Table 1 (demand items) and Table 2 (support/constraint items).
Questions were constructed so that individuals could rate levels of demand on scales from 1 t o 5 . A similar rating scale was used for the supports/constraints items but here ratings of 4 and 5 signified levels of support and 1 and 2 levels of constraint, with 3 being a neutral rating. Strain (stress) was measured using the ‘Thoughts and Feelings Index’ (Fletcher, 1989), a short questionnaire standardised on a number of occupational
316 MENTAL HANDICAP RESEARCH
Table 1 Items from the demands scale of the questionnaire
I am always under pressure to get more work done. My job requires more work than I have time to do. It’s keeping up to the standards that the nurse in charge requires that makes my job demanding. It’s keeping up to the same standards as my colleagues that makes my job demanding. It’s the continuing change that makes my job demanding. It’s the demands of the people with alearning disability that makes my job demanding. My job is made demanding by not having the right equipment and resources. Having little contact with other workers makes my job demanding. It is factors at my own home that make my job demanding. Playing an important role in the care of people with a learning disability makes my job demanding. The number of different jobs that I have to do makes my job demanding. Having to deal with the relatives of the people I work with make my job demanding. It is the cooking that I have to do that makes my job demanding. It is the poorly designed building that makes my job demanding. It is the severity of the disability of the residents that makes my job demanding. The shift system makes my job demanding. It is being unsure about what to do that makes my job demanding. Not being able to use all of my skills and knowledge makes my job demanding. It is the difficulty I have in helping the residents progress that makes my job demanding. It is having too much overtime that makes my job demanding. The behaviour of certain people with a learning disability makes my job demanding. It is the paperwork that I have to do that makes my job demanding. Certain individual staff make my job demanding. It is the cleaning I have to do that makes my job demanding. It is the laundry I have to do that makes my job demanding. It is being moved from house to house (or ward to ward) that makes my job demanding. It is having too many people living on a house/ward/unit that makes my job demanding. It is not having enough useful things to do that makes my job demanding. Having too few on shift makes my job demanding. It is feeling isolated from my colleagues that makes my job demanding. It is the lack of results that makes my job demanding. The job can be boring at times and this makes my job demanding. It is the things I have to do as a keyworker that makes my job demanding.
STRESS AND STAFF 317
Table 2 Items from the supports-constraints scale of the questionnaire
The help/encouragement, support and advice I get from the nurse i n charge.
The encouragement, support and advice I get from my colleagues.
The training I have been given.
The freedom I have in deciding what to do.
The satisfaction I get from seeing the results of my work with residents.
The general morale of other members of staff.
The support I get from my spouse or family.
The chance 1 get to talk with my colleagues at break/changeover times.
The challenge my work provides.
Knowing that I am providing an essential service to the people I work with.
The amount of work time available to me.
The amount of involvement I have in decisions affecting me at work.
The support I get from my friends.
Knowing my role in the job and health service.
Knowing exactly what to do.
The help, encouragement and advice that I get from the Doctor and/or Psychiatrist.
The help, encouragement and advice that I get from the OT.
The help, encouragement and advice that I get from the Psychologist.
The help, encouragement and advice that I get from the Speech Therapist.
The help, encouragement and advice that I get from the Physiotherapist.
The amount I am paid.
The job of key worker.
Having regular reviews/IPPs for residents.
groups which measures levels of general anxiety, depression and somatic anxiety.
The Thoughts and Feelings Index is similar to and validated against the Crown-Crisp Experimental Index, (1979) a well known and extensively used
318 MENTAL HANDICAP RESEARCH
measure. The Thoughts and Feelings Index has been used in studies of stress amongst clergy and social workers (Fletcher, 1991; Jones et al., 1991). The maximum score on each of the three scales is 16. A score of 12 or more is taken as giving rise to concern about psychological health, a score of 11 or 12 being marginal. These cut off scores are derived from a comparative validation study. A score corresponding to 12 + on the scales differentiated between ‘normal’ groups and groups of patients with psychoneurotic illness (Crown & Crisp, 1979).
Information was also collected about background characteristics such as age and marital status.
Questionnaires were distributed individually to staff where possible and the purpose of the survey was explained. They were asked to return them anonymously by post. In the hospital 47 staff were given the questionnaire of which 34 were returned (72%) with 47 out of 74 staff (64%) returning questionnaires in the community units and 31 out of 39 in the small group homes (79%).
Turnover
Turnover rates were extracted from personnel records where possible. These were calculated as described by Mercer (1979) as a crude separation rate equivalent to the labour turnover rate of Baumeister & Zaharia (1987). Rates were calculated for the staff in the units for the financial year in which the survey was conducted.
Results
When their questionnaire replies were compared using the Chi-squared test all three groups of staff were found to be generally similar in their background characteristics.
However, length of service was significantly longer in the hospital but this could have been expected as the hospital had been open for 20 years, the community facilities no more than five. There was also a difference in age of staff between the small group homes and community units, caused by an apparent policy (unwritten) of not recruiting people under 20 for work in the small group homes.
STRESS AND STAFF 319
Levels of strain
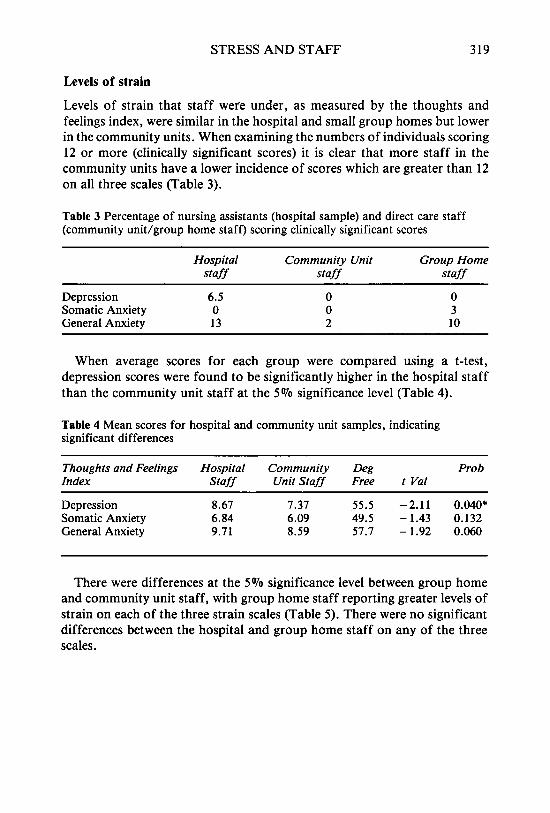
Levels of strain that staff were under, as measured by the thoughts and feelings index, were similar in the hospital and small group homes but lower in the community units. When examining the numbers of individuals scoring 12 or more (clinically significant scores) it is clear that more staff in the community units have a lower incidence of scores which are greater than 12 on all three scales (Table 3).
Table 3 Percentage of nursing assistants (hospital sample) and direct care staff (community unit/group home staff) scoring clinically significant scores
Hospital Community Unit Group Home staff staff staff
Depression 6.5 Somatic Anxiety 0 General Anxiety 13
0 0 2
0 3 10
When average scores for each group were compared using a t-test, depression scores were found to be significantly higher in the hospital staff than the community unit staff at the 5 % significance level (Table 4).
Table 4 Mean scores for hospital and community unit samples, indicating significant differences
~~~ ~
Thoughts and Feelings Hospital Community Deg Prob Index Staff Unit Staff Free t Val
There were differences at the 5% significance level between group home and community unit staff, with group home staff reporting greater levels of strain on each of the three strain scales (Table 5) . There were no significant differences between the hospital and group home staff on any of the three scales.
320 MENTAL HANDICAP RESEARCH
Table 5 Mean scores for group home community unit samples, indicating significant differences
Thoughts and Feelings Hospital Community Deg Prob Index Staff Unit Staff Free t Val
Overall turnover rates were 27% in the hospital, 15% in the community units and 24% in the group homes.
Demands
The top five demands for each group, with mean ratings, are shown in Table 6. In general community unit staff rated demands lower than the staff who worked in the small group homes who rated demands generally lower (but not always and with some exceptions) than the hospital staff.
Table 6(a) Top five demands rated by the hospital staff
Demand Mean Rating
(1) Having too few staff on shift (2) Not having the right equipment or resources (3) The continuing change (4) The behaviour of certain residents. ( 5 ) The job of keyworker
4.34 4.03 3.73 3.41 3.41
Table 6(b) Top five demands rated by the community unit staff
Demand Mean Rating
(1) Having too few staff on each shift 3.49 (2) Not having the right equipment or resources 3.45 (3) The job requires more work than there is time to do it in. 3.26 (4) The continuing change 3.12 (5) The shift system 3.07
STRESS AND STAFF 321
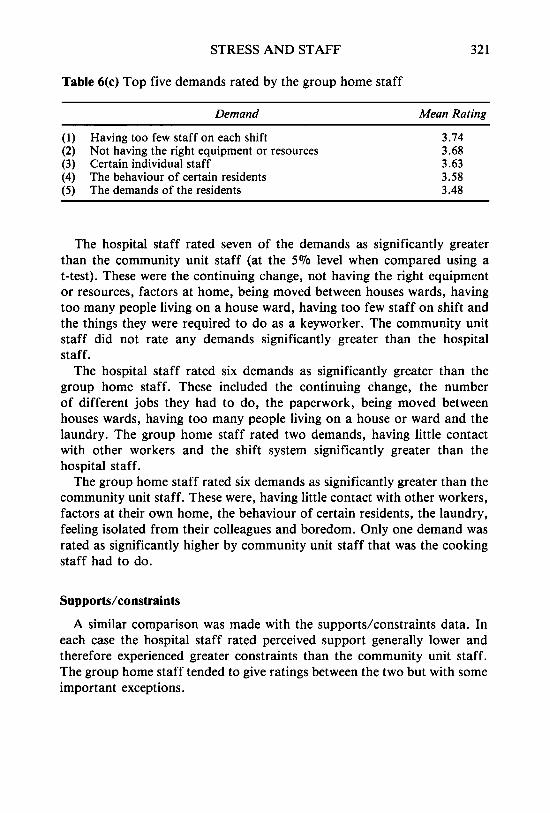
Table 6(c) Top five demands rated by the group home staff
Demand Mean Rating
(1) Having too few staff on each shift 3.74 (2) Not having the right equipment or resources 3.68 (3) Certain individual staff 3.63 (4) The behaviour of certain residents 3.58 (5) The demands of the residents 3.48
The hospital staff rated seven of the demands as significantly greater than the community unit staff (at the 5 % level when compared using a t-test). These were the continuing change, not having the right equipment or resources, factors at home, being moved between houses wards, having too many people living on a house ward, having too few staff on shift and the things they were required to do as a keyworker. The community unit staff did not rate any demands significantly greater than the hospital staff.
The hospital staff rated six demands as significantly greater than the group home staff. These included the continuing change, the number of different jobs they had to do, the paperwork, being moved between houses wards, having too many people living on a house or ward and the laundry. The group home staff rated two demands, having little contact with other workers and the shift system significantly greater than the hospital staff.
The group home staff rated six demands as significantly greater than the community unit staff. These were, having little contact with other workers, factors at their own home, the behaviour of certain residents, the laundry, feeling isolated from their colleagues and boredom. Only one demand was rated as significantly higher by community unit staff that was the cooking staff had to do.
Supports/constraints
A similar comparison was made with the supports/constraints data. In each case the hospital staff rated perceived support generally lower and therefore experienced greater constraints than the community unit staff. The group home staff tended to give ratings between the two but with some important exceptions.
322 MENTAL HANDICAP RESEARCH
Table 7(a) The five highest ranked supports for the hospital staff
Demand Mean Score
Support from spouse and family Knowing that I am providing an essential service Knowing exactly what I have to do The satisfaction received from seeing the results of work with residents Chances to talk with colleagues at break and changeover
4.26 4.25 4.19 4.06
4.06
Table 7(b) The five highest ranked supports for the community unit staff
Support Mean Score
(1) Support from spouse and family 4.54 (2) 4.51
(3) Knowing exactly what I have to do 4.19 (4) Knowing that I am providing an essential service 4.31 (5) 4.19
The satisfaction received from seeing the results of work with residents
Knowing my role in the job and health service
Table 7(c) The five highest ranked supports for the group home staff
Support Mean ~ ~~~
(1) 4.27
(2) Knowing that I am providing an essential service 4.17 (3) Having regular reviews/IPPs 4.04 (4) The training I have been given 3.92 (5) The freedom I have in deciding what to do 3.83
The satisfaction from seeing the results of work with residents
The top five support items for each group are shown in Table 7. The community unit staff rated eleven of the items as significantly more supportive than the hospital staff (all comparisons again using a t-test at 5 % sig level). These included encouragement and help from the nurse in charge, freedom in deciding what to do, satisfaction of working with the residents, morale of other staff, amount of involvement in decision making, knowing their role in the job and health service, amount paid, the job of keyworker, help from the psychologist and help from the doctor. The hospital staff did not rate any items as more supportive than the community unit staff.
The community unit staff rated six items as significantly more supportive
STRESS AND STAFF 323
than the group home staff. These were, support from spouse and family, support from friends, knowing their role in the health service, amount paid, the job of keyworker and knowing exactly what to do. There were no signifi- cant differences in favour of the group home staff with the community unit staff.
The group home staff rated two items as significantly more supportive than the hospital group, these were the amount of involvement in decision making and having regular IPPs/reviews. One item was significantly more supportive for the hospital group who found they knew exactly what to do more than the group home staff.
Not surprisingly, pay was rated as the least supportive or ‘most constraining’ factor by all three groups, but it was significantly less of a problem for the community unit staff. In all groups support from the nurse in charge was rated about half way down the list of supports, but the support received was rated as significantly greater by the community staff. All other professionals (doctor, psychologist, occupational therapist (OT), physio- therapist, speech therapist) were ranked lower on the list of supports. The OT service in both community settings was given similar ratings to that in the hospital. This means that only pay was rated lower than OTs in terms of support by the community staff and theratings given to OTs were lower than other professionals in the community.
Correlations
Correlations were calculated between all of the demands and support/ constraints items with the three scales of the Thoughts and Feelings Index. Significant correlations as identified by Pearson Correlation Coefficients (5% significance level) were examined.
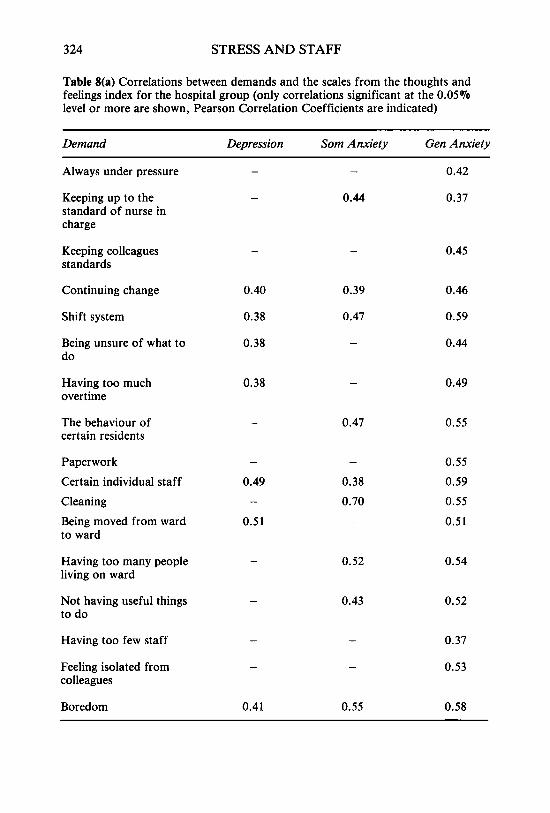
Demands
For the hospital staff 17 demand items correlated significantly and positively with at least one scale (i.e. the greater the demand the greater the strain, Table 8a). Five demand items were positively correlated for both the community unit staff and group home staff (Tables 8b and 8c).
324 STRESS AND STAFF
Table 8(a) Correlations between demands and the scales from the thoughts and feelings index for the hospital group (only correlations significant at the 0.05% level or more are shown, Pearson Correlation Coefficients are indicated)
Demand Depression Som Anxiety Gen Anxiety
Always under pressure
Keeping up to the standard of nurse in charge
Keeping colleagues standards
-
0.44
0.42
0.37
0.45
Continuing change
Shift system
Being unsure of what to do
0.40
0.38
0.38
0.39
0.47
0.46
0.59
0.44
Having too much overtime
0.38 0.49
The behaviour of certain residents
0.47 0.55
Paperwork Certain individual staff C I e a n i n g Being moved from ward to ward
0.55 0.59 0.55 0.51
-
0.49 -
0.51
-
0.38 0.70 -
Having too many people living on ward
Not having useful things to do
0.52 0.54
0.43 0.52
Having too few staff
Feeling isolated from colleagues
0.37
0.53
Boredom 0.41 0.55 0.58
STRESS AND STAFF 325
Table 8(b) Correlations between demands and scales on the thoughts and feelings index for the community unit group (only significant correlations indicated, Pearson correlation coef. shown)
Demand Depression Som Anxiety Gen Anxiety
Always under pressure 0.37 - 0.40
Keeping up the standard of 0.42 - 0.54 nurse in charge
Shift system 0.34 0.36 0.39
Having too much overtime - 0.53 0.33
Paperwork - 0.34 -
Table 8(c) Correlations between demands and scales on the thoughts and feelings index for the group home staff (only significant correlations idicated, Pearson correlation coef. shown)
Demand Depression Som Anxiety Gen Anxiety
Keeping up to standards of 0.45 - - colleagues
Shift system 0.60 0.49 0.42
Being unsure of what to do - 0.41 0.43
Laundry - 0.38 -
Feeling isolated from - colleagues
- 0.39
Supports/ Constraints
For the hospital staff eight support items were significantly negatively correlated (i.e. greater support, lower strain) with at least one scale on the thoughts and feelings index (Table 9a).
Ten items were negatively correlated for the community unit staff (Table 9b). For the group home staff there were five significant negative correlations (Table 9c).
326 MENTAL HANDICAP RESEARCH
Table 9(a) Correlations between supports/constraints and the scales from the thoughts and feelings index for the hospital group (only significant correlations indicated at 0.05% significance level, Pearson Correlation Coef shown)
~~
Support/Constraint Depression Som Anxiety Gen Anxiety
nurse in charge
from colleagues
- - Encouragement, support help from - 0.36
- 0.52 - Encouragement, support advice - 0.40
Training received - 0.53 - 0.43 - 0.45
Morale of other staff - 0.48 - 0.39 - 0.52
- 0.40
- 0.44 - 0.43
- 0.59
Chances to talk with colleagues -0.37 -
Challenge work provides -
Support from friends - 0.45 Knowing exactly what I have to do
-
- - 0.41 -
Table 9(b) Correlations between supports/constraints and the scales from the thoughts and feelings index for the community group (only significant correlations at - 0.05% level shown, Pearson Correlation coef. indicated)
Support/Constraint Depression Som Anxiety Gen Anxiety
nurse in charge Encouragement, support help from - 0.47 - 0.41 - 0.34
Freedom in deciding what I do -0.31 - -
Satisfaction got from seeing results of work with residents
- - - 0.30
- 0.39
- 0.39
- Support from spouse/family - 0.44
Chances to talk with colleagues - 0.37
Challenge work provides - 0.40
Amount of time available - 0.33
Amount of involvement in decisions - 0.59
Support from friends - 0.42
Having regular reviews/IPPs - 0.35
-
- -
- 0.39
- 0.38
- 0.37
-
-
-
- -
STRESS AND STAFF 327
Table 9(c) Correlations between supports/constraints and the scales from the thoughts and feelings index for the group home staff (only significant correlations at 0.05% level shown, Pearson Correlation coef. indicated)
Support/Constraint Depression Som Anxiety Gen Anxiety
- - Support from spouse and family
Challenge the work provides
- 0.42
- - - 0.49
- - Knowing they are providing an - 0.39 essential service
- - Knowing exactly what to do - 0.39
Having regular reviews or IPPs -0.41 - -
Discussion
A number of important methodological considerations need to be taken into account when interpreting these results. These include the relatively small size and restricted nature of the sample. Considerable differences can exist betwen health authorities and even individual units on every conceivable variable e.g. skill mix, managerial style, available support etc. All of these factors could influence the results obtained in a survey of this type and any future surveys.
However these results clearly show that the medium sized community units were a less stressful place for frontline staff to work than either the hospital or small group homes. When comparing the levels of strain measured in this study to other comparable groups, for example, social workers (Jones, Fletcher & Ibetson, 1991), the results obtained in the hospital and group homes were similar. Scores from the community units were rather lower and more comparable to those found in a well functioning company (Fletcher, 1989).
Caution needs to be taken when interpreting results which rely on self report data. However, the results tend to be supported by the turnover data. Turnover has been shown to be related to staff stress, although subject to a large number of other influences (Baumeister & Zaharia, 1987; DeKock et al., 1987). Unfortunately, data on other indicators of stress such as sickness rates were not available. Mean ratings of level of demand were generally related to the strain level reported (i.e. greater perceived demand, greater average strain levels) as were mean levels of support/constraint (i.e. greater
MENTAL HANDICAP RESEARCH
perceived support/lower constraint, the lower the average strain levels), thus providing some support for the demands, supports, constraints model. Clearly, there are similarities in the data from the different staff groups. For example, all three groups perceived the greatest demands to be from not having enough staff on each shift and not having the right equipment or resources. Also, the least supportive or most constraining factor reported by each group was the pay staff received, which is not surprising as this is generally poorly paid work! Other factors were also important to each group, such as knowing they were providing an essential service. These similarities represent features of the work common to all three environments.
There are also many differences between the groups. Examination and analysis of these differences is a complex task, but it is clearly worthwhile since by improving our understanding of these differences it may lead to improved job design, reduce strain levels and improve the quality of service. I will now look more closely at the differences between each group.
Hospital
Organisational factors seemed to be significantly more demanding in the hospital. Hospital staff rated having too many people living on a ward/house as more demanding than did staff working in community settings. This seems reasonable as, on average, at least twice as many people lived on the wards as lived in the community settings. Being moved between wards was also rated by hospital staff as more of a problem than were moves between houses by staff working in community settings. This was a common practice in the hospital when they were short staffed and was clearly disliked. Hospital staff also rated the continuing change as more demanding than did the community staff.
Other items rated more favourably by one of the groups of community staff included the paperwork, IPP system and the job of keyworker. It seems likely that all of these features of the job in the hospital were seen as an extra burden in any already demanding environment. Hospital staff felt they had less freedom in deciding what to do than community unit staff and less involvement in decision making than group home staff. These items probably represent not only physical and geographical differences but also differences in management style, with nurses in the community units rating their managers as significantly more supportive than in the hospital. Interpersonal factors are important for this group of staff. For example, the demands of residents was given a high average rating and was correlated with strain.
STRESS AND STAFF 329
In view of these findings, changes in the organisational structure of the hospital are likely to have the greatest impact on staff stress. Developing autonomy between wards would seem important. One way of doing this would be to restrict movement of staff between wards, this may help to consolidate the role of the ward manager.
Other changes which may have a significant effect would be to change the structure of the jobs in the hospital to make them more like those in the community. That is, to increase the variety of tasks performed by staff and increase their responsibilities. For example, measures such as the closure of central kitchens, so that staff would be expected to go out with residents to buy food, then cook it with them on the ward. Clearly changes like this would have implications for staffing but these could be provided, at least to some extent, by redeployment of staff.
In the hospital, resident care systems such as individual programme plans and the job of keyworker were seen as more demanding and constraining than in the community. In this context procedures need to be easy to implement with some opportunities to help staff identify resource deficiencies.
Community units
While staff in the community units reported less strain than those in the group homes or hospital, they did indicate some difficulties. For example, community unit staff perceived greater demands from the cooking than did the group home staff. This is not surprising as staff would be cooking for a larger group than in the group homes. The relatively high demand rating of the shift system and its correlation with strain levels was also indicative of problems. Since the study was completed this has been addressed by some people electing to work predominantly on nights, thus reducing the need for all staff to work rapidly rotating shifts.
It is possible that the characteristics of residents in community units may account for some of these differences. Indeed, this is the only group where there were no resident related demand features in the top five.
It may be that the diverse role of direct care staff also contributed to lower levels of strain. This would be consistent with many job redesign projects in industry (e.g. Wall & Clegg, 1981).
The overall staff group size in the community units was about 32-36 staff. Examination of staff turnover rates in the USA has led to some tentative conclusions that facilities with a staff group size of about 30 have lower turnover than either larger or smaller facilities (Zaharia & Baumeister, 1978).
330 MENTAL HANDICAP RESEARCH
Group homes
For staff working in the small group homes, isolation from colleagues and having little contact with other workers are seen as much more of a problem than is the case for staff in other settings.
Other results indicate the importance of interpersonal relationships in this setting. That is, both relationships with other staff (certain individual staff was the third most significant demand for this group) and with residents (demands rated fourth and fifth related to residents, but this contrasted with the highest rated support relating to residents).
Care in selecting staff and building effective teamwork would seem particularly important in community settings. Also more attention needs to be given to developing staff and resident relationships.
Recognition of opportunities to meet and discuss work as represented by IPP or review meetings seemed much more important for this group. These may function as times when staff can support each other, but may also give them information and confidence to cope when support is not available.
In general the role of professionals in supporting staff in all three environ- ments seems small. Staff rated help from the doctor, speech therapist, psychologist, physiotherapist and OT well down on the list of supports. The use of professional staff as support needs careful consideration, assuming these staff act as significant supports seems to be problematic.
Nursing managers were generally rated as more supportive than visiting professionals and some correlations were observed but managers were still not high on the list of supports.
Overall, working in group homes did seem to have advantages in that staff valued their freedom in deciding what to do and the amount of involvement the) had in decision making was greater. These findings broadly support those found by Allen et al. (1990) and Bersani & Heifetz (1985).
Acknowledgements
I would like to thank Dr Ben C. Fletcher for his advice and assistance. Also the management of the services for enabling the project to go ahead and the many staff who completed the questionnaires.
References
Allen, P., Pahl, J. and Quine, L. (1990) Care Staff in Transition: The Impact on Staff of Changing Services for People with Mental Handicaps. HMSO: London.
STRESS AND STAFF 33 1
Bailey, R.D. (1985) Coping With Stress in Caring. Oxford: Blackwell. Baumeister, A.A. and Zaharia, E.S. (1987) Withdrawal and commitment of basic-
care staff in residential programmes. In s. Landesman and P. Vietz (eds) Living Environments and Mental Retardation. Washington: American Association for Mental Deficiency (1987).
Bersani, H.A. and Heifetz, L.A. (1985) Perceived stress and satisfaction of direct- care staff members in community residences for mentally retarded adults. American Journal of Mental Deficiency 90, 289- 95.
Browner, C.H., Ellis, K.A., Ford, T., Silsby, J.T. and Yee, C. (1987) Stress, social support and health of psychiatric technicians in a state facility. Mental Retardation 25, 3 1 - 8.
Canton, D. J., Grossnickle, W.F., Cope, J.G., Long, T.E. and Mitchell, C.C. (1988) Burnout and stress among employees at a state institution for the mentally retarded. American Journal of Mental Retardation 93 (3) 300-30.
Chernis, C. (1980) Professional Burnout in Human Service Organisations. New York: Prager.
Claus, K. and Bailey, J. (1980) Living with Stress and Promoting Well-Being. St- Louis: Mosby.
Crown, S. and Crisp, A.H. (1979) Manual for the Crown-Crisp ExperimentalZndex. London: Hodder and Stoughton.
De Kock, U., Felce, D., Saxby, H. and Thomas, M. (1987) Staff turnover in a small group home service: A study of adults with severe and profound mental handicaps. Mental Handicap 15, 97- 101.
Fletcher, B. (C). (1989) The Cultural Audit. An Individual and Organisational Investigation. Cambridge: PSI Publications.
Fletcher, B. (C) (1990) Clergy Under Stress. London: Mowbrays. Fletcher, B. (C). (1991) Work, Stress, Diseaseand Life Expectancy. Chichester: John
Wiley. Fletcher, B. (C) and Morris, D. (1989) The well-being of London licenced taxi drivers
and ‘Knowledge boys’: Self selection or occupationally caused strain? Paper presented to the Third Conference on Health Psychology: ‘Life Styles and Health’, Utrecht University, The Netherlands, June.
Fletcher, B. (C). and Payne, R. (1982). Levels of reported stressors and strain amongst school teachers: Some UK Data. Educational Review 34, (3), 267-78.
Gibson, F., McGrath, A. and Reid, N. (1989) Occupational stress in social work. British Journal of Social Work 19, 1 - 16.
Hingley, P. and Cooper, C.L. (1986) Stress and the Nursing Manager. Chichester: Wiley.
Janman, K. Jones, J.G. Payne, R.L. and Rick, T.J. (1988) Clustering individuals as a way of dealing with multiple predictors in occupational stress research. Behavioural Medicine Spring, 17 - 29.
Jones, F., Fletcher, B. and Ibbetson, K. (1991) Stressors and strains amongst social workers: Demands, supports, constraints and psychological health. British Journal of Social Work, 21,443-69.
Karasek, R.A. (1979) Job demands, job decision latitude and mental strain: Implications for job redesign. Administrative Science Quarterly 24, 285 - 308.
Kemp, N.J. Wall, T.D., Clegg, C.W. and Cordery, J.L. (1983) Autonomous work groups in a greenfield site: A comparative study. Journal of Occupational Psychology 56, 27 1 - 8 1 .
332 MENTAL HANDICAP RESEARCH
Malin, N. (1987) Reassessing Community Care. London: Croom Helm. Marshall, J. (1980) Stress amongst nurses. In C.L.T. Cooper and J.T. Marshall (eds)
Maslach, G. and Jackson, S. (1981) The measurement of experienced burnout.
Meier, S.T. (1983) Towards a theory of burnout. Human Relations 36, 899-910. Mercer, G.M. (1979) The Employment of Nurses: Nursing Labour Turnover in the
NHS. London: Croom Helm. Motowidlow, S.J., Packard, J.S. and Manning, M.R. (1986) Occupational stress: Its
causes and consequences for job performance. Journal of Applied Psychology
Payne, R. (1979) Job demands, supports and constraints. In C. Mackay and T. Cox Responses to Stress: Occupational Aspects. London: International Publishing Corporation.
Payne, R. and J. Firth-Cozens, J. (eds). (1987) Stress in Health Professionals. Chichester: John Wiley and Sons.
Power, K.G. and Sharpe, G.R. (1988) A comparison of sources of nursing stress and job satisfaction among mental handicap and hospice nursing staff. Journal of Advanced Nursing 13, 726-32.
Sarata, B. and Jeppesen, J . (1977) Job design and staff satisfaction in human service settings. American Journal of Community Psychology 5 , 229-36
Thomson, S. (1987) Stress in staff working with mentally handicapped people. In R. Payne and J. Firth-Cozens (eds) Stress in Health Professionals. Chichester: John Wiley.
Wall, T.D. (1978) Job redesign and employee participation. In P. Warr (ed.) Psychology of Work. London: Penguin.
Wall, T.D. and Clegg, C.W. (1981) A longitudinal field study of groupwork redesign. Journal of Occupational Behaviour 2, 3 1-49.
Warr, P.B. (1987) Work Unemployment and Mental Health Oxford: Oxford University Press.
Zaharia, E.S. and Baumeister, A.A. (1978) Technician turnover and absenteeism in public facilities. American Journal of Mental Deficiency 82, 580- 93.
White Collar and Professional Stress. Chichester: John Wiley.